To end the HIV epidemic, we must consider the impact of organizational environments frontline staff are a part of. • The oppressive socio-political-economic context of the Deep U.S. South has contributed to and exacerbated the HIV epidemic at individual, community and structural levels. • This context, in combination with organizational factors (e.g. minimal resources, under-staffed organizations and cumbersome caseloads) are barriers to frontline staff providing quality care to people living with HIV. • For frontline staff, this environment results in burnout, turnover and compassion fatigue as well as dissatisfaction and poor quality care for clients. We must create effective strategies and interventions to build healthy, trauma- informed environments. Trauma-informed supervision is part of a larger strategy to implementing trauma-informed care. Supervisors are in a unique position to influence work culture and therefore, help organizations move along the continuum of implementation for trauma- informed care. Increases staff satisfaction Promotes staff retention Decreases burnout and staff turnover Negates vicarious trauma Enhances staff wellbeing Improves services provided to clients Trauma Informed Supervision (TIS) Katie McCormick, LMSW, Program Coordinator Lladira Aguilar, LMSW, Capacity Building Assistance Manager Samira Ali, PhD, MSW, Center Director BENEFITS OF TIS IMPORTANCE OF TIS "CARE OF THE STAFF IS A PREREQUISITE FOR LEADERSHIP WHO WANT TRAUMA RESPONSIVE CARE FOR [THE COMMUNITIES] THEY SERVE." - Olton, Martin, & Meeker, 2016 1 Curated by: SOURCES 1. Olton, G., Martin, C., & Meeker, E. (2016). Supervision trauma-informed care series: session four . | 2. SAMHSA. (2014). Concept of Trauma and Guidance for a Trauma-Informed Approach. 3. Guroff, E. (2018). Trauma-Informed Supervision: It’s for Everyone . Relias. Supported by grant funding from Gilead Sciences Inc. Gilead Sciences, Inc. has had no input into the development or content of these materials. Trauma-informed care is grounded in a set of four assumptions and six key principles. It realizes the pervasiveness of trauma, recognizes the signs and symptoms, responds to trauma and resists re-traumatization. A trauma-informed approach reflects adherence to six key principles rather than a prescribed set of practices or procedures. TRAUMA-INFORMED SUPERVISION AS PART OF TRAUMA-INFORMED CARE Flexibility Communication Partnership Empathy Support Self-care TIS CONCEPTS 3 Collaboration & Mutuality Empowerment, Voice & Choice Safety Trust & Transparency Peer Support Cultural, Historical & Gender Factors TIC PRINCIPLES 2 University of Houston Graduate College of Social Work SUSTAIN COMPASS Coordinating Center
