67
Treating MS in 2014 Professor Gavin Giovannoni Blizard Institute, Barts and The London School of Medicine and Dentistry
| Date post: | 01-Dec-2014 |
| Category: |
Health & Medicine |
| Upload: | gavin-giovannoni |
| View: | 1,292 times |
| Download: | 0 times |

Treating MS in 2014
Professor Gavin Giovannoni
Blizard Institute, Barts and The London School of Medicine and Dentistry

Disclosures Professor Giovannoni has received personal compensation for participating on Advisory Boards in relation to clinical trial design, trial steering committees and data and safety monitoring committees from: Abbvie, Bayer-Schering Healthcare, Biogen-Idec, Canbex, Eisai, Elan, Fiveprime, Genzyme, Genentech, GSK, GW Pharma, Ironwood, Merck-Serono, Novartis, Pfizer, Roche, Sanofi-Aventis, Synthon BV, Teva, UCB Pharma and Vertex Pharmaceuticals.
Regarding www.ms-res.org survey results in this presentation: please note that no personal identifiers were collected as part of these surveys and that by completing the surveys participants consented for their anonymous data to be analysed and presented by Professor Giovannoni.
Professor Giovannoni would like to acknowledge and thank Biogen-Idec, Genzyme and Novartis for making available data slides on natalizumab, alemtuzumab and fingolimod for this presentation.

Is the MS dogma wrong?
immune activation innate and adaptive responses
focal inflammation
BBB breakdown
oligodendrocyte toxicity & demyelination
Acute axonal transection and loss
“autoimmune endophenotype”
axonal plasticity & remyelination
delayed neuroaxonal loss and gliosis
Gd-enhancement
T2 & T1 lesions
brain & spinal cord atrophy
release of soluble markers
Clinical Attack
Disease Progression
Clinical Recovery
- biology
- clinical outcomes
- biomarkers
VIRUS (EBV, HERVs)

Charcot Project: viral aetiology
HIV and lower risk of MS: beginning to unravel a mystery using a record-linked database study
Nexø et al. Epidemiology 2013; 24:331-2
Treatment of HIV and Risk of Multiple Sclerosis
Gold et al. JNNP August 4, 2014 as 10.1136/jnnp-2014-307932.
Raltegravir → RRMS (INSPIRE STUDY) ClinicalTrials.gov ID: NCT01767701

Trial activity targeting progressive pathology
MRI Events
1st clinical attack
Time (Years)
Subclinical disease
Inflammation
Brain volume loss
Neuroaxonal loss
Dis
eas
e S
eve
rity
SPMS RRMS
1st MRI lesion
Relapses
CIS RIS R-SPMS
RIS = radiologically isolated syndrome; CIS = clinically isolated syndrome, RRMS = relapsing-remitting MS; R-SPMS = relapsing secondary progressive MS; SPMS = secondary progressive MS; PPMS = primary progressive MS
SPMS: Natalizumab, Siponimod, DMF
Late SPMS: SMART STUDY fluoxetine, amiloride, riluzole
Early SPMS: oxcarbazepine
CIS: PHENYTOIN RRMS: ? DE-FLAMES STUDY
PPMS
PPMS: Fingolimod, Ocrelizumab, Laquinimod
SP&PPMS: Ibudilast

www.ms-res.org

Questions: DMT perspective
To make an informed decision you need to ask and understand the following questions:
1. Are you sure they have MS?
2. What types of MS do they have?
3. What prognostic group do they fall into?
4. What is the risk of them not having any treatment?
5. Do they have active MS?
6. Are they eligible for treatment with a DMT?
7. Do they understand the difference between the treatment strategies of maintenance & escalation vs. induction therapy?
8. Will they be adherent on treatment?
9. What is your therapeutic target for them?

Questions: DMT perspective
To make an informed decision you need to ask and understand the following questions:
1. Are you sure they have MS?
2. What types of MS do they have?
3. What prognostic group do they fall into?
4. What is the risk of them not having any treatment?
5. Do they have active MS?
6. Are they eligible for treatment with a DMT?
7. Do they understand the difference between the treatment strategies of maintenance & escalation vs. induction therapy?
8. Will they be adherent on treatment?
9. What is your therapeutic target for them?

