Regional Philadelphia Conference Philadelphia, Pennsylvania June 21-22, 2016 Transitional Care Interventions and Improving Outcomes in Heart Failure Learning Objectives 1. Identify and mitigate barriers to providing optimal care for patients with heart failure 2. Utilize recommendations, that are based on efficacy and safety, to co-manage patients with heart failure 3. Implement strategies to enhance the utilization of transitional care teams in order to improve patient- centered outcomes in heart failure Faculty Paul J. Hauptman, MD Professor of Internal Medicine Division of Cardiology Assistant Dean, Clinical and Translational Research St. Louis University School of Medicine St. Louis, Missouri James L. Januzzi, Jr., MD, FACC, FESC Hutter Family Professor of Medicine Harvard Medical School Roman DeSanctis Endowed Clinical Scholar Massachusetts General Hospital Faculty, Harvard Clinical Research Institute Boston, Massachusetts Slides are current as of the time of printing and may differ from the live presentation due to copyright issues. Please reference www.pri-med.com/PHI for the most up-to-date version of slide sets.
Transcript
Regional Philadelphia Conference Philadelphia, Pennsylvania
June 21-22, 2016
Transitional Care Interventions and Improving Outcomes
in Heart Failure
Learning Objectives
1. Identify and mitigate barriers to providing optimal care for patients with heart failure
2. Utilize recommendations, that are based on efficacy and safety, to co-manage patients with heart failure
3. Implement strategies to enhance the utilization of transitional care teams in order to improve patient-
centered outcomes in heart failure
Faculty Paul J. Hauptman, MD Professor of Internal Medicine Division of Cardiology Assistant Dean, Clinical and Translational Research St. Louis University School of Medicine St. Louis, Missouri James L. Januzzi, Jr., MD, FACC, FESC Hutter Family Professor of Medicine Harvard Medical School Roman DeSanctis Endowed Clinical Scholar Massachusetts General Hospital Faculty, Harvard Clinical Research Institute Boston, Massachusetts
Slides are current as of the time of printing and may differ from the live presentation due to copyright issues.
Please reference www.pri-med.com/PHI for the most up-to-date version of slide sets.
Overview
The goal of the proposed activity titled: Transitional Care Interventions and Improving Outcomes in Heart Failure, is to provide education on how to improve patient outcomes through the integration of evidence-based recommendations, effective transition of care strategies across the continuum of care, and the optimization of pharmacologic therapies for patients with chronic heart failure.
Heart Failure (HF)
• 5.7 million people in the United States have heart failure– 825,000 new HF cases annually
– Projected to increase by 46% from 2012 to 2030 resulting in >8 million people HF
• One in 9 deaths in 2009 included heart failure as contributing cause
• About half of people who develop heart failure die within 5 years of diagnosis.
CDC Available: http://www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_heart_failure.htm. Accessed: September 27, 2014.Go AS, et al. Circulation. 2014;129:e28-e292.
Improvement in Heart Failure Assessmentand Management is Needed
• Direct and indirect cost estimates for HF up to $56 billion annually
• Average HF admission costs between $7,000 - $13,000 USD/admission
• Re-hospitalization rate: 50% within 6 months
• Affordable Care Act has made HF readmission a major focus for improvement
Berkowitz R, et al. Lippincotts Case Manag. 2005 Nov-Dec;10(6 Suppl):S1-15.
Vicious Cycle of Congestion in AHFPrognosis in Heart Failure•Peak VO2•6min walk distance•NE;TNF;BNP;NT-ProBNP•AII;CRP;MPO;troponin•Non-candidacy for Tx•SWI; MR•Heart Rate; S3•Depression scale•Response on VAS•Duration of HF•History of SCD•Atrial fibrillation [?]•Diastolic parameters•Serial HRQoL assessments
•Intolerance to ACEI or ßB•NYHA•Demographics: Race; Age•TW alternans; QTdispersion•SA-ECG; QRS width•EF; EDD/EDV/ESD/ESV•Etiology•Inotrope dependence •ESR; HgB; Na; WBC•Re-admission; Hospitalization•Comorbidity index•RA; PCWP; PAP [?]•GFR; creatinine; ∆•Beta receptor polymorphism
BNP/NT-proBNP and Stage C HF Prognosis
Masson S, et al. Clin Chem. 2006 Aug;52(8):1528-1538.
The Importance of Serial NP Measurements for Prognostication in Chronic HF
Masson, et al, J Am Coll Cardiol. 2008 Sep 16;52(12):997-1003.
Predicting Mortality Among Patients Hospitalized for Heart Failure: Derivation and Validation of a Clinical Model
Lee DS, et al. JAMA. 2003 Nov 19;290(19):2581-2587.
Seattle Heart Failure Model
• Derived from Prospective Randomized Amlodipine Survival Evaluation-1 (PRAISE-1)
• Validated in:– Evaluation of Losartan in the Elderly 2 (ELITE2)
– Valsartan Heart Failure Trial (Val-HeFT)
– Randomized Etanercept North American Strategy to Study Antagonism of Cytokines (RENAISSANCE)
– Others
Levy WC. Am J Cardiol. 2013 Apr 15;111(8):1235.
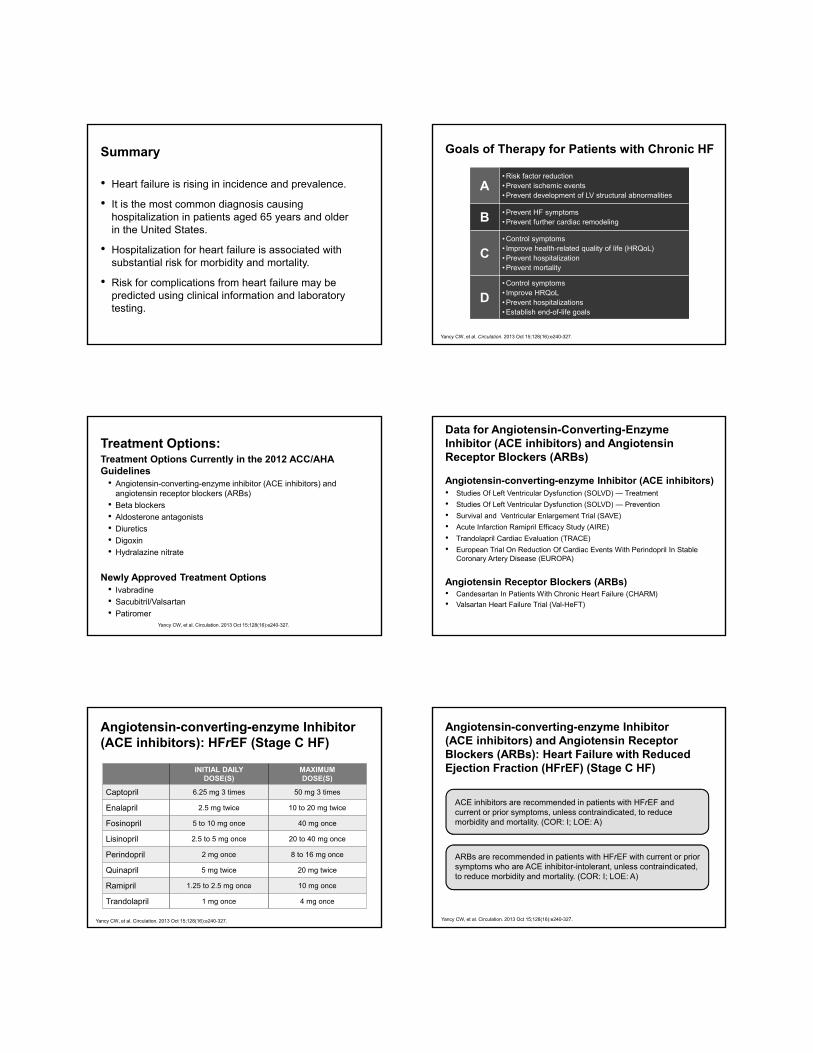
Summary
• Heart failure is rising in incidence and prevalence.
