52
TREATING TOBACCO DEPENDENCE IN MENTAL HEALTH SETTINGS PRESENTED BY SARAH WORLEY SYNOPSIS OF MATERIAL FROM RUTGERS CONFERENCE
| Date post: | 21-Jan-2018 |
| Category: |
Documents |
| Upload: | sarah-worley |
| View: | 205 times |
| Download: | 1 times |
TREATING TOBACCO DEPENDENCE IN MENTAL
HEALTH SETTINGSPRESENTED BY SARAH WORLEY
SYNOPSIS OF MATERIAL FROM RUTGERS
CONFERENCE

THE TRUTH
• HTTPS://WWW.THETRUTH.COM/ARTICLES/VIDEOS/CATMAGEDDON
• HTTPS://WWW.THETRUTH.COM/ARTICLES/VIDEOS/FINISHIT

REASONS TO TREAT TOBACCO USE
•Tobacco use kills half of our patients
•Tobacco use limits full recovery
•Tobacco use disorder is in the DSM
•Tobacco use has a negative impact on
treatment

WHY TREAT TOBACCO
DEPENDENCE IN MENTAL HEALTH
SETTINGS
• 51 million smokers in the US today
• At least 1/3 have a mental illness
• 3/4 of smokers have a past or present problem with mental illness or addiction
• Smoking is the #1 cause of death in people with mental illness or addiction

50% of deaths in schizophrenia, depression, and bipolar disorder are
attributed to tobacco• People with SMI die, on average, 25 years earlier than the general
population.
• The leading causes of death among those individuals are:
• Heart Disease
• Cancer
• Cerebrovascular
• Chronic Respiratory
• All of these causes are smoking related!
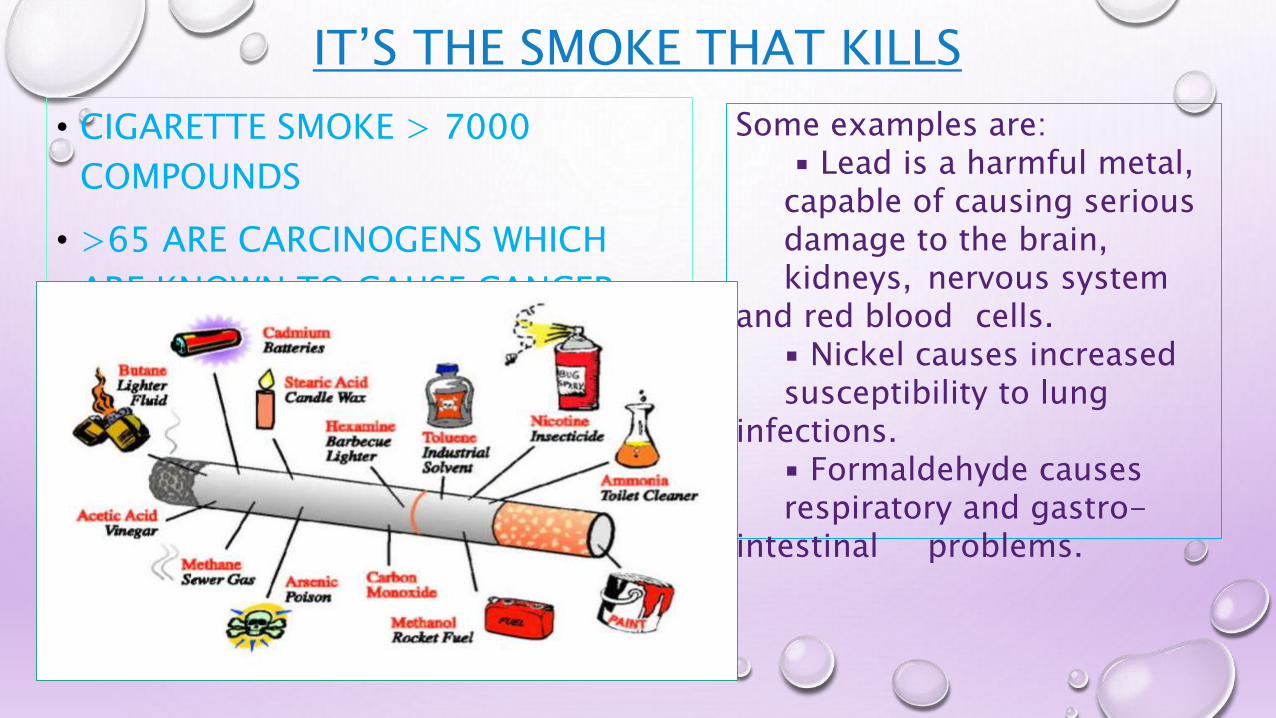
IT’S THE SMOKE THAT KILLS
• CIGARETTE SMOKE > 7000
COMPOUNDS
• >65 ARE CARCINOGENS WHICH
ARE KNOWN TO CAUSE CANCER
Some examples are:▪ Lead is a harmful metal,
capable of causing serious damage to the brain, kidneys, nervous system
and red blood cells.▪ Nickel causes increased susceptibility to lung
infections.▪ Formaldehyde causes respiratory and gastro-
intestinal problems.