What constitutes a useful diagnostic test or set of criteria?
TARGET DISORDER
PRESENT ABSENT
DIAGNOSTIC
TEST RESULT
+ a b a + b
- c d c + d
a + c b + d a + b + c + d
From these we determine the sensitivity and specificity as follows:
SENSITIVITY = a/(a+c) > 80%
SPECIFICITY = d/(b+d) > 80%
Neurobiol Aging 1998; 19:109-116.
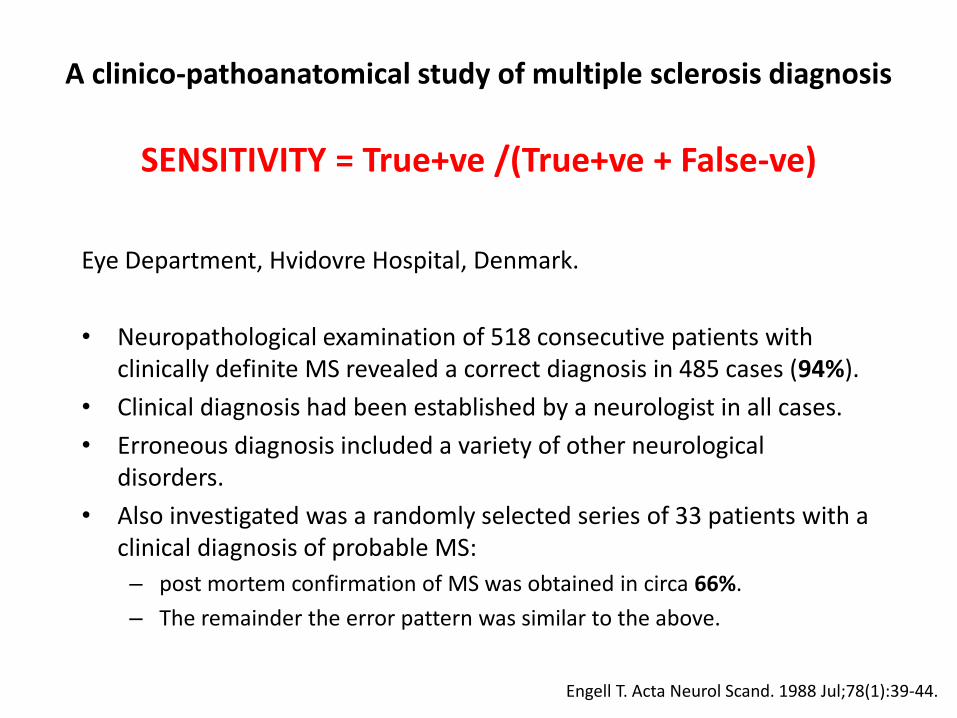
A clinico-pathoanatomical study of multiple sclerosis diagnosis
SENSITIVITY = True+ve /(True+ve + False-ve)
Eye Department, Hvidovre Hospital, Denmark.
• Neuropathological examination of 518 consecutive patients with clinically definite MS revealed a correct diagnosis in 485 cases (94%).
• Clinical diagnosis had been established by a neurologist in all cases.
• Erroneous diagnosis included a variety of other neurological disorders.
• Also investigated was a randomly selected series of 33 patients with a clinical diagnosis of probable MS:
– post mortem confirmation of MS was obtained in circa 66%.
– The remainder the error pattern was similar to the above.
Engell T. Acta Neurol Scand. 1988 Jul;78(1):39-44.

Kleinschmidt-DeMasters,et al. N Engl J Med. 2005 Jul 28;353(4):369-74.
PML complicating treatment with natalizumab and IFNb-1a for MS



A clinico-pathoanatomical study of multiple sclerosis diagnosis
SPECIFICITY = True-ve /(True-ve + False+ve) ?
~25% of cases of MS are undiagnosed in life (asymptomatic or benign cases)
Engell T. Acta Neurol Scand. 1989 May;79(5):428-30.

Other diagnoses - MRI white matter changes
• ADEM
• NMO
• Ageing
• Behcet’s syndrome
• Cerebrovascular disease
• Decompression sickness
• Fat embolism
• HIV encephalitis
• HTLV1-associated myelopathy
• Hydrocephalus
• Irradiation
• Leukodystrophies
• Migraine
• Mitochondrial encephalopathy
• MND
• Neurosarcoidosis
• Phenylketonuria
• PML
• SSPE
• SLE/APL
• Trauma
Miller DH. (1997)

Questions: DMT perspective
To make an informed decision you need to ask and understand the following questions:
1. Are you sure they have MS?
2. What types of MS do they have?
3. What prognostic group do they fall into?
4. What is the risk of them not having any treatment?
5. Do they have active MS?
6. Are they eligible for treatment with a DMT?
7. Do they understand the difference between the treatment strategies of maintenance & escalation vs. induction therapy?
8. Will they be adherent on treatment?
9. What is your therapeutic target for them?