• It is the most common diagnosis causing hospitalization in patients aged 65 years and older in the United States.
• Hospitalization for heart failure is associated with substantial risk for morbidity and mortality.
• Risk for complications from heart failure may be predicted using clinical information and laboratory testing.
Goals of Therapy for Patients with Chronic HF
Yancy CW, et al. Circulation. 2013 Oct 15;128(16):e240-327.
A• Risk factor reduction• Prevent ischemic events• Prevent development of LV structural abnormalities
B • Prevent HF symptoms• Prevent further cardiac remodeling
C• Control symptoms• Improve health-related quality of life (HRQoL)• Prevent hospitalization• Prevent mortality
D• Control symptoms• Improve HRQoL• Prevent hospitalizations• Establish end-of-life goals
Treatment Options:Treatment Options Currently in the 2012 ACC/AHA Guidelines
• Angiotensin-converting-enzyme inhibitor (ACE inhibitors) and angiotensin receptor blockers (ARBs)
• Beta blockers
• Aldosterone antagonists
• Diuretics
• Digoxin
• Hydralazine nitrate
Newly Approved Treatment Options• Ivabradine
• Sacubitril/Valsartan
• PatiromerYancy CW, et al. Circulation. 2013 Oct 15;128(16):e240-327.
Data for Angiotensin-Converting-Enzyme Inhibitor (ACE inhibitors) and Angiotensin Receptor Blockers (ARBs)
Angiotensin-converting-enzyme Inhibitor (ACE inhibitors)• Studies Of Left Ventricular Dysfunction (SOLVD) — Treatment
• Studies Of Left Ventricular Dysfunction (SOLVD) — Prevention
• Survival and Ventricular Enlargement Trial (SAVE)
• Acute Infarction Ramipril Efficacy Study (AIRE)
• Trandolapril Cardiac Evaluation (TRACE)
• European Trial On Reduction Of Cardiac Events With Perindopril In Stable Coronary Artery Disease (EUROPA)
Angiotensin Receptor Blockers (ARBs)• Candesartan In Patients With Chronic Heart Failure (CHARM)
• Valsartan Heart Failure Trial (Val-HeFT)
Angiotensin-converting-enzyme Inhibitor (ACE inhibitors): HFrEF (Stage C HF)
INITIAL DAILYDOSE(S)
MAXIMUMDOSE(S)
Captopril 6.25 mg 3 times 50 mg 3 times
Enalapril 2.5 mg twice 10 to 20 mg twice
Fosinopril 5 to 10 mg once 40 mg once
Lisinopril 2.5 to 5 mg once 20 to 40 mg once
Perindopril 2 mg once 8 to 16 mg once
Quinapril 5 mg twice 20 mg twice
Ramipril 1.25 to 2.5 mg once 10 mg once
Trandolapril 1 mg once 4 mg once
Yancy CW, et al. Circulation. 2013 Oct 15;128(16):e240-327.
Angiotensin-converting-enzyme Inhibitor (ACE inhibitors) and Angiotensin Receptor Blockers (ARBs): Heart Failure with Reduced Ejection Fraction (HFrEF) (Stage C HF)
ACE inhibitors are recommended in patients with HFrEF and current or prior symptoms, unless contraindicated, to reduce morbidity and mortality. (COR: I; LOE: A)
Yancy CW, et al. Circulation. 2013 Oct 15;128(16):e240-327.
ARBs are recommended in patients with HFrEF with current or prior symptoms who are ACE inhibitor-intolerant, unless contraindicated, to reduce morbidity and mortality. (COR: I; LOE: A)
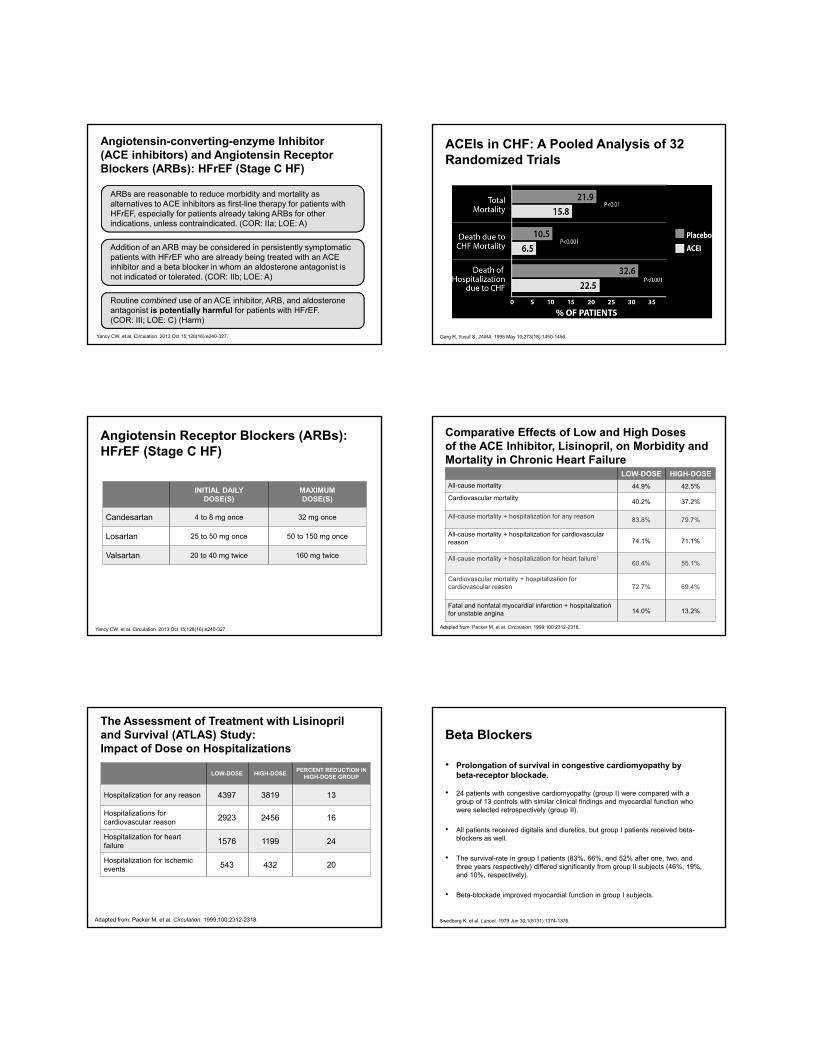
Angiotensin-converting-enzyme Inhibitor (ACE inhibitors) and Angiotensin Receptor Blockers (ARBs): HFrEF (Stage C HF)
ARBs are reasonable to reduce morbidity and mortality as alternatives to ACE inhibitors as first-line therapy for patients with HFrEF, especially for patients already taking ARBs for other indications, unless contraindicated. (COR: IIa; LOE: A)
Addition of an ARB may be considered in persistently symptomatic patients with HFrEF who are already being treated with an ACE inhibitor and a beta blocker in whom an aldosterone antagonist is not indicated or tolerated. (COR: IIb; LOE: A)
Yancy CW, et al. Circulation. 2013 Oct 15;128(16):e240-327.
