Review Treatment of elopement in individuals with developmental disabilities: A systematic review Russell Lang a, *, Mandy Rispoli a , Wendy Machalicek b , Pamela J. White a , Soyeon Kang a , Nigel Pierce a , Austin Mulloy a , Tina Fragale a , Mark O’Reilly a , Jeff Sigafoos c , Giulio Lancioni d a The Meadows Center for Preventing Educational Risk, The University of Texas at Austin, Austin, TX, USA b Portland State University, Portland, Oregon, USA c Victoria University of Wellington, New Zealand d University of Bari, Italy Research in Developmental Disabilities 30 (2009) 670–681 ARTICLE INFO Article history: Received 5 November 2008 Received in revised form 12 November 2008 Accepted 18 November 2008 Keywords: Elopement Challenging behavior Developmental disability Functional analysis ABSTRACT We reviewed studies involving the treatment of elopement in individuals with developmental disabilities. Systematic searches of three electronic databases, journals, and reference lists identified 10 studies meeting the inclusion criteria. These studies were evaluated in terms of: (a) participants, (b) procedures used to assess elopement, (c) intervention procedures, (d) results of the inter- vention, and (e) certainty of evidence. Across the 10 studies, intervention was provided to a total of 53 participants aged 3–47 years. Assessment procedures included anecdotal staff reports, participant interviews, direct observation, and modified analog functional analysis. Intervention approaches included differential reinforcement, extinction, functional communication training, response blocking, non-contingent reinforcement, shaping, and scheduled exercise. Positive outcomes were reported in 80% of the reviewed studies. The evidence base suggests that function-based assessment (e.g. functional analysis procedures) and function- based treatments (e.g. functional communication training) may be most effective in the treatment of elopement in this population. Directions for future research are offered. ß 2008 Elsevier Ltd. All rights reserved. * Corresponding author at: Department of Special Education, 1 University Station D53000, The University of Texas at Austin, Austin, TX 78712, United States. Tel.: +1 254 716 1508. E-mail address: [email protected](R. Lang). Contents lists available at ScienceDirect Research in Developmental Disabilities 0891-4222/$ – see front matter ß 2008 Elsevier Ltd. All rights reserved. doi:10.1016/j.ridd.2008.11.003
Transcript
Review
Treatment of elopement in individuals with developmentaldisabilities: A systematic review
Russell Lang a,*, Mandy Rispoli a, Wendy Machalicek b, Pamela J. White a,Soyeon Kang a, Nigel Pierce a, Austin Mulloy a, Tina Fragale a, Mark O’Reilly a,Jeff Sigafoos c, Giulio Lancioni d
a The Meadows Center for Preventing Educational Risk, The University of Texas at Austin, Austin, TX, USAb Portland State University, Portland, Oregon, USAc Victoria University of Wellington, New Zealandd University of Bari, Italy
Research in Developmental Disabilities 30 (2009) 670–681
A R T I C L E I N F O
Article history:
Received 5 November 2008
Received in revised form 12 November 2008Accepted 18 November 2008
Keywords:
Elopement
Challenging behavior
Developmental disability
Functional analysis
A B S T R A C T
We reviewed studies involving the treatment of elopement in
individuals with developmental disabilities. Systematic searches of
three electronic databases, journals, and reference lists identified 10
studies meeting the inclusion criteria. These studies were evaluated
in terms of: (a) participants, (b) procedures used to assess
elopement, (c) intervention procedures, (d) results of the inter-
vention, and (e) certainty of evidence. Across the 10 studies,
intervention was provided to a total of 53 participants aged 3–47
years. Assessment procedures included anecdotal staff reports,
participant interviews, direct observation, and modified analog
functional analysis. Intervention approaches included differential
reinforcement, extinction, functional communication training,
response blocking, non-contingent reinforcement, shaping, and
scheduled exercise. Positive outcomes were reported in 80% of the
reviewed studies. The evidence base suggests that function-based
assessment (e.g. functional analysis procedures) and function-
based treatments (e.g. functional communication training) may be
most effective in the treatment of elopement in this population.
Directions for future research are offered.
� 2008 Elsevier Ltd. All rights reserved.
* Corresponding author at: Department of Special Education, 1 University Station D53000, The University of Texas at Austin,
Austin, TX 78712, United States. Tel.: +1 254 716 1508.
Elopement, which can be defined as leaving an area without supervision or caregiver permission, isprevalent among persons with developmental disabilities (Jacobson, 1982; Lowe et al., 2007) and mayexpose a person to dangerous situations (e.g. open bodies of water, traffic). Additionally, elopementcan disrupt classroom instruction, complicate residential living, and require additional staff support toensure the person’s safety (Padgett, Garcia, & Pernice, 1984; Perrin, Perrin, Hill, & DiNovi, 2008;Thorne, 1947). Without appropriate assessment and treatment, elopement tends to persist in peoplewith developmental disabilities (Murphy et al., 2005).
