136
Training for health professionals Module – vector borne diseases
| Date post: | 17-Dec-2015 |
| Category: |
Documents |
| Upload: | erick-weaver |
| View: | 216 times |
| Download: | 1 times |

Training for health professionals
Module – vector borne diseases
22
Introduction
• The incidence of vector-borne diseases (VBD) in Europe is much greater than is generally recognized
• As a result, diagnosis and treatment are often delayed
• Health authorities often fail to allocate funding for the surveillance and control
3
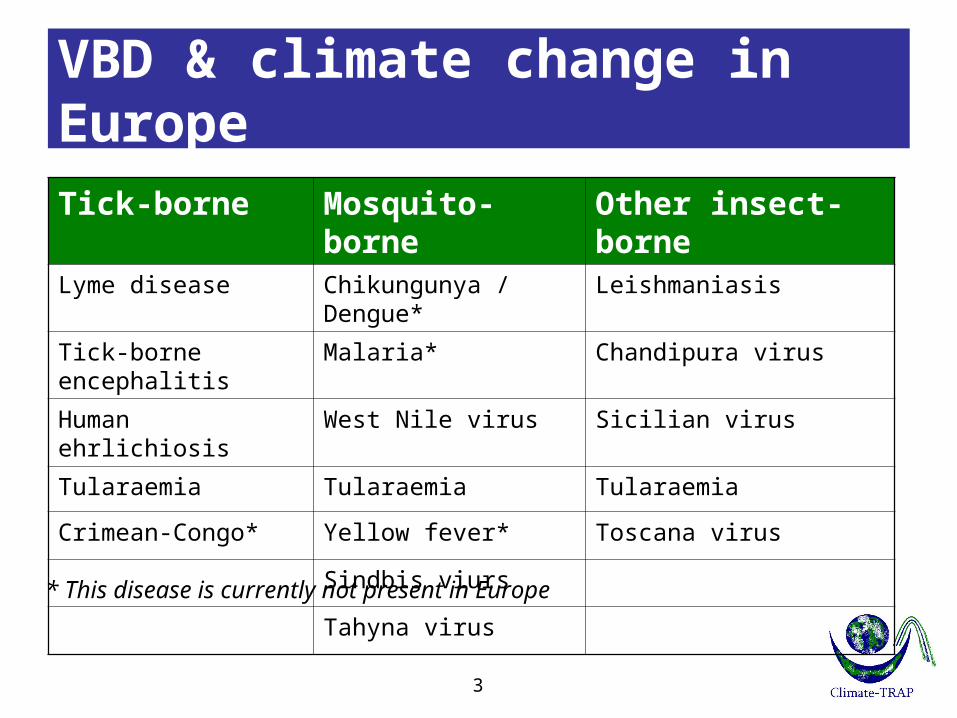
VBD & climate change in Europe
* This disease is currently not present in Europe
Tick-borne Mosquito-borne Other insect-borneLyme disease Chikungunya / Dengue* Leishmaniasis
Tick-borne encephalitis Malaria* Chandipura virus
Human ehrlichiosis West Nile virus Sicilian virus
Tularaemia Tularaemia Tularaemia
Crimean-Congo* Yellow fever* Toscana virus
Sindbis viurs
Tahyna virus

44
Module vector-borne diseases
Training topics
• Tick borne diseases
• West Nile fever (mosquito borne)
• Dengue fever (mosquito borne)
• Chikungunya fever (mosquito borne)
• Leishmaniasis (sandfly borne)

55
Outline training
• Objective• Definitions• Effect climate change on VBD• Specific information for each VBD (top-5)
– Health effects– Current situation– Future situation– Actions needed
• Summary

66
Training objective
• To learn how to be prepared for changes in public health due to climate change
• Take home message– Health impact– Mitigation and adaptation
– Preventive measures on individual & community level
77
Definitions [1]
• Mitigation = reducing the severity of climate change (reducing greenhouse gas concentrations)
• Adaptation = preparing for change (adjusting our systems to reduce harm from climate effects)

88
Definitions [2]
• Vector-borne disease (VBD) = an illness caused by an infectious microorganism (pathogen) that is transmitted to people by a vector, usually arthropods
• Arthropod = an invertebrate animal having an exoskeleton (e.g. insects or arachnids)

• Types of VBD transmission– Anthroponotic infections
• Mosquitoes (Malaria), Ticks (Lyme disease)
– Zoonotic infections• Rodents (plague), Birds (Q-fever)
• Types of VBD transmission– Anthroponotic infections
• Mosquitoes (Malaria), Ticks (Lyme disease)
Definitions [3]
Vector
Humans
Humans
VectorVector Vector
Animals
AnimalsHumans
9

1010
Definitions [4]
• Common (arthropod) vectors– Ticks– Mosquitoes– Sandflies

1111
VBD & climate change
• Climate change will affect the distribution of VBD in three ways: – directly, by the effect on virus/parasite
development and vector competence– indirectly, by the effect on the range and
abundance of the species that act as vectors– indirectly, through socio-economic changes
that affect the amount of human contact with the transmission cycles

12
VBD & climate change
• Most important climate factors– Temperature– Precipitation

13
Temperature effects
• Vector – Survival decrease/increase depending on the
species– Changes in rate of vector population growth– Changes in the susceptibility of vectors to some
pathogens– Changes in feeding rate and host contact

14
Temperature effects
• Example– Summer: more days with high(er) temperature
• Longer lifespan• Longer reproduction period• Longer activity period
– Winter: less days with low temperature• Benefits overwintering• Shorter overwintering
15
Temperature effects
• Pathogen – Decreased extrinsic incubation period of
pathogen in vector at higher temperatures– Changes in the transmission season– Changes in geographical distribution– Decreased viral replication

