TRANSPLANTATION OF NORMAL AND DECELLULARIZED SYNGENEIC, ALLOGENEIC AND XENOGENEIC CARDIAC TISSUE IN MICE AND NON-HUMAN PRIMATES Ketaki Nishikant Methe Laboratory of Transplantation and Regenerative Medicine Department of Transplantation Surgery Institute of Clinical Sciences Sahlgrenska Academy, University of Gothenburg 2020
Transcript
TRANSPLANTATION OF NORMAL AND DECELLULARIZED SYNGENEIC,
ALLOGENEIC AND XENOGENEIC CARDIAC TISSUE IN MICE
AND NON-HUMAN PRIMATES
Ketaki Nishikant Methe
Laboratory of Transplantation and Regenerative Medicine
Department of Transplantation Surgery
Institute of Clinical Sciences
Sahlgrenska Academy, University of Gothenburg
2020
Front cover - The transplantation scheme used to test the immunogenicity of DC scaffolds in syngeneic, allogeneic and xenogeneic setting, in this thesis.
Thesis title - Transplantation of normal and decellularized syngeneic, allogeneic and xenogeneic cardiac tissue in mice and non-human primates.
Figures, tables and reprints are published with permission from the copyright owners where applicable
ISBN 978-91-7833-854-2(PRINT)ISBN 978-91-7833-855-9(PDF)
Printed in Gothenburg, Sweden 2020 Printed by Brand Factory
To my parents who always inspired me for completing this book
To my husband who strengthened me during the entire course
In the memory of my grandfather and father-in-law, who would have been happy to see this book
_________________________________________
Equality is an integral part of humanity
3 INTRODUCTION
6
7
ABSTRACT
INTRODUCTION
Because of the restricted inherent capacity of regeneration and healing, trans-plantation is the only treatment for end-stage heart failure but it has limitations of donor shortage and graft rejection. Cardiac tissue engineering strategies might help to alleviate this problem. Organ specific, biocompatible and biodegradable extracellular matrices (ECM) could be the preferred option for a suitable scaffold-ing material. However, clinical trial with these matrices is still not routine prac-tice. Experimental and clinical data suggest variable outcomes after implanting decellularized (DC) scaffolds. Hence, the immunological properties of ECM and future perspectives need to be addressed. In this report we chose to study cardiac ECM to better understand its immune potential.
METHODS
A decellularizing protocol using whole porcine heart with Triton X-100 and SDC was developed. The resultant acellular cardiac matrix was analyzed for its structural, functional and mechanical strength. The same protocol was adapted to DC mouse, pig and baboon cardiac hearts. The DC ECM was further tested for its immunological potential by implantation into mouse and baboon recipients, fol-lowed by histological and immune histological examinations. Further evaluation of the immunological properties was carried out by proteomics-bioinformatics studies using Mass Spectrometry analysis at the University Core facility. Finally, DC ECM from mouse and pig were implanted into mouse recipients to better understand responses to ECM in syngeneic, allogeneic and xenogeneic settings.
ABSTRACT
8
ABSTRACT
RESULTS
Serial perfusion of Triton X-100 and SDC was effective in removing all cellu-lar and nuclear materials from whole porcine hearts. It thoroughly decellularized ECM scaffolds from cardiac tissue with cytoskeletal elements of cardio-myocytes remaining largely intact. We observed differences in the immune response for the same ECM scaffolds in mouse and baboon recipients, respectively. In mouse, the responses were more donor specific, and allogeneic scaffolds had a higher immune potential than syngeneic scaffolds. Furthermore, proteomic-bioinfor-matic analyses revealed the presence of protein S-100, α-laminin and annexin A1 in the mouse DC ECM. In pig scaffolds, we identified, coagulation factor V (fV), fibrilline, spondin 1, and hyaluronan, whereas insulin growth factor (IGF) and periostin were observed in DC ECM of baboon scaffolds. These proteins are known to be immunomodulatory and their immune potential in regard to DC ECM scaffolds should be further tested. We found a distinct immune response for syngeneic, allogeneic and xenogeneic scaffolds after implantation. The allo-geneic and xenogeneic immune responses were both T-cell driven, however, the development of these responses were different for DC ECM of allogeneic and xenogeneic scaffolds, respectively.
CONCLUSION
DC ECM has favorable properties as a scaffolding material. The evaluation protocol of DC processes described in this thesis requires further development of the immunological potential. The host immune responses cannot be general-ized as they are donor species specific. The ECM proteins themselves seem to be immunogenic which might explain differences in the distinct immune responses shown by the recipients.
Hjärtvävnad har begränsad förmåga att läka och därmed reparera skador or-sakade av till exempel hjärtinfarkter eller andra sjukdomar som skadar hjärtmus-keln. Hjärttransplantation är i dessa fall ofta den enda utvägen. Begränsningarna med hjärttransplantation är risk för avstötning, samt brist på donatorer. Ett sätt att lösa dessa problem är regenerativ medicin – ”Tissue Engineering” (TE). Genom att använda organspecifika, biokompatibla och bionedbrytbara stöd-jevävnader – s.k. Extra Cellular Matrix (ECM) försöker man reparera/återskapa den skadade vävnaden. Ännu finns inga eller mycket få kliniska studier utförda där TE används. Däremot har teknik, som innebär att genom att använda hjärt-vävnad, som sedan genomgår en process för att avlägsna celler samt genetiskt material – s.k. decellularisering (DC) – visat lovande resultat. Efter att immunol-ogiskt aktiv vävnad avlägsnats återskapas vävnaden/organet genom tillförande av nya hjärtceller eller stamceller – s.k. recellularisering (RC). Studier av ECM efter DC saknas dock. Denna avhandling visar huruvida ECM efter DC uppvisar immunogena egenskaper, som kan försvåra senare RC och transplantation.
METODER
Decellularisering påbörjas genom att fysikaliskt först frysa och därefter tina upp vävnaden. Detta förfarande förstör cellmembranen. De trasiga celldelarna inklusive DNA/RNA avlägsnas sedan med tvättmedel som t.ex. Triton X-100
12
SVENSK SAMMANFATTNING
och 2% sodium dodecyl sulfate (SDS). Metoden utvecklades först för hjärtvävnad på gris, och adapterades därefter till mus och babian. De ECM som erhålls med behandlingen analyseras grundligt avseende cellinnehåll (histologi, immunohis-tokemi), styrka (tensitometri) samt funktion (protein innehåll). ECM studerades därefter ytterligare avseende immunologiska egenskaper genom att implantera vävnad på mus och babian, följt av histologiska och immunohistokemiska analy-ser. För att studera skillnader ur ett syngent, allogent och xenogent perspektiv, utfördes Masspektrometri på vävnad innan och efter implantation av ECM från mus och gris till mottagare, som var mus.
RESULTAT
Upprepad perfusion med Triton X-100 och SDC avlägsnade effektivt celler, samt DNA och RNA från hjärtvävnad med kvarvarande närmast intakt cellskelett av cardiomyocyter. Den ECM som erhölls resulterade i olika immunsvar efter implantation i mus respektive babian. På mus var svaret beroende på donatortyp, med en högre immunogen potential hos allogen ECM än med syngen. Vidare påvisade proteomik-bioinformatik analys närvarao av protein S100, α-laminin och annexin A1 i mus ECM, medan gris ECM innehöll koagulations faktor V (fV), fibrillin, spondin1, och hyluronan. I DC babianvävnad påvisades insulin growth factor (IGF) och periostin. Dessa proteiner har immunmodulerande ef-fekter och deras betydelser och effekter i DC vävnad kräver ytterligare studier. Ett distinkt immunsvar kunde ses vid implantation av såväl syngen, allogen som xenogen. Svaret var T-cells drivet, men den vidare utvecklingen av svaret skilde sig mellan allogen och xenogen ECM.
KONKLUSION
DC ECM vävnad uppvisar väl bevarad struktur men de protokoll som an-vänds måste finjusteras ur ett immunologiskt perspektiv. Immunsvaret kan inte generaliseras utan verkar vara species specifikt. Data tyder också på att ECM pro-teiner i sig verkar kunna ha immunogen effekt, vilket skulle kunna utgöra ett problem för användning av DC vävnad i samband med transplantation om inte RC processen är tillräckligt effektiv.
I. Methe K., Bäckdahl H., Johansson B.R., Nayakawde N., Dellgren G., Sumitran-Holgersson S.; An Alternative Approach to Decellularize Whole Porcine Heart, BioResearch Open Access. 2014 December; 3(327-336).
II. Methe K., Wagner K.R., Nayakawde N.B., Banerjee D., Patil P., Antony D., Travnikova G., Premaratne G.U., Olausson M.; Immune response to normal and decellularized scaffolds in mouse, pig and non-human primates (submitted)
III. Methe K., Nayakawde N., Ghosh S., Sihlbom C., Wagner K.R., Patil P., Premaratne G.U., Olausson M.; Comparative proteomics of decellularized cardiac scaffolds from mouse, pig and non-human primates (submitted)
IV. Methe K., Nayakawde N., Banerjee D., Travnikova G., Olausson M.; Cross-talk Between Different Immune Regulatory Pathways Determines the Fate of Decellularized Grafts After Implantation (submitted)
ABBREVIATIONSAA Acetic acidAnxA1 Annexin A1AP2 Activating protein 2C3 Complement 3C4 Complement 4C9 Complement 9CD Cluster of differentiationCF4 Complement factor 4CHAPS 3-[(3-Cholamidopropyl)dimethylammonio]-1-propanesulfonateDAMP Damage associated molecular patternDAPI 4′,6-diamidino-2-phenylindoleDC Decellularized / Decellularization DNA Deoxyribonucleic acidECM Extracellular matrixFNs FibronectinsFV Factor VH&E Hematoxylin and eosinH2SO4 Sulfuric acidHAPLN3 Hyaluronan and proteoglycan link protein 3HCl Hydrochloric acidHP Haptoglobin precursorHS Heparan sulphateHSPs Heat shock proteinsIg ImmunoglobulinIGFALs Insulin-like growth factor binding protein, acid labile subunitIglc2 Immunoglobulin lambda constant 2IL1β Interleukin 1 betaMHC Major histocompatibility complex NH4OH Ammonium hydroxideNHP Non-human primatesPAA Peracetic acidPML Promyelocytic leukemia proteinPPE Polyphenyle ether PPG Polypropylene glycolRab-1A Ras related protein Rab-1ARap1 Ras-proximate-1 or Ras-related protein 1S100 A8 S100 calcium binding protein A8S100 A9 S100 calcium binding protein A9SB10 Sulfobetaine 10SB16 Sulfobetaine 16SDC Sodium deoxycholateSDS Sodium dodecyl sulphateSEM Scanning electron microscopySTAT2 Signal transducer and activator of transcription 2TEM Transmission electron microscopyTE Tissue engineeringTGF Transforming growth factorVCP Valosin containing protein
3 INTRODUCTION
20
21
DEFINITIONS
DEFINITIONSTissue engineering (TE) – TE is the field of science where knowledge of cells, engineering principles, and material sciences can be supplemented with knowl-edge of suitable biochemical and physicochemical factors to improve or replace biological tissues.
Extracellular matrix (ECM) – ECM is a 3 dimensional non-cellular portion of tissue made up of extracellular macromolecules such as collagen, elastin, enzymes, and glycoproteins that provide structural, functional and mechanical support to surrounding cells.
