Transesophageal Echocardiographic Artifact Mimicking an Aortic Valve Tumor Steven M. Neustein, MD, and Jolie Narang, MD T HE intraoperative use of transesophageal echocardio- graphy (TEE) has become a very common practice; the number of patients studied while under anesthesia has been estimated at more than 10,OOO.t Prebypass echocardi- ography has been reported to either assist or change the planned operation in 29 of 154 patients (19%) scheduled for cardiac valve surgery.2 Accurate interpretation of the echocardiogram requires an understanding of the physics of ultrasound imaging and Doppler techniques, and the iden- tification of artifacts.” A case is presented in which the presence of an artifact resembling a mass prompted an aortic root exploration in a patient undergoing a coronary artery bypass graft (CAESG) operation. CASE REPORT A 71-year-old woman presented for CABG surgery. A routine electrocardiogram (ECG) had revealed an old myocardial infarc- tion (MI), and workup of the patient led to coronary angiography, which indicated the need for CABG. Although she had a history of a silent MI, there was no history of angina or congestive heart failure. Her only other medical conditions were noninsulin- From The Mourn Sinai Medical Center, Department ofAne.sthesiol- ogy, New York, NY10029-6574. Address reprint requests to Steven M. Neustein, MD, The Mount Sinai Medical Center, Department of Anesthesiology Box 1010, One Gustave L. Levy Pld, New York, NY10029-6574. Copyright o 1992 by W B. Saunders Company 10%077019210606-0017$03.00/0 Key words: transesophageal echocardiography, aortic valve, tumor, artifact dependent diabetes mellitus, and a penicillin allergy. Glyburide was her only medication. She had a cholecystectomy 30 years prior to admission without complications. Physical examination revealed an elderly woman with a pulse 80 beats/minute, blood pressure 120180 mmHg, and weight 66 kg. The examination was otherwise unremarkable. Laboratory studies in- cluded a hemoglobin of 14.7 gm/dL, hematocrit 43%. sodium 137 mEq/L, potassium 4.7 mEq/L, and glucose 108 mEq/L. The ECG had a normal sinus rhythm at 80 beatsimin, normal intervals. normal axis, Q waves in II, III, and aVF, T wave inversions in the lateral leads. and poor R wave progression. Cardiac catheterization revealed significant stenoses in the follow- ing arteries: left anterior descending (loo%,), circumflex (80?). right coronary artery (60%) and posterior descending artery (90%). Left ventricular function was moderately depressed. No other abnormalities were noted. The patient was premeditated with morphine, 6 mg, and scopolamine. 0.2 mg. intramuscularly. She received oxygen, 3 L/min by nasal cannula. during transport to the operating room. Upon arrival in the operating room, she was monitored with ECG leads II and Vi. pulse oximetrv, and a blood pressure cuff. Catheters were placed uneventfully in a peripheral vein, right radial artery. and pulmonary artery via the right internal jugular vein. Anesthesia was induced with fentanyl, 2 mg, metocurine. 12 mg, and oxygen, and was maintained with fentanyl. metocurine. oxygen, and low concentrations of isoflurane. Following endotra- cheal intubation, a transesophageal 5.0 MHz probe (Aloka X70. Corometrics Inc, Wallingford. CT) was inserted into the esopha gus. Echocardiography revealed a circular density with a 1.3 cm diameter. seen at the level of the aortic valve adjacent to the left coronary cusp (Fig I). It was seen during late systole, and was also present during diastole. Color-flow Doppler echocardiography did Fig 1. Echocardiogram of pa- sity at the aortic valve. 724 Journalof Cardiofhoracic and Vascular Anesthesta, Vol6, No 6 (December), 1992: pp 724-727
Transcript
Transesophageal Echocardiographic Artifact Mimicking an Aortic Valve Tumor
Steven M. Neustein, MD, and Jolie Narang, MD
T HE intraoperative use of transesophageal echocardio- graphy (TEE) has become a very common practice;
the number of patients studied while under anesthesia has been estimated at more than 10,OOO.t Prebypass echocardi-
ography has been reported to either assist or change the planned operation in 29 of 154 patients (19%) scheduled for cardiac valve surgery.2 Accurate interpretation of the echocardiogram requires an understanding of the physics of ultrasound imaging and Doppler techniques, and the iden- tification of artifacts.” A case is presented in which the presence of an artifact resembling a mass prompted an
aortic root exploration in a patient undergoing a coronary
artery bypass graft (CAESG) operation.