Transcript
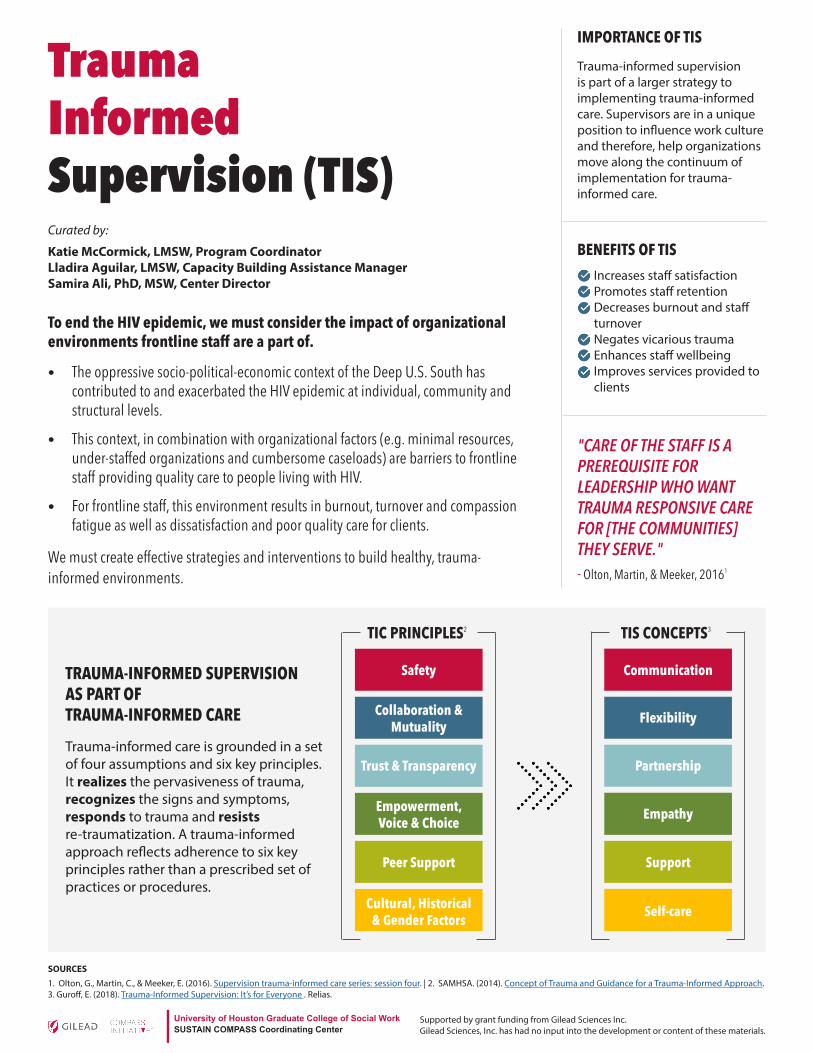
To end the HIV epidemic, we must consider the impact of organizational environments frontline staff are a part of.
• The oppressive socio-political-economic context of the Deep U.S. South has contributed to and exacerbated the HIV epidemic at individual, community and structural levels.
• This context, in combination with organizational factors (e.g. minimal resources, under-staffed organizations and cumbersome caseloads) are barriers to frontline staff providing quality care to people living with HIV.
• For frontline staff, this environment results in burnout, turnover and compassion fatigue as well as dissatisfaction and poor quality care for clients.
We must create effective strategies and interventions to build healthy, trauma-informed environments.
Trauma-informed supervision is part of a larger strategy to implementing trauma-informed care. Supervisors are in a unique position to influence work culture and therefore, help organizations move along the continuum of implementation for trauma-informed care.
Trauma Informed Supervision (TIS)Katie McCormick, LMSW, Program CoordinatorLladira Aguilar, LMSW, Capacity Building Assistance ManagerSamira Ali, PhD, MSW, Center Director
BENEFITS OF TIS
IMPORTANCE OF TIS
"CARE OF THE STAFF IS A PREREQUISITE FOR LEADERSHIP WHO WANT TRAUMA RESPONSIVE CARE FOR [THE COMMUNITIES] THEY SERVE."- Olton, Martin, & Meeker, 20161
Curated by:
SOURCES1. Olton, G., Martin, C., & Meeker, E. (2016). Supervision trauma-informed care series: session four. | 2. SAMHSA. (2014). Concept of Trauma and Guidance for a Trauma-Informed Approach.3. Guroff, E. (2018). Trauma-Informed Supervision: It’s for Everyone . Relias.
Supported by grant funding from Gilead Sciences Inc. Gilead Sciences, Inc. has had no input into the development or content of these materials.
Trauma-informed care is grounded in a set of four assumptions and six key principles. It realizes the pervasiveness of trauma, recognizes the signs and symptoms, responds to trauma and resists re-traumatization. A trauma-informed approach reflects adherence to six key principles rather than a prescribed set of practices or procedures.