The assessment and treatment of elopement presents unique challenges. In particular, asophisticated understanding of contextual variables (e.g. the setting the individual is running awayfrom) may be required for assessment (Piazza et al., 1997). Additionally, because infrequentelopement is still potentially life threatening, interventions successful in reducing, but noteliminating, elopement are not likely to be considered socially valid. Despite such challenges andthe relatively high prevalence of elopement in persons with developmental disabilities, no reviews onthe treatment of elopement in persons with developmental disabilities currently exist to guideevidence-based practice.
To facilitate evidence-based practice in this important area, we herein provide a systematic reviewof studies on the treatment of elopement for individuals with developmental disabilities. Theobjective of this review was to describe the characteristics of these studies (e.g. participants, targetbehaviors, intervention procedures), evaluate intervention outcomes, and appraise the certainty of theevidence for the existing corpus of intervention studies. A review of this type was primarily intendedto guide and inform evidence-based practice in the assessment and treatment of elopement inindividuals with developmental disabilities. A secondary aim was to identify gaps in the existingdatabase so as to stimulate future research efforts aimed at developing new and more effectiveassessments and interventions for this dangerous and common behavior.
1. Method
This review involved a systematic analysis of studies that focused on the treatment of elopement inindividuals with developmental disabilities. Each identified study that met pre-determined inclusioncriteria was analyzed and summarized in terms of: (a) participants, (b) procedures used to assesselopement, (c) intervention procedures, (d) results of the intervention, and (e) certainty of evidence.To assess the certainty of evidence, we critically appraised each study’s design and relatedmethodological details (e.g. procedural descriptions and reliability of data).
R. Lang et al. / Research in Developmental Disabilities 30 (2009) 670–681 671
1.1. Search procedures
Systematic searches were conducted in three electronic databases: Education ResourcesInformation Center (ERIC), Psychology and Behavioral Sciences Collection, and PsycINFO. Publicationyear was not restricted, but the search was limited to English-language and peer-reviewed studies. Onall three databases, the terms ‘‘elopement’’, ‘‘wandering’’, and ‘‘running away’’ plus ‘‘developmentaldisability’’, ‘‘autism’’, ‘‘mental retardation’’, ‘‘intellectual disability’’, ‘‘Down syndrome’’, or ‘‘syn-drome’’ were inserted into the keywords field. The abstracts of the resulting 75 studies were reviewedto identify studies for inclusion (see Inclusion and Exclusion Criteria below). The reference lists forstudies meeting these criteria were also reviewed to identify additional articles for possible inclusion.Hand searches, covering the year 2008, were then completed for the journals that had published theincluded studies. Our search of the databases, journals, and reference lists occurred during Septemberand October, 2008.
1.2. Inclusion and exclusion criteria
To be included in this review, the article had to describe a research study that contained anintervention for elopement for at least one person with a developmental disability. Elopementintervention was defined as implementing one or more therapeutic/teaching procedures for thepurpose of trying to decrease the person’s elopement, wandering, or running away behavior. Studiesthat focused only on the description of elopement or elopers were not included (e.g. Nussbaum, Lang,Chan, & Riviere, 1994). Additionally, studies in which a diagnosis of developmental disability wasuncertain were excluded (e.g. Hargett & Webster, 1996).
1.3. Data extraction
Each identified study was first assessed for inclusion/exclusion. Then, each included study wassummarized in terms of the following features: (a) participants, (b) procedures used to assesselopement, (c) intervention procedures, (d) results of the intervention, and (e) certainty of evidence.Various procedural aspects were noted, including setting, experimental design, inter-observeragreement, treatment integrity, and follow-up data. Main findings were summarized in terms of theextent to which participants were reported to have shown a decrease in some dimension of elopement(e.g. frequency, distance, minutes spent out of area). Certainty of evidence was evaluated byconsidering the main findings in light of the design and other methodological details. The certainty ofevidence for each study was rated as either conclusive or inconclusive based on the definitions appliedby Millar, Light, and Schlosser (2006).
Appraising the certainty of evidence followed a two-stage process. First, only studies that included anexperimental design (e.g. multiple-baseline and ABAB) could be considered as having the potential toprovide conclusive evidence. Thus, any study that lacked a recognized experimental design wasautomatically classified as inconclusive. This included narrative case studies, pre-post testing without acontrol group, and studies using A–B or intervention-only designs. Second, studies that made use of anexperimental design also had to meet four additional standards to be classified as providing conclusiveevidence: (a) The data had to provide a convincing demonstration of an intervention effect. Thisdetermination was based on visual inspection of data trends within and across phases using criteriadescribed by Kennedy (2005). For example, there had to be a clinically significant decrease of elopementwhen intervention was introduced. (b) If relevant, there had to be adequate interobserver agreement data(e.g.20%ofthe sessions and 80%orbetter agreement). (c) Thedependentand independentvariableshadtobe operationally defined. (d) The procedures had to be described in sufficient detail to enable replication.