CASE REPORT
A 71-year-old woman presented for CABG surgery. A routine electrocardiogram (ECG) had revealed an old myocardial infarc- tion (MI), and workup of the patient led to coronary angiography, which indicated the need for CABG. Although she had a history of a silent MI, there was no history of angina or congestive heart failure. Her only other medical conditions were noninsulin-
From The Mourn Sinai Medical Center, Department ofAne.sthesiol- ogy, New York, NY10029-6574.
Address reprint requests to Steven M. Neustein, MD, The Mount Sinai Medical Center, Department of Anesthesiology Box 1010, One Gustave L. Levy Pld, New York, NY10029-6574.
Copyright o 1992 by W B. Saunders Company 10%077019210606-0017$03.00/0 Key words: transesophageal echocardiography, aortic valve, tumor,
artifact
dependent diabetes mellitus, and a penicillin allergy. Glyburide was her only medication. She had a cholecystectomy 30 years prior to admission without complications.
Physical examination revealed an elderly woman with a pulse 80 beats/minute, blood pressure 120180 mmHg, and weight 66 kg. The examination was otherwise unremarkable. Laboratory studies in- cluded a hemoglobin of 14.7 gm/dL, hematocrit 43%. sodium 137 mEq/L, potassium 4.7 mEq/L, and glucose 108 mEq/L.
The ECG had a normal sinus rhythm at 80 beatsimin, normal intervals. normal axis, Q waves in II, III, and aVF, T wave inversions in the lateral leads. and poor R wave progression. Cardiac catheterization revealed significant stenoses in the follow- ing arteries: left anterior descending (loo%,), circumflex (80?). right coronary artery (60%) and posterior descending artery (90%). Left ventricular function was moderately depressed. No other abnormalities were noted.
The patient was premeditated with morphine, 6 mg, and scopolamine. 0.2 mg. intramuscularly. She received oxygen, 3 L/min by nasal cannula. during transport to the operating room. Upon arrival in the operating room, she was monitored with ECG leads II and Vi. pulse oximetrv, and a blood pressure cuff. Catheters were placed uneventfully in a peripheral vein, right radial artery. and pulmonary artery via the right internal jugular vein. Anesthesia was induced with fentanyl, 2 mg, metocurine. 12 mg, and oxygen, and was maintained with fentanyl. metocurine. oxygen, and low concentrations of isoflurane. Following endotra- cheal intubation, a transesophageal 5.0 MHz probe (Aloka X70. Corometrics Inc, Wallingford. CT) was inserted into the esopha gus.
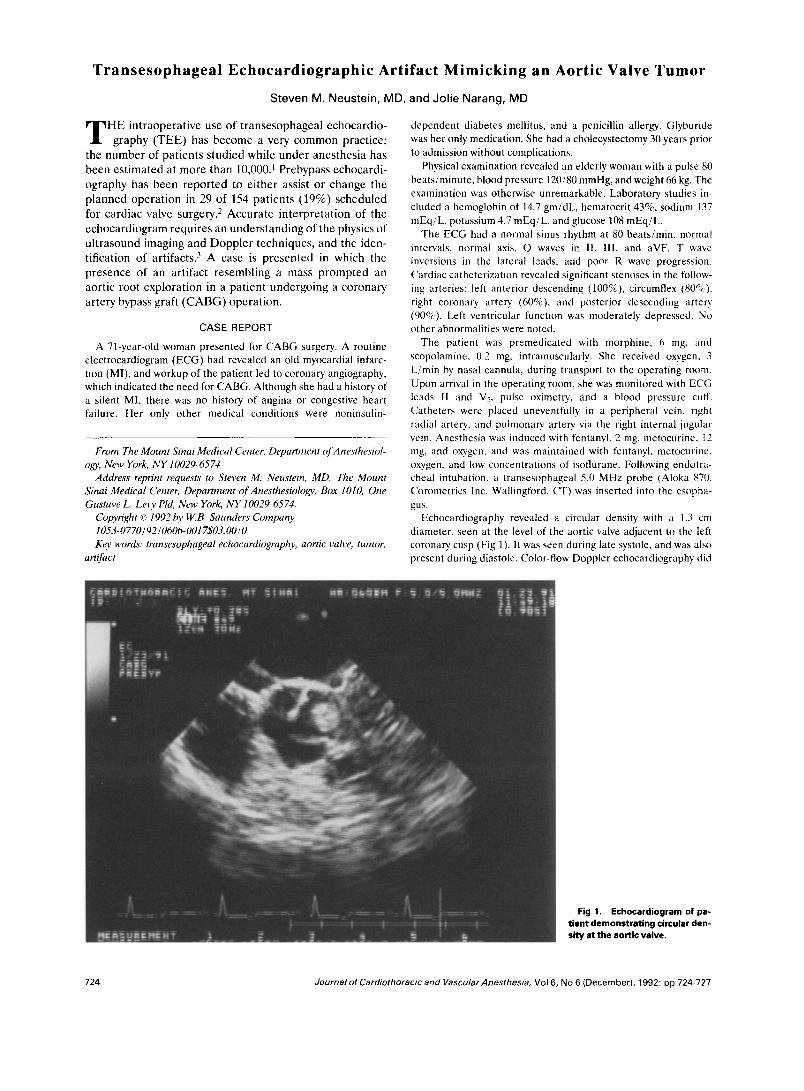
Echocardiography revealed a circular density with a 1.3 cm diameter. seen at the level of the aortic valve adjacent to the left coronary cusp (Fig I). It was seen during late systole, and was also present during diastole. Color-flow Doppler echocardiography did
Fig 1. Echocardiogram of pa-
sity at the aortic valve.
