ACTA OPHTHALMOLOGICA 61 (1983) 756-768 Universily Eye Hospital Essen, (Head: G. Mqrer-Schwickerath), FRG BJERRUM LECTURE April 23rd, 1983, (Arhus) TREATMENT OF DIABETIC RETINOPATHY WITH PHOTOCOAGULATION Results of photocoagulation therapy of proliferative retinopathy in childhood-onset and maturity-onset diabetes and an approach to the dosage in photocoagulation GERD MEYER-SCHWICKERATH and EDMUND GERKE The results of photocoagulation treatment of proliferative retinopathy in childhood onset and maturity onset diabetes are compared with each other. It is clearly shown that childhood onset diabetes needs more photocoagulation treatment than maturity onset diabetes, and that this difference is statistically significant. From this comparison we approach the problem of the dosage of photocoagulation considering either the surface of the coagulated field or the volume of the coagulated retina. Further papers on the same problem will be published from our hospital. Kqr words: proliferative diabetic retinopathy - photocoagulation. Photocoagulation for the treatment of diabetic retinopathy was introduced by Meyer-Schwickerath (1960) more than 20 years ago. The specific coagulation technique for this disease - a disseminated coagulation of the retina mainly in the midperiphery - was developed by the same author. The effectiveness of this treatment is now firmly established. Especially convincing are the well controlled Received on May 24th. 1983. 756
Transcript
A C T A O P H T H A L M O L O G I C A 61 (1983) 756-768
Universily Eye Hospital Essen, (Head: G . Mqrer-Schwickerath), FRG
B J E R R U M L E C T U R E April 23rd, 1983, (Arhus)
TREATMENT OF DIABETIC RETINOPATHY WITH PHOTOCOAGULATION
Results of photocoagulation therapy of proliferative retinopathy in childhood-onset and
maturity-onset diabetes and an approach to the dosage in photocoagulation
GERD MEYER-SCHWICKERATH and EDMUND GERKE
The results of photocoagulation treatment of proliferative retinopathy in childhood onset and maturity onset diabetes are compared with each other. I t is clearly shown that childhood onset diabetes needs more photocoagulation treatment than maturity onset diabetes, and that this difference is statistically significant. From this comparison we approach the problem of the dosage of photocoagulation considering either the surface of the coagulated field or the volume of the coagulated retina. Further papers on the same problem will be published from our hospital.
Photocoagulation for the treatment of diabetic retinopathy was introduced by Meyer-Schwickerath (1960) more than 20 years ago. T h e specific coagulation technique for this disease - a disseminated coagulation of the retina mainly in the midperiphery - was developed by the same author. T h e effectiveness of this treatment is now firmly established. Especially convincing are the well controlled
Received on May 24th. 1983.
756
Meyer-Schwickerath 8 Gerke Treatment of Diabetic Retinopathy with Photocoagulation
Juveniles with diabetes since childhood
clinical studies in the USA and Great Britain with unilateral treatment in patients with diabetic changes to a similar extent in both eyes. The beneficial effect is present in both the major forms of diabetic retinopathy, but is far more pronounced in proliferative retinopathy compared to non-proliferative retinopathy. A final explanation, however, for the efficacy of the photocoagulation treatment hitherto cannot be given. Several hypotheses have been put forward. The most striking ones are the following two:
1. A chorioretinal scar produced by photocoagulation is characterized by a breakdown of the normal structure of the pigment epithelium. Accumulated toxic substances in the retina can escape into the choroidal vasculature since the barrier function of the pigment epithelium is lost. In addition, retinal nutrition may be ameliorated by free diffusion from the choroid (Peyman et al. 197 1).
2. In proliferative diabetic retinopathy, as a rule, numerous areas of retinal malperfusion, especially in the midperiphery of the retina can be demonstrated by fluoresceinangiography (Shimizu et al. 198 1). Since retinal neovascularization very often is closely related to these hypoxic retina1 areas, it has been postulated that a vasoformative factor is produced in these areas, which provokes and maintains the existence of new vessels (Wise 196 1). If these areas are turned into atrophic scars by means of photocoagulation, this factor is no longer produced. indeed, bot theories support the entirely empirical method of photocoagulation treatment, the rationale of which is to destroy wide areas of retina. The subsequent functional defects of this procedure, such as shrinkage of the visual field and decrease or even loss of scotopic vision clarify a serious dilemma in photocoagulation treatment. I t is therefore desirable, at the present stage of knowledge, to optimize photocoagulation
Adults with maturity-onset diabetes
Table I . Criteria for the 2 groups of diabetics selected for the study.