Module Identifier
Question: What types of MS do they have?
Lublin FD, Reingold SC. Defining the clinical course of multiple sclerosis: results of an international survey. National Multiple Sclerosis Society (USA) Advisory Committee on Clinical Trials of New Agents in Multiple Sclerosis. Neurology. 1996 Apr;46(4):907-11.
RRMS R-SPMS/NR-SPMS PPMS RPMS
relapsing forms of MS vs. non-relapsing MS

Questions: DMT perspective
To make an informed decision you need to ask and understand the following questions:
1. Are you sure they have MS?
2. What types of MS do they have?
3. What prognostic group do they fall into?
4. What is the risk of them not having any treatment?
5. Do they have active MS?
6. Are they eligible for treatment with a DMT?
7. Do they understand the difference between the treatment strategies of maintenance & escalation vs. induction therapy?
8. Will they be adherent on treatment?
9. What is your therapeutic target for them?

Question: What prognostic group do you fall into?
Good prognosis Poor prognosis
Young
Female sex
Optic neuritis
Isolated sensory symptom
Full recovery from attack
Long interval to second
relapse
No disability after 5 years
Normal MRI / low lesion load
CSF negative for OCBs
Older age of onset
Male sex
“Multifocal“ onset
Efferent system affected (motor,
cerebellar, bladder)
High relapse rate in the first 2-5 years
Substantial disability after 5 years
Abnormal MRI with large lesion load
CSF positive for OCBs
Adapted from Miller et al., Lancet Neurology 2005: 4; 281-288

Question: What prognostic group do you fall into?
Favourable
Indeterminate
Poor
time Aim of
treatment

Questions: DMT perspective
To make an informed decision you need to ask and understand the following questions:
1. Are you sure they have MS?
2. What types of MS do they have?
3. What prognostic group do they fall into?
4. What is the risk of them not having any treatment?
5. Do they have active MS?
6. Are they eligible for treatment with a DMT?
7. Do they understand the difference between the treatment strategies of maintenance & escalation vs. induction therapy?
8. Will they be adherent on treatment?
9. What is your therapeutic target for them?

Question: What is the risk of not having any treatment?
MS is one of the most common causes of neurological disability in young adults2
Natural history studies indicate that it takes a median time of 8, 20 and 30 years to reach the irreversible disability
levels of EDSS 4, 6 and 7, respectively3
Up to 75% increased annualized divorce rate4
Life expectancy is reduced by 5-10 years5
7.5x greater than suicide rate than the general population6
2 out of 3 patients with RRMS were unemployed due to the disease7
Utilit
y
EDSS Status
EDSS and utilitya show a significant inverse relationship1,b
aUtility measures are derived from EQ-5D using the EuroQoL instrument. bAdapted from Orme et al 2007. Error bars depict 95% confidence intervals. Half points on EDSS are not shown on graph axis, except at EDSS 6.5.
1.Orme M et al. Value In Health. 2007;10:54-60. 2.WHO. 2008.[TK] 3. Confavreaux, Compston. 2005.[TK] 4. Coles et al. 2001.[TK] 5. Confavreaux, Vukusic. 2006.[TK] 6. Sadovnick et al. Neurology 1991;41:1193-6.
7. Morales-Gonzales. Mult Scler. 2004;10:47-54.

Consequences of increasing EDSS scores: loss of employment1
0
10
20
30
40
50
60
70
80
90
Work Capacity by Disability Level
0.0/1.0 2.0 3.0 4.0 5.0 6.0 6.5 7.0 8.0/9.0
EDSS Score
Pro
po
rtio
n o
f P
ati
en
ts ≤
65
Ye
ars
Old
Wo
rkin
g (
%)
The proportion of patients employed or on long-term sick leave is calculated as a percentage of patients aged 65 or younger.
1. Kobelt G et al. J Neurol Neurosurg Psychiatry. 2006;77:918-926;
2. Pfleger CC et al. Mult Scler. 2010;16:121-126.
Spain
Sweden
Switzerland
United Kingdom
Netherlands
Italy
Germany
Belgium
Austria
~10 yrs2

www.ms-res.org

www.ms-res.org

www.ms-res.org

www.ms-res.org

Questions: DMT perspective
To make an informed decision you need to ask and understand the following questions:
1. Are you sure they have MS?
2. What types of MS do they have?
3. What prognostic group do they fall into?
4. What is the risk of them not having any treatment?
5. Do they have active MS?
6. Are they eligible for treatment with a DMT?
7. Do they understand the difference between the treatment strategies of maintenance & escalation vs. induction therapy?
8. Will they be adherent on treatment?
9. What is your therapeutic target for them?