ADDITIONAL REASONS TO TREAT TOBACCO DEPENDENCE
• Tobacco use may worsen behavioral health outcomes, while cessation
does not worsen outcomes.
• Daily smoking predicts suicidal thoughts or attempt.
• States with an increase in $1 in state excise tax per pack of cigarettes was associated
with a 12.4% reduction in risk of suicide.
• Smoking keeps consumers from achieving recovery:
• Being Financially Stable
• Getting Jobs
• Securing Housing
• Treating tobacco-dependence is cost-effective and save healthcare
dollars.
ADDITIONAL REASONS TO TREAT TOBACCO DEPENDENCE
• Treating tobacco dependence improves employee productivity and
health.
• Behavioral health practitioners have more time than primary care
providers for psychosocial treatments for tobacco dependence.
• Tobacco use interferes with psychiatric medication.
• Addressing tobacco use fits into the current wellness and recovery
movement.
• Addressing tobacco use during treatment of other substance use
disorders increased the likelihood of long-term abstinence from
alcohol and illicit drugs by 25%.
WHY DO SO MANY CONSUMERS WITH MENTAL ILLNESS SMOKE?
There is no easy answer as to why so many
people living with mental illness smoke.
Smoking is a complex problem made up of
biological, psychological and
social/environmental factors.
BIOLOGICAL FACTORS (PHYSICAL/ BRAIN FUNCTIONS)
• People living with a mental illness may be at
increased risk for physical addiction to smoking.
•Nicotine may help improve mood, or mental
functions like attention, memory or learning, in
some people diagnosed with mental illness.

PSYCHOLOGICAL FACTORS (THINKING/ FEELING)
•People diagnosed with a mental illness may
not feel confident that they can quit.
•People diagnosed with a mental illness may
rely on smoking to help them cope with
stress.

SOCIAL FACTORS (PEOPLE/ PLACES/ THINGS AROUND YOU)
•Smoking is common in and around mental
health hospitals, treatment centers and
group homes.
•People with a mental illness may feel like it
is easier to talk with others and be around
others when they are smoking.

