13 Trauma and disasters in social and cultural context Laurence J. Kirmayer, 1 Hanna Kienzler, 2 Abdel Hamid Afana 3 and Duncan Pedersen 4 1 Division of Social and Transcultural Psychiatry, McGill University and Culture and Mental Health Research Unit, Jewish General Hospital, Montreal, Canada 2 Department of Anthropology, McGill University, Montreal, Canada 3 International Rehabilitation Council for Torture Survivors (IRCT), Copenhagen, Denmark 4 Douglas Mental Health University Institute and Division of Social and Transcultural Psychiatry, McGill University, Montreal, Canada 13.1 INTRODUCTION Trauma and disasters are important causes of human suffering both in terms of the sheer numbers of people affected and the complexity of the mental health problems that may follow. Violence has become one of the leading causes of death worldwide for people aged 15–44 years [1]. Of the total number of global injury-related deaths, about two-thirds are of ‘nonintentional’ origin (e.g. traffic accidents) while one-third are due to intentional violence, including suicides, homicides and organized violence (terror- ism, wars and armed conflict, genocide and ethnic cleansing) [2]. Both the frequency and the numbers of people affected by violence and disasters have in- creased markedly over the last 100 years, while the proportion of people surviving has also risen [3]. This means that there are many more survivors who may be affected psychologically by traumatic events. As the density of human habitation and the intensity of technological development have increased, so too has the scale of disasters. Climate change, economic disparities and political conflicts all can be expected to compound the number and complexity of disasters in the years to come [4]. Social psychiatry has a long engagement with understanding the individual and collective impacts of trauma and disasters. Much of this interest has been driven by experiences of the impact of war on soldiers and civilian populations [5]. The Holocaust and other genocides have forced consideration of the effects of massive human rights violations on the survivors as well as on subsequent generations. The experience of refugees has drawn attention to the impact of displa- cement, forced migration and torture on mental health. Of course, trauma is not only a consequence of such large-scale events but also a common occur- rence in domestic life. Early psychodynamic theory Principles of Social Psychiatry, second edition Edited by Craig Morgan and Dinesh Bhugra Ó 2010 John Wiley & Sons, Ltd. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47
Transcript
13Trauma and disasters in socialand cultural contextLaurence J. Kirmayer,1 Hanna Kienzler,2 Abdel Hamid Afana3 and Duncan Pedersen4
1 Division of Social and Transcultural Psychiatry, McGill University and Culture and Mental Health Research Unit,Jewish General Hospital, Montreal, Canada
2 Department of Anthropology, McGill University, Montreal, Canada3 International Rehabilitation Council for Torture Survivors (IRCT), Copenhagen, Denmark4 Douglas Mental Health University Institute and Division of Social and Transcultural Psychiatry, McGill University,Montreal, Canada
13.1 INTRODUCTION
Trauma and disasters are important causes of humansuffering both in terms of the sheer numbers of peopleaffected and the complexity of the mental healthproblems that may follow. Violence has become oneof the leading causes of death worldwide for peopleaged 15–44 years [1]. Of the total number of globalinjury-related deaths, about two-thirds are of‘nonintentional’ origin (e.g. traffic accidents) whileone-third are due to intentional violence, includingsuicides, homicides and organized violence (terror-ism, wars and armed conflict, genocide and ethniccleansing) [2]. Both the frequency and the numbers ofpeople affected by violence and disasters have in-creased markedly over the last 100 years, while theproportion of people surviving has also risen [3]. Thismeans that there aremanymore survivors whomay beaffected psychologically by traumatic events. As thedensity of human habitation and the intensity of
technological development have increased, so too hasthe scale of disasters. Climate change, economicdisparities and political conflicts all can be expectedto compound the number and complexity of disastersin the years to come [4].
Social psychiatry has a long engagement withunderstanding the individual and collective impactsof trauma and disasters. Much of this interest has beendriven by experiences of the impact of war on soldiersand civilian populations [5]. The Holocaust and othergenocides have forced consideration of the effects ofmassive human rights violations on the survivors aswell as on subsequent generations. The experience ofrefugees has drawn attention to the impact of displa-cement, forcedmigration and torture onmental health.
Of course, trauma is not only a consequence ofsuch large-scale events but also a common occur-rence in domestic life. Early psychodynamic theory
Principles of Social Psychiatry, second edition Edited by Craig Morgan and Dinesh Bhugra! 2010 John Wiley & Sons, Ltd.
recognized the importance of childhood trauma as afactor in psychopathology, although this was largelydisplaced by an emphasis on intrapsychic conflict [6].From the 1970s onward, the recognition of the highprevalence of child abuse and its long-term conse-quences has given renewed impetus to the study oftrauma in psychiatry [7].
Research on the impact of natural disasters hasalso influenced the development of psychiatric the-ory and practice. Eric Lindemann’s study of theaftermath of the fire at the Coconut Grove nightclubemphasized the processes of normal grieving and thevalue of crisis intervention to reduce pathologicaloutcomes of trauma and loss [8]. His work led him
to establish the first community mental health centrein the US in 1948 [9]. Kai Erikson’s study of theBuffalo Creek flood in 1973 drew attention to thelong-term effects on wellbeing of the destruction ofcommunal bonds and connectedness [10]. In recentyears, disaster psychiatry and psychology haveemerged as distinct areas of study with textbooks,journals and societies devoted to research and dis-cussion of clinical and social issues [11]. Thisdevelopment of the field has brought recognitionthat trauma and disasters may be associated withparticular types of mental health problems requiringculturally informed interventions at both individualand community levels [12].
13.2 DEFINING AND DELIMITING TRAUMA AND DISASTER
Trauma is a term originally applied to physical injuryand some of its immediate effects. Since the late1800s, trauma has increasingly come to refer to arange of psychological impacts of the experience orthreat of violence, injury and loss [13]. Events that areconsidered traumatic include violent personal assault,rape, physical or sexual abuse, severe automobileaccidents, being diagnosed with a life-threateningillness, natural or technological disasters, being kid-napped, military combat, being taken hostage, terror-ist attacks, torture and incarceration as a prisoner ofwar or in a concentration camp. The term ‘trauma’emphasizes what is common across these differentevents, but clearly each has its own particular mean-ings and consequences.
Traumatic events vary widely in terms of the natureof the threat or injury, its frequency and duration, itspersonal significance (which may change over time),the relationship of the victim to the perpetrator (in thecase of interpersonal violence or abuse), and thebroader collective meaning and social response. Whatconstitutes a trauma then is not entirely dependent onthe nature of the event but also on the personal andsocial interpretation of the event and the responses ofthe affected person, their family and community, aswell as the wider society. Culture influences the in-dividual and collective experience of trauma at manylevels: the perception and interpretation of events asthreatening or traumatic; modes of expressing and
explaining distress; coping responses and adaptation;patterns of help-seeking and treatment response.Mostimportantly, culture gives meaning to the traumaticevent itself, allowing individuals, families and com-munities to make sense of violence and adversity inways that may moderate or amplify their impact.
Disasters are situations or events involving eco-logicaldisruption, threat to lifeor injury thatnegativelyaffect large numbers of people and that overwhelmlocal capacity for adaptation, usually by destroyinginfrastructure. Disasters vary widely in their scale,scope and significance. It is useful to distinguish be-tween natural and human-caused disasters. Naturaldisasters include geophysical and meteorologicalevents like earthquakes, floods, tsunamis, tornados,volcanoesanddrought.Human-causeddisasterscanbedivided into: (i) technological accidents, such as air-line or other mass transportation accidents, industrialaccidents and structural collapses of bridges or build-ings; and (ii) willful or intentional events such asmassmurders, terrorism, war and genocide. The distinctionbetween natural and human-caused, however, is oftendifficult to make and may change with new informa-tion and interpretations; for example, the destructionfollowing an earthquakemay become a human-causeddisaster when it is realized that most of the deaths aredue to the collapse of houses built with shoddy work-manship due to corruption in the constructionindustry. Many disasters span the natural and the
human-caused because they stem from the ways hu-mankind has modified the environment (e.g. faminedue to the interaction of methods of intensive agri-culture and drought). Natural and human-made dis-asters may co-occur and interact in ways difficult todisentangle. For example, drought or famine can becaused by warfare and warfare can be ignited by
famine. The frequent coexistence and mutual aggra-vation of natural and human-instigated disasters iscentral to the notion of complex emergency, defined asa catastrophic situation marked by the destruction of apopulation’s social, economic, and politicalinfrastructure [14,15].
13.3 UNDERSTANDING TRAUMA
From an evolutionary perspective human beings havelived with the threat of violence, injury and deaththroughout history. We might expect therefore thatthere are mechanisms available to help us adapt tothreats that do not destroy us [16]. The most commonresponse to mild or moderate levels of trauma is acutedistress followed rapidly by recovery. We are biolo-gically primed to learn to be fearful and avoidant ofpotentially life-threatening situations [17]. Whenthreats are more severe and inescapable, other me-chanisms come into play, including dissociation, acognitive and attentional process of blocking out orcompartmentalizingmemory and experience. This toomay have adaptive functions, allowing individuals tosurvive intolerable situations like torture or confine-ment, but it can also impair later adaptation.
Although trauma can aggravate any psychiatric con-dition, certain disorders are presumed to have a directcausal link to trauma exposure. In any traumatic event,some individuals will have more severe or incapacitat-ing acute symptoms and some will go on to havechronic distress and disability. Others may do wellinitially but manifest significant symptoms at a latertime. These pathological outcomes reflect both indivi-dual and social vulnerabilities. Among the problemsspecifically linked to trauma are grief and other normalforms of reactive distress, depressive and anxiety dis-orders, and post-traumatic stress disorder (PTSD).
Trauma exposure may result in a variety of short-and long-term adaptive and pathological responses.Common responses during or immediately after thetraumatic event include intense autonomic arousalassociated with fear, agitated behaviour or ‘freezing’,and dissociative symptoms with an altered sense oftime speeding up or slowing down, and feelings ofderealization and depersonalization [18]. About
15–20% of people exposed to such acute events havesymptoms and impairment lasting for several days orweeks [19]. Acute stress disorder (ASD), introducedin DSM-IV, occurs within the first 4 weeks of traumaexposure and is similar to PTSD but with prominentdissociative symptoms [20]. A severe acute stressresponse is a predictor of longer term distress, includ-ing PTSD [21].
DSM-IV-TR classifies PTSD as an anxiety disorderthat is characterized by the ‘re-experiencing of anextremely traumatic event accompanied by symptomsof increased arousal and by avoidance of stimuliassociated with the trauma’ ([20], p. 429). The essen-tial features of PTSD are the development of specificsymptoms following exposure to an event that involvedactual or threatened death, or serious injury, to whichthe person responded with ‘intense fear, helplessness,or horror’ (p. 463). In addition to the stressor criterionA, the criteria for PTSD include three main symptomclusters: (B) intrusive recollection– intrusive thoughts,distressing dreams, reliving or dissociative‘flashbacks’, psychological distress and physiologicalreactivity when exposed to reminders; (C) avoidant/numbing – efforts to avoid thoughts, feelings, con-versations or activities associated with the stressor,difficulty remembering the traumatic event, socialwithdrawal and emotional numbing; and (D) hyperar-ousal – sleep problems, irritability or angry outbursts,concentration problems, hypervigilance and an exag-gerated startle response. The diagnostic criteria forPTSD in ICD-10 are similar but do not include numb-ing and do not require functional impairment; thesedifferences result in higher prevalence rates for PTSDwith ICD-10 criteria [22].
