56
Elisa R. Zanier Trauma cranico: Fisiopatologia e strategie terapeutiche

Elisa R. Zanier
Trauma cranico: Fisiopatologia e strategie terapeutiche
• Epidemiology
• Pathophysiology
•Heterogeneity
•Susceptibility
•Chronic degenerative processes
• Therapeutic strategies
•Secondary insults
•Regenerative potential
Outline

Nat Rev Neurol 2013 9(4):231-6

Main
Messages
and
Recommendations
2004
2013
• First cause of death and disabilities among young people • 7-8 million of people affected/year in Europe • Unfavorable outcome: 30% • No pharmacological treatment is available to protect against the detrimental consequences of TBI
Traumatic brain injury (TBI)

• 1.2 million die a year
• 20-50 million more are injured or
disabled
• 11th leading cause of death
• account for 2.1% of all deaths
globally
Copyright Etienne Creux, Pretoria News
Road traffic injuries are a huge public health and development problem

Global incidence
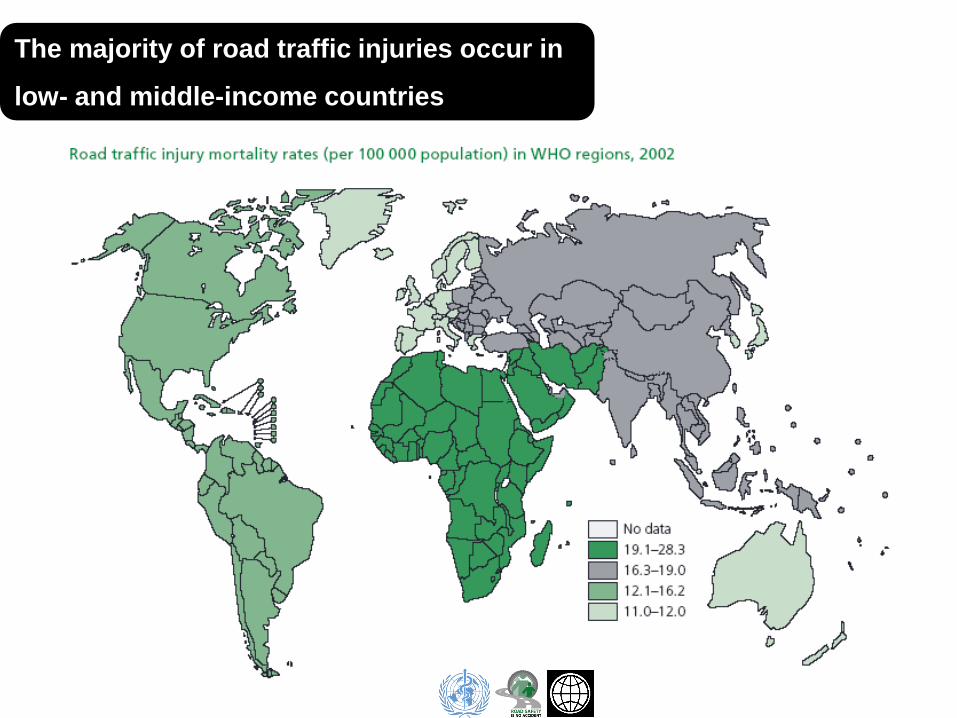
The majority of road traffic injuries occur in
low- and middle-income countries

Road traffic fatalities are predicted to increase by 67% by the year 2020
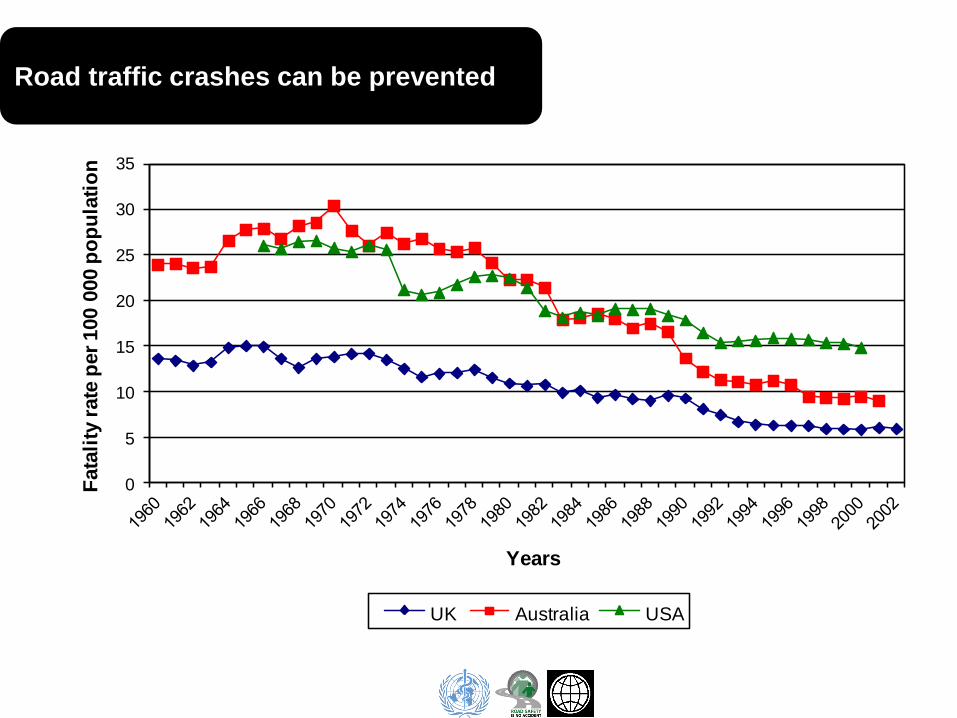
0
5
10
15
20
25
30
35
Fata
lity
rate
per
100 0
00 p
op
ula
tio
n
Years
UK Australia USA
Road traffic crashes can be prevented