1. Diagnosis o f diabetes before the 1. Diagnosis o f diabetes after the age o f 1.7 (insulin-dependent) age of 40 (primarily non-insulin-
dependent1
2. Proliferative retinopathy 2. Proliferative retinopathy before the age of 26 without age-limit
3. Three-year-period from first coagulation to last control
3. Three-year-period from first coagulation to last control
757
Meyer-Schwickerath 8 Gerke Treatment of Diabetic Retinopathy with Photocoagulation
Juveniles with diabetes since
childhood
empirically, that means to coagulate just that retinal area necessary to lead to regression of vascular proliferations keeping the functional defects at a minimum. Studies concerning this problem have already been performed by several authors (Chrick et al. 1978; Davies et al. 1979; Gerke et al. 198 1 ; Gjotterberg et al. 198 1 ; Hamilton et al. 1976; McMeel 1977; Meyer-Schwickerath et al. 1981; Schulenburg et a. 1979). The results, however, are hardly conclusive, as the number of coagulation spots recommended by the different authors varies considerably. It may be suggested, that this great variability could be elucidated by a different assessment of the patients to be treated, taking in account different types of diabetes and different types of new vessel formation at the beginning of treatment. As this approach has not yet been done up to the present, the purpose of this study is to compare the results with special regard to the quantitative aspects of photocoagula- tion treatment in - as far as possible - homogeneous groups of diabetic patients with defined types of neovascularization of the retina.
Adults with maturity-onset
diabetes
Patients and Treatment Modalities
Among the diabetic patients attending the Essen University Eye Clinic 2 groups were selected (Table 1).
Patients of the first group had to fulfill the following criteria: 1. Diagnosis of diabetes (insulin-dependent) before the age of 13 years. 2. Occurrence of proli- ferative diabetic retinopathy before the age of 26 years. 3. Duration of treatment
Table 2. Characteristics of both the different groups of diabetics.
Male Female
Age at diagnosis of diabetes (years)
16 35 35 22
6.9 k 3.4 48.0 k 6.1
Duration of diabetes (years) 15.7 f 3.1 10.2 k 6.8
Age of the beginning of coagulation treatment 22.6 k 2.3 58.2 k 7.2
758
Meyer-Schwickerath 8 Gerke Treatment of Diabetic Retinopathy with Photocoagulation
and observation after first coagulation: 3 years, range: 2 years 8 months to 3 years 4 months.
For the second group the following criteria were required: 1 . Diagnosis of diabetes (primary non-insulin-dependent) after the age of 40 years. 2. Occurrence of proliferative diabetic retinopathy without age limit. 3. Duration of treatment and observation after first coagulation: 3 years, range: 2 years 8 months to 3 years 4 months.
In the first group, juvenile patients with insulin-dependent diabetes since childhood, 3 1 patients fulfilled the 3 criteria (Table 2). In 30 patients criteria 2 and 3 were fulfilled for both eyes, but in 21 patients for one eye only. In these 21 patients, the other eye showed either no proliferative retinopathy, or that it had occurred later, or it was already so far advanced that photocoagulation treatment was no longer possible. The study therefore relates to a total of 8 1 eyes. The mean age at the diagnosis of diabetes was 6.9 ? 3.4 years (mean f SD).
The mean age at the diagnosis of proliferative retinopathy was 22.6 k 2.3 years, and the mean duration of diabetes at the time of diagnosis of retinopathy 15.7 k 3.1 years. It is of interest that there were 35 females an only 16 males in this group.
In the second group, adult patients with primarily non-insulin-dependent diabetes diagnosed after the age of 40, 57 patients fulfilled the 3 criteria (Table 2). Twenty-three patients needed insulin therapy later on in the course of their diabetes. The group comprises 91 eyes, 23 eyes had to be excluded for similar reasons as in the first group. The mean age at the diagnosis of diabetes was
1 2 3 4
TYPES OF PROLIFERATIVE DIABETIC RETINOPATHY
Fig. 1 . Grading o f proliferative diabetic retinopathy into 4 different types according to the
appearance of neovascularizations.
