Visual Diagnosis in Emergency Medicine TRAFFIC JAM IN THE DUODENUM: IMAGING AND PATHOGENESIS OF BOUVERET SYNDROME Jeffrey Forris Beecham Chick, MD,* Nikunj Rashmikant Chauhan, MD,* Jacob C. Mandell, MD,* Daniel Andrade Tinoco de Souza, MD,* Ryan James Bair, MD,† and Bharti Khurana, MD* *Department of Radiology, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts and †Department of Radiation Oncology, University of Chicago Medical Center, Pritzker School of Medicine, Chicago, Illinois Reprint Address: Jeffrey Forris Beecham Chick, MD, Department of Radiology, Brigham and Women’s Hospital, 75 Francis Street, Boston, MA 02115 CASE REPORT A 90-year-old woman with a history of cholelithiasis and chronic cholecystitis presented to the hospital with nau- sea, bilious vomiting, and anorexia for 3 days. The patient denied fevers, chills, hematemesis, hematochezia, or me- lena. Physical examination was notable for an uncomfort- able woman with epigastric tenderness. An abdominal radiograph was obtained and demonstrated pneumobilia and an enlarged gastric bubble (Figure 1). Subsequent computed tomography with intravenous contrast material was obtained and demonstrated a gallstone in the proxi- mal duodenum causing gastric distention, consistent with Bouveret syndrome (Figure 2). The patient under- went endoscopic-guided lithotripsy with resolution of symptoms. DISCUSSION Bouveret syndrome, first described in 1896, is gastric out- let obstruction caused by gallstone impaction within the proximal duodenum (Figure 3) (1). In Bouveret syn- drome, cholelithiasis coupled with inflammation leads to cholecystogastric or cholecystoduodenal fistula forma- tion, passage of gallstones into the duodenum, and gastric outlet obstruction (2,3). Presenting symptoms are non-specific and may include nausea, bilious vomiting, abdominal pain, and anorexia (2). Bouveret syndrome tends to occur in Figure 1. Single frontal radiograph of the abdomen demon- strating pneumobilia within the right upper quadrant (solid white arrows) and an enlarged gastric bubble. RECEIVED: 1 March 2013; FINAL SUBMISSION RECEIVED: 6 April 2013; ACCEPTED: 30 April 2013 e135 The Journal of Emergency Medicine, Vol. 45, No. 4, pp. e135–e137, 2013 Copyright Ó 2013 Elsevier Inc. Printed in the USA. All rights reserved 0736-4679/$ - see front matter http://dx.doi.org/10.1016/j.jemermed.2013.04.058
Transcript
The Journal of Emergency Medicine, Vol. 45, No. 4, pp. e135–e137, 2013Copyright � 2013 Elsevier Inc.
Printed in the USA. All rights reserved0736-4679/$ - see front matter
http://dx.doi.org/10.1016/j.jemermed.2013.04.058
RECEIVED: 1 MaACCEPTED: 30 A
Visual Diagnosisin Emergency Medicine
TRAFFIC JAM IN THE DUODENUM: IMAGING AND PATHOGENESIS OF BOUVERETSYNDROME
Jeffrey Forris Beecham Chick, MD,* Nikunj Rashmikant Chauhan, MD,* Jacob C. Mandell, MD,*
Daniel Andrade Tinoco de Souza, MD,* Ryan James Bair, MD,† and Bharti Khurana, MD*
*Department of Radiology, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts and †Department of RadiationOncology, University of Chicago Medical Center, Pritzker School of Medicine, Chicago, Illinois
Reprint Address: Jeffrey Forris Beecham Chick, MD, Department of Radiology, Brigham and Women’s Hospital, 75 Francis Street,Boston, MA 02115
CASE REPORT
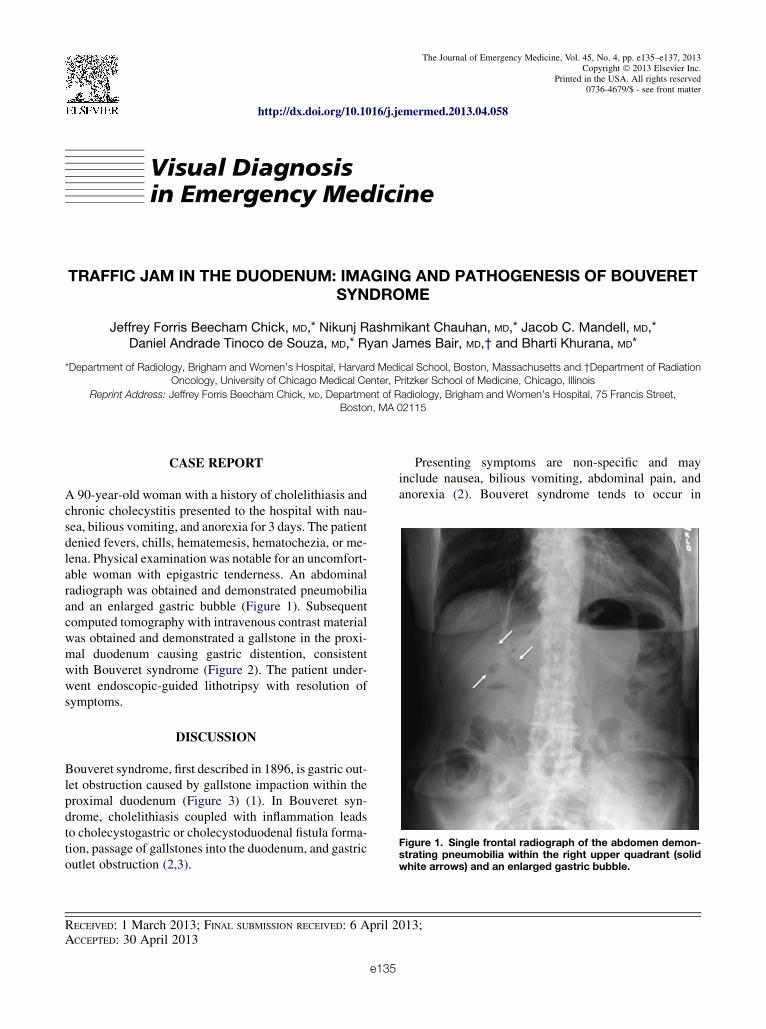