1.4. Inter-rater agreement
The first author made an initial determination as to whether each study from the pool of 75 met theinclusion criteria. After this, the fourth through eighth authors independently assessed each of thestudies against the inclusion/exclusion criteria. Agreement as to whether a study should be included
R. Lang et al. / Research in Developmental Disabilities 30 (2009) 670–681672
or excluded was obtained on 70 of the 75 studies (93%). To resolve the discrepancies, the secondauthor independently assessed the five studies on which there was initial disagreement. The overallresult was that 10 studies were included for analysis in this review.
The first, second, and third author extracted information to develop an initial summary of the 10included studies. The accuracy of these summaries was independently checked by one of theremaining co-authors using a checklist that included the initial summary of the study and a number ofquestions regarding various details of the study (e.g. Is this an accurate description of the participants?Is this an accurate description of the assessment procedures? Is this an accurate summary of thecertainty of evidence?). Co-authors were asked to read the study and the summary and then completethe checklist. In cases where the summary was not considered accurate, the co-authors were asked toedit the summary to improve its accuracy. The resulting summaries were then used in the table.
This approach was intended to ensure accuracy in the summary of studies, but it also provided ameasure of inter-rater agreement on data extraction and analysis. There were 80 items on which therecould be agreement or disagreement (i.e. 10 studies with 8 questions per study). Agreement wasobtained on 75 items (94%). In the 5 instances where aspects of the summaries were consideredinaccurate, changes were made to more accurately summarize the studies.
2. Results
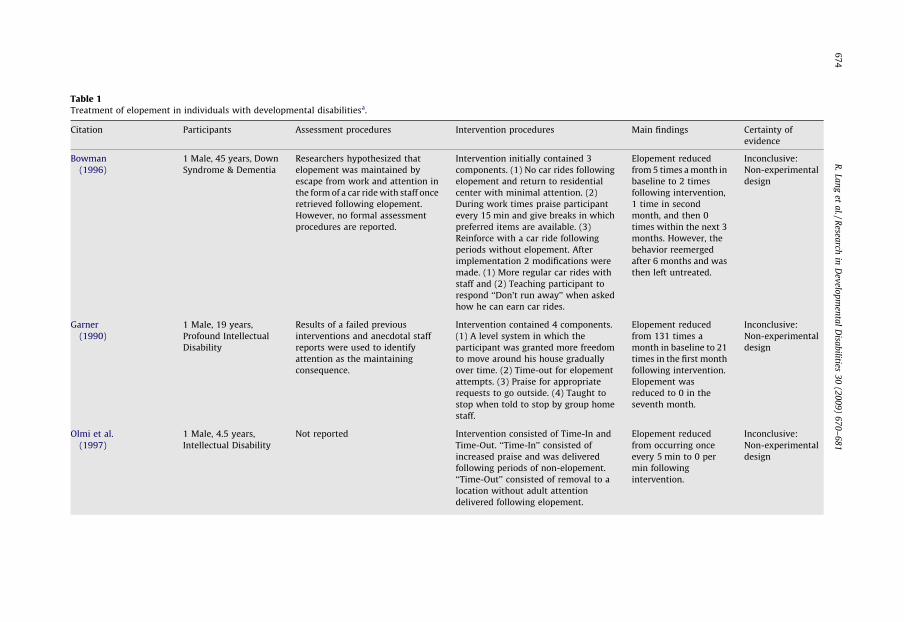
Appendix lists the 10 included studies. Table 1 summarizes the (a) participants, (b) nature ofelopement, (c) procedures used to assess elopement, (d) intervention procedures, (e) results of theintervention, and (f) certainty of evidence of these 10 studies.
2.1. Participants
Collectively, the 10 studies provided intervention to a total of 53 participants. The sample size ofindividual studies ranged from 1 to 39. Six studies included only one participant. Three studies hadtwo or three participants (see Table 1). The remaining study (Thorne, 1947) was comparatively largewith a sample size of 39. Participant ages ranged from 3 to 47 years. Thirty seven (70%) of theparticipants were male and 16 (30%) were female. The participants in these studies were diagnosedwith various types of disabilities including Asperger’s syndrome, autism, dementia, Down syndrome,emotional disorder, intellectual disability, seizure disorder, and Attention Deficit HyperactivityDisorder. The most common diagnosis (n = 47) was intellectual disability.
2.2. Settings
All of the studies reviewed provided descriptions of the intervention setting. Intervention wasimplemented in residential or institutional facilities (n = 5), community or vocational settings (n = 2),a group home (n = 1), a classroom (n = 1), and an outpatient clinic (n = 1).
2.3. Assessment procedures
All but two of the studies (Olmi, Sevier, & Nastasi, 1997; Whitaker & Saleem, 1994) discussed thefunction (maintaining consequence) of the participants’ elopement. Two studies provided ahypothesis as to the function of elopement, but did not conduct formal assessments (Bowman,1996; Rapp, Volmer, & Hovantez, 2005). The remaining six studies utilized some type of formalassessment including interviewing service providers or the participants themselves (Garner, 1990;Thorne, 1947), direct observation (Padgett et al., 1984), and functional analyses (Perrin et al., 2008;Piazza et al., 1997; Tarbox, Wallace, & Williams, 2003).
