JOURNAL OF OPHTHALMIC AND VISION RESEARCH 2014; Vol. 9, No. 4 407 INTRODUCTION A pterygium is a triangular or wing‑shaped fibrovascular overgrowth of abnormal conjunctiva onto the cornea. The Transplantation of Autologous Ex Vivo Expanded Human Conjunctival Epithelial Cells for Treatment of Pterygia: A Prospective Open‑label Single Arm Multicentric Clinical Trial Viraf Sam Vasania 1 , PhD; Aarya Hari 1 , MSc; Radhika Tandon 2 , FRCOphth; Sanjay Shah 3 , MS Suhas Haldipurkar 4 , DOMS; Smitesh Shah 5 , DOMS; Shailendra Sachan 1 , MBBS Chandra Viswanathan 1 , MD, PhD 1 Regenerative Medicine Group, Reliance Life Sciences Pvt. Ltd., Navi Mumbai, Maharashtra, India 2 Dr. Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi, India 3 Department of Ophthalmology, King Edward Memorial Hospital, Pune, Maharashtra, India 4 Laxmi Eye Institute, Panvel, Mumbai, Maharashtra, India 5 Dr. Shah’s Laser Eye Institute, Kalyan West, Thane, Maharashtra, India Original Article Correspondence to: Chandra Viswanathan, MD, PhD. Regenerative Medicine Group, Reliance Life Sciences Pvt. Ltd., R ‑ 282, T. T. C Area of MIDC, Thane Belapur Road, Rabale, Navi Mumbai ‑ 400 701, India. E‑mail: [email protected]Received: 12‑10‑2012 Accepted: 12‑10‑2013 etiology of pterygia remains largely unknown; [1] but it is believed to be caused by exposure to ultraviolet radiation, dust, and dry climates. [2] In severe cases, visual loss Abstract Purpose: To establish the efficacy and safety of ex vivo cultured autologous human conjunctival epithelial cell (hCjEC) transplantation for treatment of pterygia. Methods: Twenty‑five patients with pterygia were recruited at different centers across the country. Autologous hCjEC grafts were prepared from conjunctival biopsy specimens excised from the healthy eye and cultured ex vivo on human amniotic membrane mounted on inserts using a unique mounting device. The hCjEC grafts were then transported in an in‑house designed transport container for transplantation. Post‑surgery, the patients were followed up on days 1, 7, 14, 30, 90, and 180 as per the approved study protocol. Clinical outcomes were assessed by slit lamp examination, visual acuity, imprint cytology, fluorescein/rose bengal staining, Schirmer’s test, and photographic evaluation three and 6 months post‑transplantation. Results: Two patients were lost to follow‑up and final analysis included 23 cases. No recurrence of pterygium was observed in 18 (78.3%) patients; all of these eyes showed a smooth conjunctival surface without epithelial defects. Recurrence was observed in 5 (21.7%) patients at 3 months post‑treatment. No conjunctival inflammation, secondary infections or other complications were reported. Adequate goblet cells were present in 19 (82.6%) patients at the site of transplantation. Conclusion: We have, for the 1 st time, standardized a protocol for preparing autologous hCjEC grafts that can be safely transported to multiple centers across the country for transplantation. The clinical outcome was satisfactory for treating pterygia. Keywords: Autologous; Human Amniotic Membrane; Conjunctival Epithelial Cells; Goblet Cells; Pterygium; Multicenter Study J Ophthalmic Vis Res 2014; 9 (4): 407‑416. Access this article online Quick Response Code: Website: www.jovr.org DOI: 10.4103/2008‑322X.150800
Transcript
Journal of ophthalmic and Vision research 2014;Vol.9,No.4 407
1Regenerative Medicine Group, Reliance Life Sciences Pvt. Ltd., Navi Mumbai, Maharashtra, India2Dr. Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi, India
3Department of Ophthalmology, King Edward Memorial Hospital, Pune, Maharashtra, India4Laxmi Eye Institute, Panvel, Mumbai, Maharashtra, India
5Dr. Shah’s Laser Eye Institute, Kalyan West, Thane, Maharashtra, India
Original Article
Correspondence to: ChandraViswanathan,MD,PhD.RegenerativeMedicineGroup,RelianceLifeSciencesPvt.Ltd.,R‑282, T.T.CAreaofMIDC,ThaneBelapurRoad,Rabale, NaviMumbai‑400701,India. E‑mail:[email protected]
Received:12‑10‑2012 Accepted:12‑10‑2013
etiologyofpterygiaremainslargelyunknown;[1]butitisbelievedtobecausedbyexposuretoultravioletradiation,dust, anddry climates.[2] In severe cases, visual loss
AbstractPurpose:Toestablishtheefficacyandsafetyofex vivoculturedautologoushumanconjunctivalepithelialcell(hCjEC)transplantationfortreatmentofpterygia.Methods:Twenty‑fivepatientswithpterygiawererecruitedatdifferentcentersacrossthecountry.AutologoushCjECgraftswerepreparedfromconjunctivalbiopsyspecimensexcisedfromthehealthyeyeandculturedex vivoonhumanamnioticmembranemountedoninsertsusingauniquemountingdevice.ThehCjECgraftswerethentransportedinanin‑housedesignedtransportcontainerfortransplantation.Post‑surgery,thepatientswerefollowedupondays1,7,14,30,90,and180aspertheapprovedstudyprotocol.Clinicaloutcomeswereassessedbyslitlampexamination,visualacuity,imprintcytology,fluorescein/rosebengalstaining,Schirmer’stest,andphotographicevaluationthreeand6monthspost‑transplantation.Results: Twopatientswere lost to follow‑upandfinal analysis included23 cases.No recurrenceofpterygiumwasobservedin18(78.3%)patients;alloftheseeyesshowedasmoothconjunctivalsurfacewithoutepithelialdefects.Recurrencewasobservedin5(21.7%)patientsat3monthspost‑treatment.Noconjunctivalinflammation,secondaryinfectionsorothercomplicationswerereported.Adequategobletcellswerepresentin19(82.6%)patientsatthesiteoftransplantation.Conclusion:Wehave,forthe1sttime,standardizedaprotocolforpreparingautologoushCjECgraftsthatcanbesafelytransportedtomultiplecentersacrossthecountryfortransplantation.Theclinicaloutcomewassatisfactoryfortreatingpterygia.