UNDERSTANDING TOBACCO ADDICTION NEUROBIOLOGY
• Addiction is a developmental disease that starts in adolescence
and childhood.
• Possible biological factors include an increased genetic vulnerability, a
greater susceptibility to progressing from tobacco use to dependence,
because of a greater subjective experience of reward or pleasure, or that
tobacco/nicotine helps some of the symptoms related to a behavioral
disorder. Cigarette smoking may be an attempt to self-medicate symptoms
of depression, anxiety, boredom, loneliness, and other feelings common in
this population.
• Tobacco use in adolescents is highly correlated with other substance use
and usually precedes the onset of other substance-abuse and psychiatric
illness. There may be particular risks of progressing from tobacco use to
dependence for a subgroup of adolescents who are especially vulnerable to
mental illness and/or other addictions. Adolescents with multiple life and
UNDERSTANDING TOBACCO ADDICTION NEUROBIOLOGY
• Gateway theory:
• High school seniors using cigarettes < age 13 had 3x risk of
using marijuana.
• Nicotine binds in the cortex, hippocampus, and reward
pathways.
• Dopamine release
• Arousal, enhanced vigilance
• Appetite suppression
• Mood changes
UNDERSTANDING TOBACCO ADDICTION NEUROBIOLOGY
• Schizophrenia and tobacco
• Patients with schizophrenia smoke at nearly three times the rate of the
general population, with most studies finding prevalence rates of about 90%.
Cigarette smoking in schizophrenia may be especially reinforcing, as it may
improve psychiatric symptoms or cognitive functioning or prevent the
worsening of these symptoms during the withdrawal from nicotine.
Schizophrenics are often highly nicotine dependent and are hypothesized to
be efficient and effective smokers. Clinical observation reveals that
schizophrenics smoke nearly continuously during the day, and smoke
cigarette filters and discarded butts, which are highly concentrated with
nicotine. Some of these effects may be related to the use of antipsychotic
medications that block dopamine postsynaptic receptors. Schizophrenics
who smoke have lower rates of neuroleptic- induced Parkinsonism. Ad
libitum smoking in schizophrenics increases after initiation of haloperidol
relative to a baseline rates when free of antipsychotic medications.
Schizophrenics smoke less when treated with clozapine versus conventional
UNDERSTANDING TOBACCO ADDICTION NEUROBIOLOGY
• Depression and tobacco
• Lifetime prevalence of depression is 5–12% in men and 12–20% in women, making it extremely common and projected to cause the second greatest disease burden in the world by the year 2020. Many studies link the effects of smoking to depression and vice versa because it is common for smokers to have symptoms of depression or develop them when they are trying to quit smoking. According to the Epidemiologic Catchment Area (ECA) survey, about 70% of men and 80% of women with a history of major depression have current or past smokers and 25–40% of psychiatric patients seeking smoking cessation treatment have a past history of major depression or minor dysthymic disorder. The presence of depressive symptoms during tobacco abstinence is associated with failed quit attempts, increased probability of returning to smoking and the need for more quit attempts. Women with depression experience greater difficulty in maintaining early abstinence than non-depressed women. Data from family, adoption, and twin studies strongly support a substantial genetic influence on the initiation and maintenance of smoking, and several studies suggest a genetic predisposition to both nicotine dependence and depression. Family studies reveal smoking patterns that differ according to the subtype of depressive disorder, with the closest association observed between dysthymia

UNDERSTANDING TOBACCO ADDICTION NEUROBIOLOGY
• Attention-deficit hyperactivity disorder (ADHD) and tobacco
• Both children and adults with ADHD are significantly more likely to
smoke than non-ADHD controls. This association suggests that
people with ADHD use smoking to improve attention and cognitive
performance. Nicotine administered in a laboratory setting
significantly reduces the symptoms of ADHD, an effect seen in both
smokers and nonsmokers. Nicotine, like the psychostimulants
methylphenidate and dextroamphetamine, acts as an indirect
dopamine agonist, which is relevant to attentional processing within
the brain.

UNDERSTANDING TOBACCO ADDICTION NEUROBIOLOGY
• Anxiety disorders and tobacco
• The presence of an anxiety disorder with or without concurrent depression is associated with an increased likelihood of smoking. Smoking has been found to be a risk factor for the onset of panic disorder and elevated smoking rates are observed in patients with panic disorder. Heavy smoking in adolescence is associated with a higher risk of panic disorder, generalized anxiety disorder, and agoraphobia, even after controlling for confounding variables, such as age, educational status, and parental smoking. Smoking can lead to panic attacks, but the reverse relationship is unlikely and not supported by research findings. Posttraumatic Stress Disorder (PTSD), is associated with rates of smoking around 60%. This is true for women as well as combat veterans with PTSD. Heavy smokers with PTSD are characterized by more total PTSD symptoms as well as increased Cluster C (avoidance and numbing) and Cluster D (hyperarousal) symptoms.
• Despite patients’ subjective reports that smoking reduces anxiety, chronic nicotine use in animal studies is related to increased anxiety. It is unclear to what extent smokers experience withdrawal symptoms and misinterpret a reduction in withdrawal as anxiety relief. Serotonergic interactions with nicotine in the brain seem to mediate at least some of these effects. Serotonin may play an important role in modulating the effects of nicotine, although details of the exact circuitry are still unknown. Areas of the cortex, hippocampus, and dorsal raphe nucleus involve stimulation of 5-HT(1A) receptors and warrant further research. Data from animal and human studies suggest that under certain conditions, nicotine can act as an anxiolytic and antidepressant, but that following chronic use, anxiety is increased.

