66
Transfusion Support of Thrombotic Thrombocytopenic Purpura (TTP) Nicholas Bandarenko, MD, FCAP Director, Transfusion Services Duke University

Transfusion Support of
Thrombotic Thrombocytopenic
Purpura (TTP)
Nicholas Bandarenko, MD, FCAP
Director, Transfusion Services
Duke University

Learning Objectives
Understand the TTP syndrome and its relevance to blood banking
Be familiar with the pathogenesis and laboratory diagnosis of TTP
Explain how therapeutic apheresis is used to treat TTP
Describe the types of blood products required for management of patients: frequency , volume, and duration of transfusions
Provide strategies for ensuring adequate inventory of components
Be prepared for adverse reactions encountered in TTP
TTP: In the beginning…..
Described by Eli Moschcowitz 1924
16 year old girl
Anemia, fever, renal dysfunction,
CNS impairment, and cardiac failure
Died in 2 weeks
Autopsy: hyaline microthrombi in
arterioles and capillaries
Heart , spleen , kidney

TTP: pathophysiology
Microthrombi in
small arterioles of heart

TTP: diagnosis
PENTAD for recognition:
microangiopathic hemolytic anemia
thrombocytopenia
renal failure
mental status changes
fever
Rule out other causes such as DIC, HTN
No diagnostic test!
TTP Characteristics
Rare but increasing - 4 cases per million
Females > males 4:1
Any age from pediatric to geriatric
Mean age 40 yo
70% between ages 18-49
Patients often have no preceding health problems
No geographic or seasonal patterns
90% mortality without treatment!
10% mortality with plasma exchange
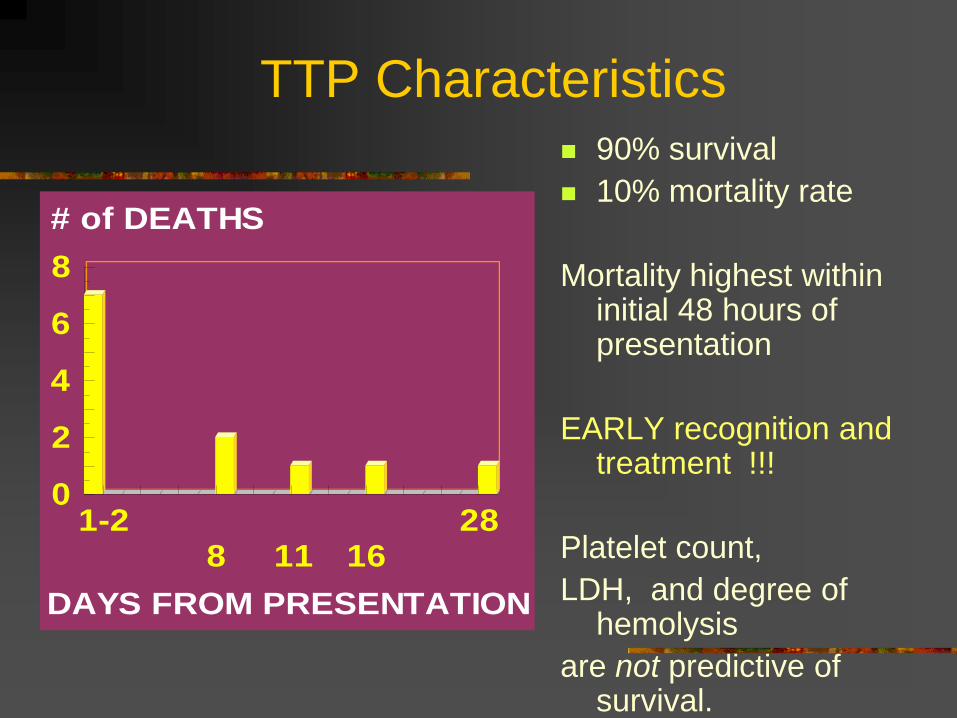
TTP Characteristics
90% survival
10% mortality rate
Mortality highest within initial 48 hours of presentation
EARLY recognition and treatment !!!
Platelet count,
LDH, and degree of hemolysis
are not predictive of survival.
1-28 11 16
28
DAYS FROM PRESENTATION
0
2
4
6
8
# of DEATHS