What is traumatic brain injury ?
heterogeneity

heterogeneity

Thomas J. Deerinck
University of California, San Diego, USA

Neuron
Astrocyte
Microglia
Oligodendrocyte
Pericyte
Endothelial cell
Minutes Hours Days Months
TBI and primary injury

Neuron
Astrocyte
Microglia
Oligodendrocyte
Pericyte
Endothelial cell
TBI
heterogeneity
TBI and primary injury
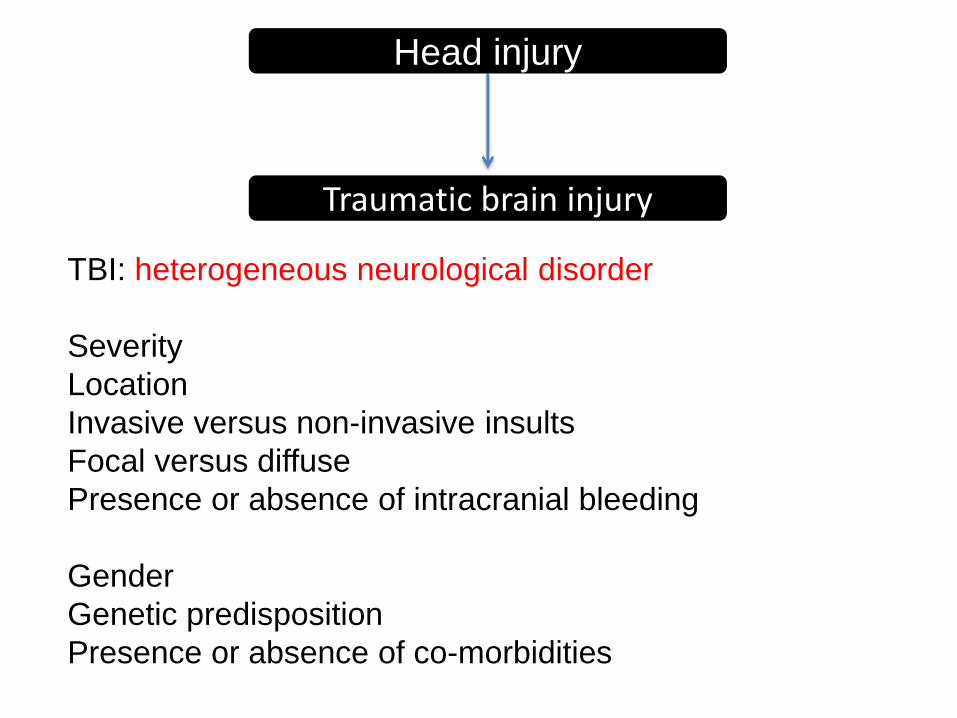
TBI: heterogeneous neurological disorder
Severity
Location
Invasive versus non-invasive insults
Focal versus diffuse
Presence or absence of intracranial bleeding
Gender
Genetic predisposition
Presence or absence of co-morbidities
Head injury
Traumatic brain injury

Inflammation &
apoptosis
Excitotoxicity
Minutes Hours Days Months
energy failure
excitotoxicity
depolarization
necrosis
inflammation
programmed cell death
Ba
d o
utc
om
e
TBI associated events

Time after TBI
Level of
response Cumulative injury
Temporal evolution of brain damage

