55
Unit 10: Treating the Dually Unit 10: Treating the Dually Infected Patient Infected Patient Botswana National Tuberculosis Programme Manual Training for Medical Officers
| Date post: | 15-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | alemu-chemeda |
| View: | 48 times |
| Download: | 2 times |
Unit 10: Treating the Dually Unit 10: Treating the Dually Infected PatientInfected Patient
Botswana National Tuberculosis Programme Manual Training for Medical Officers
Slide 10-2Unit 10: Treating the Dually Infected Patient
ObjectivesObjectives
At the end of this unit, participants will be able to:• Explain the relationship between TB and HIV • Describe the effects of immune suppression on TB
progression• Describe the ways in which TB and HIV care can be
integrated• Identify and address challenges to integrating TB
and HIV care• Describe the additional treatments for all TB/HIV
patients• Manage ART in a patient on TB therapy
Slide 10-3Unit 10: Treating the Dually Infected Patient
• HIV/AIDS is the #1 infectious killer in the world—TB is #2
• Many people have both infections
• Botswana TB/HIV co-infection rate is 84%*
HIVHIV
TBTB
HIV & TBHIV & TB
*Source: BNTP, 2007. Source: WHO, 2006.
A Deadly Infectious DiseaseA Deadly Infectious Disease
Slide 10-4Unit 10: Treating the Dually Infected Patient
The TB/HIV Relationship (1) The TB/HIV Relationship (1)
• TB increases HIV progression• Dually infected and untreated persons often
have very high HIV viral loads• Immunosuppression progresses more quickly,
and survival may be shorter despite successful treatment of TB
• Persons who were co-infected have a shorter survival period than persons with HIV who never had TB disease
Slide 10-5Unit 10: Treating the Dually Infected Patient
The TB/HIV Relationship (2)The TB/HIV Relationship (2)
• Screen all HIV-infected patients for TB
• Conduct a complete history as well as a physical examination
• Screen all patients for TB who present in other situations where there is a high burden of HIV, such as medical wards, VCT centres and PMTCT facilities
Slide 10-6Unit 10: Treating the Dually Infected Patient
Immune Suppression Immune Suppression and TB Progressionand TB Progression• HIV-positive person is more likely to progress to TB
disease following infection• HIV-positive person has a greater risk of reactivation• HIV-positive person has a high risk of relapse or
reinfection after treatment• HIV-positive person has a 10% annual risk of
developing active TB (versus 10% lifetime risk among HIV negative individuals)
Source: WHO, 2004
Slide 10-7Unit 10: Treating the Dually Infected Patient
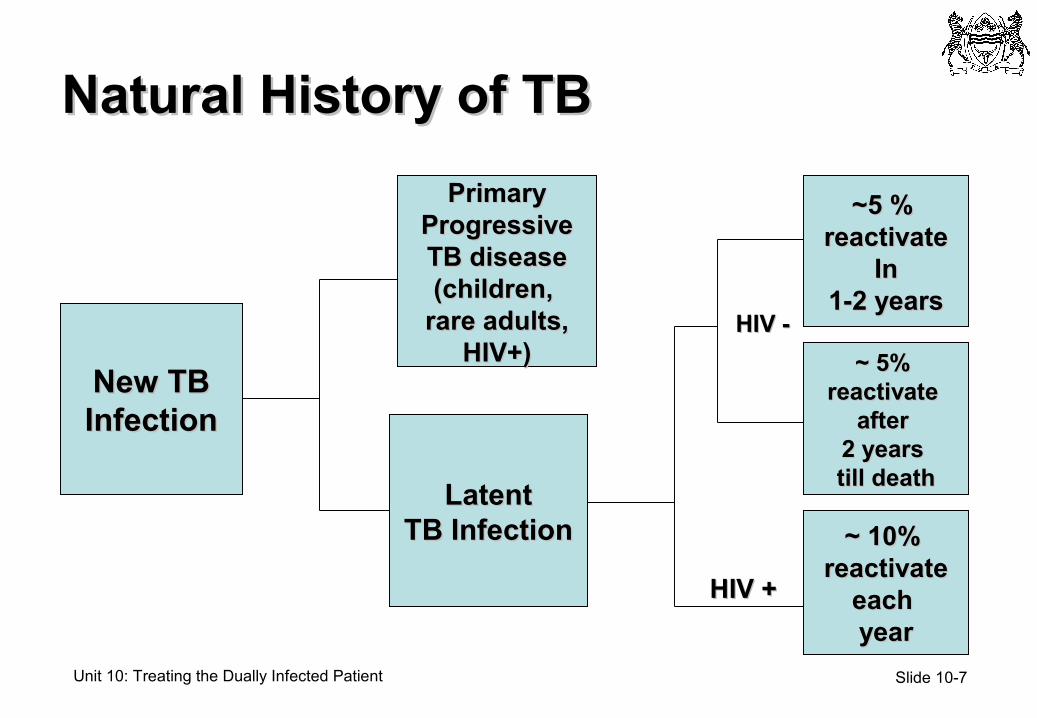
Natural History of TBNatural History of TB
New TBNew TBInfectionInfection
LatentLatentTB InfectionTB Infection
PrimaryPrimaryProgressiveProgressiveTB diseaseTB disease(children, (children,
rare adults,rare adults,HIV+)HIV+)
~~ 10% 10% reactivatereactivate
each each yearyear
~~ 5% 5% reactivate reactivate
after after 2 years 2 years till deathtill death
~~5 % 5 % reactivatereactivate
InIn1-2 years1-2 years
HIV +HIV +
HIV -HIV -
Slide 10-8Unit 10: Treating the Dually Infected Patient
0
2
4
6
8
