38
1 By. Ms. Shanta Peter
| Date post: | 16-Jul-2015 |
| Category: |
Healthcare |
| Upload: | shanta-peter |
| View: | 235 times |
| Download: | 3 times |

1
By. Ms. Shanta Peter
Shock
“A momentary pause in the act of
death.”John Collins Warren, 1800s
“Shock is a symptom of its cause.”
Isolated head injury does not cause shock

Categories of Shock
• HYPOVOLEMIC
• CARDIOGENIC
• DISTRIBUTIVE
• OBSTRUCTIVE

Goals of Shock
Resuscitation
• Restore blood pressure
• Normalize systemic perfusion
• Preserve organ function

Time to Trauma Death
• 50% deaths occur at scene within minutes:– CNS injury 40-50%– Hemorrhage 30-40%
• 50% after hospital arrival:– 60% die within first 4 hrs– 84% die within first 12 hrs– 90% die within first 24 hrs
• Hemorrhage accounts for 50%Deaths in the
first 24 hours
Hemorrhagic Shock Definition
Hemorrhagic Shock
–Reduction in tissue perfusion below that necessary to meet metabolic needs
Inadequate Perfusion
6
Confounding Factors In Response To Hemorrhage
• Patients age
• Pre-existing disease / meds
• Severity of injury
• Access to care
• Duration of shock• Amount pre-hospital fluid-EMS
• Presence of hypothermia
7
Treatment of Traumatic shock
Compensated Traumatic shock :
Easy recovery with appropriate resuscitative measures
• Decompensated Traumatic Shock :
Cellular damage – secondary to hypo-perfusion, toxic metabolic effects
Reversible but recovery period is extended
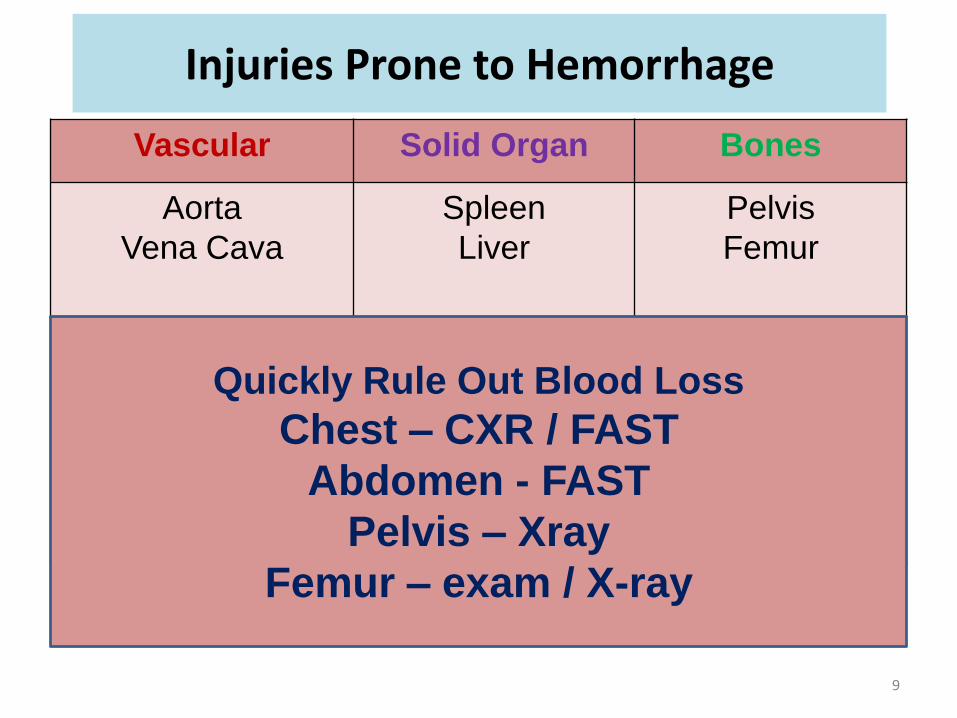
Injuries Prone to Hemorrhage
Vascular Solid Organ Bones
Aorta
Vena Cava
Spleen
Liver
Pelvis
Femur
Quickly Rule Out Blood Loss
Chest – CXR / FAST
Abdomen - FAST
Pelvis – Xray
Femur – exam / X-ray
9
Classic Signs & Symptoms of Shock
• Change in mental stability
• Tachycardia
• Cool, clammy, skin
• Prolonged capillary refill
• Narrow pulse pressure
• Hypotension
• Decreased urine output
10

