å¡ CASE REPORT å¡ Treatment of Lymphocytic Hypophysitis by High-Dose Methylprednisolone Pulse Therapy Keiko YAMAGAMI, Katsunobu YOSHIOKA,Haruna Sakai, Mariko FUKUMOTO, Tetsuya Yamakita, Masayuki Hosoi, Tomofusa ISHII, Toshihiko SATO, Shiro Tanaka and Satoru FuJII Abstract A 26-year-old woman3 months post-partum was ad- mitted to our hospital suffering from gross visual distur- bance. Magnetic resonance imaging (MRI) revealed a pituitary mass, extending into the suprasellar cistern, with intense gadolinium enhancement. Lymphocytic hy- pophysitis (LHy) was suspected, and the patient received high dose methylprednisolone pulse therapy (HDMPT). Her visual disturbance was dramatically ameliorated on the first day following initiation of HDMPT,and MRI re- vealed marked mass reduction. Her pituitary function re- covered 6 months after therapy. This case report suggests that HDMPT proved effective for mass reduction of se- vere LHyand could obviate the need for a useless sur- gery. (Internal Medicine 42: 168-173, 2003) Key words: lymphocytic hypophysitis, high dose methyl- prednisolone pulse therapy, pituitary mass, vis- ual disturbance, magnetic resonance imaging Introduction Lymphocytic hypophysitis (LHy) is a rare autoimmune disease, usually diagnosed following pituitary biopsy, or di- agnosed unexpectedly during assessment for a presumed pi- tuitary adenoma. Recently, corticosteroid therapy has been recommended when LHy is suspected clinically, even with- out pathological confirmation (1, 2). Although high dose (1 mg/body weight) prednisolone is usually preferred in order to allow quick evaluation of the therapeutic response, when gross visual disturbance is present, the response time may be delayed. In fact, gross visual disturbance may be potentially irreversible, resulting in surgical intervention. The role of high-dose methylprednisolone pulse therapy (HDMPT) in such cases has rarely been reported. In this report, we outline a case of LHywith gross visual disturbance, showing remarkable improvement of symptoms one day post-initiation of HDMPT therapy, with MRI confir- mationof massreduction. For editorial comment, see p 137. Case Report A 26-year-old womanwas admitted to our hospital on January 12, 2001 with a headache and visual field defect. She had delivered without complication of a female infant on October 26, 2000. Twomonths postpartum, she consulted an ophthalmologist due to headache and poor vision. Ophthalmologic examination revealed bitemporal hemiano- pia and the patient was referred to our hospital for further ex- amination. At the time of admission, the patient was 159.2 cm tall and weighed 51.2 kg. Her blood pressure was 1 10/60 mmHg, with a pulse rate of 84/min. No goiter or enlargement of lymph nodes was noted. The remainder of the examination was unremarkable. Laboratory findings on admission re- vealed mild normochromic anemia as shown in Table 1. Her corrected visual acuity was 0.1 in the right eye and 0.01 in the left eye, and critical fusion frequency (CFF) was low, particularly in the left eye (right 41 Hz, left 10 Hz). In the MRI study performed on January 15, the sagittal Tl-weighted image of contrast material revealed a mass en- larging the sella turcica extending into the suprasellar cistern, and abutting the optic chiasm (Fig. 1A). The mass showed intense enhancementafter administration of contrast mate- rial. The clinical course and MRIfindings were suspicious for LHy. The patient's visual impairment was severe enough to From Department of Internal Medicine, Osaka City General Hospital, Osaka Received for publication June 17, 2002; Accepted for publication October 9, 2002 Reprint requests should be addressed to Dr. Keiko Yamagami, Department of Internal Medicine, Osaka City General Hospital, 2-13-22 Miyakojima- Hondori, Miyakojima, Osaka 534-0021 168 Internal Medicine Vol. 42, No. 2 (February 2003)
Transcript
å¡ CASE REPORT å¡
Treatment of Lymphocytic Hypophysitis by High-DoseMethylprednisolone Pulse Therapy
A 26-year-old woman3 months post-partum was ad-mitted to our hospital suffering from gross visual distur-bance. Magnetic resonance imaging (MRI) revealed apituitary mass, extending into the suprasellar cistern,with intense gadolinium enhancement. Lymphocytic hy-pophysitis (LHy) was suspected, and the patient receivedhigh dose methylprednisolone pulse therapy (HDMPT).Her visual disturbance was dramatically ameliorated onthe first day following initiation of HDMPT,and MRI re-vealed marked mass reduction. Her pituitary function re-covered 6 months after therapy. This case report suggeststhat HDMPTproved effective for mass reduction of se-vere LHyand could obviate the need for a useless sur-gery.