TRAUMA-INFORMED SUPERVISION AS PART OF TRAUMA-INFORMED CARE Flexibility
Communication
Partnership
Empathy
Support
Self-care
TIS CONCEPTS3
Collaboration & Mutuality
Empowerment, Voice & Choice
Safety
Trust & Transparency
Peer Support
Cultural, Historical & Gender Factors
TIC PRINCIPLES2
University of Houston Graduate College of Social WorkSUSTAIN COMPASS Coordinating Center
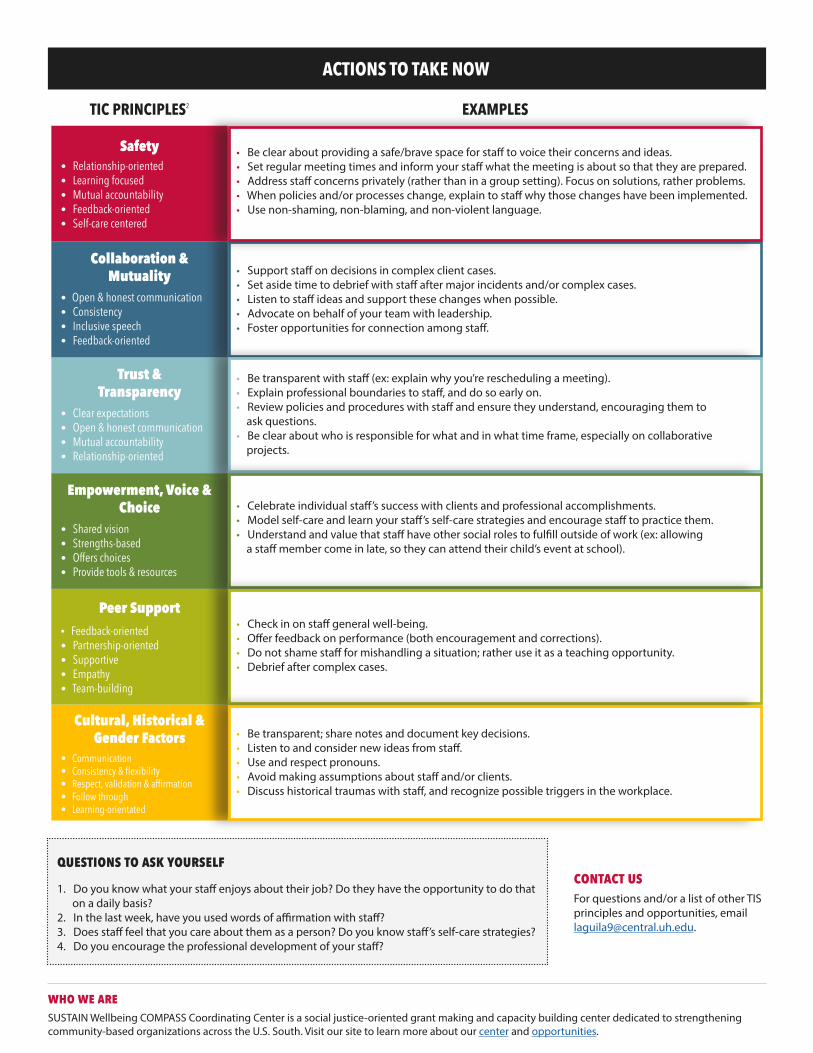
Safety • Be clear about providing a safe/brave space for staff to voice their concerns and ideas.• Set regular meeting times and inform your staff what the meeting is about so that they are prepared. • Address staff concerns privately (rather than in a group setting). Focus on solutions, rather problems. • When policies and/or processes change, explain to staff why those changes have been implemented. • Use non-shaming, non-blaming, and non-violent language.
• Support staff on decisions in complex client cases.• Set aside time to debrief with staff after major incidents and/or complex cases.• Listen to staff ideas and support these changes when possible. • Advocate on behalf of your team with leadership. • Foster opportunities for connection among staff.
Collaboration & Mutuality
• Open & honest communication • Consistency• Inclusive speech • Feedback-oriented
Trust & Transparency
• Clear expectations • Open & honest communication • Mutual accountability • Relationship-oriented
• Be transparent with staff (ex: explain why you’re rescheduling a meeting). • Explain professional boundaries to staff, and do so early on. • Review policies and procedures with staff and ensure they understand, encouraging them to ask questions.• Be clear about who is responsible for what and in what time frame, especially on collaborative projects.