PTSD has an explicit causal mechanism built intoits diagnostic criteria: exposure to an unexpected or
TRAUMA AND DISASTERS IN SOCIAL AND CULTURAL CONTEXT 157
unpredictable event that involves possible seriousinjury or death to oneself or others and leads toappraisal of the event as threatening and so to intensefear, helplessness, horror and other negative emotions(shame, guilt, anger); these in turn influence memoryand other cognitive-emotional-sensory processing ofthe event such that it leaves lasting traces in the brainand behaviour [23]. A major component of the syn-drome of PTSD is subserved by a conditioned emo-tional response of fear [17]. Reminders of the contextwhere threat originally occurred evoke anxiety andthis ismanaged by cognitive and behavioural efforts toavoid such contextual cues, resulting in emotionalnumbing and withdrawal.
Fear conditioning can be long lasting, but in theordinary course of events, repeated exposure tothe same cues without any fearsome outcome even-tually results in a decrease in conditioned fear, hyper-arousal and avoidance behaviour–a process called‘extinction’. It is now known that extinction involvesa type of learning distinct from fear conditioning,involving different neural pathways. In fact, the ori-ginal conditioned fear is not erased or replaced butsimply suppressed by extinction learning. The twotypes of learning have different characteristics; fearconditioning is quicker and generalizes more easilythan extinction learning. As a result, a small change inenvironmental cues can reinstate the originallylearned fear [24,25]. This helps to account for thephenomenon of triggering or reactivation of symp-toms in patients with PTSD [26].
These biological mechanisms are important forunderstanding the causes and chronicity of PTSD,the dynamics of triggering and re-experiencing, andthe effectiveness of exposure therapy as a treatment,but PTSD involves additional cognitive and beha-vioural responses mediated by forms of learning andmemory, as well as processes of recall and narrativeelaboration that are regulated by the personal meaningof the traumatic events [27]. Both recollection andnarration also involve social processes so that trau-matic outcomes reflect the culturally sanctioned occa-sions for remembering and forgetting [28].
The prevalence of PTSD in any population depends,in part, on rates of exposure to trauma which, in turn,depend on social circumstances [29]. Traumaticevents are common but unequally distributed in the
population. Surveys in the US have found 50–60% ofindividuals are exposed to a traumatic event at somepoint in their lives [30]. The likelihood of developingPTSD after a traumatic event varies with the type ofevent and the magnitude of the trauma, ranging from5 to 10% of those exposed to a natural disaster, to 20%of those exposed to criminal assault, 40% of thoseexposed to combat and more than 50% of thoseexposed to rape [30,31]. Women appear to have agreater risk of developing PTSD after trauma expo-sure, although this may partly reflect gender differ-ences in symptom expression [22].
PTSD was initially framed as a normal or at leastinevitable response to extreme circumstances. How-ever, longitudinal research soon clearly showed thatonly some individuals exposed to the same type ofseverely traumatic event develop PTSD and that pre-morbidpersonality andpsychopathologyare importantdeterminants of vulnerability. As most people whoshow transient symptoms resembling PTSD (heigh-tened arousal, anxiety, irritability, nightmares, intru-sive thoughts)will recover over a period of days,weeksor months (depending on the severity of the trauma),PTSD can beviewed a disorder of recovery [32].Meta-analyses of risk and protective factors for PTSD showthat among the strongest predictors of PTSD aftertrauma exposure are life stress and lack of socialsupport [33]. Thus, social factors determine the riskof exposure to trauma and the likelihood of recovery.These risk and recovery factors are related to eachother through the structures of family, community andwider social institutions. It is useful, therefore, to thinkof a social ecology of trauma risk and recovery [34].
Depression is also a common response in manysituations involving trauma, particularly when therehas been significant loss. The losses commonly asso-ciated with trauma and disasters may include loss ofloved ones and possessions, but also loss of status,role, home, community and the familiar routines ofeveryday life. The co-occurrence of depression andPTSD complicates the course of each disorder [35].
Somatic symptoms are common consequences oftrauma andmay reflect physiological dysregulation aswell as culturally shaped idioms of expression ofdistress [36,37]. For example, a study of Salvadoranwomen refugees in North America, who had fled ElSalvador to escape large-scale political violence,
found that the women described their suffering as‘nervios’, a cultural idiom that covered an array ofdysphoric emotions (anxiety, fear, anger) and diversesomatic complaints, including bodily pains, shaking,trembling and calor (sensations of heat). Althoughsome of the bodily symptoms that follow traumaexposure may be related to PTSD, panic disorder,
generalized anxiety disorder or depression, thereare other processes of physiological dysregu-lation, increased muscle tension and bodily preoccu-pation mediated by cognitive and social processesthat contribute to such ‘medically unexplained’symptoms [38].
13.4 DISASTERS
Disasters have health impacts at multiple levels, in-dividual (physiological, psychological), family, com-munity, societal, international and global. The socialimpact of disasters reflects theirmagnitude, the level ofpre-existing infrastructure, level of infrastructure pre-served, the meaning of events (human-caused or not);the response of the community and local population;the response of government and larger society; and theinternational response. The impact of most disasters ismore severe in developing countries, which lack re-sources and infrastructure to respond adequately.
Although awhole population or communitymay beexposed to a disaster, people are affected differently.The psychological impact of a disaster on any givenindividual depends on both the personal and collectivesignificance of and response to the catastrophic event.Groups recognized to be at particular risk for mentalhealth consequences includewomen (especially preg-nant women, single mothers, widows) and children.Internally displaced people, refugees and others pre-viously exposed to trauma are also at increased risk forpsychological re-traumatization. In general, peoplewith pre-existing mental health problems, includingdepression and anxiety, are especially vulnerable [39].
The prevalence of psychiatric morbidity followinga disaster is associated with its magnitude but alsowith the level of perceived threat to life and risk ofrecurrence, lack of predictability and controllability,loss, injury, exposure to the dead and grotesque, andthe extent of destruction of community infrastruc-ture [40]. Estimates of PTSD following a disasterrange from 30 to 40% among those directly exposedto 10–20% for rescue workers and 5–10% for thegeneral population [29]. Symptoms of depression anddemoralization are strongly related to the degree ofloss experienced as a result of the disaster [41].
Disasters are associated with increased levels ofmedically unexplained somatic symptoms bothacutely and over survivors’ life spans [42].
Disasters lead to psychiatric morbidity throughmany pathways: physical injury, exposure to terrifyingevents, loss of loved ones, loss of employment, liveli-hood and income, loss of familiar environment, do-mestic and communal place. These losses and injuriesinteract with other social determinants of health in-cluding pre-existing social structural and politicalproblems. For the same amount of loss and physicaldamage, human-made disasters may have more severepsychological consequences owing to the ways theyundermine basic social emotions of trust and solidarity.
There are three broad approaches to the impact oftrauma and disaster on mental health outcomes. Theclinical psychiatric approach focuses on the effects oftrauma in causing psychopathological conditions likePTSD, depression and other potentially disablingconditions. Individual vulnerability due to pre-exist-ing personality traits, coping styles and mental healthproblems help predict who will develop persistentproblems after trauma exposure.
A second approach focuses on individuals’ re-sources and resilience. For example, conservation ofresources (COR) theory, developed by Hobfoll,groups resources into four broad categories: objectresources (e.g. material possessions with either func-tional utility or symbolic value); condition resources(e.g. social roles or status like marriage, employment,membership in groups or organizations); personalcharacteristic resources (e.g. values, traits or attitudeslike optimism, sense of meaning and purpose); andenergy resources (e.g. time,money, information) [43].Resource loss due to trauma is associated with dis-tress [44]. Disasters produce distress and limit coping
TRAUMA AND DISASTERS IN SOCIAL AND CULTURAL CONTEXT 159
by reducing individuals’ resources in each of theseareas. Coping and adaptation, therefore, can be im-proved by interventions that maximize these re-sources. Of course these resource domains are notindependent but correlated in ways that reflect acommunity’s social structure and dynamics.
A third approach recognizes the dynamic nature ofthe interaction between different resource domainsand focuses on the role of social positioning in in-dividual and group vulnerability and resilience. Thismore dynamic view could be termed ‘socialecological’, in that it sees each person as locatedwithin a system that has its own dynamics. Disastersdiffer from isolated traumatic events affecting indi-viduals in that they affect thewhole community,whichordinarily provides the secure base for each person’sadaptive responses to stress, trauma and loss. Depend-ing on the degree towhich a disaster disrupts the socialfabric and weakens bonds between people, commu-nities may respond with mobilization and increasedsolidarity or with demoralization, disorganization anddisintegration. The level of psychiatric distress in thepopulation plays a role in these social responses, butthey have their own dynamics that reflect local his-tories and systemic issues of politics, identity andcommunity. These local systemic dynamics are em-bedded in larger global economic and political re-sponses that influence the mental health outcomes ofdisasters.
In the face of a disaster that seems to come from‘outside’ and that does not destroy too much infra-structure, communities may pull together and experi-ence a high degree of solidarity. For example, inJanuary 1998, Quebec experienced an ice storm inwhich the accumulation of ice brought down the mainpower transmission lines into the city of Montreal,leaving 3 million people without electricity in themidst of winter. Despite the challenge posed by thisloss of power and cold temperatures, there was anenhanced sense of comradery among neighbours, whoheated water for coffee over camping stoves andhuddled around battery-operated radios waiting fornews. There was no increase in use of mental healthservices by patients with severe mental illness [45].However, even during this relatively limited event,with little social disruption or loss of life, many peopleexperienced high levels of stress with potential long-
term sequelae. For example, there is evidence for aneffect of maternal stress during the ice storm on thesubsequent cognitive development of their infantswho were exposed in utero [46].
At the other extreme in terms of the magnitudedisaster, in Sri Lanka following the tsunami of26 December 2004, there was massive loss of life anddestruction of entire settlements and villages alongtwo-thirds of the country’s coast. This occurredagainst a backdrop of political violence that hadaffected the country for decades, eroding family sta-bility and community solidarity [47]. A survey in oneseverely affected area found that 40% of the popula-tion had mild to moderate symptoms of depression,anxiety or PTSD [48]. Another survey of childrenliving in three tsunami affected areas found rates ofPTSD that were not related to the tsunami of4.6–8.5%, while tsunami related PTSD was found inan additional 13.9–38.8% [49]. Another study ofadolescents from two villages in southern Sri Lankafound that post-tsunami depressive and PTSD symp-toms were associated with prolonged displacement,social losses, family losses and their mothers’ level ofmental health problems [50]. A positive mother–childrelationship had a protective effect.
Generally, human-caused disasters result in morepsychiatric morbidity than those that are attributed tonatural events [51]. When events can be attributed tospecific individuals or groups, fear and anger may bedirected towards them. When the human causesare harder to identify, emotional distress may bemore diffuse and anger may be harder to resolve,with greater risk for long-term mental healthconsequences.
Disasters due to terrorism are a dramatic illustrationof these factors both because terrorist acts are directlycaused by individual agency and because they delib-erately aim to maximize the anxiety, insecurity, help-lessness and vulnerability of a population [52]. In thewake of the attacks of 11 September 2001, high levelsof symptomatology were reported not only amongthose directly affected at the ground zero, or living inthe city of New York, but across the country. A surveyimmediately following the attacks found that 44% ofadults had one or more ‘substantial’ symptoms ofdistress [53]; two months later this dropped to16% [54]. New categories of trauma emerged, like
vicarious PTSD incurred while watching repetitiveTVimages of the attacks [55]. The threat of recurrencebecame an ongoing preoccupation, contributing to anew sense of collective vulnerability.