(Internal Medicine 42: 168-173, 2003)
Key words: lymphocytic hypophysitis, high dose methyl-prednisolone pulse therapy, pituitary mass, vis-ual disturbance, magnetic resonance imaging
Introduction
Lymphocytic hypophysitis (LHy) is a rare autoimmunedisease, usually diagnosed following pituitary biopsy, or di-agnosed unexpectedly during assessment for a presumed pi-tuitary adenoma. Recently, corticosteroid therapy has been
recommendedwhen LHy is suspected clinically, even with-out pathological confirmation (1, 2). Although high dose (1mg/body weight) prednisolone is usually preferred in orderto allow quick evaluation of the therapeutic response, whengross visual disturbance is present, the response time maybedelayed. In fact, gross visual disturbance may be potentiallyirreversible, resulting in surgical intervention. The role of
high-dose methylprednisolone pulse therapy (HDMPT) in
such cases has rarely been reported.In this report, we outline a case of LHywith gross visualdisturbance, showing remarkable improvement of symptomsone day post-initiation of HDMPTtherapy, with MRI confir-mationof massreduction.
For editorial comment, see p 137.
Case ReportA 26-year-old womanwas admitted to our hospital onJanuary 12, 2001 with a headache and visual field defect.
She had delivered without complication of a female infant onOctober 26, 2000. Twomonths postpartum, she consulted anophthalmologist due to headache and poor vision.Ophthalmologic examination revealed bitemporal hemiano-
pia and the patient was referred to our hospital for further ex-amination.
At the time of admission, the patient was 159.2 cm talland weighed 51.2 kg. Her blood pressure was 1 10/60 mmHg,with a pulse rate of 84/min. No goiter or enlargement oflymph nodes was noted. The remainder of the examinationwas unremarkable. Laboratory findings on admission re-vealed mild normochromic anemia as shown in Table 1. Hercorrected visual acuity was 0.1 in the right eye and 0.01 inthe left eye, and critical fusion frequency (CFF) was low,
particularly in the left eye (right 41 Hz, left 10 Hz).In the MRI study performed on January 15, the sagittalTl-weighted image of contrast material revealed a mass en-larging the sella turcica extending into the suprasellar cistern,and abutting the optic chiasm (Fig. 1A). The mass showedintense enhancementafter administration of contrast mate-rial. The clinical course and MRIfindings were suspiciousfor LHy.
The patient's visual impairment was severe enough to
From Department of Internal Medicine, Osaka City General Hospital, OsakaReceived for publication June 17, 2002; Accepted for publication October 9, 2002Reprint requests should be addressed to Dr. Keiko Yamagami, Department of Internal Medicine, Osaka City General Hospital, 2-13-22 Miyakojima-
Hondori, Miyakojima, Osaka 534-0021
168 Internal Medicine Vol. 42, No. 2 (February 2003)
Lymphocytic Hypophysitis and Pulse
Table 1. Laboratory Data on AdmissionBlood cell count Urea nitrogen 14.3 mg/dl U rinalv sisWhite blood cell 4,03 0/mm3 C reatinine 0.9 mg/dl O sm o la l it y 6 3 8 mO s m /k g H2 O
band cell 8 % U rem ic acid 5.3 mg/dlsegmented cell 32 % S od iu m 139 mEq/l E n do crin olo gical fin din gslymphoid cell 4 1% P otassiu m 3.5 mEq/Z F r e e T 3 2 . 1 p g / m lM on o cyte 1 1% C hloride 104 mEq/ / F r e e T 4 0 . 6 n g / d lE osin op hil 8 % G lu co se 87 mg/dl T S H 0 . 2 5 u l U / m lB asophil 0 % C R P 0.06 mg/dl A C T H 1 5 p g / m l