• Celebrate individual staff’s success with clients and professional accomplishments. • Model self-care and learn your staff’s self-care strategies and encourage staff to practice them. • Understand and value that staff have other social roles to fulfill outside of work (ex: allowing a staff member come in late, so they can attend their child’s event at school).
• Check in on staff general well-being. • Offer feedback on performance (both encouragement and corrections).• Do not shame staff for mishandling a situation; rather use it as a teaching opportunity. • Debrief after complex cases.
Cultural, Historical & Gender Factors
• Communication • Consistency & flexibility • Respect, validation & affirmation • Follow through • Learning-orientated
• Be transparent; share notes and document key decisions.• Listen to and consider new ideas from staff. • Use and respect pronouns. • Avoid making assumptions about staff and/or clients.• Discuss historical traumas with staff, and recognize possible triggers in the workplace.
EXAMPLESTIC PRINCIPLES2
ACTIONS TO TAKE NOW
Questions to Ask Yourself
1. Do you know what your staff enjoys about their job? Do they have the opportunity to do that on a daily basis? 2. In the last week, have you used words of affirmation with staff? 3. Does staff feel that you care about them as a person? Do you know staff’s self-care strategies?4. Do you encourage the professional development of your staff?
ContACt usFor questions and/or a list of other TIS principles and opportunities, email [email protected].
SUSTAIN Wellbeing COMPASS Coordinating Center is a social justice-oriented grant making and capacity building center dedicated to strengthening community-based organizations across the U.S. South. Visit our site to learn more about our center and opportunities.
Using Motivational Interviewing Skills in Supervision (Adapted from Miller and Rollnick, 2013)
OARS: Open Questions “Tell me more about that” “What approaches have you tried thus far?” Open questions invite others to talk about what is important to them as well as to elaborate on a topic. They are the opposite of closed questions that typically result in a limited response. Open questions are used in supervision to draw out information, ideas, and feelings to enable supervisees to clarify and develop their practice. OARS: Affirmations “You used your reflective listening skills very effectively in that situation” “That sounds like a good idea. Let’s try it.” Affirmations are statements and gestures that recognize a person’s strengths and positive behaviors. Affirmations build confidence in one’s abilities. To be effective, affirmations need to be genuine and congruent. OARS: Reflective Listening “This has been stressful for you.” “You’re wondering if you could have prevented him from getting hospitalized.” Reflective listening is a primary skill in building and maintaining effective supervisory relationships. It fosters clear communication, builds trust, and helps develop the supervisee’s confidence. Reflective listening appears deceptively easy, but takes hard work and skill to do well. There are three basic levels of reflective listening: Repeating or rephrasing – listener repeats or substitutes synonyms or phrases; stays close to what the speaker has said. Paraphrasing – listener makes a major restatement in which the speaker’s meaning is inferred. Reflection of feeling – listener emphasizes emotional aspects of communication through feeling statements – deepest form of listening. OARS: Summaries “Let me see if I understand.” “Here is what I think I’ve heard. Tell me if I’ve missed anything.” Summaries are special applications of reflective listening. They are particularly helpful at transition points, for example, after the person has spoken about a particular topic, has recounted a personal experience, or when the conversation is nearing an end. Summarizing helps to ensure that there is clear communication between the speaker and listener. Also, it can provide a stepping stone towards determining “next steps.”
