Trattamento del tromboembolismo Prof. Stefania Basili Centro Aterotrombosi – Divisione di I Clinica Medica (Direttore Prof. Francesco Violi) , tromboembolismo venoso: gestione della anticoagulazione.
Transcript
Trattamento del tromboembolismo
Prof. Stefania Basili
Centro Aterotrombosi – Divisione di I Clinica Medica
(Direttore Prof. Francesco Violi),
tromboembolismo venoso: gestione della
anticoagulazione.
VTE is under recognized and
goes
When diagnosis is based on clinical signs and symptoms:
• <50% of all cases of No tests to
predict who will
TERZA PIU’ COMUNE CAUSA DI MORTE CARDIOVASCO
VTE is the silent killer
goes undiagnosed
• <50% of all cases of fatal PE are detected prior to death
• 80% of cases of DVT are clinically silent
predict who will have a VTE
CARDIOVASCOLARE
• PREVENTION IS KEY!!
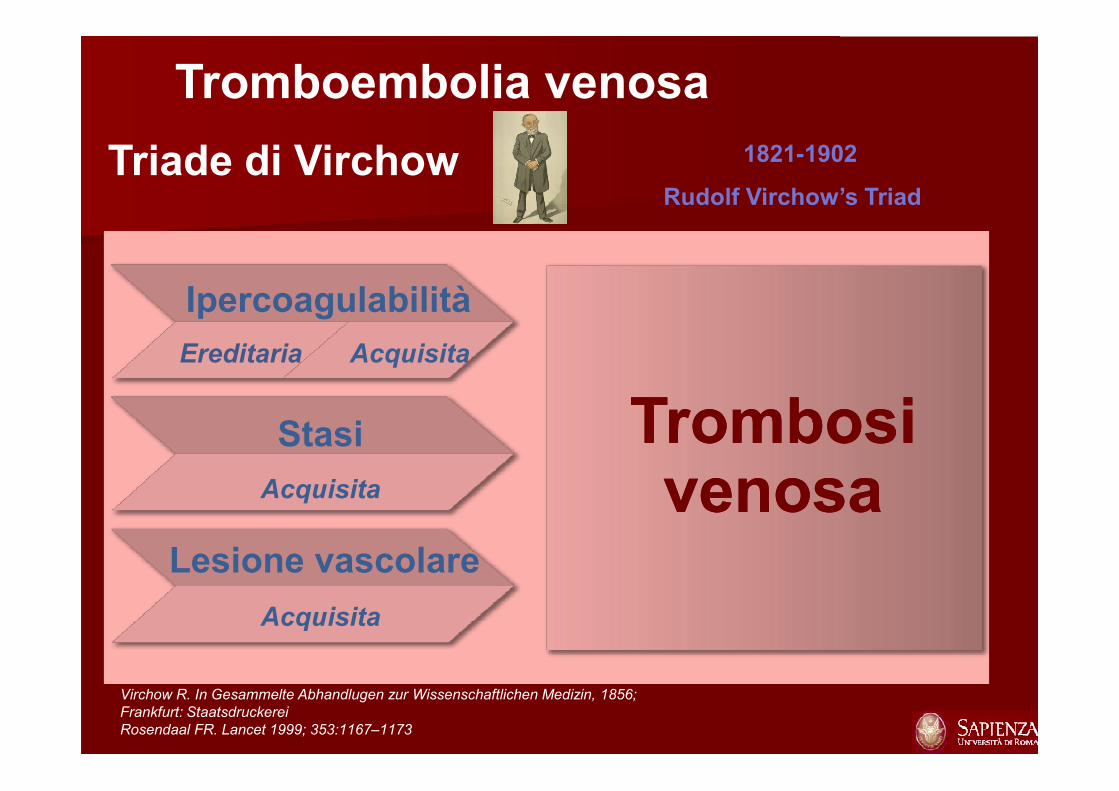
Tromboembolia venosa
Triade di Virchow
Ipercoagulabilità
AcquisitaEreditaria
TrombosiTrombosi
1821-1902
Rudolf Virchow’s Triad