Red blood cell 40 6x lO 7mm 3 A C E 12.9 IU/Z C or t i s o 1 4 . 1 u g / d lH em og lob in l l.1 g/d l L y so zy m e 6.2 ug/ml A D H 3 .6 7 p g/m lPl atelet 2 9 .9x lO4/ul G H 7 . 0 4 n g / m l
Im m u n ity tests P ro l a c t i n 9 . 4 n g / m lBlood chemistry A n tinu clear an tibo dy neg ative L H 0 . 4 m l U / m lT otal protein 6.3 g/dl An ti TPO a ntibody neg ative F S H 7 . 4 m l U / m iA lbu m in 4.0 g/dl A nti thy ro globu lin antib od y n egativ eA m y lase 2 17 TU /Z A nti rat pituitary antib od y neg ativeA ST 2 7 IU /ZA L T 2 4 TU /ZA L P 16 4 TU /ZL D H 24 7 TU //
warrant immediate intervention to relieve the mass effect.Although such surgery in LHy leads to rapid relief of neuro-logical symptoms, it is deleterious on the pituitary function.Further, because the patient hoped to conceive another in-fant, we decided to perform surgery only if she did not re-spond to steroid therapy. The patient agreed with treatmentplan. Therefore, we administered HDMPT (1 g methyl-prednisolone daily for three days). One-day status-postHDMPT initiation, the patient's visual sensation becomeclear and her headache was dramatically improved. MRI
taken 3 days later revealed marked mass reduction (Fig. IB).Weconfirmed LHy, and a pharmacological dose of predni-solone (30 mg daily) was initiated. Her visual acuity was im-proved to 0.15 in the right eye and 0.3 in the left eye, and
CFF was also improved (right 43 Hz, left 35 Hz). When thedose of prednisolone was tapered to 25 mg daily, the patientcomplained of the return of poor vision. Subsequent MRIre-vealed pituitary re-enlargement (Fig. 1C). Therefore, methyl-prednisolone pulse therapy (0.5 g daily for two days) wasinitiated, resulting in vision improvement and MRI-confirmed pituitary mass reduction (Fig. ID). High doses ofprednisolone (50 mg daily) were initiated and tapered gradu-ally without recurrence of the disease on low-dose pre-
dnisolone (10 mg daily) (Fig. 3).Endocrine assessment prior to the initiation of steroid
thyrotropin (0.25 plU/ml), and a low, blunted thyrotropin re-sponse to thyrotropin releasing hormone (TRH) (Fig. 2A).Cortisol and adrenocorticotropin (ACTH) were low, and
ACTH response to corticotropin releasing hormone wasblunted. Follicle stimulating hormone (FSH) and luteinizinghormone (LH) responses to LH releasing hormone wereblunted. Growth hormone (GH) and prolactin responses
proved to be blunted during provocative testing. Posterior pi-tuitary function was deemed normal because she had normalurine output with a urinary osmolality of 638 mOsm/kgH2O,and antidiuretic hormone was 3.67 pg/ml. Furthermore, shehad normal urine output even after initiation of steroid ther-apy. Neither anti-thyroid nor anti rat pituitary antibodieswere detected. Endocrinological examination 6 months afterinitiation of steroid therapy revealed normalization of thyroidfunction and normal TSHand ACTHresponses to provoca-tive testing. The GH response to GH releasing hormone(GRH) was marked (Fig. 2B).
Discussion
LHyis a rare autoimmune disease, usually diagnosed bypituitary biopsy or unexpectedly during the work-up for apresumed pituitary adenoma. Recently, it has been proposedthat the diagnosis of LHycan be made without pathologicalconfirmation in a high proportion of patients (3). In this set-ting, the differential diagnosis includes pituitary adenoma,sarcoidosis, tuberculosis, syphilis, and primary granulo-
matous hypophysitis. The present patient was diagnosed ashaving LHy without pituitary biopsy for the following rea-sons.