Treating Hemorrhagic Shock- 6 Steps
• Step 1: Optimize oxygenation – Airway management
• Step 2: Identify and control immediate threats to central perfusion.
• Step 3: Identify and assess severe intracranial injuries.
• Step 4: Identify and control potentially life-threatening thoracic and abdominal injuries.
• Step 5: Identify and control potentially limb
threatening injuries.
• Step 6: Identify and treat non-critical injuries. 11
HemorrhagicShock
Assessment12

• pH• Serum Lactate• Base Deficit• Echocardiography• Arterial Wave –
Analysis (Art line)
• Mentation
• Skin Perfusion
• Pulse
• Blood Pressure
• Pulse Pressure
• Shock Index
• Urine Output
Init
ial A
ss
es
sm
en
t
Re
su
sc
ita
tio
n E
nd
po
ints
Assessment Vs. Resuscitation Endpoints
13
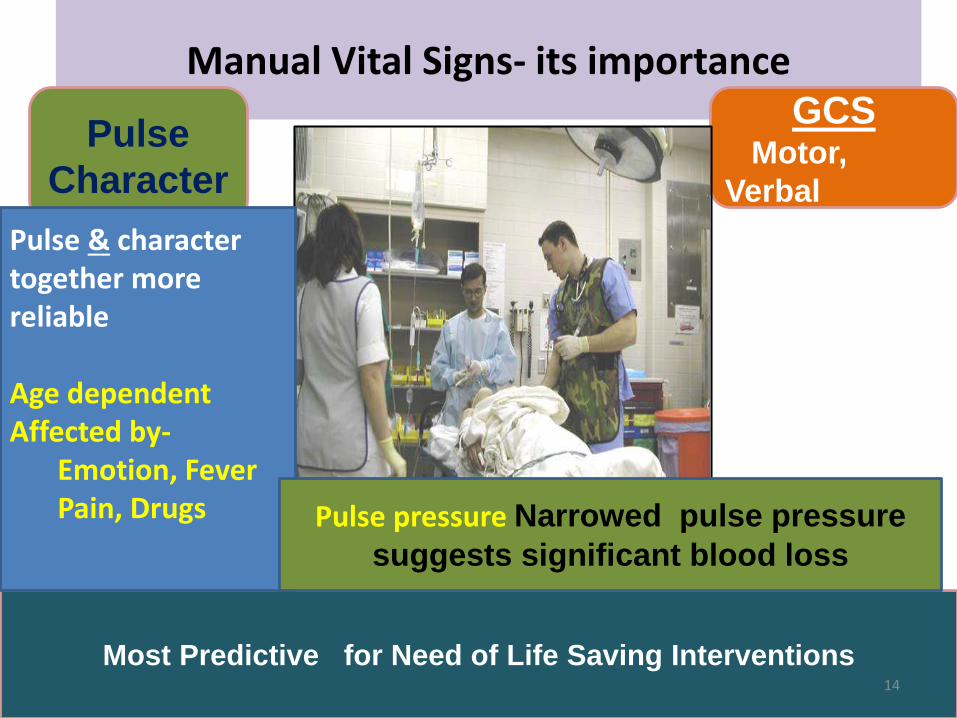
Manual Vital Signs- its importanceGCS
Motor,
Verbal
Pulse
Character
Most Predictive for Need of Life Saving Interventions