Scaffold – Structure providing support to cells or tissues.
Decellularization (DC) – DC is the process by which cellular and nuclear materi-als can be removed by physical, chemical or enzymatic methods from the tissue to leave a complex mixture of extracellular matrix proteins.
Recellularization (RC) – RC is the repopulation of acellular ECM scaffolds of tissue or organs with organ specific cell types or stem cells.
Syngeneic – Relating to or involving tissues or cells from genetically similar or identical individuals and hence in an immunologically compatible setting.
Allogeneic - Relating to or involving tissues or cells from genetically dissimilar and hence in an immunologically incompetent setting, although coming from individuals from the same species.
Xenogeneic - Relating to or involving tissues or cells from different species. Homograft – Tissue graft from a donor of the same species as the recipient.
Foreign body reaction – A modified wound healing response due to the presence of a foreign implant and usually characterized by encapsulation of tissue, fibro-sis or presence of multinucleate giant cells.
22
DEFINITIONS
Host response – The reaction of the host living system to the presence of foreign material.
Immunogenicity – The ability of any substance to provoke inflammation.
Transplantation – The process of taking an organ or living tissue and implanting it to another part of the body in the same individual or into the body of another individual.
Implantation – The process of inserting tissues or artificial objects into the body of an individual especially by surgery
Biocompatibility – Ability of tissue or an organ to be in contact with a living system without producing an adverse effect.
Biodegradability – The ability of material to be broken down over time as a result of biological activity.
Integration – The formation of a direct interface between an implant and sur-rounding tissue without altering surrounding soft tissue.
Absorption of tissue – Tissue which has been implanted is taken up/absorbed by the host surrounding tissue.
23
DEFINITIONS
3 INTRODUCTION
24
25
AIMS OF THESIS
AIMS OF THESIS
• To develop a protocol for preparing DC ECM scaffold from cardiac tissue
• To analyze and compare host immune responses in mouse and baboon recipients directed against donor DC cardiac ECM scaffolds from mouse, pig and baboon hearts
• To analyze the immunological properties of protein mixtures comprising DC cardiac scaffolds from mouse, pig and baboon hearts
• To characterize the immune response triggered after implantation of donor mouse and pig DC ECM scaffolds in mouse recipients
3 INTRODUCTION
26
27
INTRODUCTION
End-stage organ failure is a significant health and economic burden on society which usually results in the death of an individual unless a suitable donor organ can be transplanted as replacement therapy. The field of tissue engineering (TE) has developed over time to provide an alternative source of transplant organs. TE is a fascinating technique whose foundation relies on three basic components; scaffolds, cells and signals. The concept of TE for re-growing organs in the labo-ratory was first put forward in 1993 by Langer and Vacanti1. Work in this field still revolves around the three basic components raising crucial questions. How can we regrow organs, how can we stimulate patient specific tissue, and which clues can we utilize to enable regrowth of tissue in vivo in the host? Until now, the success of TE grafts has mainly been limited to graft patches in support-ing the needs of patients2-4. Replacement of thick vascular grafts still requires considerable refinement before this goal is likely to be achieved. Scaffolding materials that constitute graft patches can be synthetically or biologically de-rived. Synthetic scaffolds offer advantages in terms of structural and mechanical properties which can be modified according to the cell’s requirements. This approach helps to regulate cell behavior by changing the scaffold topography. However, biologically derived scaffolding material also possesses inherent advantages such as organ specific arrangement of macromolecules, dynamic reciprocity, antibacterial activity, biocompatibility and biodegradability5. These properties favor biological rather than synthetic as the preferred source for scaffolding material. Extracellular matrix (ECM) is popularly used as a natural
INTRODUCTION
28
INTRODUCTION
scaffold in tissue engineering for human welfare6-12. In the current work, we have evaluated the host immune response to syngeneic, allogeneic, and xenogeneic donor ECM isolated from cardiac tissue.
1. SIGNIFICANCE OF ECM IN CARDIAC TISSUE
Cardiac ECM is the dynamic entity which regulates the responses of cardi-ac tissues toward their surroundings. The myocardium is composed of cardio-myocytes, fibroblasts, leukocytes, and cardiac vascular cells. In the myocardium, fibroblasts are the dominant cell population. Fibroblasts are responsible for de-positing the bulk of ECM proteins such as collagen, fibronectin, vitronectin, col-lagenases, in cardiac tissues. Cardio-myocytes make up only 20-30% of all cells in cardiac tissue. In congenital or age-related cardiac disease, the cardio-myocytes remain in a fairly normal state but cardiac ECM is affected. Therapies for car-diac failure are always directed towards monitoring conditions of cardiac ECM, such as fibrosis and remodeling. For instance, degradation and accumulation of collagen matrix is different in infarct and non-infarct heart. Also, in cases of dilated cardiomyopathy, dysfunctional collagen matrix is observed in affected areas whereas normal collagen matrix is present in the rest of the heart13. The expression of non-structural ECM proteins such as glycoproteins, proteoglycans and glycosaminoglycan play an important role in the plasticity of cardiac tissue in different pathologies of heart14. Evidence suggests that the role of ECM in cardiac tissue is a decisive factor in adult heart and is influential in its embry-ological stages. Representatives of all ECM macromolecules can be found in developing cardiac tissues15.
2. DC CARDIAC ECM AS BIOSCAFFOLDS
The concept of DC was first introduced by William Poel in 1948 and was scaled up for in vivo application by Badylack in 199516. However, this concept was actively applied to cardiac tissues only in the last decade. Ott et al, in 2008, reported DC in cardiac tissue of the rat which was later extended to various animal species. These early studies provided hope that DC cardiac ECM could be used as a template for various tissue engineering purposes17,18.
The use of cardiac DC ECM is associated with several unique advantages. The geometry and vasculature tree of cardiac tissue is unique when compared to other organs and is necessary for the electric potential of cardio-myocytes. Thus, the use of DC ECM from native cardiac tissue can facilitate the proliferation
29
INTRODUCTION
and activation of cardio-myocytes. Being biodegradable, it is also suitable as a cardiac patch in infarcted hearts. It can provide effective mechanical compensa-tion to the myocardium. The retained growth factors and contractile proteins during DC are believed to be supportive for myocardial regeneration. However, the regeneration of functional whole heart is still not feasible. The underlying reasons may be due to variations in preparing DC ECM. In addition, repopula-tion by cardio-myocytes may be inadequate and non-homogenous with effective diffusion limited by the thickness of walls comprising the cardiac compart-ments. One possible approach to circumnavigate these problems is to modify the cardiac DC ECM scaffolds by combining them with bioactive molecules such as polyphenyle ether (PPE), polypropylene glycol (PPG), collagen hydrogels, and transforming growth factor beta (TGF-β) to produce composite cardiac scaf-folds. This technique is relatively new and requires further research to more clearly establish this procedure. The DC ECM patches have been mostly studied in rat tissue but very few studies describe the use of DC ECM in large animal models20,21. In this study we have tested and compared DC ECM of cardiac tissues
FIGURE 1 Timeline of major milestones using DC ECM scaffolds for myocardial repair. hiPSC, human induced pluripotent stem cells; dECM, decellularized extracellular matrix, from Pawan et al19
30
INTRODUCTION
from mouse, pig and baboon in mouse and baboon.
3. PREPARATION OF DC ECM SCAFFOLDS
DC is the process by which all cellular and nuclear materials are removed by either chemical, physical or enzymatic methods to leave a complex mixture of ECM proteins on which cells can propagate, proliferate and differentiate to form a functional tissue. Various methods are available to achieve this and they are broadly classified into two groups; physical methods and chemical methods. In the case of physical methods, various methods such as freeze-thawing, mechanical stripping of the cells, high hydrostatic pressure, supercritical carbon dioxide, sonication and agitation are routinely practiced. The various chemical methods include different surfactants as well as acids and bases that can be used to lyse and solubilize the cellular and nuclear materials from the tissue22-24. These treatments effectively disrupt the cell membrane and remove intracellular organelles. Surfactants used for these purposes are commonly classified based on their charges such as ionic, non-ionic and zwitterionic surfactants. Ionic deter-gents/surfactants are believed to disrupt protein-protein interactions and are ef-fective in solubilizing the cellular and nuclear remnants from the tissue. Non-ionic detergents act on protein-lipid and lipid-lipid interactions and are believed to be less harsh on the tissue architecture. Zwitterionic detergents have a greater tendency to denature proteins since they contain properties of both ionic and non-ionic detergents. Sodium dodecyl sulfate (SDS) and sodium deoxycholate (SDC) (ionic surfactants), triton X-100 (non-ionic surfactant), and CHAPS and SB10 and SB16 (zwitterionic surfactants) are commonly used detergents in TE applications. In the case of alkalis and bases, acetic acid (AA), per acetic acid (PAA), hydrochlo-ric acid (HCl), sulfuric acid (H2SO4), and ammonium hydroxide (NH4OH) can be used in the DC process. Among these, PAA is the most extensively studied alkali for DC purposes. However, the use of alkali and bases have proven detri-mental for DC of tissues leaving them as a poor choice of DC agent. As an alter-native, enzymatic DC is more specific in its action. DNase, collagenase and tryp-sin are the common examples used in DC. However, use of DNase is not without limitations and it has been shown to induce inflammatory responses after implantation. Trypsin and collagenases are also detrimental to ECM components24. It has become apparent that organ-perfusion DC models which remove the majority of the cellular material are mandatory for successful development of tissue-engineered whole hearts25.
31
INTRODUCTION
4. CHARACTERIZATION OF DC ECM SCAFFOLDS
The residual cellular or nuclear material in DC ECM scaffolds from the donor can impart the biocompatibility events and elicit a host immunological response. The efficacy of successful DC was determined by checking the residual amount of double stranded deoxyribonucleic acid (DNA) (which should be <50ng/mg of dry weight of tissue), the length of the DNA material (which should be <200 base pairs of DNA), and by confirming the absence of nuclear material by viewing histological sections. However, these criteria are insufficient as confirmation of removal of nuclear material to establish the success of DC. More rigorous param-eters need to be applied to ensure complete removal of residual cellular contents from DC tissues. Additional analytical parameters include toxicity testing with elution assays26, enzyme-based assays for measurement of residual phospho-lipids27, and measurement of endotoxins23. Different techniques giving a more detailed insight about the ECM tissue components should also be added to the evaluation protocol. Typically used techniques range from antibody-based tech-niques such as immunohistochemistry, through enzyme-linked immunosorbent assays to western blot or electrophoresis which characterize the protein content of scaffolds. However, for more detailed investigation, spectrometric methods such as HPLC, LC-MS, ToF-SIMS, or MALDI/ToF should be considered. Un-fortunately, these techniques are still difficult to interpret because of the immense overlap between different peptides in the MS output. Luminex technology offers a more detailed and specific analyzes of the protein mixture comprising the DC ECM.
