92
| Date post: | 14-Dec-2015 |
| Category: |
Documents |
| Upload: | wilfrid-mosley |
| View: | 217 times |
| Download: | 1 times |

TRAUMA INFORMED CARE
Trauma Informed OregonStephanie Sundborg, MS
AGENDA - WELCOMINGIntent – context
• Creating common language/knowledge • What is trauma? How does it impact
engagement with services?• How do I start thinking about trauma
informed practices?What to consider
• Care of self • Experience – you are the expert in your system
BE GENTLE:
New territory ahead

AGENDA
9:00-9:15 Welcome & Overview
9:15-9:30 TIC 101
9:30-10:30 Acute & Complex Trauma Impact
10:30-11:00 Through a Trauma Lens Activity
11:00-11:15 BREAK
11:15-11:45 TIC Application: safety, power, value
11:45-12:00 Rescue or throw your colleague under bus
12:00-12:15 Examples
12:15-12:45 Hotspots
12:45-1:00 Next Steps and Wrap up

How this relates to the people you see
How this relates to your role
How can you use this info when working with each other?
YOUR CHALLENGE – LISTEN FOR

BEING TRAUMA INFORMED?
SO HELP ME UNDERSTAND….

What does this have to do with the people I work with (clients and or co-
workers)?
What does this have to do with my role?
YOUR CHALLENGE…
TRAUMA INFORMED CARE
“Trauma-informed organizations, programs, and services are based on an understanding of the vulnerabilities or triggers of trauma survivors that traditional service delivery approaches may exacerbate, so that these services and programs can be more supportive and avoid re-traumatization.”
(SAMHSA’s Concept of Trauma and guidance for a Trauma-Informed Approach, 2014 http://store.samhsa.gov/shin/content/SMA14-4884/SMA14-4884.pdf)

TO BE TRAUMA INFORMED
realize the widespread impact of trauma and understand potential paths for recovery;
recognize the signs and symptoms of trauma in clients, families, staff, and others involved with the system; and
respond by fully integrating knowledge about trauma into policies, procedures, and practices, and seek to actively resist re-traumatization”
(SAMHSA’s Concept of Trauma and guidance for a Trauma-Informed Approach, 2014 http://store.samhsa.gov/shin/content/SMA14-4884/SMA14-4884.pdf)
Trauma Recovery/Trauma Specific Services
• Reduce symptoms• Promote healing• Teach skills• Psycho-empowerment, mind-body, other
modalities.
TRAUMA SPECIFIC SERVICES VS. TIC
Trauma Sensitive• Bring an awareness of trauma into view• Trauma lens
Trauma Informed Care• Guide policy, practice, procedure based on
understanding of trauma• Assumption: every interaction with trauma
survivor activates trauma response or does not.• Corrective emotional experiences.• Parallel process
TRAUMA INFORMED CARE

PRINCIPLES OF PRACTICE
With a foundation of awareness and understanding, organizations can strive to reflect three central principles of TIC, by creating policies, procedures, and practices that:
• create safe context,• restore power, and• value the individual.

OUR WORK IS TO
Prevent re-traumatization – triggers
• How can you know?
Recognize early warning signs
• Know your work/population
Intervene – deescalate
• Multi-level – micro, macro

You may already be doing TI practices
• Because of the population you serve• Because it is good practice
It is more than what happens between a person accessing service and a provider.
A REMINDER…

WHAT DO YOU MEAN BY TRAUMA?
TAKE A STEP BACK…
WHAT IS TRAUMA?
Can be single event.
More often multiple events, over time (complex, prolonged trauma).
Interpersonal violence or violation, especially at the hands of an authority or trust figure, is especially damaging.
Three Es of Trauma (SAMHSA, 2014)
• Events
• Experience
• Effects
http://store.samhsa.gov/shin/content/SMA14-4884/SMA14-4884.pdf
Negative Stress (Distress)
TolerableDifficult and challenging
but we react and then recover
Toxic Chronic or repeated circumstances or events
Overwhelms coping skillsBio-chemical response
Can change brain chemistry and function
TRAUMATIC EVENTS
• Physical assault
• Sexual abuse
• Emotional or psychological abuse
• Neglect/abandonment
• Domestic Violence
• Witnessing abuse/violence
• War/Genocide
• Accidents
• Natural or man-made disasters
• Dangerous environment
• Witness or experience street violence
• Poverty
• Homelessness
• Historical Trauma and Current Oppression

WHY IS THIS TOPIC IMPORTANT?
SO HELP ME UNDERSTAND….
WE KNOW
Trauma is pervasive.
Trauma’s impact is broad, deep and life-shaping.
Trauma differentially affects the more vulnerable.
Trauma affects how people approach services.
The service system has often been activating or re-traumatizing.
"WITH ABUSE, YOU SUFFER LOSS OF SOUL, LOSS OF SELF AND LOSS OF MEANING."
"IN THE SYSTEM, YOU MUST FIGHT EVERY DAY, EVERY MINUTE, TO KEEP FROM FEELING WORTHLESS - TO KEEP YOUR SPIRIT ALIVE."
K.W. (SURVIVOR)
From “In Their Own Words: Trauma survivors and professionals they trust tell what hurts, what helps, and what is needed for trauma services” (1997) Jennings, A. and Ralph, R.
"Your history follows you no matter what you do in the present. I only got assaultive one time and that was when they tore the head off my stuffed doll that I had had for a lifetime. Now providers tell me I'm dangerous and I terrify people. My history follows me.”
We know what works for us and what we need, but no one will listen or take us seriously.
I got traumatized because of trusting
people, and asking me to make a contract
with you demands I trust you - which I
can't.
IMPACT ON CHILDREN & FAMILIES
National sample – 60% of 0-17 experienced or witnessed maltreatment, bullying, or assault within year.
One in four experience traumatic event prior to age 16
In Head Start sample (n=113), 58% caregivers and 27% of children had 4+ ACEs.
Sample (n=155) Head Start, 66% community violence
Nurse Family Partnership (n=209), 41% of mothers and fathers had 2-3 ACEs.
(Costello, 2002; Blodgett, 2012; Briggs-Gowan et al 2010; Finkelhor, 2009; Shahinfar et al, 2000)
IMPACT ON HIGH RISK ADULTS
• High rates of sexual/physical assault among women with
substance abuse challenges (up to 99%).
• Link between substance abuse and domestic violence
(up to 80% co-occurrence).
• Sex work and trauma history (up to 99%)
• Public mental health clients and histories of trauma (up
to 90%, most with complex trauma).
Childhood trauma especially linked with Borderline
Personality Disorder, Dissociative Identity Disorder.
Social Workers, Domestic Violence and Sexual Assault:65 % had at least one symptom of secondary traumatic stress (Bride, 2007); 70% experienced vicarious trauma (Lobel, 1997).
Law Enforcement:33% showed high levels of emotional exhaustion and reduced personal accomplishment; 56.1 percent scored high on the depersonalization scale (Hawkins, 2001).
Child Welfare Workers:50% traumatic stress symptoms in severe range (Conrad & Kellar-Guenther, 2006).
Preschool Teachers:30% annual turn over
IMPACT ON WORKFORCE
http://www.olgaphoenix.com/statistics-painful-truth-about-vicarious-trauma/
WHY NOW? IS IT A FAD?
Enormous advances in neurobiology in the last two decades, brain imaging.
Developmental neuroscience, interpersonal neurobiology.
Adverse Childhood Experiences Study
• Link with mental, behavioral, and physical outcomes
• Compelling evidence for a public health perspective
WHAT IT DOESN’T MEAN
It doesn’t mean excusing or permitting/justifying unacceptable behavior
• Supports accountability, responsibility
It doesn’t mean just being nicer
• Compassionate yes, but not a bit mushy
It doesn’t ‘focus on the negative’
• Skill-building, empowerment• Recognizing strengths