759
Meyer-Schwickerath 8 Gerke Treatment of Diabetic Retinopathy with Photocoagulation
Table 3. Criteria for the term stabilization used for the purpose of this study.
Stabilization within the 3-year-period of coagulation and control
Criteria
1. Proliferations unchanged or ameliorated (from type 2 to type 1) or Diseappeared
2. N o haemorrhages during the last 6 months 3. At least 2/3 of fundus visible
48.0 f 6.1 year (mean f SD). The mean duration of diabetes at the diagnosis of retinopathy was 10.2 f 6.8 years. It is interesting to note that there were only 22 females and 35 males in this group.
Retinopathy was classified into the following 4 types (Fig. 1): Type 1 : Peripheral prliferations only. Type 2: Proliferation from the disc with or without peripheral proliferations. Type 3: Peripheral proliferations with epiretinal or intravitreal haemorrhages. Type 4: Proliferations from the disc and peripheral proliferations and epiretinal or intravitreal haemorrhages.
Out of the 8 1 of the juvenile group with insulin-dependent diabetes, 3 1 had type 1, 20 type 2, 9 type 3 and 2 1 type 4 changes. Out of 9 1 eyes in the adult group with primarily non-insulin-dependent diabetes 45 had type 1, 14 type 2, 10 type 3 and 22 type 4 changes.
Three years after the start of therapy all eyes with tractiondetachment were classified as types 3 or 4, because all of them had accompanying intravitreal haemorrhages.
Guidelines of therapy
The technique of disseminated photocoagulation in the retinal midperiphery with a Zeiss-xenon-photocoagulator was used in all patients. The spot size was 3 degrees, exposure time about 0.5 seconds. In a few cases, in which intravitreal haemorrhages prevented photocoagulation, intrascleral peripheral diathermy coagulation or transconjunctival cryocoagulation was performed.
In a small percentage the argon-laser (Coherent Radiation 800) was used for additional coagulation at the posterior pole. Spot size was 200 microns, exposure time from 0.2-0.5 seconds.
760
Meyer-Schwickerath B Gerke Treatment of Diabetic Retinopathy with Photocoagulation
At the beginning of therapy in the juvenile group each eye, within one month, received 2 treatments of about 150 coagulation spots each. In the adult group, often only one coagulation session of about 150-200 spots was done at the beginning of therapy. In order to decide at the subsequent controls - in intervals of 1-3 months - whether additional treatment was necessary or not, the term stabilization served as an important guideline (Table 3). Proliferative diabetic retinopathy was considered stabilized during the 3-year-period of treatment and control if the vascular proliferations were unchanged or ameliorated or if they had disappeared and intravitreal haemorrhages had not occurred within the last 6 months.
At the end of the 3-year-period for stabilization 2/3 of the fundus had to be visible. It was the aim to perform, if needed, additional coagulation treatment up to
stabilization. In a great percentage even complete regression of the proliferations was achieved (37% in the juvenile group and 59% in the adult one). In some cases the desired stabilization could not be achieved by coagulation therapy. This was mainly due to dense intravitreal haemorrhages or early traction detachments, which prevented the extensive supplimentary coagulation that had been planned.
NUMBER OF EVES
L O
30
20
NOT
STABILIZED
STABILIZED
2 3 4 TYPE OF PROLIFERATIONS
Fig. 2. Results of coagulation therapy on the course of proliferations for both the juvenile and the
adult group at the end of the 3-year-period.
76 1
Meyer-Schwickerath 8 Gerke Treatment of Diabetic Retinopathy with Photocoagulation
NUMBER
OF EYES 40
30
20
10
0
AMAUROSIS. LP. HM
from ?&, to 04
from 05 to 18
TYPE OF PFX)LIFERATIONS
Fig. 3 . Results of coagulation therapy on visual acuity for both the juvenile and the adult group at
the end of the 3-year-period.
Results
T h e fundus appearance, either stabilized or not, at the end of the 3-year-period of treatment and observation is shown for both groups in Fig. 2. In the juvenile group at that time 52 eyes out of 81 eyes (64%) can be classified as stabilized, and in the adult group 66 out of 9 1 eyes (73%). Whether proliferative retinopathy is stabilized or not is highly dependent upon the type of proliferation at the beginning of photocoagulation. The ratio stabilizedhon-stabilized in both groups deteriorates from type 1 to type 4. It can be seen from Fig. 2, that this ratio is shifting at only slightly different levels in both groups. In the adult group there is a range of stabilization from 89% in eyes with type 1 changes (40 out of 45 eyes) to 590/ o in . eyes with type 4 changes (13 out of 22 eyes). In the juvenile group the percentage of stabilization in eyes with type 1 changes is only 77% (24 out of 3 1 eyes) shifting to 38% (8 out of 2 1 eyes) in eyes with type 4 changes.