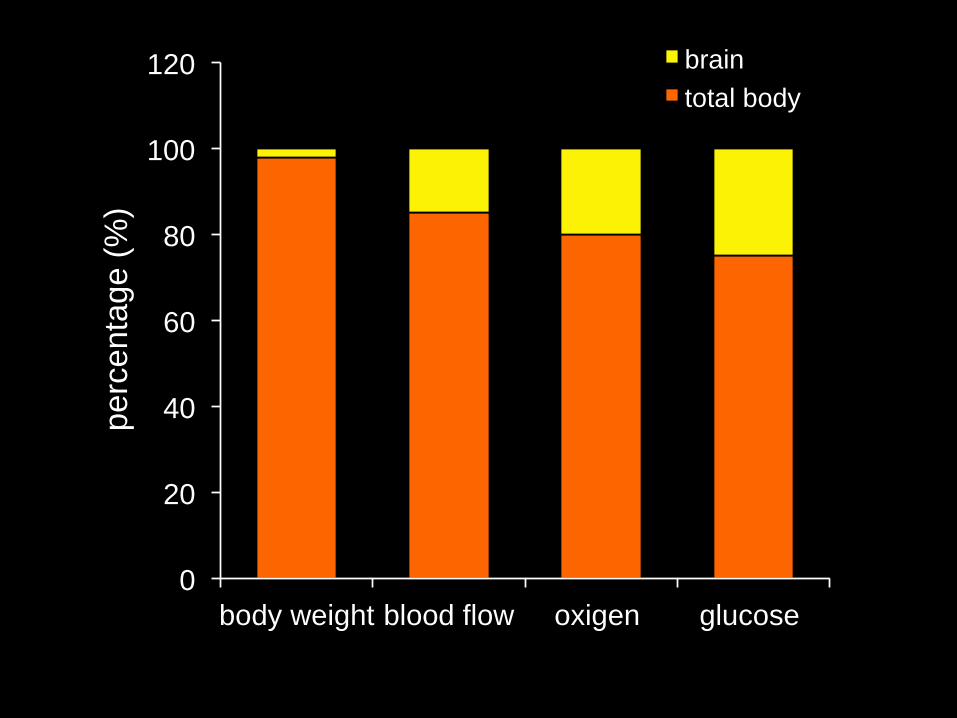
Multitracer PET studies
Comprehensive regional metabolic picture
Glucose
utilization
(CMRglc)
CBF Oxygen
utilization
(CMRO2)
Oxygen
extractio
n
(OEF)
Sokoloff, 1960
0
20
40
60
80
100
120
body weight blood flow oxigen glucose
pe
rcenta
ge (
%)
brain
total body
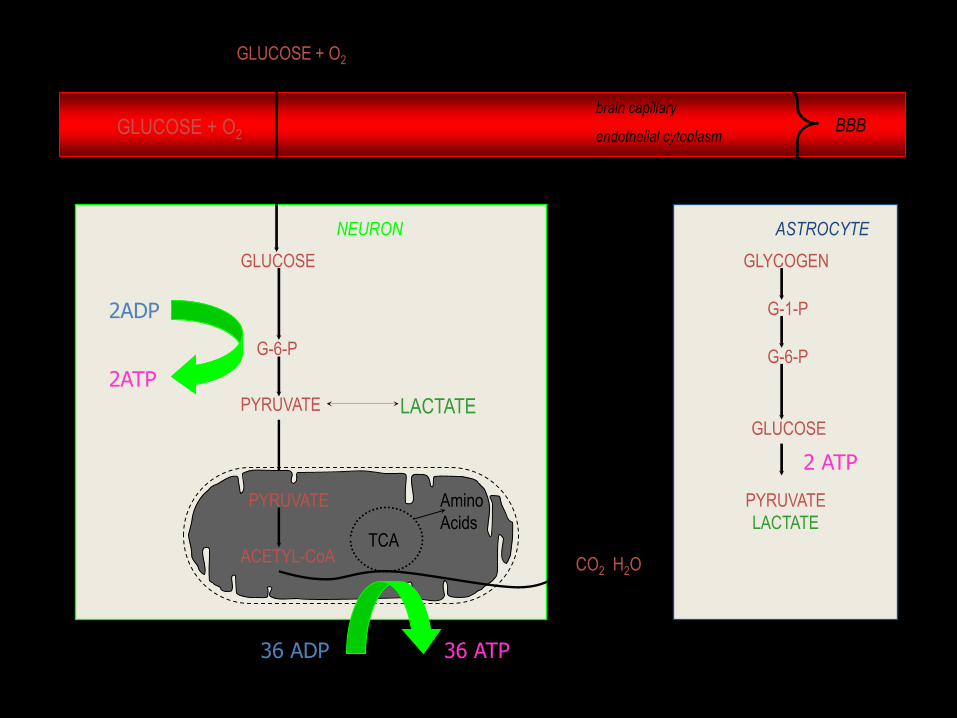
NEURON ASTROCYTE
BBB brain capillary
endothelial cytoplasm
PYRUVATE
ACETYL-CoA TCA
CO2 H2O
Amino
Acids
GLUCOSE + O2
LACTATE
GLUCOSE
G-6-P
PYRUVATE
•Sihver, 2000, Uppsala University
GLYCOGEN
GLUCOSE
G-6-P
G-1-P
PYRUVATE
LACTATE
2ATP
36 ATP
2 ATP
GLUCOSE + O2
2ADP
36 ADP

Functional activity
ATP ADP
Energy generation
4X1021 molecules of ATP/min

Acceleration - Deceleration
Rotation
Traumatic brain injury: concussion
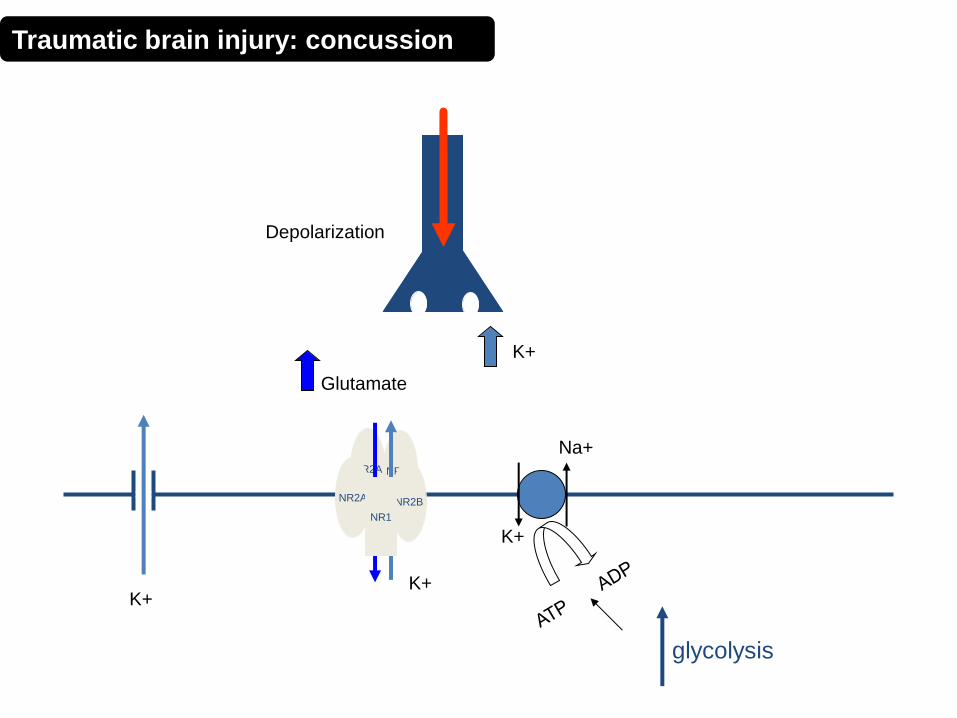
NR2A NR2B
NR2A NR2B
NR1
Glutamate
glycolysis
K+
K+
Na+
Depolarization
K+ K+
Traumatic brain injury: concussion