WHAT CAN I LEARN FROM THE ACE STUDY?
SO HELP ME UNDERSTAND….
TRAUMA IS PUBLIC HEALTH ISSUE
Adverse Childhood Experiences Study (Kaiser & CDC, 1995)
• 17,337 Kaiser enrolled adults• ACE score cumulative based on 10
experiences in childhood.• Includes mix of interpersonal violence and
family dysfunction
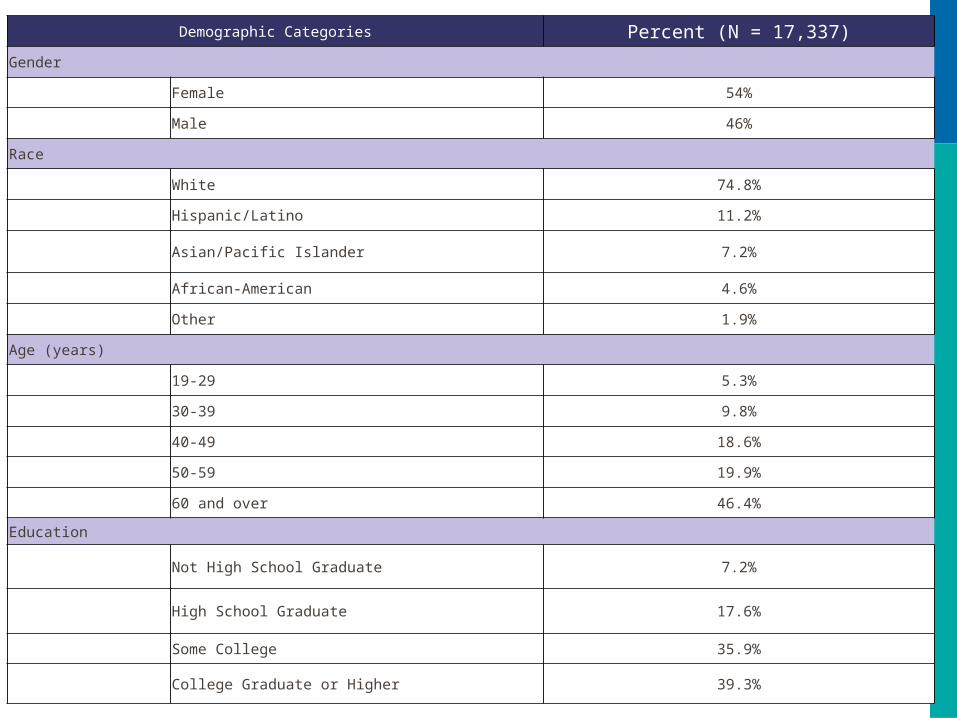
Demographic Categories Percent (N = 17,337)
Gender
Female 54%
Male 46%
Race
White 74.8%
Hispanic/Latino 11.2%
Asian/Pacific Islander 7.2%
African-American 4.6%
Other 1.9%
Age (years)
19-29 5.3%
30-39 9.8%
40-49 18.6%
50-59 19.9%
60 and over 46.4%
Education
Not High School Graduate 7.2%
High School Graduate 17.6%
Some College 35.9%
College Graduate or Higher 39.3%
ACE SCORE INCLUDES:
• Lack of nurturance and support (emotional neglect).
• Hunger, physical neglect, lack of protection (homelessness).
• Divorce in the home.
• Alcoholism or drug use in home.
• Mental illness or attempted suicide among household members.
• Incarceration of household member.
Two-thirds of sample had a score of 1 or more; ~1 out of 6 had score of 4 or more.
In Oregon (n=4,000): 62% at least 1; 16% four or more (BRFSS, 2011)

THE CUMULATIVE IMPACT
ACE study (scores 0-10)
• Score of 4 or more:• Twice as likely to smoke• 12 times as likely to have attempted suicide.• Twice as likely to be alcoholic.• 10 times as likely to have injected street drugs.
Linear relationship with:
• Prostitution, mental health disorders, substance abuse, early criminal behavior.
• Physical health problems, early death.