16
Precipitation effects
• Vector – Survival: increased rain may increase larval
habitat – Excess rain can eliminate habitat by flooding– Low rainfall can create habitat as rivers dry into
pools (dry season mosquitoes)– Decreased rain can increase container-breeding
mosquitoes by forcing increased water storage

17
Precipitation effects
• Vector (continued) – Heavy rainfall events can synchronize vector
host-seeking and virus transmission– Increased humidity increases vector survival
and vice-versa
• Pathogen– Few direct effects but some data on humidity
effects on parasite development
18
Summary effects climate change
• Climate change has the potential to – Increase range or abundance of animal
reservoirs and/or arthropod vectors – Enhance transmission – Increase importation of vectors or pathogens

Module – vector borne diseases
Tick-borne diseases

2020
Tick-borne diseases
• Ticks are a distinct group of mites
• As blood feeding parasites, ticks are able to transmit a wide variety of pathogens
• This may cause tick-borne infections and diseases affecting– Animals– Humans

2121
Tick-borne diseases
• Stages of the tick life-cycle1. Egg
2. Larva
3. Nymph
4. Adult
• Ticks can transmit disease during the three last life-cycle stages.

2222
Tick-borne diseases
• Tick-borne diseases to be aware of in Europe include:– Lyme borreliosis (LB)– Tick-borne encephalitis (TBE)– Tick-borne relapsing fever (TBRF)– Crimean-Congo haemorrhagic fever (CCHF)
2323
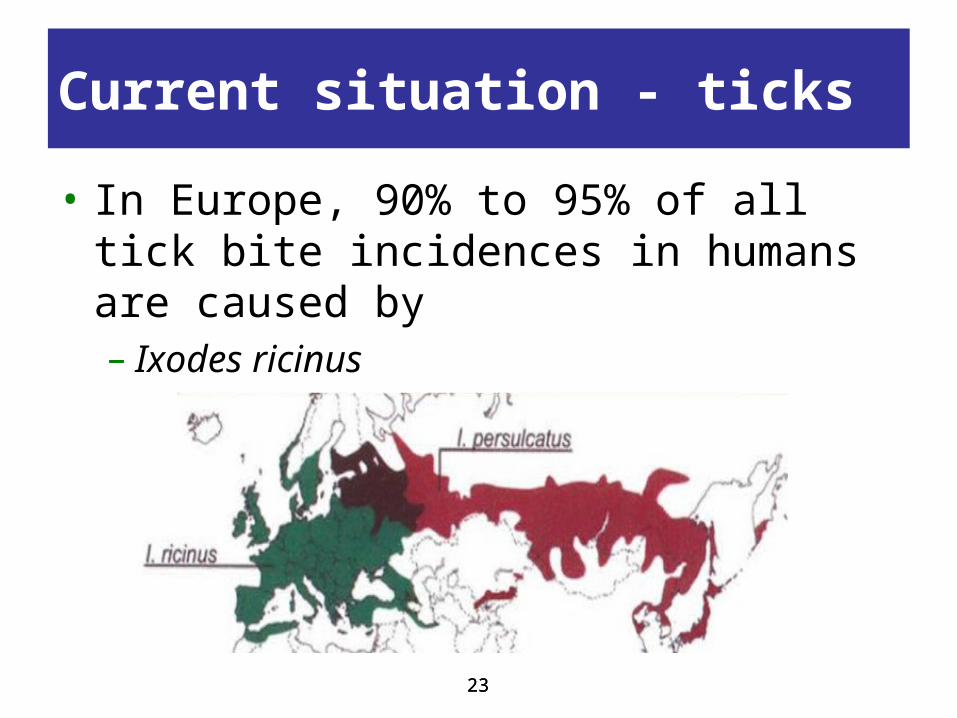
Current situation - ticks
• In Europe, 90% to 95% of all tick bite incidences in humans are caused by– Ixodes ricinus– Ixodes persulcatus

2424
Current situation
• Yearly number of cases in Europe– Lyme borreliosis: ~ 85,000– Tick-borne encephalitis: ~5,000-8,000– Tick-borne relapsing fever: rare– Crimean-Congo haemorrhagic fever:
endemic in Bulgaria since 1950 (‘50-’08: 1,568 cases; 17% mortality), recently new area’s

Climate & ticks
2525
• Climate suitability for the tick I. ricinus - Stable trends

2626
Climate & ticks
• Climate suitability for the tick I. ricinus- Random trends
Future situation ticks
• Climate change– Distribution to higher latitudes and altitudes
• Climate conditions– Temperature
• During summer: temperature > 5-8 ºC• During winter: high enough to continue life cycle
– Humidity• Sufficient to prevent both eggs and ticks from
drying out
27

Tick borne disease
- Lyme borreliosis -

Lyme borreliosis (LB)
• Lyme borreliosis = a bacterial infection caused by member of the genus Borrelia
• Vector borne– Bite by infected tick (B. burgdorferi)– Tick species I. ricinus (Europe)
• Bacteria resevoir host– many species of small mammals– ground-feeding birds
29

LB – health symptoms
• Health symptoms– Local skin rash (80-90% of cases)– Neuroborreliosis (main complication, 10%)– Meningoencephalitis (less common)
• Risk groups– All persons exposed to risk of tick bites are at
risk of becoming infected.
30

LB – geographical distribution
• In Europe, the mean prevalence of B. burgdorferi infected ticks is about 12%
• Regions with highest tick infection rates are located in central Europe– Austria, Czech Republic, Southern Germany,
Switzerland, Slovakia and Slovenia– Nymphs > 10%, adults > 20%
31

LB - available warning systems
• Lyme borreliosis is not a notifiable disease in the European Union (in contrast to USA)
• No licensed vaccine is currently available
• Main methods of preventing infection are avoiding tick bites and early removal of attached ticks.
32
Tick borne disease
- Tick-borne encephalitis -