TTP: diagnosis
Microangiopathic Hemolytic Anemia (MAHA)
Mechanical RBC destruction
Red Cell Fragments or schistocytes
May be associated with platelet count
TTP: diagnosis
Diverse Causes of MAHA:
TTP
Malignant hypertension (systolic BP > 200)
DIC, sepsis
HELLP syndrome (preclampsia)
Metastatic adenocarcinoma
Intravascular prosthetic devices: e.g. LV assist device

TTP: diagnosis
Complete Blood Count
will show
Low platelet count
Can be <10k
Schistocytes
Anemia is variable
Plasma may be
hemolyzed, dark red-
brown or icteric Peripheral blood smear with schistocytes
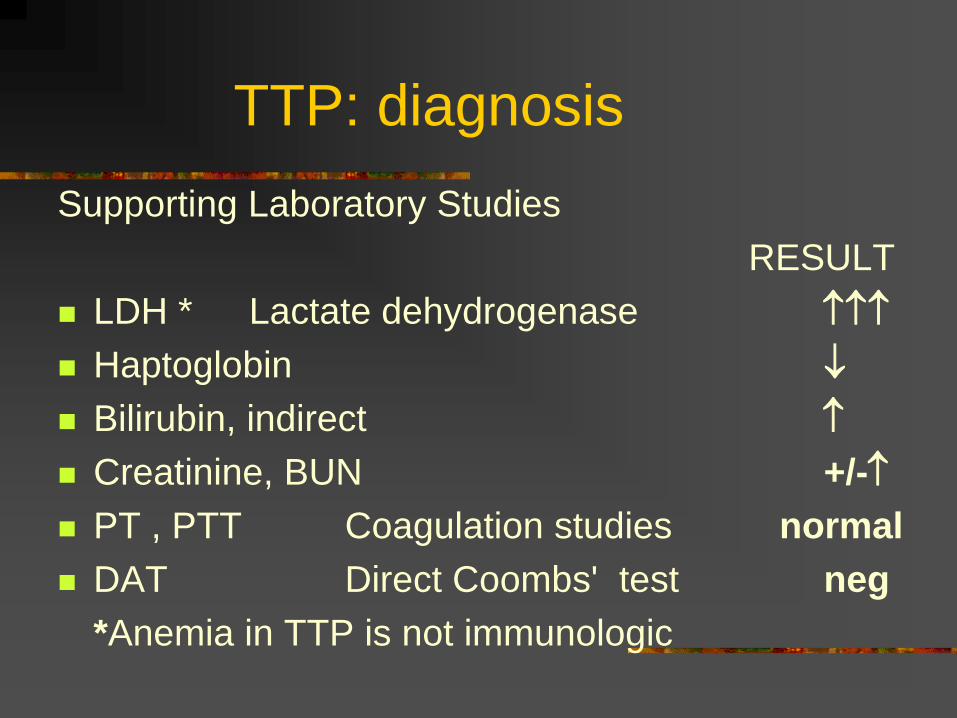
TTP: diagnosis
Supporting Laboratory Studies
RESULT
LDH * Lactate dehydrogenase
Haptoglobin
Bilirubin, indirect
Creatinine, BUN +/-
PT , PTT Coagulation studies normal
DAT Direct Coombs' test neg
*Anemia in TTP is not immunologic

TTP is found in many clinical settings
Primary or Idiopathic
Secondary causes of TTP
Connective Tissue Disease (SLE)
Hormonal (menses, pregnancy, OCP's)
Infection
Diarrhea ( HUS )
Drugs : quinine, ticlid, plavix, FK506, cyclosporin
Chemotherapy: cis platinum, mitomycin c
Transplant (BMT, solid organ)
TTP: pathophysiology
Hmmmm…. what’s going wrong here?