Pulse & character together more reliable
Age dependentAffected by-
Emotion, FeverPain, Drugs Pulse pressure Narrowed pulse pressure
suggests significant blood loss
14
Permissive Hypotension
• Many hypothesize that one should not raise blood pressure
to more than ¾ of pre-injury levels (~80 mmHg).
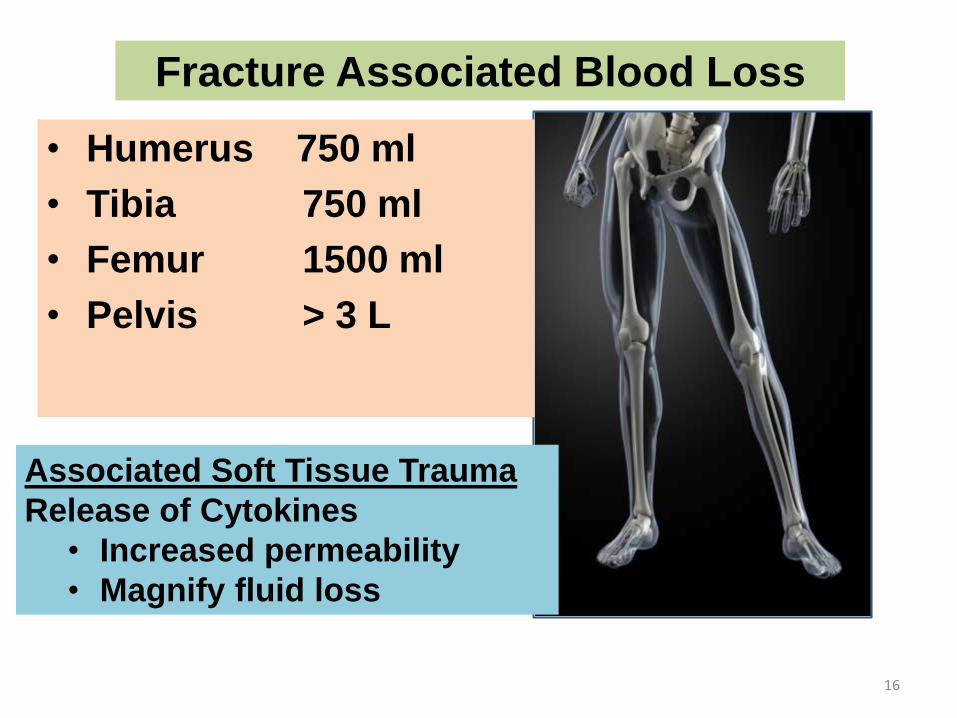
• Humerus 750 ml
• Tibia 750 ml
• Femur 1500 ml
• Pelvis > 3 L
Fracture Associated Blood Loss
Associated Soft Tissue Trauma
Release of Cytokines
• Increased permeability
• Magnify fluid loss
16
Assessing for Sources of Hemorrhage
• Chest radiography: – Tension pneumothorax? Massive hemothorax?
Aortic injury?
• Pelvis radiography: Pelvic ring disruption?
• Focused Assessment with Sonographyfor Trauma (FAST):– Pneumo/hemo-thorax? Hemo-pericardium?
Hemo-peritoneum?– If positive, then emergency laparotomy.– If negative, continue resuscitation, treat other
causes. 17