Tick-borne encephalitis (TBE)
• Tick-borne encephalitis = disease caused by a virus of the Flaviviridae family
• Vector borne– Bite by infected tick– Tick species I. ricinus (Europe)
• Virus reservoir host– Mainly small rodents– Also insectivores and carnivores
34
TBE – transmission mode
• Other transmission modes– By consumption of infected unpasteurised
dairy products.– Not directly from human to human, apart from
mother to the foetus– Laboratory accidents (needle-stick injuries or
aerosol infection)
35

TBE – health symptoms
• Health symptoms– Two third of human TBE virus infections is
asymptomatic– Clinical cases
• 1st fase: nonspecific symptoms (fever, fatigue etc.)• 2nd fase: central nervous system affected
• Several TBE virus infection subtypes– European, Far Eastern, Siberian
36
TBE – health symptoms
• European subtype– Milder compared to other subtypes– 20-30% of patients experiencing the 2nd phase– Severe neurological sequelae in 10% of patients– Mortality rate 0.5-2%
• Risk groups– All persons exposed to risk of tick bites are at
risk of becoming infected.
37

TBE – geographical distribution
• TBE has become a growing public health challenge in Europe and other parts of the world
• The number of human cases of TBE in all endemic regions of Europe has increased by almost 400% in the last 30 years
• The risk areas have spread and new foci have been discovered
38

TBE – geographical distribution
• TBE is present in– Southern Scandinavia– Central and Eastern Europe
• Risk of contracting the disease from a single bite is 1 in 600 in endemic regions
39

40
TBE - available warning systems
• Notifiable disease in 16 European countries, including– 13 European Union (EU) Member States– 3 non-EU Member States
• A vaccine is available
• People at high risk of an infection are vaccinated in Sweden and other countries

Tick borne disease
- Tick-borne relapsing fever -

• TBRF = a bacterial infection caused by member of the genus Borrelia
• Vector borne– Bite by infected tick– Tick species Ornithodoros
• Bacteria reservoir host– Ticks– Small mammals/birds/reptiles/bats
Tick-borne relapsing fever (TBRF)
42

TBRF – health symptoms
• Health symptoms– High fever (> 39-40°C)– Other symptoms include
• Intensive asthenia, headache, arthralgia, myalgia, neck stiffness, stomach ache and nausea.
• Splenomegaly and hepatomegaly, usually associated with jaundice, and elevated pulse and blood pressure are common.
• Following the initial fever episode further relapses will occur
43

TBRF – risk groups
• Two epidemiological types of TBRF have been described:– Sporadic TBRF
• Observed in ‘at-risk’ groups like soldiers, hunters, campers, field workers or travellers
• Developed countries
– Endemic TBRF• Caused by rare but regular contact with infected
ticks directly living in rural human dwellings• Developing countries
44

TBRF – geographical distribution
• The greatest endemic risk in Europe lies in the Iberian Peninsula, particularly in the Mediterranean part, and in Asia Minor
• Reports of imported TBRF cases have come from the UK, Belgium and France
• The number of cases is underestimated because most infections are benign, and no diagnosis is made
45

TBRF – available warning systems
• TBRF is not a notifiable disease in the European Union
• No licensed vaccine is currently available
• Main methods of preventing infection are:– Avoiding tick-infested areas– Avoiding tick bites
46

TBRF – available warning systems
• Main methods of preventing infection (continued)– Removal or decreasing tick vectors and
natural vertebrate reservoirs from buildings• Chemical treatments• Natural predators like domestic cats• Limiting rodent-friendly environments inside and
around buildings
47

Tick borne disease
- Crimean-Congo haemorrhagic fever -
Crimean-Congo haemorrhagic fever (CCHF)• CCHF = a viral infection caused by the
genus Nairovirus, Bunyaviridae family
• Vector borne– Bite by infected tick (nymph or adult)– Tick species Hyalomma
• Virus resevoir host– Immature ticks: hares and hedgehogs– Mature ticks: domestic animals (cattle etc.)
49

CCHF – transmission mode
• Other transmission mode:– direct contact with infected blood or body
fluids– contaminated medical equipment or supply
50

CCHF- health symptoms
• Health symptoms– A sudden onset of febrile illness with
headache, myalgia, backache and joint pain, abdominal pain and vomiting.
– Frequently followed by:• Haemorrhagic manifestations• Necrotic hepatitis may occur• Large ecchymosis and uncontrolled bleeding from
venipuncture sites are common features.
51

CCHF – health symptoms
• Mortality rate of CCHF is ~ 30% with death occuring in the 2nd week of illness
• Risk groups– Farmers, veterinarians and abattoir workers in
endemic areas– Healthcare workers (when nursing CCHF
patients)– Outdoor activities in endemic areas
52

CCHF - geographic distribution
• The geographic range of CCHF virus is known to be the most extensive of the tick borne viruses important to human health.
• In Europe, cases have been reported from Albania, Bulgaria, Kosovo, Turkey and the former Soviet Union
• In Greece, the first human case of CCHF infection was reported 2008
53
CCHF – available warning systems
• CCHF is not a notifiable disease on European Union level
• No validated specific antiviral therapy for CCHF.
• Main methods of preventing infection are:– Avoiding tick-infested areas– Avoiding tick bites
54

CCHF – available warning systems
• Main methods of preventing infection (continued)– Removal or decreasing tick vectors and
natural vertebrate reservoirs from buildings• Chemical treatments• Natural predators like domestic cats• Limiting rodent-friendly environments inside and
around buildings
55

56
Summary – tick borne diseases
• Tick borne disease & climate change– Distribution to higher latitudes and altitudes
• Tick-borne diseases to be aware of in Europe– Lyme borreliosis – Tick-borne encephalitis– Tick-borne relapsing fever– Crimean-Congo haemorrhagic fever