2.4. Intervention procedures
Elopement was most commonly treated with intervention packages. Combinations of thefollowing intervention components were utilized: (a) differential reinforcement, (b) extinction, (c)
R. Lang et al. / Research in Developmental Disabilities 30 (2009) 670–681 673
Table 1Treatment of elopement in individuals with developmental disabilitiesa.
Citation Participants Assessment procedures Intervention procedures Main findings Certainty of
evidence
Bowman
(1996)
1 Male, 45 years, Down
Syndrome & Dementia
Researchers hypothesized that
elopement was maintained by
escape from work and attention in
the form of a car ride with staff once
retrieved following elopement.
However, no formal assessment
procedures are reported.
Intervention initially contained 3
components. (1) No car rides following
elopement and return to residential
center with minimal attention. (2)
During work times praise participant
every 15 min and give breaks in which
preferred items are available. (3)
Reinforce with a car ride following
periods without elopement. After
implementation 2 modifications were
made. (1) More regular car rides with
staff and (2) Teaching participant to
respond ‘‘Don’t run away’’ when asked
how he can earn car rides.
Elopement reduced
from 5 times a month in
baseline to 2 times
following intervention,
1 time in second
month, and then 0
times within the next 3
months. However, the
behavior reemerged
after 6 months and was
then left untreated.
Inconclusive:
Non-experimental
design
Garner
(1990)
1 Male, 19 years,
Profound Intellectual
Disability
Results of a failed previous
interventions and anecdotal staff
reports were used to identify
attention as the maintaining
consequence.
Intervention contained 4 components.
(1) A level system in which the
participant was granted more freedom
to move around his house gradually
over time. (2) Time-out for elopement
attempts. (3) Praise for appropriate
requests to go outside. (4) Taught to
stop when told to stop by group home
staff.
Elopement reduced
from 131 times a
month in baseline to 21
times in the first month
following intervention.
Elopement was
reduced to 0 in the
seventh month.
Inconclusive:
Non-experimental
design
Olmi et al.
(1997)
1 Male, 4.5 years,
Intellectual Disability
Not reported Intervention consisted of Time-In and
Time-Out. ‘‘Time-In’’ consisted of
increased praise and was delivered
following periods of non-elopement.
‘‘Time-Out’’ consisted of removal to a
location without adult attention
delivered following elopement.
Elopement reduced
from occurring once
every 5 min to 0 per
min following
intervention.
Inconclusive:
Non-experimental
design
R.
Lan
get
al./R
esearch
inD
evelo
pm
enta
lD
isab
ilities3
0(2
00
9)
67
0–
68
16
74
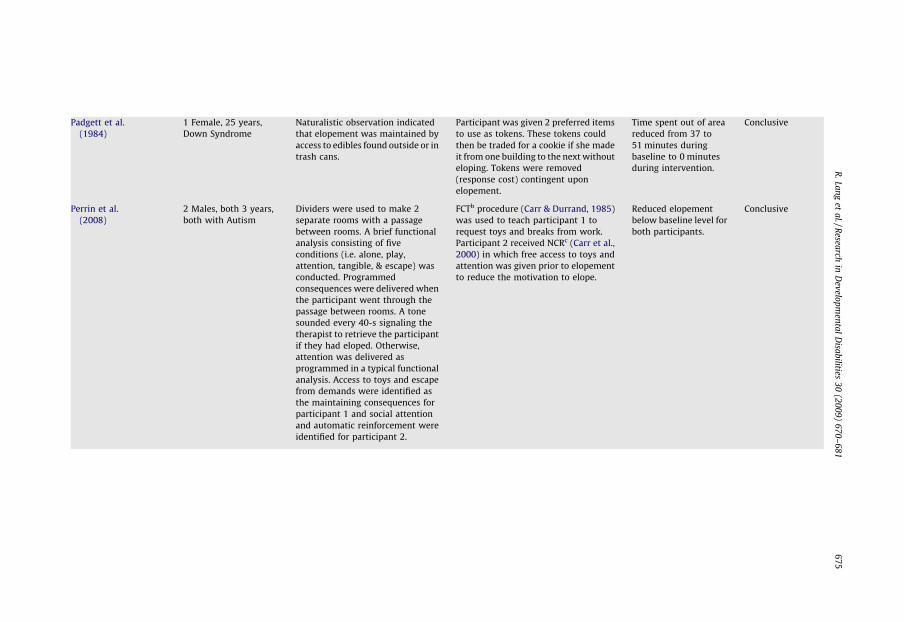
Padgett et al.
(1984)
1 Female, 25 years,
Down Syndrome
Naturalistic observation indicated
that elopement was maintained by
access to edibles found outside or in
trash cans.