10
12
14
16
HIV-positive HIV negative
Death
within
6 m
onth
s o
f T
B d
iagnosis
(%
)
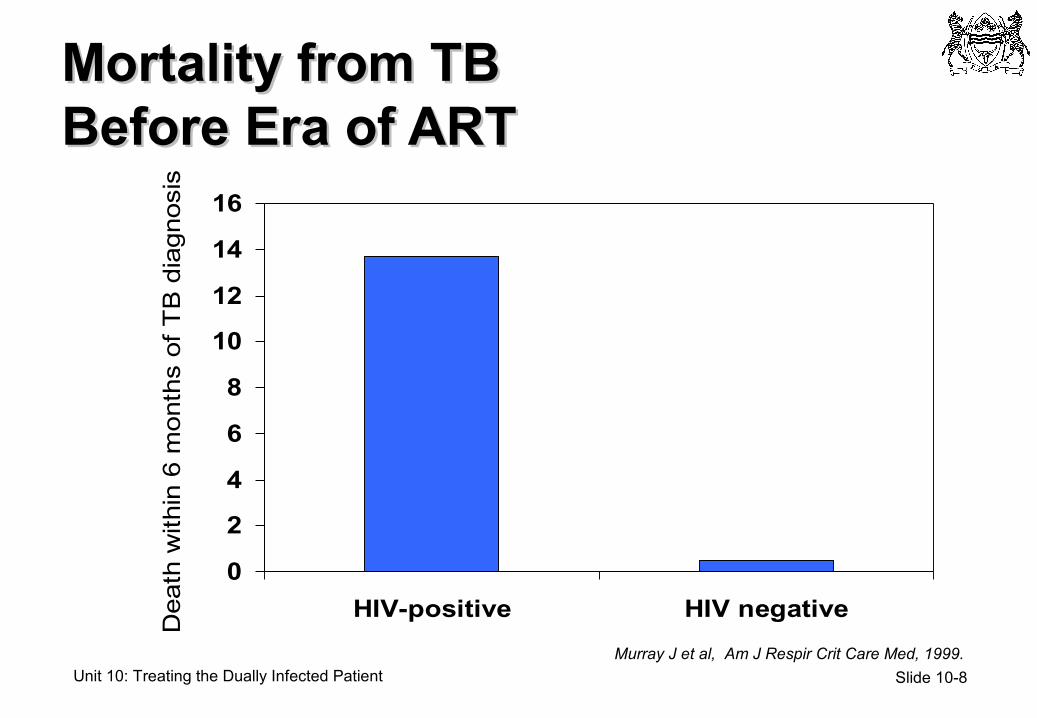
Mortality from TB Mortality from TB Before Era of ARTBefore Era of ART
Murray J et al, Am J Respir Crit Care Med, 1999.
Slide 10-9Unit 10: Treating the Dually Infected Patient
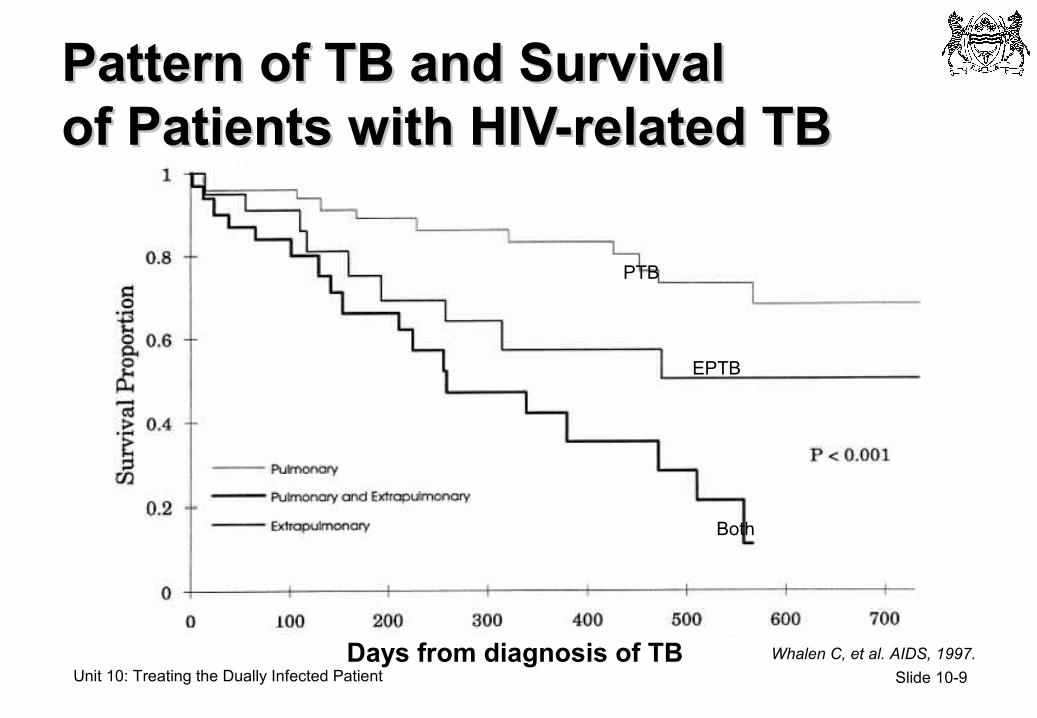
Pattern of TB and Survival Pattern of TB and Survival of Patients with HIV-related TBof Patients with HIV-related TB
Whalen C, et al. AIDS, 1997.
PTB
EPTB
Both
Days from diagnosis of TB
Slide 10-10Unit 10: Treating the Dually Infected Patient
Screening for HIV in TB PatientsScreening for HIV in TB Patients
• Purpose• Identify TB suspects and patients who are also HIV
positive
• All TB patients with HIV are eligible for ART, it’s just a matter of timing of ART initiation
• Method• At every health care encounter with TB patient:
• Counsel on HIV prevention strategies
• Offer Routine HIV testing if testing not previously done
• CD4 count should be obtained on any HIV positive individual
Slide 10-11Unit 10: Treating the Dually Infected Patient
Screening for TB at HIV ClinicsScreening for TB at HIV Clinics
• Purpose• Identify HIV-positive persons eligible for IPT• Identify HIV-positive persons who may have active
TB
• Method• At each health care encounter, ask about:
• History of TB and prior treatment for TB• Current IPT or history of IPT• TB signs and symptoms
Slide 10-12Unit 10: Treating the Dually Infected Patient
Early Diagnosis: Better OutcomesEarly Diagnosis: Better Outcomes
• Decrease in mortality for treated patients• Decrease in period of transmission to others
especially family members who may be HIV infected
• Decrease in transmission in the community• Identification of at-risk contacts in a timely
manner
Slide 10-13Unit 10: Treating the Dually Infected Patient
TB and HIV Care StrategiesTB and HIV Care Strategies
Persons with TB• Rapid diagnosis and
initiation of TB treatment• Test all TB patients for HIV• Maximise treatment
completion rates• Offer cotrimoxazole
preventive therapy to HIV+ in TB system
• Assess HIV+ for ART eligibility and refer
HIV-positive Persons• Screen for active TB at
every health system encounter
• Rapid TB diagnosis and initiation of TB treatment
• Reduce TB incidence with IPT
• Reduce TB incidence with effective ART
• Minimise exposures to active TB cases
Slide 10-14Unit 10: Treating the Dually Infected Patient
TB and HIV Treatment StrategiesTB and HIV Treatment Strategies
TB Care and Treatment• Individual
• Control their disease• Restore health and ADL*• Preserve their position in
family and community
• Community• Decrease the spread of TB
infection • Mitigate against TB stigma
from society• Enforce prevention
HIV Care and Treatment• Individual
• Control their disease• Restore health and ADL*• Preserve their position in
family and community
• Community• Decrease the spread of HIV
infection • Mitigate against HIV stigma
from society• Enforce prevention
Slide 10-15Unit 10: Treating the Dually Infected Patient
Challenges to Integration Challenges to Integration
What do you think are the challenges to
integrating the two services?