PLEASE CONSIDER THE…
Challenges
• Tobacco use still causes more deaths
each year than does alcohol, heroin,
cocaine, HIV, homicides, suicides,
fires, and accidents combined
• One third to one half of all cigarettes
smoked in the US are smoked by
people who have had a mental illness
or substance use disorder
• Mental health professionals and
systems are addressing tobacco less
often than in other areas of
healthcare
Changes
• Old view…Quitting tobacco will make them worse.
• New view…Quitting tobacco is part of recovery from a mental illness or substance use disorder. Quitting tobacco won’t hinder progress and might even be beneficial in ways beyond health improvement.
• As administrators or treatment providers we may experience mixed feelings about addressing tobacco. On the one hand we desire and have hope for different situations or outcomes, while at the same time we can be fearful of rocking the boat or reluctant to leave our comfort zone. Addressing tobacco use along with your clients’ other conditions requires confronting old beliefs and ways of doing things as well as attitudes and views of people and what is possible. To be successful, this process of change must take place at multiple levels – with individuals, staff, and the organization. It is important to recognize that nationally, individual clinicians and behavioral health organizations are confronting these same issues, yet recognizing that addressing tobacco use is possible

NICOTINE WITHDRAWALThere is a general consensus that those who smoke at least 10 cigarettes per day,
or those who smoke within 60 minutes of waking, are moderately dependent, and
those who smoke at least 20 cigarettes per day, or within 30 minutes of waking
are highly nicotine dependent.
Withdrawal symptoms can mimic a number of mental health illness symptoms
such as:
• Dysphoric or depressed mood
• Insomnia
• Irritability, frustration, or anger
• Anxiety
• Difficulty concentrating
• Restlessness
• Decreased heart rate
• Increased appetite or weight gain
Withdrawal symptoms can last up to four weeks.

ASSESSMENTS USED TO ASSESS NICOTINE DEPENDENCE
•The Fagerstrom Test for Nicotine
Dependence
•The Hooked on Nicotine Checklist

NICOTINE DEPENDENCE ASSESSMENTS
OTHER FACTORS TO BE ASSESSED
•Patient Self-efficacy
•Environmental Factors and Social Support
•Patient Beliefs about Smoking and Quitting

TREATMENT OPTIONS
•Pharmacotherapy
•Psychosocial Therapy
•Psychotherapeutic Treatments
•Supportive Treatment
•Practical Counseling

PHARMACOLOGICAL THERAPY OPTIONS AND WHY
•HARD TO QUIT WITHOUT TREATMENT
• 70% of smokers report wanting to quit someday
• Few people quit successfully without treatment
• Only 1/3 of quitters (without treatment) remain abstinent
for 2 days
• < 5% ultimately successful on a given quit attempt

PHARMACOLOGICAL THERAPY OPTIONS AND WHY
•RATIONALE
•Doubles changes of successful quit
• Cost-effective
• Reduce or eliminate withdrawal
• Lessen/delay weight gain
• Block reinforcing effects of nicotine

PHARMACOLOGICAL THERAPY OPTIONS
FIRST-LINE TREATMENTS (FDA APPROVED)
•Nicotine Replacement Therapy
• Buproprion
• Zyban/Wellbutrin
• Varenicline
• Chantix
Counseling + Medications = Best treatment plan

PHARMACOLOGICAL THERAPY OPTIONS
• Nicotine Replacement
• Patch
• Gum
• Lozenge
• Inhaler
• Nasal Spray
• Bupropion
• Varenicline
Available OTC but may be covered with prescription state Medicaid.
PHARMACOLOGICAL THERAPY OPTIONS
NICOTINE MEDICATIONS
• Not a carcinogen
• Use high enough dose
• Scheduled better than PRN
• Use long enough time period
• Can be combined with bupropion
• Can be combined with each other
• Have almost no contraindications
• Have no drug-drug interactions
• Safe enough to be OTC

PHARMACOLOGICAL THERAPY OPTIONS
•Smokers misinformed about safety/efficacy
of nicotine
•Not a carcinogen
•Not a significant risk factor for cardiovascular
events
Risk-Benefit ratio supports nicotine
medications over using tobacco
PHARMACOLOGICAL THERAPY OPTIONSCOMBINATION THERAPIES
Improve abstinence rates
Decrease withdrawal
Well-tolerated
• Certain combinations of first-line medications have been shown to be effective smoking cessation
treatments. Effective combination medications are:
• Nicotine patch + nicotine gum or nicotine lozenge or nicotine nasal spray or nicotine inhaler
• Nicotine patch + bupropion SR
• Combining Varenicline with NRT agents is not recommended and may have higher rates of side
effects (e.g., nausea, headaches)
• Varenicline is a partial agonist (causes a little Dopamine release but not enough to be addictive)
• Partially stimulates receptor “Antagonist” –blocks nicotine binding
a4B2 (no good effects from nicotine are felt)
• Some DA release at NAcc
• Prevents Withdrawal