5. HOST RESPONSE TO ECM SCAFFOLDS
As a general rule, implantation of acellular scaffold is not harmful to pa-tients. However, the use of ECM scaffolds is not routine practice in the clinic. The underlying reason may be the high failure rate of these scaffolds resulting in immune rejection. Hence, analyzes of the precise immune potential of ECM scaffolds has become an inherent part of the evaluation protocol. Immunogenic properties of the scaffolds can be analyzed by in vitro and in vivo testing. In vitro techniques such as viability studies, maturation studies, activation studies, protein-based assays, relative gene-expression based assays, and functional assays enables us to fulfill 3R’s which reduces both experimentation time and costs28. However, outcomes from in-vitro and in-vivo methods for certain scaffolds
32
INTRODUCTION
poorly correlate making in-vivo testing a much more reliable method for predicting the immunological potential of the scaffolds29. For in-vivo analyzes, the host response is always characterized by observing the foreign body reaction developed against scaffold and/or by analyzing the immunological parameters developed in the serum30-32. However, serum responses might be the result of any systemic disturbances and hence, site specific analyzes of the scaffolds is a more reliable and suitable method of investigation. Nevertheless, ethical and practi-cal aspects regarding the necessary sacrifice of experimental animals must be considered. We have employed different in-vivo settings to analyze the immune potential of DC ECM scaffolds. The tissues were stained for different immune markers and serum samples were also analyzed with a microarray for inflamma-tion. We observed that site specific histochemical analyzes as well as proteomic analyzes of the implanted tissues provides a more specific and accurate interpre-tation than that from serum parameters.
Implantation of scaffolds in a host is followed by the healing process gener-ally believed to consist of four steps; homeostasis, inflammation, proliferation and remodeling33. During the homeostatic phase, coagulation prevents further bleeding and helps in establishing firm contact between host and donor tissue. During the inflammatory phase, the secretion of MMPs lead to matrix degrada-tion. This is followed by deposition of new matrix by living cells. The reduction of MMP secretion and infiltration of fibroblasts is usually evident during the proliferation and remodeling phases.
Despite the range of DC techniques and chemical cross linking to mask an-tigenic epitopes, DNA and DAMP molecules have limited the time to which scaffolds are able to support organ function34-36. Host responses to biological scaffold material varies widely according to techniques used for preparation of these scaffolds 37. The responses generally involve both the innate and acquired immune system. The available literature suggests that upon placing the implant in vivo, first it is infiltrated exclusively by polymorphonuclear cells followed by mononuclear cells which phagocytose cellular debris and foreign material from the graft.
In the present study, we have characterized the immune response by stain-ing the retrieved cardiac ECM from different implantation settings. Antibodies targeted against macrophages, dendritic cells, neutrophils, B and T lymphocytes, mast cells and eosinophils are described.
33
INTRODUCTION
6. IMMUNOGENICITY OF ECM SCAFFOLDS
ECM molecules are normally concealed by cellular components of tissues and hence they are not recognized by the immune system directly. However, the DC process used in our study, to generate the ECM as a bioscafffold, directly exposes the ECM components to the host immune system. The ECM components released under stress can trigger sterile inflammation by acting as damage associated molecular patterns (DAMPs). Heparan sulphates (HS)38 or hyluronan present 39 in ECM are osmotically active components and their swelling can regu-late cell migration and cancer metastasis. Low molecular weight hyluronan has been shown to be pro-inflammatory and proangiogenic in nature40. Collagen/elastin membranes can induce an interleukin-1-beta (IL1β)-induced pro-inflam-matory response. These membranes have a predominance of 25F9 cell macro-phages which are responsible for chronic inflammation41. Elastin peptides also have been reported to induce a TH1 response 42. Decorin has been described in various inflammatory processes 43,44. Collagen V and VI have been shown to be pro-inflammatory 45,46. In addition, minor ECM components such as mindin, biglycan, entactin/nidogen, vitronectin, acetyl PGP, and tinacine have been shown to have a role in immune reactionst. These ECM molecules have also been shown to play an immunogenic role when exposed at the peptide level. Hence, it is important to appreciate how ECM molecules might react when they are present within their 3 dimensional natural architecture. This understand-ing should be an important asset when generating new tissues in context with regulation of various cell signaling cascades towards facilitating the growth of tissue and accommodation of the graft in the host.
5 METHODS
34
35
MATERIAL AND METHODS
The methods used in the thesis are described briefly in this section. The detailed description of the respective protocols is present in the Material and Methods section of Papers I-IV.
1. ETHICAL CONSIDERATIONS
The mouse hearts (Papers II-IV) and porcine hearts (Papers I-IV) used for this work were procured from laboratory animals at The Experimental Biomedicine Center, Gothenburg University. Baboon hearts were sourced from The Mannheimer Foundation, Florida and the corresponding import permits were obtained from The Jordbruksverket Ethics Committee (Dnr 4.10.18-11077/17, Nr 51136/17, Göteborg, Sweden) for approved delivery of the organs to Gothenburg University.
The implantation experiments for the rodent model were performed according to relevant guidelines and regulations approved by Gothenburg University’s Experimental Biomedicine Center. Ethical approval for this study was obtained from The Jordbruksverket Ethics Committee (Dnr 151/14, 2475/19, Göteborg, Sweden).
The implantation experiments for the baboon model (Papio hamadryas) were performed at The Mannheimer Foundation, Florida, according to the relevant
MATERIAL AND METHODS
36
MATERIAL AND METHODS
guidelines and regulations of the Welfare Act of U.S. Department of Agriculture (USDA) and AAALAC. Ethical approval (Protocol no. 2015-10) was granted by the Institutional Animal Care and Use Committee (IACUC).
2. SCAFFOLD PREPARATION
In the current work, ECM scaffolds were prepared by a DC perfusion-agi-tation method to remove cellular and nuclear material from cardiac tissue. We used 1% Triton X-100 and 1-4% SDC for this purpose. Perfusion of detergent through the tissue’s native vasculature helps the detergent penetrate throughout the whole tissue. The choice of a perfusion method was more suitable for DC pig and baboon hearts because of their more robust structure which supports cannulation whereas an agitation method was more appropriate for mouse hearts where there is insufficient support for cannulation in the later stages of DC. The combined perfusion-agitation method helped to expedite the entire process of DC. Using this method, we were able to completely dispense with enzymatic treatment. The detailed technique is described in Paper I for DC of porcine hearts. This technique was adopted to prepare DC scaffolds from mouse, pig and baboon hearts (Papers II-IV).
FIGURE 2 Figure 2A represents the protocol for DC, whereas Figure 2B represents the perfu-sion setup used during the DC process
37
MATERIAL AND METHODS
3. CHARACTERIZATION OF DC MATRIX
3.1 An assessment of the DC status of ECM scaffolds
The sections of DC scaffolds were checked with DAPI (Paper I), H&E (Papers II & III) to identify any remnants of nuclear material microscopically. The DC scaffolds were digested with DNeasy® Blood and Tissue kit, 250, (Qiagen, Sol-lentuna, Sweden) to extract and quantify the possible DNA remnant (Papers I & II). The extracted DNA was electrophoresed through 1.5% agarose gel to reveal the length of possible remnants of DNA fragments in DC scaffolds (Paper II). The tissues analyzed in Paper II were also used as a sample source for the studies published in Papers III and IV. The electron microscopic examination of resul-tant DC matrix is carried out in order to understand the quality of the resultant scaffold in terms of its acellularity (Paper I).
3.2 An assessment of ECM scaffold macromolecules
Tissues were stained for antibodies against different ECM molecules such as collagen, elastin, fibronectin, laminin and hyaluronic acid. The histological comparison of the ECM proteins in DC scaffolds with normal cardiac tissues helped to predict if there was any alteration in the natural arrangement of these molecules during the fabrication process. The examination of DC cardiac scaffolds through scanning electron microscopy (SEM) and transmission electron microscopy (TEM) helped to reveal the ultra-structure of the DC scaffolds which is a major limitation in the application of optical microscopy. Quantitative analyzes of normal and DC cardiac tissues were also carried out for collagen, elastin, and GAGs to understand the effect of surfactants on the quantities of these molecules (Paper I). Assessment of alteration of growth fac-tors during the DC process was performed using Luminex assay (Paper I).
3.3 Biomechanical assessment of ECM scaffolds
ECM of cardiac tissue helps to maintain the structural integrity of the heart and enables transmission of the sarcomere generated force to the ventricles for creating the necessary pressure to physiologically pump blood throughout the body. The mechanical strength of the heart is necessary to support this func-tion. The stiffness and elasticity of the ECM scaffold also plays an important role when it comes to cell migration and cell differentiation. Normal and DC cardiac
38
MATERIAL AND METHODS
scaffolds were tensile tested to evaluate the alteration in strength of cardiac ECM during DC (Paper I).
3.4 Proteomic assessment of ECM scaffolds
With this technique, we aimed to identify all potential immunological triggers which could appear during preparation of scaffolds but normally escape detection because their immunological function is simply unknown. Proteins present in DC and/or implanted scaffolds from mouse, pig and baboon cardiac tissue were identified using proteomics. The protein mixture was fractionated through reversed-phase chromatography. The fractions were first passed through liquid chromatography-mass spectrometry and then through mass spectrometry a second time to record spectra. Proteins containing more than 2 unique peptides were chosen for further analyzes using bioinformatics. The identified interac-tions of proteins through bioinformatics helped to speculate the immunologi-cal potency of DC scaffolds, (Papers III & IV). However, one should not forget that bioinformatics is a predictive tool and confirmatory tests should also be employed before accepting or rejecting any hypotheses based on this analyzes.
4. TRANSPLANTATION STUDIES WITH DC MATRIX
Analyzes of the host response against normal and DC cardiac tissue is partially described in Papers II and IV. Previous studies describing the host response directed against DC ECM yielded contradictory findings despite the use of similar materials. Hence, the validity and the reliability of the choice of scaffold and its implementation could come into question. In the current work, we sought to omit batch to batch differences arising from the DC scaffold f abrication process. We prepared all DC scaffolds from mouse, pig and baboon
FIGURE 3 This figure represents the Instron 5566 system used for testing the mechanical properties of DC cardiac pig scaffolds
39
MATERIAL AND METHODS
cardiac tissue similarly and implanted them in a consistent manner in mouse and baboon recipients.
This transplanting setting and selected donor-recipient combinations enabled us to focus on the variation in immune response specifically direct-ed against different donor ECM material when transplanted across different immunological barriers into the recipient. The analyzes of immune responses for donor pig scaffolds in mouse and baboon recipients showed that the predictions for DC xeno-ECM scaffolds cannot be generalized. Our experimental approach also enabled us to investigate the nature of the host mouse recipient immune response against donor DC mouse, pig and baboon cardiac scaffolds for syngeneic, allogeneic and xenogeneic ECM scaffold settings. By also choosing baboon as a recipient, we were able to determine if larger animal species immunologically behaved in the same way as their smaller counterparts in terms of identifying and accommodating different donor ECM scaffolds across differ-ent immune barriers. Critical analyzes of infiltrating immune cells in syngeneic, allogeneic and xenogeneic matrices in the mouse recipient helped us to characterize the immune response in more detail. It is often the case that such studies are limited to a few specific parameters such as foreign body reaction or macrophage and lymphocyte response against a particular scaffold. However, in consideration of both ethical and practical issues relating to experiments with mouse and baboon recipients, we decided to change the implantation site of cardiac ECM scaffolds. The functionality of the implanted graft was also compromised since implants were located heterotopically. In this setting, ECM grafts are ‘free floating’ and not anastomosed.