Ex vivo Expansion of Autologous Human Conjunctival Epithelial Cells; Vasania et al
408 Journal of ophthalmic and Vision research 2014; Vol. 9, No. 4
mayarisefrominducedirregularcornealastigmatism,cornealstromalscarringandobscurationofthevisualaxis.[3,4]Severalsurgicalmethodshavebeenemployedformanagementofpterygium.Simpleexcisionusingthebarescleratechniquehasbeenshowntobeassociatedwitharecurrencerateofmorethan70%.[5‑8]Thishighrecurrence rate has led to the search for adjunctive treatmentoptionssuchaschemotherapyorradiotherapy.Differentsurgicaltechniquescombinedwithadjuvantssuch asmitomycin‑C,[9] β-irradiation,[10] thiothepa,[11] anti‑VEGF(vascularendothelialgrowthfactor)agents,[12] andmorerecently,alcohol[13]havebeentriedinvariouscombinationsforthetreatmentofpterygia.Theuseofamnioticmembranegrafts(AMG)hasbeen
showntobeefficaciousintreatingprimarypterygia.[14] AMGservesasanalternative toconjunctival tissue ineyeswithlargeconjunctivaldefectsandinadequatetissueto cover thebare sclera, commonly seen in recurrentpterygia.[15]However,intermsofpreventingrecurrence,most studieshave shown this treatmentmodality tobe less effective thanconjunctivalautografting.[16] The conjunctivalautograftingtechniquewas introducedbyKenyonetalin1985andhasbecomeapopulartreatmentforrecurrentandadvancedpterygia.[17]Althoughmoretimeconsuming,conjunctivalautograftingisamuchsaferandeffectiveapproachthanchemotherapyorradiotherapy.This technique, targeted to reduce recurrence, hasresulted invaryingdegreesof success.[18] Recurrence ratesashighas39%afterconjunctivalautograftinghasbeen reported.[19] Limbal‑conjunctival autografts afterpterygiaexcisionhavealsoshownpromisefortreatmentofrecurrentpterygia.[20,21]
There iswide variation in the extent of surgicalexcisionofpterygiaandsubconjunctivalfibrovasculartissuebyvarious investigators.[22,23]Excisionof largerconjunctival grafts from thebulbar conjunctivamayhelp reduce the recurrence rate ofpterygia butmayresult in complications such as scarring,fibrosis andinflammationatthedonorsite.[24]Sincethepreferredsiteforautograftexcisionisthesuperiorbulbarconjunctiva,patientsrequiringsubsequentglaucomasurgerycouldfacefurtherproblems.In1997,Pellegrinietalreportedthefirstsuccessful
use of ex vivoexpansionforautologoustransplantationwithoutinducingiatrogenicinjurynormallyassociatedwith autograft excision.[25] Since then, this techniqueis beingused extensively for treatingvariousoculardisorderswithlong‑termpositiveclinicaloutcome.[26,27] The use of cultivated and ex vivoexpandedconjunctivalepithelialcellsheetsfortreatmentofpterygiahasbeeninpracticeforafewyearsnow.Theadvantagesofusingcultivated conjunctival epithelium include reductionin inflammationandearlyepithelialization leading tofasterrecovery.[28‑29]
Wehavestandardizedamethod for ex vivo culture ofautologousconjunctivalepithelialcellswhichwould
benefitpatientswhoaregeographicallydistantfromthecellculturefacility.Duringthedevelopmentstage,themajorchallengewaspreparationofhumanconjunctivalepithelialcell(hCjEC)graftswhichcouldbetransportedtohospitalsacrossthecountry.Toovercomethisissue,wedevelopedanoveldeviceformountinghumanamnioticmembrane (HAM)whichwould serve as a substratefor culturing the cells.[30] Further,wealsodesignedatransportcontainerwhichwouldensuregraftintegrityduringshipment.[31]Tothebestofourknowledge,thisisthefirstmulticentricclinicalstudytoassessthesafetyandefficacyofautologoushCjECgraftstransportedacrossthecountryandusedfortreatmentofpterygia.
METHODS
ThisstudyadheredtothetenetsoftheDeclarationofHelsinki andwasapprovedby the ethics committeesofthestudysites.Informedconsentwasobtainedfromallparticipants.ThestudywasconductedatfoursitesacrossthecountryfromJanuary2008toDecember2009.Twenty‑fivepatientswereenrolledinthestudyaspertheinclusioncriteria[Table1].