Of course, the distinction between ‘natural’ cata-strophes like earthquakes, tsunami, hurricanes andhuman-caused catastrophes like industrial accidents,war or terrorism depends on specific ways of inter-preting events. Some people in the US believe thatgovernment should control the forces of nature; hencenatural disasters can be blamed on human error ormalfeasance [56]. From some religious or culturalperspectives, all events may have moral meaning aspart of causal chains that include human or spiritualagency (like karma, sin or divine judgement). Contra-riwise, peoplemay view even events caused by humanagency as preordained or following an impersonallogic. Thus, in the Cambodian genocides perpetratedby the Khmer Rouge, many people interpreted thecatastrophe as following from their individual kamma(karma) and so felt a measure of responsibility fortheir own misfortune [57]. This attribution mutes theexternal expression of anger and desire for revenge
and urges the survivor to follow a morally uprightpath. On the other hand, karma implies an ultimatemoral order that would ensure that the perpetrators ofthe atrocities will pay for their actions in futuremiserable rebirths. Political circumstances also maylimit any possibilities to name perpetrators and seekjustice or redress.
Even events that seem to be entirely natural exerttheir effects unequally on a population in ways thatreveal pre-existing social inequalities and injustices.In recent earthquakes, the pattern of destruction hasreflected economic disparities and corruption asthose with substandard housing, built by ‘cuttingcorners’, were most affected. The flooding of NewOrleans due to hurricane Katrina had differentialeffects on the poor and marginalized that reflectedthe long history of racial discrimination [58]. Thus anatural disaster laid bare the structural violence ofsociety. This social meaning has both material andmoral consequences, influencing who finds safehaven and looks forward to rebuilding their life andwho endures prolonged displacement, neglect anddespair.
13.5 TECHNOLOGICAL DISASTERS
Urbanization and industrialization have brought withthem many benefits but also new types of collectivevulnerability. Mass transportation has created thepotential for accidents that affect hundreds of peoplein an instant. New technologies have created newtypes of disaster with unique characteristics that fol-low from their unique physical properties. For exam-ple, the release of radioactivity from the Chernobyldisaster had long-term and long-range effects with anincrease in cancer and other radiation-related dis-eases [39]. The petrochemical disaster in Bhopalresulted in an enormous range of respiratory, ocular,gastrointestinal and other conditions [59]. In bothcases, there were also long-term psychological effectson the exposed populations, with persistent feelings ofanxiety, depression and medically unexplainedsymptoms.
Independent of actual exposure, the conviction thatone has been exposed to toxic chemicals or radiationmay be a risk factor for long-term psychological
distress, even among those who emigrate from thesite of disaster [60]. Those who are evacuated may beat increased risk for mental health problems owing tothe disruption of their lives. However, those whoremain in the vicinity of an industrial accident mayface the greatest challenge. In the case of the ThreeMile Island nuclear reactor accident, people whocontinued to live near the reactor reported feeling lesscontrol over their lives and thiswas associated, in turn,with higher levels of somatic, anxiety and depressivesymptoms even years after the event [61].
The legal and political meaning of technologicaldisasters may bring vulnerable populations into directconflict with powerful commercial interests. Techno-logical disasters may be viewed as accidents due torisks inherent in a useful technology or as stemmingfrom human errors, action or inaction. To the extentthey are viewed as due to human action, there is alwayssome person or corporate entity to blame. However,largecorporationsoftenare able todeflect the efforts of
TRAUMA AND DISASTERS IN SOCIAL AND CULTURAL CONTEXT 161
individuals or groups to seek redress. Ongoing litiga-tion and struggle over restitution from those respon-sible for the catastrophes can greatly complicate theprospects for recovery, as illustrated by the protractedstruggles over compensation following the ExxonValdez oil spill [62]. The spill disrupted fishing activ-
ities, creating severeeconomichardship,but thosewhowere plaintiffs in the civil suit suffered greater levels ofstress over the course of the litigation. The persistentangerassociatedwithperceivedinjustices thathavenotbeen acknowledged or redressed contributes to long-term distress following technological disasters [63].
13.6 WAR AND POLITICAL VIOLENCE
Ethnic conflict, organized violence and wars havebeenmajor causes of suffering, ill health andmortalitythroughout history [2]. In recent decades, the numberof victims and survivors of traumatic events hassignificantly increased as war, armed conflict andpolitical upheaval have engulfed civilian populationsworldwide, contributing to additional burden of dis-ease, death and disability. War has always exposedboth combatants and civilians to trauma but, with theadoption of newmethods ofwarfare, recent years haveseen a dramatic increase in the proportion of civiliancasualties. During World War II, about 50% of thedirect casualties were civilians; in the 1980s this figurerose to 80% and by 1990 it was fully 90%, with thelargest number being women and children [64].
War and political conflicts have structural causesand often occur in societies that are already facingeconomic hardship. The collapse of formal economiesand the emergence of economic crises in the marginalareas of the global economy lead to further impover-ishment, food insecurity and ethnic and religioustensions over diminishing resources. Consequently,predatory practices, rivalry, political violence andinternal wars may erupt [65]. In the last 60 years therehave been over 200wars and armed conflicts, in whichthemain targets are often the poorest sectors of societyand marginalized ethnic groups.
Armed conflict results in significant psychiatricmorbidity but the pattern varies across cultures. In astudy of 3048 respondents in Algeria, Cambodia,
Eritrean refugees in Ethiopia and Gaza in Palestine,de Jong, Komproe and Van Ommeren compared ratesof depression, anxiety disorders, PTSD and somato-form disorders among those exposed to armed-con-flict-associated violence and those without such ex-posure [66]. Overall, PTSD was the most commondisorder for those directly exposed to violence, whileanxiety disorders were the most common disorder forthose not directly exposed. There were high levels ofcomorbidity of PTSD with anxiety or mood disordersin Algeria and Cambodia. However, there was alsosubstantial variation in the overall prevalence andrelative rates of disorders, which was due not only tothe nature or severity of the disorder but to culturalvariations in modes of expression of distress. Forexample, in Cambodia, anxiety disorders were morecommon than PTSD among those exposed to vio-lence. Somatoform disorders were more commonamong those exposed to violence only in the Palestinesample.
The health consequences of political violence andwars extend beyond death, disease and trauma-relatedpsychiatric illness, to include the pervasive effects ofdestruction of the economic and social institutions andthewhole fabric of society. As such, the consequencesof violent conflict can be observed not only in in-dividuals – in their biographies and life trajectories –but also in collective memory and identity and com-munal strategies for coping with violence andadversity [65,67].
13.7 REFUGEES
Refugees fleeing war or persecution are very vulner-able as they cannot count on protection from their ownstate, and it is often their own government that is
responsible for threatening and persecuting them. The1951 Refugee Convention defines a refugee as some-one who ‘owing to a well-founded fear of being
persecuted for reasons of race, religion, nationality,membership of a particular social group, or politicaloption, is outside the country of his nationality, and isunable to or, owing to such fear, is unwilling to availhimself of the protection of that country’ [68]. TheRefugee Convention obligates governments to pro-vide a safe haven for those fleeing persecution. How-ever, many countries treat refugee claimants withsuspicion and have policies aimed at discouragingothers from seeking asylum [69]. These policies ofdeterrence, which may include detention under harshconditions, have serious mental health effects [70].
Epidemiological studies have demonstrated bothshort- and long-term effects of trauma on refugeemental health and disability. For example, a surveyof Vietnamese refugees who resettled in Australiafound that 8% of the participants had mental disor-ders [71]. Trauma exposure was the strongest pre-dictor of mental health status. Although the risk of amental disorder decreased over time, people whosufferedmore than three traumatic events had a higherrisk of mental illness after 10 years compared withpeople with no traumatic exposure. A longitudinalstudy of Bosnian refugees found that fully 45% metDSM-IV criteria for depression, PTSD or both [72].
Ameta-analysis of 56 reports published from1959 to2002, representing 22 221 refugees, found that mentalhealth status was worse among those living in institu-tional accommodation, with restricted economic op-portunity, internally displaced, repatriated to a countrythey had fled or with unresolved conflicts in theircountry of origin [73]. A study of 1348 refugees from
Vietnam and Laos who were resettled in Canada afterhaving lived in refugee camps for a variable period oftime, found that although chronic strain (such as flight,internment and resettlement) was a major risk formental health problems, post-migration factors, includ-ing support fromtheethnic communityand theprospectfor integration in the receiving society, were crucialdeterminants of outcome [74]. For refugee children aswell as for adults, the quality of their post-migrationreception in the new country is a better predictor thanpre-migration trauma exposure of mental health [75].
Survivors of political violence, persecution or tor-ture, whomust flee their countries of origin to survive,suffer complex losses and transitions associated withforced migration, the process of seeking asylum andthe enduring dilemmas of exile [69]. The process ofconvincing immigration authorities that one has beentortured and so has a valid claim to refugee status mayin itself become a situation of psychological retrau-matization [69,76,77]. Thismay be exacerbated by thefact that such individuals may be reluctant to divulgeexperiences like torture, rape or other forms of traumain health care settings. Refugees also may have con-tinuing fears for the safety of family left behind anduncertainty about the possibility of reuniting withloved ones. Despite the profound impact of traumaon wellbeing, post-migration factors including socialsupports, employment and occupational status areamong the strongest predictors of positive out-come [73,74,78]. Effective resettlement policies andprogrammes can therefore make a significant contri-bution to refugee mental health.
13.8 TORTURE
Torture constitutes an extreme form of trauma inwhichthe perpetrator actively seeks not only to threaten thevictimwithpain, injuryordeathbutalso todehumanize,control, humiliate and oppress the victim, and throughthem, a whole community [79]. Despite internationalefforts to prevent torture as a human rights violation, itcontinues to be practised by many countries [80]. Theattackon theWorldTradeCentreon11September2001led to an increase in torture practices when manycountries joined the so-called ‘war on terror’, using thesloganof‘protectingpublicsecurity’ to justify theuseof
torture to extract information – human rights violationsinwhich health care professionals took part [81–84]. Inreality, torture yields unreliable information and is usedprimarilyasatool forrepressingpoliticaloppositionandinstillingfear in thecommunityandsocietyat large.Thepoliticaluseof torturehasacorrosiveeffectonthemoralorder of a society and constitutes an important obstacleto the development of democratic institutions and uni-versal human rights [85].
Compared to other forms of trauma or naturaldisasters, torture constitutes a profound violation of
TRAUMA AND DISASTERS IN SOCIAL AND CULTURAL CONTEXT 163
personal integrity and dignity because it underminesthe moral basis of human relatedness and community.Perpetrators create a situation of extreme powerless-ness, uncertainty and loss of control in their victims,but the effects of torture spread far beyond the im-mediate victim to include fragmentation of family andcommunity networks through the spread of fear andmistrust, and the erosion of social and politicalsolidarity [86–90].
Torture involves awide range ofmethods of physicaland psychological abusewith diverse consequences forsurvivors.Rape and related forms of sexual torture haveespecially severe effects for bothmen and women [91].Survivors who had strong political convictions andwere prepared for the possibility of being tortured dueto their activism generally fare better than those forwhom the torture was arbitrary or unrelated to theirconvictions [92,93]. Many forms of torture leave vic-tims with profound feelings of shame, guilt and dis-grace because of the powerlessness, degradation andhumiliation they have experienced, and this may im-pede help-seeking [94,95]. Individuals who must con-tinue to live in proximity to the perpetrators of violenceand torture must suppress or ‘manage’ their feelings tomaintain the social order [96,97].