Virchow R. In Gesammelte Abhandlugen zur Wissenschaftlichen Medizin, 1856;
Frankfurt: Staatsdruckerei
Rosendaal FR. Lancet 1999; 353:1167–1173
Stasi
Lesione vascolare
Acquisita
Acquisita
Trombosivenosa
Trombosivenosa
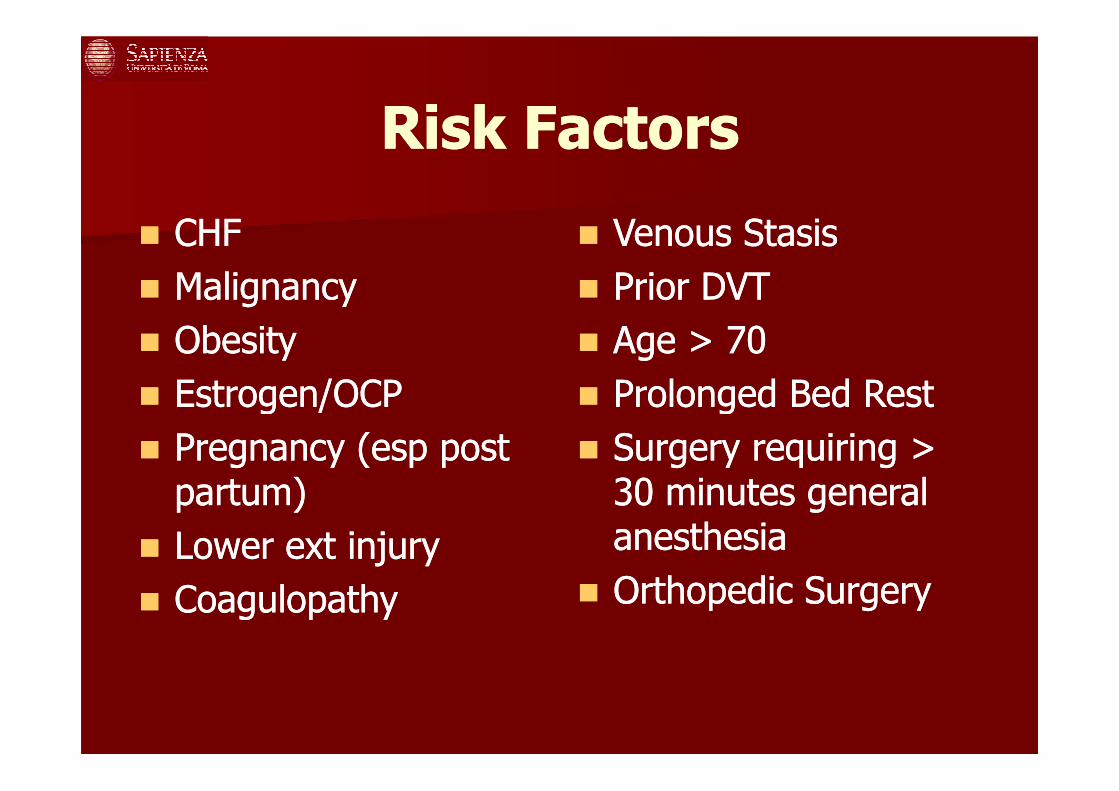
Risk FactorsRisk Factors
�� CHFCHF
�� MalignancyMalignancy
�� ObesityObesity
�� Estrogen/OCPEstrogen/OCP
�� Venous StasisVenous Stasis
�� Prior DVTPrior DVT
�� Age > 70Age > 70
�� Prolonged Bed RestProlonged Bed Rest�� Estrogen/OCPEstrogen/OCP
�� Pregnancy (esp post Pregnancy (esp post partum)partum)
�� Lower ext injuryLower ext injury
�� CoagulopathyCoagulopathy
�� Prolonged Bed RestProlonged Bed Rest
�� Surgery requiring > Surgery requiring > 30 minutes general 30 minutes general anesthesiaanesthesia
�� Orthopedic SurgeryOrthopedic Surgery
Definizione di Tromboembolismo Venoso Definizione di Tromboembolismo Venoso
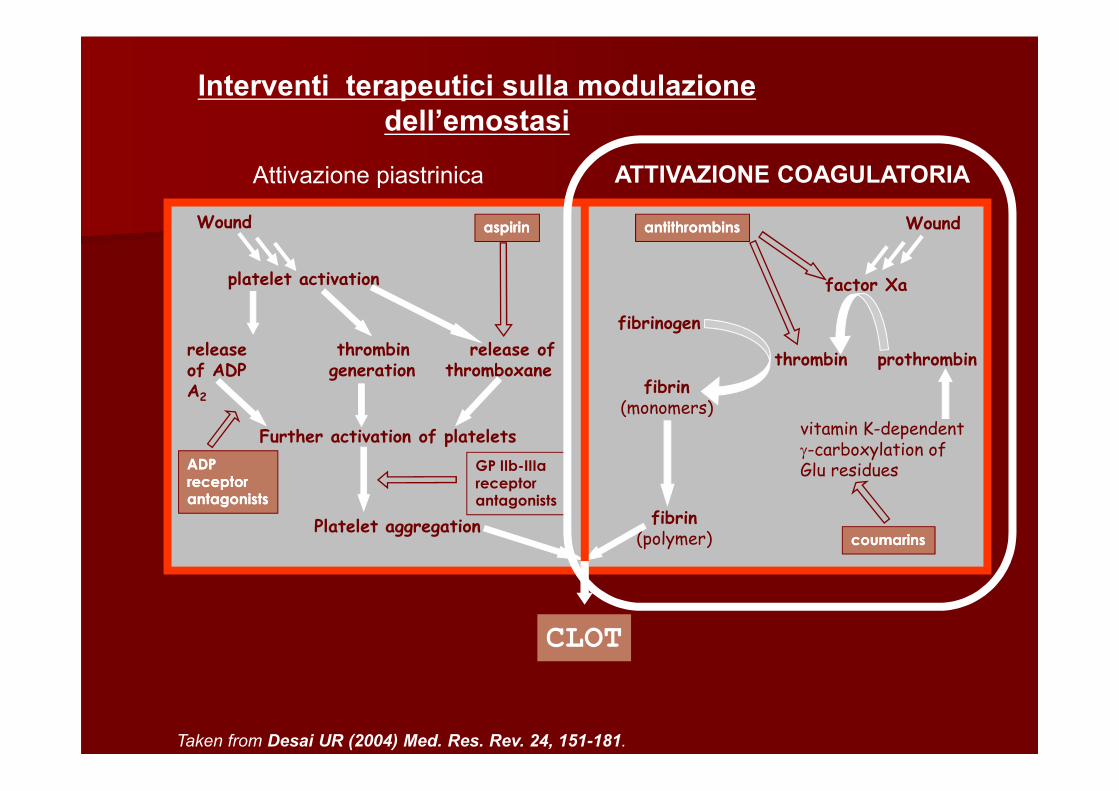
Taken from Desai UR (2004) Med. Res. Rev. 24, 151-181.
UFH
Come agiscono le eparine?