ADVERSE CHILDHOOD EXPERIENCES(WWW.ACESTUDY.ORG)
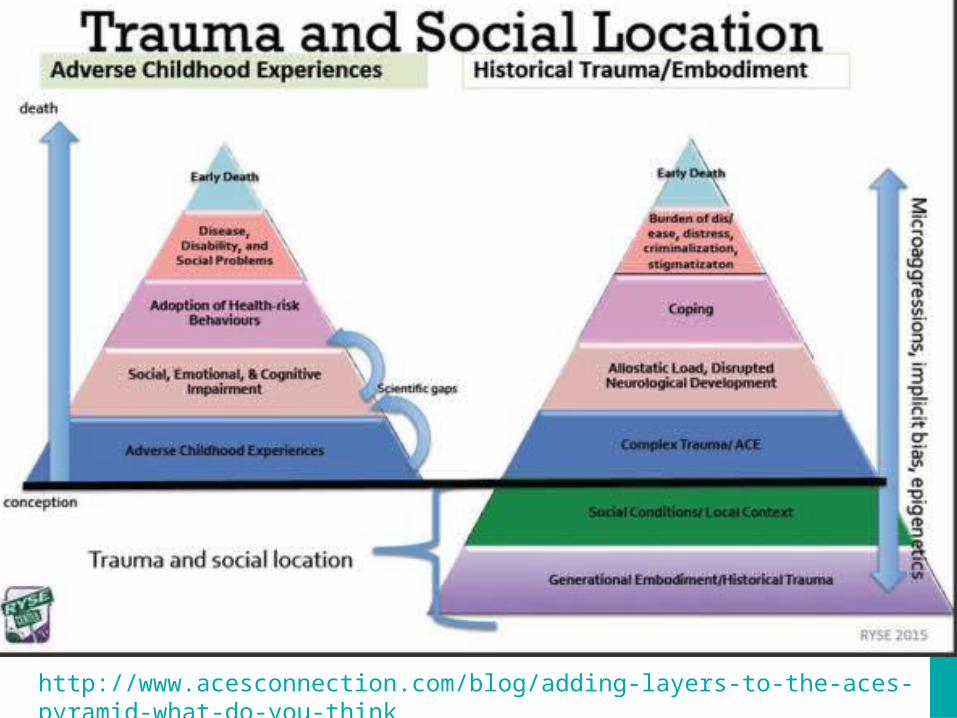
http://www.acesconnection.com/blog/adding-layers-to-the-aces-pyramid-what-do-you-think
WHY DOES TRAUMA HAVE THIS EFFECT?
SO HELP ME UNDERSTAND….
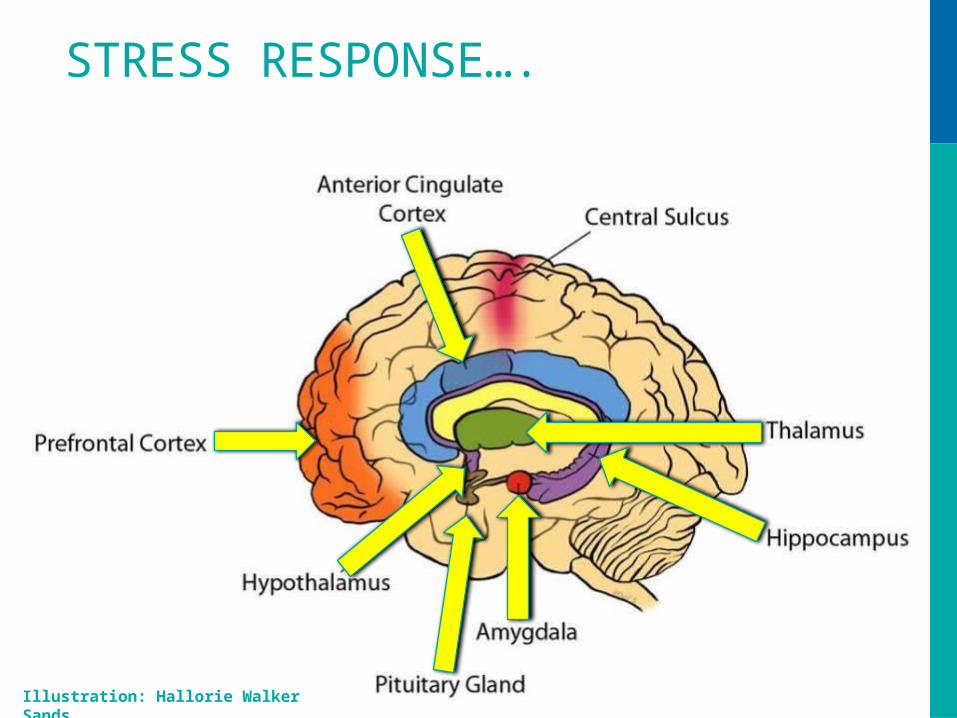
STRESS RESPONSE….
Illustration: Hallorie Walker Sands
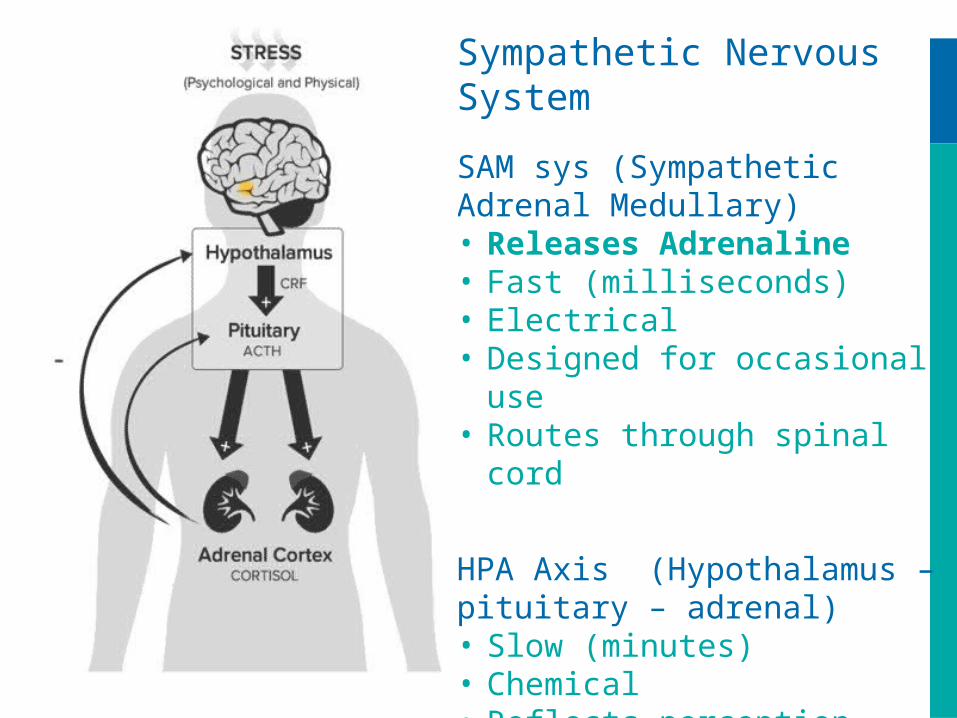
Sympathetic Nervous System
SAM sys (Sympathetic Adrenal Medullary)• Releases Adrenaline• Fast (milliseconds)• Electrical• Designed for occasional use• Routes through spinal cord
HPA Axis (Hypothalamus – pituitary – adrenal)• Slow (minutes)• Chemical• Reflects perception• Releases cortisol
ENVIRONMENT BRAIN BEHAVIOR
Input from the environment• vision, hearing, smell, taste, touch
In between stuff – mental activities• Perception, attention, memory, learning
Output in the environment (Behavior)• Smiling, laughing, yelling, fighting, eating, listening, speaking,
walking
WHY