What strategies can you suggest to address these
potential challenges?
Slide 10-16Unit 10: Treating the Dually Infected Patient
Treating a Person with HIV and TBTreating a Person with HIV and TB
• Common scenario in Botswana
• TB case definitions are the same regardless of HIV status
• TB treatment is the priority
• Clinician should decide the optimal timing for initiation of ART during TB treatment guided by National policy
Slide 10-17Unit 10: Treating the Dually Infected Patient
When to Start ART When to Start ART During TB TherapyDuring TB Therapy• All HIV-infected TB patients qualify for ART
• CD4<100 should start ART within one to two weeks after start of ATT
• CD4 100 – 200 should start ART within two to four weeks after start of ATT
• CD4s>200 may defer ART until end of ATT
• HIV-infected patients already on ART who develop TB should begin anti-TB meds immediately
• Management of TB patients on ART is complex and patient care needs to be coordinated with IDCC
Slide 10-18Unit 10: Treating the Dually Infected Patient
ART in the Botswana ART in the Botswana National ProgrammeNational Programme
Special Order:
ABC (Abacavir), TDF (Tenofovir)
NRTIs NNRTIs PIs
AZT (Zidovudine) 3TC (Lamivudine)d4T (Stavudine)ddI (Didanosine)
(AZT+3TC) (Combivir)
EFV (Efavirenz)NVP (Nevirapine)
LPV/r (Kaletra or Alluvia)RTV (Ritonavir)SQV (Saquinavir)

Slide 10-19Unit 10: Treating the Dually Infected Patient
TB Disease Progression TB Disease Progression with HIV Co-infection with HIV Co-infection
Source: de Jong BC et al, Annu Rev Med, 2004.
• TB progresses more rapidly with HIV co-infection• Up to 10% of co-infected individuals develop active
tuberculosis each year• 10%–20% lifetime risk among those without HIV infection
• ART alone can reduce the risk of progression to active tuberculosis in latently infected individuals by as much as 80%–92%
• Patients on or about to start ART should still be offered IPT if they meet the criteria
Slide 10-20Unit 10: Treating the Dually Infected Patient
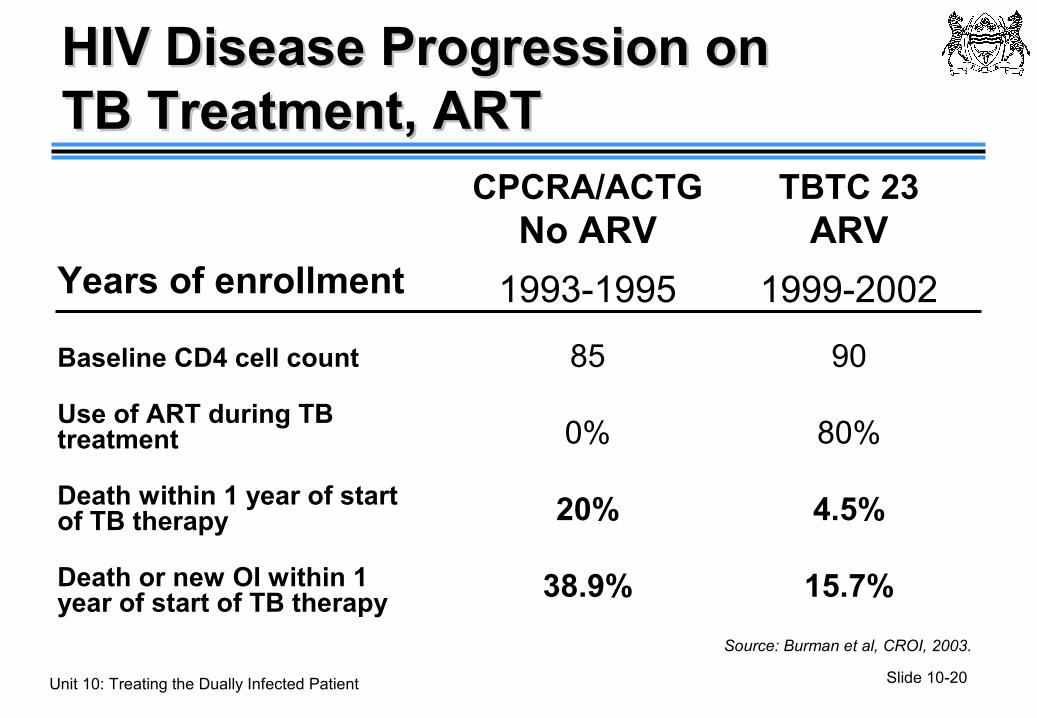
Years of enrollment
Baseline CD4 cell count
Use of ART during TB treatment
Death within 1 year of start of TB therapy
Death or new OI within 1 year of start of TB therapy
TBTC 23ARV
1999-2002
90
80%
4.5%
15.7%
CPCRA/ACTGNo ARV
1993-1995
85
0%
20%
38.9%
HIV Disease Progression on HIV Disease Progression on TB Treatment, ARTTB Treatment, ART
Source: Burman et al, CROI, 2003.
Slide 10-21Unit 10: Treating the Dually Infected Patient
• Appropriate treatment of TB• TB treatment regimens are the same for HIV-
infected patients as for non-infected patients
• Assure adherence with TB treatment (use of directly observed therapy, DOT)
• Cotrimoxazole prophylaxis
• ART
How To Improve How To Improve Outcomes of HIV-Related TB?Outcomes of HIV-Related TB?