Practical Diagnosis of Shock
• Perform a targeted physical examination
Diagnostic testing:-
• Chest radiography,
• Pelvis radiography, and
• Bedside ultrasound
• Objective serum makers of tissue perfusion (serum lactate or base deficit)
• Send for CBC, type/cross
• DON’T delay resuscitation for lab results
18
Diagnostic Peritoneal Aspiration (DPA)
Can be done
• if - FAST in blunt abdominal trauma.
• If DPA +ve , then emergency laparotomy.
• If DPA –ve , then seek and treat other sources.
– Perform serial abdominal exams.
– Perform serial FAST exams.
– If patient stabilizes, then CT.
• Get surgery involved!
19
FAST Algorithm
• Unstable patient + FAST OR.
• Stable pt + FAST abdominal CT.
• Stable pt, low mechanism of injury ,
- FAST observation, serial exams.
• CT is the “Gold Standard”.
20

Hypo-perfusion --- Think wisely and explore …Patients don’t suddenly deteriorate !
21
HemorrhagicShock
Lab Values
22
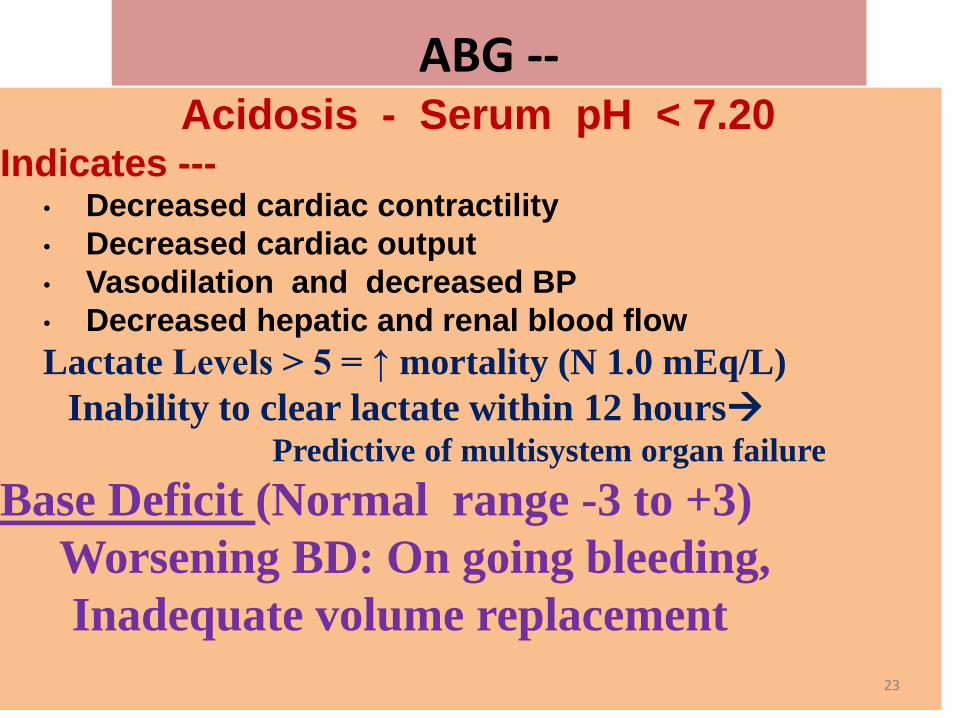
ABG --Acidosis - Serum pH < 7.20
Indicates ---• Decreased cardiac contractility
• Decreased cardiac output
• Vasodilation and decreased BP
• Decreased hepatic and renal blood flow
Lactate Levels > 5 = ↑ mortality (N 1.0 mEq/L)
Inability to clear lactate within 12 hoursPredictive of multisystem organ failure
Base Deficit (Normal range -3 to +3)
Worsening BD: On going bleeding,
Inadequate volume replacement
23

International Normalized Ratio (INR)
Value
Normal 0.8 - 1.2
Anticoagulant Use 2.0 - 3.0
Hemoglobin / HematocritIn Acute blood loss – unreliable
Baseline result to use as comparison
24

Estimate the BP from Pulse ? ( Rough& Quick)
60
70
80
80
• If you can palpate this
pulse---------
you know the SBP is
roughly this number
MAP ..
25

HemorrhagicShock
Treatment
26

IV Access Principles in Shock• Fastest, simplest route best (antecubital)
• Large bore, short length (14-16G,2” length)
• 2 lines -minimum
Optimally
• Two people attempting simultaneously
• Two different sites (above & below diaphragm)
• Two to three sites required per major trauma
• Progression [PIV → Femoral → Subclavian]
• Consider Intraosseous (IO) early as rescue device
27
Avoid IV Access--
• Injured limb
• Distal to possible
vascular wound
• Femoral access with injury below diaphragm
I.V Access in Shock Femoral, Sub Clavian JugularIntraosseous Devices (Temp)
28

Fluid Resuscitation
29

Crystalloids (Isotonic Solutions)
Balanced electrolyte solutions similar to ECF
Rapidly equilibrates across compartments
Only 25% remain in IVS after 17
minutes!
30

Hespan /Hesteril• Plasma volume expander
• 500cc expands blood volume 800cc (Half life is 17 mins)
• Safe and effective at 500cc bolus
• Consider ……..– May cause coagulopathy in large doses (>2L dose)
– Renal tubular dysfunction concern
2-3 L LR500ml
HetastarchEquivalent
31
Treatment of Hemorrhagic Shock
• Type and cross match for 6-8 units of blood -immediately.
(Massive transfusion defined as
> 10 U of PRBCs in 24 hrs)
• Consider use of PRBC to platelet to FFP ratio of 1:1:1
– May result in decreased need for blood products
(Give calcium to prevent citrate toxicity )
32