FIGURE 4 The transplantation scheme used to test the immunogenicity of DC scaffolds in syngeneic, allogeneic and xenogeneic setting
40
MATERIAL AND METHODS
4.1 Animals and surgical procedures
Preparations described in Paper II were based on 145 Balb/C mice, around 8 weeks’ old. The animals served as recipients in the mouse models and were housed in The Experimental Biomedicine Center, Gothenburg University, from Day 3 until Month 3, after implantation of DC scaffolds. Among these mice, 63 mice were also treated as an experimental source as described in Paper IV. Paper II also describes the study in which 4 adult baboons were selected as recipients for non-human primates (NHP) models and which were housed in The Mannheimer Foundation, Florida from Week 1 up to Month 3, after surgery. The rodent surgical procedure follows implantation of normal and DC cardiac tissues from mouse, pig and baboon into the greater omentum of the recipient mouse (Papers II & IV). Whereas, the NHP surgical procedure involves the subcuta-neous implantation of normal and DC cardiac tissue from pig and baboons in baboon recipients (Paper II).
FIGURE 5 The schematic diagram presenting transplantation procedure used in different recipients
41
MATERIAL AND METHODS
4.2 Overview of study design
Our study objectives were to compare the differences in immune response arising from implantation of syngeneic, allogeneic and xenogeneic DC ECM scaffolds. The detailed study design is illustrated in Paper II. The study contains two horizons. One horizon analyzes the host response against DC ECM scaffolds based on the recipient and a second horizon analyzes the host response towards DC ECM scaffolds based on the donor. For comparison of immune responses based on the recipient, the study was mainly divided into two groups. Group I included mouse recipients and Group II included baboon recipients. The groups were further divided according to the donor. Group I was further divided into four sub-groups: Group A with syngeneic implants, Group B with allogeneic im-plants, Group C with xenogeneic pig implants and Group D with xenogeneic baboon implants. Paper IV describes advanced analyzes of the implants from Groups A, B and C. Group II recipients received normal and DC cardiac implants from baboon and pig, respectively.
4.3 Histopathological analyzes of the implanted tissues
The harvested implants from Group I and Group II were analyzed using H&E staining for possible microscopic changes. Various comparisons are described in Paper II detailing the similarities and uniqueness of different ECM scaffolds based on their integration and/or absorption rates, pathological changes and activation of the host immune system. Analytical parameters for harvested implants were the presence of leukocytes and granulocytes, giant body cells, necrosis, fibrosis and angiogenesis, as well as capsule formation, tissue adhesion with surrounding tissue, and the rate of resorption of the tissue. The explanted tissues were scored anonymously by two external pathologists and two researchers in addition.
Analyzes of inflammatory markers in implanted tissues
In Paper II, Group I was analyzed for activation of major histocompatibility complex molecules. In Paper IV, the harvested implants from Groups A, B and C were further analyzed using immunohistochemistry for 19 different inflammato-ry markers which describe neutrophils, macrophages, dendritic cells, eosinophils, mast cells, T cells, B cells, and immune regulatory cells. The information about antibodies and their respective dilutions can be found in Paper IV.
42
MATERIAL AND METHODS
The number and stages of infiltrating B lymphocytes were determined by characterizing different lineages of B lymphocytes. The CD19 marker was used to identify naïve B lymphocytes whereas, the CD 38 marker was used to identify mature or activated B lymphocytes. The deposition of immunoglobu-lin (Ig) molecules was characterized by staining the tissues with IgG and IgM antibodies. The presence of B regulatory cells was characterized by IL10 anti-body. The infiltration pattern of T lymphocytes was analyzed by staining the tissues for various lineages of T-lymphocytes. The cells were then stained with antibodies against the CD3, CD4, CD8, as well as the CD25, CD69 and CD49 receptor (see paper IV). The CD3 molecule is present on all T lymphocytes and helps to activate cytotoxic or helper T cells whereas CD4 represents the T helper cell population. CD8 is a marker for cytotoxic T lymphocytes. CD25 appears in the late activation phase of T cells, whereas CD69 is an early activation molecule for T cells and CD49 molecules represent T regulatory cells. The professional antigen presenting cells such as macrophages were characterized by staining the tissues for CD68, CD163 and F4/80 whereas dendritic cells were characterized by staining the tissue for DC-sign antibody. The granulocytes were analyzed by characterizing the tissue for neutrophils (Ly6G molecule), mast cells, and eosino-phils (CCR3 molecules).
Positively stained cells were quantified and plotted onto a graph to help appreciate the deviation in the infiltration pattern of these cells over time. Inflam-matory cytokines were analyzed from the serum samples of mice from Groups A, B and C. Proteins of the implants from these three groups were also identified using proteomics. They were then analyzed for possible upregulated pathways after implantation to better understand the fate of the respective scaffold.
5. SCORING OF HISTOLOGICAL DATA
The immuno-stained images from Papers II and IV were quantified for the relative abundance of different stains. The algorithm for scoring was developed by Gothenburg University’s imaging core facility. The pixel classifica-tion was applied to identify different stain combinations using Ilastik. The labeled images were loaded into Fiji. The number of pixels corresponding to the relative abundance of each stain in each image was quantified. The detailed protocol for this is described in Paper IV.
5 METHODS
43
6. STATISTICAL METHODS
In Papers I, II and IV data are expressed as mean ± standard error. In Paper I, statistical significance was determined using paired t-test for the quantitative analyzes of DNA, ECM components and growth factor analyzes. The Mann-Whitney U test was performed to determine differences in biomechanical properties of native and DC scaffolds. To identify outliers, the Grubb test was applied. In Papers II and IV, the Wilcoxon rank sum test was additionally em-ployed to determine the significance of differences.
5 METHODS
44
45
RESULTS
Results from all studies are described elaborately in the respective papers enlisted at the end of this thesis. Here follows an account of the representative observations from Papers I to IV.
Paper I . An alternative approach to DC whole porcine heart
Perfusion-agitation cycles of triton X-100 and SDC effectively achieved DC whole porcine hearts within 8 cycles. Figure 6 depicts the pale colored DC pig heart in comparison with normal pig heart.
Qualitative and quantitiative assessments were able to validate the protocol for preservation of tissue structure after DC. DAPI staining in Figure 7 repre-sents the loss of blue fluorescence in DC sections as compared with normal sec-tions, confirming the acellular state of DC tissues. We were also able to preserve the fiber orientation of ECM macromolecules during the entire DC process as revealed by Masson’s trichrome, elastin, fibronectin, hyaluronic acid and heparan sulphate staining in Figure 7.
Quantitative assessment in Figure 8 also showed there were no significant decreases in ECM components during the DC process, apart from GAGs. The amounts of growth factors were also largely unaffected during the DC process. However, elastic modulus analyzes showed increased stiffness of the left ventricle versus right ventricle after DC.
RESULTS
46
RESULTS
FIGURE 6 Comparison of morphological changes in normal and DC porcine heart
FIGURE 7 Histological characterization of normal and DC cardiac tissue for confirmation of acellularity and preservation of ECM molecules
The SEM and TEM analyzes of the DC tissues in Figure 9 revealed no traces of elements that are formed by cellular membranes or cytoplasmic inclusions or connective tissue cells and microvasculature after DC of the cardiac tissue but the cross-striated apparatus of myocytes was still present in most tissue areas.
47
RESULTS
Paper II. Immune response to normal and DC scaffolds in mouse, pig and non-human primates
Mouse, pig and baboon cardiac tissues were DC using the present protocol and implanted into mouse and baboon recipients. Tissues harvested at regular time intervals from Day 3 to Month 3 revealed no foreign body reaction to any
FIGURE 9 Photos showing ultrastructure of DC scaffolds as revealed by SEM and TEM techniques
FIGURE 8 Graphical representation of characterization of Normal and DC porcine heart for quantitative analysis of ECM macromolecules, growth factors and mechanical strength
48
RESULTS
FIGURE 10 Morphological examination of the normal and DC ECM graft after in-vivo testing in mouse and baboon recipients
FIGURE 11 Histological examination of normal and DC ECM graft after in-vivo testing in mouse recipients
49
RESULTS
scaffold at any time point. Baboon immune responses were more robust than those in mouse recipients.
In Figure 10 the morphology of normal and DC cardiac implants in mouse and baboon recipients can be compared up to the final time point. This figure enables us to identify or analyze differences in the integration and/or absorption pattern as well as the effect of these implants on the surrounding tissue of the recipient.
Histological examination of scaffolds from mouse recipients showed the trigger for immune activation of syngeneic and allogeneic scaffolds. The degree of immune activation was higher in allo-scaffolds. Irrespective of the differ-ence, both syngeneic and allogeneic scaffolds were completely integrated with surrounding tissue without the development of any scar tissue as shown in Fig-ure 10 and 11. However, xenogeneic tissues developed a scar after implantation. Scars developed by porcine DC ECM were eventually integrated into the host but the scars of DC ECM of non-human primates (NHPs) became inflamed.
In baboon recipients, all ECM scaffolds were integrated with the surround-ing tissue without developing any noticeable histopathological changes in the implanted areas, Figure 12.
FIGURE 12 Histological examination of the normal and DC ECM grafts after in-vivo testing in baboon recipients
50
RESULTS
FIGURE 13 Heatmap showing the diversity of protein mixture constituting the ECM scaffold of mouse, pig and baboon DC scaffolds
Paper III. Comparative proteomics of decellularized cardiac scaffolds from mouse, pig and baboon
The underlying reasons behind chaotic responses for ECM scaffolds in mouse were analyzed by identification of proteins present in ECM scaffolds before implantation using proteomics global assays. The analyzes showed that all three ECM scaffolds, from mouse, pig and baboon are individually different, Figure 13. Mouse scaffold contains a less varied protein composition than pig or baboon scaffolds. Pig ECM scaffolds are richer in protein diversity and contain a greater number of unique proteins specific to porcine origin.
Immune enrichment analyzes of all scaffolds showed that pig ECM contains a greater number of immune related proteins than baboon or mouse scaffolds. Almost 24% immune proteins were common to all three scaffolds as shown in Figure 14.
The classification of the protein mixtures from these scaffolds showed all scaffolds are characterized by a unique type of functional enrichment. The unique proteins common to the source ECM scaffolds are enlisted in Table 1.
51
FIGURE 14 DAVID analysis of the immunity proteins identified in mouse, pig and baboon DC ECM scaffolds
TABLE 1 Table enlist the unique proteins identified in respective DC scaffolds
52
RESULTS
Paper IV. Cross-talk between different immune regulatory pathways determines the fate of DC grafts after implantation
Analyzes of the immune reactions developed by the various ECM scaffolds revealed distinct differences in the adaptive immune responses for syngeneic, allogeneic and xenogeneic scaffolds (Figure 15). Syngeneic scaffolds showed elevated responses indicated by increases in F4/80 macrophages and CD38+ cells. Whereas, allogeneic scaffolds showed elevated responses for B cells, dendritic cells, CD25+ cells and CD8+ cells. In the case of xenogeneic scaffolds (porcine ECM), we observed that the immune response was not complex. There was only a trigger for CD4+ cells and mast cells on immune-histochemical analyzes. Rather, we observed strong signals for phagocytosis using bioinformat-ics analyzes of implanted porcine ECMs. Also, we did not observe complicated immune responses with baboon xeno-implants but activation of CD163+ cells was dominant throughout the three-month period (manuscript not listed in this thesis).