Slide 10-22Unit 10: Treating the Dually Infected Patient
TB Treatment and TB Treatment and Outcome of HIV-Related TBOutcome of HIV-Related TB• Poor adherence to TB treatment is associated with
the following adverse outcomes• Treatment failure: patient suffers morbidity or mortality of
TB• Increased risk of TB drug resistance or MDR complicating
future treatment of the patient• Continued transmission of TB and development of new
cases of active TB• Possible transmission of drug resistant or MDR TB
• DOT can lead to improved outcomes by supporting better adherence practices
Slide 10-23Unit 10: Treating the Dually Infected Patient
Cotrimoxazole Preventative Cotrimoxazole Preventative Therapy (CPT) (1)Therapy (CPT) (1)• Reduces the risk of
• Pneumocystis jiroveci pneumonia (PCP)• Toxoplasmosis• Bacterial infections
• Reduces deaths and hospitalisations
• Also effective against:• Pneumococcus, salmonella, nocardia and malaria
Slide 10-24Unit 10: Treating the Dually Infected Patient
CPT (2)CPT (2)
• All HIV-positive TB patients should receive CPT regardless of the CD4 count for, at least, the duration of anti-TB treatment
• Extend CPT beyond the end of anti-TB treatment if the CD4 cell count is less than 200 cells/mm3
Source: WHO, 2006
Slide 10-25Unit 10: Treating the Dually Infected Patient
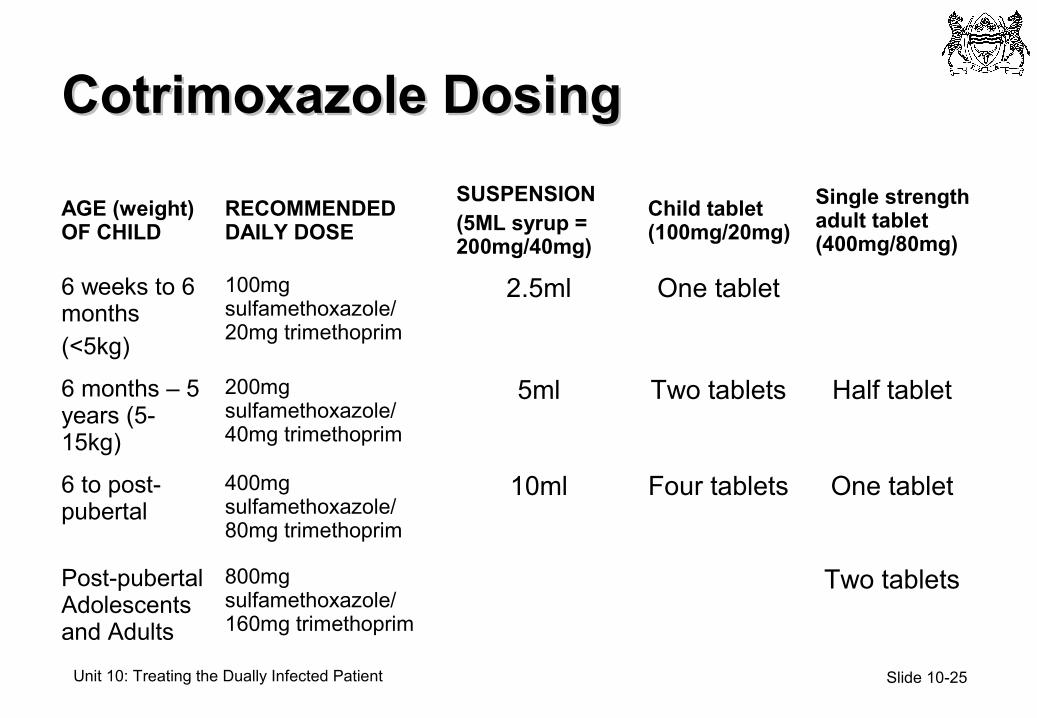
Cotrimoxazole DosingCotrimoxazole Dosing
AGE (weight) OF CHILD
RECOMMENDED DAILY DOSE
SUSPENSION(5ML syrup = 200mg/40mg)
Child tablet (100mg/20mg)
Single strength adult tablet (400mg/80mg)
6 weeks to 6 months(<5kg)
100mg sulfamethoxazole/ 20mg trimethoprim
2.5ml One tablet
6 months – 5 years (5-15kg)
200mg sulfamethoxazole/ 40mg trimethoprim
5ml Two tablets Half tablet
6 to post-pubertal
400mg sulfamethoxazole/ 80mg trimethoprim
10ml Four tablets One tablet
Post-pubertal Adolescents and Adults
800mg sulfamethoxazole/ 160mg trimethoprim
Two tablets
Slide 10-26Unit 10: Treating the Dually Infected Patient
• Identification of patients who will benefit from antiretroviral therapy
• Drug-drug interactions• Immune reconstitution events• Overlapping ARV and TB medicine side effect • Adherence with multi-drug therapy for two infections• Coordinating care between TB and HIV care
providers
Issues in Using Issues in Using ART During TB TherapyART During TB Therapy
Slide 10-27Unit 10: Treating the Dually Infected Patient
Immune Function and Immune Function and Survival During TB TreatmentSurvival During TB Treatment
Source: Mansouthi W et al., J Acquir Immune Defic Syndr, 2006.