Question: Do you have active MS?
vs.
1
2
3
Clinical
MRI
Biomarkers

Questions: DMT perspective
To make an informed decision you need to ask and understand the following questions:
1. Are you sure they have MS?
2. What types of MS do they have?
3. What prognostic group do they fall into?
4. What is the risk of them not having any treatment?
5. Do they have active MS?
6. Are they eligible for treatment with a DMT?
7. Do they understand the difference between the treatment strategies of maintenance & escalation vs. induction therapy?
8. Will they be adherent on treatment?
9. What is your therapeutic target for them?

Question: Are they eligible for treatment with a DMT?
MSer
Neurologist
Payers
Regulator



Relapsing-MS
Active Inactive Highly-active Rapidly-evolving severe

Active Inactive HA RES

Treatment Selection & treating-2-target
Choosing therapy
X Y Z
Define the Individual’s MS
No
Treatment failure? Yes
• Patient’s preferences?
• Your choice?
Individual measures:
• Evidence of disease activity?
• Tolerability/safety?
• Adherence?
• Drug or inhibitory markers?
Monitoring
• MS prognosis
• Life style and goals
• Shared goals for therapy
Rebaseline
Rebaseline:
• IFNβ, natalizumab, fingolimod,
teriflunomide, DMF=3-6 months
• Glatiramer acetate=9 months
• Alemtuzumab=24 months
DMF=dimethyl fumarate.

Gd
T2
CU
R
DP
15% vs 47% Δ 32%
13% vs 68% Δ 55%
6% vs 37% Δ 31%
Effect of natalizumab on clinical and radiological disease activity in MS: a retrospective analysis of the
Natalizumab Safety and Efficacy in Relapsing-Remitting MS (AFFIRM) study
Havrdova et al. Lancet Neurol. 2009 Mar;8(3):254-60.

Treatment Ladder
1st-line A
1st-line B
1st-line C
1st-line D
1st-line E
2nd-line N
2nd-line M
3rd-line y
3rd-line X

Questions: DMT perspective
To make an informed decision you need to ask and understand the following questions:
1. Are you sure they have MS?
2. What types of MS do they have?
3. What prognostic group do they fall into?
4. What is the risk of them not having any treatment?
5. Do they have active MS?
6. Are they eligible for treatment with a DMT?
7. Do they understand the difference between the treatment strategies of maintenance & escalation vs. induction therapy?
8. Will they be adherent on treatment?
9. What is your therapeutic target for them?

MS is an autoimmune disease hypothesis
15-20 year experiment
“hit hard and early ”
Question: Do you understand the difference between the treatment strategies of maintenance and escalation and induction therapy?
What is your treatment philosophy? maintenance-escalation vs. induction
survival analysis

Questions: DMT perspective
To make an informed decision you need to ask and understand the following questions:
1. Are you sure they have MS?
2. What types of MS do they have?
3. What prognostic group do they fall into?
4. What is the risk of them not having any treatment?
5. Do they have active MS?
6. Are they eligible for treatment with a DMT?
7. Do they understand the difference between the treatment strategies of maintenance & escalation vs. induction therapy?
8. Will they be adherent on treatment?
9. What is your therapeutic target for them?

In MS, patients with long gaps in treatment are at greater risk of relapse than more adherent patients1
Lower adherence to MS therapy is associated with a higher risk of relapse2
Treatment gaps and poor adherence are associated with increased relapse rates
Good adherence
is the key to
optimizing
outcomes
1. Al-Sabbagh A et al. J Neurol 2008;255(Suppl. 2):S79 2. Steinberg SC et al. Clin Drug Invest 2010;30:89-100. Copyright © 2010, Adis Data Information BV MPR, Medication Possession Ratio
Comparison of relapse risk ratios by level of adherence in patients with MS2
80 <80 <75 <70 <65 <60 0.90
0.95
1.00
1.05
1.10
1.15
Rel
apse
ris
k ra
tio
MPR (%)

Forgetfulness is a primary cause of non-adherence
Pain at injection site
Not confident in treatment benefits
Other
Headache
Skin reaction
Depression
Financial reasons
Forgot to administer
Flu-like symptoms
Injection anxiety
Dosing schedule difficult/inconvenient
Weakness
Did not pick up medicine
Nobody available to administer
Pregnancy/planned pregnancy
Did not feel need for injection
Tired of taking injections
Fatigue
50%
20%
17%
15%
13%
12%
10%
10%
10%
9%
8%
6%
5%
4%
3%
2%
2%
1%
0 20 40 60 Patients (%)
Re
aso
ns
for
mis
sin
g o
ne
or
mo
re in
ject
ion
s
Psychological factors
– forgetfulness and
complacency – impact
adherence
Observational GAP study
Devonshire V et al. Eur J Neurol 2011;18:69-77 Patients could have reported more than one reason for non-adherence. When counting injection-related reasons for non-adherence, each patient was counted only once. GAP, Global Adherence Project