Routine combined use of an ACE inhibitor, ARB, and aldosterone antagonist is potentially harmful for patients with HFrEF. (COR: III; LOE: C) (Harm)
ACEIs in CHF: A Pooled Analysis of 32 Randomized Trials
Garg R, Yusuf S. JAMA. 1995 May 10;273(18):1450-1456.
Angiotensin Receptor Blockers (ARBs):HFrEF (Stage C HF)
INITIAL DAILYDOSE(S)
MAXIMUMDOSE(S)
Candesartan 4 to 8 mg once 32 mg once
Losartan 25 to 50 mg once 50 to 150 mg once
Valsartan 20 to 40 mg twice 160 mg twice
Yancy CW, et al. Circulation. 2013 Oct 15;128(16):e240-327.
Comparative Effects of Low and High Doses of the ACE Inhibitor, Lisinopril, on Morbidity and Mortality in Chronic Heart Failure
Adapted from: Packer M, et al. Circulation. 1999;100:2312-2318.
1
LOW-DOSE HIGH-DOSE
All-cause mortality 44.9% 42.5%
Cardiovascular mortality40.2% 37.2%
All-cause mortality + hospitalization for any reason 83.8% 79.7%
All-cause mortality + hospitalization for cardiovascular reason 74.1% 71.1%
All-cause mortality + hospitalization for heart failure1
60.4% 55.1%
Cardiovascular mortality + hospitalization for cardiovascular reason 72.7% 69.4%
Fatal and nonfatal myocardial infarction + hospitalization for unstable angina 14.0% 13.2%
The Assessment of Treatment with Lisinopriland Survival (ATLAS) Study: Impact of Dose on Hospitalizations
Adapted from: Packer M, et al. Circulation. 1999;100:2312-2318.
LOW-DOSE HIGH-DOSEPERCENT REDUCTION IN
HIGH-DOSE GROUP
Hospitalization for any reason 4397 3819 13
Hospitalizations for cardiovascular reason 2923 2456 16
Hospitalization for heart failure 1576 1199 24
Hospitalization for ischemic events 543 432 20
Beta Blockers
• Prolongation of survival in congestive cardiomyopathy by beta-receptor blockade.
• 24 patients with congestive cardiomyopathy (group I) were compared with a group of 13 controls with similar clinical findings and myocardial function who were selected retrospectively (group II).
• All patients received digitalis and diuretics, but group I patients received beta-blockers as well.
• The survival-rate in group I patients (83%, 66%, and 52% after one, two, and three years respectively) differed significantly from group II subjects (46%, 19%, and 10%, respectively).
• Beta-blockade improved myocardial function in group I subjects.
Swedberg K, et al. Lancet. 1979 Jun 30;1(8131):1374-1376.
Effects of Sympathetic Activation and Norepinehrine
• Peripheral vasoconstriction
• Sodium retention and hypokalemia
• Induction of cardiac hypertrophy
• Restrict coronary vasodilation
• Increase automaticity of cardiac cells
• Increase in HR
• Potentiate activity of the Renin-Angiotensin System (RAS)
• Trigger of apoptosis via multiple pathways including oxidative stress
Data for Beta Blockers:
• US Carvedilol Trials (65%↓)
• Cardiac Insufficiency Bisoprolol Study II (CIBIS-2) (34%↓)
Plus: Carvedilol Post-Infarct Survival Control in Left Ventricular Dysfunction (CAPRICORN) and Carvedilol Or Metoprolol European Trial (COMET)
Exceptions: Beta-blocker Evaluation of Survival Trial (BEST) and Study of the Effects of Nebivolol Intervention on Outcomes and Re-hospitalisation in Seniors With Heart Failure (SENIORS)
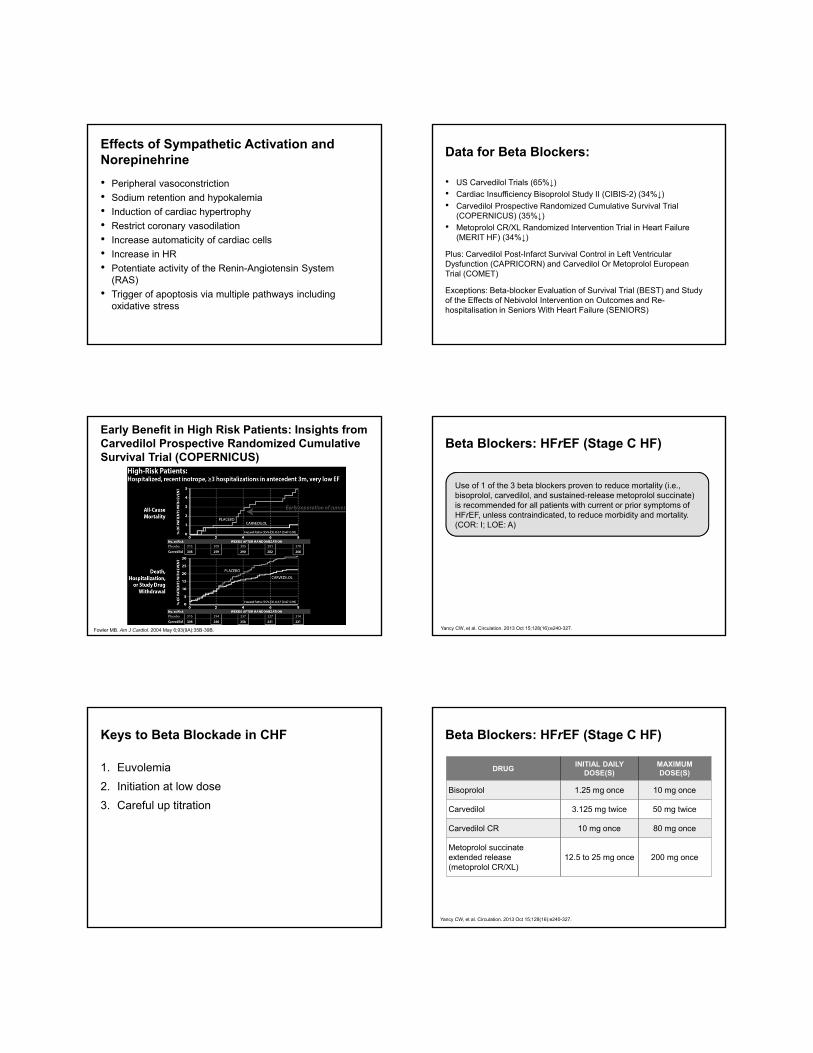
Early Benefit in High Risk Patients: Insights from Carvedilol Prospective Randomized Cumulative Survival Trial (COPERNICUS)
Fowler MB. Am J Cardiol. 2004 May 6;93(9A):35B-39B.