• Survival during TB treatment is associated with level of immune function
• ART can substantially reduce mortality among HIV/TB co-infected patients
• Initiation of ART within six months of TB diagnosis can improve survival
Slide 10-28Unit 10: Treating the Dually Infected Patient
Who Would Benefit from ARVsWho Would Benefit from ARVsDuring TB Therapy?During TB Therapy?• HIV is associated with markedly increased
mortality during TB treatment
• Early deaths (< 30 days after TB diagnosis) often due to TB; later deaths - other complications of HIV
• All HIV+ patients with TB are stage 3 (pulmonary) or 4 (extra-pulmonary) and are eligible for ART
Slide 10-29Unit 10: Treating the Dually Infected Patient
Benefits and RisksBenefits and Risks
• Benefits:• Strengthen immune system for fighting TB and other
infections
• Avoid deaths due to OIs and AIDS during TB therapy
• Risks• Drug interactions limit ART regimens
• Immune reconstitution inflammatory syndrome
• Drug toxicity
Slide 10-30Unit 10: Treating the Dually Infected Patient
Treatment of TB for HIV-Positive Treatment of TB for HIV-Positive PersonsPersons
Initial treatment phase should consist of
• Isoniazid (H)
• Rifampicin (R)
• Pyrazinzamide (Z)
• Ethambutol (E)
Slide 10-31Unit 10: Treating the Dually Infected Patient
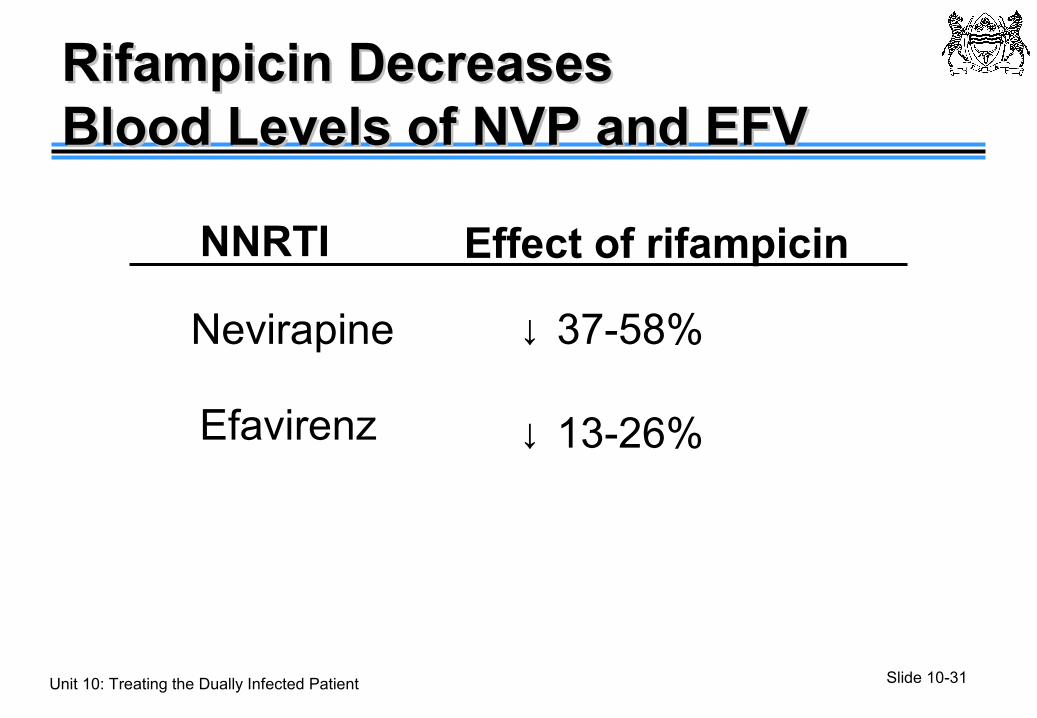
Rifampicin Decreases Rifampicin Decreases Blood Levels of NVP and EFVBlood Levels of NVP and EFV
NNRTI Effect of rifampicin
Nevirapine ↓ 37-58%
Efavirenz ↓ 13-26%
Slide 10-32Unit 10: Treating the Dually Infected Patient
ART and Rifampicin-BasedART and Rifampicin-BasedTB TherapyTB Therapy
• AZT/3TC/EFV* • Men• Women outside of child bearing years • Children >3 years old
• AZT/3TC/NVP*• Women of child bearing age• Children < 3 years old
*Note: if Hb < 7.5, substitute AZT with d4T
Slide 10-33Unit 10: Treating the Dually Infected Patient
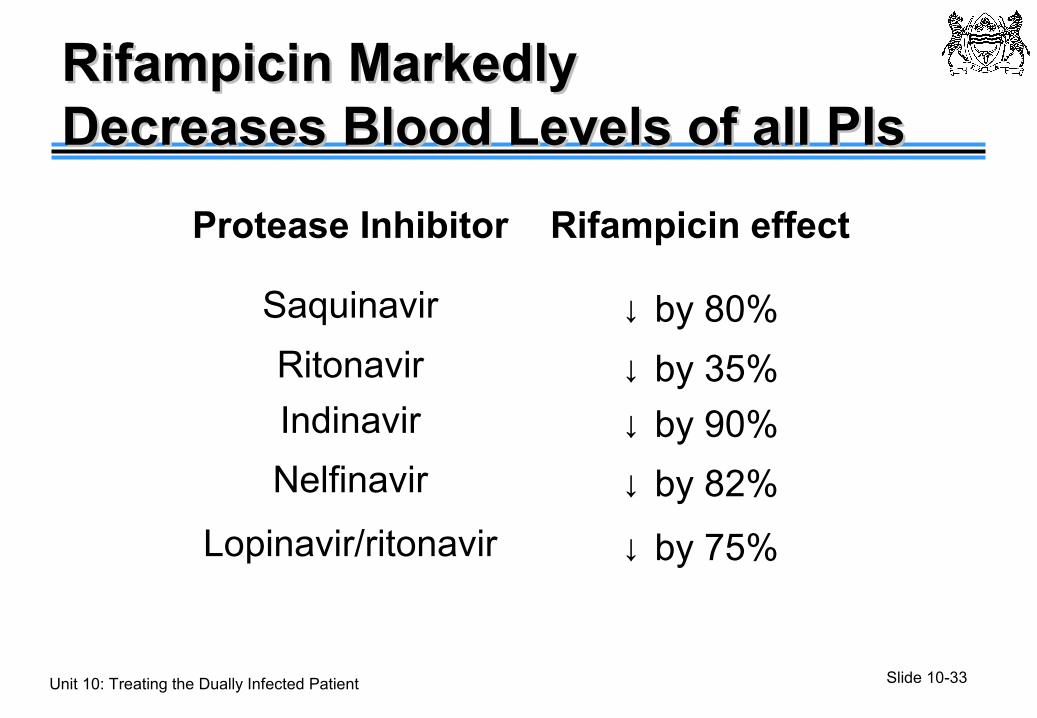
Rifampicin Markedly Rifampicin Markedly Decreases Blood Levels of all PIsDecreases Blood Levels of all PIs
Protease Inhibitor Rifampicin effect
Saquinavir ↓ by 80%
Ritonavir ↓ by 35%Indinavir ↓ by 90%
Nelfinavir ↓ by 82%
Lopinavir/ritonavir ↓ by 75%
Slide 10-34Unit 10: Treating the Dually Infected Patient
Treatment Options: ART During Treatment Options: ART During Rifampicin-Based TB TherapyRifampicin-Based TB Therapy
Ritonavir boosting of other PIs can achieve adequate blood levels: • Lopinavir/ritonavir, 400mg/400mg BD
• = 3 capsules Kaletra + 3 capsules ritonavir BD• =2 tablets Alluvia* + 3 capsules ritonavir BD
• Lopinavir/ritonavir, 800mg/200mg BD• =6 capsules Kaletra BD• =4 tablets Alluvia* BD
Slide 10-35Unit 10: Treating the Dually Infected Patient