Human Amniotic Membrane ProcessingPlacentaswereobtained,afterdueconsentingprocess,frommothersundergoingCaesareansectionandwereused toprepareHAM.Screening tests for infectiousdiseasewere done for human immunodeficiencyviruses1and2(HIV‑1,HIV‑2),hepatitisBandCviruses
Table 1. Criteria for selection of patients for the study
Journal of ophthalmic and Vision research 2014;Vol.9,No.4 409
Ex vivo Expansion of Autologous Human Conjunctival Epithelial Cells; Vasania et al
(HBV,HCV) by polymerase chain reaction (PCR)and for cytomegalovirus (CMV‑IgM,CMV‑IgG), andSyphilis IgM/IgGby serology.Amnioticmembranewasprocessedaccording to themethodproposedbyKimet al.[32] Briefly, theplacentawas cleanedunderaseptic conditions and the amnionwas separatedfrom the chorionbybluntdissection.Themembranewas cut into pieces admeasuring 4 cm× 4 cm andplacedonseparatepiecesofnitrocellulosepaper.Eachmembranewasplacedinthesterilespecimencryogenicvial(ThermoFisherScientific‑Nunc,DK‑4000Roskilde,Denmark) containingDulbecco’smodified Eagle’smedium (DMEM) (Invitrogen‑Gibco,Carlsbad,CA,USA) and glycerol (SigmaAldrich, St. Louis,MO,USA)[1:1]andcryopreservedat−80°C.Sterilitychecksandendotoxintestswereperformedbeforereleasingthemembranesforclinicaluse.
Mounting on Human Amniotic MembraneOnthedayofbiopsyprocessing,twomembraneswerethawed andwashed thricewith sterileDulbecco’sphosphate‑buffered saline (DPBS) (Invitrogen‑Gibco,Carlsbad,CA,USA)for5mineachtime.Thebasementmembrane side of HAMwas then treated withtrypsin‑EDTA(Invitrogen‑Gibco,Carlsbad,CA,USA)for15minat37°C.Theamnioticepitheliumwasgentlyremovedusinga cell scrapperandwashed thrice for5mininDPBS(1X)toremovecellulardebris.TheHAMwasoriented correctly, asdescribedby
Zakaria et al,with its basementmembrane facingupwards.[33]Thenitrocellulosemembraneonthemillicellinsert(MilliporeCorporation,Billerica,MA,USA)wasgentlypeeledoff.Theinsertwasthenplacedontopofthemembrane and the edgesof themembranewerepulledovertherimoftheinsert.Thisisnowreferredtoas“HAMconstruct”.TheHAMconstructwasthenflippedoverandplacedon thebaseof themountingdevice[Figure1a].AsiliconeringwasslippedontotheHAMconstructusingtheplungerofthemountingdeviceinordertoprovideawrinkle‑freesubstrate[Figure1b].TheHAMconstructwasthenflippedbackandplacedinthe6‑wellplate(ThermoFisherScientific‑Nunc,DK‑4000Roskilde,Denmark)containingsupplementalhormonalepithelialmedium(SHEM).
Preparation of Human Conjunctival Epithelial Cell GraftsConjunctival biopsies, approximately 2mm× 4mmin size,withunderlying stromawereobtainedunderstrictasepticconditionsfromthesuperiorfornixofthecontralateralhealthyeyeofpatients.Biopsiescollectedattherespectivesitesbytrainedinvestigatorsweresentto the currentGoodManufacturingPractices (cGMP)facilityforprocessing.Theyweretransportedat2°C–8°CinSHEM[Table2].Thebiopsywascutintopiecesand
seededontwoHAMconstructsinSHEM.Thecultureswereincubatedat37ºCinanatmosphereof5%CO2 and 95%air.Growthofcellsfromtheexplantswasmonitoredwithaninvertedphase‑contrastmicroscope(OlympusCorporation,Tokyo,Japan)foraperiodof14–21days.Theculturemediumwasreplenishedonalternatedays.
Uniqueness of the Transport ContainerThe transport containerwas designed to hold thegraft assembly in place and protect the graft from
Table 2. Composition of supplemental hormonal epithe‑lial medium
Figure 1. (a and b) Indigenously designed andpatentedmountingdevice formountinghumanamnioticmembraneonto amillicell insert, (c) In‑housedesigned andpatentedstainless steel transport container for transportationof thegrafttohospitalsite.
c
ba
Ex vivo Expansion of Autologous Human Conjunctival Epithelial Cells; Vasania et al
410 Journal of ophthalmic and Vision research 2014; Vol. 9, No. 4
damageduring transport. The transport container iscylindricalinshape,madeofSS316Landhasascrewcaplid[Figure1c].Aspeciallydesignedsiliconegasketholdsthegraftfirmlyinplaceandpreventsleakageofmediumduringtransport.
Packaging of the GraftUponattainingconfluence(approximately14–21days),thegraftswereindividuallypackagedinthein‑housedesignedtransportcontainers.Thegraftassemblywasplacedgentlyinsidethecontainerandthemediumwasaddedslowlyalongthesides.Thesiliconegasketwasplacedontopandthecontainerwasclosedwiththelid.Thepreparedgraftsweretransportedtothehospitalsitefortransplantationwithin24hofpackaging.Onlyonegraftwasneeded for the transplantation.The secondgraftwas sent as a standby in theunlikely event ofdamagetothefirstgraft.