UCLA Brain Injury Research Center
Increased brain glucose utilization following TBI in the rat

(Yamakami & McIntosh, 1991) 30
40
50
60
70
80
90
100
110
0 15 30 1 2 4 24
Time (minutes) (hours)
% Pre-Injury values
[14C]-iodoantipyrine
autoradiography
Min
Max
Decreased cerebral blood flow following TBI in the rat

Animal
Autoradiography
10.7 8.6 20 37
rCBF
ml/100g/min
lCMRglc
mg/100g/min
CT
(raw)
Mismatch of CMRglc and CBF following TBI

Energy crisis
Ca2+
Mitochondrial function
NR2A NR2B
NR2A NR2B
NR1
K+
Na+
glycolysis
Mg++
Depolarization
Glutamate
Traumatic brain injury: concussion

Depression lCMR glc 3 Days Following
Lateral F-P Brain Injury
lCMR glc
(µmols/100g/min)
<3
0
5
0
70
90
110
130
>150
UCLA Brain Injury Research Center
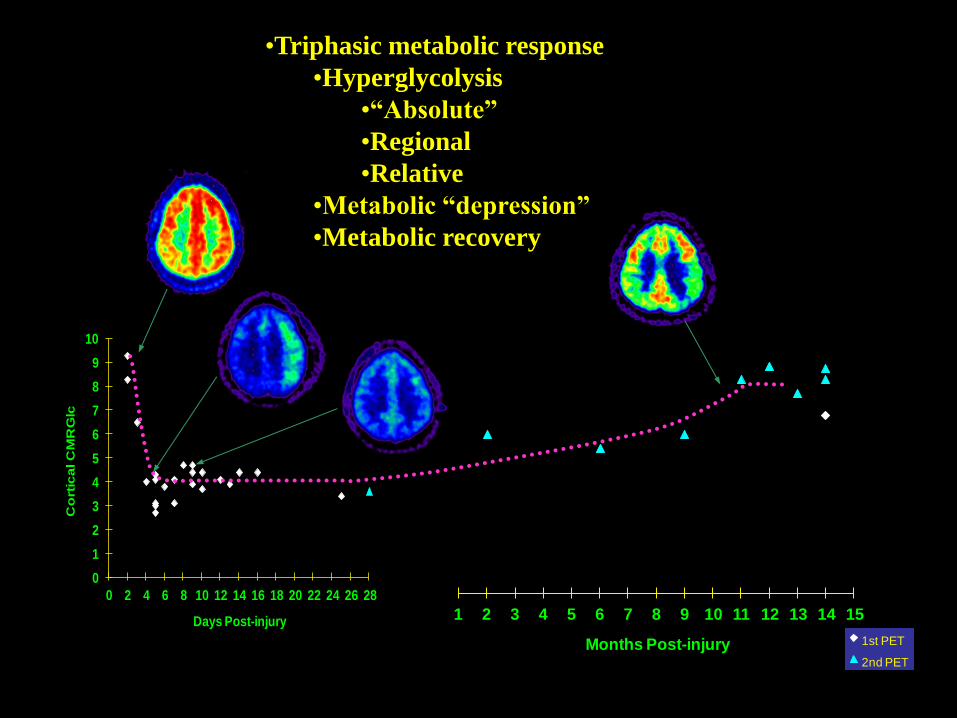
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Months Post-injury 1st PET
2nd PET
0
1
2
3
4
5
6
7
8
9
10
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28
Co
rtic
al C
MR
Glc
Days Post-injury
•Triphasic metabolic response
•Hyperglycolysis
•“Absolute”
•Regional
•Relative
•Metabolic “depression”
•Metabolic recovery
DeWitt DS: New Horizons 1995
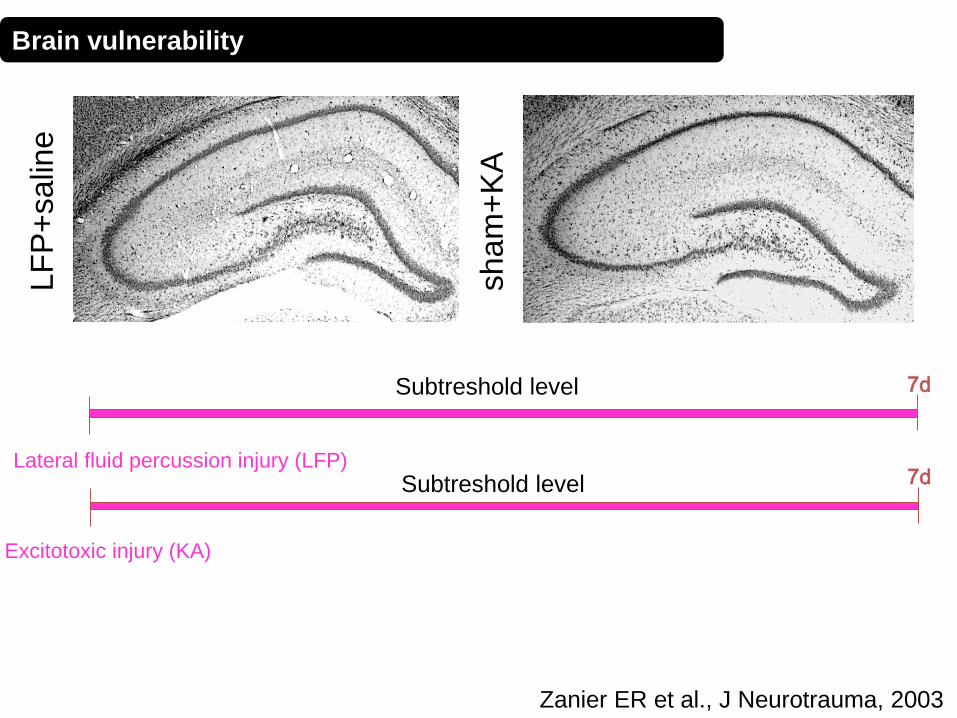
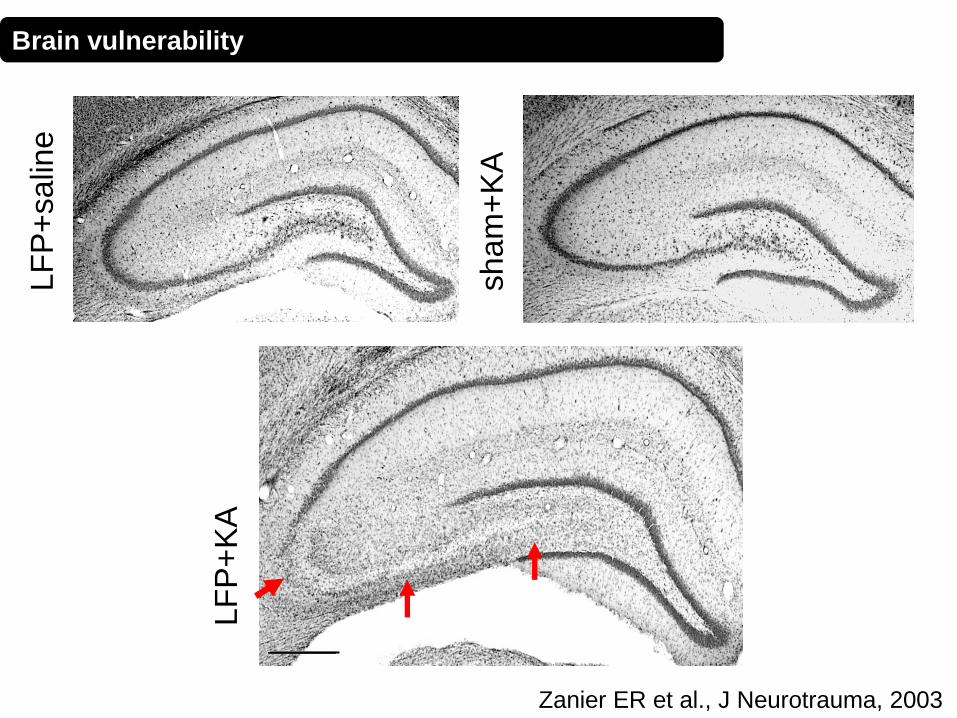
• vascular factors that increase the likelihood of ischemia (SUSCEPTIBILITY) • altered ability to withstand insults (SENSITIVITY)
The injured brain is vulnerable to even otherwise tolerable alterations
lower threshold for energy failure
Enhanced VULNERABILITY after TBI
Zanier ER, et al., J Neurotrauma, 2003
Brain vulnerability