• Long-term memory• Learning• Judgment• Problem solving• Decision making
•Survival functions
• Incoming sensory
•Orienting attention
•Reflexive Perception (e.g. startle)
• Perception• Selective
attention• Working
Memory
Downstairs BrainBefore conscious awareness; reflexive
Behavior
MezzanineCognition/Conscious awareness
Upstairs BrainHigher level thinking
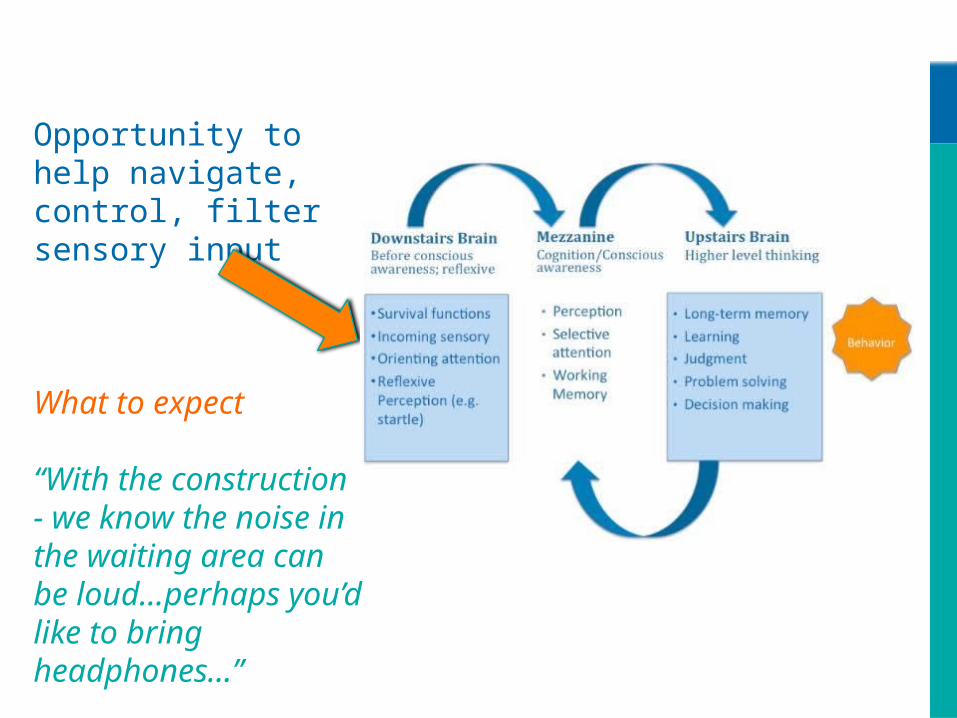
Opportunity to help navigate, control, filter sensory input
What to expect
“With the construction - we know the noise in the waiting area can be loud…perhaps you’d like to bring headphones…”
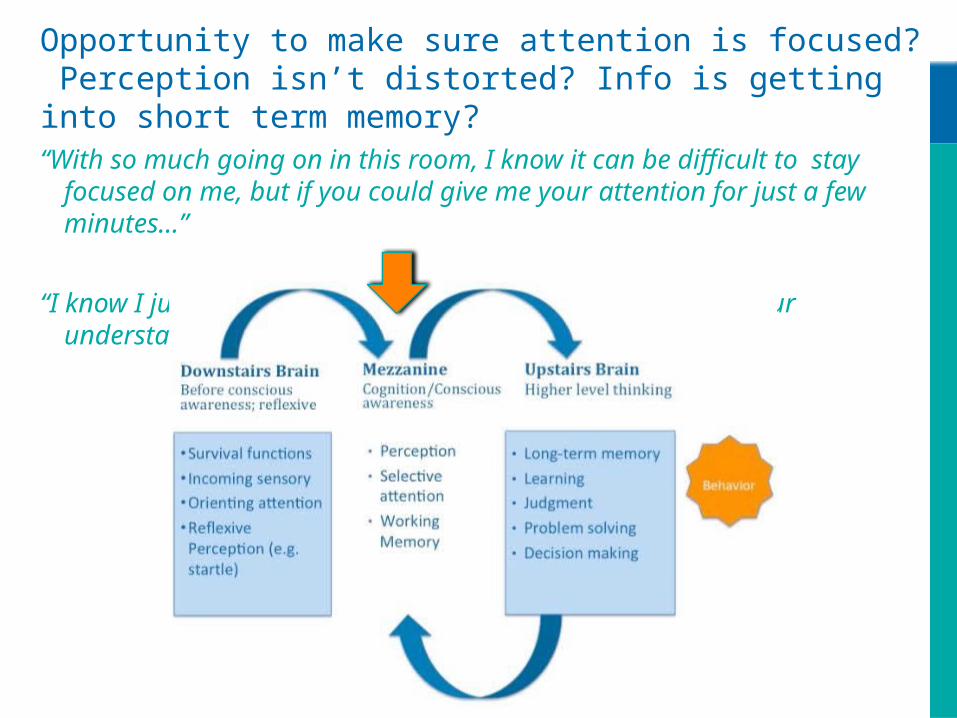
Opportunity to make sure attention is focused? Perception isn’t distorted? Info is getting into short term memory?“With so much going on in this room, I know it can be difficult to stay focused on
me, but if you could give me your attention for just a few minutes…”
“I know I just gave you a lot of information, can you tell me your understanding of next steps”
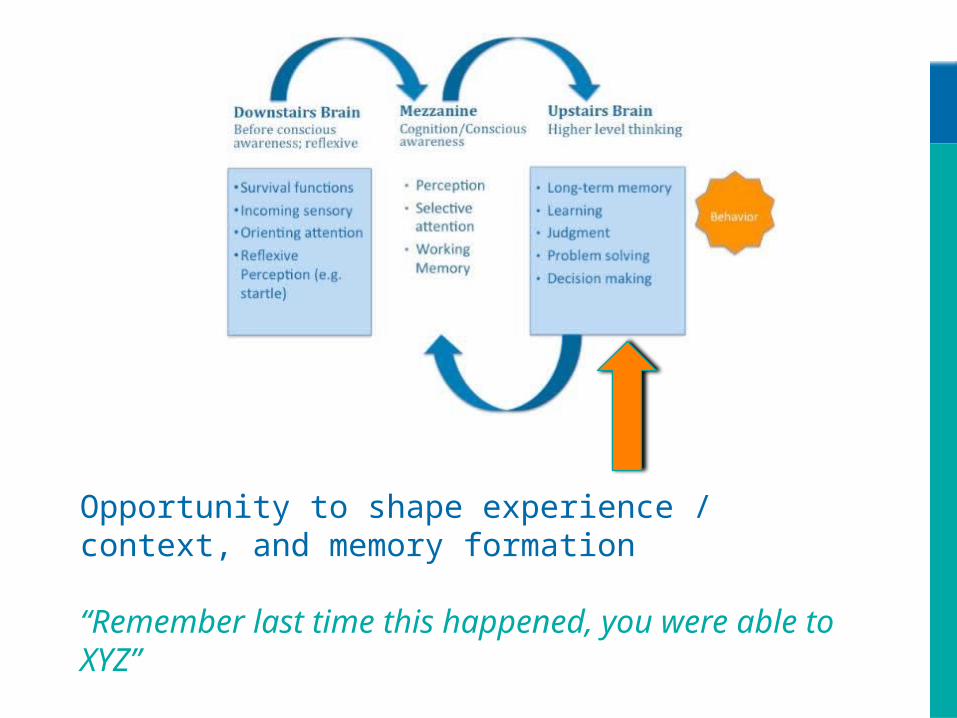
Opportunity to shape experience / context, and memory formation
“Remember last time this happened, you were able to XYZ”