In most cases of LHy, as with our patient, initial clinical
Internal Medicine Vol. 42, No. 2 (February 2003) 169
Yamagamiet al
w
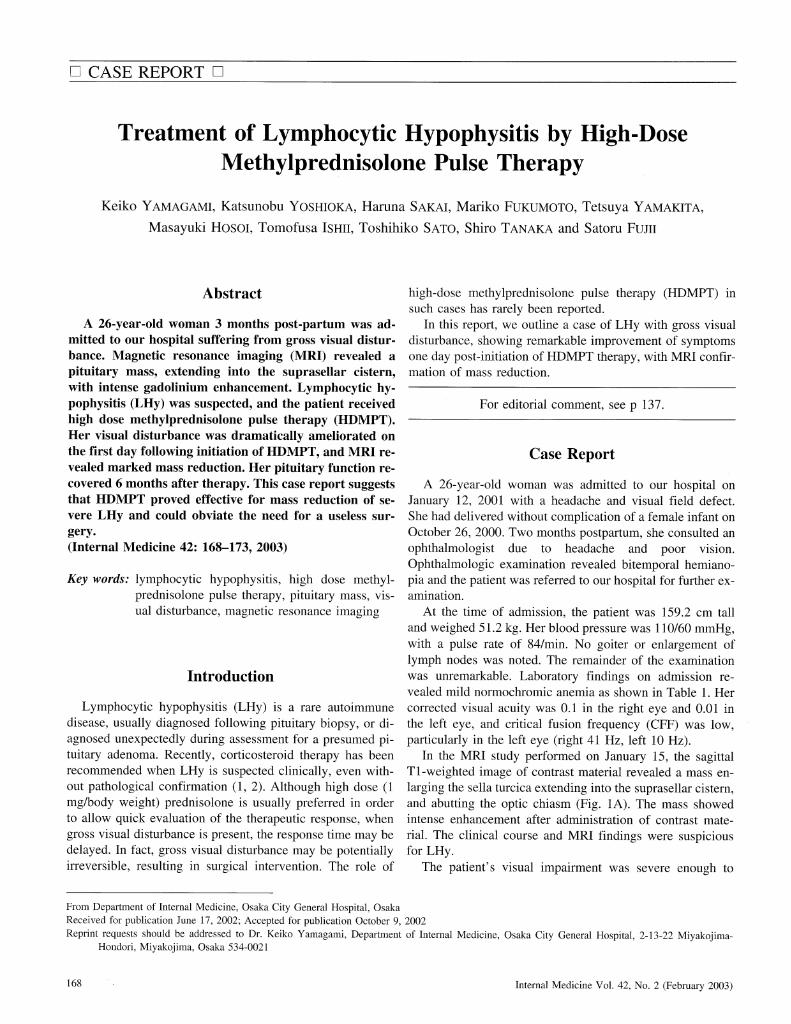
Figure 1. A: Magnetic resonance imaging (MRI) finding on January 15 shows a mass enlarging the sella turcica, and extend-ing into the suprasellar cistern. B: MRIfinding on January 19, after three days of methylprednisolone pulse therapy (1 gdaily), shows mass reduction. C: MRI finding on January 30 shows pituitary re-enlargement. D: MRI finding on February9, after two days of methylprednisolone pulse therapy (0.5 g daily), shows mass reduction.
symptomsoccur in young womenin the third trimester ofgestation or in the postpartum period. It has been reportedthat neuron-specific enolase, which is expressed in normal
human pituitary, is localized in normal humanplacenta, thusestablishing a direct link between pituitary and placentalautoantigens. This link provides a theoretical basis for thestrong predilection of LHyto occur during or after preg-nancy (4).
It has been reported that MRIstudies are useful for thedifferentiation of LHy from pituitary adenoma. Marked and
homogeneouscontrast enhancement of the pituitary gland ischaracteristic of LHy, while pituitary macroadenomastypi-cally show only moderate enhancement (5). In the presentcase, pituitary adenoma was unlikely because gadolinium
uptake by the pituitary gland was intense and homogeneous.Furthermore, rapid regression of the pituitary mass immedi-ately following high-dose HDMPTmade the diagnosis of pi-tuitary adenoma even less likely. Medical history, laboratoryfindings (angiotensin-converting enzyme for sarcoidosis,
treponema pallidum test for syphilis), and chest radiography
170 Internal Medicine Vol. 42, No. 2 (February 2003)
Lymphocytic Hypophysitis and Pulse
CR H 1 00 u g i. v.