Case Study: M.L. (1)Case Study: M.L. (1)
• 31 year old female with HIV infection diagnosed 5 years ago
• She has been non-adherent to ART• She presented with fever and cough of 2-3
weeks duration• Exam: a small (1 cm) submandibular lymph
node was found on the right side• Lab: CD4 count 26, Sputum smears x 2
positive for AFB
Slide 10-36Unit 10: Treating the Dually Infected Patient
Case Study: M.L. (2)Case Study: M.L. (2)
• M.L. was started on TB medications (EHRZ) plus ART as inpatient
• 2 wks after starting medications, she developed increased cervical lymphadenopathy with worsening respiratory symptoms
• Repeat CD4 count was 120 • A CXR was done
Slide 10-37Unit 10: Treating the Dually Infected Patient
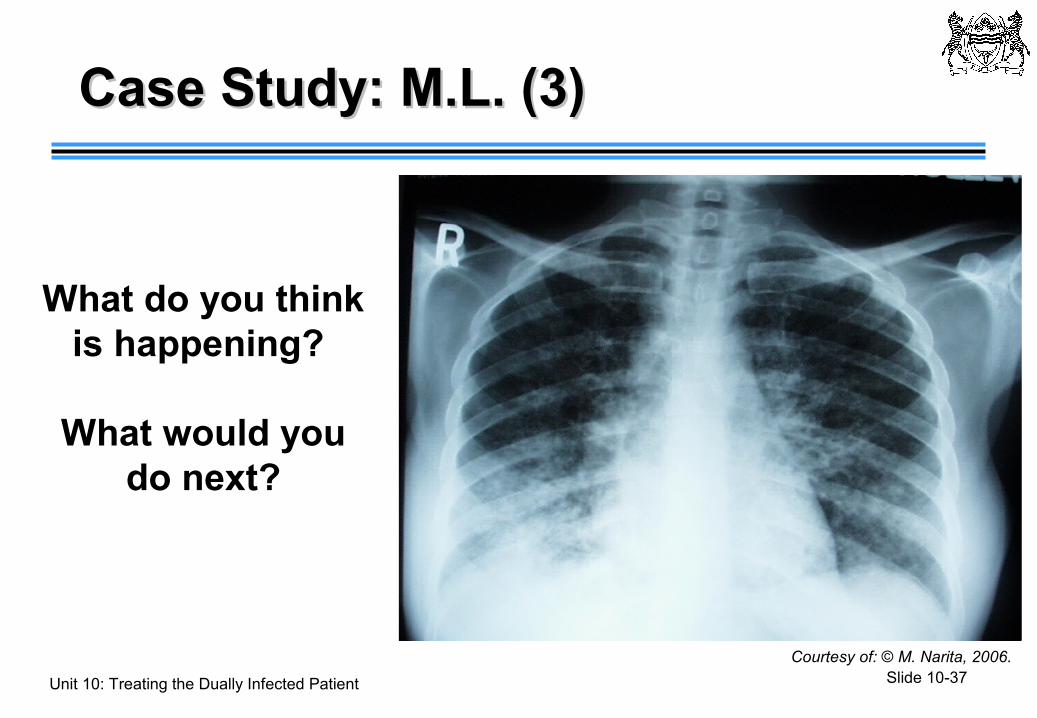
Courtesy of: © M. Narita, 2006.
What do you think is happening?
What would you do next?
Case Study: M.L. (3)Case Study: M.L. (3)
Slide 10-38Unit 10: Treating the Dually Infected Patient
• HIV medications were discontinued
• TB medications were continued
• Repeat CXR was done• M.L.’s CD4 decreased
to 34
Case Study: M.L. (4)Case Study: M.L. (4)
Courtesy of: © M. Narita, 2006.
Slide 10-39Unit 10: Treating the Dually Infected Patient
Case Study: M.L. (5)Case Study: M.L. (5)
• ART resumed 3 months into TB treatment
• TB was cured
• At the end of TB treatment her CD4 was 342
Slide 10-40Unit 10: Treating the Dually Infected Patient
• Improved immune response against MTB leads to new or worsening signs or symptoms despite effective TB treatment
• Closely associated with starting ARV (days to weeks), but rarely associated with starting TB therapy
• Natural history• Duration - days to months• Waxing and waning is common
Immune Reconstitution Immune Reconstitution Inflammatory Syndrome (IRIS)Inflammatory Syndrome (IRIS)
Slide 10-41Unit 10: Treating the Dually Infected Patient
• Fever• New or worsening lymphadenitis - peripheral or
central nodes• New or worsening pulmonary infiltrates, including
respiratory failure• New or worsening pleuritis, pericarditis, or ascites• Intracranial tuberculomas, worsening meningitis• Disseminated skin lesions• Epididymitis, hepatosplenomegaly, soft tissue
abscesses
IRIS Among Patients with HIV/TBIRIS Among Patients with HIV/TB
Slide 10-42Unit 10: Treating the Dually Infected Patient
• Shorter time from the initiation of TB therapy to the initiation of antiretroviral therapy (e.g., within six weeks)
• Low initial CD4 count or high viral load at ART initiation• CD4 count rises rapidly on ART
• Good immunological and virological response during ART
• Extrapulmonary or disseminated diseaseSource: Colebunders R, et al., Int J Tuberc Lung Dis, 2006.