SENSORY AND THE TRAUMA BRAIN
• More sensitive to incoming sensory information
• Sensory information act as triggers
• Top down input may be distorted – not available
Connecting to behavior: Do you notice survivors are more aware or bothered by sensory input?

• Divided attention is better –hyper vigilance and the ability to pay attention to a lot of stimuli at once
• Selective attention is worse in general but better for threatening stimuli
• Sustained attention worse
Connecting to behavior: Do you notice survivors have a harder time focusing attention? Are they easily distracted?
ATTENTION AND THE TRAUMA BRAIN
• Memory for facts, information, and episodes is impaired – damage to hippocampus
• Working memory is usually not great – frontal lobe activation is decreased
• HOWEVER - Implicit memory is strong for threatening stimuli
• Connecting to behavior: Do survivors forget appointments, treatment plans, what was discussed last time? But, is their memory for threat situations or details good?
MEMORY AND THE TRAUMA BRAIN
• Frontal lobe function is impaired – affecting judgment, decision making, planning, reasoning
• Poorer regulation - attention and impulse control • Anxiety related, perseverative loops
Connecting to behavior: Do survivors perseverate, fixate? Do they show problems with impulse control? Struggle with making decisions or planning
EXEC FUNC AND THE TRAUMA BRAIN
Past experiences, motives, contexts, or suggestions prepare us to perceive in a certain way
(Perceptual Expectancy)
“We don’t see things as they are. We see them as we are”
Anais Nin
PROCESSING – TOP DOWN

OUR WORK IS TO
Prevent re-traumatization – triggers
Recognize early warning signs
• Know your work/population
Intervene – deescalate
WHEN TRAUMA HAPPENS….
Freeze, Flight, Fight, Fright
Complex trauma - Chronic Trauma overtime
Traumatic Stress – Toxic stress
How does this “look” in parents, families, children? In staff?
CLIENTS MAY…
• Feel unsafe
• Engage in harmful behaviors
• Tend toward anger and aggression
• Feel hopeless or helpless
• Continue unhelpful patterns of behavior
• Feel hyper aroused with memory and communication problems
• Have trouble managing emotions
• Be overwhelmed, confused, depressed
• Not be able to imagine any other future

EARLY WARNING SIGNS
• Bouncing leg
• Fist clenching
• Hand wringing
• Giggling or other emotional responses (inappropriate)
• Pacing
• Loud voice
• Can’t sit still
• Restlessness
• Swearing

WHEN TRAUMA HAPPENS….
Central Nervous System becomes unbalanced
Parasympathetic Nervous Sys:Rest and Digest
Sympathetic NS:Arousal system Fight or Flight

TRAUMA AND THE BRAIN
Over-developed amygdala (limbic system).
• Fight, flight, or freeze reactions
Under-developed frontal lobe.
• Harder to bring on-line when amygdala is working so hard
The good news?
• The brain is plastic; rewiring is possible.• Healing/recovery are possible

SOCIAL, EMOTIONAL, COGNITIVE
Emotional Reactions• Feelings – emotional regulation• Alteration in consciousness• Hypervigilence
Psychological and Cognitive Reactions• Concentration, slowed thinking, difficulty with
decisions, blameBehavioral or physical
• Pain, sleep, illness, substance abuseBeliefs
• Changes your sense of self, others, world• Relational disturbance
INTERGENERATIONAL
Prenatal stress can affect HPA axis function
• Early and chronic abuse is associated with permanent sensitization of HPA axis
Trans generational Transmission of Trauma
• Lower cortisol levels in mothers and babies of mothers who developed PTSD following World Trade Center attacks
• In rats, exposure to high levels cortisol prenatally (3rd trimester) associated with low birth weight, hypertension, glucose intolerance as adults
Care and Attachment can Buffer Trauma/ Stress
• Early care (tactile) leads to a reduction of CRH neurons in hypothalamus (Karsten & Baram, 2013) – must be recurrent
INTERGENERATIONALLY – TRAUMA ….
Changes neurobiology and DNA
Affects caregiving attachment / bonding
Provides a narrative that is learned and carried on