4 00
V
3 00fcuOa
20 0
b 10 0
ACTH Cortisol
O'V
0 30 60
T RH 5 00 ug i .v .
(m in )
T S H
20 , *
a 15
蝣¥u3 10E ^ ^ ^ ^ s =CO rH 5
90
PRL
120
100
60
40
20
0
bo
GH
30 60
(min)
FSH
90
LH
120
120
A
Cortisol
TR H 5 00 jug i. v.
2 0 i
^
6 15
p3 10Xt- < 5
TSH ' å PRL
GH
B
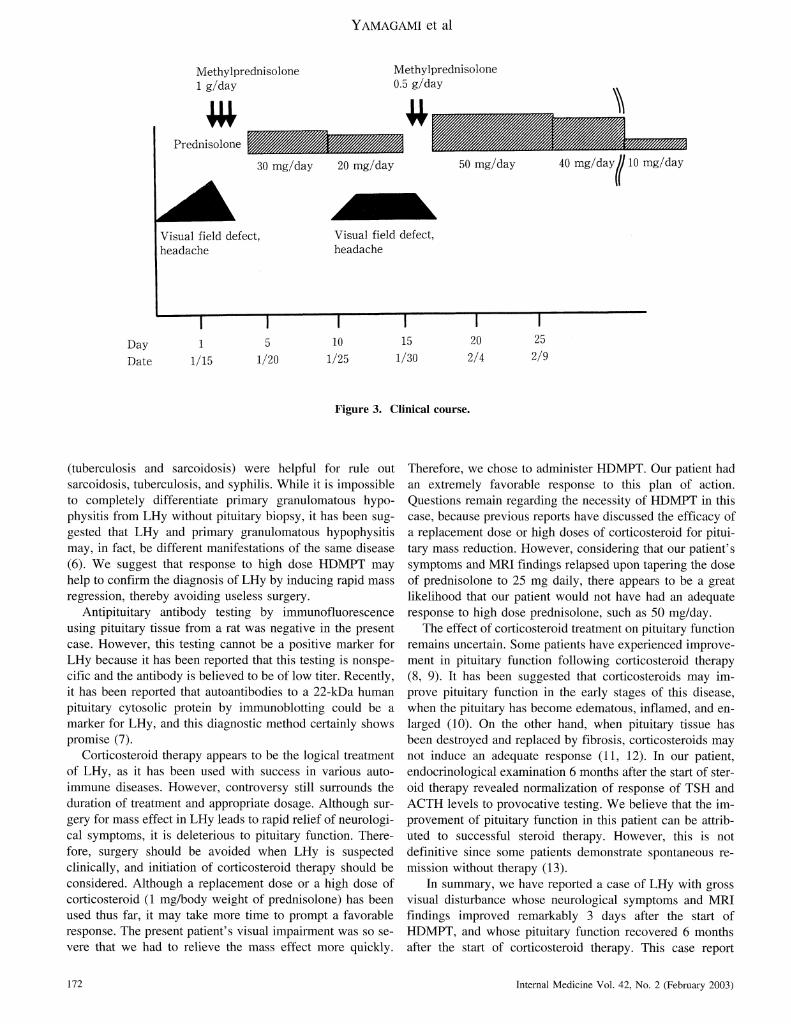
Figure 2. Response of pituitary and adrenal hormones to intravenous injection of CRH(100 jug), GRH(100 jig), TRH(500jig), and LH-RH(100 jag) before (A) and after (B). CRH: corticotropin releasing hormone, GH: growth hormone, GRH: GHreleasing hormone, TRH thyrotropin releasing hormone, LH: luteinizing hormone, FSH: follicle stimulating hormone, LH-RH: LH releasing hormone, TSH: thyrotropin, ACTH:adrenocorticotropin.