• Public health surveillance at the European level (compulsory notification system in all countries)
• Educate the public on interventions against ticks
• Further research on tick distribution
What actions are needed?
57

Module – vector borne diseases
Mosquitoes borne diseasesWest Nile – Dengue - Chikungunya

5959
Mosquitoes-borne
• This training– Culex mosquitoes West Nile fever– Aedes mosquitoes Dengue fever– Asian Tiger mosquitoes Chikungunya fever
(Aedes albopictus)
Mosquito borne disease
- West Nile fever -

61
West Nile – mosquito borne
• West Nile fever = disease caused by a virus of the Flaviviridae family (West Nile virus, WNV)
• Vector borne– Bites of infected mosquitoes– Culex mosquitoes species
• Virus reservoir host– Birds

– Direct transmission between animals has been seen experimentally
– Infected humans and horses do not seem to spread the virus to other mammals
– Person-to-person transmission has not been reported
– In rare cases, the virus has been spread by blood transfusions, organ transplants, and transplacental transmission
West Nile – transmission mode
62

63
West Nile – health effects
• Asymptomatic infections (~80%)
• Clinical symptoms– Mild
• Flu-like symptoms, including fever, headache and body aches.
• Most uncomplicated infections resolve in 3-6 days– Severe clinical cases
• Neuro-invasive disease: there may be signs of encephalitis, meningo-encephalitis or meningitis.

64
West Nile – health effects
• An estimated 1 out of 140 - 320 infections results in meningitis or encephalitis.
• The case fatality rate in patients with neuro-invasive illness ranges from 4% to 14%; it can reach 15–29% in patients over 70 years old.
• Concurrent disorders such as diabetes or immunosuppression increases the risk of death.
65
West Nile – mosquito borne
• Culex species (Cx. spp.) – Large number of spp. world wide (> 700) – About 20 spp. are present in Europe– Infection and transmission rates are variable
• Example: mosquitoes from the Rhone delta, France
Cx. modestus Cx. pipiens Infection rate: 89.2% 38.5%
Transmission rate: 54.5% 15.8%
66
Current situation
• Worldwide distribution Cx. mosquitoes– Distributed worldwide– They can be found in tropical and temperate
climate zones on all continents except Antarctica
• Europe distribution Cx. mosquitoes– Wetland areas of high biodiversity– Cx. pipiens spp. urban/city dweller
67
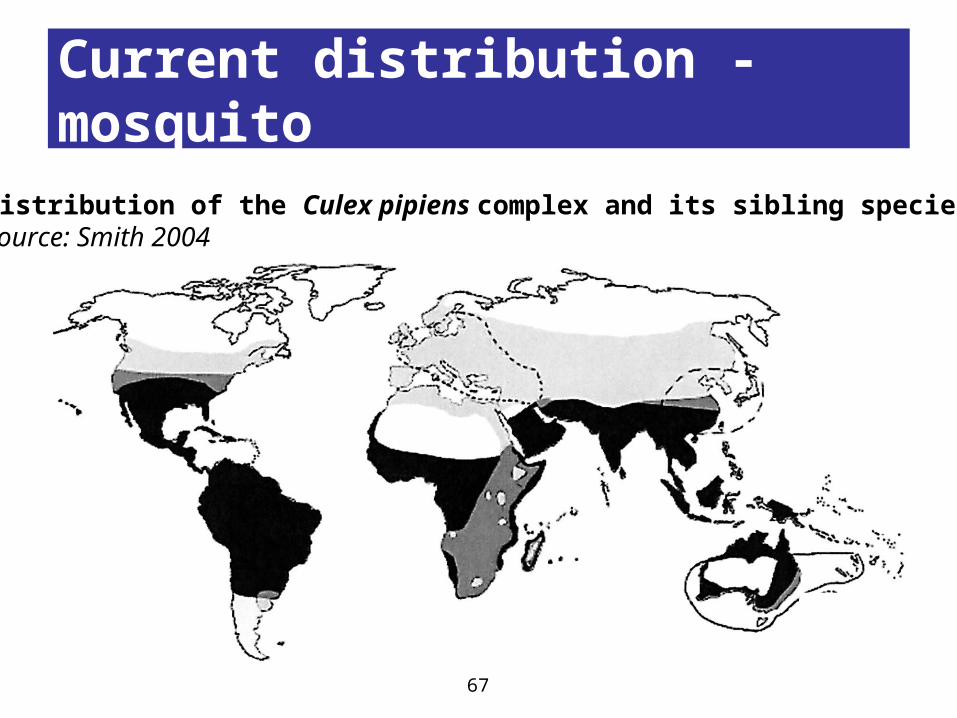
Current distribution - mosquito
Distribution of the Culex pipiens complex and its sibling speciesSource: Smith 2004

68
West Nile – health impact
• West Nile Fever worldwide– West Nile Fever is distributed worldwide– Outbreaks may occur in humans, birds, and horses in
Africa, Europe, Russia, India, and Australia
• West Nile Fever Europe– Erratic and spatially and temporally limited
phenomena– Occurring quite unpredictably, even if all conditions
appear to be present in a definite place

69
West Nile – health impact
• Risk groups– People over 50 years old are at higher risk of
developing severe neurological disease and should take special care to avoid mosquito bites.

70
Current distribution West Nile

71
Available warning systems
Country Control measures
Greece • Enhanced surveillance for human cases
• Adulticiding (ultra-low volume spraying) of mosquitoes in villages with human cases
• Public education campaigns for personal protection
• Education and guidance to school teachers and health care personnel
Romania • Seasonal surveillance for human cases
• Blood safety measures
Turkey • Improved surveillance (active and passive) for human cases
• Inclusion of WNV as a notifiable disease for 2011 season

7272
Available warning systems
• West Nile fever is a notifiable disease in the European Union
• The ECDC is responsible for the surveillance of infectious diseases in the European Union.