Common sequelae of torture include symptoms ofanxiety, depression and symptoms of acute stressdisorder with dissociative symptoms [98]. Post-trau-matic stress disorder (PTSD) is very common amongsurvivors and its likelihood increases with the severityof the torture [83,93,99]. Other common symptomsthat may occur with PTSD or independently include:chronic pain, sexual dysfunction, phobias, night-mares, memory impairment, social withdrawal, diffi-culty maintaining intimate or long-term relationships,and psychotic-like symptoms including ideas of re-
ference and superstitious thinking. Chronic pain mayreflect neuropathic damage from torture, links be-tween bodily sensations of memories of torture, pro-cesses of somatic amplification due to psychologicaldistress and culturally shaped idioms of distress thatencourage a focus on the body [100–102].
Feelings of violation, anger and injustice, while notalways correlated with PTSD or another psycho-pathology, may constitute significant clinical pro-blems in their own right [103]. The anger and aggres-sion that survivors often experience as a consequenceof their torture experiences may be displaced on toother people, particularly their families. Even whenthere is no overt conflict or abuse within the family,children may be strongly affected by the suffering oftheir parents and the community. For example, Puna-maki, Qouta and El Sarraj found that exposure totraumatic events increased Palestinian children’s po-litical activities and psychological adjustmentproblems’ – both effects were independent of thequality of perceived parenting [104]. Rehabilitationinterventions therefore must be extended to includethe families and communities of the victims.
Treatment of survivors of torture requires a broadperspective onmental health that encompasses family,community and the politics of social integration.Community-based approaches have become increas-ingly accepted as an integral part of treatment. Thismodel calls for a broader role for health professionalsas advocates and facilitators whowork collaborativelywith other nonmedical professionals from law, media,community development and human rights to promoteempowerment as survivors are assisted to help them-selves. The focus of rehabilitation is on strengthsrather than weaknesses, resilience rather than vulner-ability, health not disease.
13.9 GENOCIDE
TheUnited Nations Convention on the Prevention andPunishment of the Crime of Genocide (CPPCS),defines genocide as:
. . . any of the following acts committed with intent todestroy, in whole or in part, a national, ethnical, racialor religious group, as such: killing members of the
group; causing serious bodily or mental harm tomembers of the group; deliberately inflicting on thegroup conditions of life, calculated to bring about itsphysical destruction in whole or in part; imposingmeasures intended to prevent births within the group;[and] forcibly transferring children of the group toanother group.
The Holocaust and other genocides (e.g. in Rwa-nada, Bosnia–Herzegovina, Darfur) have starkly pre-sented the immediate and transgenerational effects ofmassive human rights violations and the systematicdestruction of communities [105]. Despite recogni-tion of these catastrophes, there has been a tragic lackof political will in the international community tointervene in ways that could prevent or mitigate theloss of life.
Clearly genocide, involving violence on a massivescale, can have severe effects on survivors’ mentalhealth. A study of four communities affected by thegenocide in Rwanda found the prevalence of PTSDsymptoms depended on traumatic exposure and variedfrom12.2 to 33.8% [106].A study of refugee survivorsof the genocide in Bosnia-Herzegovina who resettledin Australia found no differences in PTSD risk for thegroup most exposed to human rights violations (in-ternment in concentration camps, torture) comparedto the general war-exposed group [107]. Exposure to athreat to life predicted PTSD, while both threat to lifeand traumatic loss were associated with symptomseverity and disability.
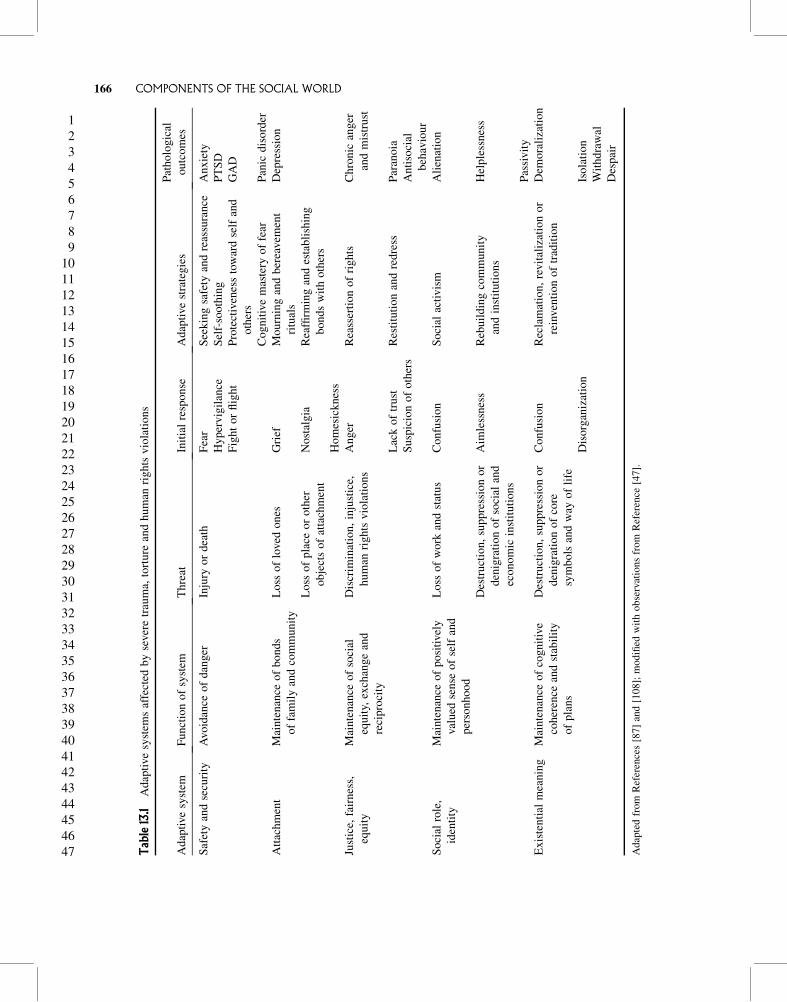
Mass human rights violations such as those thatoccur in situations of political violence, ethnic cleans-ing or genocide have effects at many levels. At thelevel of the individual, Silove has described theseeffects in terms of different adaptive systems, includ-ing systems involved in safety, attachment, sense ofjustice or fairness, existential meaning and social roleor identity [87,108]. Each of these biosocial systemsgives rises to specific forms of distress in response tospecific types of threat or loss (Table 13.1). There are avariety of psychological and social adaptive responsesthat aim to re-establish the normal functioning orequilibrium of the system and when those fail, parti-cular forms of psychopathology may result. Interven-tion strategies can be viewed as acting to restore theseadaptive functions. These same mechanisms operatein other forms of trauma and disasters to varyingdegrees.
There has been much interest in the possibility oftransgenerational transmission of trauma in the con-text of genocide [109,110]. Clearly, however, theexperience of the second and third generation is notprecisely the same as the first and the pathways oftransmission point also to a transformation in the
nature of suffering. A parent who has endured greattrauma in a concentration camp may react in manyways: with irritability, distraction or overprotective-ness. Each of these will have different effects on thechild, all of which might be attributed to the parent’strauma. In most cases, these are not PTSD but pro-blems in adjustment, anxiety, interpersonal relation-ships and so on.
Yehuda and colleagues examined transgenera-tional trauma in a group of adult offspring of Holo-caust survivors and a demographically similar com-parison group [111]. Although adult offspring ofHolocaust survivors did not experience more trau-matic events, they had a greater prevalence of currentand lifetime PTSD and other psychiatric diagnosesthan the demographically similar comparison sub-jects. The findings demonstrate an increased vulner-ability to PTSD and other psychiatric disordersamong offspring of Holocaust survivors, thus iden-tifying adult offspring as a possible high-risk groupwithin which to explore the individual differencesthat constitute risk factors for PTSD. Other studieshave little evidence of increased psychopathology inthe second- and third-generation children of Holo-caust survivors [112].
Individual stories of trauma serve to ground col-lective identity and call for a moral and politicalresponse. The appropriation of trauma to stabilize acollective identity may have benefits for the indivi-dual. Theremust be a public place for stories of traumafor them to be told, acknowledged and legitimated.Collective identity, history and legal mechanisms canplay a role in creating this place. Transgenerationallinks may serve psychological and political functions,becoming a central theme in the individual’s identityand a basis for the political aspirations of a group oreven a nation [113].
For example, for indigenous peoples in NorthAmerica, current mental health problems prevalentin some communities have come to be seen as theconsequence of historical trauma following fromEuropean colonization of the Americas and subse-quent policies of forced assimilation [114,115]. Theeffort to survive as a people when a whole way of lifehas been undermined and dismantled poses specialsocial, moral and psychological challenges that arenot captured by constructs like PTSD [116,117].
Current clinical guidelines for the treatment of traumaemphasize cognitive behavioural therapy, exposuretherapy and the treatment of comorbidity (most oftendepression, anxiety disorders, substance use) [118].There is some evidence for the effectiveness of trau-ma-focused psychotherapeutic interventions for indi-viduals with persistent trauma-related symptoms orPTSD [119].
Prolonged exposure therapy aims to allow extinc-tion of conditioned emotional responses of fear. Cog-nitive behaviour therapy works more broadly tochange modes of interpreting and responding totrauma cues, reduce catastrophizing thoughts andreinforce adaptive coping. Narrative exposure therapyinvolves a blend of approaches and can be used withboth children and adults across cultures [120–122]. Itinvolves constructing a life narrative than includes areview of traumatic experiences, revisiting the asso-ciated emotions and bodily feelings to allow habitua-tion to the physiological arousal; the process of narra-tion gives the trauma memories and experiencesstructure through retelling and composing a writtentestimony.
Although antidepressants and othermedications arewidely used, there is little evidence for the effective-ness of pharmacotherapy in the treatment of PTSD ortrauma-related disorders [123]. Treatment is usuallysymptomatic, to improve sleep, control pain and treatconcomitant depression and anxiety. Beta-blockershave been used to reduce autonomic arousal. Thereis intriguing evidence that the use of propranololduring a guided process of trauma recall can diminishemotional arousal on subsequent recollection withoutthe presence of the medication [124]. This raises theprospect that it may be possible to decouple traumamemory from some of its distressing and disablingphysical effects.
There is increasing recognition of the need to con-sider mental health issues in disaster relief. The 2004guidelines produced by the Sphere Project, whichinvolved a global consultation process to establishminimum standards for humanitarian response, covermental health for the first time [125]. There is an
emerging consensus on best practices in disaster man-agement, although the evidence base is limited [126].The WHO Report on ‘Mental Health in Emergencies’and the Inter-Agency Standing Committee (IASC)emphasize that it is crucial to protect and improvepeople’s mental health and psycho- social wellbeing inthe midst of an emergency through (a) psychologicalfirst aid provided by a variety of community workersfor people experiencing acute trauma-induced distressand (b) care by trained and supervised health staff forpeople with severe mental disorders, including severePTSD [127,128]. The principles of psychological firstaid include: maintaining a calm presence, providing asafe and comfortable setting, stabilizing emotionallyoverwhelmed survivors, gathering information aboutcurrent needs and concerns, providing practical assis-tance, giving information about common psychologi-cal reactions and appropriate coping strategies, andlinking the individual with local services and sourcesof further help. Humanitarian aid workers and com-munity leaders need training in the basic psychologicalskills required to provide psychological first aid, emo-tional support and recognition of common mentalhealth problems that should be referred to pro-fessionals [129].