TTP: pathophysiology
Earliest research implicated
Endothelial cells damage
Sheer stress caused by blood flow
Abnormalities in vWF (von Willebrand
Factor)
Resulting in abnormal aggregation of
platelets causing thrombi in
microvasculature

TTP: pathophysiology
vWF von Willebrand Factor important in clot initiation and platelet aggregation.
Moake, et al
vWF multimers abnormal in relapsing TTP Unusually large multimers of vWF Or missing large multimers of vWF suggesting
consumption during acute episode
Multimers may unfold under sheer stress
Predispose to platelet aggregation Ultralarge multimers have qualitatively stronger
mechanical binding to platelets

TTP: unusually large vWF multimersMultimeric patterns of plasma
vWF
TTPNormal plasma

ADAMTS13
vWF protease: 150 kd single chain glycoprotein
Rapidly breaks vWF into smaller sized multimers when released from damaged endothelial cells
Discovered that the function of this enzyme in the plasma was deficient in TTP

TTP: vWF Protease Functional Activity
before and after treatment of TTP

TTP: pathophysiology
ADAMTS13 Protease defect:
Inherited deficiency / absence
Acquired inhibitor
IgG like autoantibody which blocks protease
Results in an in vWf multimers
Not specific to TTP but very characteristic
Severe deficiency <10% activity
Presence of autoimmune inhibitor
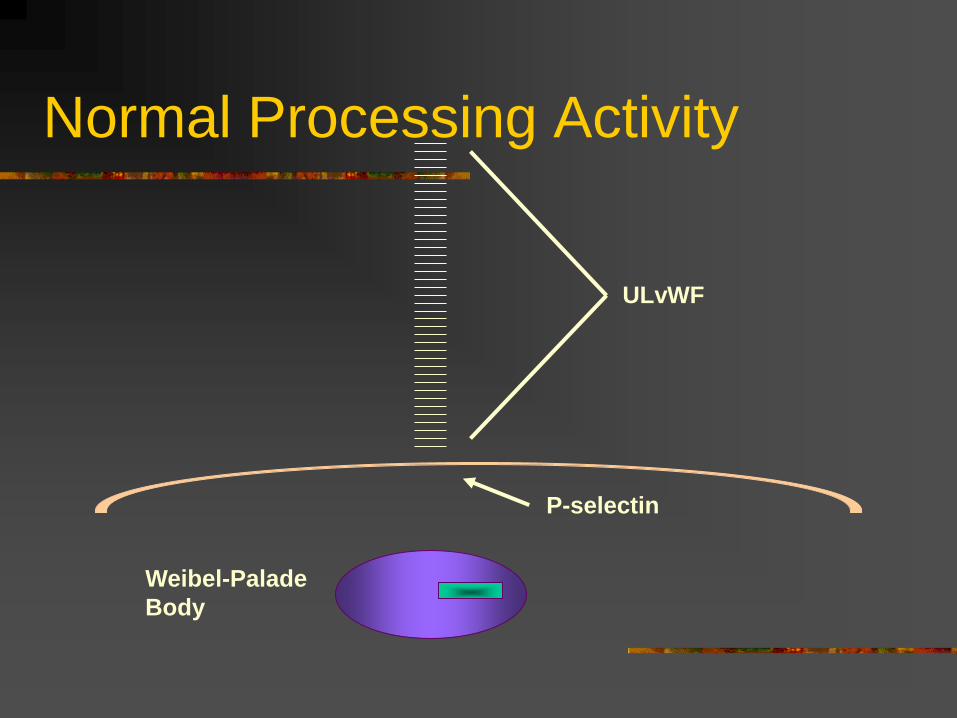
Normal Processing Activity
P-selectin
ULvWF
Weibel-Palade
Body

Normal Processing Activity

TTP Pathophysiology

TTP Pathophysiology

TTP Pathophysiology
TTP: pathophysiology
Protease defect is NOT ALWAYS seen in patients
presenting with TTP
May be different pathophysiologic
mechanisms
ADAMTS13 not currently available as
a rapid test