762
Meyer-Schwickerath 8 Gerke Treatment of Diabetic Retinopathy with Photocoagulation
RETINAL SURFPCE RETINAL SURFACE
UP TO ORP. SERWTA UP TO THE AEOUATOR
71 '1.
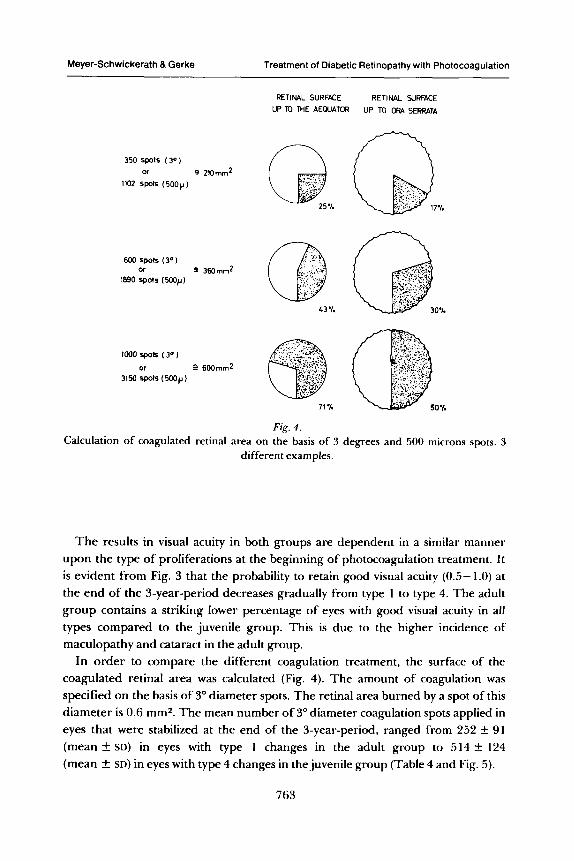
Fir. 4 . v
Calculation of coagulated retinal area on the basis of 3 degrees and 500 microns spots. 3 different examples.
T h e results in visual acuity in both groups are dependent in a similar manner upon the type of proliferations at the beginning of photocoagulation treatment. It is evident from Fig. 3 that the probability to retain good visual acuity (0.5- 1.0) at the end of the 3-year-period decreases gradually from type 1 to type 4. The adult group contains a striking lower percentage of eyes with good visual acuity in a11 types compared to the juvenile group. This is due to the higher incidence of maculopathy and cataract in the adult group.
In order to compare the different coagulation treatment, the surface of the coagulated retinal area was calculated (Fig. 4). The amount of coagulation was specified on the basis of 3" diameter spots. The retinal area burned by a spot of this diameter is 0.6 mm2. The mean number of 3" diameter coagulation spots applied in eyes that were stabilized at the end of the 3-year-period, ranged from 252 k 91 (mean k SD) in eyes with type 1 changes in the adult group to 514 k 124 (mean f SD) in eyes with type 4 changes in the juvenile group (Table 4 and Fig. 5).
763
Meyer-Schwickerath 8 Gerke Treatment of Diabetic Retinopathy with Photocoagulation
Type of proliferations maturity-onset
Number of coagulation spots (3" 4 870 p diameter) up to 'stabilization'
Juveniles with Adults with
diabetes since maturity-onset child hood diabetes
1 327 f 154 (n = 24) 252 f 91 (n = 40)
2
3
4 514 f 124(n = 8) 395 132(n = 13)
503 f 208(n = 15)
417 k 165 (n = 5)
311 k 128(n = 7)
321 f 135(n = 6)
T
1 2 3 d
TYPE OF PROLlF€RAllONS
Fin. 5.
' JUVENILES
ADUL 1.5
- Number of coagulation spots up to stabilization within the 3 years period for juveniles and
adults.
764
Meyer-Schwickerath 8 Gerke Treatment of Diabetic Retinopathy with Photocoagulation
The difference between these 2 amounts of coagulations is significant (P < 0.01) using the Mann Whitney U-Test. Further significant differences in the number of coagulation spots were found in regard to both groups of diabetes as well as to the 4 types of proliferations. The Mann Whitney U-Test was always used.