Beta Blockers: HFrEF (Stage C HF)
Use of 1 of the 3 beta blockers proven to reduce mortality (i.e., bisoprolol, carvedilol, and sustained-release metoprolol succinate) is recommended for all patients with current or prior symptoms of HFrEF, unless contraindicated, to reduce morbidity and mortality. (COR: I; LOE: A)
Yancy CW, et al. Circulation. 2013 Oct 15;128(16):e240-327.
Keys to Beta Blockade in CHF
1. Euvolemia
2. Initiation at low dose
3. Careful up titration
Beta Blockers: HFrEF (Stage C HF)
Yancy CW, et al. Circulation. 2013 Oct 15;128(16):e240-327.
Pitt B, et al. N Engl J Med. 1999;341(10):709-717.Zannad F, et al. N Engl J Med. 2011;364(1):11-21. Pitt B, et al. N Engl J Med. 2003;348(14):1309-1321.
Issues:1. 30-day event rate
2. b. Mechanism (K+ v. fibrosis)
3. c. Patient selection
Aldosterone antagonists: HErEF (Stage C HF)
Aldosterone receptor antagonists [or mineralocorticoid receptor antagonists (MRA)] are recommended in patients with NYHA class II-IV and who have LVEF of 35% or less, unless contraindicated, to reduce morbidity and mortality. Patients with NYHA class II should have a history of prior cardiovascular hospitalization or elevated plasma natriuretic peptide levels to be considered for aldosterone receptor antagonists. Creatinine should be 2.5 mg/dL or less in men or 2.0 mg/dL or less in women (or estimated glomerular filtration rate >30 mL/min/1.73m2) and potassium should be less than 5.0 mEq/L. Careful monitoring of potassium, renal function, and diuretic dosing should be performed at initiation and closely followed thereafter to minimize risk of hyperkalemia and renal insufficiency. (COR: I; LOE: A)
Yancy CW, et al. Circulation. 2013 Oct 15;128(16):e240-327.
Aldosterone antagonists: HErEF (Stage C HF)
Aldosterone receptor antagonists are recommended to reduce morbidity and mortality following an acute MI in patients who have LVEF of 40% or less who develop symptoms of HF or who have a history of diabetes mellitus, unless contraindicated. (COR: I; LOE: B)
Inappropriate use of aldosterone receptor antagonists is potentially harmful because of life-threatening hyperkalemia or renal insufficiency when serum creatinine greater than 2.5 mg/dL in men or greater than 2.0 mg/dL in women (or estimated glomerular filtration rate <30 mL/min/1.73m2), and/or potassium above 5.0 mEq/L. (COR: III; LOE: B) (Harm)
Yancy CW, et al. Circulation. 2013 Oct 15;128(16):e240-327.
Aldosterone Antagonists: HFrEF (Stage C HF)
Yancy CW, et al. Circulation. 2013 Oct 15;128(16):e240-327.
DRUGINITIAL DAILY
DOSE(S)MAXIMUMDOSE(S)
Spironolactone 12.5 to 25 mg once 25 mg once or twice
Eplerenone 25 mg once 50 mg once
Diuretics: HFrEF (Stage C HF)
Diuretics are recommended in patients with HFrEF who have evidence of fluid retention, unless contraindicated, to improve symptoms. (COR: I; LOE: C)
Yancy CW, et al. Circulation. 2013 Oct 15;128(16):e240-327.
Data for Digoxin
Issues:
1. Not tested in the Beta Blocker era
2. Gender concerns
3. Efficacy and serum dig concentration
4. Mechanism of action?
Dig use is decreasing - Acute Decompensated Heart Failure National Registry (ADHERE) and Trial of Lifestyle Interventions for Blood Pressure Control (PREMIER) data
Digoxin: HFrEF (Stage C HF)
Digoxin can be beneficial in patients with HFrEF, unless contraindicated, to decrease hospitalizations for HF. (COR: IIa; LOE: B)
Yancy CW, et al. Circulation. 2013 Oct 15;128(16):e240-327.
The combination of hydralazine and isosorbide dinitrate is recommended to reduce morbidity and mortality for patients self-described as African Americans with NYHA class III–IV HFrEFreceiving optimal therapy with ACE inhibitors and beta blockers, unless contraindicated. (COR: I; LOE: A)
Yancy CW, et al. Circulation. 2013 Oct 15;128(16):e240-327.
A combination of hydralazine and isosorbide dinitrate can be useful to reduce morbidity or mortality in patients with current or prior symptomatic HFrEF who cannot be given an ACE inhibitor or ARB because of drug intolerance, hypotension, or renal insufficiency, unless contraindicated. (COR: IIa; LOE: B)
Hydralazine Nitrate: HFrEF (Stage C HF)
DRUGINITIAL DAILY
DOSE(S)MAXIMUMDOSE(S)
Hydralazine and isosorbide dinitrate
Hydralazine: 25 to 50 mg, 3 or 4 times daily and isorsorbide dinitrate: 20 to 30 mg 3 or 4 times daily
Hydralazine: 300 mg daily in divided doses and isosorbide dinitrate 120 mg daily in divided doses
Yancy CW, et al. Circulation. 2013 Oct 15;128(16):e240-327.
Treatment Options:
Treatment Options Currently in the Guidelines• Angiotensin-converting-enzyme Inhibitor (ACE inhibitors) and
• Ivabradine is a hyperpolarization-activated cyclic nucleotide-gated channel blocker indicated to reduce the risk of hospitalization for worsening heart failure in patients with stable, symptomatic chronic heart failure with left ventricular ejection fraction ≤ 35%, who are in sinus rhythm with resting heart rate ≥ 70 beats per minute and either are on maximally tolerated doses of beta blockers or have a contraindication to beta-blocker use.
• This medication was approved on April 15, 2015.
FDA News Release. Available: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm442978.htm.Accessed: March 2, 2016.