Risk Factors for IRISRisk Factors for IRIS
Slide 10-43Unit 10: Treating the Dually Infected Patient
Managing IRIS Managing IRIS
• Inform patients about the possibility of an event after starting ART– may feel like the “TB is coming back”
• Evaluate for possible TB treatment failure • Drug resistance, non-adherence, malabsorption
• Assess for other HIV-related complications, e.g., another opportunistic infection
• Management of symptoms, e.g., use non-steroidal anti inflammatory drugs
• For severe symptoms may need to use steroids (prednisolone), 1 mg/kg or even stop ART temporarily
Slide 10-44Unit 10: Treating the Dually Infected Patient
Case Study: MikaCase Study: Mika
• A 40 year-old male from Gaborone presents with fever for 4 weeks, cough with bloody sputum, sweats and weight loss of 7kg
• Chest X-ray shows right lobe infiltrate• Sputum AFB x 1 results “scanty” • His HIV test is positive and CD4 is180
cell/cu mm
Slide 10-45Unit 10: Treating the Dually Infected Patient
Case Study: Case Study: Mika at 2 months ATTMika at 2 months ATT
• Mika returns after two months
• His fevers, cough, and night sweats have stopped and he has gained 5kg
• His TB regimen is changed to the continuous phase (R/H)
• He is started on ART
X-ray shows improvement
Source: I-TECH, Tanzania
Slide 10-46Unit 10: Treating the Dually Infected Patient
Case study: Mika at 4 Months ATTCase study: Mika at 4 Months ATT
• Mika comes back for his 2nd ART monitoring visit
• He reports fever, cough and night sweats have returned
• He has taken his ARTs as prescribed but thinks they are making him more sick and would like to stop them
Slide 10-47Unit 10: Treating the Dually Infected Patient
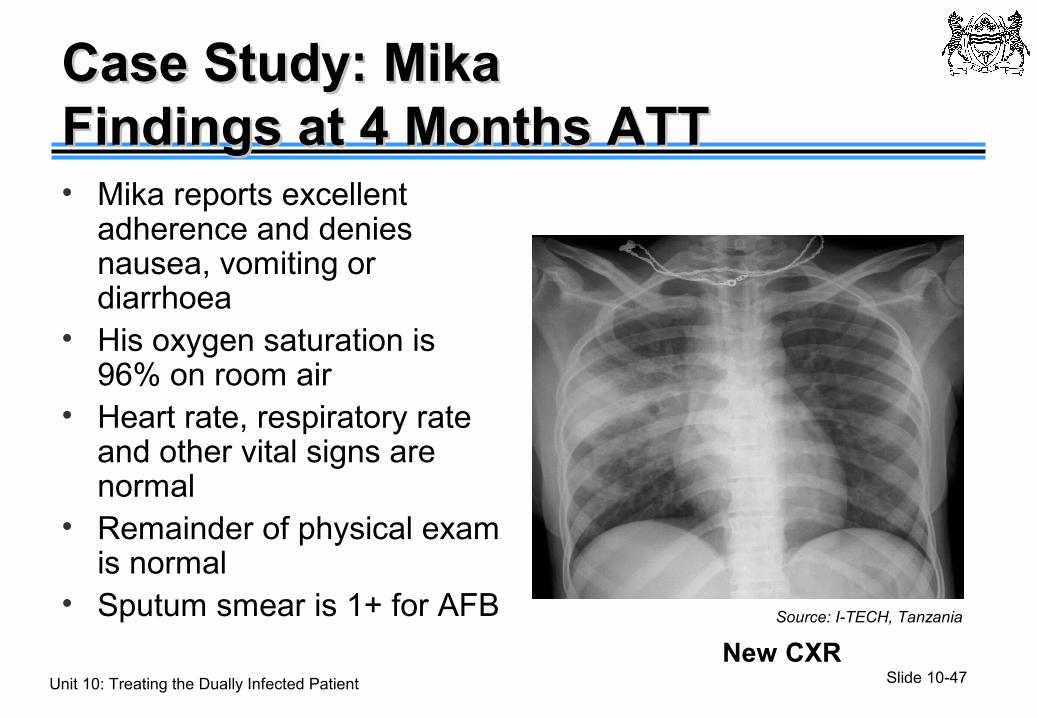
Case Study: MikaCase Study: MikaFindings at 4 Months ATTFindings at 4 Months ATT• Mika reports excellent
adherence and denies nausea, vomiting or diarrhoea
• His oxygen saturation is 96% on room air
• Heart rate, respiratory rate and other vital signs are normal
• Remainder of physical exam is normal
• Sputum smear is 1+ for AFB
New CXR
Source: I-TECH, Tanzania
Slide 10-48Unit 10: Treating the Dually Infected Patient
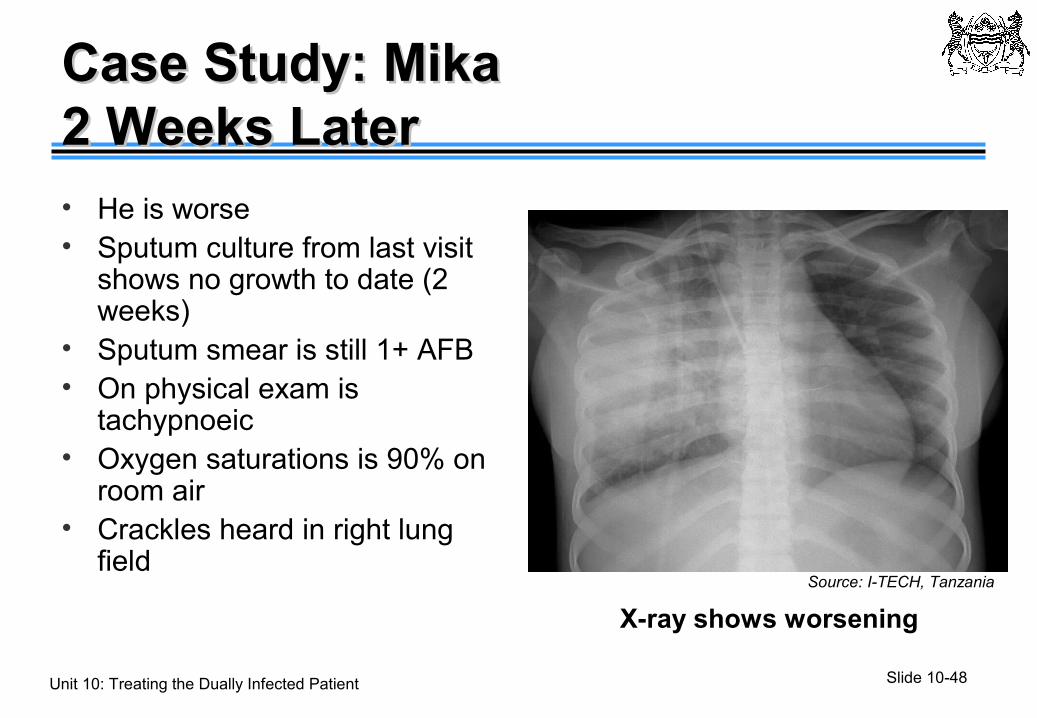
Case Study: Mika Case Study: Mika 2 Weeks Later2 Weeks Later• He is worse• Sputum culture from last visit
shows no growth to date (2 weeks)
• Sputum smear is still 1+ AFB• On physical exam is
tachypnoeic• Oxygen saturations is 90% on
room air• Crackles heard in right lung
field
X-ray shows worsening
Source: I-TECH, Tanzania
Slide 10-49Unit 10: Treating the Dually Infected Patient
Adverse Events During Adverse Events During Combined TB+HIV Treatment (1)Combined TB+HIV Treatment (1)
Common adverse events include:• Peripheral neuropathy - more common with
use of ddI & d4T• Skin rash
• TB drugs• Cotrimoxazole• Nevirapine • Other drugs
• Hepatitis, due to TB drugs or unknown causesSource: Dean GL, et.al., AIDS, 2002.
