Stop overuse of antibiotics in humans – rational use Dominique L. Monnet, Senior Expert and Head of Disease Programme Antimicrobial resistance and Healthcare-associated infections (ARHAI) European Centre for Disease Prevention and Control Copenhagen, 15 March 2012
Transcript
Stop overuse of antibiotics in humans – rational use Dominique L. Monnet, Senior Expert and Head of Disease Programme Antimicrobial resistance and Healthcare-associated infections (ARHAI) European Centre for Disease Prevention and Control
Copenhagen, 15 March 2012
Scenario planning: key certainties
• Antibiotic resistance will exist as long as antibiotics are used
• New resistance mechanisms will necessarily emerge
• Antibiotics will always be misused to a certain extent
• Compliance with hand hygiene and other infection control measures will never be 100%
Photo: FreeFoto.cm
Disclaimer: The expert opinion expressed on this slide is personal and may not be understood or quoted as being made on behalf of or reflecting the position of ECDC.
Antibiotic resistance: a battle that we can can win?
3
270
280
290
300
310
320
330
1000 1200 1400 1600 1800 2000 Car
bo
n d
ioxi
de
mix
ing
rati
o in
ice
core
s (P
PM
)
Year
Carbon dioxide mixing ratio in ice cores, Antarctica (PPM)
Antibiotics discovered
Source: Etheridge et al. (CSIRO), Carbon Dioxide Information Analysis Center, http://cdiac.ornl.gov; Danish Staphylococcus Reference Laboratory, Statens Serum Institut, Denmark; and EARSS/EARS-Net.
0
20
40
60
80
100
MR
SA (
%)
MRSA, Denmark (blood, %, Y-2 axis)
MRSA, EU (blood and CSF, population-weighted %, Y-2 axis)
Prevention and control of AMR
Activities in only a few countries
Activities in many countries
No
Yes
Scenario planning: uncertainties and implications
Ne
w a
nti
bio
tics w
ith
a
no
ve
l m
ech
an
ism
of
acti
on
• Must rely on rational use of existing antibiotics and on infection control
• Mitigation an achievable goal?
• Must rely on rational use of existing antibiotics and infection control
• Increase awareness among new generations
• New antibiotics always essential
• Focus on rational use of new and other antibiotics
• Re-emphasise infection control
• Market for new antibiotics mostly empiric treatment of severe inf.
• Focus on detection and control of emerging AMR
• Re-emphasise rational use of antibiotics
Disclaimer: The expert opinion expressed on this slide is personal and may not be understood or quoted as being made on behalf of or reflecting the position of ECDC.
What is rational use of antibiotics in human medicine?
5
• No self-medication
• Only when prescribed by a medical doctor (or a nurse)
• Only when indicated
• Correct dose
• Correct dose intervals
• Correct duration
Antibiotics obtained without a prescription EU Member States, 2002 & 2009
0
5
10
15
20
Aust
ria
Belg
ium
Bulg
aria
Cypru
s
Cze
ch R
ep.
Denm
ark
Est
onia
Fin
land
Fra
nce
Germ
any
Gre
ece
Hungary
Irela
nd
Italy
Latv
ia
Lithuania
Luxem
bourg
Malta
Neth
erlands
Pola
nd
Port
ugal
Rom
ania
Slo
vakia
Slo
venia
Spain
Sw
eden
UK
Resp
ondents
who o
bta
ined
antibio
tics
without
a p
resc
ription
at
a p
harm
acy
or
els
ew
here
(%
)
Eurobarometer (2002)
Eurobarometer (2009)
Source: European Commission, Eurobarometer. In: Lancet Infect Dis 2012 Mar;12(3):182-3.
Sales of antibiotics without prescription: SWOT analysis
7
Strengths Weaknesses
• EU Directive transposed in the national law of each individual Member State
• Some Member States are taking action
• Varying levels of law enforcement
• National habits and cultural differences (can law be enforced when the public and professionals are not aware of the need for change?)
• Potential savings for national insurance systems (prescription-only medicines obtained OTC often are reimbursed)
• Pressure for change of some antibiotics from prescription- only medicine to pharmacy (POM-to-P) status (already in UK for azithromycin for proven Chlamydia infection)
Opportunities Threats
A.C.T.I.O.N.
A.C.T.I.O.N.
Disclaimer: The expert opinion expressed on this slide is personal and may not be understood or quoted as being made on behalf of or reflecting the position of ECDC.