Participant was given 2 preferred items
to use as tokens. These tokens could
then be traded for a cookie if she made
it from one building to the next without
eloping. Tokens were removed
(response cost) contingent upon
elopement.
Time spent out of area
reduced from 37 to
51 minutes during
baseline to 0 minutes
during intervention.
Conclusive
Perrin et al.
(2008)
2 Males, both 3 years,
both with Autism
Dividers were used to make 2
separate rooms with a passage
between rooms. A brief functional
analysis consisting of five
conditions (i.e. alone, play,
attention, tangible, & escape) was
conducted. Programmed
consequences were delivered when
the participant went through the
passage between rooms. A tone
sounded every 40-s signaling the
therapist to retrieve the participant
if they had eloped. Otherwise,
attention was delivered as
programmed in a typical functional
analysis. Access to toys and escape
from demands were identified as
the maintaining consequences for
participant 1 and social attention
and automatic reinforcement were
identified for participant 2.
FCTb procedure (Carr & Durrand, 1985)
was used to teach participant 1 to
request toys and breaks from work.
Participant 2 received NCRc (Carr et al.,
2000) in which free access to toys and
attention was given prior to elopement
to reduce the motivation to elope.
Reduced elopement
below baseline level for
both participants.
Conclusive
R.
Lan
get
al./R
esearch
inD
evelo
pm
enta
lD
isab
ilities3
0(2
00
9)
67
0–
68
16
75
Table 1 (Continued )
Citation Participants Assessment procedures Intervention procedures Main findings Certainty of
evidence
Piazza et al.
(1997)
3 Males, age 10, 11, & 4
years old. (1)
Intellectual Disability,
Autism, Attention
Deficit, Seizure
Disorder, (2)
Intellectual Disability,
Autism, Bipolar
Disorder, & (3) Cerebral
Palsy, Seizure Disorder,
Learning & Speech
Delays
Naturalistic observation identified
possible maintaining consequences
for each participant. Analog
functional analyses were arranged
to approximate these idiosyncratic
variables (Hanley, Iwata, & McCord,
2003). Two joined assessment
rooms were simultaneously
available to the participant during
functional analysis conditions. For
the third participant, the functional
analysis was conducted in an open
common area. Programmed
consequences were delivered when
the participants eloped to the
adjoining room, or in the case of the
third participant, when he broke
away from the therapist. For each
participant, the functional analyses
indicated multiply maintained
elopement. Thus, follow-up
reinforcer-assessment conditions
were created in which the differing
maintaining consequences were
compared to a control condition
(e.g. free toy play). Final results
indicated attention was the
maintaining consequence for
participants 1 and 3, and preferred
tangibles for participant 2.
Participant 1: Non-contingent access to
preferred items. Participant 2:
Differential reinforcement of
alternative behavior plus blocking of
elopement. Participant 3:
reinforcement for absence of behavior.
Reduced elopement
below baseline levels
for all 3 participants.
Conclusive
Rapp et al.
(2005)
1 Female,14 years old,
Autism
Naturalistic observation identified
escape and avoidance of swimming
pool as the maintaining
consequence for elopement.
Systematic desensitization consisting
of progressive stages of exposure (i.e.
approach pool, sit in chair near pool,
moving chair towards pool, entering
pool, standing in pool, and then
swimming). Each step was reinforced
with praise and/or small edibles.
Attempts to elope were blocked during
intervention.
Gradual reduction in
elopement, results
generalized across
settings and
maintained at 10-
month follow-up.
Conclusive
R.
Lan
get
al./R
esearch
inD
evelo
pm
enta
lD
isab
ilities3
0(2
00
9)
67
0–
68
16
76
Tarbox et al.
(2003)
3 Males 6, 28, & 39
years old, (1) Asperger’s
Syndrome, (2)
Intellectual Disability,
& (3) Intellectual
Disability
Modified analog functional
analyses were implemented by
trained caregivers in contrived
clinical settings arranged to
approximate the variables
associated with each participant’s
elopement (i.e. enclosed public area
or table at vocational program). 10-
s demand, attention, and control
conditions were implemented for
each participant. Confederates
were used during sessions to
ensure the safety of participants.
Access to tangibles was identified
as the maintaining consequence for
participants 1 and 2. Access to
attention was identified as the
maintaining consequence for
participant 3.
Participant 1 and 2: FCTb to request
tangibles plus blocking elopement.
Participant 3: non-contingent access to
attention and a 5-s delay in attention
contingent upon elopement.
Elopement decreased
below baseline levels
for all 3 participants.
Conclusive
Thorne (1947) 25 Males, 14 Females,
ages 10 to 44 years old,
all with Intellectual
Disability
Participants interviewed by
psychiatrist to determine
motivation for elopement. Found
most common causes were
suggestions to elope made by other
patients, or to escape/avoid social
situations (e.g. teasing).
Staff told to maintain ‘‘high morale’’
and make living conditions as pleasant
as possible. Punished with one week in
isolation following 3rd elopement.