Despite the consensus on best practices in an initialdisaster response, there are still many questions aboutappropriate interventions. The interventions offered indisaster situations are diverse and include materialsupport (shelter, food, clothing), psychoeducation,psychological debriefing, cognitive behavioural ther-apy (CBT), narrative exposure therapy, eyemovementdesensitization and reprocessing (EMDR) and com-munity-based interventions. CBT and narrative expo-sure therapy have been shown to be helpful forindividuals with trauma-related PTSD [122,130], andcommunity-based approaches that work towardsstrengthening social supports and reintegration mayfit better in some cultural contexts [131]. However,there is a lack of strong evidence for any specifictreatment.
Although exposure therapy has proven effective forisolated discrete traumas, it remains uncertain
TRAUMA AND DISASTERS IN SOCIAL AND CULTURAL CONTEXT 167
whether it is equally effective for those exposed tomultiple, repetitive or pervasive trauma like that seenin survivors of torture or genocide [132,133]. There islittle evidence that psychoeducational approaches canhelp prevent post-traumatic disorder or other types ofpsychological distress [134].While theremay be otherbenefits from existing interventions, and they maywork for some individuals or groups, more work isneeded to identify effective prevention strategies.
Psychological debriefing, which until recently wasa popular intervention, is no longer recommended.Debriefing is based on the assumption that retellingthe trauma story provides emotional release, relearn-ing and cognitive reorganization. One influential ver-sion was developed as a group intervention in the US,as a support method for fire fighters [135]. This was awork group of professionals who knew each other,who were exposed to similar traumatic events, weretrained to respond to disasters and remained con-nected to a larger stable social environment. All ofthese contextual elements may not be present whenthe method is applied in other settings: the peopleaffected may have been thrown together by the events,they may have experienced very different levels andtypes of threat and loss, they may face a profoundlydisrupted social environment and theymay come froma cultural background that does not encourage openexpression of private feelings or potentially shamefulevents. Even in the US, there is evidence that theintense re-exposure that may occur in psychologicaldebriefing can retraumatize some individuals.
The funding and delivery of humanitarian aid isincreasingly organized on an international level tofacilitate faster and more effective responses to major
emergencies affecting large numbers of people. As aresult, however, disaster scenes may be inundated bymental health professionals and other disaster workerswho further strain local resources and inadvertentlycontribute to the problems rather than to their solution.
There is agreement that post-disaster strategiesmust address the broad impact of disasters, promotinga sense of safety, calming, self- and collective efficacy,feelings of connectedness and hope [136]. Translatingthese general goals into specific interventions, how-ever, requires consideration of individual and com-munity psychology, an ecosocial perspective andawareness of local social, economic and politicalconstraints and cultural meaning systems. Culturalissues have been only minimally integrated into cur-rent disaster guidelines [137].
Cultural issues raise important considerations in thepractical response to disaster that may have mentalhealth consequences. Efforts to rebuild infrastructurethat do not sufficiently consider the social and culturalcontext may have negative effects on post-disasteradaptation. Following the 2004 tsunami, large quan-tities of aid poured into severalAsian countries (in partbecause foreigners saw the tsunami as a blamelessmisfortune) and communities pulled together to con-front and copewith adversities [138]. In Sri Lanka, forexample, the aid was used to reconstruct housing inways that have proved problematic for some commu-nities. Fishermen were moved inland and resettled inhouses built without the accustomed level of privacy,organization of interior space and ability to accom-modate extended family [139]. Lack of attention tocultural context undermined the effectiveness of thiswell-intentioned support.
13.11 CONTINUING CONTROVERSIES
In addition to the unresolved questions abouttreatment efficacy, there are broader controversiesin the field of trauma and disaster mental health,concerning the cross-cultural applicability and uti-lity of the diagnosis of PTSD; the value of testi-mony or explicit talk about trauma versus contain-ment; and the role of Truth and ReconciliationCommissions or other forms of restorative justicein recovery.
The construct of PTSD has been valuable for focus-ing attention on one specific form of anxiety response,but limited in terms of the wide range of impacts andthe importance of other personal and social factors inproducing resilient outcomes or prolonged sufferingand pathology. The field of trauma and disaster psy-chiatry is far wider than the compass of PTSD.
Although the symptoms of PTSD can be identifiedacross cultures, its clinical and social relevance
remain contentious. Structured diagnostic interviewsand self-report scales based on the diagnostic criteriafor PTSD have been translated into local languages,permitting investigators to distinguish trauma-relateddisorders from similar kinds of psychological distress.Other scales are available to assess the level of traumaexposure and trauma-related symptomatology [140].These include the Harvard Trauma Questionnaire(HTQ) and measures for assessing anxiety and de-pression [141]. These instruments can be adapted tonew cultural groups, though problems of clinical andcultural validity remain [142]. However, symptomstend to be nonspecific indicators of distress and, inthemselves, do not demonstrate the presence of adiscrete disorder of clinical significance. Measures offunctional impairment are essential to define a thresh-old for disorder warranting clinical attention.
Critics argue that mainstream approaches to diag-nosis and treatment overlook the extent to whichtrauma experience is culture-specific. The Westerndiscourse on trauma is embedded in a particularcultural and moral framework and becomes proble-matic in other cultural contexts [143]. Personal, po-litical, social and cultural factors mediate the experi-ence of war or other forms of violence. Practitionersunfamiliar with the local culture and situation applygeneric assessment tools and interventions that forceindividuals into a limited repertoire of categories andresponses [144]. People are encouraged to understandtheir suffering through the prism of individualisticpsychological models that may not fit local values andconcepts of the person [145]. As well, the dominanceof the PTSDmodel tends to suppress other approachesand silence local perspectives on what is helpful andimportant in the wake of a disaster.
The distress and suffering that accompany war orother forms of collective violence are not necessarilypathological responses to traumatic events, butmay benormal responses to existential predicaments [146].Such suffering is resolved in a social context throughfamilial, sociocultural, religious and economic activ-ities that make the world comprehensible for peoplebefore, during and after catastrophes [14,147].The roots of recovery from trauma and disaster lie inthe restoration of the functional social environment,i.e. through improved living conditions, activities,employment, a stable community and social order.
On this view, instead of offering psychological coun-selling, humanitarian aid programmes should ac-knowledge resilience and retain the social rehabilita-tion frameworks, starting with the strengthening ofdamaged local capacities in line with localpriorities [148].
A related controversy concerns the appropriatestrategy for dealing with severe trauma of the sortfound among refugees and survivors of torture. Whilesome approaches to rehabilitation of survivors oftorture, genocide or other human rights violationsemphasize the importance of giving testimony, thismay not fit well with all social, cultural or religiouscontexts. Thevalue of testimonyhas been embraced inLatin America and taken up by the InternationalRehabilitation Council for Torture Victims in Copen-hagen [149]. However, many Asian traditions empha-size the values of equanimity and containment andmay view the open airing of suffering as unhealthy anddisruptive to the social order. Political and mentalhealth goals then come into conflict with social normsand cultural values and the implications of this fortrauma outcomes remain uncertain. Part of the benefitin telling one’s story comes from giving it a coherentframe, part comes from having a sympathetic otherperson bear witness and part comes from the largersocial–historical process of recording a personal andcollective truth. However, all of these depend to someextent on the social reception of the testimony. Furtherwork is needed to understand the tradeoffs involved inspeaking out or remaining silent in specific social,cultural and political contexts [150,151].
The functions of testimony have taken on newdimensions in the context of Truth and ReconciliationCommissions like that of South Africa, which aim torestore justice andmoral order to a community rent bylongstanding political violence and injustice. This, inturn, has raised questions about the socialmechanismsfor reconciliation and forgiveness that hope to repairboth the justice and existential systems by ensuringpublic acknowledgement of past human rights viola-tions and providing a healing ritual that brings someclosure to otherwise unassimilable events. The meta-phor of the psychological wound and the notion ofhealing have governed the truth and reconciliationprocess. However, this is an inaccurate or incompletemodel of the complex psychological and social
TRAUMA AND DISASTERS IN SOCIAL AND CULTURAL CONTEXT 169
processes put into play; the process involves issues ofjustice, equity and safety as well as woundedness andwholeness [152].
The ability of victims and their families to partici-pate in legal proceedings or other public means ofholding perpetrators accountable may provide com-fort for them; it may also act as an effective tool for theprevention of torture [153]. In some instances, how-ever, the truth and reconciliation process can beharmful to participants. Individuals who already havePTSD may benefit little and may have their traumaticmemories activated and experience an exacerbation of
their condition [154]. The public, ‘quasi-legal’ con-text of the Truth and Reconciliation Commission maybe threatening to some people and destabilizing for acommunity. Mental health practitioners have a role toplay to ensure that the process of recounting does notcause further damage. This may involve helping todesign a setting and procedure that is therapeutic (e.g.by giving control to the narrator) and supportingindividuals participating in Commission hear-ings [155]. Other forms of restorative justice basedon traditional methods of conflict resolution facesimilar challenges when applied to mass violence.
13.12 CONCLUSION
Trauma has become a dominant trope in discussions ofthe contemporary world [156]. Like any metaphor itreveals and it conceals. What the metaphor of traumareveals is the supervenient effects of extreme violenceon suffering. Even healthy people can be torn downand permanently marked by the most severe forms ofviolence. Yet the response of most people, even toserious trauma, is resilience and recovery.
A social and cultural perspective suggests that itis crucial for clinicians to understand traumaticevents and disasters in their broader social, eco-nomic and political context. These politics shapethe production of psychiatric knowledge about trau-ma, the personal social and cultural contexts thatare singled out for clinical attention, the ways thatprofessionals and institutions apply trauma diag-noses and treatment, the dynamics of social supportand the processes of conflict resolution. Althoughviolence always has very personal impacts, it isclear that states, international organizations, globaleconomic institutions and mass media are all in-volved in the creation, maintenance and resolutionof the conflicts that lead to structural, interpersonaland mass violence [157]. Suffering is fundamentallya social experience in several ways: it involves aninterpersonal engagement with pain and hardshiplived in intimate and communal social relationships;it is framed in terms of available cultural models ofthe nature of adversity and corresponding appro-priate moral responses; and it is part of professionaldiscourses of medicine and the mental health pro-
fessions that organize forms of suffering asbureaucratic categories and objects of technicalintervention [158].
Understanding stories of trauma requires an un-derstanding of the collective dimensions of violenceand social suffering. Trauma experience is em-bedded in and emerges from multiple contexts,including biological processes of learning and mem-ory; embodied experiences of injury, pain and fear;narratives of personal biography; the knowledge andpractices of cultural and social systems; and thepower and positioning of political struggles enactedon individual, family, community and nationallevels [27].
The language of trauma, however, tends to draw asimple arc from the violent event through the psycho-logical processes of the individual (where they mayexhibit resilience or vulnerability) to bodily symp-toms of affliction. In reality, the events we call traumaare part of larger configurations of suffering that havetheir own social ecology and political economy. Dis-crete trauma and disasters occur against a backdrop ofstructural violence that renders some groups andindividuals far more vulnerable; focusing exclusivelyon the trauma may deflect attention from these en-during forms of disadvantage – in some instance,however, a catastrophe may throw these into starkrelief as was seen, for example, with hurricane Ka-trina. It is important for mental health practitionersand psychiatric researchers to appreciate these largersocial contexts of suffering. Without such awareness,
we risk becoming part of the machinery that deflectsattention from social inequalities and structural vio-lence on to individuals’ psychology.