In‑Process TestingDuringgraftpreparation,spentmediumwascheckedforsterilitybydirectinoculationmethodasprescribedin the current IndianPharmacopoeia and endotoxintest using the Limulus Amebocyte Lysate (LAL)gel‑clotmethod (WakoChemicals, Richmond,VA,USA)atdifferent stagesduring theprocess [Table3].Mycoplasmatestingofthespentmediumwascarriedoutasperthemanufacturer’sinstructions(MinervaBiolabsGmbH,Berlin,Germany).
Characterization of the Human Conjunctival Epithelial Cell GraftAfter successful transplantation, the second graftwassentbacktothefacility.Theexpandedcellswerecheckedforviabilityandexpressionofkeymarkersbysemi‑quantitativeRT‑PCR.
Gene Expression Profiling by Semi‑ Quantitative Reverse Transcription‑ polymerase Chain ReactionRNA extraction was performed using RNeasyMini Kit (QIAGEN,Hilden, Germany) as per themanufacturer’sinstructions.OnemicrogramofRNAwasconvertedintocomplementaryDNA(cDNA)utilizingthefirststrandsynthesiskit(Invitrogen,Carlsbad,CA,USA) as per themanufacturer’s protocol. PCRwasperformedasreportedpreviously.[34]TheprimerdetailsareasgiveninTable4.
Cellular CharacterizationDuring the standardizationprocess for preparationof hCjEC grafts, immunofluorescence stainingwasperformed to confirm the identity of conjunctival
epithelial cells. Formalin‑fixed paraffin‑embeddedsectionsofhCjECgraftweredeparaffinizedwithxyleneandgradedalcoholtreatment.Thesectionsweredippedin 10mM sodium citrate buffer, pH 6.0 for antigenretrieval.Thesectionswereheatedinamicrowaveovenfor30 s andpermeabilizedwith0.2%TritonX‑100 inphosphate‑bufferedsaline(PBS).Thenon‑specificbindingsiteswereblockedwith3%bovineserumalbumin(BSA)inPBSfor60minutesat4°C.Sectionswereincubatedwithmouseanti‑cytokeratinepithelialcloneAE1(Millipore,Billerica,MA,USA),mouseanti‑cytokeratin epithelialcloneAE3(Millipore,Billerica,MA,USA),goatanti‑mucinMUC4(SantaCruzBiotechnology,SantaCruz,CA,USA),andmouseanti‑mucinMUC5AC (Millipore,Billerica,MA,USA)overnightat4°CfollowedbyincubationwiththeirrespectiveFITC‑conjugatedsecondaryantibodiesfor30minutesat4°C.Excessantibodieswerewashedoffandsamplesweremountedinimmunofluorescencemountingmedium(Sigma‑Aldrich,St.Louis,MO,USA)andobservedunderafluorescencemicroscope(NikonE600)forthepresenceofimmunoreactivecells.
Surgical ProcedureThe surgicalprocedurewas carriedout asdescribedpreviously.[18]Underlocalanesthesiawith2%lignocaine,theheadofthepterygiumwascompletelyremovedbybluntdissection.ThehCjECgraftwaswashed4timeswithDPBS (1X) containingD‑glucose and sodiumpyruvate (Invitrogen‑Gibco,Carlsbad,CA,USA)andplacedoverthediseasedconjunctivalsurfacewiththeepithelialcellsfacingupwards.Thegraftwastrimmedtofittheentireconjunctivaldefect,includingthebulbarsurface of the fornix and the deeper portion of thepalpebralaspectofthefornix, ifrequired.Itwasthensecured to the recessed conjunctival edgewitha fewinterrupted or running 8.0 vicryl sutures so that itsmarginremainedplacedundertheconjunctivalmargins.Sutureswere tied carefully ensuring that the trailing
Journal of ophthalmic and Vision research 2014;Vol.9,No.4 411
Ex vivo Expansion of Autologous Human Conjunctival Epithelial Cells; Vasania et al
suturedidnotdragalongthesurfaceofthemembrane.Ifclinicallyrequired(basedoninvestigator’sdiscretion),the conjunctival graftwas then tucked to the deepfornixbyamusclehookanchoredtothepalpebralsideofthefornixbypassingtwoorthreedouble‑armed6.0vicrylsuturesthroughthefullthicknessofthelidandsecuredtotheskinwithsiliconebolsters.Therestoftheconjunctivalgraftwasthensecuredandflattenedtothebulbar aspectby interrupted10.0nylon sutureswithsuperficialscleralbites.Atopicalbroad‑spectrumantibioticwasusedandthe
Statistical AnalysisDataprocessing, tabulation of descriptive statistics,andcalculationof inferentialstatisticswasperformedprimarilyusingSASsoftware(release9.0orhigher)forWindows.Statisticalanalysiswasperformedusing95%confidenceintervalalongwithcountsandproportions.
RESULTS
ThedemographicandclinicaldetailsaresummarizedinTable 5.A total of 25patients from fourdifferentcenterswere recruited. These patients underwentpterygium excision followed by transplantation ofautologoushumanconjunctivalepithelialcellgraft.Thepatientsincluded12(48.0%)maleand13(52.0%)femalesubjectswithmeanageof43.9(range,25–67)years.Allpatientswerefollowedfor6months.Two(8.0%)patientswerelosttofollow‑up.