74% of participants did
not elope more than 2
more times following
intervention.
Inconclusive:
Non-experimental
design
Whitaker
and Saleem
(1994)
1 Male, 47 years,
Intellectual Disability
Not reported. Scheduled walking trips with staff. Reduced elopement,
but self-injury
increased.
Inconclusive:
Non-experimental
design
a Studies are listed in alpha-chronological order by year of publication and then by the first author’s surname.b Functional communication training.c Non-contingent reinforcement.
R.
Lan
get
al./R
esearch
inD
evelo
pm
enta
lD
isab
ilities3
0(2
00
9)
67
0–
68
16
77
time out procedure, (d) token economy, (e) response cost, (f) functional communication training, (g)response blocking, and (h) non-contingent reinforcement. Whitaker and Saleem (1994) was the onlystudy to evaluate a single component intervention (i.e. scheduled periods of exercise).
2.5. Study designs
Study designs were classified as experimental or non-experimental. Five of the studies involving atotal of 43 participants were classified as non-experimental (see Table 1). Four of the studies in thiscategory utilized an AB design (Bowman, 1996; Garner, 1990; Olmi et al., 1997; Whitaker & Saleem,1994). Thorne (1947) conducted a records review to determine the number of elopements from aresidential facility. Five studies involving 10 participants were classified as experimental. Two studiesimplemented reversal designs (Padgett et al., 1984; Rapp et al., 2005), and one study utilized analternating treatments design (Perrin et al., 2008). Two studies consisted of different experimentaldesigns for different participants. Piazza et al. (1997) implemented both multielement and ABABdesigns. Tarbox et al. (2003) used a multielement design embedded within a multiple baseline designfor two participants and an ABAB design for the third participant.
2.6. Reliability of data and treatment integrity
Seven studies reported the reliability of data collection with respect to the dependent variables,such as by collecting interobserver agreement (IOA). In all cases the resulting percentages ofagreement were at or above the generally accepted standard of 80% (Kennedy, 2005). Procedures toassess treatment integrity were conducted in one study (Perrin et al., 2008). In this study theresearchers assessed the extent to which the interventionist implemented the treatment using achecklist of treatment procedures.
2.7. Outcomes
Outcomes were classified as positive, mixed, or negative based on the data presented by theauthors. Positive outcomes were defined as outcomes in which the participant showed improvementon all target behaviors with intervention or in which improvement was noted for all participantswithin the study. Mixed outcomes were defined as studies in which some of the participantsdemonstrated improvement in the target behavior while others did not or in which improvement wasnoted in some but not all of the target behaviors. Negative outcomes were defined as participants notshowing improvement in the target behavior. Overall, 80% of the studies reported positive outcomes(see Table 1) and 20% reported mixed outcomes (Bowman, 1996; Thorne, 1947). No studies reportednegative outcomes.
2.8. Certainty of evidence
The certainty of evidence in each study was classified as conclusive or inconclusive. The certainty ofevidence for an intervention effect was rated as conclusive for five studies (Padgett et al., 1984; Perrinet al., 2008; Piazza et al., 1997; Rapp et al., 2005; Tarbox et al., 2003). For the other five studies, thecertainty of evidence for an intervention effect was judged to be inconclusive. These inconclusiveratings were due to the use of non-experimental designs (Bowman, 1996; Garner, 1990; Olmi et al.,1997; Thorne, 1947; Whitaker & Saleem, 1994).
3. Discussion
Our systematic search yielded 10 studies targeting the treatment of elopement in individuals withdevelopmental disabilities. Summaries of these studies revealed that the existing literature base isperhaps best described as limited with respect to the overall scope and quality of the existing corpus ofstudies. In terms of scope, the current database must be considered limited because of the sheerpaucity of studies (n = 10) and the relatively few number of participants (n = 53) (39 from Thorne,
R. Lang et al. / Research in Developmental Disabilities 30 (2009) 670–681678
1947). In terms of methodological quality, perhaps the most important limitation is that many of thestudies appeared to lack a recognized experimental design. Thus the reports of positive outcomes for80% of the studies must be interpreted with caution.
In terms of the main aim of this paper, to advance evidence-based practice for treatment ofelopement in individuals with developmental disabilities, none of the reviewed treatments wouldqualify as ‘‘well established’’ evidence-based practice according to Odom et al. (2005). However, thereviewed research does suggest that elopement may often be maintained by operant contingenciesand reduced by function-based interventions (Perrin et al., 2008; Piazza et al., 1997; Tarbox et al.,2003). The studies with the most conclusive evidence ostensibly suggest a two-step process;practitioners should (a) assess elopement to identify its operant function, and (b) implement afunction-based intervention.