LF
P+
salin
e
Zanier ER, et al., J Neurotrauma, 2003
7d
Lateral fluid percussion injury (LFP)
Subtreshold level
Brain vulnerability
sham
+K
A
LF
P+
salin
e
Zanier ER et al., J Neurotrauma, 2003
7d
Lateral fluid percussion injury (LFP) 7d
Subtreshold level
Subtreshold level
Excitotoxic injury (KA)
Brain vulnerability

sham
+K
A
LF
P+
salin
e
Zanier ER et al., J Neurotrauma, 2003
7d
Lateral fluid percussion injury (LFP) 7d
Excitotoxic injury (KA)
Subtreshold level
Subtreshold level
7d
LFP KA
Brain vulnerability
sham
+K
A
LF
P+
salin
e
LF
P+
KA
Zanier ER et al., J Neurotrauma, 2003
Brain vulnerability
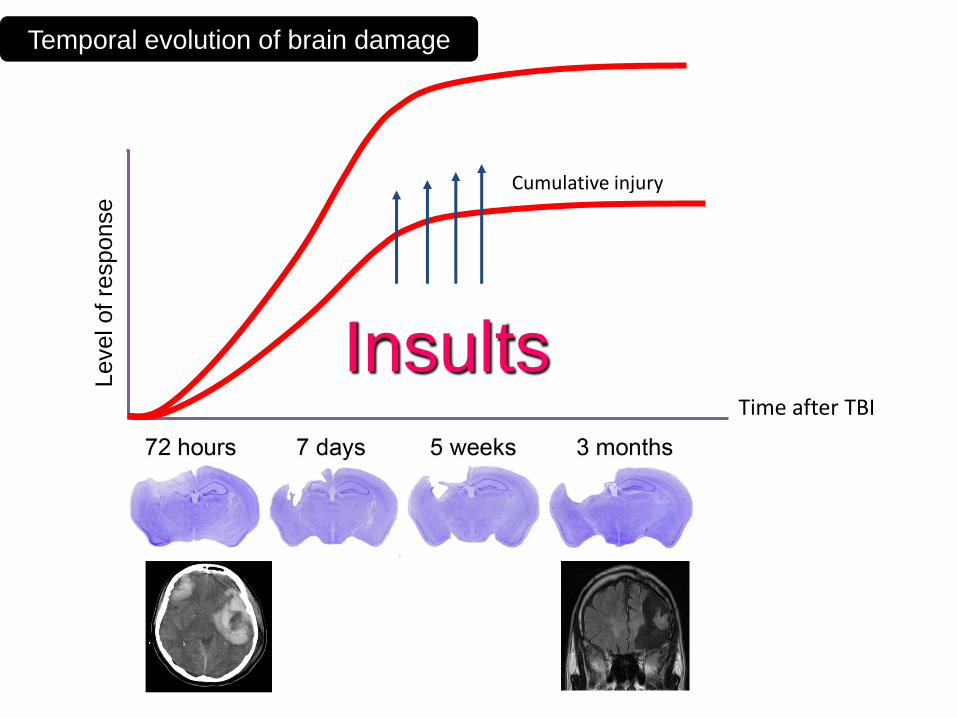
Time after TBI
Level of
response Cumulative injury
Temporal evolution of brain damage
Insults