Impact of regulation on ”prescription only” sales of antibiotics, Chile
8
• Sep. 1999: regulatory measures introduced as part of ”Action plan to assure rational Antibiotic Use”, incl.: • Restriction of antibiotic sales to prescription-only
• Enforced supervision by regulatory authorities
• Public campaign, leaflets and posters in pharmacies
• 1998 to 2002: sales of oral antibiotics decreased by 43%
• Since 2002: increase to a level close to the 1997 baseline
• Need for other concomitant interventions, e.g. improving the knowledge and attitudes of consumers and prescribers
Source: The evolving threat of antimicrobial resistance. WHO, 2012.
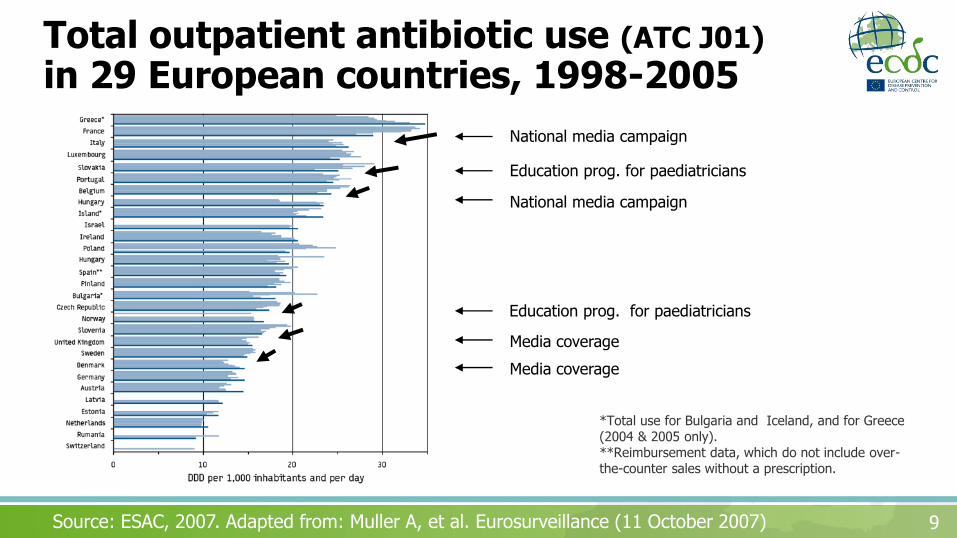
Total outpatient antibiotic use (ATC J01) in 29 European countries, 1998-2005
9 Source: ESAC, 2007. Adapted from: Muller A, et al. Eurosurveillance (11 October 2007)
*Total use for Bulgaria and Iceland, and for Greece (2004 & 2005 only). **Reimbursement data, which do not include over-the-counter sales without a prescription.
National media campaign
National media campaign
Media coverage
Media coverage
Education prog. for paediatricians
Education prog. for paediatricians
Decreases in antimicrobial resistance following national media campaigns
10 Source: French Nat. Ref. Ctr. for S. pneumoniae (Courtesy: E. Varon, L. Gutmann & B. Schlemmer) & Belgian Nat. Ref. Ctrs. for S. pneumoniae and for S. pyogenes (Courtesy: BAPCOC, H. Goossens)
Awareness campaigns on the prudent use of antibiotics / AMR: SWOT analysis
11
Strengths Weaknesses
• Several examples of best practice in Member States
• European Antibiotic Awareness Day (antibiotic.ecdc.europa.eu)
• Cultural differences between Member States
• Must be repeated every year
• Potential large savings for national insurance systems (8€ saved for 1€ invested)
• Use national culture characteristics as levers for change
• ”Campaign fatigue” (need to regularly vary and update key messages)
• Communicating on AMR (rather than prudent use) may lead to more prescriptions
Opportunities Threats
A.C.T.I.O.N.
A.C.T.I.O.N.
Disclaimer: The expert opinion expressed on this slide is personal and may not be understood or quoted as being made on behalf of or reflecting the position of ECDC.