www.gileadcompass.com
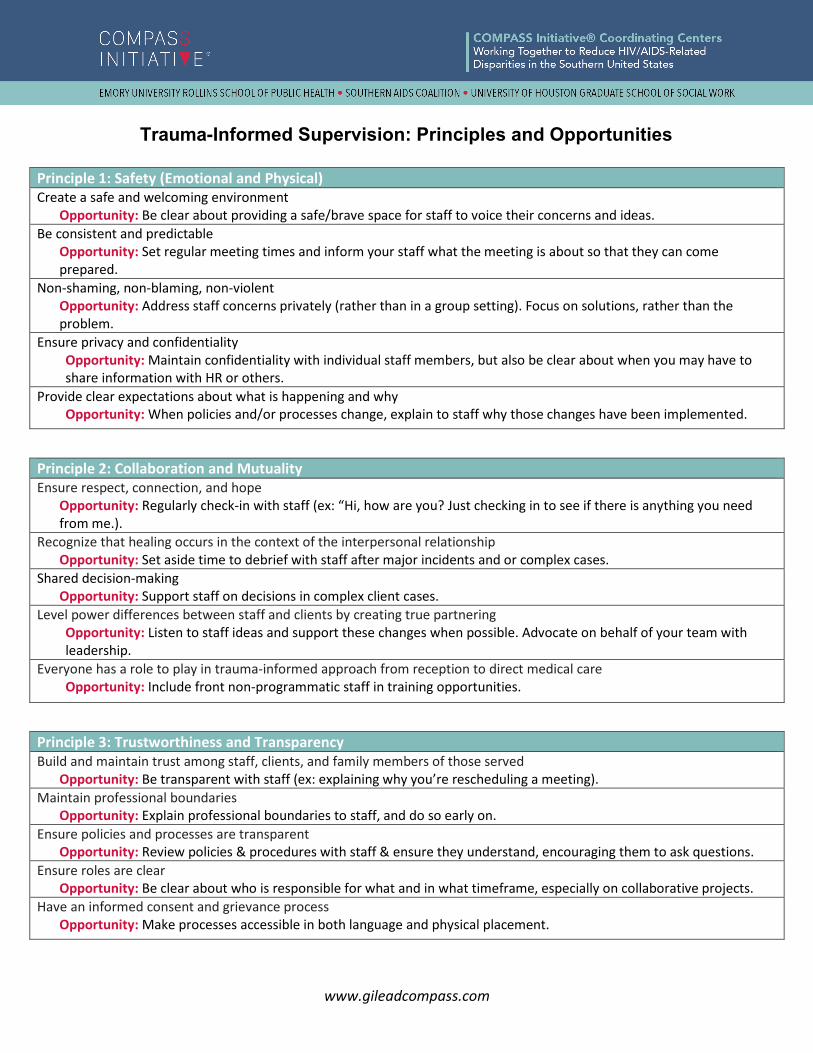
Trauma-Informed Supervision: Principles and Opportunities
Principle 1: Safety (Emotional and Physical) Create a safe and welcoming environment
Opportunity: Be clear about providing a safe/brave space for staff to voice their concerns and ideas. Be consistent and predictable
Opportunity: Set regular meeting times and inform your staff what the meeting is about so that they can come prepared.
Non-shaming, non-blaming, non-violent Opportunity: Address staff concerns privately (rather than in a group setting). Focus on solutions, rather than the problem.
Ensure privacy and confidentiality Opportunity: Maintain confidentiality with individual staff members, but also be clear about when you may have to share information with HR or others.
Provide clear expectations about what is happening and why Opportunity: When policies and/or processes change, explain to staff why those changes have been implemented.
Principle 2: Collaboration and Mutuality Ensure respect, connection, and hope
Opportunity: Regularly check-in with staff (ex: “Hi, how are you? Just checking in to see if there is anything you need from me.).
Recognize that healing occurs in the context of the interpersonal relationship Opportunity: Set aside time to debrief with staff after major incidents and or complex cases.
Shared decision-making Opportunity: Support staff on decisions in complex client cases.
Level power differences between staff and clients by creating true partnering Opportunity: Listen to staff ideas and support these changes when possible. Advocate on behalf of your team with leadership.
Everyone has a role to play in trauma-informed approach from reception to direct medical care Opportunity: Include front non-programmatic staff in training opportunities.