Metabolismo
depresso
Ridotto flusso
ematico
cerebrale
Morte cellulare
e
danni neurologici
Riduzione della
pressione
Crisi
comiziali
Carenza di
ossigeno
Febbre
Fallimento
energetico
Secondary insults
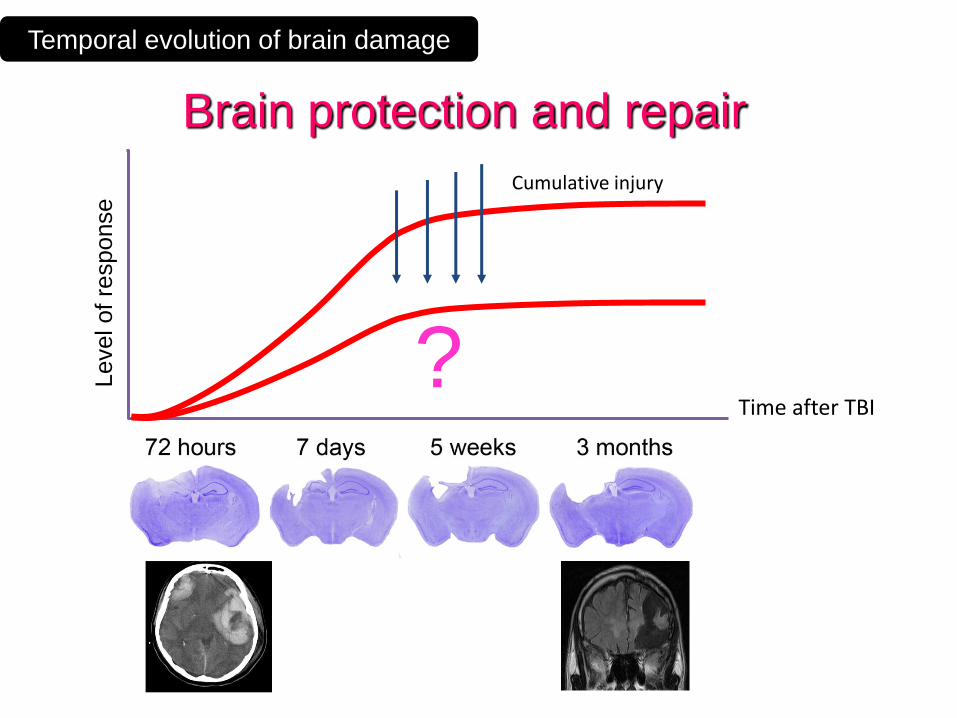
Time after TBI
Level of
response Cumulative injury
Temporal evolution of brain damage
Brain protection and repair
?
More than 30 Phase-3 trials have failed to show significance for
their primary end point.
Most of these trials targeted single factors proposed to mediate
secondary injury.
Therapeutic strategies for TBI
Endogenous
brain protection
Plasticity &
regeneration
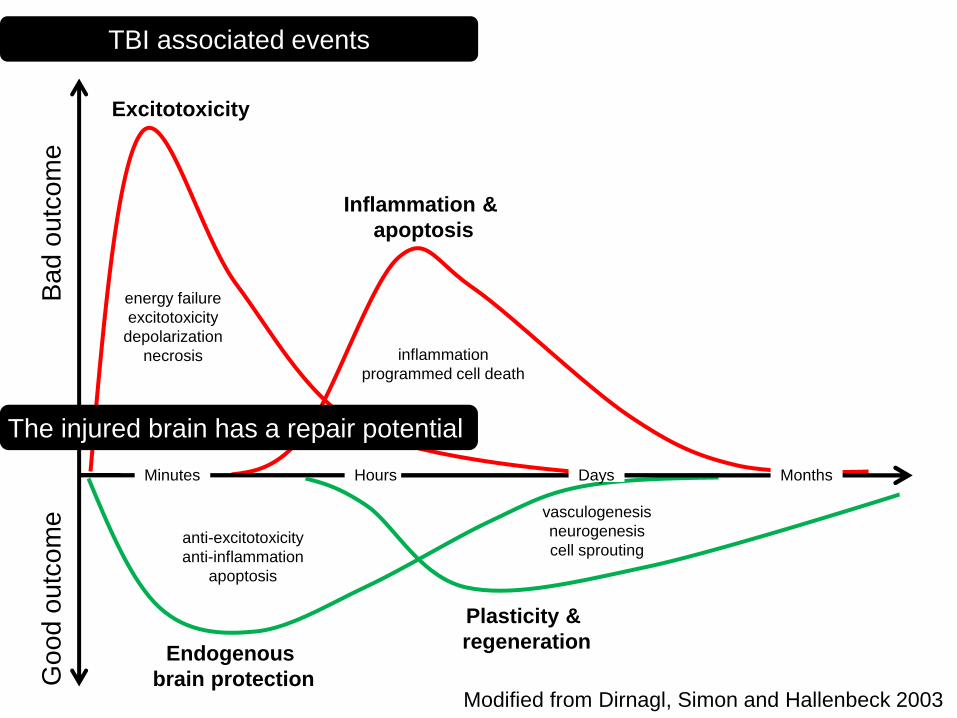
Inflammation &
apoptosis
Excitotoxicity
Minutes Hours Days Months
energy failure
excitotoxicity
depolarization
necrosis
anti-excitotoxicity
anti-inflammation
apoptosis
inflammation
programmed cell death
vasculogenesis
neurogenesis
cell sprouting
Modified from Dirnagl, Simon and Hallenbeck 2003
Go
od
ou
tco
me
B
ad
ou
tco
me
TBI associated events
The injured brain has a repair potential