7373
Future situation
• Current situation Europe– Autochthonous WNV infections in several
countries during the transmission season
• Future situation & climate change– The dynamics of transmission of WNV are
complex difficult to predict the situation for Europe in the coming years
– Data indicate that the epidemiology of WNV in Europe is changing

7474
What actions are needed? [1]
• Development of a vaccine
• Need for integrated multidisciplinary surveillance systems and response plans
• Raising the awareness of clinicians and veterinarians of the clinical presentation of WNV disease in humans and horses– Particularly during the mosquito season from
June to October– Primarily in areas considered as at major risk
surrounding (irrigated areas and river deltas)

7575
What actions are needed? [2]
• More research to– Suitable habitats for birds that would increase
the bird-mosquito-human interface– Competent vector species– Establish limits around WNV affected areas– Identify potential new at-risk areas– Study the cycle of transmission and the
maintenance of WNV in the environment over the years

Mosquito borne disease
- Chikungunya fever -- Dengue fever -

77
Chikungunya & Dengue
• Chikungunya fever = disease caused by a virus of the Togaviridae family (CHIKV)
• Dengue fever = disease caused by a virus of the Flaviviridae family (dengue virus; DENV)
• Vector borne– Transmitted from human to human by bites of
infected mosquitoes

78
Chikungunya & Dengue
• Vector borne (continued)– Aedes mosquitoes species (both CHIKV and
DENV)
• Virus reservoir host– Humans
• Bites of infected mosquitoes
• Direct contact with infected blood or body fluids
• Contaminated medical equipment or supply
• Can be transmitted from mother to child
Transmission mode
79
Climate change & Aedes mosquitoes
- Chikungunya fever -- Dengue fever -

81
Chikungunya & Dengue
• Aedes mosquito species– Ae. aegypti
• Diurnal biting habits• Once endemic in Europe, disappeared after WWII
– Ae. albopictus (Asian tiger mosquito)• Not host-specific• Present in southern Europe
AegyptiAlbopictus
82
Current situation
• Worldwide distribution Aedes mosquitoes– Climate conditions
• Overwintering conditions: 0°C January isotherm with ≥ 500 mm annual rainfall
• Development: monthly mean temperature ≥ 10°C • Transmission: monthly mean temperature ≥ 20°C
– Risk zones Chikungunya/Dengue fever• Originally, Africa, Southeast Asia, Indian
subcontinent and islands in the Indian Ocean• Increasing presence of Aedes mosquitoes in
Southern Europe new risk zone?
83
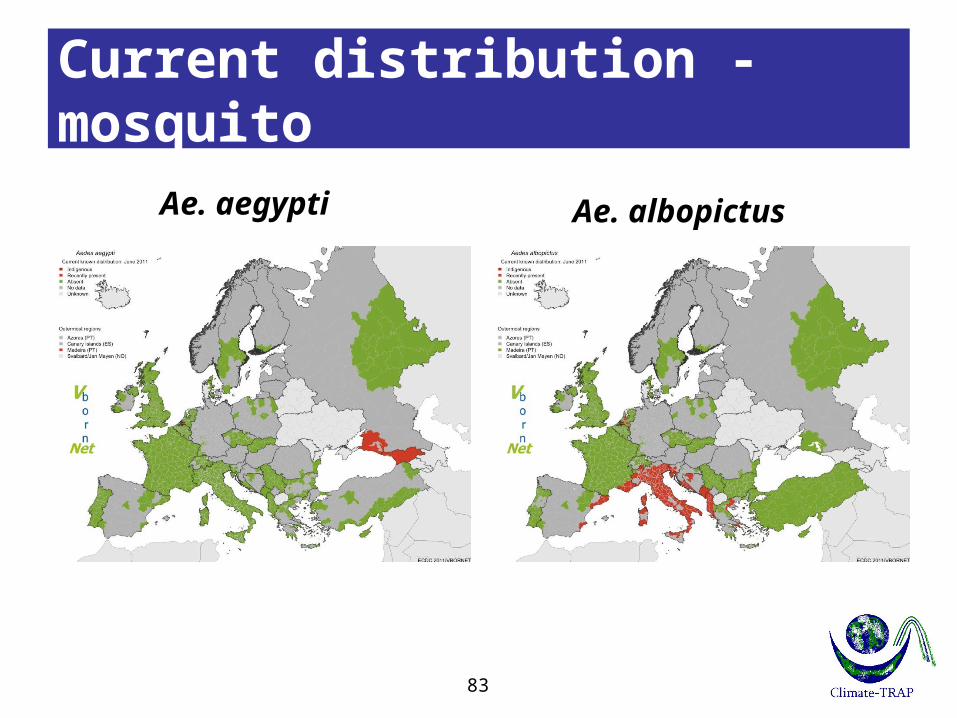
Current distribution - mosquito
Ae. aegypti Ae. albopictus