LMWH
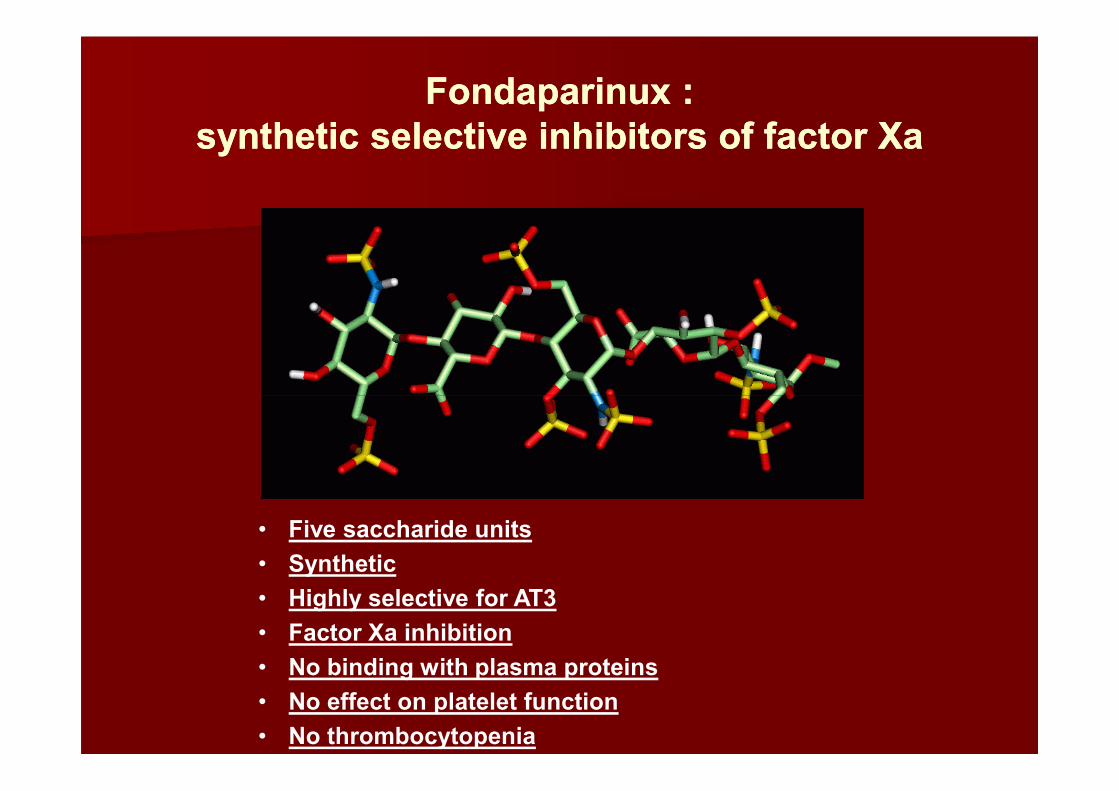
FondaparinuxFondaparinux ::
synthetic synthetic selective inhibitors of factor selective inhibitors of factor XaXa
• Five saccharide units
• Synthetic
• Highly selective for AT3
• Factor Xa inhibition
• No binding with plasma proteins
• No effect on platelet function
• No thrombocytopenia
1941 First clinical use (short term)1944 Use of dicumarol in long-term
prophylaxis after MI1948 Synthesis of warfarin as a rat poison1954 Warfarin introduced in clinical practice
Vitamin K antagonists
Sweet clover
Melilotus alba
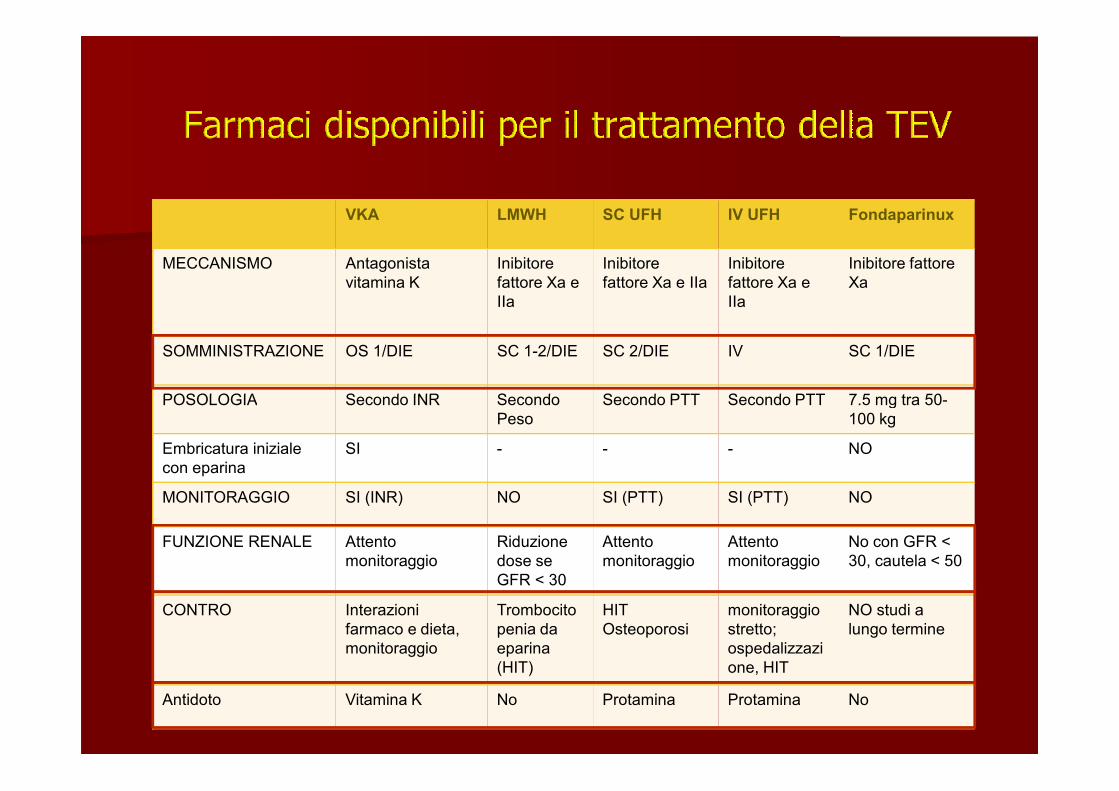
VKA LMWH SC UFH IV UFH Fondaparinux
MECCANISMO Antagonista
vitamina K
Inibitore
fattore Xa e
IIa
Inibitore
fattore Xa e IIa
Inibitore
fattore Xa e
IIa
Inibitore fattore
Xa
SOMMINISTRAZIONE OS 1/DIE SC 1-2/DIE SC 2/DIE IV SC 1/DIE
POSOLOGIA Secondo INR Secondo Secondo PTT Secondo PTT 7.5 mg tra 50-POSOLOGIA Secondo INR Secondo
Peso
Secondo PTT Secondo PTT 7.5 mg tra 50-
100 kg
Embricatura iniziale
con eparina
SI - - - NO
MONITORAGGIO SI (INR) NO SI (PTT) SI (PTT) NO
FUNZIONE RENALE Attento
monitoraggio
Riduzione
dose se
GFR < 30
Attento
monitoraggio
Attento
monitoraggio
No con GFR <
30, cautela < 50
CONTRO Interazioni
farmaco e dieta,
monitoraggio
Trombocito
penia da
eparina
(HIT)
HIT
Osteoporosi
monitoraggio
stretto;
ospedalizzazi
one, HIT
NO studi a
lungo termine
Antidoto Vitamina K No Protamina Protamina No
New Oral anticoagulants and their targets in the coagulation pathwaysNew Oral anticoagulants and their targets in the coagulation pathways
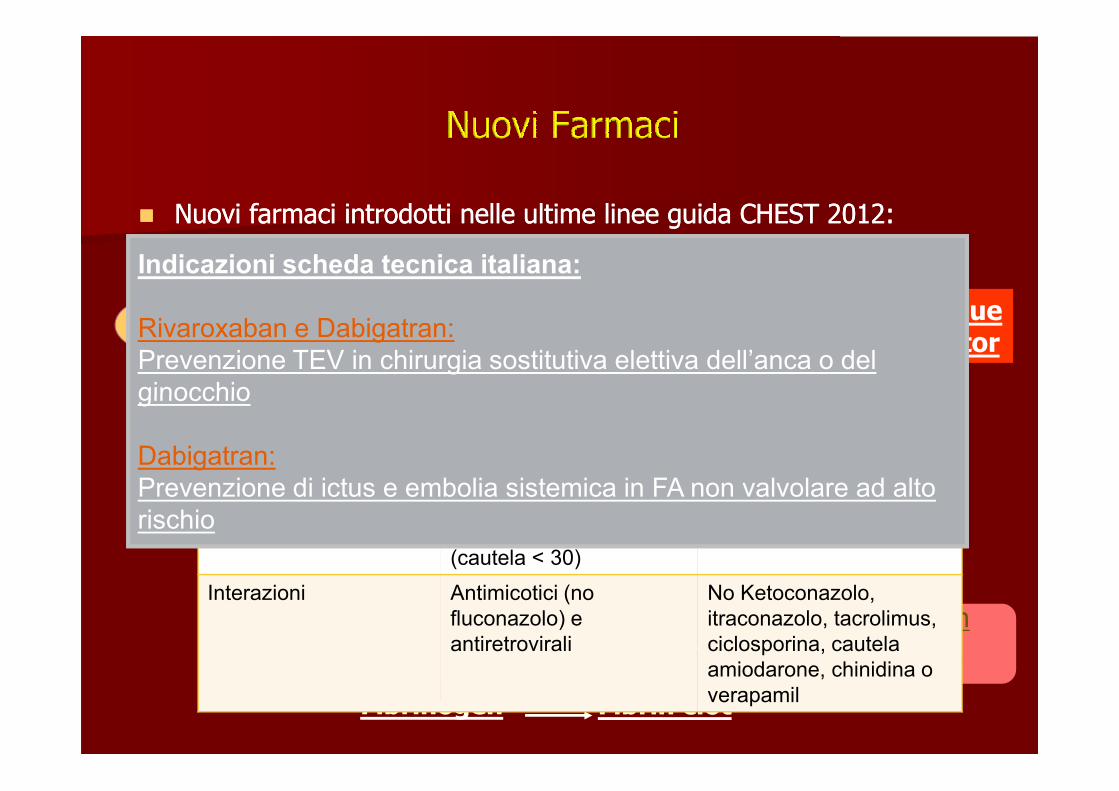