Time after Traumatic Brain Injury
Level of
response
Endogenous compenstation and remodeling
Cumulative injury
TBI associated events

More than 30 Phase-3 trials have failed to show significance for
their primary end point.
Most of these trials targeted single factors proposed to mediate
secondary injury.
Need to focus on:
Strategies that affect simultaneously multiple injury mechanisms.
Neurorestorative strategies that enhance endogenous restorative
brain plasticity processes to improve functional recovery.
Therapeutic strategies for TBI

More than 30 Phase-3 trials have failed to show significance for
their primary end point.
Most of these trials targeted single factors proposed to mediate
secondary injury.
Need to focus on:
Strategies that affect simultaneously multiple injury mechanisms.
Mesenchymal stem cells: induce multiple protective mechanisms
Neurorestorative strategies that enhance endogenous restorative
brain plasticity processes to improve functional recovery.
Mesenchymal stem cells: induce mechanisms of repair
Therapeutic strategies for TBI
Mesenchymal stromal cells to reprogramme the local microenviroment
•In different injury models it has been shown that MSC can induce multiple mechanisms of protection and repair
•Distinctive advantages of mesenchymal stromal cells (MSC): •Safe •Easily available •Free of ethical problem •Already used in the clinical setting for non-neurological conditions

2014
Mesenchymal stem cells for TBI
2014

Zanier et al., Cellular Therapy for Stroke and CNS Injuries. Springer in press
Toxic and protective events affected by MSCs
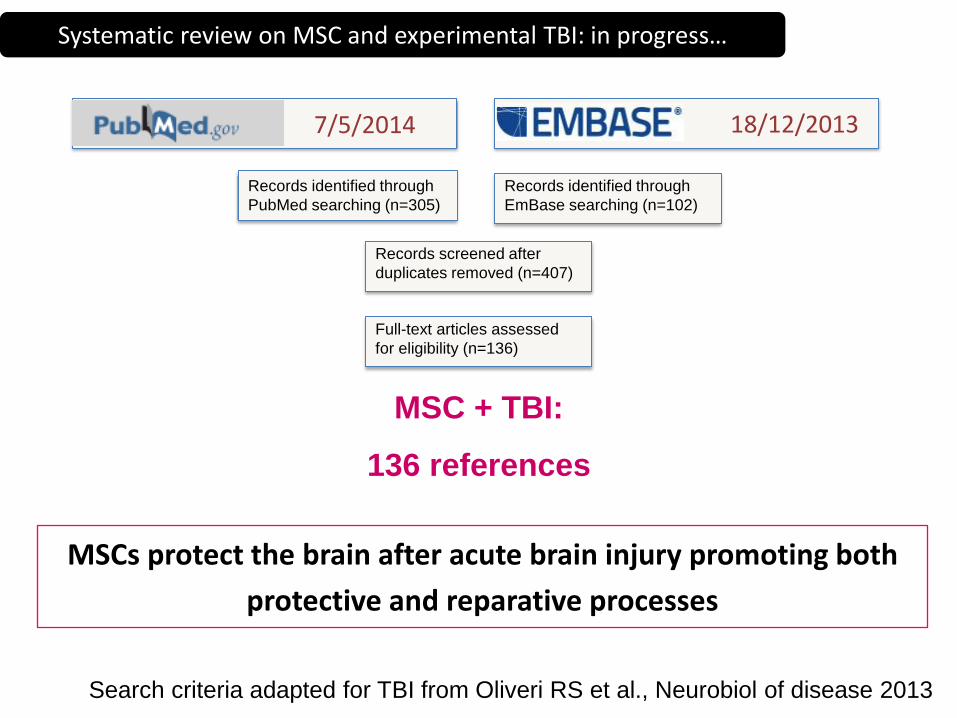
MSC + TBI:
136 references
MSCs protect the brain after acute brain injury promoting both
protective and reparative processes
Records identified through
PubMed searching (n=305)
Records identified through
EmBase searching (n=102)
Records screened after
duplicates removed (n=407)
Full-text articles assessed
for eligibility (n=136)
7/5/2014 18/12/2013
Systematic review on MSC and experimental TBI: in progress…
Search criteria adapted for TBI from Oliveri RS et al., Neurobiol of disease 2013