84
Future situation – minimum impact
Climate change & long term impact on Ae. Albopictus distribution
Year 2030
Year 2030
85
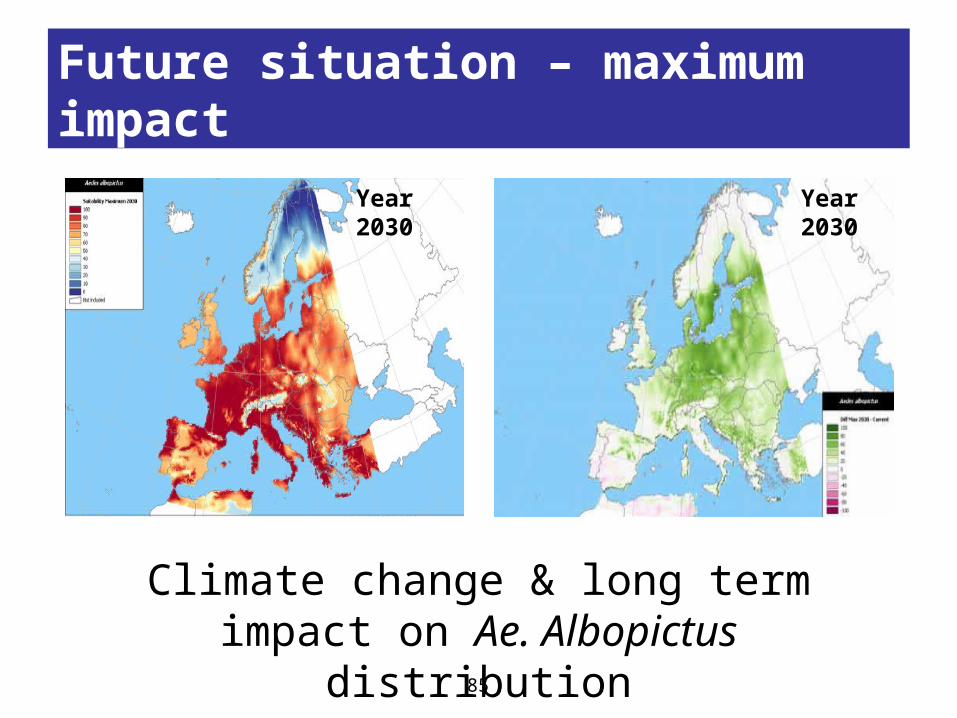
Future situation – maximum impact
Climate change & long term impact on Ae. Albopictus distribution
Year 2030
Year 2030

8686
Future situation
• Maps show the risk of establishment of Aedes albopictus
• The maps do not report the risk of transmitting exotic viruses, nor can one extrapolate from them to assess any such risk
• Analysing this risk would require a significant number of additional datasets, e.g. vector capacity in the given eco-climatic settings which are currently not available

Mosquito borne disease
- Chikungunya -
88
Chikungunya – health effects
• Clinical symptoms– Incubation time of 4-7 days (range 1-12)– Sudden onset of high fever (>38.5°C)– Other (flu-like) symptoms:
• Headache, backpain, myalgia, arthralgia, rash
Similar to Dengue fever
• Treatment– Symptoms generally resolve within 7-10 days– No vaccine or medication currently available

89
Chikungunya – health effects
• Possible complications– Gastro-intestinal complications, cardio-
vascular decompensation or meningo-encephalitis
– Fatalities have been reported mainly in aged patients or where the patient’s immune system was weakened by underlying conditions

90
Chikungunya – health impact
• World wide– ‘52: Tanzania – ‘60s: Southeast Asia: India ~ 1.39 million cases– ‘80s: Small outbreaks: Thailand < 12,000 cases– ‘01-’07: Major outbreaks islands Indian Ocean
(1/3 of population) and India ~ 1.42 million cases
• Europe– ‘07: outbreak in Italy 247 cases
91
Chikungunya – health impact
• Risk groups– There are no particular risk groups: anyone
exposed to the infected vector may become infected with the virus
• Vulnerable population for severe illness– Pregnant women– Children under 12 years old– People with immune disorders or server
chronic illnesses

9292
Current distribution – Chikungunya

9393
Available warning systems
• Chikungunya is not a notifiable disease in most of the European countries.
• There is no commercial chikungunya vaccine
• Prevention of chikungunya is currently based on individual protection against mosquito bites

Mosquito borne disease
- Dengue fever-

95
Dengue – health effects
• Asymptomatic infections (40-80%)
• Clinical symptoms– Mild fever– “Classic” dengue fever
• Server flu-like symptoms: high fever, severe headache, pain behind the eyes, muscle and joint pains and rash
– Dengue haemorrhagic fever / Dengue shock• <5 % of all cases, mostly children and adolescents• Increase of vascular permeability that can lead to
life-threatening hypovolemic shock

96
Dengue – health impact
• World wide– 2.5 billion people (two fifths of the world's
population) are now at risk from dengue– WHO estimates there may be 50 million
dengue infections every year
• Europe– Last endemic was in 1927-78 in Greece– However, imported cases frequently reported
(travellers that have visited endemic areas)

97
Dengue – health impact
• Risk groups– There are no particular risk groups: anyone
exposed to the infected vector may become infected with the virus
• Since there are four virus serotypes, it is possible to get dengue multiple times within a lifetime

9898
Current distribution - Dengue
9999
Available warning systems
• Dengue is not a notifiable disease on European Union level
• There is no dengue vaccine, but this is an active field of research
• Prevention of dengue is currently based on individual protection against mosquito bites

Future situation
- Chikungunya fever -- Dengue fever -

101101
Future situation
• Current situation Europe– Mosquito biting activity is highest in mid-
afternoon.– Incidental, travellers that visited endemic areas
• Future situation & climate change– At present, no good prediction models
available
102102
What actions are needed? [1]
• Short term– Providing information to all people traveling from the
affected areas with high disease incidence – Providing dengue/chikungunya virus fact sheets to
physicians, as returning travelers may present with the disease,
– Reminding medical staff of the need to follow universally accepted precautions when handling samples from all patients
– Advising European Union member states on blood donation policies
– Assessing the capability and capacity of laboratories in Europe to diagnose dengue/chikungunya fever

103
What actions are needed? [2]
• Long term– Further studies and documentation of vector
competence and capacity of Ae. albopictus would be useful in areas in Europe where these vectors are known to be present.
– Areas at risk of vector establishment need to be identified and regularly monitored, and vector surveillance implemented or strengthened in these areas.
– Measures to prevent the introduction of Ae. albopictus through the used tyre trade and plants transported in water (e.g. Dracaena species) should be considered.
104
Summary – mosquito borne [1]
• Aedes species (dengue and chikungunya virus)– It can be concluded that the temperate strains of
Aedes albopictus are here to stay — and that they will spread (Southern Europe)
– New Aedes populations may become established in other parts of Europe
• Culex species (West Nile virus)– Autochthonous transmission of West Nile fever in
several European countries– Data indicate that the epidemiology of WNV in
Europe is changing
105
Summary – mosquito borne [2]
• Actions– Surveillance of the introduction and spread of this
vector, in particular in areas at risk, is important in order to be prepared for the mosquito’s role in the transmission of diseases
– Education of public (risk areas and travelers) and health professionals
• Preventive measures• Health effects• Treatment
– Advising European Union member states on blood donation policies