�� Nuovi farmaci introdotti nelle ultime linee guida CHEST 2012:Nuovi farmaci introdotti nelle ultime linee guida CHEST 2012:
VIIaXIa
XIIaTissue factor
Rivaroxaban(Xarelto) 10 mg/die
Rivaroxaban Dabigatran
Posologia 10 mg o.d. (no peso) 220 mg o.d. (no peso)
Indicazioni scheda tecnica italiana:
Rivaroxaban e Dabigatran:
Prevenzione TEV in chirurgia sostitutiva elettiva dell’anca o del
ginocchio
Xa
IXa
Fibrinogen Fibrin clot
Factor II(prothrombin) Dabigatran
(Pradaxa) 220 mg/die
Posologia 10 mg o.d. (no peso) 220 mg o.d. (no peso)
150 mg bid se FA
Monitoraggio No No
Antidoto No No
Funzione renale No in GFR < 15
(cautela < 30)
No in GFR < 30
Interazioni Antimicotici (no
fluconazolo) e
antiretrovirali
No Ketoconazolo,
itraconazolo, tacrolimus,
ciclosporina, cautela
amiodarone, chinidina o
verapamil
ginocchio
Dabigatran:
Prevenzione di ictus e embolia sistemica in FA non valvolare ad alto
rischio
TREATMENT of VENOUS THROMBOEMBOLISMTREATMENT of VENOUS THROMBOEMBOLISM
�� Both Pulmonary embolism and DVT are Both Pulmonary embolism and DVT are treated the sametreated the same
�� An adequate level of anticoagulation is An adequate level of anticoagulation is �� An adequate level of anticoagulation is An adequate level of anticoagulation is essentialessential
�� Patients will have variable effect of Patients will have variable effect of anticoagulantsanticoagulants
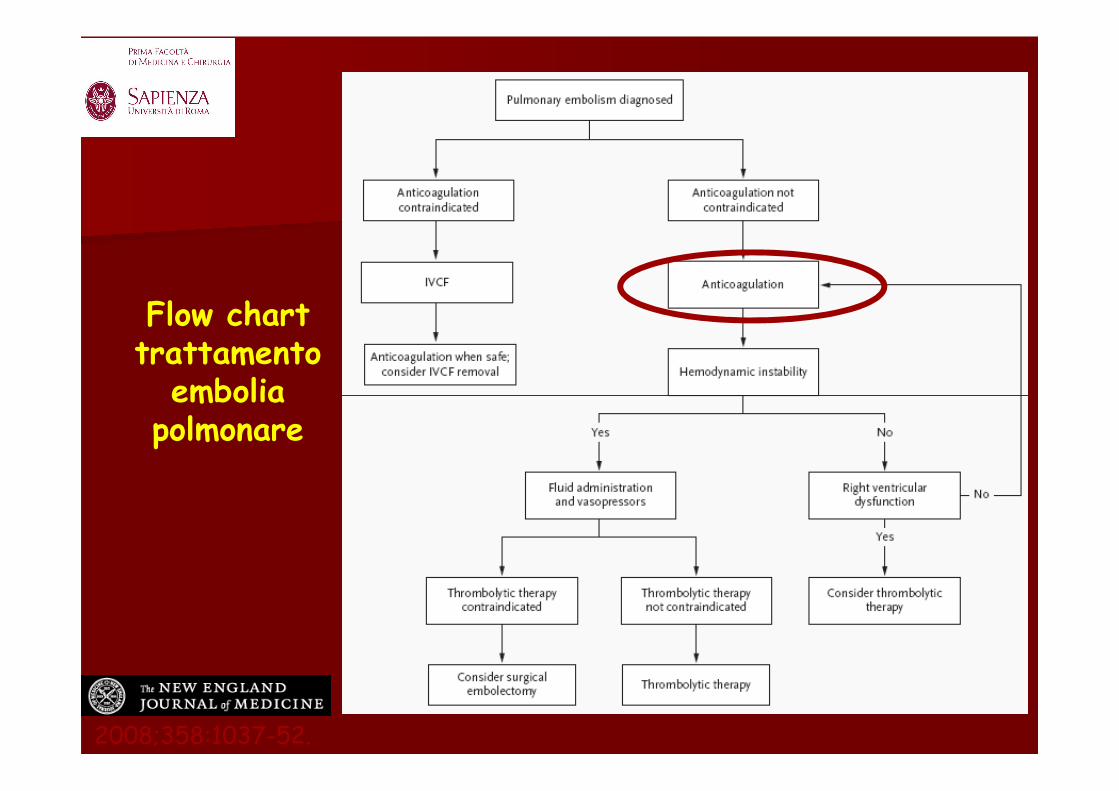
Choice of Initial Anticoagulant Regimen in Patients With Proximal DVT /PE
In patients with ACUTE DVT of the leg, we suggest LMWH or
fondaparinux over IV UFH (Grade 2C) and over SC UFH
(Grade 2B for LMWH; Grade 2C for fondaparinux)..