Zanier et al., Cellular Therapy for Stroke and CNS Injuries. Springer in press
Clinical Trials (CTs) registered in ClinicalTrials.gov on stem/stromal cells.
Search performed on 12-2-2014.
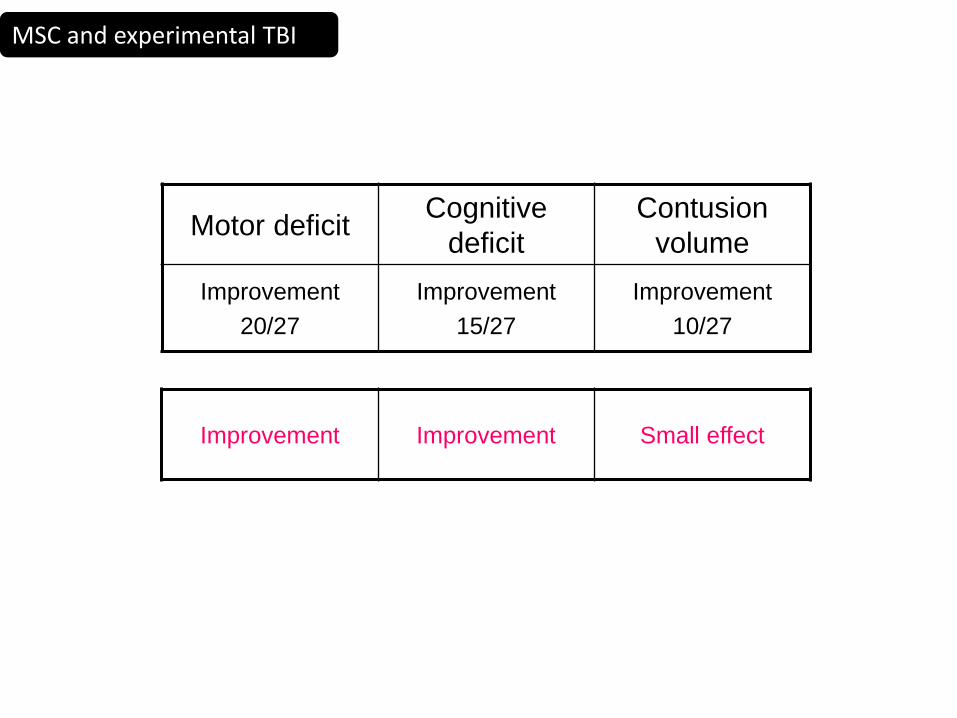
Motor deficit Cognitive
deficit
Contusion
volume
Improvement
20/27
Improvement
15/27
Improvement
10/27
Improvement Improvement Small effect
MSC and experimental TBI

•MSC isolated from different tissues are NOT
equivalent
•Protocols used to prepare the cells affect their
properties
Maximize efficacy
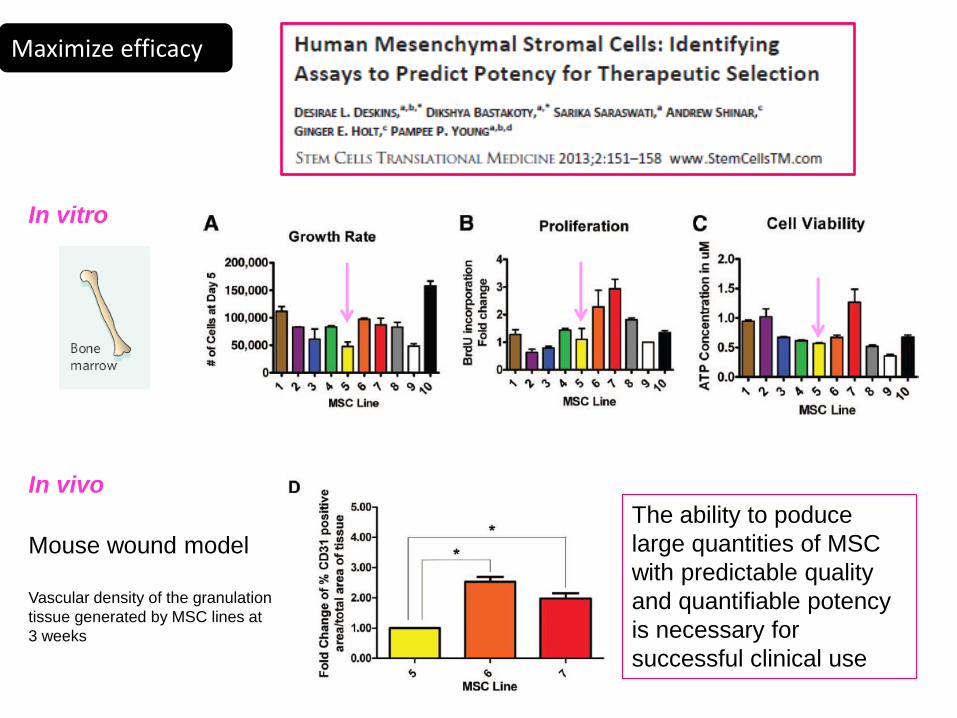
In vitro
In vivo
Mouse wound model
Vascular density of the granulation
tissue generated by MSC lines at
3 weeks
The ability to poduce
large quantities of MSC
with predictable quality
and quantifiable potency
is necessary for
successful clinical use
Maximize efficacy
• Maximum information about efficacy and safety must be obtained from ongoing and planned clinical trials
• Mechanism of actions:
– To select the optimal cell type/source/culture condition
– To induce maximum recovery
– To select the most suitable patient
What is needed to translate stem cells into effective therapies following TBI

• Epidemiology
• Pathophysiology
•Heterogeneity
•Susceptibility
•Chronic degenerative processes
• Therapeutic strategies
•Secondary insults
•Regenerative potential
Outline

Erica Carlino Daiana De Blasio Stefano Fumagalli Federica Marchesi Davide Olivari Franca Orsini Emanuela Parotto Carlo Perego Francesca Pischiutta Eliana Sammali Gloria Vegliante Pia Villa Rosalia Zangari Maria Grazia De Simoni
UCLA Neurotrauma Laboratory Terapia Intensiva Neuroscienze
MILANO POLICLINICO

