PHARMACOLOGICAL THERAPY OPTIONS
VARENICLINE AND NEUROPSYCHIATRIC SIDE EFFECTS
• Studies not sponsored by Pfizer
• Industry and non-industry funded studies
• NO increased risk of suicide
• NO increased risk of suicidal ideation
• NO increased risk of depression
• NO increased risk of irritability
• NO increased risk of aggression
• Increased risk of sleep disorders
• Increased risk of insomnia
• Increased risk of abnormal dreams
• Reduced risk of anxiety

PHARMACOLOGICAL THERAPY OPTIONS
BLACK BOX WARNINGS
• Antidepressants- suicidal ideation in children
• Lithium- toxicity
• Depakote- hepatic failure
• Lamictal- Toxic epidermal necrolysis
• Wellbutrin- serious allergy, seizure
• Antipsychotics- mortality elderly dementia-psychosis

PSYCHOSOCIAL THERAPY
•Motivational Interviewing
• Behavioral health providers have the required skill
set
• You already help your patients with:
• Problem-Solving
• Coping with difficult situations/emotions
• Social skills training
• Making better choices
• Avoiding high risk situations
PSYCHOSOCIAL THERAPY
•NO SCIENTIFIC EVIDENCE THE FOLLOWING
THERAPIES HELP PEOPLE QUIT SMOKING:
• Hypnosis
• Acupuncture
• Laser therapy (like acupuncture, but no needles)
• E-cigarettes
• Little evidence for e-cigarette efficacy
• Not demonstrated to be as safe as available FDA approved
treatments
• Not regulated by the FDA so chemicals can change per purchase
per producer
PSYCHOSOCIAL THERAPY
WHAT ABOUT THOSE NOT INTERESTED IN QUITTING?
• Build motivation for later
• MI: Decisional balance
• 5 A’s
• Ask about tobacco use
• Advise to quit
• Assess willingness
• Assist in quit attempt
• Arrange follow-up
• Discuss reduction-to-quit
• Use Learning About Healthy Living Manual
PSYCHOSOCIAL THERAPYLEARNING ABOUT HEALTHY LIVING MANUAL- A copy of the manual has been
added to the S:Drive Therapy
Workbook Folders
• Tailored specifically for those with serious mental illness to engage those
who are unmotivated to talk not only about quitting smoking but other
healthy living habits.
• Manual developed to help lower motivated smokers
• For mental health settings
• Group format
• Education on range of topics
• Healthy eating
• Increasing activity

PSYCHOTHERAPY TREATMENTS
•GROUP COUNSELING
• Cost/time effective
• Additional support
• Accepted treatment in Mental Health and addiction
treatment settings
• Modeling
+ Seeing success/use of cessation meds
+ Effective coping
+ May change treatment program norms
- Vocal/outgoing continuing smokers
PSYCHOTHERAPY TREATMENTS
• INDIVIDUAL COUNSELING
• Less time effective, but benefits from greater intensity
• Intervention components can be more personalized
• Facilitates therapeutic alliance
• Avoids shy/anxious/non-talkative patient falling
through cracks in a group

SUPPORTIVE TREATMENT• ENCOURAGE
• Demonstrate your belief your patient can quit
• Note all the available options
• Note that ½ of all smokers have been able to quit
• Note that you’ve helped others quit
• COMMUNICATE CARING/CONCERN
• “How do you feel about quitting?”
• “I’m here to help you.”
• “I know this is tough”
• TALK ABOUT THE QUITTING PROCESS
• Learn about why patient wants to quit
• Learn about previous successes
• Learn about previous difficulties (just enough to avoid them this time)

PRACTICAL COUNSELING• PROVIDE BASIC INFORMATION
• Addiction, not just a “habit”
• Withdrawal
• Meds
• RECOGNIZE HIGH-RISK SITUATIONS
• The treatment program
• Stress, other smokers, alcohol
• Smoking paraphernalia, availability of cigarettes
• DEVELOP COPING SKILLS
• Anticipate and avoid temptations & triggers
• Cognitive and behavioral strategies for:
• Reducing stress/negative affect
• Coping with smoking urges