In patients with ACUTE PE, we suggest LMWH or
fondaparinux over IV UFH (Grade 2C for LMWH; Grade 2B for
fondaparinux) and over SC UFH (Grade 2B for LMWH; Grade 2C
for fondaparinux).
Timing of Initiation of VKA and Associated Duration of
Parenteral Anticoagulant Therapy
In patients with ACUTE DVT of the leg, we recommend early
initiation of VKA (eg, same day as parenteral therapy is started)
over delayed initiation, and continuation of parenteral
anticoagulation for a minimum of 5 days and until the
international normalized ratio (INR) is 2.0 or above for at least
24 h (Grade 1B).
In patients with ACUTE PE, we recommend early initiation of
VKA (eg, same day as parenteral therapy is started) over
delayed initiation, and continuation of parenteral
anticoagulation for a minimum of 5 days and until the INR is
2.0 or above for at least 24 h (Grade 1B).
• Clinical scenario/patient risk factors
• Thrombophilia work up
Determine Recurrence Risk of VTE
• Thrombophilia work up
• Residual vein thrombosis on Ultrasound
• D-dimer testing
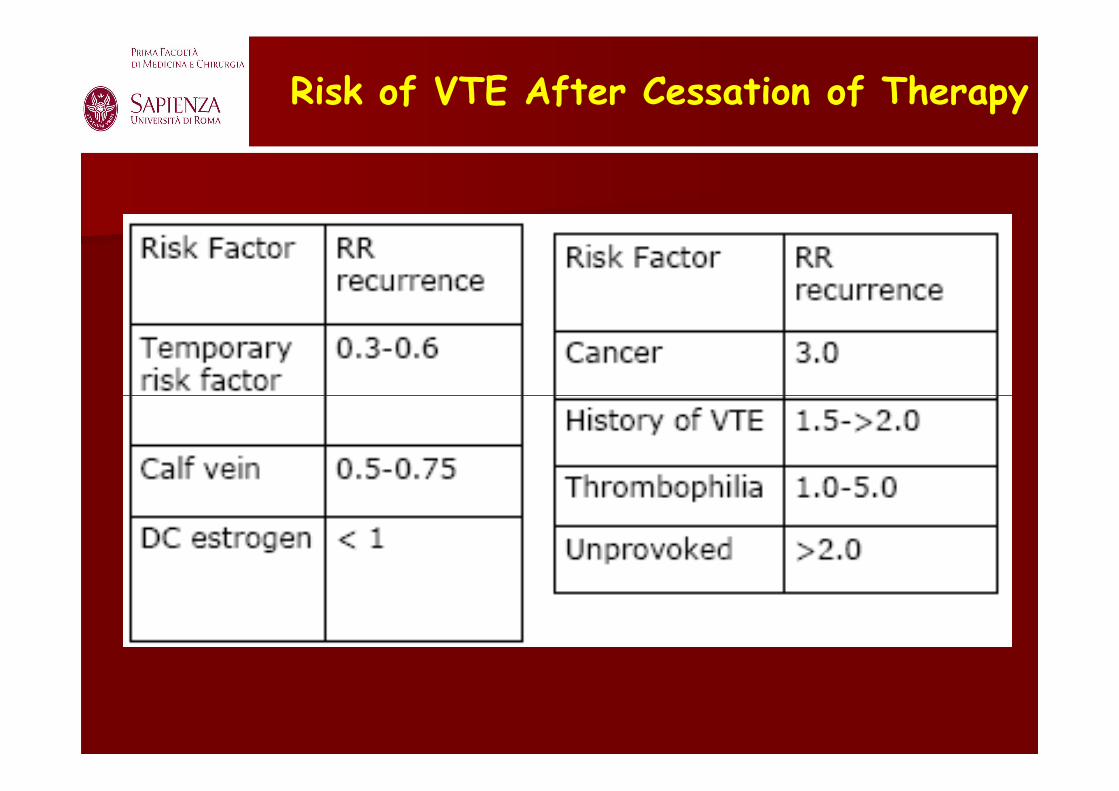
Risk of VTE After Cessation of Therapy
Risk of VTE Recurrence After Cessation of VTE
Risk factorRisk factor 1 st yr1 st yr Next 5 yrsNext 5 yrs
Distal DVTDistal DVT 3%3% <10%<10%
MinorMinor
TransientTransient
3%3% 10%10%
MajorMajor 55--6%6% 15%15%MajorMajor
TransientTransient
55--6%6% 15%15%