A 90-year-old woman with a history of cholelithiasis andchronic cholecystitis presented to the hospital with nau-sea, bilious vomiting, and anorexia for 3 days. The patientdenied fevers, chills, hematemesis, hematochezia, or me-lena. Physical examination was notable for an uncomfort-able woman with epigastric tenderness. An abdominalradiograph was obtained and demonstrated pneumobiliaand an enlarged gastric bubble (Figure 1). Subsequentcomputed tomography with intravenous contrast materialwas obtained and demonstrated a gallstone in the proxi-mal duodenum causing gastric distention, consistentwith Bouveret syndrome (Figure 2). The patient under-went endoscopic-guided lithotripsy with resolution ofsymptoms.
Figure 1. Single frontal radiograph of the abdomen demon-strating pneumobilia within the right upper quadrant (solidwhite arrows) and an enlarged gastric bubble.
DISCUSSION
Bouveret syndrome, first described in 1896, is gastric out-let obstruction caused by gallstone impaction within theproximal duodenum (Figure 3) (1). In Bouveret syn-drome, cholelithiasis coupled with inflammation leadsto cholecystogastric or cholecystoduodenal fistula forma-tion, passage of gallstones into the duodenum, and gastricoutlet obstruction (2,3).
rch 2013; FINAL SUBMISSION RECEIVED: 6 April 2pril 2013
e135
Presenting symptoms are non-specific and mayinclude nausea, bilious vomiting, abdominal pain, andanorexia (2). Bouveret syndrome tends to occur in
Figure 2. Axial, coronal, and axial images from computed tomography of the abdomen and pelvis with intravenous contrastmaterial demonstrating pneumobilia (solid white arrows), a cholecystoduodenal fistula (dashed white arrows), and a largeimpacted hypoattenuating gallstone within the proximal duodenum (solid red arrows) causing gastric distention suggestive ofgastric outlet obstruction (white asterisks), consistent with Bouveret syndrome.
e136 J. F. B. Chick et al.
elderly women and is associated with a high rate ofmortality (2).
Bouveret syndrome may be suggested by imagingstudies, with diagnosis confirmed by endoscopy. Abdom-inal radiography is uncommonly the primarymodality fordiagnosis, but may demonstrate pneumobilia and a dis-tended stomach. Computed tomography often confirmsthe cholecystoduodenal fistula, impacted gallstone, andgastric outlet obstruction; although the gallstone may beisoattenuating to fluid in 15–25% of cases (4–6).Endoscopy typically reveals the gallstone within theduodenum (2,6).
A variety of endoscopic treatment methods includingstone retrieval, laser lithotripsy, and extracorporealshockwave lithotripsy may be utilized for proximalimpactions, whereas surgery may be necessary for distalobstructions (7,8). Although controversial, fistula repairis unnecessary in the vast majority of cases due tospontaneous fistula closure. In rare cases, however,including persistent symptoms or gallbladdermalignancy, cholecystectomy with surgical fistularepair may be performed (9,10).
REFERENCES
1. Bouveret L. Stenose du pylore adherent a la vesicule [French]. Re-vue Medicale (Paris) 1896;16:1000–11.
2. Cappell MS, Davis M. Characterization of Bouveret’s syndrome:a comprehensive review of 128 cases. Am J Gastroenterol 2006;101:2139–46.
3. Lowe AS, Stephenson S, Kay CL, May J. Duodenal obstruction bygallstone (Bouveret’s syndrome): a review of the literature. Endos-copy 2005;37:82–7.
Figure 3. Multiple schematic diagrams demonstrating thedevelopment of Bouveret syndrome including: cholelithiasis(top panel), gallstone erosion through the gallbladder wall(middle panel), and cholecystoduodenal fistulawith gallstoneimpaction in the proximal duodenum causing gastric outletobstruction (bottom panel). The small black circles in the bil-iary tree indicate pneumobilia (bottom panel).















![[Micro] pathogenesis](https://static.documents.pub/doc/80x56/55a726df1a28ab7e5e8b45a7/micro-pathogenesis.jpg)