FIGURE 15 Classification of infiltrating immune cells in normal and DC cardiac scaffolds
53
RESULTS
FIGURE 15 Classification of infiltrating immune cells in normal and DC cardiac scaffolds
5 METHODS
54
55
DISCUSSION
Significance of developing a proficient DC protocol to obtain ECM scaffold from cardiac tissue
We have successfully DC whole porcine cardiac tissues. The suggested DC protocol in this study is not detrimental and renders the natural architecture of cardiac tissue unharmed making it a biochemically and mechanically stable entity. The chemicals we used in this protocol are not harsh to the ECM scaffolds and result in an acceptable intact scaffold. Triton X-100 is a commonly used DC agent and leaves the tissue’s ultrastructure and mechanical properties unharmed48,49. The use of SDC is also known to retain the structural proteins in ECM, making it functionally active and biocompatible50,51. However, it is be-lieved that the use of SDC creates agglutination of DNA and thereby use of DN-ase becomes necessary for SDC treated scaffolds51. In our protocol, we did not use DNase but were still able to achieve removal of nuclear material to a great extent. The use of DNase is known to induce inflammation upon implantation of DC ECM scaffolds52.
It is pertinent to mention that current criteria which qualify the acellular state of any ECM is inadequate. The removal of nuclear content does not guarantee ECM material to be free of donor elements which can catalyze inflammatory responses in vivo52. Although we were successful in removing nuclear material and cytoplasmic inclusions, we found remnants of cytoskeletal elements in our scaffold after DC. Donor material remnants were also evident in other studies
DISCUSSION
56
DISCUSSION
carried out on lung and uterus53-55. Caution in employing harsh DC treatments to remove these materials should be exercised because such treatments may alter the biocompatibility of ECM scaffolds. A balance should be achieved to select DC treatments that leave a residual threshold level of material which does not compromise immune tolerance and recellularization of the scaffold implant. Relevant in vivo implantation and/or in vitro studies with these scaffolds are necessary to evaluate the immunogenic potential and develop appropriate protocols suitable for clinical application.
Suitable DC scaffolds may provide optimal templates for recellularization and tissue recreation. Their clinical potential includes use as surgical patches and aids for drug and growth factor delivery. The nature of surgical materials for a scaffold can be synthetic or adulterated or natural ECM products56. However, problems of stenosis, calcium deposition, thrombogenesis and risk of infection have limited their wide spread use in the clinic. Most of the time, biodegrad-able materials are the preferred choice for ECM products. Being biodegradable means that surgical intervention to remove the implant after a specified time is spared. DC ECM scaffolds can be prepared from various tissues and organs57 and can be used as mode of drug or growth factor delivery for promoting tissue healing and avoiding hospital born infections58,59. However, there are inherent drawbacks such as compromised strength or inferior biomechanical properties when compared to their metallic or synthetic counterparts. The potential inflam-mation is another integral lacuna associated with biodegradable or bioabsorbable materials during its integration in the host17. Accordingly, careful preparation of DC scaffolds is necessary to achieve their desirable goals by circumventing their pitfalls.
Discrepancies in immunological outcomes of ECM scaffolds upon transplantation
The failure of homograft or xenograft during a patient’s life time has resulted in advancements in the use of DC scaffolds for clinical applications. However, the functionality of DC xenografts has been observed to degenerate over time60. DC homograft provide satisfactory results. Up until now, only one research group has studied DC homograft in patients61-63. They showed that DC pulmonary heart valve grafts could provide the basis for autologous regeneration in 46 patients. However, in 1 patient the graft failed. The ethnic background of the patient was speculated as the underlying reason. The patient was half Asian and received a graft of Caucasian origin. This conclusion may seem surprising because the ECM
57
DISCUSSION
scaffold was not of xeno-origin. The ECM scaffold is believed to be identical across races. However, in the present study, we also observed the severity of the immune response for allogeneic scaffolds relative to syngeneic scaffolds in mouse recipients. This suggests differences between ECM scaffolds in the allogeneic and syngeneic settings despite being of the same species origin. We believe the fate of DC cardiac ECM is determined by both host and donor species. It indicates the importance of strain consideration while interpreting the usefulness of ECM materials in in vivo.
An important observation in baboon recipients was the relative ease that they handled the healing response compared to mouse recipients. This should serve as an alert when scaling up observations made in the mouse to likely outcomes in the clinic. Very few studies have discussed direct comparisons of immune differences across mammalian species. In this context, one should be alerted to the potential limitations in interpreting results from DC SIS ECM scaffolds30.
Our investigations have also shed new light on differences in the process and rate of absorption of ECM scaffolds according to donor origin rather than the belief that differences are a function of variations in manufacturing. Moreover, this study questions the immunological inertness of ECM proteins per se and the theory of conservation of ECM proteins through the evolutionary tree.
Despite the general rationale that ECM scaffolds are evolutionarily conserved and this has been an aspiration for creating ECM scaffolds for reconstruction therapies, ECM scaffolds have been shown to yield discrete results in various clinical settings64. In one sense a universal common healing response followed despite ECM scaffolds of different origin but then different responses have been observed despite ECM scaffolds of the same origin. In one clinical application for treatment of volumetric muscle loss, ECM scaffolds were prepared from urinary bladder or small intestine or dermis for 13 patients. All patients showed an in-crease in post-operative muscle tissue formation at the implant site65. In another application, treatment of esophageal adenocarcinoma using ECM scaffolds pre-pared from small intestine and urinary bladder resulted in a normal mucosa and no recurrence of cancer at the implantation site66. In a study with mixed results, patients treated with allogeneic ECM scaffolds, such as SynerGraft-treated heart valves, developed diverse immune outcomes in in vivo studies67. An intense acute cellular response was associated with the use of GraftJacketTM and RestoreTM
but did not lead to adverse remodeling outcomes. The response was mainly neutrophil dominant following the use of the CuffPatchTM scaffold. These scaffolds also show non-uniform host responses64.
These disparities are often contributed to different manufacturing
58
DISCUSSION
methods and assessment aids23,68,69 instead of placing more emphasis on monitoring biological parameters. Furthermore, these disparities are the basis for our second objective in this thesis work.
Our second aim was to analyze the host immune response in mouse and baboon recipients towards donor DC cardiac ECM from mouse, pig and baboon. We hypothesized that this approach could differentiate between the underly-ing reasons for the disparities arising in the immune response. That is, are the disparities simply the result of the fabrication processes or the consequences of dynamicity of ECM or are they related to the biology of the recipient?
If ECM scaffolds undergo a similar fabrication process but create ambiguous results, then is the ECM per se immunogenic?
We have used global proteomics to characterize the protein mixture of an ECM scaffold from mouse, pig and baboon and predicted the possible potential immunogenic proteins using a bioinformatics tool. We were able to enlist the proteins specific and common to mouse, pig and baboon ECM scaffolds which could be immunogenic. Protein immunogenicity has not been studied before in context with tissue engineering or scaffold structures. We believe that early absorption or integration of mouse scaffolds in Paper II is guided by proteins S100 A6, Anx-A1 and MMP9. Anti-inflammatory proteins were uniquely observed in pig scaffolds. In DC baboon scaffolds, the protein periostin was identified. Periostin could drive scar tissue formation in DC as reported in Paper II. Both DC mouse and baboon scaffolds exhibited the presence of proteins C4a and fibrinogen. These are acute phase reactants which drive the aggressive im-mune reaction upon implantation as we observed for allogeneic and xenogeneic (baboon) scaffolds described in Paper II. All three scaffolds contained protein adapter protein 2 (AP2), heparan sulfate, heat shock proteins, and valosin – con-taining proteins. All these proteins have the potential to directly or indirectly contribute to recruitment and activation of immune cells and development of inflammation. This study may offer other researchers guidance on the possible immunogenic peptides present in ECM. These peptides are known for their immunomodulatory properties but their role in determining the fate of implants in the host has received little attention. There is a need to shift the focus of ECM material research from conventionally known immunogenic proteins such as collagen, fibronectins, mindins or gal and non-gal antibodies towards novel unexplored proteins. This revised approach could bring us closer to achiev-ing the desired results with ECM scaffolds. Further, we may be better placed to
59
DISCUSSION
circumvent the problem of disparities we observe with different ECM materials and reach consensus on what we accept as a suitable implant.
In the clinic, ECM implants are known to elicit anti-gal and anti-non-gal antibodies. Both antibodies have been shown to direct extensive macrophage infiltration and ECM degradation70. Better knowledge of the nature of ECM components may also provide us with a clearer understanding of binding niches which immune cells target to infiltrate and proliferate the implant. In in vitro studies, ECM components have also been shown to induce: activation of platelets; complement cascades; monocyte, lymphocyte and granulocyte recruitment; activation as well as cell binding71. Various ECM fragments have been shown to release peptides in the presence of MMPs in vivo re-sulting in signals for immune cell activation. Hence, the ECM per se is able to act as a reservoir which induces inflammation inside the host. Our un-derstanding of these processes is incomplete while an extensive analyzes of all ECM cryptic peptides is lacking in the literature. The literature is also insufficient whether ECM from different species are identical and do they elicit similar immune responses? These unanswered questions stimulated us to embark on the next study.
If ECM is immunogenic then how does the host react to an implant after transplantation?
In our various host-donor implant settings, we observed an array of varying immune responses despite the fact that all implants were DC cardiac ECM scaffolds. If we explore this phenomenon in terms of differences in donor species (mouse and pig heart), then we also begin to appreciate distinct differences for syngeneic and allogeneic ECM (mouse heart, Balb/C strain and C57BL/6J strain). Despite these differences, the inflammatory processes had resolved in all ECM scaffolds by the end of the observation period with consequent integration and/or absorptionof the implant into the host tissue (relevant histology is presented in Paper II). We postulate that for syngeneic ECM scaffolds, tolerance was achieved mainly by F4/80+ macrophages whereas for allogeneic and xenogeneic (pig) ECM scaffolds tolerance was achieved mainly by T cells. However, cell recruitment and development of the immune response, and differentiation of T cells was different for both allogeneic and xenogeneic (pig) ECM scaffolds. In the case of baboon xenogeneic ECMs we were unable to confirm resolution of inflammation within the period of observation. The absence of an immune trigger to stimulate T and B cells and the continuous presence and over-expression of CD163+ macrophages
60
DISCUSSION
can explain scar tissue formation in baboon ECM implants (histology data presented in Paper II, immunology data not shown). In this context, an important observation in Paper III describes the presence of immunological proteins in both DC mouse and pig ECM scaffolds. These proteins could function in guiding T cells, and macrophage recruitment, proliferation and differentiation in the in vivo setting. In contrast, periostin protein was mainly detected in baboon ECM scaffolds.This protein is widely known to be responsible for overexpression of macrophages, and thereby scar tissue formation. Our in vivo studies showed that porcine tissues do not elicit an adverse immune response68. Although these implants do exhibit a rigorous immune response, the nature of the response can usually be characterized as anti-inflammatory in action. Several studies have proposed the activation of a Th1 and/or Th2 pathway with regard to xenogeneic implants whereby the Th1 pathway is associated with transplant rejection and the Th2 pathway is related to graft acceptance 71-73. It has been suggested that unknown factors as components of ECM material hinder ECM scaffold expression of TNF-α and INF-γ preventing maturation of Th1 responses’74. It is generally accepted that the healing process that follows implant of biomateri-als consists of an early response characterized by infiltration of polymor-phonuclear leukocytes, then neutrophils followed by monocytes, and finally macrophages. These macrophages secrete different cytokines and growth factors which trigger tissue recreation. For healthy tissue, a balance between new matrix deposition in the form of scar tissue and its degradation by proteolysis needs to be achieved. Resolution of inflammation is a key governing factor for achieving this balance. However, until now the mechanisms triggering these responses have not been well understood.