Eight studies discussed the operant function of elopement and implemented function-basedinterventions. The methods used to assess elopement varied considerably. Three studies observedparticipants in their natural environments and noted environmental changes that seemed to correlatewith elopement (Bowman, 1996; Padgett et al., 1984; Rapp et al., 2005). When these changes appearedto produce a pleasant consequence for the person’s eloping, that consequence was hypothesized to bethe function (maintaining consequence) for elopement. Treatment then consisted of either makingthat consequence contingent on the non-occurrence of elopement (i.e. differential reinforcement ofother behavior) or it was given freely to the participant prior to elopement so as to remove themotivation to elope (i.e. non-contingent reinforcement). For example, Bowman (1996) utilized thismethod with a participant who was observed in his residential care facility. The researcher noted thatelopement was likely to occur when the participant was given independent work to complete.Additionally, following elopement, the participant usually received a car ride (a preferred activity)back to his residence. Escape from work and access to a car ride were hypothesized to be the functionsof elopement. Treatment was then designed to match these functions by providing the participantwith more frequent car rides and breaks from work.
Two studies used interview procedures to identify potential functions for elopement. Garner(1990) interviewed the participant’s teacher and Thorne (1947) interviewed the participantsthemselves. The interview simply consisted of asking the person why elopement occurred or whatwas obtained or avoided by eloping. Reasonable answers were then hypothesized to function asreinforcement for elopement. In the Thorne (1947) study, psychiatrists interviewed the patients of aninpatient facility regarding their elopement. The most common response concerned avoiding socialsituations and being teased. The corresponding intervention included a function-based component(i.e. instructing the staff to ‘‘maintain a higher morale’’ that included limiting the teasing amongpatients) and a non-function-based punishment component (i.e. restricted freedoms).
The above methods may be effective in some instances, but are ultimately limited because theoperant function of elopement was determined via indirect methods (i.e. observation by researcher orteacher) and potentially biased self-reports. Additionally, such methods do not systematically testmultiple potential functions. A more reliable method for assessing function, and therefore more likelyto lead to successful treatment, is to directly test environmental contingencies in an experimentaldesign. Only three studies employed functional analysis procedures that utilized rigorousexperimental designs (Perrin et al., 2008; Piazza et al., 1997; Tarbox et al., 2003). In theseassessments, potential functions are first hypothesized (e.g. obtaining preferred tangibles or activities,obtaining attention, avoiding task demands, and avoiding attention) and then situations in whichthese contingencies can be delivered following elopement are contrived. By comparing the rates ofelopement when a specific potential consequence is made contingent upon elopement to rates in acontrol condition where all possible consequences are freely provided, a more confident empiricallyvalidated function can be determined. Table 1 describes the assessment procedures andcorresponding interventions for the studies which utilized these methods (Perrin et al., 2008; Piazzaet al., 1997; Tarbox et al., 2003).
In regards to our second aim, which was to identify gaps in the literature, several topics for futureresearch have arisen from this review. Foremost is the need for more research in which the effects ofinterventions designed to reduce elopement are evaluated using rigorous experimental methods thatoffer the potential for providing a greater certainty of evidence. Single-subject methodology may offer
R. Lang et al. / Research in Developmental Disabilities 30 (2009) 670–681 679
researchers a viable design for assessing and intervening on elopement, but the studies to date havecontained a small number of participants, the generality of these assessment and interventionprocedures remains to be determined.
To advance evidence-based practice in the treatment of elopement, future research is needed tofurther establish the effectiveness of functional analysis and function-based interventions. Severalimplications arise from this assertion. First, research should focus on developing appropriate methodsfor directly assessing the operant function of elopement. Such methodology may need to includerefined versions of traditional functional analysis procedures to address safety concerns. Interestingly,no study reported the use of functional assessment interviews or rating scales (e.g. Questions AboutBehavioral Functions Scale [QABF]) to initially identify the consequences maintaining elopement(Applegate, Matson, & Cherry, 1999; Freeman, Walker, & Kaufman, 2007; Matson, Bamburg, Cherry, &Paclawskyj, 1999). The successful assessment and treatment of elopement may require thedevelopment of systematic procedures for initially identifying the social consequence(s) maintainingelopement.
Second, this literature base suggests that function-based treatments, in which the implementedstrategies directly match the assessed function for elopement, may be effective in decreasing thebehavior. However, no study directly compared function-based to non-function-based treatments forelopement. Future research could explore such comparisons in order to enhance understanding of theimportance of a relation between the function of elopement and corresponding treatment.
While 80% of the studies reviewed here reported positive results, only two studies reported thecomplete elimination elopement (Olmi et al., 1997; Padgett et al., 1984). Due to the dangerous natureof the problem, perhaps more stringent criteria for classifying study outcomes as positive should beemployed. Future research should seek new treatments that effectively eliminate such behavior.
Acknowledgements
The authors would like to thank the Eli and Edythe L. Broad Center for Asperger’s Research at theKoegel Autism Center, University of California, Santa Barbara for their support.
References
Applegate, H., Matson, J. L., & Cherry, K. E. (1999). An evaluation of functional variables: Affecting severe problem behaviors in adultswith mental retardation by using the Questions About Behavioral Function Scale (QABF). Research in Developmental Disabilities,20, 229–237.