724 Journalof Cardiofhoracic and Vascular Anesthesta, Vol6, No 6 (December), 1992: pp 724-727
TRANSESOPHAGEAL ECHOCARDIOGRAPHIC ARTIFACT 725
Fig 2. Ect rocardiogram of another patient showing a circular density at the aortic valve during systole (2A) and diastole (28). No fillin were seen 01 1 angiography.
not reveal al ny aortic insufficiency. TEE examination in the longitu- dinal plane revealed thickening of the left coronary aortic valve leaflet. A pr obe for epicardial echocardiography was unavailable at the time. F :urther review of the angiogram did not show any evidence of a filling defect that could be compatible with an aortic
mass. The echo data were reviewed and confirmed by a In expert echocardiographer in the cardiology department, and the decision to explore the aortic root was made. The circular der lsity was believed to be either a tumor or nodule, and even if the pa tient was asymptomatic, the mass could enlarge and/or embolize if left in
g defects
726 NEUSTEIN AND NARANG
Fig 3. Echocardiogram showing circular density at the aortic valve, in same location as in Figs 1 and 2.
place. In addition to distal anastomoses to the left anterior descending, first diagonal, first obtuse marginal, and left ventricu- lar branch of the right coronary, and posterior descending coronary arteries, exploration of the aortic root was performed while the aorta was cross-clamped. Exploration via a transverse incision in the aorta of both the aortic root and the ventricular side of the aortic valve was negative. The aortic valve was entirely normal.
Following a cross-clamp time of 97 minutes and a total pump time of 139 minutes, the patient was easily weaned off CPB and required no vasopressor support. The same density was still present by TEE during the postbypass period. The postoperative course was uneventful, and the patient was extubated the next morning.
Several weeks following the operation presented above, another patient undergoing CABG had a similar artifact on TEE (Fig 2). No filling defect was seen on angiography, and due to the experience of the first case presented, the aortic root was not explored. The density was present both prebypass and postbypass. A similar echocardiogram from a third patient undergoing a routine CABG is shown in Fig 3.
DISCUSSION
TEE has become very useful in the operating room, and can influence both anesthetic and surgical management.
TEE routinely provides an assessment of left ventricular filling and ejection, and can reveal segmental wall motion abnormalities (SWMA). The presence of new intraopera- tive SWMAs is a more sensitive sign of myocardial ischemia than ST segment changes on the electrocardiogram.4J In both of these studies, the echocardiograms were analyzed
off-line. Real-time analysis of the echocardiogram is less revealing.6 The use of a quad screen system with simulta- neous display of previous images with the real-time images allows improved detection of SWMAS.~
TEE has also become important in the diagnosis of cardiac tumors and thrombi. TEE is better than transtho- racic echocardiography (TTE) for viewing the left atria1 appendage, atria1 masses, pulmonary veins, and atrioventric- ular valves.’ Whereas myxomas most commonly occur in the atria, papillomas are usually attached to either the valve leaflets or annulus.’ Papillary fibroelastoma are rare tumors of the heart that are usually attached to the valves.x~y
To the authors’ knowledge, there has only been one case report in which an aortic valve tumor was discovered with the use of TEE.]” In that patient, who was scheduled to undergo CABG, TEE revealed a 1 cm by 1 cm mass located by the right coronary leaflet of the aortic valve. The mass did not move with the aortic valve, which was normal in appearance, and there was no aortic insufficiency. Review of the coronary cineangiogram showed a filling defect, which moved with the aortic valve, and prolapsed into the right coronary artery ostium. Aortic root exploration re- vealed a 1 cm tumor attached to the right coronary cusp by a 1 cm pedicle. Pathologic examination of the tumor deter- mined that it was a papillary fibroelastoma. Similarly, in this case report, the density seen on TEE did not move with the aortic valve, there was no evidence of aortic insufficiency. and the appearance of the aortic valve was normal. How- ever, the coronary cineangiogram did not reveal any filling defect in the case of the artifact.