61
DISCUSSION
3 INTRODUCTION
62
63
CONCLUSION
CONCLUSIONS
• The perfusion-agitation model with Triton X-100 and SDC presented in this thesis offers a successful and simple protocol for DC of cardiac tissue. However, even with rigorous DC steps, it is difficult to remove the actin-myosin components entirely from DC cardiac matrices.
• The host immune response directed against donor DC ECM material is species specific; thus one is not able to generalize the host response towards ECM scaffolds.
• Transplantation studies employed in this thesis highlight the possible immunogenicity of ECM proteins per se.
• The host immune response towards DC cardiac tissue is donor species specific.
3 INTRODUCTION
64
65
REFLECTIVE STATEMENTS
REFLECTIVE STATEMENTS AND FUTURE PERSPECTIVES
In Study 1, we acknowledged that DC treatment has both advantages and disadvantages for TE. This method of preparing the scaffold is simple and inexpensive. The ECM scaffolds prepared using this technique are biocompat-ible with and become integrated within the host tissue. However, the rather laborious preparation methods required in the laboratory render this product vulnerable to infection. The DC of thick vascular tissues also cannot guarantee uniform removal of cells and nuclear debris in those areas having less intricate capillary networks. DC products do not meet the standards of native tissue in terms of mechanical strengthening of growing tissue. Batch to batch variation in scaffolds will arise according to the physiological health of the donor which is difficult to control or even reverse. Hence, it is necessary to focus the DC pro-tocol on modification of evaluation criteria along with better DC strategies. The use of composite DC structures could be preferable to native DC patches, especially when it comes to support of the biomechanical properties of the tissue75,76. Coating of DC products with suitable bioactive components is also another attractive option for improving recellularization or dampening the host immune response.
In Study 2, we observed that ECM scaffolds become absorbed and/or inte-grated into the surrounding host tissue. This property makes ECM scaffolds an attractive choice for: TE purposes in areas where they are used for strengthening the surrounding tissues such as skin burns, abdominal wall repair, healing bone defects or anterior cruciate ligaments, and patch working for cardiac tissues.
66
REFLECTIVE STATEMENTS
However, in areas where mechanical sturdiness is necessary such as treatment of the airway tract, these properties could turn out to be harmful. The imbalance between secretion of MMPs and deposition of new matrix usually leads to graft disappearance after transplantation. DC scaffolds should be equipped with materials that resist or dampen the effect of MMPs. Ideally, care should be taken to facilitate matrix deposition or fibroblast infiltration into DC ma-trices after implantation. Once again, the coating of ECM scaffolds with bio-active materials or administration of respective drugs to the host is an option to achieve this goal. The concept of an appropriate pore size in the scaffold-ing materials is necessary to consider in this context. If we can manipulate the pore size of DC scaffold according to the type of cells we wish to infiltrate, then we can bypass overstimulation of phagocytes. However, this approach may be too challenging when applied to naturally derived vascular DC scaf-folds. The use of DC scaffolds in the form of bio printing ink also presents a promising approach. Our animal model studies should be more rigorously planned to differentiate between what makes some scaffolds disintegrate/inte-grate with surrounding tissues and what makes some scaffolds recellularized.
In Study 3, we appreciated that ECM proteins can be immunogenic per se. Literature cites evidences of ECM fragments eliciting specific immune responses. This could be a beneficial factor to the extent that it attracts infiltration of host cells and initiates the remodeling process of implanted scaffolds. However, there is insufficient knowledge of which ECM fragments do actually emit immune signals. We know the ECM proteins by virtue of their tissue support act as a scaffolding material. However, it is time to shift the focus to the immunological properties of ECM molecules that arise as cryptic peptides during wear and tear mechanisms elicited by the host as observed in in vivo. We should also realize that we have still not discovered all the ECM proteins comprising different ECM scaffolds. It is usually debated that apart from ECM structural and functional proteins, inadequate quantities of other proteins are present to trigger an immune response. However, from time to time an immune response has been shown to be triggered. Therefore, more detailed analytical methods such as proteomics and bioinformatics should be employed to better evaluate the immunogenic properties of scaffolds. The role of animal knock-out studies with deletion of specific proteins could be confirmatory.
In Study 4, we understood that scaffolds were disappeared by macro-phages, mast cells and dendritic cells. Also, we learned that after reaching the
67
REFLECTIVE STATEMENTS
peak immune response, dampening of inflammation was led by CD8+ T cells for allogeneic and xenogeneic implants whereas syngeneic implants presented with completely distinct responses. The literature also provides evidence that DC scaffolds evoke macrophage and leukocyte responses. Description of these observations tends to be generalized rather than specific. In contrast, in the present investigations, we were able to characterize these responses. Our results indicate that host macrophages and T lymphocytes are the cells that constitute the immune response. The development of these responses are donor spe-cies specific and the initiation, maturation and resolution of these responses is entirely different from one species to another. This knowledge provides us with a greater insight how to modify and supplement the post-implant course to achieve host acceptance of donor ECM scaffolds.
Strengths and weaknesses associated with this thesis can be summarized. This study provides a simple and inexpensive tool for DC of cardiac tissues. The DC cardiac scaffolds prepared in this work are biocompatible and biodegradable. However, the remnants of actin-myosin components in the DC scaffold may be a weakness associated with this protocol. More studies need to be carried out to understand if these remnants are beneficial for the purpose of recellularization or harmful with regard to immune provocation.
Our comparative immune study with DC scaffolds from donor mouse, pig and baboon cardiac tissues is to our knowledge the first time that a work offers a comparative analysis of DC cardiac scaffolds from different donors, and recipients in one setting. However, ethical considerations associated with ex-periments in baboons limit our study to a smaller sample size and dissimilar transplantation schemes in our baboons and mouse models. The choice of mouse as an implant recipient was major limitation in the study design because the im-mune responses of mice usually differ from the response in humans.
Our methodological strategy and results demonstrate the feasibility of using a proteomics-bioinformatics approach for detailed investigation of ECM proteins. However, overlapping of peptides during the MS-output make interpretation of results difficult and confirmatory techniques are required to supplement this analysis. Predictions of the immunogenicity of ECM components in our bioscaf-folds require further testing to determine pro- or anti-inflammatory structures.
Our last study presents a detailed characterization of immune responses toward the syngeneic, allogeneic and xenogeneic DC scaffolds. Armed with this type of characterization, we are better placed to manipulate the host immune responses towards DC scaffolds following implantation.
3 INTRODUCTION
68
69
ACKNOWLEDGEMENTS
I would like to take this opportunity to thank Prof. Michael Olausson for supervising me through the entire doctorate course. You extended me support during a difficult time when I had to switch supervisors. Without this support, I would have been unable to perform my laboratory studies. Your ideas and scientific suggestions were excellent and not superficial. I learned the skills of digging deep into the topic with you. I was able to enjoy the journey and growth throughout my PhD subject material without feeling stressed. Along with human scientific skills, I acquired the value of patience, and forgiveness from you. Your enthusiasm for good science was always and will always be an inspiring factor for me. You are a wonderful person, I met in my life.
I would like to thank my parents for their trust in me and their support while I was far away from home. I want to thank them for all the things they made possible but especially for giving me the opportunity to study and learn. Without your vision for my childhood, I would not have been here. You always shape my spirit and spirituality.
I would like to thank Prof. Jon Karlsson who was my mentor in the last phase of my PhD and Prof. Goran Dellgren who was my mentor in the initial phase of my PhD. They enabled me to fulfill my role and needs as a student.
I would like to thank Debashish Banerjee, as my unofficial mentor, and as a good friend for life. You were always at the receiving end of my frustrations and I apologize for that. Thank you for always being with me irrespective of my mood
ACKNOWLEDGEMENTS
70
ACKNOWLEDGEMENTS
tantrums. I would like to thank Galyna Travnikova who never stopped lending me a reliable and helping hand, and as friend for life.
I would like to thank my friends Yolanda, Goditha, Deepti, Uzair, Meghnad, Margareta, and Meghashree for being with me and cheering with me. You made the journey of this course memorable.
I would like to thank Pradeep Patil with whom I had both a friend and foe relationship. You helped me to settle not only in the lab but in Gothenburg too. My initial days could have become difficult without you. I also want to express my thanks and gratitude to Prof. Suchitra Holgersson for opening the doors of Sweden for me and expressing affection in the initial days of my PhD.
Last but not least, I would like to Thank Nikhil as my colleague, friend, adviser, husband and critic. You are the backbone of my life and the smile and trust on your and our kids’ faces give me strength to fight every battle of my life.
71
ACKNOWLEDGEMENTS
3 INTRODUCTION
72
73
REFERENCES
1 Langer, R. & Vacanti, J. P. Tissue engineering. Science (New York, N.Y.) 260, 920-926, doi:10.1126/science.8493529 (1993).
2 Streeter, B. W. & Davis, M. E. Therapeutic Cardiac Patches for Repai-ring the Myocardium. Advances in experimental medicine and biology 1144, 1-24, doi:10.1007/5584_2018_309 (2019).
3 Ghetti, M. et al. Decellularized human dermal matrix produced by a skin bank A new treatment for abdominal wall defects. Annali italiani di chirurgia 5, 443-448 (2017).
4 Costa, A. et al. Biological Scaffolds for Abdominal Wall Repair: Future in Clinical Application? Materials (Basel, Switzerland) 12, doi:10.3390/ma12152375 (2019).
5 Kim, Y. S., Majid, M., Melchiorri, A. J. & Mikos, A. G. Applications of decellularized extracellular matrix in bone and cartilage tissue engineering. Bioengineering & translational medicine 4, 83-95, doi:10.1002/btm2.10110 (2019).
6 Brown, B. N. & Badylak, S. F. Extracellular matrix as an inductive scaffold for fun-ctional tissue reconstruction. Transl Res 163, 268-285, doi:10.1016/j.trsl.2013.11.003 (2014).
7 Aiyelabegan, H. T. & Sadroddiny, E. Fundamentals of protein and cell interactions in biomaterials. Biomedicine & pharmacotherapy 88, 956-970, doi:10.1016/j.biopha.2017.01.136 (2017).
8 Atala, A., Bauer, S. B., Soker, S., Yoo, J. J. & Retik, A. B. Tissue-engineered auto-logous bladders for patients needing cystoplasty. Lancet (London, England) 367, 1241-1246, doi:10.1016/s0140-6736(06)68438-9 (2006).
9 Barber, F. A., Herbert, M. A. & Coons, D. A. Tendon augmentation grafts: biomecha-nical failure loads and failure patterns. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the Inter-national Arthroscopy Association 22, 534-538, doi:10.1016/j.arthro.2005.12.021 (2006).