NEUROBIOLOGY TAKE AWAYS
Attention can be a problem:
• Amygdala in survivors is hyper-vigilant – scanning for real or perceived threat; attentional control from frontal lobe is decreased
Communication is challenging: dominance of RH
• Decreased verbal (left hemisphere) – hypersensitive to nonverbal (right hemisphere) – prone to misinterpret.
Memory is impaired – damage to hippocampus due to excess cortisol:
• Explicit memory (hippocampus) – facts, stories, pictures – impaired
• Implicit memory (amygdala – acute trauma) often clear and sharp

Our brains change and welcome change.
Positive interactions which communicate safety and connection are foundational to changing unproductive brain patterns.
Every interaction the survivor has with a provider system has the potential of
• adding to the trauma experiences, • reactivation of trauma memories, • or providing a sense of safety and enhancing emotional
regulation.
MORE TAKE AWAYS

ACTIVITY
Through a trauma lens…
education statements
A TRAUMA LENS
What might the NON Trauma informed system say about this person?
Using a trauma lens – what could be going on?
1.
2.
3.
TRAUMA EDUCATION STATEMENT:
What we know about trauma is __[that trauma survivors often started using substances]__ because/to [either prevent feeling greater pain, to feel something, or because it was forced onto them
You are meeting with Kiesha to complete paperwork for services she requested. She keeps rustling through her bag while your talking, looking outside your office, and checking her phone. She can’t seem to settle down and focus.
Jack calls all of his providers, multiples times. The calls are often about the same thing. He is often asking for tangible goods & can be verbally aggressive. For example last week he called requesting bus tickets. One of his providers said “I think I can get you some” but he kept calling the other providers.
Pat agrees to MH counseling in a team mtg but “no shows” for the intake. During follow-up she states she is very interested but “no shows” again.
Tim is completing an intake for your services. Your program has several rules and protocols that need to be followed to successfully complete. Tim’s referral states that he has difficulty with authority and following rules and doesn’t accept help from others.
Sue successfully completed her substance abuse treatment program. Part of the safety plan for her to have her 4 y/o is no contact with her abuser. While out one day she runs into her ex-partner who was abusive. Her DHS worker finds out, confronts her about it and she doesn’t tell the truth saying “it never happened”.
BREAK

JUST BREATHEJULIE BAYER SALZMAN & JOSH SALZMAN
(WAVECREST FILMS)
JUST BREATHE
HOW DO I DO THIS?
SO HELP ME UNDERSTAND….
THE FOUNDATION
Trauma Awareness
• Trauma education and training for all staff;• Hiring, management, and supervision practices;• Policies and procedures for referral, intake,
termination;• Universal precaution and/or universal
screening;• Recognition of vicarious trauma and the
appropriate care of staff;• Knowledge of effective trauma recovery
services;
THE FOUNDATION
Understanding impact of historical trauma and all forms of oppression
• Ongoing training for all staff• Ongoing inclusion of consumer voice• Procedures and practices that promote
and sustain accountability
PRINCIPLES OF PRACTICE
With a foundation of awareness and understanding
Organizations can strive to reflect three central principles of TIC, by creating policies, procedures, and practices that:
• create safe context,• restore power, and• value the individual.
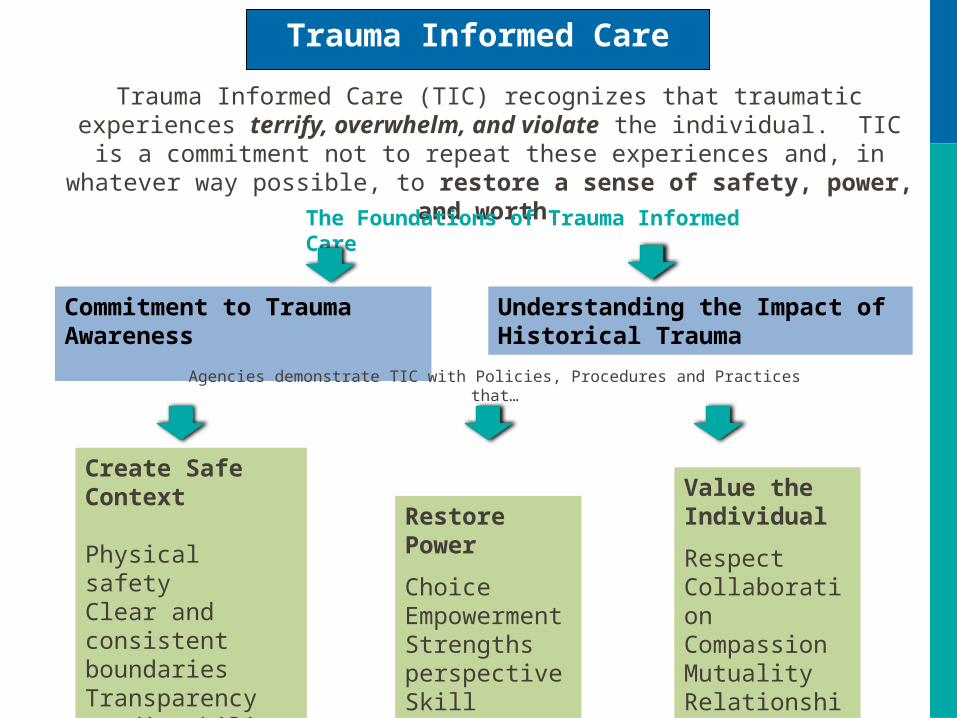
Trauma Informed Care
Trauma Informed Care (TIC) recognizes that traumatic experiences terrify, overwhelm, and violate the individual. TIC is a commitment not to repeat these experiences and, in
whatever way possible, to restore a sense of safety, power, and worth.
The Foundations of Trauma Informed Care
Commitment to Trauma Awareness Understanding the Impact of Historical Trauma
Agencies demonstrate TIC with Policies, Procedures and Practices that…
Create Safe Context
Physical safetyClear and consistent boundariesTransparencyPredictabilityChoice
Restore Power
ChoiceEmpowermentStrengths perspectiveSkill building
Value the Individual
RespectCollaborationCompassionMutualityRelationship
NON-TRAUMA INFORMED SERVICES
• Consumers are labeled as manipulative, needy, disabled, attention seeking
• Misuse or overuse of displays of power-keys, security, demeanor
• Culture of secrecy – no advocates, poor staff monitoring
• expectations
• Patient compliance vs collaboration
• Staff disempowered then pass on …
• SU has to show interest….motivation
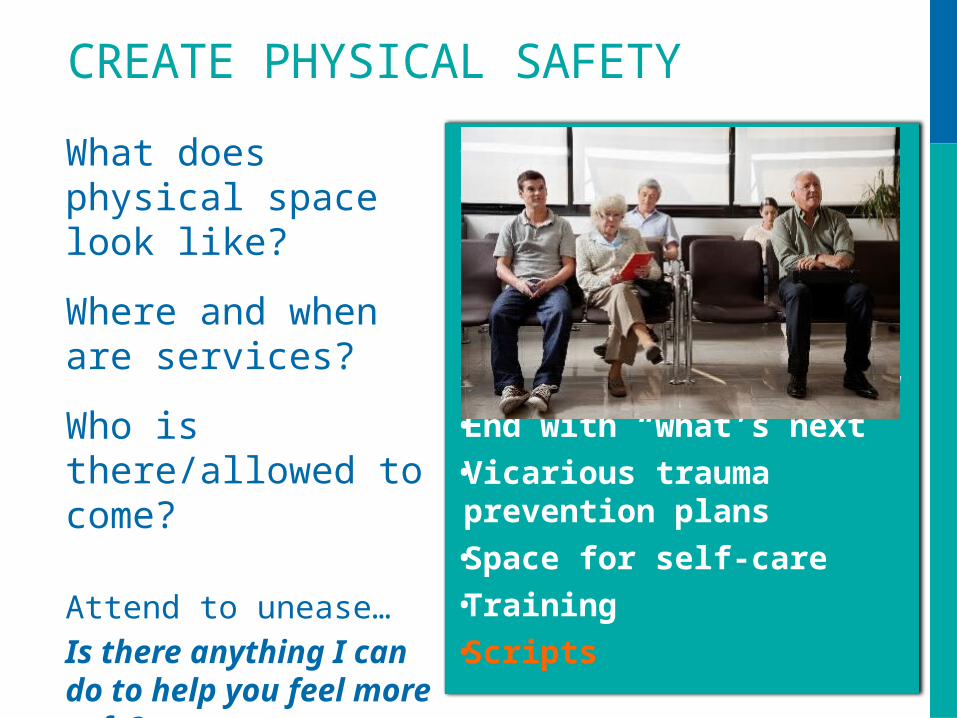
CREATE PHYSICAL SAFETY
What does physical space look like?
Where and when are services?
Who is there/allowed to come?
Attend to unease…Is there anything I can do to help you feel more safe?
• Lighting• Bathrooms• Exits/entrances• Signage about what to
expect, where to go…• Home visiting plans.• End with “what’s next” • Vicarious trauma
prevention plans• Space for self-care• Training• Scripts