Questions: DMT perspective
To make an informed decision you need to ask and understand the following questions:
1. Are you sure they have MS?
2. What types of MS do they have?
3. What prognostic group do they fall into?
4. What is the risk of them not having any treatment?
5. Do they have active MS?
6. Are they eligible for treatment with a DMT?
7. Do they understand the difference between the treatment strategies of maintenance & escalation vs. induction therapy?
8. Will they be adherent on treatment?
9. What is your therapeutic target for them?

No evident disease activity: NEDA
Gd, gadolinium. 1. Havrdova E, et al. Lancet Neurol 2009; 8:254–260; 2. Giovannoni G, et al. Lancet Neurol 2011; 10:329–337.
Treat-2-target
No evidence of disease activity defined as:1,2
× No relapses
× No sustained disability progression
× No MRI activity
× No new or enlarging T2 lesions
× No Gd-enhancing lesions
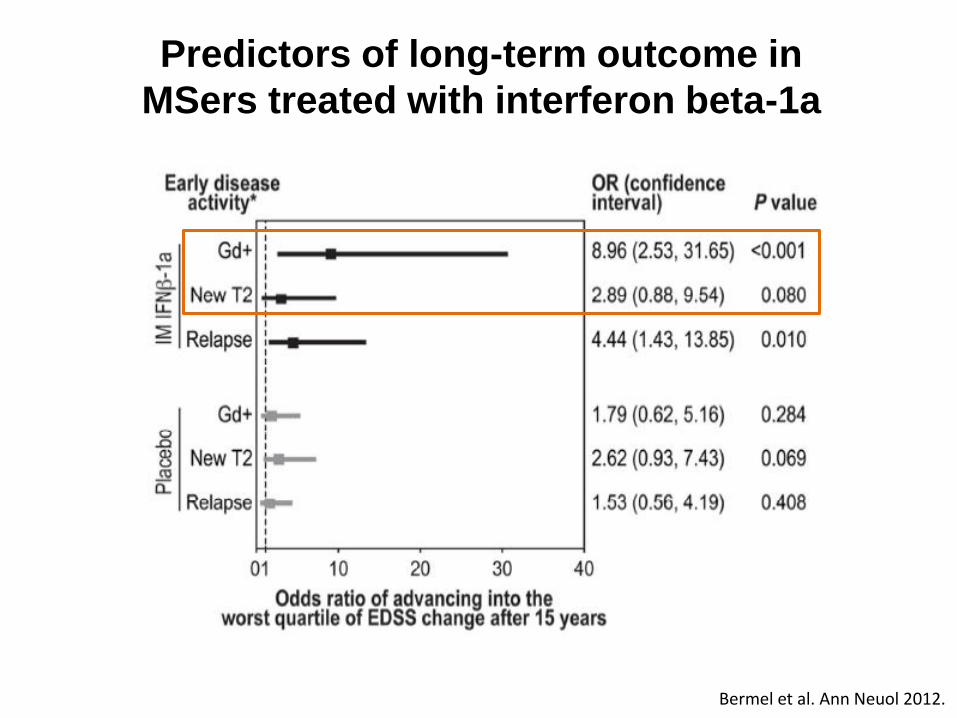
Bermel et al. Ann Neuol 2012.
Predictors of long-term outcome in
MSers treated with interferon beta-1a

MRI to monitor treatment response to IFNβ: a meta-analysis
Dobson et al. Neurology 2013.
Study or Subgroup Odds Ratio
IV, Random, 95% CI
Kinkel 2008
Prosperini 2009
Total (95% CI) 9.86 (2.33, 41.70)
Study or Subgroup Odds Ratio
IV, Random, 95% CI
Kinkel 2008
Pozzilli 2005
Prosperini 2009
Sormani 2011
Total (95% CI) 2.69 (0.72, 10.04)
0.01 0.1 1 10 100 Disease Less Likely Disease More Likely
One New T2 Lesion
Favors Experimental Favors Control
100 10 1 0.1 0.01
Two or More New T2 Lesions

Study or Subgroup Odds Ratio
IV, Random, 95% CI
Kinkel 2008
Rio 2008
Total (95% CI) 5.46 (2.48, 12.04)
MRI to monitor treatment response to IFNβ: a meta-analysis
Study or Subgroup Odds Ratio
IV, Random, 95% CI
Kinkel 2008
Pozzilli 2005
Tomassini 2006
Total (95% CI) 3.34 (1.36, 8.22)
0.01 0.1 1 10 100 Disease Less Likely Disease More Likely
One New Gd+ Lesion
0.01 0.1 1 10 100
Disease Less Likely Disease More Likely
Two or More New Gd+ Lesions
Dobson et al. Neurology 2013.