10 Brigido, S. A. The use of an acellular dermal regenerative tissue matrix in the tre-atment of lower extremity wounds: a prospective 16-week pilot study. International wound journal 3, 181-187, doi:10.1111/j.1742-481X.2006.00209.x (2006).
11 Butler, C. E. & Prieto, V. G. Reduction of adhesions with composite AlloDerm/po-lypropylene mesh implants for abdominal wall reconstruction. Plastic and reconstructive surgery 114, 464-473 (2004).
12 Liyanage, S. H., Singh, A., Savundra, P. & Kalan, A. Pulsatile tinnitus. The Journal of laryngology and otology 120, 93-97, doi:10.1017/s0022215105001714 (2006).
REFERENCES
74
REFERENCES
13 Weber, K. T. From inflammation to fibrosis: a stiff stretch of highway. Hypertension (Dallas, Tex. : 1979) 43, 716-719, doi:10.1161/01.HYP.0000118586.38323.5b (2004).
14 Rienks, M., Papageorgiou, A. P., Frangogiannis, N. G. & Heymans, S. Myocardial extracellular matrix: an ever-changing and diverse entity. Circ Res 114, 872-888, doi:10.1161/circresaha.114.302533 (2014).
15 Lockhart, M., Wirrig, E., Phelps, A. & Wessels, A. Extracellular matrix and heart development. Birth defects research. Part A, Clinical and molecular teratology 91, 535-550, doi:10.1002/bdra.20810 (2011).
16 Badylak, S. F. et al. The use of xenogeneic small intestinal submucosa as a bioma-terial for Achilles tendon repair in a dog model. J Biomed Mater Res 29, 977-985, doi:10.1002/jbm.820290809 (1995).
17 Kc, P., Hong, Y. & Zhang, G. Cardiac tissue-derived extracellular matrix scaffolds for myocardial repair: advantages and challenges. Regenerative biomaterials 6, 185-199, doi:10.1093/rb/rbz017 (2019).
18 Moroni, F. & Mirabella, T. Decellularized matrices for cardiovascular tissue engine-ering. American journal of stem cells 3, 1-20 (2014).
19 Kc, P., Hong, Y. & Zhang, G. Cardiac tissue-derived extracellular matrix scaffolds for myocardial repair: advantages and challenges. Regenerative biomaterials 6, 185-199, doi:10.1093/rb/rbz017 (2019).
20 Sarig, U. et al. Natural myocardial ECM patch drives cardiac progenitor ba-sed restoration even after scarring. Acta biomaterialia 44, 209-220, doi:10.1016/j.act-bio.2016.08.031 (2016).
21 Wainwright, J. M. et al. Right ventricular outflow tract repair with a cardiac biolo-gic scaffold. Cells, tissues, organs 195, 159-170, doi:10.1159/000331400 (2012).
22 Blaudez, F., Ivanovski, S., Hamlet, S. & Vaquette, C. An overview of decellularisation techniques of native tissues and tissue engineered products for bone, ligament and tendon regeneration. Methods (San Diego, Calif.), doi:10.1016/j.ymeth.2019.08.002 (2019).
23 Keane, T. J., Swinehart, I. T. & Badylak, S. F. Methods of tissue decellularization used for preparation of biologic scaffolds and in vivo relevance. Methods (San Diego, Calif.) 84, 25-34, doi:10.1016/j.ymeth.2015.03.005 (2015).
24 Crapo, P. M., Gilbert, T. W. & Badylak, S. F. An overview of tissue and whole organ decellularization processes. Biomaterials 32, 3233-3243, doi:10.1016/j.biomaterials.2011.01.057 (2011).
25 Gilbert, T. W., Sellaro, T. L. & Badylak, S. F. Decellularization of tissues and organs. Biomaterials 27, 3675-3683, doi:10.1016/j.biomaterials.2006.02.014 (2006).
26 Morris, A. H., Chang, J. & Kyriakides, T. R. Inadequate Processing of Decellularized Dermal Matrix Reduces Cell Viability In Vitro and Increases Apoptosis and Acute Inflamma-tion In Vivo. BioResearch open access 5, 177-187, doi:10.1089/biores.2016.0021 (2016).
27 Abid, S. & El-Hayek, K. Which mesh or graft? Prosthetic devices for abdominal wall reconstruction. Br J Hosp Med (Lond) 77, 157-158, 159-161, doi:10.12968/hmed.2016.77.3.157 (2016).
28 Lock, A., Cornish, J. & Musson, D. The Role of In Vitro Immune Response Assess-ment for Biomaterials. Journal of functional biomaterials 10, 31, doi:10.3390/jfb10030031 (2019).
29 Lock, A., Cornish, J. & Musson, D. S. The Role of In Vitro Immune Response As-sessment for Biomaterials. Journal of functional biomaterials 10, doi:10.3390/jfb10030031 (2019).
30 Aamodt, J. M. & Grainger, D. W. Extracellular matrix-based biomaterial scaffolds
75
REFERENCES
and the host response. Biomaterials 86, 68-82, doi:10.1016/j.biomaterials.2016.02.003 (2016).
31 Cravedi, P. et al. Regenerative immunology: the immunological reaction to bioma-terials. Transplant international : official journal of the European Society for Organ Trans-plantation 30, 1199-1208, doi:10.1111/tri.13068 (2017).
32 Morais, J. M., Papadimitrakopoulos, F. & Burgess, D. J. Biomaterials/tissue interac-tions: possible solutions to overcome foreign body response. The AAPS journal 12, 188-196, doi:10.1208/s12248-010-9175-3 (2010).
33 Wissing, T. B., Bonito, V., Bouten, C. V. C. & Smits, A. Biomaterial-driven in situ car-diovascular tissue engineering-a multi-disciplinary perspective. NPJ Regenerative medicine 2, 18, doi:10.1038/s41536-017-0023-2 (2017).
34 Lotze, M. T., Deisseroth, A. & Rubartelli, A. Damage associated molecular pattern molecules. Clinical immunology (Orlando, Fla.) 124, 1-4, doi:10.1016/j.clim.2007.02.006 (2007).
35 Bianchi, M. E. DAMPs, PAMPs and alarmins: all we need to know about danger. Journal of leukocyte biology 81, 1-5, doi:10.1189/jlb.0306164 (2007).
36 Gilbert, T. W., Sellaro, T. L. & Badylak, S. F. Decellularization of tissues and organs. Biomaterials 27, 3675-3683, doi:10.1016/j.biomaterials.2006.02.014 (2006).
37 Badylak, S. F. & Gilbert, T. W. Immune response to biologic scaffold materials. Seminars in immunology 20, 109-116, doi:10.1016/j.smim.2007.11.003 (2008).
38 Rozario, T. & DeSimone, D. W. The extracellular matrix in development and morp-hogenesis: a dynamic view. Dev Biol 341, 126-140, doi:10.1016/j.ydbio.2009.10.026 (2010).
39 Toole, B. P. Hyaluronan in morphogenesis. Semin Cell Dev Biol 12, 79-87, doi:10.1006/scdb.2000.0244 (2001).
40 Stern, R., Asari, A. A. & Sugahara, K. N. Hyaluronan fragments: an information-rich system. Eur J Cell Biol 85, 699-715, doi:10.1016/j.ejcb.2006.05.009 (2006).
41 Klein, B., Schiffer, R., Hafemann, B., Klosterhalfen, B. & Zwadlo-Klarwasser, G. Inflammatory response to a porcine membrane composed of fibrous collagen and elastin as dermal substitute. J Mater Sci Mater Med 12, 419-424 (2001).
42 Debret, R. et al. Elastin-derived peptides induce a T-helper type 1 polarization of human blood lymphocytes. Arterioscler Thromb Vasc Biol 25, 1353-1358, doi:10.1161/01.ATV.0000168412.50855.9f (2005).
43 Koninger, J. et al. The ECM proteoglycan decorin links desmoplasia and inflamma-tion in chronic pancreatitis. J Clin Pathol 59, 21-27, doi:10.1136/jcp.2004.023135 (2006).
44 Comalada, M. et al. Decorin reverses the repressive effect of autocrine-produced TGF-beta on mouse macrophage activation. J Immunol 170, 4450-4456 (2003).
45 Vittal, R. et al. Type V collagen induced tolerance suppresses collagen deposition, TGF-beta and associated transcripts in pulmonary fibrosis. PLoS One 8, e76451, doi:10.1371/journal.pone.0076451 (2013).
46 Luther, D. J. et al. Absence of type VI collagen paradoxically improves cardiac function, structure, and remodeling after myocardial infarction. Circ Res 110, 851-856, doi:10.1161/circresaha.111.252734 (2012).
47 Morwood, S. R. & Nicholson, L. B. Modulation of the immune response by extra-cellular matrix proteins. Archivum immunologiae et therapiae experimentalis 54, 367-374, doi:10.1007/s00005-006-0043-x (2006).
48 Liu, X., Li, N., Gong, D., Xia, C. & Xu, Z. Comparison of detergent-based decellula-rization protocols for the removal of antigenic cellular components in porcine aortic valve. Xenotransplantation 25, e12380, doi:10.1111/xen.12380 (2018).
76
REFERENCES
49 Mendoza-Novelo, B. et al. Decellularization of pericardial tissue and its impact on tensile viscoelasticity and glycosaminoglycan content. Acta biomaterialia 7, 1241-1248, doi:10.1016/j.actbio.2010.11.017 (2011).
50 Syed, O., Walters, N. J., Day, R. M., Kim, H. W. & Knowles, J. C. Evaluation of decellularization protocols for production of tubular small intestine submucosa scaffolds for use in oesophageal tissue engineering. Acta biomaterialia 10, 5043-5054, doi:10.1016/j.actbio.2014.08.024 (2014).
51 Gilpin, A. & Yang, Y. Decellularization Strategies for Regenerative Medicine: From Processing Techniques to Applications. BioMed research international 2017, 9831534, doi:10.1155/2017/9831534 (2017).
52 Wong, M. & Griffiths, L. Immunogenicity in xenogeneic scaffold generation: Antigen removal vs. decellularization. Acta biomaterialia 10, doi:10.1016/j.actbio.2014.01.028 (2014).
53 Platz, J. et al. Comparative Decellularization and Recellularization of Wild-Type and Alpha 1,3 Galactosyltransferase Knockout Pig Lungs: A Model for Ex Vivo Xenogeneic Lung Bioengineering and Transplantation. Tissue engineering. Part C, Methods 22, 725-739, doi:10.1089/ten.TEC.2016.0109 (2016).
54 Hellstrom, M. et al. Towards the development of a bioengineered uterus: compa-rison of different protocols for rat uterus decellularization. Acta biomaterialia 10, 5034-5042, doi:10.1016/j.actbio.2014.08.018 (2014).
55 Daly, A. et al. Initial Binding and Recellularization of Decellularized Mouse Lung Scaffolds with Bone Marrow-Derived Mesenchymal Stromal Cells. Tissue engineering. Part A 18, 1-16, doi:10.1089/ten.TEA.2011.0301 (2011).
56 Hinderer, S., Layland, S. L. & Schenke-Layland, K. ECM and ECM-like materials - Biomaterials for applications in regenerative medicine and cancer therapy. Advanced drug delivery reviews 97, 260-269, doi:10.1016/j.addr.2015.11.019 (2016).