Slide 10-50Unit 10: Treating the Dually Infected Patient
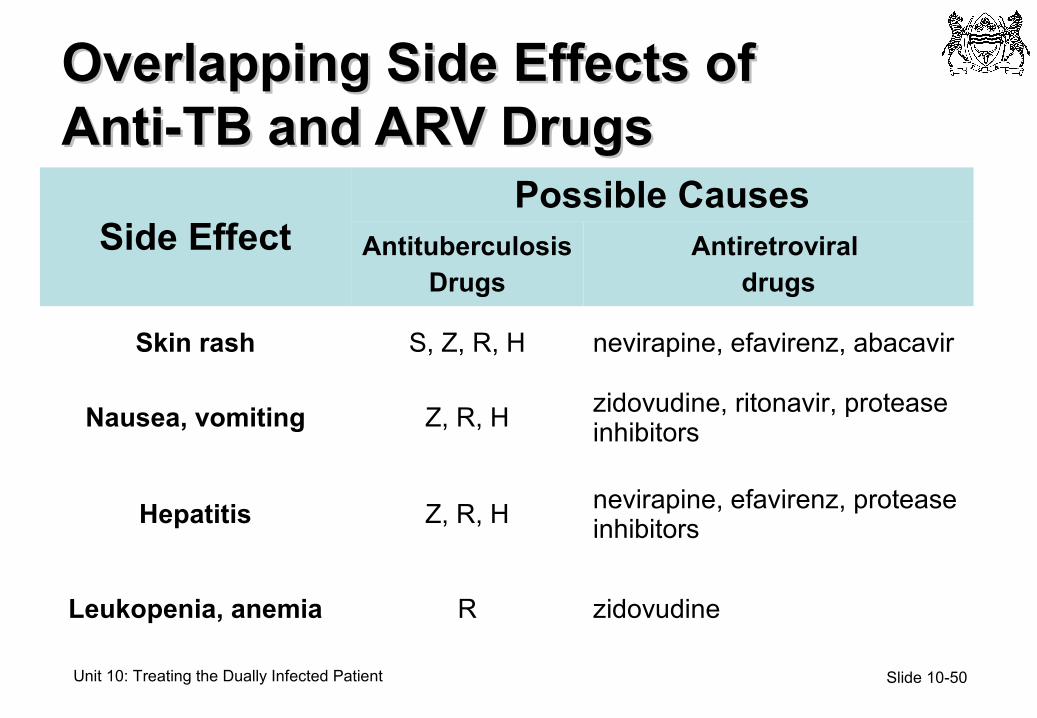
Overlapping Side Effects ofOverlapping Side Effects ofAnti-TB and ARV DrugsAnti-TB and ARV Drugs
Side EffectPossible Causes
Antituberculosis Drugs
Antiretroviral drugs
Skin rash S, Z, R, H nevirapine, efavirenz, abacavir
Nausea, vomiting Z, R, H zidovudine, ritonavir, protease inhibitors
Hepatitis Z, R, H nevirapine, efavirenz, protease inhibitors
Leukopenia, anemia R zidovudine
Slide 10-51Unit 10: Treating the Dually Infected Patient
Adverse Events During Adverse Events During Combined TB+HIV Treatment (2)Combined TB+HIV Treatment (2)
• Some adverse events related to advanced AIDS, some to other infections or malignancies, and some to their treatment
• Few events result in permanent discontinuation of first-line TB drugs, even though therapy may have been temporarily discontinued
Do not give up on the first-line TB drugs unless it is clear that one of them is causing a
severe side effect!Source: Dean GL, et.al., AIDS, 2002.
Slide 10-52Unit 10: Treating the Dually Infected Patient
Managing Adverse EventsManaging Adverse Events
• Do one thing at a time-- makes it easier to decide the cause of an event
• Stop medications for severe adverse events• Use sequential re-challenge to decide the cause of
an event• Don’t switch from the first-line TB drugs (especially
INH and RIF) without evidence of an association with a significant side effect
• Remember IRIS as a possible cause of adverse events during treatment
Slide 10-53Unit 10: Treating the Dually Infected Patient
Increasing TB/HIV Increasing TB/HIV Treatment Adherence Treatment Adherence • TB treatment uses directly observed therapy
(DOT)-- use DOT visits for TB treatment to enhance adherence to antiretroviral therapy
• Try to coordinate medication pickups where possible
Slide 10-54Unit 10: Treating the Dually Infected Patient
Preventing Active TB Preventing Active TB Among HIV-Infected PersonsAmong HIV-Infected PersonsFour strategies:
1. INH Preventive Treatment2. Antiretroviral Therapy3. Infection Control
• HIV+ Health Care Workers should avoid TB exposure (medical and TB wards)
1. TB case finding• Early case-detection and effective TB therapy
(effective DOTS program)
Slide 10-55Unit 10: Treating the Dually Infected Patient
Key PointsKey Points
• Both TB and HIV increase the other’s disease progression
• Early Diagnosis of TB has better outcomes for patients, families and community
• Standard TB treatment correctly implemented cures TB in TB/HIV
• ART for eligible patients greatly improves survival• Different ART regimens are required because of
drug interactions with rifampicin

