Table 4. Primers used for semi‑quantitative RT‑PCR
Ex vivo Expansion of Autologous Human Conjunctival Epithelial Cells; Vasania et al
412 Journal of ophthalmic and Vision research 2014; Vol. 9, No. 4
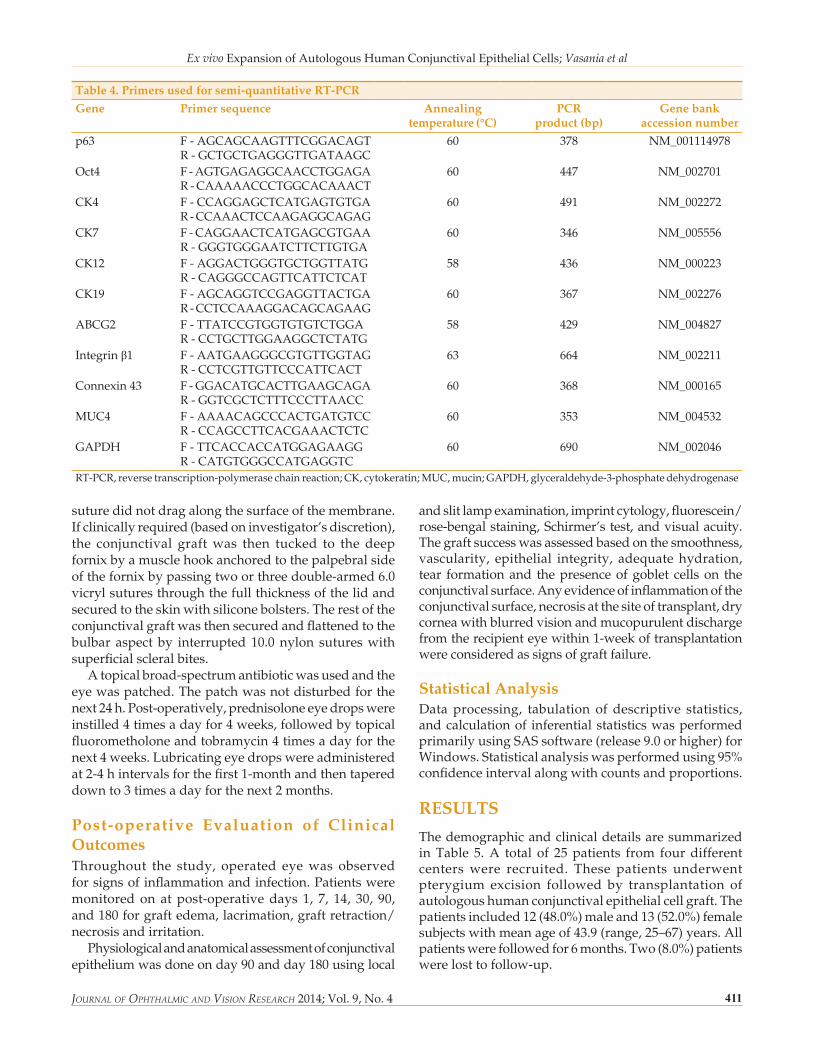
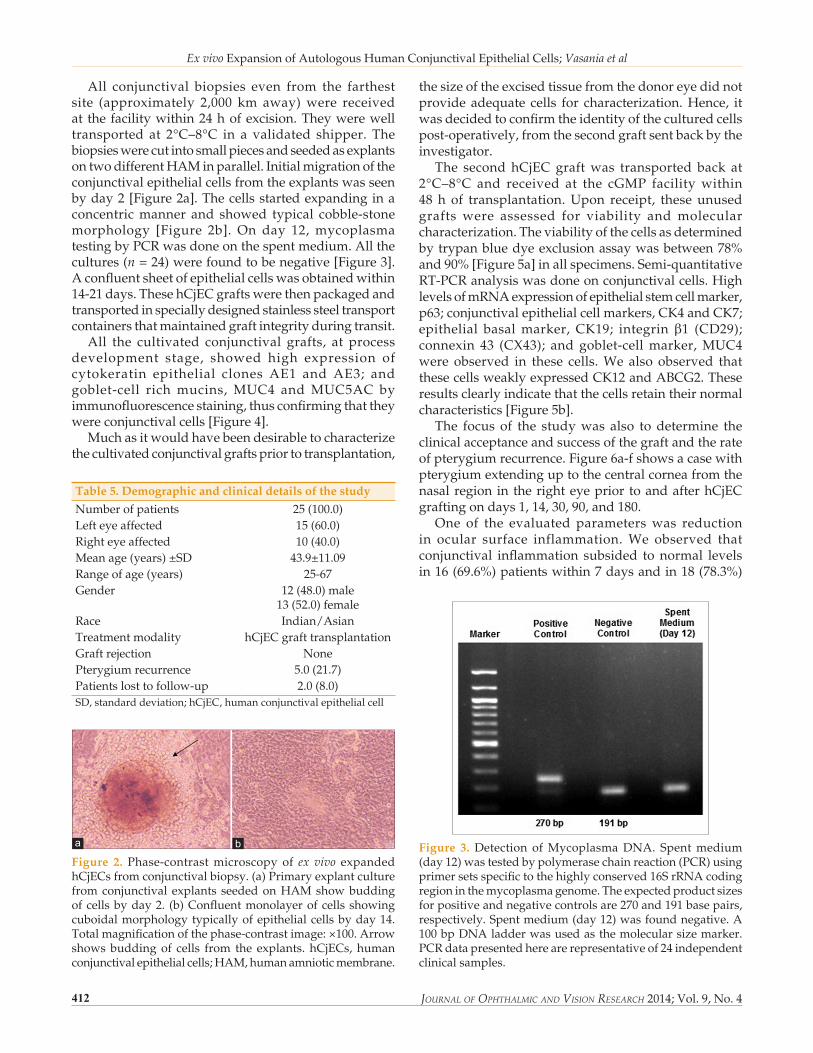
All conjunctival biopsies even from the farthestsite (approximately 2,000 km away)were receivedat the facilitywithin24hofexcision.Theywerewelltransported at 2°C–8°C in a validated shipper. ThebiopsieswerecutintosmallpiecesandseededasexplantsontwodifferentHAMinparallel.Initialmigrationoftheconjunctivalepithelialcellsfromtheexplantswasseenbyday2[Figure2a].Thecellsstartedexpandinginaconcentricmanner and showed typical cobble‑stonemorphology [Figure 2b]. On day 12,mycoplasmatestingbyPCRwasdoneonthespentmedium.Allthecultures (n=24)werefoundtobenegative[Figure3].Aconfluentsheetofepithelialcellswasobtainedwithin14‑21days.ThesehCjECgraftswerethenpackagedandtransportedinspeciallydesignedstainlesssteeltransportcontainersthatmaintainedgraftintegrityduringtransit.All the cultivated conjunctival grafts, at process
development stage, showed high expression ofcytokeratin epithelial clones AE1 and AE3; andgoblet‑cell richmucins,MUC4 andMUC5AC byimmunofluorescencestaining,thusconfirmingthattheywereconjunctivalcells[Figure4].Muchasitwouldhavebeendesirabletocharacterize
thesizeoftheexcisedtissuefromthedonoreyedidnotprovide adequate cells for characterization.Hence, itwasdecidedtoconfirmtheidentityoftheculturedcellspost‑operatively,fromthesecondgraftsentbackbytheinvestigator.The secondhCjECgraftwas transported back at
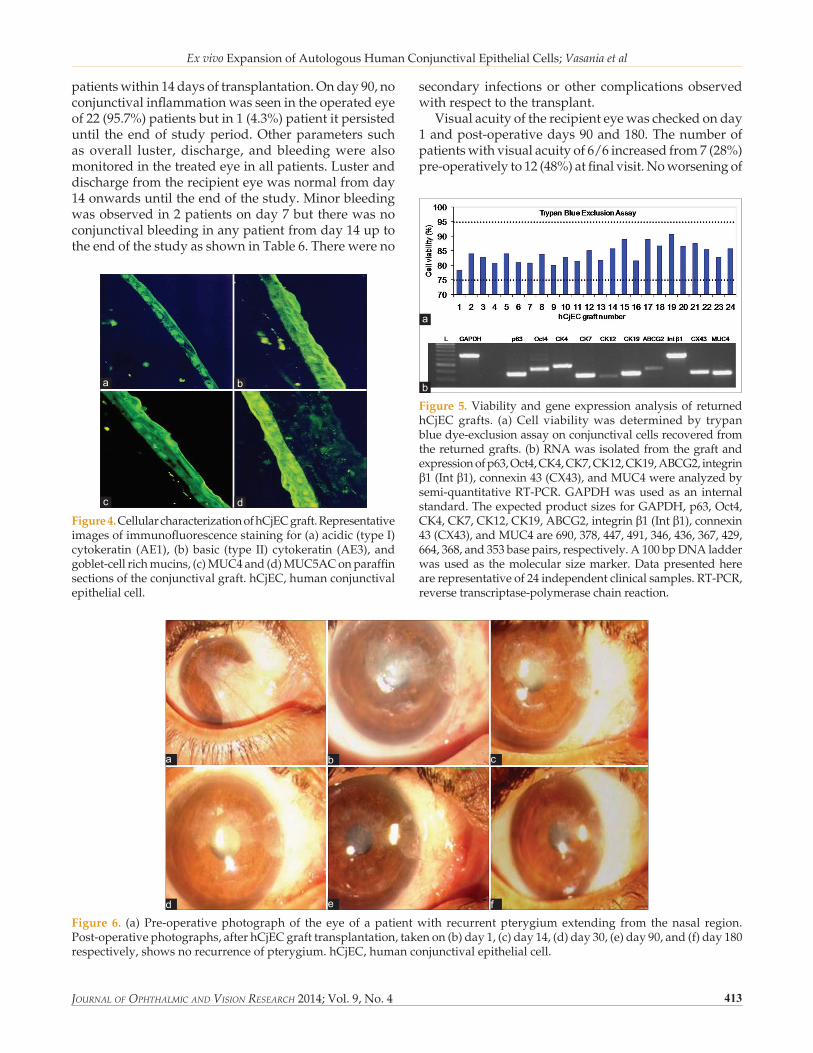