UnprovokedUnprovoked At least 10%At least 10% 30%30%
RecurrentRecurrent >10%>10% >30%>30%
Major risk factors: major surgery, major trauma, cancerMinor risk factors: OCP, HRT, pregnancy, airline travel, non-major surgery, minor traumaAssociated medical diseases- IBD, nephrotic syndrome, cancer, sickle cell, multiple myeloma, Waldentrom’s, MGUS, Bechets, P.Vera, APLS
Provoked
TERAPIA 3 MESI SEMPRE
(indipendentemente dal rischio emorragico)
TEV provocata
STOP
TEV NON provocata
Terapia a lungo
termine
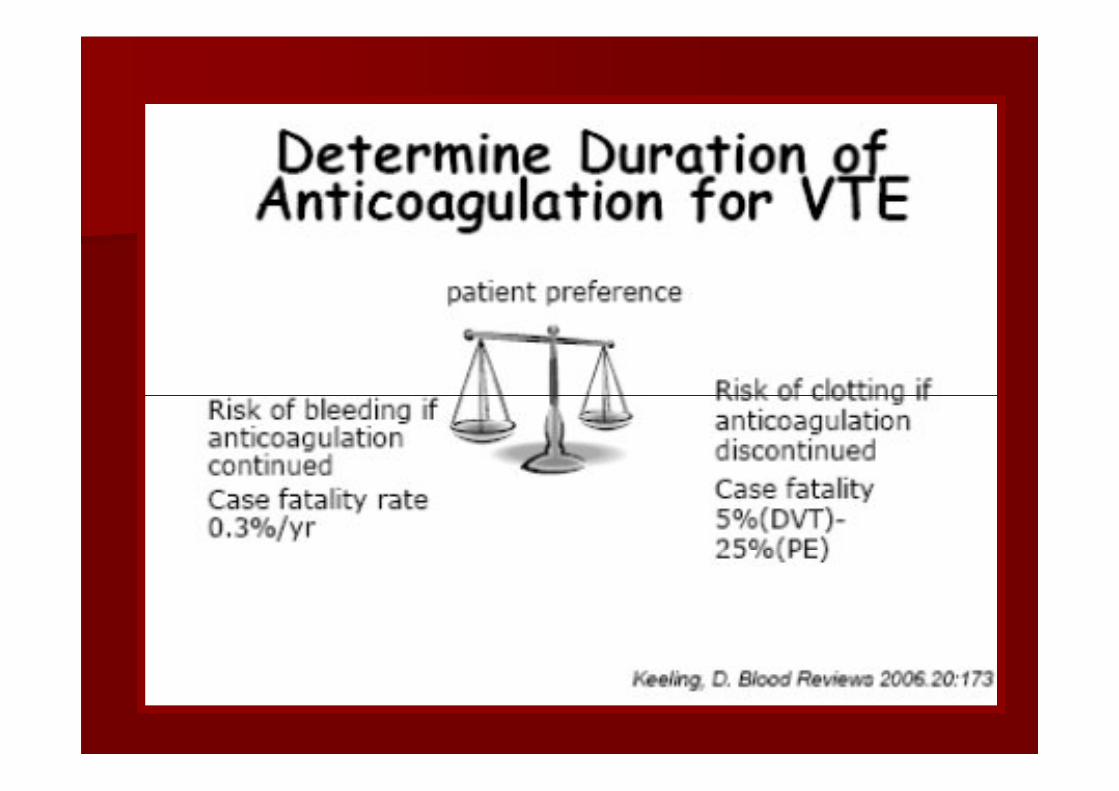
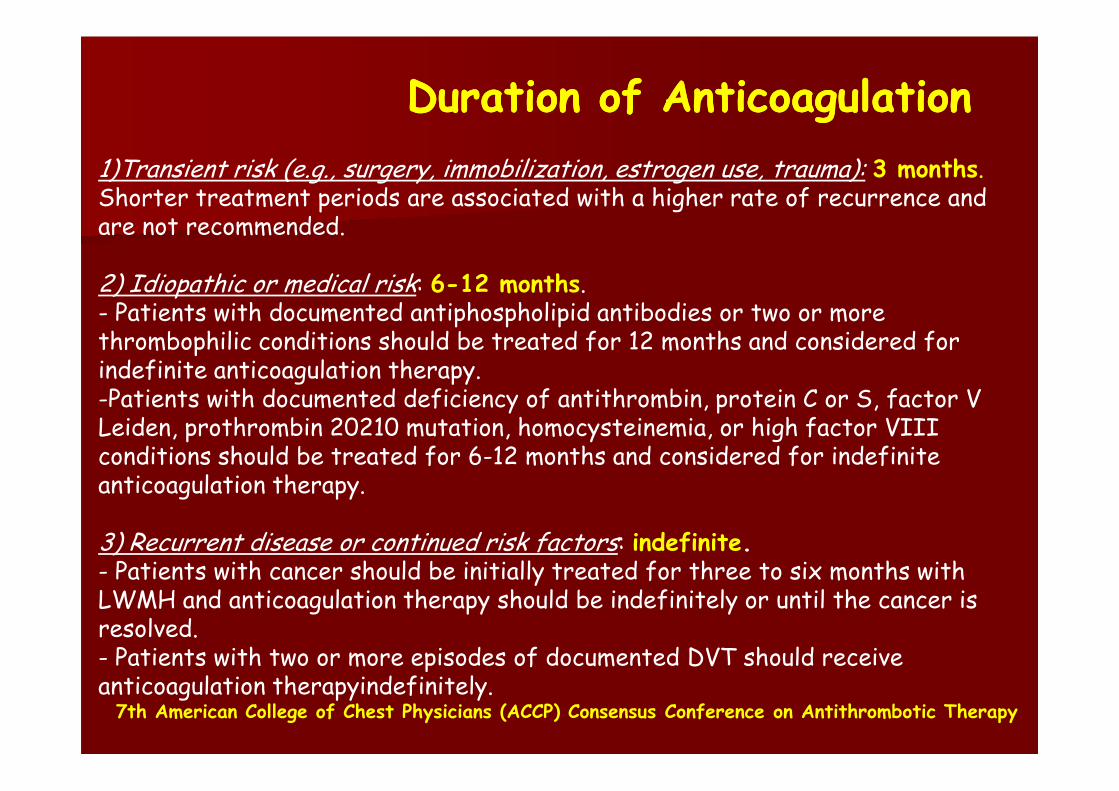
Duration of AnticoagulationDuration of Anticoagulation
1)Transient risk (e.g., surgery, immobilization, estrogen use, trauma): 3 months.Shorter treatment periods are associated with a higher rate of recurrence and are not recommended.
2) Idiopathic or medical risk: 6-12 months.- Patients with documented antiphospholipid antibodies or two or more thrombophilic conditions should be treated for 12 months and considered for indefinite anticoagulation therapy.-Patients with documented deficiency of antithrombin, protein C or S, factor V -Patients with documented deficiency of antithrombin, protein C or S, factor V Leiden, prothrombin 20210 mutation, homocysteinemia, or high factor VIII conditions should be treated for 6-12 months and considered for indefinite anticoagulation therapy.