The war on terror, global warming and the press ofhumanity seeking to escape political violence andnatural catastrophes all make the problems of traumaand disaster important issues in contemporary psy-chiatry. We need a body of research that takes socialand cultural context carefully into consideration andclinical approaches that address the real concerns ofindividuals, families and communities responding tothe range of challenges brought by trauma and disasterin all their myriad forms.
REFERENCES
1. Krug, E. G., Dahlberg, L. L., Mercy, J. A. et al. (2002)World Report on Violence and Health, World HealthOrganizaton, Geneva. Available from: http://www.who.int/violence_injury_prevention/violence/world_ report/en/.
2. Murray, C. J. L., King, G., Lopez, A. D. et al. (2002)Armed conflict as a public health problem. BritishMedical Journal, 324 (7333), 346–349.
3. Center for Research on the Epidemiology of Disasters(2009) EM-DAT: Emergency Events Database, Uni-versit!e Catholique de Louvain – Ecole de Sant!e, Pub-lique, Louvain, Belgium [cited 16 April 2009]. Avail-able from: http://www.emdat.be/Database/terms.html.
4. McMichael, A. J.,Woodruff, R. E. andHales, S. (2006)Climate change and human health: present and futurerisks. Lancet, 367 (9513), 859–869.
5. Young, A. (1995) The Harmony of Illusions: InventingPosttraumatic Stress Disorder, Princeton UniversityPress, Princeton, New Jersey.
6. van der Kolk, B. A., Herron, N. and Hostetler, A.(1994) The history of trauma in psychiatry. PediatricClinics of North America, 17 (3), 583–600.
7. Hacking, I. (1995) Rewriting the Soul, Princeton Uni-versity Press, Princeton, New Jersey.
8. Lindemann, E. (1944) Symptomatology and manage-ment of acute grief. American Journal of Psychiatry,101, 141–148.
9. Dixon, L. and Goldman, H. (2004) Forty years ofprogress in community mental health: the role ofevidence-based practices. Administration and Policyin Mental Health, 31 (5), 381–392.
10. Erikson, K. T. (1976) Loss of communality at BuffaloCreek. American Journal of Psychiatry, 133 (3),303–305.
11. Ursano, R. J. (2007) Textbook of Disaster Psychiatry,Cambridge University Press, Cambridge, New York.
12. Marsella, A. J. (2008) Ethnocultural Perspectives onDisasters and Trauma: Foundations, Issues, andApplications, Springer, New York.
13. Leys, R. (2000) Trauma: A Genealogy, University ofChicago Press, Chicago, Illinois.
14. Almedom, A. M. and Summerfield, D. (2004) Mentalwell-being in settings of ‘complex emergency’: a re-view. Journal of Biosocial Science, 36 (04), 381–388.
15. Mollica, R. F., Cardozo, B. L., Osofsky, H. J. et al.(2004)Mental health in complex emergencies.Lancet,364 (9450), 2058–2067.
16. Konner, M. (2007) Trauma, adaptation, and resilience:a cross-cultural and evolutionary perspective, in Un-derstanding Trauma: Biological, Psychological andCultural Perspectives (eds L. J. Kirmayer, R. Lemel-son and M. Barad), Cambridge University Press, NewYork, pp. 300–338.
17. Rau, V. and Fanselow, M. S. (2007) Neurobiologicaland neuroethological perspectives on fear and anxiety,in Understanding Trauma: Integrating Biological,Clinical, and Cultural Perspectives (eds L. J. Kir-mayer, R. Lemelson and M. Barad), Cambridge Uni-versity Press, New York, pp. 27–40.
18. Cardena, E. and Spiegel, D. (1993) Dissociative reac-tions to the San Francisco Bay earthquake of 1989.American Journal of Psychiatry, 150 (3), 474–478.
19. Brewin, C. R., Andrews, B., Rose, S. and Kirk, M.(1999) Acute stress disorder and posttraumatic stressdisorder in victims of violent crime.American Journalof Psychiatry, 156 (3), 360–366.
20. American Psychiatric Association (2000) Diagnosticand Statistical Manual of Mental Disorders: DSM-IV-TR, 4th edn, American Psychiatric Association,Washington, DC.
21. Brewin, C. R., Andrews, B. and Rose, S. (2003)Diagnostic overlap between acute stress disorder andPTSD invictims of violent crime.American Journal ofPsychiatry, 160 (4), 783–785.
22. Peters,L.,Issakidis,C.,Slade,T.andAndrews,G.(2006)Gender differences in the prevalence of DSM-IV andICD-10 PTSD. Psychological Medicine, 36 (1), 81–89.
23. Brewin, C. R. and Holmes, E. A. (2003) Psychologicaltheories of posttraumatic stress disorder. Clinical Psy-chology Review, 23 (3), 339–376.
TRAUMA AND DISASTERS IN SOCIAL AND CULTURAL CONTEXT 171
24. Quirk, G. J., Milad, M. R., Santini, E. and Lebron, K.(2007) Learning not to fear: a neural sustems approach,in Understanding Trauma: Integrating Biological,Clinical, and Cultural Perspectives (eds L. J. Kir-mayer, R. Lemelson and M. Barad), Cambridge Uni-versity Press, New York, pp. 60–77.
25. Barad, M. and Cain, C. K. (2007) Mechanisms of fearextinction: toward improved treatment for anxiety, inUnderstanding Trauma: Integrating Biological, Clin-ical, and Cultural Perspectives (eds L. J. Kirmayer, R.Lemelson andM.Barad), CambridgeUniversity Press,New York, pp. 78–97.
26. Bouton, M. E. and Wadell, J. (2007) Some biobeha-vioral insights into persistent effects of emotionaltrauma, in Understanding Trauma: Integrating Bio-logical, Clinical, and Cultural Perspectives (eds L. J.Kirmayer, R. Lemelson and M. Barad), CambridgeUniversity Press, New York, pp. 41–59.
27. Lemelson, R., Kirmayer, L. and Barad, M. (2007)Trauma in context: integrating cultural, clinical andbiological perspectives, in Understanding Trauma:Integrating Biological, Clinical, and Cultural Per-spectives (eds L. J. Kirmayer, R. Lemelson and M.Barad), Cambridge University Press, New York,pp. 451–474.
28. Kirmayer, L. J. (1996) Landscapes of memory: trau-ma, narrative and dissociation, in Tense Past: CulturalEssays on Memory and Trauma (eds P. Antze and M.Lambek), Routledge, London, pp. 173–198.
29. Galea, S., Nandi, A. and Vlahov, D. (2005) Theepidemiology of post-traumatic stress disorder afterdisasters. Epidemiologic Reviews, 27, 78–91.
30. Kessler, R. C., Sonnega, A., Bromet, E. et al. (1995)Posttraumatic stress disorder in the National Comor-bidity Survey.Archives ofGeneral Psychiatry, 52 (12),1048–1060.
31. Breslau, N., Kessler, R. C., Chilcoat, H.D. et al. (1998)Trauma and posttraumatic stress disorder in the com-munity: the 1996 Detroit Area Survey of Trauma.Archives of General Psychiatry, 55 (7), 626–632.
32. Shalev, A. (2007) PTSD: a disorder of recovery? inUnderstanding Trauma: Biological, Psychologicaland Cultural Perspectives (eds L. J. Kirmayer, R.Lemelson andM.Barad), CambridgeUniversity Press,New York, pp. 207–223.
33. Brewin, C. R., Andrews, B. and Valentine, J. D. (2000)Meta-analysis of risk factors for posttraumatic stressdisorder in trauma-exposed adults. Journal of Con-sulting and Clinical Psychology, 68 (5), 748–766.
34. Charuvastra, A. and Cloitre, M. (2008) Social bondsand posttraumatic stress disorder. Annual Review ofPsychology, 59, 301–328.
35. Momartin, S., Silove, D., Manicavasagar, V. and Steel,Z. (2004) Comorbidity of PTSD and depression: as-sociations with trauma exposure, symptom severityand functional impairment in Bosnian refugees re-settled in Australia. Journal of Affective Disorders,80 (2–3), 231–238.
36. Kirmayer, L. J. (1996) Confusion of the senses: im-plications of ethnocultural variations in somatoformand dissociative disorders for PTSD, in EthnoculturalAspects of Post-Traumatic Stress Disorders: Issues,Research and Clinical Applications (eds A. J. Marsel-la, M. J. Friedman, E. T. Gerrity and R. M. Scurfield),American Psychological Association, Washington,DC, pp. 131–164.
37. Groleau, D. and Kirmayer, L. J. (2004) Sociosomatictheory in Vietnamese immigrants’ narratives of dis-tress. Anthropology and Medicine, 11 (2), 117–133.
38. Kirmayer, L. J. and Young, A. (1998) Culture andsomatization: clinical, epidemiological, and ethno-graphic perspectives. Psychosomatic Medicine, 60(4), 420–430.
39. Bromet, E. J. andHavenaar, J.M. (2002)Mental healthconsequences of disasters, in Psychiaty in Society (edsN. Sartorius, W. Gaebel, J. J. Lopez-Ibor and M. Maj),John Wiley & Sons, Inc., New York, pp. 241–261.
40. Davidson, J. R. andMcFarlane, A.C. (2006) The extentand impact of mental health problems after disaster.Journal of Clinical Psychiatry, 67 (suppl. 2), 9–14.
41. Arata, C.M., Picou, J. S., Johnson, G. D. andMcNally,T. S. (2000) Coping with technological disaster: anapplication of the conservation of resources model tothe Exxon Valdez oil spill. Journal of TraumaticStress, 13 (1), 23–39.
42. van den Berg, B., Grievink, L., Yzermans, J. andLebret, E. (2005) Medically unexplained physicalsymptoms in the aftermath of disasters. EpidemiologicReviews, 27, 92–106.
43. Hobfoll, S. E. (1989)Conservation of resources. Anewattempt at conceptualizing stress. American Psychol-ogist, 44 (3), 513–524.
44. Hobfoll, S. E., Tracy, M. and Galea, S. (2006) Theimpact of resource loss and traumatic growth onprobable PTSD and depression following terroristattacks. Journal of Traumatic Stress, 19 (6), 867–878.
45. McMurray, L. and Steiner, W. (2000) Natural disastersand service delivery to individuals with severe mental
illness – ice storm. Canadian Journal of Psychiatry –Revue Canadienne De Psychiatrie, 45 (4), (1998)383–385.
46. Laplante, D. P., Brunet, A., Schmitz, N. et al. (2008)Project Ice Storm: prenatal maternal stress affectscognitive and linguistic functioning in 5 1/2-year-oldchildren. Journal of the American Academy of Childand Adolescent Psychiatry, 47 (9), 1063–1072.
47. Somasundaram, D. (2007) Collective trauma in north-ern Sri Lanka: a qualitative psychosocial–ecologicalstudy. International Journal of Mental Health Sys-tems, 1 (1), 5.
48. Hollifield, M., Hewage, C., Gunawardena, C. N. et al.(2008) Symptoms and coping in Sri Lanka 20–21months after the 2004 tsunami. British Journal ofPsychiatry, 192 (1), 39–44.