57 Hoshiba, T., Lu, H., Kawazoe, N. & Chen, G. Decellularized matrices for tissue engi-neering. Expert opinion on biological therapy 10, 1717-1728, doi:10.1517/14712598.2010.534079 (2010).
58 Strobel, H. A., Qendro, E. I., Alsberg, E. & Rolle, M. W. Targeted Delivery of Bioactive Molecules for Vascular Intervention and Tissue Engineering. Frontiers in pharmacology 9, 1329, doi:10.3389/fphar.2018.01329 (2018).
59 Yao, Q. et al. Recent development and biomedical applications of decellularized extracellular matrix biomaterials. Materials science & engineering. C, Materials for biological applications 104, 109942, doi:10.1016/j.msec.2019.109942 (2019).
60 Lin, C. H., Hsia, K., Ma, H., Lee, H. & Lu, J. H. In Vivo Performance of Decellularized Vascular Grafts: A Review Article. International journal of molecular sciences 19, doi:10.3390/ijms19072101 (2018).
61 Neumann, A. et al. Early systemic cellular immune response in children and young adults receiving decellularized fresh allografts for pulmonary valve replacement. Tissue engineering. Part A 20, 1003-1011, doi:10.1089/ten.TEA.2013.0316 (2014).
62 Cebotari, S. et al. Use of fresh decellularized allografts for pulmonary valve repla-cement may reduce the reoperation rate in children and young adults: early report. Circula-tion 124, S115-123, doi:10.1161/circulationaha.110.012161 (2011).
63 Tudorache, I. et al. Decellularized aortic homografts for aortic valve and aorta ascendens replacement. European journal of cardio-thoracic surgery : official journal of the European Association for Cardio-thoracic Surgery 50, 89-97, doi:10.1093/ejcts/ezw013 (2016).
64 Valentin, J. E., Badylak, J. S., McCabe, G. P. & Badylak, S. F. Extracellular matrix bioscaffolds for orthopaedic applications. A comparative histologic study. The Journal of bone and joint surgery. American volume 88, 2673-2686, doi:10.2106/jbjs.e.01008 (2006).
77
REFERENCES
65 Morris, A. H., Stamer, D. K. & Kyriakides, T. R. The host response to naturally-derived extracellular matrix biomaterials. Seminars in immunology 29, 72-91, doi:10.1016/j.smim.2017.01.002 (2017).
66 Badylak, S. F. Extracellular matrix and the immune system: friends or foes. Nature Reviews Urology 16, 389-390, doi:10.1038/s41585-019-0196-0 (2019).
67 Wong, M. L. & Griffiths, L. G. Immunogenicity in xenogeneic scaffold generation: antigen removal vs. decellularization. Acta biomaterialia 10, 1806-1816, doi:10.1016/j.act-bio.2014.01.028 (2014).
68 Sandor, M. et al. Host response to implanted porcine-derived biologic materi-als in a primate model of abdominal wall repair. Tissue engineering. Part A 14, 2021-2031, doi:10.1089/ten.tea.2007.0317 (2008).
69 Bryan, N. et al. Characterisation and comparison of the host response of 6 tissue-based surgical implants in a subcutaneous in vivo rat model. Journal of applied biomaterials & functional materials 13, 35-42, doi:10.5301/jabfm.5000172 (2015).
70 Galili, U. Avoiding detrimental human immune response against Mammalian ex-tracellular matrix implants. Tissue engineering. Part B, Reviews 21, 231-241, doi:10.1089/ten.TEB.2014.0392 (2015).
71 Mariani, E., Lisignoli, G., Borzi, R. M. & Pulsatelli, L. Biomaterials: Foreign Bo-dies or Tuners for the Immune Response? International journal of molecular sciences 20, doi:10.3390/ijms20030636 (2019).
72 Crupi, A., Costa, A., Tarnok, A., Melzer, S. & Teodori, L. Inflammation in tissue engi-neering: The Janus between engraftment and rejection. European journal of immunology 45, 3222-3236, doi:10.1002/eji.201545818 (2015).
73 Allman, A. et al. Xenogeneic extracellular matrix grafts elicit a TH2-restricted immune response. Transplantation 71, 1631-1640, doi:10.1097/00007890-200106150-00024 (2001).
74 Badylak, S. F. & Gilbert, T. W. Immune response to biologic scaffold materials. Seminars in immunology 20, 109-116, doi:10.1016/j.smim.2007.11.003 (2008).
75 Shridhar, A., Gillies, E., Amsden, B. G. & Flynn, L. E. Composite Bioscaffolds Incor-porating Decellularized ECM as a Cell-Instructive Component Within Hydrogels as In Vitro Models and Cell Delivery Systems. Methods in molecular biology (Clifton, N.J.) 1577, 183-208, doi:10.1007/7651_2017_36 (2018).
76 Kowalski, P. S., Bhattacharya, C., Afewerki, S. & Langer, R. Smart Biomaterials: Re-cent Advances and Future Directions. ACS Biomaterials Science & Engineering 4, 3809-3817, doi:10.1021/acsbiomaterials.8b00889 (2018).


































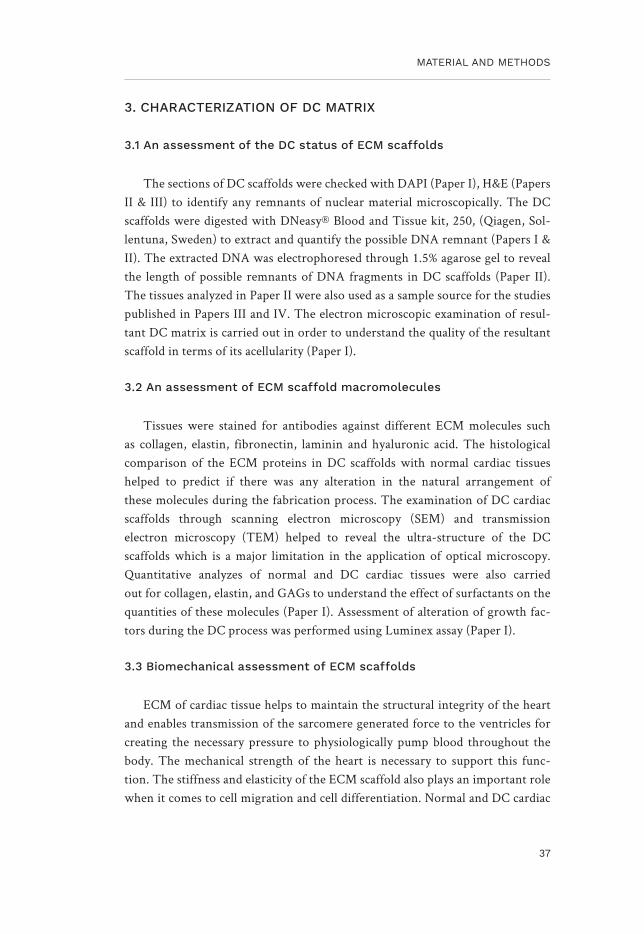

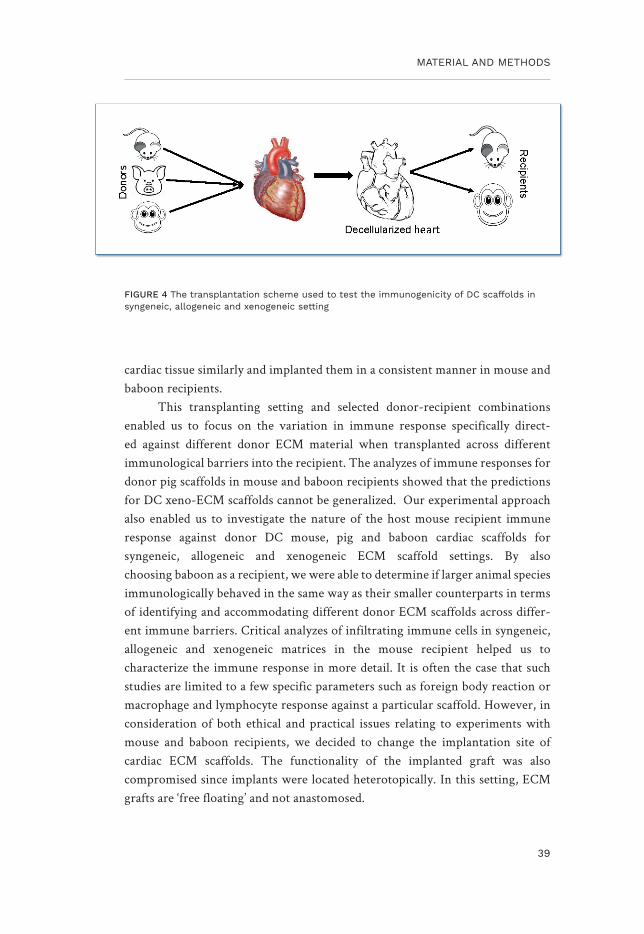


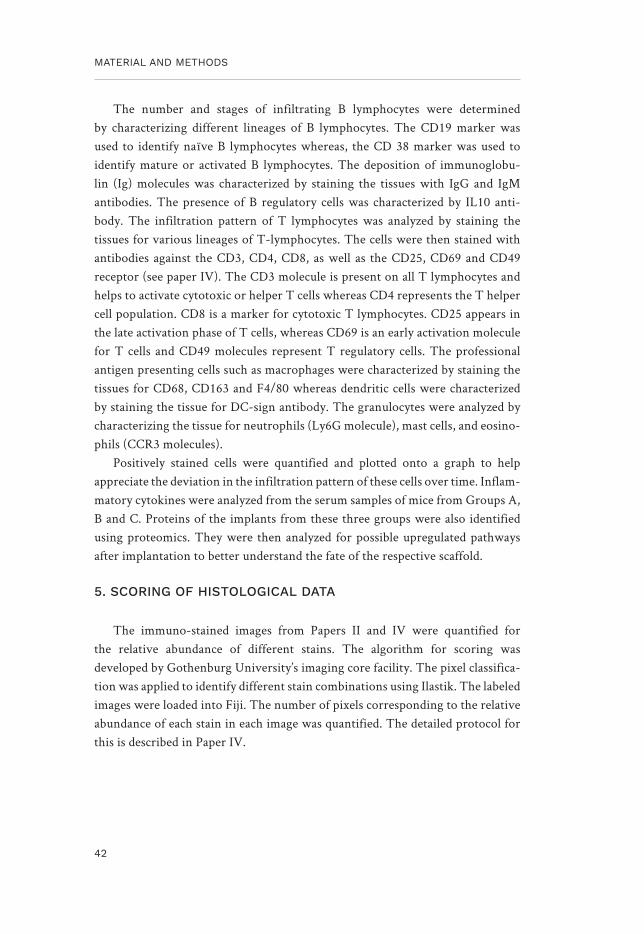

































![Kidney Transplantation (Renal Transplantation) Auto Saved]](https://static.documents.pub/doc/80x56/577d22b31a28ab4e1e9807d7/kidney-transplantation-renal-transplantation-auto-saved.jpg)