Strongest predictor of disability progression on
IFNβ therapy is progression itself
Disease activity during 2 years of treatment and prediction of disability progression* at 6 years
Group Sensitivity (%)
(CI) Specificity (%)
(CI)
A. An increase of at least one EDSS step confirmed at 6 months 85 (64–95) 93 (86–97)
B. Occurrence of any relapse 80 (58–92) 51 (41–61)
C. Occurrence of two or more relapses 45 (26–66) 81 (72–82)
D. A decrease in relapse rate less than 30% compared with 2 years before therapy
40 (22–61) 86 (77–91)
E. A decrease in relapse rate less than 50% compared with 2 years before therapy
40 (–61) 81 (72–88)
F. No decrease or identical relapse rate compared with 2 years before therapy
35 (18–57) 88 (79–93)
G. Definition A or B 90 (70–97) 48 (38–58)
H. Definition A or E 85 (64–95) 76 (66–83)
I. Definition A and B 75 (53–89) 97 (91–99)
J. Definition A and E 40 (22–61) 99 (94–99)
*EDSS score ≥6.0 or increase in at least 3 EDSS steps.
Río J et al. Ann Neurol. 2006;59:344-352.

NEDA is a sensitive outcome
1.87
5.29
2.75
2.92
3.41
1.64
2.29
0 1 2 3 4 5 6
Dimethyl fumarate (DEFINE)
Natalizumab (AFFIRM)
Cladribine (CLARITY)
Fingolimod (FREEDOMS)
sc IFN β-1a (DoF)
Teriflunomide (TEMSO)
Alemtuzumab (CARE MS II)
Increase in proportion of NEDA patients relative to comparator
Patients with RRMS over 2 years. Increase in proportion of patients with NEDA versus placebo (except CARE MS II)
All data from post hoc analyses of randomized controlled trials in patients with RRMS. Table adapted from Bevan CJ and Cree BA. JAMA Neurol 2014;71:269-70, with the exception of: TEMSO. Freedman et al. Neurology 2012;78 [Meeting
Abstract s 1]: PD5.007; sc IFN b1-a sc. Data on file; CARE MS II. Coles AJ et al. Lancet 2012;380:1829-39
versus sc IFN b-1a
Slide courtesy Prof. Mark Freedman, EFNS-ENS Istanbul 2014

The modified Rio score can predict disability progression and response to IFN-β therapy
*No qualifying relapses or confirmed EDSS progression; †Percentage calculated using total number of patients with a particular modified Rio score at Week 48; ‡No clinical activity, gadolinium-enhancing lesions, or new/enlarging T2 lesions. EDSS, Expanded Disability Status Scale
Outcomes after 1 year of IFN-β treatment Modified Rio score
≤5 new T2 lesions and 0 relapses 0
≤5 new T2 lesions and 1 relapse, or >5 new T2 lesions and 0 relapses 1
≤5 new T2 lesions and ≥2 relapses, or >5 new T2 lesions and 1 relapse 2
>5 new T2 lesions and ≥2 relapses 3
Higher modified Rio score predicts greater risk of progression1
Modified Rio score at Week 48 (REGARD)
Clinical activity-free* at Week 96 n (%)†2
Disease activity-free at Week 96 n (%)‡2
Yes No Yes No
0 (n=156) 121 (77.6) 35 (22.4) 53 (34.0) 103 (66.0)
1 (n=42) 3 (7.1) 39 (92.9) 0 42 (100)
2 (n=5) 0 5 (100) 0 5 (100)
Total (N=203) 124 79 53 150
Wo
rse
nin
g d
ise
ase
1. Sormani MP et al. Mult Scler J 2013;19:605-12 2. Freedman M et al. Mult Scler J 2013;19(Suppl. 1):262 [P610]
Slide courtesy Prof. Mark Freedman, EFNS-ENS Istanbul 2014

*As measured by modified Rio score. EDSS, Expanded Disability Status Scale; RRMS, relapsing–remitting MS; tiw, three times weekly
Faster disability progression seen in patients with worse Rio-defined disease activity*
Kaplan–Meier cumulative incidence curves of time to confirmed EDSS progression by modified Rio score in patients with RRMS receiving sc IFN β-1a 44 µg tiw
156 42
155 41
151 39
144 33
138 27
No. of patients at risk: Rio score 0 Rio score 1
Baseline Week 24 0.0
0.1
0.2
Cu
mu
lati
ve in
cid
en
ce
0.3
0.4
0.5
Week 48 Week 72 Week 96
O (n=156) 1 (n=42)
Rio score group
Time to 3-month EDSS confirmed progression
Freedman M et al. Mult Scler J 2013;19(Suppl. 1):262 [P610]
Slide courtesy Prof. Mark Freedman, EFNS-ENS Istanbul 2014