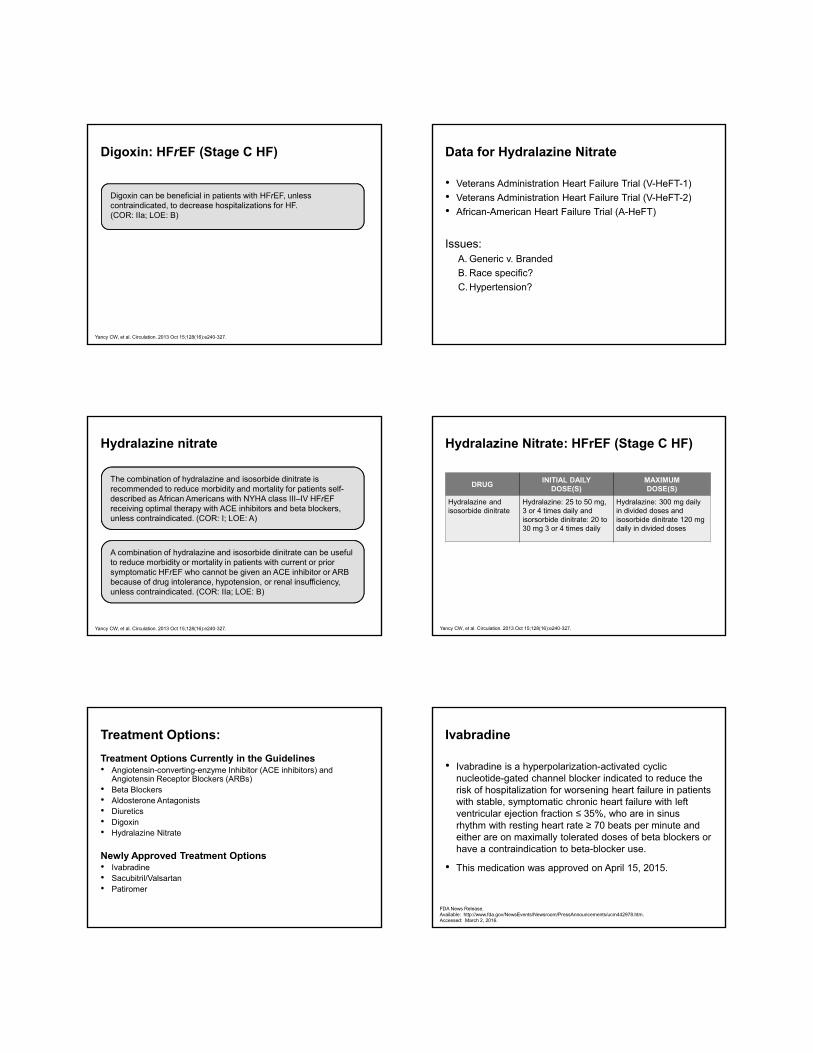
Heart Rate Reduction Through /f Current Inhibition
Adapted from: Thollon C, et al. Br J Pharmacol. 1994;112:37-42. DiFrancesco A, et al. Drugs. 2004;64:1757-1765.
Ivabradine and Outcomes in Chronic HF:The SHIFT Study
• Double blind, placebo controlled randomized controlled trial in symptomatic HF patients in normal sinus rhythm with HR >70 beats/min and EF <0.35.
• Patient were hospitalized within past year and on stable Rx including a beta blocker, if tolerated.
• Randomized to ivabradine 7.5 mg bid or placebo.
• Primary end-point was cardiovascular death or HF hospitalization.
Swedberg K, et al. Lancet. 2010 Sep 11;376(9744):875-885.
Background Rx in Systolic Heart Failure Treatment with the /f Inhibitor IvabradineTrial (SHIFT)
Swedberg K, et al. Lancet. 2010 Sep 11;376(9744):875-885.
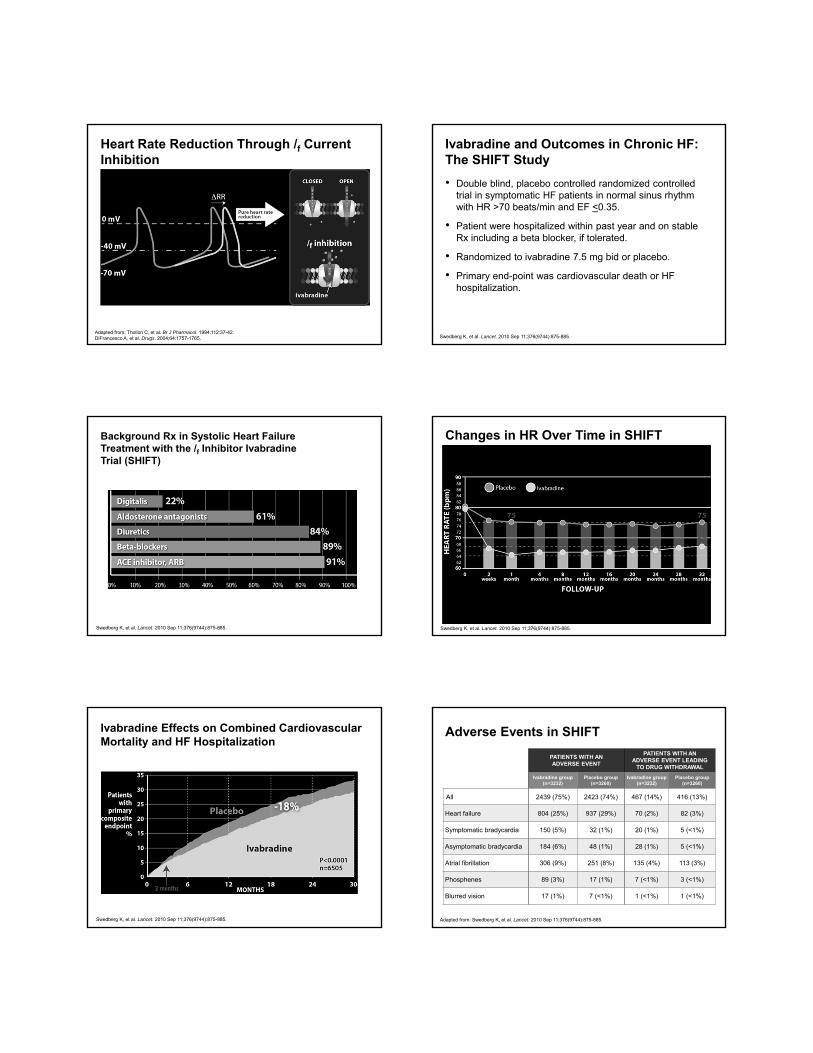
Changes in HR Over Time in SHIFT
Swedberg K, et al. Lancet. 2010 Sep 11;376(9744):875-885.
Ivabradine Effects on Combined Cardiovascular Mortality and HF Hospitalization
Swedberg K, et al. Lancet. 2010 Sep 11;376(9744):875-885.
Adverse Events in SHIFT
Adapted from: Swedberg K, et al. Lancet. 2010 Sep 11;376(9744):875-885.
• Starting dose is 5 mg twice daily. After 2 weeks of treatment, adjust dose based on heart rate. The maximum dose is 7.5 mg twice daily.
• In patients with conduction defects or in whom bradycardia could lead to hemodynamic compromise, initiate dosing at 2.5 mg twice daily.
FDA News Release. Available: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm442978.htm.Accessed: March 2, 2016.
Sacubitril / Valsartan
• Combination therapy containing sacubitril, a neprilysininhibitor, and valsartan, an angiotensin II receptor blocker (ARB)
• Indicated to reduce the risk of cardiovascular death and hospitalization for heart failure (HF) in patients with chronic heart failure (CHF) (NYHA class II-IV) and reduced ejection fraction
• Approved July 7, 2015
Fala L. Am Health Drug Benefits. 2015 Sep; 8(6):330-334.
Sacubitril / Valsartan – First in Class Dual-acting Angiotensin Receptor Neprilysin Inhibitor
• Sacubitril / Valsartan is a crystalline complex comprised of 6 valsartan moieties together with 6 moieties of a neprilysininhibitor, sacubitril (AHU377).