49. Neuner, F., Schauer, E., Catani, C. et al. (2006) Post-tsunami stress: a study of posttraumatic stress disorderin children living in three severely affected regions inSri Lanka. Journal of Traumatic Stress, 19 (3),339–347.
50. Wickrama,K. A. andKaspar, V. (2007) Family contextof mental health risk in tsunami-exposed adolescents:findings from a pilot study in Sri Lanka. Social Scienceand Medicine, 64 (3), 713–723.
51. Norris, F. H., Friedman, M. J., Watson, P. J. et al.(2002) 60,000 disaster victims speak: Part I. An em-pirical review of the empirical literature, 1981–2001.Psychiatry, 65 (3), 207–239.
52. Alexander, D. A. and Klein, S. (2003) Biochemicalterrorism: too awful to contemplate, too serious toignore: subjective literature review. British Journal ofPsychiatry, 183, 491–497.
53. Schuster,M. A., Stein, B. D., Jaycox, L. et al. (2001) Anational survey of stress reactions after the September11, 2001, terrorist attacks. New England Journal ofMedicine, 345 (20), 1507–1512.
54. Stein, B.D., Elliott,M.N., Jaycox, L.H. et al. (2004)Anational longitudinal study of the psychological con-sequences of the September 11, 2001, terrorist attacks:reactions, impairment, and help-seeking. Psychiatry,67 (2), 105–117.
55. Blanchard, E. B., Kuhn, E., Rowell, D. L. et al. (2004)Studies of the vicarious traumatization of collegestudents by the September 11th attacks: effects ofproximity, exposure and connectedness. BehaviourResearch and Therapy, 42, 191–205.
56. Blocker, T. J. and Sherkat, D. E. (1992) In the eyes ofthe beholder: technological and naturalistic interpreta-
tions of a disaster. Industiral Crisis Quarterly, 6,153–166.
57. Hinton,A. L. (2005)WhyDid TheyKill?: Cambodia inthe Shadow of Genocide, University of CaliforniaPress, Berkeley, California.
58. Galea, S., Brewin, C. R., Gruber, M. et al. (2007)Exposure to hurricane-related stressors and mentalillness after hurricane Katrina. Archives of GeneralPsychiatry, 64 (12), 1427–1434.
59. Pastel, R. H. (2007) What have we learned aboutmass chemical disasters? Psychiatric Annals, 37(11), 754–765.
60. Foster, R. P. and Goldstein, M. F. (2007) Chernobyldisaster sequelae in recent immigrants to the UnitedStates from the former Soviet Union (FSU). Journal ofImmigrant and Minority Health, 9 (2), 115–124.
61. Davidson, L. M., Baum, A. and Collins, D. L. (1982)Stress and control-related problems at Three MileIsland. Journal of Applied Social Psychology, 12(5), 349–359.
62. Picou, J. S., Marshall, B. K. and Gill, D. A. (2004)Disaster, litigation, and the corrosive community.Social Forces, 82 (4), 1493–1522.
63. Solomon, M. J. and Thompson, J. (1995) Anger andblame in three technological disasters. Stress Medi-cine, 11, 199–206.
64. Turpin, J. (1998)Many faces: women confrontingwar,in The Women and War Reader (eds L. A. Lorentzenand J. Turpin), New York University Press, New Yorkand London, pp. 3–18.
65. Pedersen, D. (2002) Political violence, ethnic conflict,and contemporary wars: broad implications for healthand social well-being. Social Science and Medicine,55, 175–190.
66. de Jong, J. T., Komproe, I. H. and Van Ommeren, M.(2003) Common mental disorders in postconflict set-tings. Lancet, 361 (9375), 2128–2130.
67. Pedersen, D. andKienzler, H. (2008) Ethnic conflict, inEncyclopedia of PublicHealth (ed. K. Heggenhougen),Academic Press, San Diego, California, pp. 508–518.
68. UNHCR (1992) Handbook on Procedures and Cri-teria for Determining Refugee Status under the 1951Convention and the 1967 Protocol Relating to theStatus of Refugees, United Nations High Commissionon Refugees, Geneva, Contract No.: June 23.
69. Silove, D., Steel, Z. and Watters, C. (2000) Policies ofdeterrence and the mental health of asylum seekers.Journal of the AmericanMedical Association, 284 (5),604–611.
TRAUMA AND DISASTERS IN SOCIAL AND CULTURAL CONTEXT 173
70. Silove, D., Austin, P. and Steel, Z. (2007) No refugefrom terror: the impact of detention on the mentalhealth of trauma-affected refugees seeking asylumin Australia. Transcultural Psychiatry, 44 (3),359–393.
71. Steel, Z., Silove, D., Phan, T. and Bauman, A. (2002)Long-term effect of psychological trauma on themental health of Vietnamese refugees resettled inAustralia: a population-based study. Lancet, 360(9339), 1056–1062.
72. Mollica, R. F., Caridad, K. R. and Massagli, M. P.(2007) Longitudinal study of posttraumatic stressdisorder, depression, and changes in traumatic mem-ories over time in Bosnian refugees. Journal of Ner-vous and Mental Disease, 195 (7), 572–579.
73. Porter,M. andHaslam,N. (2005) Predisplacement andpostdisplacement factors associated with mentalhealth of refugees and internally displaced persons:a meta-analysis. Journal of the American MedicalAssociation, 294 (5), 602–612.
74. Beiser, M. (2006) Longitudinal research to promoteeffective refugee resettlement. Transcultural Psychia-try, 43 (1), 56–71.
75. Montgomery, E. (2008) Long-term effects of organizedviolence on young Middle Eastern refugees’ mentalhealth. Social Science and Medicine, 67 (10),1596–1603.
76. Rousseau, C., Cr!epeau, F., Foxen, P. and Houle, F.(2002) The complexity of determining refugeehood: amultidisciplinary analysis of the decision-making pro-cess of the Canadian Immigration and Refugee Board.Journal of Refugee Studies, 15 (1), 43–70.
77. Kirmayer, L. J. (2007) Failures of imagination: therefugee’s predicament, in Understanding Trauma:Biological, Psychological and Cultural Perspectives(eds L. J. Kirmayer, R. Lemelson and M. Barad),Cambridge University Press, New York, pp. 363–381.
78. Carlsson, J. M., Olsen, D. R., Mortensen, E. L. andKastrup, M. (2006) Mental health and health-relatedquality of life: a 10-year follow-up of tortured refu-gees. Journal of Nervous and Mental Disease, 194(10), 725–731.
79. United Nations (1989) United Nations ConventionAgainst Torture and Other Cruel, Inhuman or Degrad-ing Treatment or Punishment. New York: United Na-tions, Contract No.: GARes. 39/46, 39 GAORSupple-ment (No. 51) at 197, UN Document A/39/51, openedfor signature 4 February 1985, entered into force 26June 1987.
80. Stern, S. (2007) Torture debates.Global Researcher, 1(9), 211–236.
81. Lewis, A. (2004) Making torture legal. New YorkReview of Books, 51 (12), 4–8.
82. Clark, P. A. (2006)Medical ethics at Guantanamo Bayand Abu Ghraib: the problem of dual loyalty. Journalof Law Medicine and Ethics, 34 (3), 570–580, 481.
83. Basoglu, M., Livanou, M. and Crnobaric, C. (2007)Torture vs other cruel, inhuman, and degrading treat-ment: is the distinction real or apparent? Archives ofGeneral Psychiatry, 64 (3), 277–285.
84. Danner, M. (2009) The Red Cross torture report: whatit means. New York Review of Books, 56 (7), April 30,http://www.nybooks.com/articles/22614.
85. Afana, A. H. (2007) Torture. International Review ofRed Cross, 89 (867), 505–514.
86. Jaranson, J. and Popkin, M. (eds) (1998) Caring forVictims of Torture, American Psychiatric Press, Inc.,Washington, DC.
87. Silove, D. (1999) The psychosocial effects of torture,mass human rights violations, and refugee trauma:toward an integrated conceptual framework. Journalof Nervous and Mental Disease, 187 (4), 200–207.
88. Kagee,A. andNaidoo,A.V. (2004)Reconceptualizingthe sequelae of political torture: limitations of a psy-chiatric paradigm. Transcultural Psychiatry, 41 (1),46–61.
89. Kira, I. A., Templin, T., Lewandowski, L. et al. (2006)The effects of torture: two community studies. Peaceand Conflict: Journal of Peace Psychology, 12 (3),205–228.
90. Campbell, T. A. (2007) Psychological assessment,diagnosis, and treatment of torture survivors: a review.Clinical Psychology Review, 27 (5), 628–641.
91. Loncar,M.,Medved, V., Jovanovic, N. andHotujac, L.(2006) Psychological consequences of rape onwomen in 1991–1995 war in Croatia and Bosniaand Herzegovina. Croatian Medical Journal, 47 (1),67–75.
92. Basoglu, M., Mineka, S., Paker, M. et al. (1997)Psychological preparedness for trauma as a protectivefactor in survivors of torture. Psychological Medicine,27 (6), 1421–1433.
93. Johnson, H. and Thompson, A. (2008) The develop-ment and maintenance of post-traumatic stress disor-der (PTSD) in civilian adult survivors of war traumaand torture: a review. Clinical Psychology Review, 28(1), 36–47.
94. Wilson, J. P. and Drozdek, B. (2004) Broken Spirits:The Treatment of Traumatized Asylum Seekers, Re-fugees,War, and Torture Victims, Brunner-Routledge,New York.
95. Moreno, A., Piwowarczyk, L., LaMorte, W. W. andGrodin,M. A. (2006) Characteristics and utilization ofprimary care services in a torture rehabilitation center.Journal of Immigrant and Minority Health, 8 (2),163–171.
96. Bagilishya, D. (2000) Mourning and recovery fromtrauma: in Rwanda, tears flow within. TransculturalPsychiatry, 37 (3), 337–354.
97. Lemelson, R., Kirmayer, L. J. and Barad, M. (2007)Trauma in context: integrating cultural, clinical, andbiological perspectives, in Understanding Trauma:Biological, Psychological and Cultural Perspectives(eds L. J. Kirmayer, R. Lemelson and M. Barad),Cambridge University Press, New York, pp. 451–474.
98. Turner, S. andGorstunsworth, C. (1990) Psychologicalsequelae of torture. British Journal of Psychiatry, 157,475–480.
99. Mollica, R. F., McInnes, K., Pham, T. et al. (1998) Thedose-effect relationships between torture and psychia-tric symptoms in Vietnamese ex-political detaineesand a comparison group. Journal of Nervous andMental Disease, 186 (9), 543–553.
100. Thomsen, A. B., Eriksen, J. and Smidt-Nielsen, K.(2000) Chronic pain in torture survivors. ForensicScience International, 108 (3), 155–163.
101. Kirmayer, L. J. (2002) The refugee’s predicament.L’Evolution Psychiatrique, 67, 724–742.
102. Olsen, D. R., Montgomery, E., Carlsson, J. and Fold-spang, A. (2006) Prevalent pain and pain level amongtorture survivors: a follow-up study. Danish MedicalBulletin, 53 (2), 210–214.
103. Basoglu, M., Livanou, M., Crnobaric, C. et al. (2005)Psychiatric and cognitive effects of war in formerYugoslavia: association of lack of redress for traumaand posttraumatic stress reactions. Journal of theAmerican Medical Association, 294 (5), 580–590.
104. Punamaki, R.-L., Qouta, S. and El Sarraj, E. (1997)Relationships between traumatic events, children’sgender, and political activity, and perceptions of par-enting styles. International Journal of BehavioralDevelopment, 21 (1), 91–109.