Relapses
Unreported relapses
Clinical disease progression
Subclinical relapses: focal MRI activity
Focal gray and white matter lesions not detected by MRI
Brain atrophy
Spinal fluid neurofilament levels
MS Iceberg
Clinical activity
Focal MRI activity
Hidden focal and diffuse MRI activity
Microscopic or biochemical pathology
Biomarkers

Control Multiple sclerosis
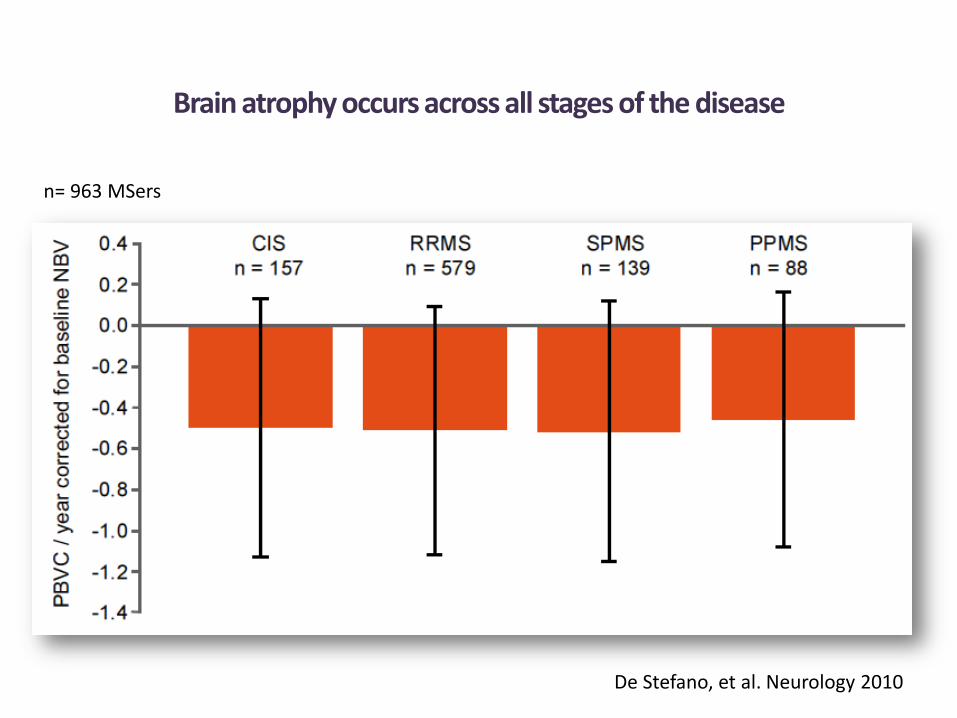
Brain atrophy occurs across all stages of the disease
De Stefano, et al. Neurology 2010
n= 963 MSers
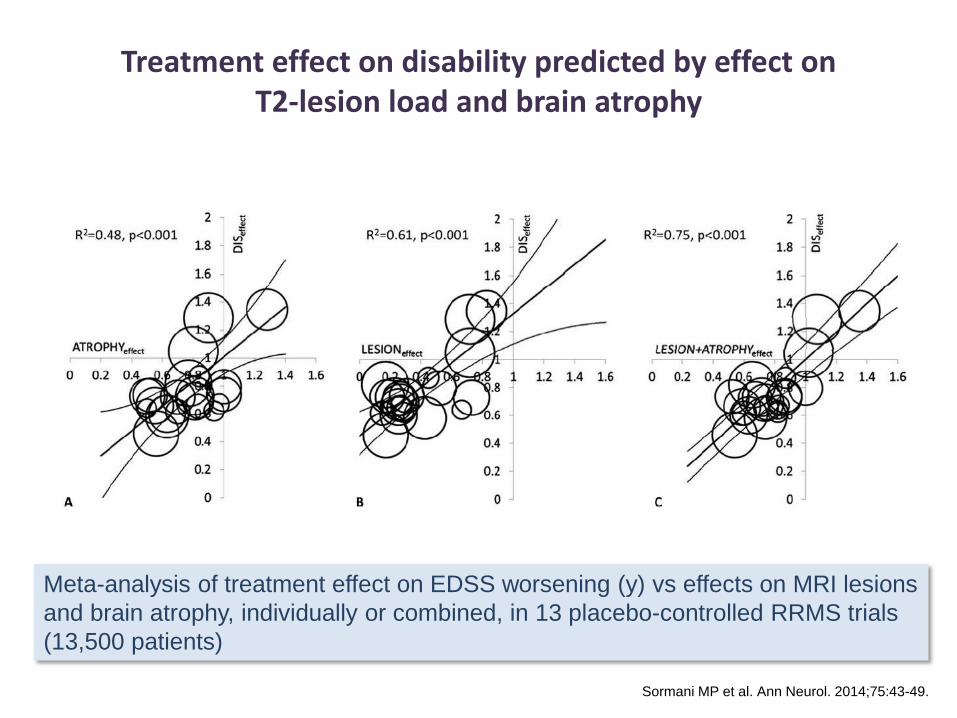
Treatment effect on disability predicted by effect on T2-lesion load and brain atrophy
Meta-analysis of treatment effect on EDSS worsening (y) vs effects on MRI lesions
and brain atrophy, individually or combined, in 13 placebo-controlled RRMS trials
(13,500 patients)
Sormani MP et al. Ann Neurol. 2014;75:43-49.