• Valsartan in LCZ696 (now known as Entresto) is present in anionic form, and is thus more bioavailable than in valsartan as a free acid. 200mg of LCZ696 is equivalent to 160mg of standard valsartan
• The combination of valsartan (ARB) and sacubitril (neprilysininhibitor) is though to work synergistically to block deleterious RAS activation while enhancing endogenous protective pathways.
Gu et al. J Clin Pharmacol 2010Vardeny et al. Clin Pharmacol Ther 2013Vardeny et al. JACC Heart Fail 2014
Sacubitril / Valsartan Mechanism of Action
Prospective Comparison of ARNI with ACE-I to Determine Impact on Global Mortality and Morbidity in Heart Failure (PARADIGM-HF) Study Sacubitril/valsartan in HFrEF Patients
• Phase III RCT evaluating the efficacy and safety profile of Sacubitril/valsartan vs enalapril in 8,436 patients with NYHA Class II-IV symptoms, EF <35% and elevated BNP level.
• Open label run-in may have selected responders
• Primary endpoint - Sacubitril/valsartan is superior to enalapril in delaying time to composite of CV mortality and HF hospitalization.
• PARADIGM-HF was prematurely stopped by the DMC due to evidence that patients receiving Sacubitril/valsartan lived longer without being hospitalized for heart failure than those who received standard care with ACE-inhibitor enalapril.
McMurray JJ, et al. N Engl J Med. 2014 Sep 11;371(11):993-1004.
PARADIGM-HF: Outcomes
McMurray JJ, et al. N Engl J Med. 2014 Sep 11;371(11):993-1004.
Sacubitril/
valsartan
(n=4187)
Enalapril
(n=4212)
Hazard Ratio
(95% CI)
P
Value
Primary endpoint914
(21.8%)
1117
(26.5%)
0.80
(0.73-0.87)0.0000002
Cardiovascular
death
558
(13.3%)
693
(16.5%)
0.80
(0.71-0.89)0.00004
Hospitalization for
heart failure
537
(12.8%)
658
(15.6%)
0.79
(0.71- 0.89)0.00004
All Cause Mortality711
(16.9%)
835
(19.8%)
0.84
(0.76-0.93)0.0001
PARADIGM-HF: Effects of Sucubitril/Valsartan vs. Enalapril
Adverse Events During Randomized Treatment
Adapted from: McMurray JJ, et al. N Engl J Med. 2014 Sep 11;371(11):993-1004.
* Shown are results of the analyses of prespecified safety events at any time after randomization. The numbers of patients who permanently discontinued a study drug were as follows: for hypotension, 36 (0.9%) in the LCZ696 groupand 29 (0.7%) in the enalapril group (P = 0.38); for renal impairment, 29 (0.7%) and 59 (1.4%), respectively (P = 0.002); and for hyperkalemia, 11 (0.3%) and 15 (0.4%), respectively (P = 0.56).** Angioedema was adjudicated in a blinded fashion by an expert committee.
EVENT Sacubitril/Valsartan(N=4187)
Enalapril(N=4212)
HYPOTENSION
SymptomaticSymptomatic with systolic blood pressure <90 mm Hg
588 (14.0)
112 (2.7)
388 (9.2)
59 (1.4)
ELEVATED SERUM CREATININE
≥ 2.5 mg/dl≥ 3.0 mg/dl
139 (3.3)
63 (1.5)
188 (4.5)
83 (2.0)
ELEVATED SERUM POTASSIUM
> 5.5 mmol/liter
> 6.0 mmol/liter
674 (16.1)
181 (4.3)
727 (17.3)
236 (5.6)
COUGH 474 (11.3) 601 (14.3)
ANGIOEDEMA**
No treatment or use of antihistamines only
Use of catecholamines or glucocorticoids without hospitalization
Hospitalization without airway compromise
Airway compromise
10 (0.2)
6 (0.1)
3 (0.1)
0
5 (0.1)
4 (0.1)
1 (<0.1)
0
Effect of Sacubitril / Valsartan on Natriuretic Peptide (NPs)
Sacubitril / Valsartan Dose Selection and Titration
Equivalent of >10mg Enalapril:Lisinopril >10mgRamipril >5mg
STOP ACEifor 36 hoursbefore starting
Valsartan/Sacubitril to prevent angioedema
Start Valsartan/Sacubitril 49/51mg bid, increase to 97/103mg bid in 2-4 weeks
Equivalent of ≤10mg Enalapril:Lisinopril ≤10mgRamipril ≤5mg
Start Valsartan/Sacubitril 24/26mg bid, increase to 49/51mg bid in 2-4 weeks, and then 97/103mg bid
Equivalent of > 160mg Valsartan:Losartan > 50mgOlmesartan > 10mg
Start Valsartan/Sacubitril 49/51mg bid, increase to 97/103mg bid in 2-4 weeks
Equivalent of ≤ 160mg Valsartan:Losartan ≤ 50mgOlmesartan ≤ 10mg
Start Valsartan/Sacubitril 24/26mg bid, increase to 49/51mg bid in 2-4 weeks, and then 97/103mg bid
Not currently taking ACEi’sor ARB’s
Start Valsartan/Sacubitril 24/26mg bid, increase to 49/51mg bid in 2-4 weeks, and then 97/103mg bid
Patiromer
• Patiromer is a polymer anion and a calcium sorbitol counterion complex that binds potassium in the lumen of the gastrointestinal tract and increases fecal potassium excretion, leading to lower serum potassium levels.
• This medication was approved on October 21, 2015.
1. Bushinsky DA, et al. Poster presented at: ASN Kidney Week 2014; Philadelphia, PA; November 11-16, 2014; Poster SA-PO153.
2. Weir MR, et al. N Engl J Med. 2015;372(3):211-221.
Patiromer
• Patiromer is indicated for the treatment of hyperkalemia.
• Adult Dosage: Oral: Initial: 8.4 g once daily; adjust dose at ≥1-week intervals in increments of 8.4 g (maximum dose: 25.2 g/day).
1. Bushinsky DA, et al. Poster presented at: ASN Kidney Week 2014; Philadelphia, PA; November 11-16, 2014; Poster SA-PO153.
2. Weir MR, et al. N Engl J Med. 2015;372(3):211-221.
Evaluation of the Efficacy and Safety of Patiromer (PEARL-HF)
One hundred and five patients with HF and a history of hyperkalaemiaresulting in discontinuation of a renin-angiotensin-aldosterone system inhibitor/blocker and/or beta-adrenergic blocking agent or chronic kidney disease (CKD) with an estimated glomerular filtration rate of <60 mL/min were randomized to double-blind treatment with 30 g/day Patiromer or placebo for 4 weeks.
In Development
• Sodium zirconium cyclosilicate (ZS-9) is an insoluble, non-absorbed zirconium silicate with a high in-vitro binding capacity for potassium ions even in the presence of other competing ions.
• A new drug application was rejected for this medication by the U S Food and Drug Administration on May 26, 2016.
Drugs.com. ZS Pharma Announces FDA Acceptance of ZS-9 New Drug Application. Available: http://www.drugs.com/nda/zs_9_150729.html. Accessed: March 3, 2016..
AstraZeneca. Complete Response Letter from US FDA. Available: https://www.astrazeneca.com/media-centre/press-releases/2016/astrazeneca-receives-complete-response-letter-from-us-fda-for-sodium-zirconium-cyclosilicate-zs-9-for-oral-suspension-for-treatment-of-hyperkalaemia-27052016.html. Accessed: June 1, 2016.