In the juvenile group the difference in the amount of coagulation spots applied in eyes with type 1 changes is different versus those eyes with type 2 changes (P < 0.0 1) and type 4 changes (P < 0.05).
In the adult group a significant lower number of spots was given in eyes with type 1 changes compared with those with type 4 changes (P < 0.0 1).
Comparing identical types of proliferations in both groups of diabetics the difference in the number of coagulations in type 2 is significant (P < 0.05) as well as the difference in type 4 (P < 0.05) in both groups.
According to the guidelines of the photocoagulation treatment, the entire amount of coagulation spots for a single eye was fractioned into the initial dose and to one or more supplementary doses in case the initial one had not led to stabilization. The number of coagulation sessions performed up to stabilization within the 3-year-period is shown for both the juvenile group and the adult group in Table 5.
Table 5. Number of coagulation sessions for each eye stabilized at
the end of the 3-year-period.
Number of coagulation sessions up to ‘stabilization’
Juveniles with Adults with diabetes since maturity-onset
childhood diabetes
Min 1 Min 1 1.5 2‘2 Max5 Max 4 1 st year
Min 0 0,4 Min 0
Max 2 Max 2 2ndyear 0.3
Min 0 Min 0 Max 1 Max 2 3rdyear 0.1 0.1
765
Meyer-Schwickerath & Gerke Treatment of Diabetic Retinopathy with Photocoagulation
Discussion
It is well known that the type of diabetes plays an important role for the severity and the course of proliferative diabetic retinopathy. For the juvenile diabetics with childhood-onset insulin-dependent diabetes, the clinical course has been described as 'rapid, bloody, blinding' (Beaumont et al. 1972). whereas in non-insulin- dependent maturity-onset diabetics retinopathy consists in background forms with maculopathy often for a long time. Dramatic changes with sudden development of severe neovascularizations are relatively rare events. Nevertheless in all diabetics, as this can be derived from the DRS-Study (Diabetic Retinopathy Study Research Group 1979) the types of proliferations are the main criteria for the risk of severe visual loss, mostly due to intravitreal haemorrhages.
The number of coagulation spots used for treatment of proliferative diabetic retinopathy has been reported by several authors (Crick et al. 1978; Davies et al. 1979; Gerke et al. 1981; Gjotterberg et al. 1981; Hamilton et al. 1976; McMeel 1977; Meyer-Schwickerath 1960; Schulenburg et al. 1979). A few out of them have also attempted the calculation of the coagulated retinal area. The calculation of the retinal areas on the basis of 3" diameter coagulation spots from the studies of the mentioned authors for the purpose of the present study gives clear evidence of considerable differences. For the treatment of proliferative diabetic retinopathy with type 2 changes (graded according to the classification used in the present study) the mean number of coagulation spots applied was about 750, ranging from 530 u p to more than 1000. In contrast, in the present study only 3 1 1 k 208 in the juvenile group were given. The results obtained in those studies can hardly be compared with the results of the present study, for at least 2 reasons: 1. Grouping into non-insulin-dependent and insulin-dependent patients has not been attempted and 2. the time of observation was much shorter than 3 years.
Neglecting these facts, in one of the studies (Davies et al. 1979) the obtained success rate is roughly similar to the success rate of the present study. But the considerably major coagulated ratinal area reported in these studies in contrast to the present one is difficult to explain. I t can be speculated, that, though the coagulated retinal area may be equal, the applied coagulation technique with the argon-laser or the xenon-photocoagulator could help to elucidate this question: since the argon-laser burn usually is performed with an exposure time of 0.1 to 0.2 sec. and the xenon burn at an exposure time of about 0.5 sec. or more, the coagulated retinal volume most probably is different (Bornfeld et al. 1981). The major retinal volume would therefore be coagulated by the xenon technique compared to the argon laser technique, though the coagulated retinal areas may be equal. Indeed, the coagulation therapy in some of the mentioned studies is done by
766
Meyer-Schwickerath 8 Gerke Treatment of Diabetic Retinopathy with Photocoagulation
means o f the argon laser, the present one, however, mainly by the xenon photocoagulator. This speculation fits well to the hypothesis, that ischemic retina has t o be destroyed for the treatment of proliferative diabetic retinopathy.