Hemostatic Resuscitation
• Early diagnosis in ED
• 1:1 ratio (PRBC to FFP)
• Early frequent:
– Cryoprecipitate
– Platelets
• Minimal crystalloids
• Stop the bleeding
33

Component Therapy vs. Whole Blood
1 u PRBC
335ml, Hct 55%
1u Plasma
275ml, 80% Coags
1 u Platelets
50ml, 5.5X1010
Total: 650 ml
Hct 29%
Platelest 88,000
Coag Factors 65%
Whole Blood 500 ml
Hct 38-50%
PLTs 150-400,000
Coag Factors 100%
34
Complications of Transfusion
• Impaired O2 release from Hge
• Immunosuppression + infection
– leuko reduced
• Coagulopathy
• Hypothermia
• Ca, K, pH
• Transfusion-related acute lung injury
• Hemolytic transfusion reaction

Urine Output
Adult 0.5 ml / kg / hour
Child 1.0 ml / kg / hour
Toddler 1.5 ml / kg / hour
Infant 2.0 ml / kg / hour
Emergency Laparotomy Indications
• Peritonism: (symptoms of peritonitis without actual inflammation of peritoneum )
• Free air under the diaphragm
• Significant gastrointestinal hemorrhage
• Hypotension with +ve FAST scan or +ve DPA
Do NOT keep trauma patients if you
lack resources to care for them!
37
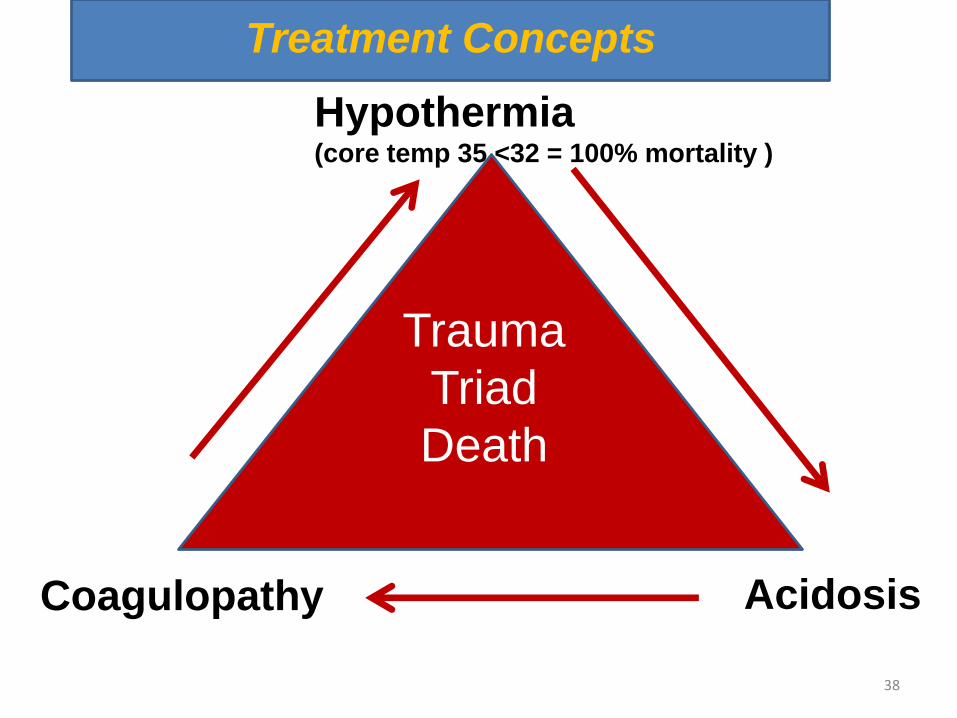
Coagulopathy
Hypothermia (core temp 35 <32 = 100% mortality )
Acidosis
Trauma
Triad
Death
38
Treatment Concepts

