TTP
CURRENT MANAGEMENT
Emergent Treatment with Plasma
Preferred treatment is Therapeutic Plasma Exchange (TPE)
apheresis
Means “to separate”
The process of removing normal or
abnormal blood constituents from
circulating blood
Donation of blood
Treatment of disease
“Pheresis” often used and synonym
Therapeutic Apheresis
Therapeutic Plasma Exchange
Plasma separation (plasmapheresis) and
replacement
Other nomenclature/abbreviations:
TPE = therapeutic plasma exchange
PLEX

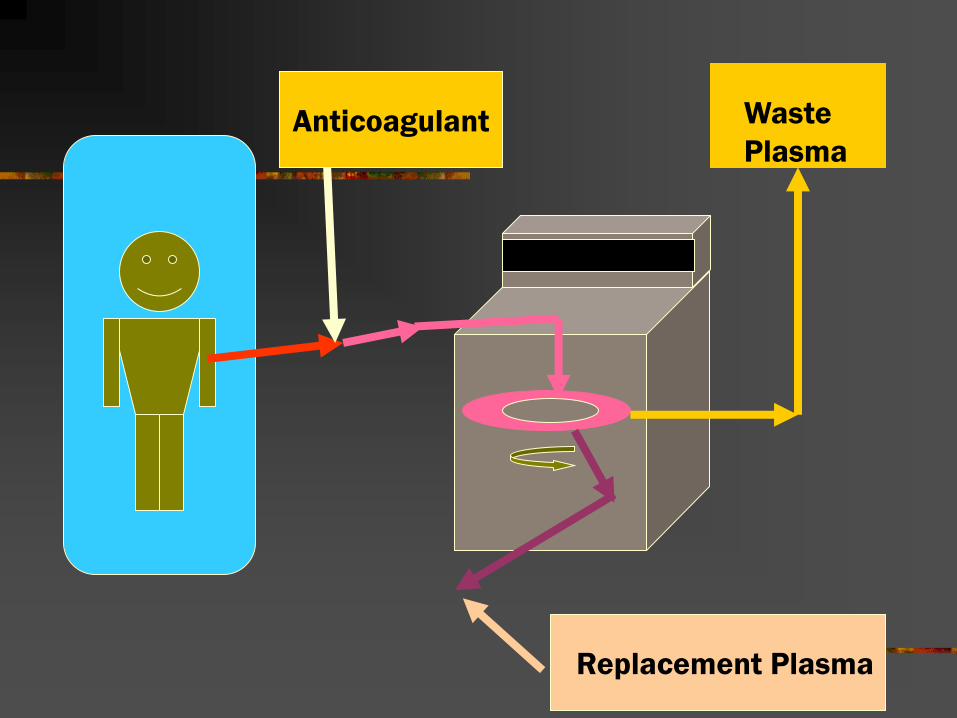
Apheresis Machine

Anticoagulant
Anticoagulant

Anticoagulant

Waste
Plasma Anticoagulant
Waste
Plasma
Replacement Plasma
Anticoagulant

Product
Replacement Plasma
Anticoagulant


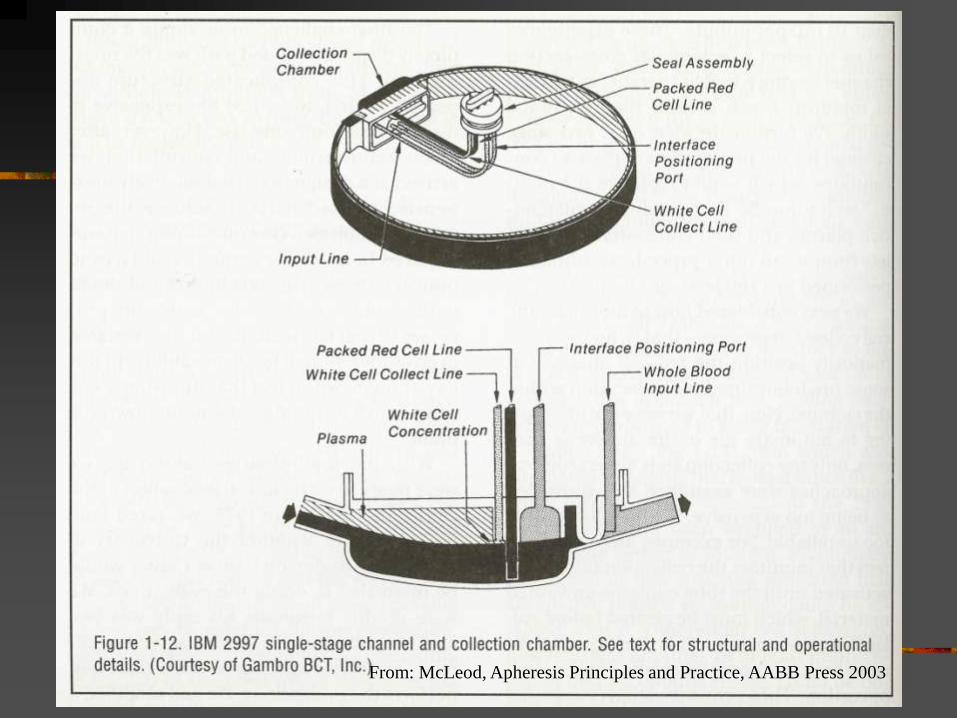
From: McLeod, Apheresis Principles and Practice, AABB Press 2003
Emergent plasma exchange (TPE)
1 Plasma Volume of the patient is removed and replaced with donor plasma from the blood bank Average plasma volume is 3000mL
Range 2500-4000 mL
May be 8 to 15 units of plasma required
Plasma exchange is repeated daily In some severe cases physicians may increase
plasma volume exchanged
Or increase the frequency to 2 times a day
Treatment continues until platelet count is normal >150k for 2 days
Treatment of TTP with TPE

TPE is preferred instead of simple
transfusion of plasma
Click here to type presentation title
Click here to type subtitle
Rock et al. Comparison of plasma exchange with plasma infusion in the treatment of TTP. Canadian Apheresis Study Group NEJM 325:393-7, 1991
7 year
N=102

Fresh Frozen Plasma
FP24
Thawed Plasma

Blood Bank Support of TTP
Plasma and LOTS of it
CALL YOU BLOOD SUPPLIER!