3) Recurrent disease or continued risk factors: indefinite.- Patients with cancer should be initially treated for three to six months with LWMH and anticoagulation therapy should be indefinitely or until the cancer is resolved.- Patients with two or more episodes of documented DVT should receive anticoagulation therapyindefinitely.
7th American College of Chest Physicians (ACCP) Consensus Conference on Antithrombotic Therapy
The optimal duration of oral anticoagulation in
patients with idiopathic venous thromboembolism
is uncertain.
Optimal duration of TAO
PROLONG Study
Cumulative Incidence of and Hazard Ratios (HRs) for Main Outcomes
Palareti G et al. N Engl J Med 2006;355:1780-1789
is uncertain.
Testing of D-dimerlevels may
play a role in the assessment of the need for prolonged
anticoagulation
F.C.S.A.
2009
TVP/EP idiopatica o fattori di rischio persistenti (trombofilia): 3-6 mesi
Se trombofilia grave o multipla: 1 anno/indefinitamenteSe trombofilia grave o multipla: 1 anno/indefinitamente
Se D-DIMERO +++ dopo 1 mese: ripresa trattamento
Se recidive: indefinitamente
Neoplastici: lungo termine fino alla remissione della neoplasia. Valutare utilizzo LMWH a dosi terapeutiche per almeno 6 mesi.
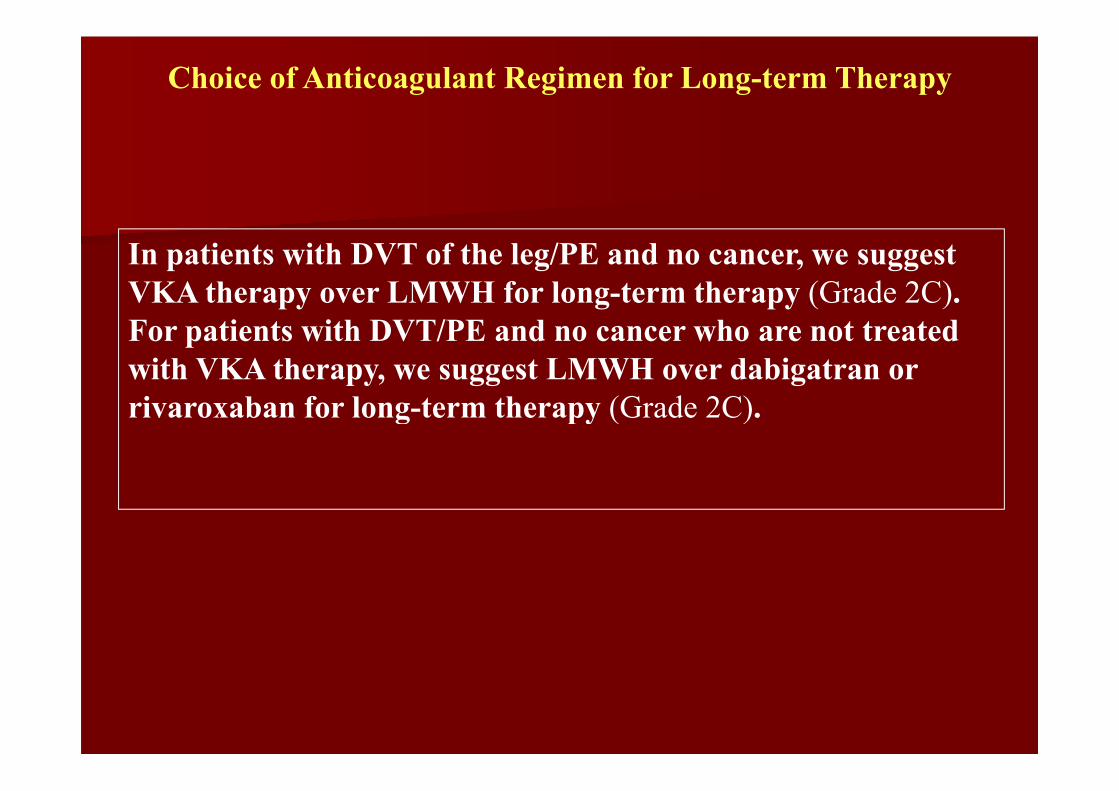
Choice of Anticoagulant Regimen for Long-term Therapy
In patients with DVT of the leg/PE and no cancer, we suggest
VKA therapy over LMWH for long-term therapy (Grade 2C).
For patients with DVT/PE and no cancer who are not treated
with VKA therapy, we suggest LMWH over dabigatran or
rivaroxaban for long-term therapy (Grade 2C). rivaroxaban for long-term therapy (Grade 2C).
Choice of Anticoagulant Regimen for Long-term Therapy
In patients with DVT of the leg and cancer, we suggest LMWH
over VKA therapy (Grade 2B).
In patients with DVT and cancer who are not treated with
LMWH, we suggest VKA over dabigatran or rivaroxaban for
long-term therapy (Grade 2B).
Remarks (3.3.1-3.3.2): Choice of treatment in patients with and without cancer is
sensitive to the individual patient's tolerance for daily injections, need for laboratory sensitive to the individual patient's tolerance for daily injections, need for laboratory
monitoring, and treatment costs.
LMWH, rivaroxaban, and dabigatran are retained in patients with renal impairment,
whereas this is not a concern with VKA.