2°C–8°C and received at the cGMP facilitywithin48h of transplantation.Upon receipt, theseunusedgrafts were assessed for viability andmolecularcharacterization.Theviabilityofthecellsasdeterminedbytrypanbluedyeexclusionassaywasbetween78%and90%[Figure5a]inallspecimens.Semi‑quantitativeRT‑PCRanalysiswasdoneonconjunctivalcells.HighlevelsofmRNAexpressionofepithelialstemcellmarker,p63;conjunctivalepithelialcellmarkers,CK4andCK7;epithelial basalmarker, CK19; integrinβ1 (CD29);connexin 43 (CX43); and goblet‑cellmarker,MUC4were observed in these cells.We also observed thatthesecellsweaklyexpressedCK12andABCG2.Theseresultsclearlyindicatethatthecellsretaintheirnormalcharacteristics[Figure5b].The focus of the studywas also todetermine the
clinicalacceptanceandsuccessofthegraftandtherateofpterygiumrecurrence.Figure6a‑fshowsacasewithpterygiumextendinguptothecentralcorneafromthenasal region in therighteyeprior toandafterhCjECgraftingondays1,14,30,90,and180.One of the evaluated parameterswas reduction
in ocular surface inflammation.We observed thatconjunctival inflammation subsided tonormal levelsin16(69.6%)patientswithin7daysandin18(78.3%)
Table 5. Demographic and clinical details of the study
Figure 2. Phase‑contrastmicroscopy of ex vivo expandedhCjECsfromconjunctivalbiopsy.(a)Primaryexplantculturefromconjunctival explants seededonHAMshowbuddingofcellsbyday2. (b)Confluentmonolayerofcells showingcuboidalmorphologytypicallyofepithelialcellsbyday14.Totalmagnificationofthephase‑contrastimage:×100.Arrowshowsbuddingof cells from the explants. hCjECs,humanconjunctivalepithelialcells;HAM,humanamnioticmembrane.