Blood Bank Support of TTP
What type of plasma is used?
FFP, FP24, or CPP (cryopoor plasma)
Cryopoor plasma is the supernatant plasma left
over from the manufacture of Cryoprecipitate
Contains less von Willebrand factor, multimers are
smaller
Once considered better than FFP, it is now
considered equivalent to FFP
TTP is the only indication for CPP

Blood Bank Support of TTP
Prepare to order type specific plasma in
large quantities from blood supplier
Plan to thaw multiple units
simultaneously—can delay treatment
May cause inventory concerns
Group AB and Group B TTP patients
Relative scarcity of these plasma ABO types
AB plasma needed in reserve for trauma
Blood Bank Support of TTP
What if plasma resources are limited?
Discuss with physician these options:
If using FFP or FP24, advise use of CPP for all or
some of plasma for replacement
Use of partial replacement of removed plasma with
5% albumin from pharmacy
Albumin is standard replacement in other diseases
treated with TPE
HOWEVER, albumin is not therapeutic by itself
1 liter of initial replacement with albumin followed by 2
liters of plasma has been standard of care at many
academic medical centers
Packed RBCs

Blood Bank Support of TTP
Red Cell Transfusions
KEEP TYPE AND SCREEN CURRENT!

Blood Bank Support of TTP
Red Cell Transfusions
Patients present with anemia which can be
symptomatic
Further problem is that when putting patient on
apheresis machine there is another 3%
hemodilution
Apheresis personnel may also request some
pRBCs
Transfusions may be required until hemolysis
due to MAHA subsides

platelets

Blood Bank Support of TTP
AVOID PLATELET TRANSFUSION!