CREATE EMOTIONAL SAFETY
Transparency• Explain the “why”• Clear and specific language
Predictability• What’s next
Clear & consistent boundaries• Be able to state and model• Allowed to speak up re:
vicarious trauma• Vicarious trauma
prevention plansChoice
• Understanding your role
• Being able to say no.
• Access to records
• Access to job expectations before hire
• Psy evals and assessments
CREATE EMOTIONAL SAFETY
• Understanding your role
• Being able to say no.
• Access to records
• Access to job expectations before hire
• Psy evals and assessments
RESTORE POWER
Empowerment
• Advocate, modelChoice
• As much as possible• Keep it real; explain the
whyStrengths Perspective
• Adaptability• Focus on the future
Skill building
• Every encounter
Things to think about
• Learned Helplessness
• Competence & confidence
• 3 choices
• Relationships not used as threat
• Frontal lobe
• Peer Support

VALUE THE INDIVIDUAL
Respect• Life experience and strengths
Collaboration• Referrals, teams, meetings
Compassion• Not an excuse but an explanation• Self Care
Relationship, Mutuality, Authenticity
• Modeling, boundaries, learning, partnering
Things to think about
•Structure to have voices heard
•Acknowledgement
•Giving voice to –
•Advocating for…
ACTIVITY
Rescue or throw your colleague under the bus

Your client is in the lobby and is pacing - seems unable to settle down and keeps asking for water.
Colleague says:
“You should give her a surprise UA”
Correction:
I understand what you are saying but I also know that our offices often make people feel unsafe because of why they are here or because they are triggered by the smells and sounds so I will check in with her and assess her sense of safety…..

You’re in a group setting and a member says “I can only calm down by drinking or smoking pot and taking the Klonapin my psychiatrist gave me.”
Colleague says:
“Does your psychiatrist know you’re drinking and smoking pot? That sounds really dangerous, especially since you’re also taking Klonapin!”
Correction:
It sounds like it is hard to get your body to calm down and you have found that what works is… I have some concern about mixing the Klonapin and wonder if you could talk to your dr….
John is a new member to group and on the first day he moves a chair out of the circle and puts it near the door to sit.
Colleague says:
“Sorry dude. This is not an “all about John” group. If you want to get credit for being here I suggest you bring your chair back and join the group. ”
Correction: acknowledge common fears, options and group inclusiveness – respond to the co-worker without putting John on the spot. “Sometimes it takes people a little while to feel safe with a new group…”

“You are asking me about my abuse history, what about you, have you experienced abuse?”
Colleague says:
“We are not here to talk about me. It’s not appropriate for me to answer that ”
Correction:
This is a common question people ask, often to find out if we can relate and whether we’re ok. It is hard to not be touched by trauma, and we do support each other, but I am going to leave it there for now because I don’t want you to feel you can’t share with us [me] because you worry about triggering us [me]
TRAUMA INFORMED CARE
ON THE GROUND
Restorative Justice
Positive behavioral supports
Reduced expulsions/suspensions, eliminating the need for the alternative school.
How is this trauma informed?
• Attending to the whole person, recognizing strengths, bringing compassion first.
IN THE SCHOOLS…

Resident Council formed
Clients invited to negotiate for changes in rules and policies
What about TIC?
• Respect, collaboration, strengths-based, empowering
IN ADDICTIONS TREATMENT…
“Many of the policies and procedures currently in place at the WRC were either amended or created by clients.”