Whatever the explanation of this difference may be, photocoagulation treatment for proliferative diabetic retinopathy hitherto is a n entirely empirical treatment. It is not causative, but symptomatic and by necessity destructive. Therefore, the aim for therapy by photocoagulation is to apply the adequate dose in the individual case. The individual patient has to be treated by a n individual approach according to the type of diabetes a n d according to the type of proliferations. T h e dilemma of necessary retinal destruction and subsequent defects such as shrinkage of visual field and decrease in scotopic vision can be resolved best in this way. The guidelines for the photocoagulation therapy that may be concluded from this study are therefore: 1. An initial treatment u p to the number of coagulation spots elaborated for the individual eye according to the type of diabetes and to the type of proliferations. 2. A close follow-up with documentation whether stabilization is achieved or not. 3. Re-treatment in case retinopathy is not stabilized.
With these guidelines it seems possible to treat eyes with a very bad prognosis as in childhood-onset diabetics with results relatively similar to eyes with a n initially better prognosis as in adult-onset diabetics. Overtreatment in this way may be avoided and irreversible side-effects may be kept to a minimum.
References
Beaumont P & Hollows F C (1972): Classification of diabetic retinopathy with therapeutic implications. Lancet 1 : 4 19.
Bornfeld N, Gerke E & El-Hifnawi E (1982): Licht- und rasterelektronenmikroskopische Untersuchungen an frischen und vernarbten Xenon-Lichtkoagulationsherden der Netzhaut von ‘mini-pigs’. Fortschr Ophthalmol79: 15 1 - 154.
Chen H ( 1976): Response of proliferative diabetic retinopathy to xenon-arc photocoagula- tion. Trans Ophthalmol Soc U K 96: 224.
Crick M D P, Chignell H & Schilling J S (1978): Argon Laser v. Xenon arc photocoagulation in proliferative diabetic retinopathy. Trans Ophthalmol Soc UK 98: 170.
Davies e W G, OConnell E J A, Murray A & Winter J (1979): Peripheral retinal ablation in diabetic retinopathy. Trans Ophthalmol97: 17.
Diabetic Retinopathy Study Research Group (1976): Preliminary Report on Efects on Photocoagulation Therapy. Am J Ophthalmol8 1 : 383.
Diabetic Retinopathy Study Research Group (1979): Four risk factors for severe visual loss in diabetic retinopathy. Arch Ophthalmol97: 654.
Gerke E & Meyer-Schwickerath G (198 1): Koagulationstherapie der proliferativen diabe- tischen Retinopathie bei Jugendlichen. Klin Monatsbl Augenheilkd 179: 157.
767
Meyer-Schwickerath 8 Gerke Treatment of Diabetic Retinopathy with Photocoagulation
Gjiitterberg M & Blomdahl S (1981): Human Electroretinogram after Argon Laser Photo-
Hamilton A M, Townsend C. Kohoury D & Could E (1976): Treatment of the new vessels on
McMeel J W (1977): In: Davis M D et al. (eds). Symposium on Retinal Disease, p 116. Mosby,
Meyer-Schwickerath G (1960): Light-Coagulation. Mosby St. Louis. Meyer-Schwickerath G & Fried M (198 I ) : Treatment of diabetic retinopathy with photo-
coagulation. How many coagulations have to be performed in the individual case? Dev Ophthalmol2: 265.
Peyman G A, Spitznas M & Straatsma B (197 1) : Chorioretinal diffusion of peroxidase before and after photocoagulation. Invest Ophthalmol 10: 489.
Schulenburg W E, Hamilton A M & Blach R-K (1979): A comparative study of argon laser and krypton laser in the treatment of diabetic optic disc neovascularisation. Br J Ophthalmol63: 4 12.
Shimizu K, Gerke E & Muraoka K (1981): Midperipheral Fundus Involvement in Diabetic Retinopathy. Ophthalmology 88: 601.
Wise G M (1961): Factors influencing new vessel formation. Am J Ophthalmol52: 637.
coagulation of different retinal areas. Ophthalmic Res 13: 42.
the disc in diabetic retinopathy Trans Ophthalmol SOC UK 96: 228.
St. Louis:
Author’s addre.r.7:
Prof. Dr. G. Meyer-Schwickerath, Universitats-Augenklinik Essen, Hufelandstrasse 55, D-4300 Essen, FRG.