A classification scheme of artifacts that interfere with the analysis of ultrasound has been proposed: (1) artifacts suggesting the presence of structures not actually present: (2) artifacts that remove real echoes from the display or obscure information; and (3) artifacts that distort the size. shape, or brightness of a structure.” Examples of the first class of artifacts are reverberations from highly reflective surfaces,” and refractive artifacts simulating hepatic pseudo- tumors in patients with ascites.‘?
The apparent artifact presented in this case report. which has not been previously reported, could be classified in both the first and third categories; the distortion of a structure. which led to an artifact suggesting the presence of a structure not actually present. The artifact presented here may have been caused by an oblique sectioning through the aortic valve, which produced a tangential view through an aortic valve cusp during a portion of the cardiac cycle. The presence of aortic insufficiency, movement of the density with the aortic valve, or a tissue density that is different from the aortic valve would suggest that the density is more likely to be an actual mass or vegetation, as opposed to an artifact. The circular density presented in this case report was confirmed to be an artifact by the aortic root explora- tion. This additional procedure increased the risk of air embolism to the patient, but fortunately the postoperative course was uneventful.
TRANSESOPHAGEAL ECHOCARDIOGRAPHIC ARTIFACT 727
REFERENCES
1. Clements F: The Evaluation of the Anesthesiologist-Echocar- diographer, in de Bruijn NP, Clements FM (eds): Intraoperative Use of Echocardiography. Philadelphia, PA, Lippincott, 1991, pp 1-12
2. Sheikh KH, deBruijn NP, Rankin JS, et al: The utility of transesophageal echocardiography and Doppler color flow imaging in patients undergoing cardiacvalve operations. J Am Coil Cardiol 15:363-372, 1990
3. Evans RG: Medical diagnostic ultrasound instrumentation and clinical interpretation. JAMA 265:1155-1159, 1991
4. Smith JS, Cahalan MK, Benefiel DJ, et al: Intraoperative detection of myocardial ischemia in high-risk patients: Electrocar- diography versus two-dimensional transesophageal echocardiogra- phy. Circulation 72:1015-1021, 1985
5. Leung JM, O’Kelley B, Browner WS, et al: Prognostic importance of postbypass regional wall motion abnormalities in patients undergoing coronary artery bypass graft surgery. Anesthe- siology 71:16-25, 1989
6. Saada M, Cahalan MK, Lee E, et al: Real-time evaluation of echocardiograms. Anesthesiology 71:A344,1989
7. Seward JB: Cardiac tumors and thrombus: Transesophageal echocardiographic experience, in Khandheria B, Brennecke R, et al (eds): Transesophageal Echocardiography. Heidelberg, Ger- many, Springer-Verlag, 1989, pp 120-128
8. McAllister MA, Feroglio JJ Jr: Tumors of the cardiovascular system. Atlas of tumor pathology. Armed Forces Institute of Pathology 1978, pp 20-25
9. Almagro VA, Perry LS, Choi H, Pintar K: Papillary tibroelas- toma of the Heart. Arch Path01 Lab Med 106:318-321, 1982
10. Narang J, Neustein SN, Israel D: Transesophageal echocar- diography for diagnosis and excision of aortic valve tumor. J Cardiothorac Vast Anesth 6:68-69, 1992
11. Council on Scientific Affairs: Medical Diagnostic Ultra- sound Instrumentation and Clinical Interpretation. JAMA 265: 1155-1159,199l
12. Skwarok DJ, Goiney RC, Cooperberg PL: Hepatic pseudo- tumors in patients’with ascites. J Ultrasound Med 5:5-8,1986