ba
Journal of ophthalmic and Vision research 2014;Vol.9,No.4 413
Ex vivo Expansion of Autologous Human Conjunctival Epithelial Cells; Vasania et al
Figure 6. (a)Pre‑operativephotographof the eyeof apatientwith recurrentpterygiumextending from thenasal region.Post‑operativephotographs,afterhCjECgrafttransplantation,takenon(b)day1,(c)day14,(d)day30,(e)day90,and(f)day180respectively,showsnorecurrenceofpterygium.hCjEC,humanconjunctivalepithelialcell.
d
cb
f
a
e
Ex vivo Expansion of Autologous Human Conjunctival Epithelial Cells; Vasania et al
414 Journal of ophthalmic and Vision research 2014; Vol. 9, No. 4
transplantationwereseenin17(73.9%)patientsonday30andin19(82.6%)patientsbyday180.Nogobletcellwasseenin3(13%)patientsattheendofthestudy.Inaddition,Schirmer’stestconfirmedadequatehydrationwithpresenceoftearsinall23(100%)patientsatdays90and180.No recurrence of pterygiumwas observed in
18 (78.3%) patients until day 180 and conjunctivalsurfaceappearedclinicallynormalinthesepatientsfrom3monthspost‑operatively.Intheremaining5(21.7%)patients, pterygium recurrencewasobservedwithin6months.
DISCUSSION
Pterygia are complex fibrovascular conjunctivalovergrowthsonthecorneaandsurgicalexcisionisthemostprevalenttreatmentoption.Recurrenceiscommonand therefore, newer approaches to treat pterygiaarebeing contemplatedand triedby researchersandophthalmic surgeons.[15]More recently, autologousconjunctival epithelial cellgraftinghasbeen reportedforreconstructingconjunctivaldefects.[29] The results of ourclinicaltrialtoassessthesafetyandefficacyofsuchautologousgrafts to stabilize the conjunctival surfacehavebeenpromising.ThisclinicalstudywasconductedwithformalapprovalfromtheDrugControllerGeneralofIndia,thehighestapprovingauthority,intheIndiancontext.Allproceduresforgraftpreparationincludingcell characterization and transport conditionswereestablishedpriortocommencementofthestudy.Conjunctivalepithelialcell transplantationrequires
a carrier tissue, as it is notpossible to transfer thesecells alone.Anatural basementmembrane,HAM isalreadyinclinicaluseandisbelievedtominimizeocularinflammation,reducepainandaidinepithelialization.[35] HAMhasbeenusedascarriertissueforconjunctivalstemcells.[29]Inourstudy,weusedHAMasthesubstratumforculturingconjunctivalepithelialcells.ThehCjECgraftswerepreparedfromtheipsilateral
conjunctivaltissue.Regardlessofage,thebiopsysampleswere all 2mm×4mm in size andall of themwereculturedonHAMaspertheproceduredescribedinthemethods section.Thequalityof thepreparedgraft isdirectlyrelatedtotheconjunctivalbiopsytissueexcisedfromthedonoreye.Despitethisinherentvariation,ourresultsshowedconsistencyinthequalityofthegraftspreparedusingthisstandardizedmethod.Transporting the grafts todistant sites across the
countrywas a challenge.Wedidvalidation runs toestablish the logistics and transport conditions. Thein‑house designed transport containermaintainedproper orientation and integrity of the graft during
transit.Our validation study showed that the graftcan be transported at 2°C–8°Cwithout affecting itsviabilityand integrity [Table7].No instanceofgraftdamagewasnotedduringtransport.Also,cellviabilityofallreturnedgraftswasfoundtobegreaterthan80%whenassessed48haftersurgery.Atthehospitalsite,the doctors and the paramedical staffwere trainedtohandlethegrafttoensurethatthereisnodamageduringtransplantation.Mostofourpatientshadprimarypterygiawhilefive
caseshad recurrent lesions.Theprimaryobjectiveofthestudywastoassessfeasibilityofthegraftthroughmanifestations such as inflammation, graftmelting,mucopurulentdischarge,necrosis,andrednessontherecipienteye.Theentirestudywasuneventfulwithnocaseshavingpost‑operativeinfectionsorredness.Minoradverseeventslikeeyepainandlocalirritationsubsidedwithmedications.