-1.0%
-0.8%
-0.6%
-0.4%
-0.2%
0.0% Years 0-2
-0.82%
-0.80%
P=0.822†
Placebo (N=315) Natalizumab (N=627)
Year 0-1* Year 1-2
-0.40%
-0.56%
-0.43%
-0.24%
P=0.004†
P=0.002†
†Difference between treatments; ‡Change from baseline; Miller DH et al. Neurology 2007;68:1390-1401.
AFFIRM Study: natalizumab and brain atrophy
Mean
(S
E)
perc
en
tag
e c
han
ge i
n B
PF

Fingolimod has an early and sustained effect on the rate of brain atrophy compared with placebo and IFNb-1a IM
FREEDOMS, 2 years
Fingolimod 0.5 mg (n = 356)
Placebo (n = 329)
***
*
**
6 0 12 24
Time (months)
0
-0.4
-0.8
-1.2
-1.6
-2.0
−38%
vs placebo p<0.001
Ch
ange
in m
ean
BV
fro
m
bas
elin
e (%
)
TRANSFORMS, 1 year
0 12
Time (months)
0.0
-0.4
-0.6
-1.0
IFNb-1a IM (n = 359)
Fingolimod 0.5 mg (n = 368)
−40%
vs IFNb-1a IM p<0.001
*** -0.2
-0.8
Ch
ange
in m
ean
BV
fro
m
bas
elin
e (%
)
ITT population with evaluable MRI images. Note: n numbers for FREEDOMS data reflect the number of patients with available data at 24 months. *p<0.05; **p<0.01; ***p<0.001 vs comparator; p-values are for comparisons over Months 0-6, Months 0-12, Months 0-24 BV, brain volume; ITT, intent-to-treat. Gilenya™ Prescribing Information 19 April 2012. Reproduced with permission. Kappos L et al. N Engl J Med 2010; 362: 387-401, and Cohen JA et al. N Engl J Med 2010; 362: 402-415. Copyright © 2011 Massachusetts Medical Society. All rights reserved

Reduction in brain atrophy on alemtuzumab

Case studies

38-year-old teacher with relapsing–remitting MS under the care of a hospital in central London Glatiramer acetate treatment for 3 years (good adherence and tolerance) Relapse with a mild left sensory loss Referred to me for a second opinion Switched to interferon β (intramuscular interferon β-1a; www.msdecisions.org.uk) Mild persistent flu-like side effects and lymphopenia 12/12’s neutralizing antibodies screen negative Volunteers for new research programme, which included a gadolinium-enhanced MRI protocol
Teacher

38-year-old teacher with relapsing–remitting MS As a result of fatigue and cognitive problems she is forced to take
early retirement Although fully functional she develops depression and anxiety In her spare time she spends a lot of time on the web and becomes
an expert patient Widely read
Net savvy; regular follower of www.ms-res.org
Teacher X


Teacher X

Rheumatoid arthritis End-stage joint disease

Conclusions
MS is a bad disease – Mortality, disability, unemployment, divorce, suicide
cognitive impairment, etc.
Era of individualised profiling – Prognosis, risk, treatment and monitoring
New treatment paradigm – Therapeutic ladder
– Maintenance vs. induction therapy
– Improved risk mitigation tools
– New treatment paradigm of treat-2-target of NEDA or no evidence of disease activity
– Future target to prevent organ damage

