Blood Bank Support of TTP
Platelet Transfusions
Avoid transfusion of platelets
Anecdotal reports of TTP patients
experiencing acute worsening and death
following transfusion of platelets
Most platelets are well tolerated
Flag / warn staff to check with MD to be
sure there is an indication
Central line placement, concern of head bleed

TTP: Adjunct therapies in TTP
Steroids: dosage typically 1mg/kg/day
Anti-platelet drugs
Rituximab (anti B cell immune therapy)
Plasma Infusions- for maintenance
therapy and chronic TTP
Splenectomy

Response Time by Replacement
0<8 days
<14 days<21 days
>21 days0
25
50
75
100
cu
mu
lati
ve
% r
es
po
nd
ing
ALL
FFP
CPP>50%
5%Alb/PL
CPP>75%
J of Clin Apheresis 13:133-141, 1998. United States Thrombotic Thrombocytopenic Purpura
Apheresis Study Group (US TTP ASG): Multicenter Survey and Retrospective Analysis of
Current Efficacy of Therapeutic Plasma Exchange

CURRENT CLINCIAL OUTCOMES
60-65% complete remission
35-40% relapse rate
Early relapse-days to weeks
Late recurrence- months
No diagnostic test to predict relapse

Adverse reactions
TTP patients have a
higher risk of allergic
and other
complications
Coordinate reporting
of Rxns with the
apheresis unit
Allergic reactions
Reutter JC, Sanders K, et al Incidence of Allergic Reactions with Fresh Frozen Plasma or
Cryo-supernatant Plasma in the Treatment of Thrombotic Thrombocytopenic Purpura.
Journal of Clinical Apheresis 2001 16(3):134-138.
Retrospective Analysis of TTP patients 1982-1999
received all FFP or all CPP (n=41)
not premedicated with antihistamine (e.g. Benadryl) until after 1st rxn