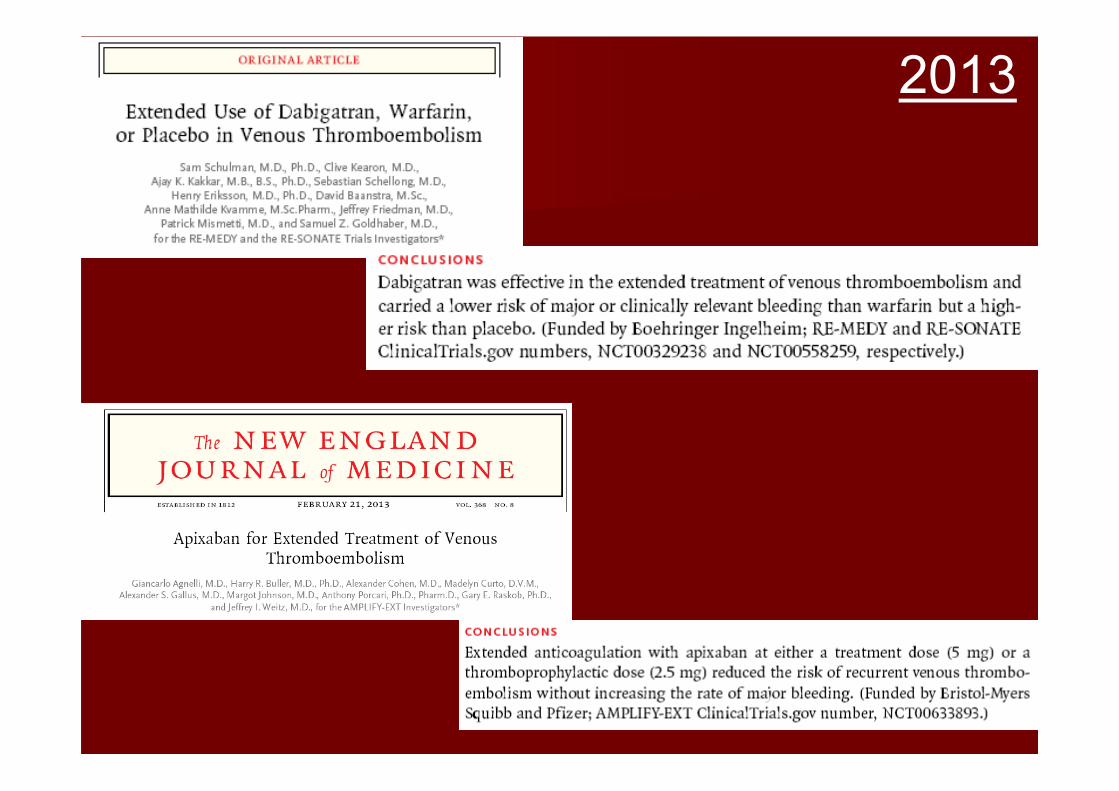
Treatment of VTE with dabigatran or rivaroxaban, in addition to being less burdensome to
patients, may prove to be associated with better clinical outcomes than VKA and LMWH
therapy. When these guidelines were being prepared (October 2011), postmarketing
studies of safety were not available. Given the paucity of currently available data and that
new data are rapidly emerging, we give a weak recommendation in favor of VKA and
LMWH therapy over dabigatran and rivaroxaban, and we have not made any
recommendations in favor of one of the new agents over the other.
Long-term Treatment of Patients With PE
In patients with PE and cancer, we suggest LMWH over VKA
therapy (Grade 2B). In patients with PE and cancer who are
not treated with LMWH, we suggest VKA over dabigatran or
rivaroxaban for long-term therapy (Grade 2C).
Remarks (6.6-6.7): Choice of treatment in patients with and without cancer is
sensitive to the individual patient's tolerance for daily injections, need for sensitive to the individual patient's tolerance for daily injections, need for
laboratory monitoring, and treatment costs. Treatment of VTE with dabigatran or
rivaroxaban, in addition to being less burdensome to patients, may prove to be
associated with better clinical outcomes than VKA and LMWH therapy. When
these guidelines were being prepared (October 2011), postmarketing studies of
safety were not available. Given the paucity of currently available data and that
new data are rapidly emerging, we give a weak recommendation in favor of
VKA and LMWH therapy over dabigatran and rivaroxaban, and we have not
made any recommendation in favor of one of the new agents over the other.
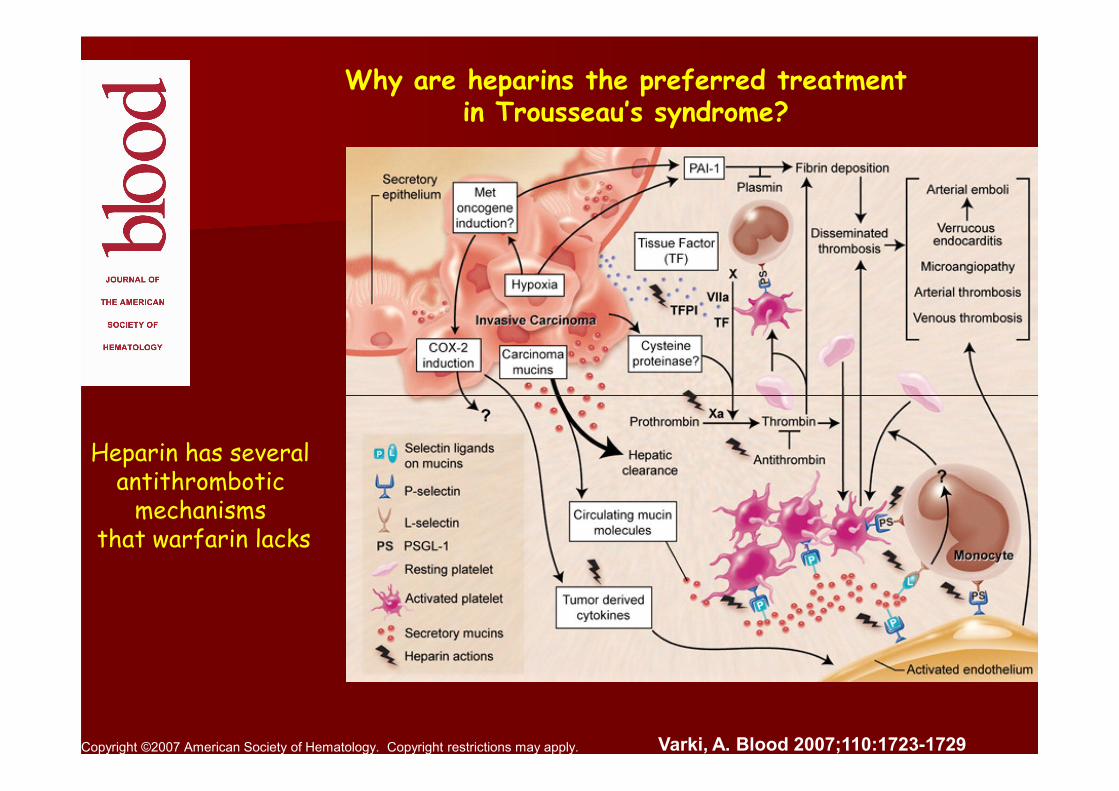
Why are heparins the preferred treatmentin Trousseau’s syndrome?