Principle 3: Trustworthiness and Transparency Build and maintain trust among staff, clients, and family members of those served
Opportunity: Be transparent with staff (ex: explaining why you’re rescheduling a meeting). Maintain professional boundaries
Opportunity: Explain professional boundaries to staff, and do so early on. Ensure policies and processes are transparent
Opportunity: Review policies & procedures with staff & ensure they understand, encouraging them to ask questions. Ensure roles are clear
Opportunity: Be clear about who is responsible for what and in what timeframe, especially on collaborative projects. Have an informed consent and grievance process
Opportunity: Make processes accessible in both language and physical placement.
Principle 5: Peer Support Recognize that peer support and mutual self-help are key vehicles for: Establishing safety and hope
Opportunity: Encourage a buddy system to ensure safety when leaving after business hours. Building Trust
Opportunity: Avoid micromanaging staff to demonstrate you trust them. Enhance collaboration
Opportunity: Encourage staff to share successes and challenges with one another. Using stories and lived experience to promote recovery and healing
Opportunity: Hold weekly meetings to discuss complex cases, solicit feedback & learn ways to manage difficult cases.
Principle 6: Cultural, Historical and Gender Factors Actively move past cultural stereotypes and biases
Opportunity: Avoid making assumptions about staff and/or clients. Provide gender responsive services
Opportunity: Encourage staff to include their pronouns in their email signature. Recognize and address historical traumas
Opportunity: Discuss historical traumas with staff, and recognize possible triggers in the workplace for staff. Incorporate policies, protocols & processes that are responsive to the racial, ethnic, and cultural needs of individuals served
Opportunity: Create space for learning about the communities staff are a part of.
Principle 4: Empowerment, Voice and Choice Validate strengths & resilience
Opportunity: Celebrate individual staff success with clients. Use strengths to build & enhance healthy coping skills
Opportunity: Learn your staff’s self-care strategies and encourage staff to use them. Understand past coping mechanisms & normalcy of the response to a not normal situation
Opportunity: Do not shame staff for mishandling a situation; rather use it as a teaching opportunity. Apply strengths-based perspective
Opportunity: These questions will help in learning more about your staff: 1) What do you enjoy most in your day to day work activities? 2) What part of your role is the most exciting to you and why? or 3)What are some of your professional goals? How can I support?
Value social roles Opportunity: Understand and value that staff have other social roles to fulfill outside of work (ex: allowing a staff member come in late, so they can attend their child’s event at school).
Increase and ensure individual control & autonomy Opportunity: Give staff choices when scheduling meetings.
Frame experiences of survivorship, not victimization Opportunity: Ensure that you are modeling a strengths-based perspective and people first language.
Who We Are: SUSTAIN Wellbeing COMPASS Coordinating Center is a social justice-oriented grant making and capacity building center dedicated to strengthening community-based organizations across the U.S. South. Visit our site to learn more about our center and opportunities.
Supported by grant funding from Gilead Sciences, Inc. Gilead Sciences, Inc. has had no input into the development or content of these materials.