Educational programmes for the public and for professionals: SWOT analysis
12
Strengths Weaknesses
• Several examples of best practice in Member States
• e-Bug programme for junior/senior school children (www.e-bug.eu)
• Eurobarometer (as a measure of knowledge of general public)
• Limited space in various curricula (schools, universities)
• Limited public funds available for continuous education of professionals (in many Member States)
• Increasing interest (general public, media, parents, school teachers, professional societies, media)
• New technical possibilities (phone apps, social networks)
• Limited sustainability of e-Bug (after end of EU project)
• Pressure for direct-to- consumer advertising for prescription-only medicines
Opportunities Threats
A.C.T.I.O.N. A.C.T. I.O.N.
Disclaimer: The expert opinion expressed on this slide is personal and may not be understood or quoted as being made on behalf of or reflecting the position of ECDC.
Financial incentives/disincentives: SWOT analysis
13
Strengths Weaknesses
• Several examples from Member States: - BE: perioperative prophylaxis - DK: delisting of antibiotics - FR: free Strep test for GP - DK: extra income for rapid diagnostic tests
• Most antibiotics are available as (cheap) generics
• In hospitals, the costs of antibiotics do not necessarily impact the hospital budget (depending on the country)
• Potential savings for national insurance systems (if incentives/disincentives are properly placed)
• Professionals and the public may resist change if perceived as done only for saving costs
Opportunities Threats
A.C.T.I.O.N.
Disclaimer: The expert opinion expressed on this slide is personal and may not be understood or quoted as being made on behalf of or reflecting the position of ECDC.
Effects of delisting of fluoroquinolones (mainly ciprofloxacin), Denmark
EL CY* FR IT LU BE SK PL PT MT° IE LT* ES** IS BG CZ FI UK HU DK AT NO DE SI SE NL EE LV
DD
D p
er
10
00
in
ha
bita
nts
an
d p
er
da
y
Penicillins (J01C) Cephalosporins and other beta-lactams (J01D)
Tetracyclines (J01A) Macrolides, lincosamides and streptogramins (J01F)
Quinolones (J01M) Sulfonamides and trimethoprim (J01E)
Other J01 classes
Source: European Surveillance of Antimicrobial Consumption (ESAC), 2011.
Outpatient antibiotic (J01) use, by antibiotic class according to ATC classification, 2009
* Total use, i.e. including inpatients, for Cyprus and Lithuania.
** Reimbursement data, i.e. not including over-the-counter sales without a prescription, for Spain
Malta: 2008 data
Targets / benchmarking of antibiotic consumption: SWOT analysis
16
Strengths Weaknesses
• Clear message about the objective (size of decrease, by a certain date)
• A few Member States are taking the lead
• Choice of target may be difficult (e.g., size of achievable decrease? measurement unit?)
• Potential large savings for national insurance systems
• Uncertainty about antibiotic consumption threshold below which the number of adverse effects due to non prescription of antibiotics (to patients who really need them) would increase
Opportunities Threats
A.C.T.I.O.N.
Disclaimer: The expert opinion expressed on this slide is personal and may not be understood or quoted as being made on behalf of or reflecting the position of ECDC.
Rapid diagnostic tests: SWOT analysis
17
Strengths Weaknesses
• Several positive experiences from Member States
• Contributes to a more rational use of antibiotics
• Implementation may vary depending on country (who performs the test? who pays for the test?)
• Potential savings for national insurance system
• Business opportunity
• Misuse of test may result in increasing expenses for national insurance system (potential threat)
Opportunities Threats
A.C.T.I.O.N.
Disclaimer: The expert opinion expressed on this slide is personal and may not be understood or quoted as being made on behalf of or reflecting the position of ECDC.
Vaccines: SWOT analysis
18
Strengths Weaknesses
• Several examples from Member States and other countries (pneumococcal conjugate vaccine)
• Reduces burden of the disease covered by vaccine
• Serotype replacement means need for new vaccines
• Cost of vaccination (for national insurance system or for the patient if not reimbursed)
• Not for healthcare-associated infections (so far)
• Business opportunity
• Difficult-to-reach populations in most countries
• Should not distract us from working at improving use of antibiotics
Opportunities Threats
A.C.T.I.O.N.
Disclaimer: The expert opinion expressed on this slide is personal and may not be understood or quoted as being made on behalf of or reflecting the position of ECDC.
For at få punktopstilling på teksten (flere niveauer
tekst uden punktopstilling,
Time for ACTION Reducing overuse
Awareness and education: prudent use (primary care, healthcare settings)
Commitment: professional, individual, political
Targets / benchmarking: primary care, hospitals
Incentives: rapid diagnostic tests, absence from work for sick child, vaccination