Bowman, L. (1996). Behavior modification and down syndrome dementia: A case study of treatment in real life setting. Develop-mental Disabilities Bulletin, 42, 58–67.
Carr, J., Coriaty, S., Wilder, D., Gaunt, B., Dozier, C., Britton, L., et al. (2000). A review of ‘‘noncontingent’’ reinforcement astreatmentfor aberrant behavior of individuals with developmental disabilities. Research in Developmental Disabilities, 21, 377–391.
Carr, E. G., & Durrand, V. M. (1985). Reducing behavior problems through functional communication training. Journal of AppliedBehavior Analysis, 18, 111–126.
Freeman, K. A., Walker, M., & Kaufman, J. (2007). Psychometric properties of the Questions About Behavioral Function Scale in a childsample. American Journal of Mental Retardation, 2, 122–129.
Garner, M. (1990). The treatment of elopement behavior in a retardate using a graduated levels program. Journal of Behavior Therapyand Experimental Psychiatry, 21, 277–280.
Hanley, G. P., Iwata, B. A., & McCord, B. E. (2003). Functional analysis of problem behavior: A review. Journal of Applied BehaviorAnalysis, 36, 147–185.
Hargett, M. Q., & Webster, R. E. (1996). Treatment integrity and acceptability with families: A case study of a child with school refusal.Psychology in the Schools, 33, 319–324.
Jacobson, J. W. (1982). Problem behavior and psychiatric impairment within a developmentally delayed population I: BehaviorFrequency. Applied Research in Mental Retardation, 3, 121–139.
Kennedy, C. H. (2005). Single-case designs for educational research. Boston: Allyn & Bacon.Lowe, K., Allen, D., Jones, E., Brophy, S., Moore, K., & James, W. (2007). Challenging behaviours: Prevalence and topographies. Journal of
Intellectual Disability Research, 51, 625–636.Matson, J. L., Bamburg, J. W., Cherry, K. E., & Paclawskyj, T. R. (1999). A validity study on the Questions About Behavior Function
(QABF) Scale: Predicting treatment success for self-injury, aggression, and stereotypies. Research in Developmental Disabilities, 20,163–176.
Millar, D. C., Light, J. C., & Schlosser, R. W. (2006). The impact of augmentative and alternative communication intervention on thespeech production of individuals with developmental disabilities: A research review. Journal of Speech, Language, and HearingResearch, 49, 248–264.
R. Lang et al. / Research in Developmental Disabilities 30 (2009) 670–681680
Murphy, G., Beadle-Brown, J., Wing, L., Gould, J., Shah, A., & Holmes, N. (2005). Chronicity of challenging behaviours in people withsevere intellectual disabilities and/or autism: A total population sample. Journal of Autism and Developmental Disorders, 35, 405–418.
Nussbaum, D., Lang, M., Chan, B., & Riviere, R. (1994). Characterization of elopers during remand: Can they be predicted? TheMETFORS experience. American Journal of Forensic Psychology, 12, 17–37.
Odom, S. L., Brantlinger, E., Gersten, R., Horner, R. H., Thompson, B., & Harris, K. R. (2005). Research in special education: ScientificMethods and evidence-based practices. Exceptional Children, 71, 137–148.
Olmi, J. D., Sevier, R. C., & Nastasi, D. F. (1997). Time-in/time-out as a response to noncompliance and inappropriate behavior withchildren with developmental disabilities: Two case studies. Psychology in School, 34, 31–39.
Padgett, W. L., Garcia, H. D., & Pernice, M. B. (1984). A travel training program: Reducing wandering in a residential center fordevelopmentally disabled persons. Behavior Modification, 8, 317–330.
Perrin, C. J., Perrin, S. H., Hill, E. A., & DiNovi, K. (2008). Brief functional analysis and treatment of elopement in preschoolers withautism. Behavioral Interventions, 23, 87–95.
Piazza, C. C., Hanley, G. P., Bowman, L. G., Ruyter, J. M., Lindauer, S. E., & Saiontz, D. M. (1997). Functional analysis and treatment ofelopement. Journal of Applied Behavior Analysis, 30, 653–672.
Rapp, J., Vollmer, T., & Hovanetz, A. N. (2005). Evaluation and treatment of swimming pool avoidance exhibited by an adolescent girlwith autism. Behavior Therapy, 36, 101–105.
Tarbox, R. S., Wallace, M. D., & Williams, L. (2003). Assessment and treatment of elopement: A replication and extension. Journal ofApplied Behavior Analysis, 36, 239–244.
Thorne, F. C. (1947). The problem of institutional elopements. American Journal of Mental Deficiency, 4, 637–643.Whitaker, S., & Saleem, A. (1994). The effect on non-contingent exercise on purposeless wandering and self injury in a man with a
profound learning difficulty. Behavioral and Cognitive Psychotherapy, 22, 99–102.
R. Lang et al. / Research in Developmental Disabilities 30 (2009) 670–681 681