While you were growing up, during your first 18 years of life: 1. Did a parent or other adult in the household often or very often…
swear at you, insult you, put you down, or humiliate you? OR Act in a way that made you afraid that you might be physically hurt? Yes No
2. Did a parent or other adult in the household often or very often… push, grab, slap, or throw something at you? OR Ever hit you so hard that you had marks or were injured? Yes No
3. Did an adult or person at least 5 years older than you ever…
touch or fondle you or have you touch their body in a sexual way? OR attempt or actually have oral, anal, or vaginal intercourse with you? Yes No
4. Did you often or very often feel that …
no one in your family loved you or thought you were important or special? OR your family didn’t look out for each other, feel close to each other, or support each other? Yes No
5. Did you often or very often feel that … you didn’t have enough to eat, had to wear dirty clothes, and had no one to protect you? OR your parents were too drunk or high to take care of you or take you to the doctor if you needed it? Yes No
6. Were your parents ever separated or divorced? Yes No 7. Was your mother or stepmother:
often or very often pushed, grabbed, slapped, or had something thrown at her? OR sometimes, often, or very often kicked, bitten, hit with a fist, or hit with something hard? OR ever repeatedly hit at least a few minutes or threatened with a gun or knife? Yes No
8. Did you live with anyone who was a problem drinker or alcoholic or who used street drugs? Yes No 9. Was a household member depressed or mentally ill, or did a household member attempt suicide? Yes No 10. Did a household member go to prison? Yes No 11. Did you experience repeated bullying as a child? Yes No 12. Did you repeatedly experience discrimination based on ethnicity, skin color or sexual orientation? Yes No 13. Did you live in a neighborhood that experienced gang related violence? Yes No 14. Did you ever live in a foster home or group home? Yes N0
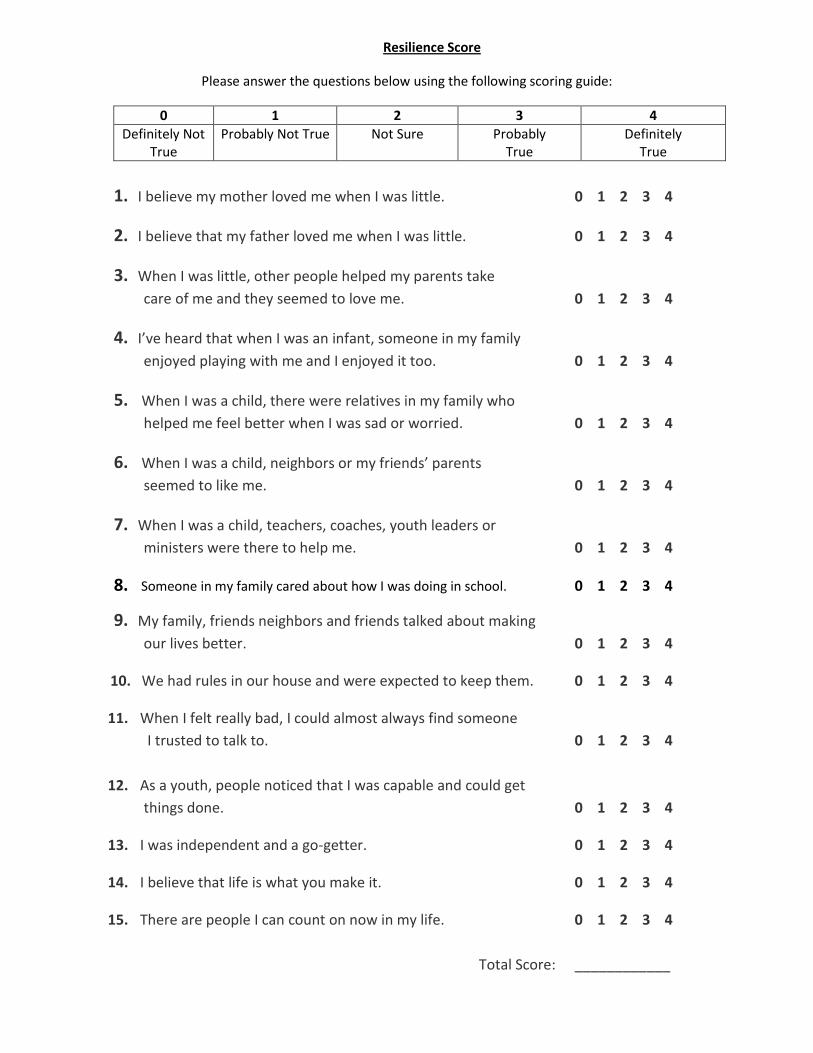
Resilience Score
Please answer the questions below using the following scoring guide:
0 1 2 3 4
Definitely Not True
Probably Not True Not Sure Probably True
Definitely True
1. I believe my mother loved me when I was little. 0 1 2 3 4
2. I believe that my father loved me when I was little. 0 1 2 3 4
3. When I was little, other people helped my parents take
care of me and they seemed to love me. 0 1 2 3 4
4. I’ve heard that when I was an infant, someone in my family
enjoyed playing with me and I enjoyed it too. 0 1 2 3 4
5. When I was a child, there were relatives in my family who
helped me feel better when I was sad or worried. 0 1 2 3 4
6. When I was a child, neighbors or my friends’ parents
seemed to like me. 0 1 2 3 4
7. When I was a child, teachers, coaches, youth leaders or
ministers were there to help me. 0 1 2 3 4
8. Someone in my family cared about how I was doing in school. 0 1 2 3 4
9. My family, friends neighbors and friends talked about making
our lives better. 0 1 2 3 4
10. We had rules in our house and were expected to keep them. 0 1 2 3 4
11. When I felt really bad, I could almost always find someone
I trusted to talk to. 0 1 2 3 4
12. As a youth, people noticed that I was capable and could get
things done. 0 1 2 3 4
13. I was independent and a go-getter. 0 1 2 3 4