Pediatric clinic adopted screening for ACEs to engage parents in a different way
Showing compassion, building relationship, increasing sense of safety, collaboration
IN HEALTHCARE…
After an assessment -themes of Physical Safety, Confidentiality, Transparency, & Choice.
• more private interview spaces, improved lighting, gender neutral bathrooms –key access.
• Measure progress in “ways that honor client choice”
• Consumer Satisfaction Survey changed
IN AN ANTIPOVERTY AGENCY…
“All sites were assessed for safety, welcoming environment, and confidentiality.”
Staff developed & delivered TIC presentations
• for the Board• for departments
Hiring and onboarding practices
Yoga classes, 5 day in a row vacation, transparency/appreciation meetings
IN HOUSING…
“It’s definitely starting to infuse more into the daily part of our jobs, but it’s always a work in process (which I think is how it should be always considered….)”
Creating physically welcoming environments
• Attend to sense of safety and care for clients
• A different experience for staff as well
IN DHS BRANCH OFFICES…
Wrote agency-wide policy for TIC
Staff Wellness Plans
Altered physical environment to include and integrate peer supports
IN A MENTAL HEALTH CLINIC…

Staff Training and Information• Common language• Motivation, buy-in
Management support• Early & Ongoing Commitment
TIC Workgroup• Assess• Prioritize
• Communicate• Recommend
HOW DID THEY DO IT?
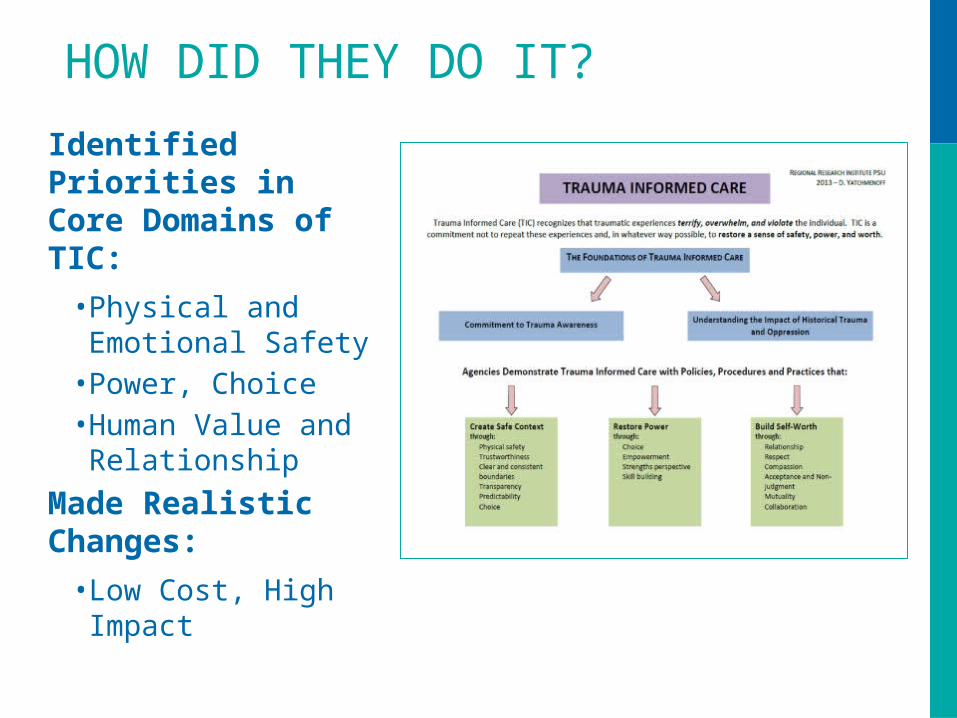
Identified Priorities in Core Domains of TIC:
• Physical and Emotional Safety
• Power, Choice• Human Value and
Relationship
Made Realistic Changes:
• Low Cost, High Impact
HOW DID THEY DO IT?

A CULTURE OF TIC
Involves all aspects of program activities, setting, relationships, and atmosphere (more than implementing new services).
Involves all groups: administrators, supervisors, direct service staff, support staff, and consumers.
Involves making trauma-informed change into a new routine, a new way of thinking and acting.

WHAT DIFFERENCE DOES IT MAKE?
• Service Recipients can participate in their own care.
• Service Recipients gain skills for self-regulation and self-advocacy.
• Service Recipients can remain engaged even when there are bumps in the road.
• The work is more rewarding for staff.
• Vicarious trauma/worker stress is reduced.
The National Center for Trauma-Informed Care and Alternatives to Seclusion and Restraint (NCTIC)
http://www.samhsa.gov/nctic National Association of State Mental Health Program Directors
http://www.nasmhpd.org/TA/nctic.aspxTrauma-Informed Organizational Toolkit – The National Center on Family Homelessness
http://www.familyhomelessness.org/media/90.pdfNational Center for Domestic Violence, Trauma & Mental Health
http://www.nationalcenterdvtraumamh.orgNational Child Traumatic Stress Network
http://www.nctsn.org/National Council for Community Behavioral Healthcare- Trauma Informed BHC
http://www.thenationalcouncil.org/wp-content/uploads/2012/11/NC-Mag-Trauma-Web-Email.pdfThe National Institute for Trauma and Loss in Children
https://www.starr.org/training/tlcThe National Association of States Directors of Developmental Disabilities Services
http://www.nasddds.org/resource-library/behavioral-challenges/mental-health-treatment/trauma-informed-care/national-center-for-trauma-informed-care/
National Center for Social Work Trauma Education and Workforce Development
http://www.ncswtraumaed.org/Chadwick Center for Children and Families
http://www.chadwickcenter.org/CTISP/ctisp.htm
NATIONAL HAPPENINGS

Trauma Informed Oregon website
traumainformedoregon.org
THANK YOU!
Stephanie Sundborg

