Device Therapy Considerations
• Once medical therapy has been optimized, patients who continue to have an ejection fraction less than 35% should be considered for device therapy and referral to a specialists.
ACC / AHA Guidelines for HFpEF
Yancy CW, et al. Circulation. 2013 Oct 15;128(16):e240-327.
Systolic and diastolic blood pressure should be controlled according to published clinical practice guidelines. (COR: I; LOE: B)
Diuretics should be used for relief of symptoms due to volume overload. (COR: I; LOE: C)
Coronary revascularization for patients with CAD in whom angina or demonstrable myocardial ischemia is present despite GDMT. (COR: IIa; LOE: C)
Management of Atrial Fibrillation (AF) according to published clinical practice guidelines for HFpEF to improve symptomatic HF. (COR: IIa; LOE: C)
Use of beta-blocking agents, ACE inhibitors, and ARBs for hypertension in HFpEF. (COR: IIa; LOE: C)
ARBs might be considered to decrease hospitalizations in HFpEF. (COR: IIb; LOE: B)
Nutritional supplementation is not recommended in HFpEF. (COR: No Benefit; LOE: C)
2016 American College of Cardiology, American Heart Association and Heart Failure Society of America updated guidelines
Ivabradine can be beneficial to reduce HF hospitalization for patients with symptomatic (NYHA class II-III) stable chronic HFrEF (LVEF ≤35%) who are receiving guideline directed evaluation and management (GDEM), including a beta blocker at maximum tolerated dose, and who are in sinus rhythm with a heart rate of 70 bpm or greater at rest (37-40). (COR: IIa; LOE: B-R)
Yancy CW, et al. Circulation. 2016 May 20. [Epub ahead of print].
In patients with chronic symptomatic HFrEF NYHA class II or III who tolerate an ACE inhibitor or ARB, replacement by an ARNI is recommended to further reduce morbidity and mortality. (COR: I; LOE: ARNI: B-R) (sacubitril/valsartan)
Jencks SF, et al. N Engl J Med. 2009 Apr 2;360(14):1418-1428.
Re-Admissions Data: Context
• Diagnosis: Heart Failure
– 26.9% -30 day readmission
– 7.6% -proportion of all readmissions
• Reasons:
– Heart Failure 37.0%
– Pneumonia 5.1%
– Renal Failure 3.9%
Jencks SF, et al. N Engl J Med. 2009 Apr 2;360(14):1418-1428.
Prognostication in Heart Failure Can Be Simple: Impact of Hospitalizations
Setoguchi S, et al. Am Heart J. 2007 Aug;154(2):260-266.
Penalties, Year One
• Year One: Maximum penalty of 1% of Medicare billings for Heart Failure, Pneumonia and Post MI.
• Year Three: Maximum penalty of 3%
• Now includes 30-day readmissions following Total Hip and Total Knee Replacement surgery and COPD
“Hospital Readmissions Reduction Program”
Joynt K et al JAMA 2013
Penalties, Year One
“Hospital Readmissions Reduction Program”
Joynt K et al JAMA 2013
Hospitals with High Penalties(mean 0.72%)
Characteristic Percent Penalized Multivariable Adjusted OR
Hospital Size Large 40 1.98
Medium 35 2.09
Small 28 1.0 (ref)
Teaching Status Major 44 1.56
Not 33 1.0 (ref)
Safety Net Yes 44 2.38
No 30 1.0 (ref)
Penalties, Year Four
• Hospitals penalized: 2592 based on data from July 11-Jun 14
• Total penalties $420,000,000
• Only 209 were not penalized in the prior round
• Mean payment reduction: 0.61
• Number with max penalty (3.00): 39
• Number with penalty ≥1.00: 506
“Hospital Readmissions Reduction Program”
Rau J. Kaiser Health News, Aug 5, 2015
Re-Admission Themes
1. Hospitals at risk fit a pattern
2. Regional differences exist
3. Length of stay is not divorced from re-admission
4. Interventions Matter
5. Not all Interventions Matter
6. Rates of readmissions may not be an indicator of quality of hospital care
7. Will decreased readmissions lead to lower mortality or is that not the point?
Hospital Re-Admission Performance and Patterns of Re-Admission: Retrospective Cohort Study of Medicare Admissions
Dharmarajan K, et al. BMJ. 2013 Nov 20;347:f6571.
High performing: 30-day RSRR lower than the national rate with >95% probability.Low performing:30-day RSRR higher than the national rate with >95% probability
Predictors of Re-Admission:Not Physiology?
Causes of Hospital Readmission forHeart Failure
Ashton CM, et al. Ann Intern Med. 1995 Mar 15;122(6):415-421.
Predictors of Re-Admission:Not Physiology?
An automated model to identify heart failure patients at risk for 30-day readmission or death using electronic medical record data.
Amarasingham R, et al. Med Care. 2010 Nov;48(11):981-988.
Multivariable 30-Day Predictors
Amarasingham R, et al. Med Care. 2010 Nov;48(11):981-988.
Demographics, Health Behavior, Utilization (all p<0.05)
History of depression / anxiety 1.44
Single / Male 1.47 / 1.37
Number of home address changes 1.13
Residence in lowest socioeco quartile 1.30
History of Cocaine 1.78
History of missed clinic visit 1.35
Use of health system pharmacy 0.72
Prior in-patient hospitalizations 1.17
Presented to Emergency Department (ED) between 0600-1800
1.38
Roles of Nonclinical and Clinical Data in Prediction of 30-day Re-Hospitalization or Death Among Heart Failure Patients
Multivariable Predictive Model of 30-Day Death or Re-Admission With the Use of Clinical Data
Huynh QL, et al. J Card Fail. 2015 May;21(5):374-381.
Roles of Nonclinical and Clinical Data in Prediction of 30-day Re-Hospitalization or Death Among Heart Failure Patients
Multivariable Predictive Model of 30-Day Death or Re-Admission With the Use of Nonclinical Data
1. Length of hospital stay (per 3 days)
2. Living alone (vs. Living with family/relatives)
3. Age at admission (per year)
4. Discharge during winter (vs. other seasons)
5. Remoteness index categories
6. Number of coded diagnoses at discharge
7. Male sex
Huynh QL, et al. J Card Fail. 2015 May;21(5):374-381.