14. I believe that life is what you make it. 0 1 2 3 4
15. There are people I can count on now in my life. 0 1 2 3 4
Total Score: ____________
Substance Abuse and Mental Health Services Administration. SAMHSA’s Concept of Trauma and Guidance for a Trauma-Informed Approach. HHS Publication No. (SMA) 14-4884. Rockville, MD: Substance Abuse and Mental Health Services Administration, 2014.
Six Key Principles to a Trauma-Informed Approach
SAFETY: Throughout the organization, staff and the people they serve, whether children or adults, feel
physically and psychologically safe; the physical setting is safe and the interpersonal interactions promote a
sense of safety. Understanding safety as defined by those served is a high priority.
TRUSTWORTHINESS and TRANSPARENCY: Organizational operations are conducted with transparency with
the goal of building and maintaining trust with clients and family members, among staff, and others involved
in the organization.
PEER SUPPORT: Peer support and mutual self-help are key vehicles for establishing safety and hope,
building trust, enhancing collaboration, and utilizing their stories and lived experience to promote recovery
and healing. The term “peers” refers to individuals with lived experiences of trauma, or in the case of
children this may be family members of children who have experienced traumatic events and are key
caregivers in their recovery. Peers have also been referred to as “trauma survivors.”
COLLABORATION AND MUTUALITY: Importance is placed on partnering and the leveling of power
differences between staff and clients and among organizational staff from clerical and housekeeping
personnel, to professional staff to administrators, demonstrating that healing happens in relationships and
in the meaningful sharing of power and decision-making. The organization recognizes that everyone has a
role to play in a trauma-informed approach.
EMPOWERMENT, VOICE AND CHOICE: Throughout the organization and among the clients served,
individual’s strengths and experiences are recognized and built upon. As such, operations, workforce
development and services are organized to foster empowerment for staff and clients alike. Organizations
understand the importance of power differentials and ways in which clients, historically, have been
diminished in voice and choice and are often recipients of coercive treatment. Clients are supported in
shared decision-making, choice, and goal setting to determine the plan of action they need to heal and
move forward. This is a parallel process as staff needs to feel safe, as much as people receiving services.
CULTURAL, HISTORICAL, and GENDER ISSUES: The organization actively moves past cultural stereotypes and
biases (e.g. based on race, ethnicity, sexual orientation, age, religion, gender identity, geography, etc.);
offers access to gender responsive services; leverages the healing value of traditional cultural connections;
incorporates policies, protocols, and processes that are responsive to the racial, ethnic and cultural needs of
individuals served; and recognizes and address historical trauma.
















![Untitled-6 [] · tis 1227-2539 (1996) tis 1390-2539 (1996) tis 1227-2539 (1996) tis 1390-2539 (1996) tis 1227-2539 (1996)](https://static.documents.pub/doc/80x56/5e1a6a0f6b8d9f48bd19bcad/untitled-6-tis-1227-2539-1996-tis-1390-2539-1996-tis-1227-2539-1996-tis.jpg)