UNIQUE ISSUES FOR PEOPLE WITH MENTAL ILLNESS
• Persistent psychiatric symptoms
• Poor social skill
• Cognitive limitations
•Difficulty forming a therapeutic alliance
UNIQUE ISSUES FOR PEOPLE WITH MENTAL ILLNESS
• PSYCHIATRIC SYMPTOMS
• Assess psychiatric symptoms each session
• Determine relationship between symptoms and
smoking
• Assess concerns about smoking and their symptoms
• Address symptoms specific coping
• Collaborate with treatment team

UNIQUE ISSUES FOR PEOPLE WITH MENTAL ILLNESS
•SOCIAL SKILLS
• Drug refusal
• Problem solving
• Reduce anger
• Facilitate conversations
• Asking for social support
• Letting family/friends know they are quitting
UNIQUE ISSUES FOR PEOPLE WITH MENTAL ILLNESS
•COGNITIVE LIMITATIONS
• Take extra time when warranted
• Use repetition
• Assess understanding of topics
• Enhance self-efficacy
• Cognitive limitations may inflate OR deflate self-
efficacy
UNIQUE ISSUES FOR PEOPLE WITH MENTAL ILLNESS
•THERAPEUTIC ALLIANCE
• Show empathy- quitting is hard!
• Utilize underlying perspective MI
• Partnership
• Acceptance
• Evocation
• Compassion
• Use Engaging skills of MI

BENEFITS TO QUITTING SMOKING
• You will live longer. People who stop smoking before age 35
avoid 90% of the health risks attributable to tobacco. Even
those who quit later in life can significantly reduce their risk of
dying at a younger age.
• Food will smell and taste better
• Ordinary activities will no longer leave you out of breath
(climbing stairs, light housework)
• You will have more money
• You will have fewer infections including the flu, cold,
pneumonia, and others
• Your skin will have a fresher look and may look younger
BENEFITS TO QUITTING SMOKING
• Within 20 minutes
• Blood pressure and pulse goes back to normal
• After 8 hours
• The carbon monoxide level in your blood drops to normal and the oxygen level
increases
• 24 hours after quitting
• Your chance of heart attack decreases
• 2 weeks to 3 months after quitting
• Your circulation improves and your lung function increases up to 30%
• From 1 to 9 months after quitting
• You stop coughing and breathe easier and your overall energy increases. Your cilia
(tiny hair like structures that more mucus out of the lungs) regain normal function in
the lungs, increasing the ability to handle mucus, clean the lungs, and reduce

BENEFITS TO QUITTING SMOKING
• 1 year after quitting
• The risk of coronary heart disease is cut in half
• 5 years after quitting
• Your chances of lung cancer death and stroke are cut in half
• 10 years after quitting
• The chances of lung cancer are equal to that of a non-smoker. The risk of
cancer of the mouth, throat, esophagus, bladder, kidney, and pancreas
decrease
• 15 years after quitting
• The risk of coronary heart disease is the same as a non-smoker
• 1 year after quitting
• The risk of coronary heart disease is cut in half
• 5 years after quitting
• Your chances of lung cancer death and stroke are cut in half
• 10 years after quitting
• The chances of lung cancer are equal to that of a non-smoker. The risk of
cancer of the mouth, throat, esophagus, bladder, kidney, and pancreas
decrease
• 15 years after quitting
• The risk of coronary heart disease is the same as a non-smoker

CONCLUSIONS
• Too few patients receive tobacco dependence
specific treatment; whether that is
pharmacological, psychosocial,
psychotherapeutic, support, or counseling.
•Combinations of medications and therapeutic
treatments will likely be most effective
•Behavioral health professionals have
requisite skills!
RECOMMENDATIONS• Tobacco use disorders should be added to treatment plans and addressed
with appropriate interventions.
• Patients should be properly screened to make sure symptoms being
displayed are not the results of tobacco withdrawal as the symptoms look
similar to other mental health disorders.
• While policy already states smoking on LRC property is against the rules,
all employees should also be unidentifiable as smokers (i.e. smell,
smoking paraphernalia).
• Quit support program for staff
• Education on effects of smoking and possible treatment
• Incentive plan
• Psychiatrists should be educated on the different NRT methods which can
be used for patients diagnosed with a tobacco use disorder so the

TREATING TOBACCO DEPENDENCE IN BEHAVIORAL HEALTH SETTINGS BIBLIOGRAPHY
AVAILABLE ON THE S:DRIVE

