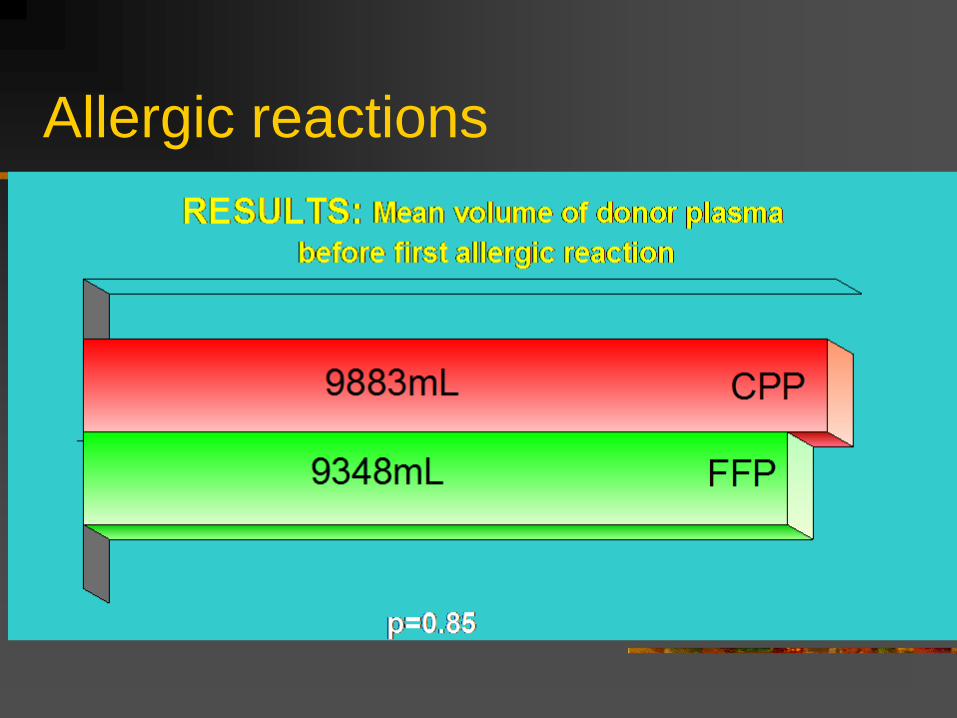
Allergic reactions
Allergic reactions

Allergic reactions
Urticaria/hives are commonly seen in TTP
patients
frequency of 55%-76%
tend to occur after 30 to 35 donor
exposures
or 9 to 10 liters of plasma
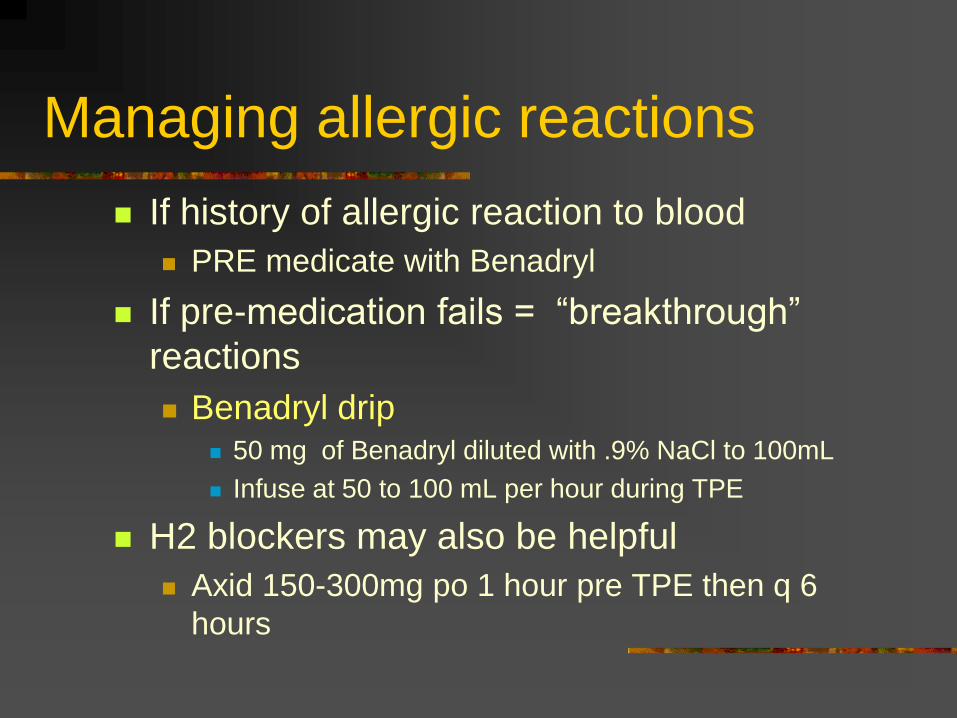
Managing allergic reactions
If history of allergic reaction to blood
PRE medicate with Benadryl
If pre-medication fails = “breakthrough”
reactions
Benadryl drip 50 mg of Benadryl diluted with .9% NaCl to 100mL
Infuse at 50 to 100 mL per hour during TPE
H2 blockers may also be helpful
Axid 150-300mg po 1 hour pre TPE then q 6
hours

Managing allergic reactions
For patients with severe plasma sensitivity or problematic frequent allergic reactions:
5% albumin and plasma
Initial half of the plasma exchange is done with 5% albumin
The second half of the procedure is completed with plasma
May also use this replacement combination for AB blood type

Management issues: citrate
ACD anticoagulation for apheresis plus citrate in
the plasma replacement.
Higher incidence of citrate related symptoms
Paresthesias
N & V
Hypotension
Flatus
EKG changes

Challenges for TTP
Unsure how long to treat and how close
to follow up
Currently cannot detect subclinical
disease
Cannot predict relapse
Still have mortality rate of 10%
ADAMTS13 (vWF protease) deficiency
not pathognomonic

TTP: On the Horizon
Multicenter studies:
NIH Transfusion Medicine/ Hemostasis Clinical Research Network 16 Academic Centers with a clinical
coordinating center
STAR Study now enrolling
TPE and rituximab versus TPE alone
Risk factors of TTP: Northwestern University (SERFTTP) NIH funded multicenter study
Epidemiology, risk factors (drugs), and pathophysiology


