Module – vector borne diseases
Leishmaniasis – sandfly borne

107107
Leishmaniasis – sandfly borne
• Leishmaniasis = disease caused by Leishmaniasis parasite
• Vector borne– zoonotic or anthroponotic– usually by the bite of a phlebotomine sandfly
species
• Parasite reservoir hosts– Wild animals (fox, rodents, wolves etc.)– Domestic animals (dogs)

• Bite by an infected sandfly
• Can be transmitted from mother to child
• Contaminated medical equipment or supply (shared syringes)
Transmission mode
108

109109
• Asymptomatic leishmania infections
• Forms of leishmaniasis– CL: Cutaneous (most common)– ML: Mucocutaneous – VL: Visceral (most severe, affecting
organs)– Canine leishmaniasis (dogs)
Leishmaniasis – health effects

110110
Leishmaniasis – sandfly borne
• 500 phlebotomine species, but only about 30 transmit leishmaniasis
• Only the female sandfly transmits the parasites
• 8 medically important in Europe

111111
Current situation
• Worldwide distribution of parasite & sandflies– Areas that have at least one month with a
mean temperature of 20°C
• European distribution of parasite & sandflies– South of latitude 45oN and less than 800 m
above sea level– Recent data suggest that the area has been
expanded

112112
Current distribution – sandfly
P. papatasi P. perfiliewi
P. neglectus/syriacusP. ariasi
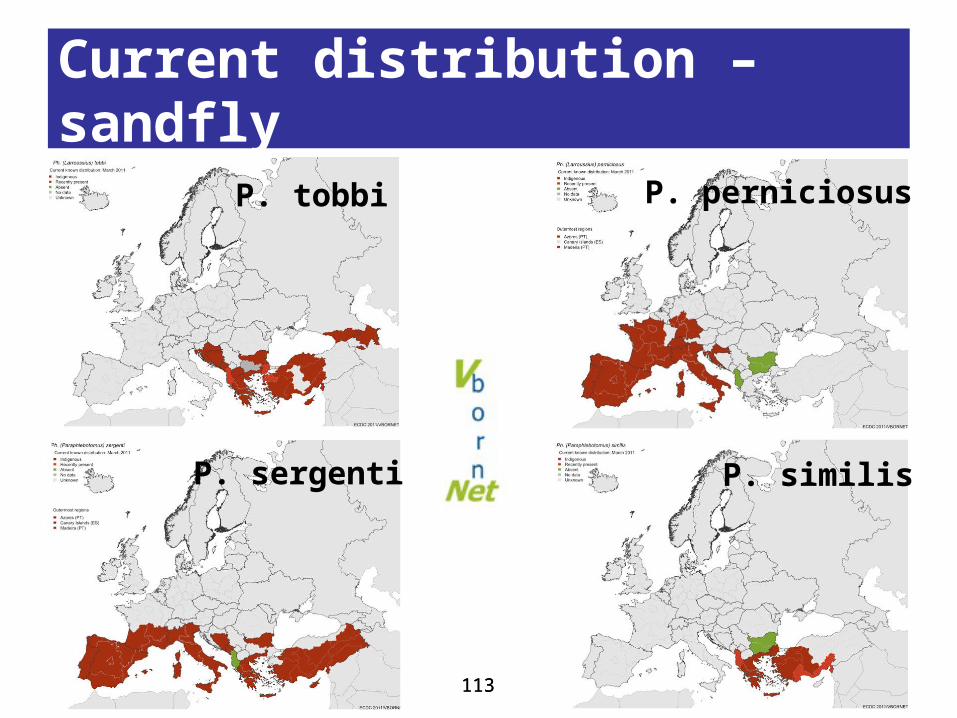
113113
Current distribution – sandfly
P. sergenti P. similis
P. tobbi P. perniciosus

114114
Leishmaniasis – health impact
• World wide– An estimated 12 million people are infected– 2 million estimated new cases/year
• Europe– Incidence of leishmaniasis in humans is relatively
low (0.02- 0.49/100,000)– 700 estimated new cases/year for Southern
European countries (3,950 if Turkey is included)
115115
Leishmaniasis – health impact
• Risk groups leishmania infections– There are no specific risk groups for
leishmania infections
• Risk groups leishmaniasis– HIV-positive people (visceral leishmaniasis) – Intravenous drug users who share syringes
116116
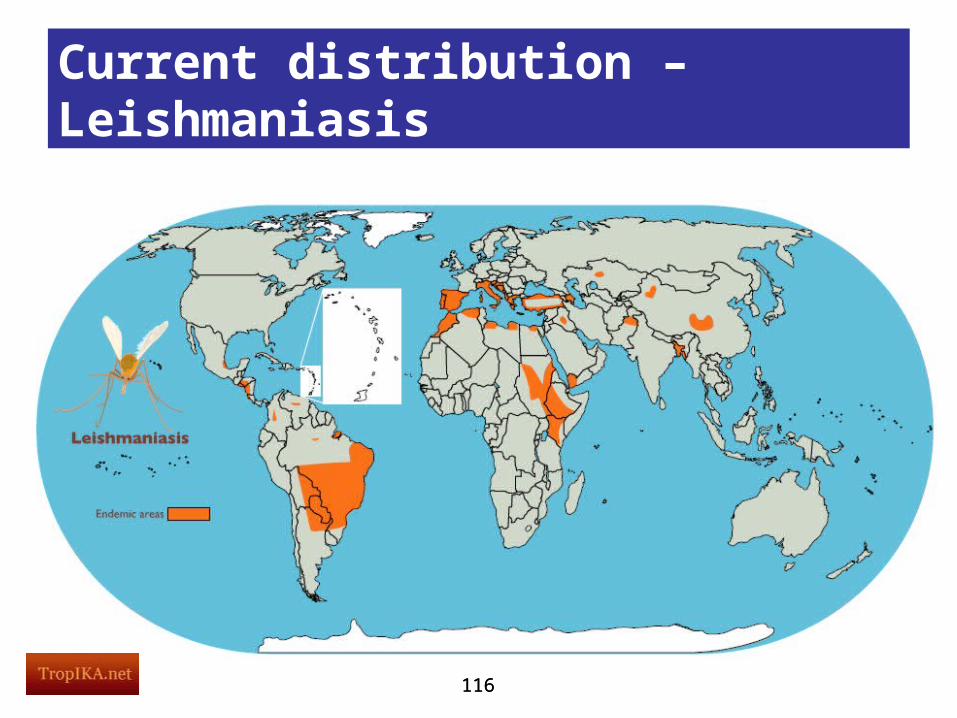
Current distribution – Leishmaniasis