Table 6. Parameters monitored in the recipient eye post‑transplantation
Table 7. Stability study of the hCjEC* grafts (n=10)
Parameter analyzed
Storage time at 2°C‑8°C
6 h 12 h 24 h 48 h
Attachmentofcells Good Good Good GoodMorphologyofcells Cuboidal Cuboidal Cuboidal CuboidalCellviability% 95±2 90±2 88±3 82±3pHofthetransportmedium
7.2 7.3 7.5 8.3
*hCjEC,humanconjunctivalepithelialcell
Journal of ophthalmic and Vision research 2014;Vol.9,No.4 415
Ex vivo Expansion of Autologous Human Conjunctival Epithelial Cells; Vasania et al
Surgicalexcisionremainstheconventionaltreatmentfor pterygium and recurrence is themost commonundesirableoutcome.Thetwoimportantconcernsinpterygiumsurgeryaretoreducepterygiumrecurrenceandminimize complications arising from surgery.Thereisnostandarddefinitionofrecurrencebutwhenafibrovascular outgrowth is observed at the site ofpreviouslyexcisedpterygium,itisgenerallyacceptedasrecurrence.[15]Ithasbeenreportedthatatleast97%of all recurrencesmanifestwithin the 1st year after excision.[36]Muchas itwouldhavebeendesirabletoextend follow‑up to 1‑year, our approved protocolwaslimitedto6months.However,wedidfollowthepatientsforupto1‑yearthroughtelephoneinteractionswith the investigator, purely out of interest. In ourstudy, 18 (78.3%) patients had no recurrence ofthe pterygia at 6months. Informal communicationconfirmed that therewas no recurrence in thesepatientsevenafter1‑year.Ocular surface inflammation plays a significant
roleinincreasingtheriskofpterygiumrecurrence.Hence, control of inflammation before and aftersurgeryisessentialforreducingrecurrencerate.Inour study, conjunctival inflammation subsided in18(78.3%)patientswithin14dayspost‑operativelyand no conjunctival inflammationwas present in22 (95.7%) patients by day 90. This observationcontinued until the end of the study. No otherseriouscomplicationswerereportedduringthestudyindicatingthathCjECgraftwaswelltoleratedatthesiteoftransplantation.Integrity of the conjunctiva is a very important
endpoint. The conjunctival surface became smoothgraduallybytheendof3monthsandcontinueduptotheendofthestudy.Further,attheendof1‑year,wehadinformalcommunicationthattherewasnochangeinthesmoothnessatthetransplantsite.Presence of adequate goblet cells is a critical
parameterthatreflectstheoverallhealthoftheocularsurface.[37]Atleast19(82.6%)patientsshowedsufficientgoblet cells at day 180. This is another importantindicator of normal conjunctival regenerationpost‑transplant.In other studies, transplantationof an autologous
with longer follow‑upwill beneededbeforeone canconsider thismethodas thepreferred alternative fortreatmentofpterygia.
ACKNOWLEDGEMENTS
Theauthorswould like to thankRelianceLifeSciencesPvt.Ltd. (www.rellife.com) forproviding the opportunity andfinancial support to carryout the clinical study.TheyalsothankAllIndiaInstituteofMedicalSciences,NewDelhi;KingEdwardMemorialHospital,Pune;LaxmiEyeInstitute,Panvel;andDr.Shah’sLaserEyeInstitute,Kalyanforconductingthisstudy.
18. TiSE,CheeSP,DearKB,TanDT.Analysisofvariationinsuccessrates in conjunctival autografting for primary and recurrentpterygium. Br J Ophthalmol2000;84:385‑389.
Ex vivo Expansion of Autologous Human Conjunctival Epithelial Cells; Vasania et al
416 Journal of ophthalmic and Vision research 2014; Vol. 9, No. 4
23. TanDT, Chee SP, Dear KB, LimAS. Effect of pterygiummorphology on pterygium recurrence in a controlled trialcomparingconjunctivalautograftingwithbarescleraexcision.Arch Ophthalmol1997;115:1235‑1240.
27. Sangwan VS, Matalia HP, Vemuganti GK, Fatima A,IfthekarG, Singh S, et al. Clinical outcome of autologouscultivated limbal epithelium transplantation. Indian J Ophthalmol2006;54:29‑34.
28. Tan DT, Ang LP, Beuerman RW. Reconstruction of theocular surface by transplantation of a serum‑free derivedcultivated conjunctival epithelial equivalent.Transplantation 2004;77:1729‑1734.
33. ZakariaN,KoppenC,VanTendelooV,BernemanZ,HopkinsonA,TassignonMJ. Standardized limbal epithelial stem cell graftgeneration and transplantation.Tissue Eng Part C Methods 2010;16:921‑927.
34. VasaniaVS,PrasadP,GillRK,MehtaA,ViswanathanC,SarangS, et al.Molecularandcellularcharacterizationofexpandedandcryopreservedhumanlimbalepithelialstemcellsrevealuniqueimmunologicalproperties. Exp Eye Res2011;92:47‑56.
How to cite this article: Vasania VS, Hari A, Tandon R, Shah S, Haldipurkar S, Shah S, et al. Transplantation of autologous ex vivo expanded human conjunctival epithelial cells for treatment of pterygia: A prospective open-label single arm multicentric clinical trial. J Ophthalmic Vis Res 2014;9:407-16.
Source of Support: Nil. Conflict of Interest: None declared.