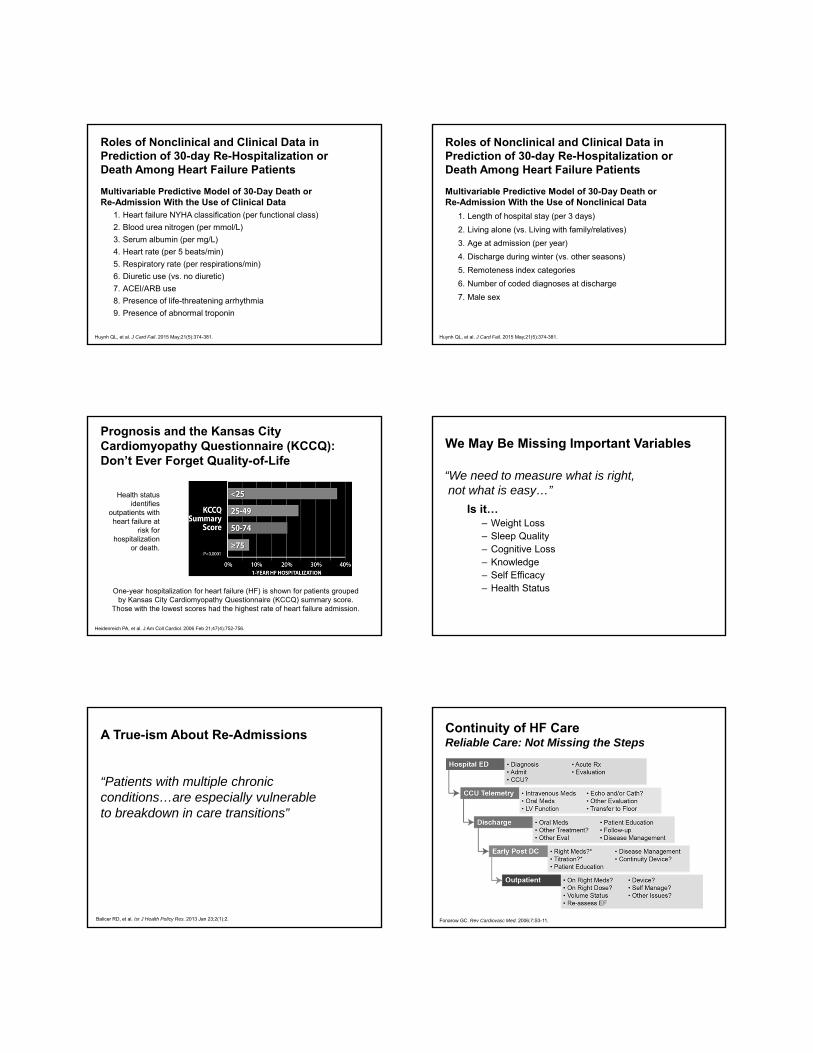
Prognosis and the Kansas City Cardiomyopathy Questionnaire (KCCQ): Don’t Ever Forget Quality-of-Life
Health status identifies
outpatients with heart failure at
risk for hospitalization
or death.
One-year hospitalization for heart failure (HF) is shown for patients grouped by Kansas City Cardiomyopathy Questionnaire (KCCQ) summary score.
Those with the lowest scores had the highest rate of heart failure admission.
Heidenreich PA, et al. J Am Coll Cardiol. 2006 Feb 21;47(4):752-756.
We May Be Missing Important Variables
Is it…– Weight Loss– Sleep Quality– Cognitive Loss– Knowledge– Self Efficacy– Health Status
“We need to measure what is right, not what is easy…”
A True-ism About Re-Admissions
Balicer RD, et al. Isr J Health Policy Res. 2013 Jan 23;2(1):2.
“Patients with multiple chronic conditions…are especially vulnerable to breakdown in care transitions”
Continuity of HF CareReliable Care: Not Missing the Steps
Fonarow GC. Rev Cardiovasc Med. 2006;7:S3-11.
Inpatient and Transitions of Care
Multidisciplinary HF disease-management programs are recommended for patients at high risk for hospital readmission, to facilitate the implementation of GDMT, to address different barriers to behavioral change, and to reduce the risk of subsequent re hospitalization for HF. (COR: I; LOE: B)
Yancy CW, et al. Circulation. 2013 Oct 15;128(16):e240-327.
Scheduling an early follow-up visit (within 7 to 14 days) and early telephone follow-up (within 3 days) of hospital discharge is reasonable. (COR: IIa; LOE: B)
Use of clinical risk prediction tools and/or biomarkers to identify patients at higher risk for postdischarge clinical events is reasonable. (COR: IIa; LOE: B)
Hospital Variation in Early Follow-up After Heart Failure Hospitalization
Follow-up Visit within 7 days = 37.5%
225 Hospitals
Hernandez et al. JAMA. 2010;303:1716-1722.
Better Effectiveness After Transition –Heart Failure (BEAT-HF)• 1437 patients hospitalized for HF were randomized to health coaching calls and
telemonitoring (N = 715) or to the usual care arm (N = 722) for 180 days.
• Telemonitoring used electronic equipment that collected daily information about blood pressure, heart rate, symptoms, and weight. Centralized registered nurses conducted telemonitoring reviews, protocolized actions, and telephone calls.
• 83% of the 715 patients in the intervention arm used the telemonitoring equipment, resulting in 221,211 remote observations.
• Patients received a median of six calls during the 6-month study.
• Despite the intervention, no significant effect on the 30 or 180-day readmission rate. The adjusted 30-day all-cause mortality rate was significantly decreased in the intervention arm, but not the 180-day mortality rate.
Ong MK, et al. JAMA Intern Med. 2016 Mar 1;176(3):310-318.
Wireless Pulmonary Artery Hemodynamic Monitoring in Chronic Heart Failure: A Randomized Controlled Trial
• 550 patients with NYHA class III heart failure with both preserved and reduced LVEF and previous hospital admission for heart failure were randomly assigned to management with a wireless implantable hemodynamic monitoring (W-IHM) system (treatment group) or to a control group for at least 6 months.
• In 6 months, 83 heart-failure-related hospitalizations were reported in the treatment group (n=270) compared with 120 in the control group (n=280).
• Now FDA approved
Abraham WT, et al. Lancet. 2011;377(9766):658-666.
H2H Strategies to Reduce HF
1. ≥ 1 Quality Improvement team for reducing readmission for HF
2. Monitor proportion of discharged patients with follow-up appointment within 7 days
3. Monitor 30-day readmission rates
4. Provide info about medications --purpose, which were new, which changed in dose/frequency, which stopped
5. Have pharmacist conduct medication reconciliation at discharge
American College of Cardiology. H2H Available: http://cvquality.acc.org/en/Initiatives/H2H/About-H2H.aspx. Accessed: March 2, 2016.
H2H Strategies to Reduce HF
6. Provide patients/caregivers direct contact info for a specific physician (for emergencies)
7. Arrange an outpatient follow-up appointment before patients leave the hospital
8. Ensure outpatient physicians are alerted to patient’s discharge within 48hours
9. Call patients regularly post discharge; follow- up on needs or to provide education
American College of Cardiology. H2H Available: http://cvquality.acc.org/en/Initiatives/H2H/About-H2H.aspx. Accessed: March 2, 2016.
In Conclusion
• 5.7 million people in the United States have heart failure– 825,000 new HF cases annually
– Projected to increase by 46% from 2012 to 2030 resulting in >8 million people HF
• About half of people who develop heart failure die within 5 years of diagnosis.
• There are multiple medications available for the treatment of HFrEFincluding new meds released in the last year.
• There are few effective therapies for patients with normal ejection fraction HF.
• Re-admissions for HF remain a continuing and costly problem.
• Strategies to reduce readmission include early follow-up, guideline directed therapy and improved communication with PCPs
CDC Available: http://www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_heart_failure.htm. Accessed: September 27, 2014.Go AS, et al. Circulation. 2014;129:e28-e292.