117117
Current distribution – Leishmaniasis
Source: Dujardin 2008

118118
Available warning systems
• Compulsory notification system– Portugal: compulsory for VL– Spain: compulsory for VL in 12/17
autonomous communities– Greece: compulsory for VL and CL– Cyprus: compulsory for VL and CL– Turkey: compulsory for VL and CL

119119
Future situation
• Current situation Europe– Sandfly biting activity is strongly seasonal, restricted to
summer months in most areas– Southern Europe, below 800m above sea level
• Future situation & climate change– Prolonged activity periods and shorter diapause
periods (overwintering)– Extend northwards and into higher altitudes– At present, no good prediction models available

120120
What actions are needed?
• Public health surveillance at the European level (compulsory notification system in all countries)?
• Educate the public on interventions against sandflies
• Further research
121121
What actions are needed?
• Interventions against sandflies– Insect repellents such as DEET– Insecticides– Use of insecticide impregnated nets and bed
nets– Dog: topical applications and deltamethrin-
impregnated collars

122122
What actions are needed?
• Further research on– Alternative modes of transmission– Effective vaccine for human leishmaniasis
• immunisation strategy for Mediterranean populations
– Effective vaccine for canine leishmaniasis • to control the infections in vector reservoir dogs
– Better predictive modelling of disease transmission

123
Summary – sandfly borne [1]
• Currently, Leishmaniasis infected sandflies are present in Southern Europe (max. 800m above sea level)
• Climate change may extend this risk area northwards and into higher altitudes
• Actions– Surveillance of the introduction and spread of
this vector

124
Summary – sandfly borne [2]
• Actions (continued)– Education of public (risk areas and travelers)
and health professionals• Preventive measures• Health effects• Treatment
Module – vector borne diseases
SUMMARY

126126
Training objective
• To learn how to be prepared for changes in public health due to climate change
• Take home message– Health impact– Mitigation and adaptation
– Preventive measures on individual & community level
127
Summary – module VBD [1]
• Health impact climate change– Tick borne disease highest tick infection
rates in central Europe may spread to northern areas
– Mosquito borne disease
• West Nile virus spatially and temporally limited. However, autochthonous transmissions.
• Chikungunya outbreak in Italy in 2007. In future, Southern Europe may be at risk.

128
Summary – module VBD [2]
• Health impact climate change (continued)– Mosquito borne disease
• Dengue currently not present in Europe. In future, Southern Europe may be at risk.
– Sandfly borne disease Leishmaniasis is endemic in Southern Europe. In future, risk area may extend northwards and into higher altitudes

129
Summary – module VBD [3]
• Adaptation– Surveillance of the introduction and spread of
the vector, in particular in areas at risk– Providing information to all people traveling
from the affected areas with high disease incidence
– Providing fact sheets to physicians– Reminding medical staff of the need to follow
universally accepted precautions when handling samples from all patients
130
Summary – module VBD [4]
• Adaptation (continued)– Advising European Union member states on
blood donation policies– Assessing the capability and capacity of
laboratories in Europe to diagnose vector borne disease
– Development of vaccines

131
Summary – module VBD [5]
• Preventive measures on individual level– Avoiding risk areas (if possible)– When staying in affected areas
• Wear long-sleeved shirts and long trousers, and trousers tucked into socks
• Use insect repellents such as DEET• If possible, sleep under bed nets pre-treated with
insecticides• If possible, set the air conditioning to a low
temperature at night

132
Summary – module VBD [6]
– When staying in affected areas (continued)• Good screens on windows and doors• Remove tick within 24 hours (hard ticks)

133
Summary – module VBD [7]
• Preventive measures on community level– Blood donation restrictions have to be
considered in areas where a vector borne virus is circulating
– Limiting vector friendly environments (next slides)
134
Summary – module VBD [8]
• Ticks– Chemical treatment– Natural predators like domestic cats– Limiting rodent-friendly environments inside
and around buildings– Acaricides may be useful on domestic
animals to control CCHF virus-infected ticks if used 10–14 days prior to slaughter or to export of animals from enzootic regions

135
Summary – module VBD [9]
• Mosquitoes– Insecticides– Removal of breeding sites around buildings:
emptying stagnant water in and around the houses on a weekly basis
• Limiting vector friendly environments -sandflies– Dog: topical applications and deltamethrin
impregnated collars

Websites
• www.climatetrap.eu
• www.ecdc.eu
• www.who.int/globalchange/en/
136136
More information

