105. Power, S. (2002) A Problem from Hell: America andthe Age of Genocide, Basic Books, New York.
106. Pham, P. N.,Weinstein, H.M. and Longman, T. (2004)Trauma and PTSD symptoms in Rwanda: implications
for attitudes toward justice and reconciliation. Journalof the American Medical Association, 292 (5),602–612.
107. Momartin, S., Silove, D., Manicavasagar, V. and Steel,D. (2003) Dimensions of trauma associated with post-traumatic stress disorder (PTSD) caseness, severityand functional impairment: a study of Bosnian refu-gees resettled in Australia. Social Science and Medi-cine, 57, 775–781.
108. Silove, D. (2007) Adaptation, ecosocial safety signals,and the trajectory of PTSD, inUnderstanding Trauma:Biological, Psychological and Cultural Perspectives(eds L. J. Kirmayer, R. Lemelson and M. Barad),Cambridge University Press, New York, pp. 242–258.
109. Danieli, Y. (1998) International Handbook of Multi-generational Legacies of Trauma, Plenum Press,New York.
110. Kellermann, N. P. (2001) Transmission of Holocausttrauma–an integrative view. Psychiatry, 64 (3),256–267.
111. Yehuda, R., Schmeidler, J., Wainberg, M. et al. (1998)Vulnerability to posttraumatic stress disorder in adultoffspring of Holocaust survivors. American Journal ofPsychiatry, 155, 1163–1171.
112. Sigal, J. J. (1998) Long-term effects of the Holocaust:empirical evidence for resilience in the first, second,and third generations. Psychoanalytic Review, 85 (4),579–585.
113. Kidron, C. A. (2004) Surviving a distant past: a casestudy of the cultural construction of trauma descendantidentity. Ethos, 31 (4), 513–544.
114. Brave Heart, M. Y. H. (2004) The historical traumaresponse among Natives and its relationship withsubstance abuse: a Lakota illustration, in Healing andMental Health for Native Americans (eds E. Nebelkofand B. M. Phillips), Altamira Press, Walnut Creek,California, pp. 7–18.
115. Whitbeck, L. B., Adams, G. W., Hoyt, D. R. andChen, X. (2004) Conceptualizing and measuring his-torical trauma among American Indian people. Amer-ican Journal of Community Psychology, 33 (3–4),119–130.
116. Lear, J. (2006) Radical Hope: Ethics in the Face ofCulturalDevastation, HarvardUniversity Press, Cam-bridge, Massachusetts.
117. Gone, J. P. and Kirmayer, L. J. (in press) On theWisdom of Considering Culture and Context in Psy-chopathology, inContemporaryDirections in Psycho-pathology: Toward the DSM-V and ICD-11 (eds T.
TRAUMA AND DISASTERS IN SOCIAL AND CULTURAL CONTEXT 175
laurencekirmayer
Millon, R. F. Krueger and E. Simonsen), Guilford,New York.
118. National Institute for Clinical Excellence (2005) TheManagement of Post Traumatic Stress Disorder inPrimary and Secondary Care, NICE, London.
119. Institute of Medicine (IOM) (2008) Treatment ofPosttraumatic Stress Disorder: An Assessment of theEvidence, National Academies Press, Washington,DC.
120. Neuner, F., Schauer, M., Klaschik, C. and Elbert, T.(2004) A comparison of narrative exposure therapy,supportive counseling, and psychoeducation for treat-ing posttraumatic stress disorder in an African refugeesettlement. Journal of Consulting and Clinical Psy-chology, 72 (4), 579–587.
121. Schauer, M., Elbert, T. and Neuner, F. (2005) Narra-tive Exposure Therapy: A Short-Term Intervention forTraumatic Stress Disorders After War, Terror, orTorture, Hogrefe & Huber, Toronto.
122. Bichescu, D., Neuner, F., Schauer, M. and Elbert, T.(2007) Narrative exposure therapy for political im-prisonment-related chronic posttraumatic stress dis-order and depression. Behaviour Research andTherapy, 45 (9), 2212–2220.
123. American Psychiatric Association (2004) Practiceguideline for the treatment of patients with acute stressdisorder and posttraumatic stress disorder. AmericanJournal of Psychiatry, 161 (Suppl. 11), 3–31.
124. Brunet, A., Orr, S. P., Tremblay, J. et al. (2008) Effectof post-retrieval propranolol on psychophysiologicresponding during subsequent script-driven traumaticimagery in post-traumatic stress disorder. Journal ofPsychiatric Research, 42 (6), 503–506.
125. Sphere Project (2004) Humanitarian Charter andMinimum Standards in Disaster Response, SphereProject, Geneva.
126. van Ommeren,M., Saxena, S. and Saraceno, B. (2005)Mental and social health during and after acute emer-gencies – emerging consensus? Bulletin of the WorldHealth Organization, 83 (1), 71–77.
127. World Health Organization (2003) Mental Health inEmergencies: Mental and Social Aspects of Health ofPopulations Exposed to Extreme Stressors, WorldHealth Organization, Geneva.
128. Inter-Agency Standing Committee (2007) IASCGuidelines on Mental Health and Psychosocial Sup-port in Emergency Settings, Inter-Agency StandingCommittee, Geneva.
129. Eisenman, D., Weine, S., Green, B. et al. (2006) TheISTSS/Rand guidelines on mental health training ofprimary healthcare providers for trauma-exposed po-pulations in conflict-affected countries. Journal ofTraumatic Stress, 19 (1), 5–17.
130. Schwarz-Langer, G., Deighton, R. R., Jerg-Bretzke, L.et al. (2006) Psychiatric treatment for extremelytraumatized civilwar refugees from formerYugoslavia.Possibilities and limitations of integrating psycho-therapy and medication. Torture, 16 (2), 69–80.
131. Stepakoff, S., Hubbard, J., Katoh, M. et al. (2006)Trauma healing in refugee camps in Guinea: a psy-chosocial program for Liberian and Sierra Leoneansurvivors of torture and war. American Psychologist,61 (8), 921–932.
132. Basoglu, M. (2006) Rehabilitation of traumatisedrefugees and survivors of torture. British MedicalJournal, 333 (7581), 1230–1231.
133. Kinzie, D. (2007) PTSD among traumatized refugees,in Understanding Trauma: Biological, Psychologicaland Cultural Perspectives (eds L. J. Kirmayer, R.Lemelson and M. Barad), Cambridge UniversityPress, New York, pp. 194–206.
134. Wessely, S., Bryant, R. A., Greenberg, N. et al. (2008)Does psychoeducation help prevent post traumaticpsychological distress? Psychiatry, 71 (4), 287–302.
135. Parker, I. (2004) Victims and volunteers. The NewYorker, 26, 50–61.
136. Hobfoll, S. E.,Watson, P., Bell, C. C. et al. (2007) Fiveessential elements of immediate and mid-term masstrauma intervention: empirical evidence. Psychiatry,70 (4), 283–315, discussion 6–69.
137. Batniji, R., VanOmmeren,M. and Saraceno, B. (2006)Mental and social health in disasters: relating quali-tative social science research and the Sphere Standard.Social Science and Medicine, 62 (8), 1853–1864.
138. Ghodse, H. and Galea, S. (2006) Tsunami: under-standing mental health consequences and the unpre-cedented response. International Review of Psychiatry(Abingdon, England), 18 (3), 289–297.
139. Peoples Rural Development Association (PRDA)(2008)Mental Health and Wellbeing of CommunitiesAffected byConflcit and Tsunami in Sri Lanka, PRDA,Colombo, August 23.
140. Hollifield, M., Warner, T. D., Lian, N. et al. (2002)Measuring trauma and health status in refugees: acritical review. Journal of the American MedicalAssociation, 288 (5), 611–621.
141. Mollica, R. F., Caspi-Yavin, Y., Bollini, P. et al. (1992)The Harvard Trauma Questionnaire. Validating across-cultural instrument for measuring torture, trau-ma, and posttraumatic stress disorder in Indochineserefugees. Journal of Nervous andMental Disease, 180(2), 111–116.
142. Shoeb, M., Weinstein, H. and Mollica, R. (2007) TheHarvard Trauma Questionnaire: adapting a cross-cultural instrument for measuring torture, trauma andposttraumatic stress disorder in Iraqi refugees. Inter-national Journal of Social Psychiatry, 53 (5),447–463.
143. Kienzler, H. (2008) Debating war-trauma and post-traumatic stress disorder (PTSD) in an interdisciplinaryarena. Social Science and Medicine, 67 (2), 218–227.
144. Atlani, L. and Rousseau, C. (2000) The politics ofculture in humanitarian aid to refugees having experi-enced sexual violence. Transcultural Psychiatry, 37(3), 435–449.
145. Kirmayer, L. J. (1989) Psychotherapy and the culturalconcept of the person. Sant!e, Culture, Health, 6 (3),241–270.
146. Summerfield,D. (2004)Cross-cultural perspectives onthe medicalization of human suffering, in Posttrau-matic Stress Disorder: Issues and Controversies (ed.G. Rosen), John Wiley & Sons, Ltd, Chichester, WestSussex, and Hoboken, New Jersey, pp. 233–245.
147. Jones, L. (2004) Then they started shooting, in Grow-ing up in Wartime Bosnia, Harvard University Press,Cambridge, Massachusetts.
148. Summerfield, D. (2000) Conflict and health: war andmental health: a brief overview. British Medical Jour-nal, 321 (7255), 232–235.
149. Cienfuegos, A. J. and Monelli, C. (1983) The testi-mony of political repression as a therapeutic instru-ment. American Journal of Orthopsychiatry, 53 (1),43–51.
150. Weine, S. M., Kulenovic, A. D., Pavkovic, I. andGibbons, R. (1998) Testimony psychotherapy inBosnian refugees: a pilot study. American Journal ofPsychiatry, 155, 1720–1726.
151. Lustig, S. L.,Weine, S. M., Saxe, G. N. and Beardslee,W. R. (2004) Testimonial psychotherapy for adoles-cent refugees: a case series. Transcultural Psychiatry,41 (1), 31–45.
152. Avruch, K. (in press) Truth and reconciliation com-missions: problems in transitional justice and thereconstruction of identity. Transcultural Psychiatry,47 (1).
153. Allan, A., Allan, M. M., Kaminer, D. and Stein, D. J.(2006) Exploration of the association between apologyand forgiveness amongst victims of human rightsviolations. Behavioral Sciences and the Law, 24 (1),87–102.
154. Kaminer, D., Stein, D. J., Mbanga, I. and Zungu-Dirwayi, N. (2001) The Truth and ReconciliationCommission in South Africa: relation to psychiatricstatus and forgiveness among survivors of humanrights abuses. British Journal of Psychiatry, 178,373–377.
155. Silove, D., Zwi, A. B. and le Touze, D. (2006) Do truthcommissions heal? The East Timor experience. Lan-cet, 367 (9518), 1222–1224.
156. Fassin, D. and Rechtman, R. (2009) The Empire ofTrauma: An Inquiry into the Condition of Victimhood,Princeton University Press, Princeton, New Jersey.
157. Das, V. and Kleinman, A. (2000) Introduction, inViolence and Subjectivity (eds V. Das, A. Kleinman,M. Ramphele and P. Reynolds), University ofCalifornia Press, Berkeley, California, pp. 1–18.
158. Kleinman, A., Das, V. and Lock, M. (eds) (1997)Social Suffering, University of California Press,Berkeley, California.