Internal Medicine Vol. 42, No. 2 (February 2003) 171
Yamagamiet al
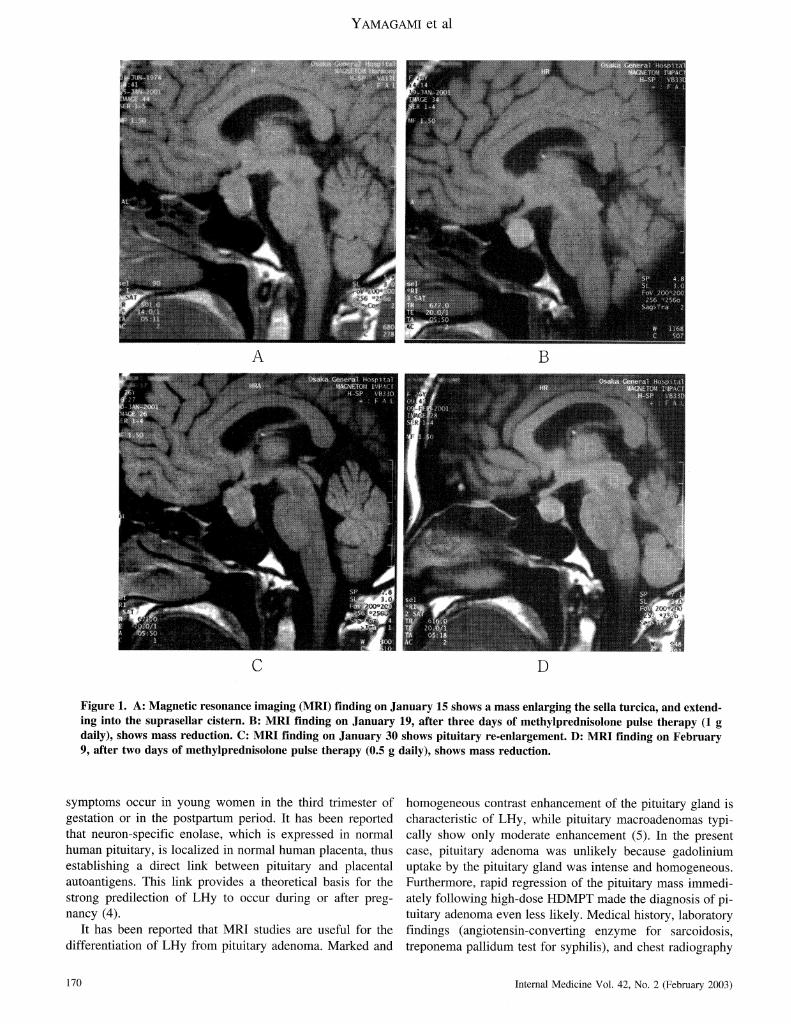
Methylprednisol one1 g/day
Methylprednisolone0.5 g/day
w
30 mg/day 20 mg/day
Visual field defect,headache
50 mg/day 40 mg/dayII 10 mg/day
Visual field defect,headache
D a y 1 5 1 0 1 5 2 0 2 5
D a te 1 / 1 5 1 / 2 0 1 / 2 5 1 / 3 0 2 / 4 2 / 9
Figure 3. Clinical course.
(tuberculosis and sarcoidosis) were helpful for rule outsarcoidosis, tuberculosis, and syphilis. While it is impossibleto completely differentiate primary granulomatous hypo-physitis from LHy without pituitary biopsy, it has been sug-gested that LHy and primary granulomatous hypophysitismay, in fact, be different manifestations of the same disease(6). Wesuggest that response to high dose HDMPTmayhelp to confirm the diagnosis of LHy by inducing rapid massregression, thereby avoiding useless surgery.
Antipituitary antibody testing by immunofluorescenceusing pituitary tissue from a rat was negative in the presentcase. However, this testing cannot be a positive marker forLHy because it has been reported that this testing is nonspe-cific and the antibody is believed to be of low titer. Recently,it has been reported that autoantibodies to a 22-kDa humanpituitary cytosolic protein by immunoblotting could be amarker for LHy, and this diagnostic method certainly showspromise (7).
Corticosteroid therapy appears to be the logical treatmentof LHy, as it has been used with success in various auto-immunediseases. However, controversy still surrounds the
duration of treatment and appropriate dosage. Although sur-gery for mass effect in LHy leads to rapid relief of neurologi-cal symptoms, it is deleterious to pituitary function. There-fore, surgery should be avoided when LHy is suspectedclinically, and initiation of corticosteroid therapy should beconsidered. Although a replacement dose or a high dose ofcorticosteroid (1 mg/body weight of prednisolone) has beenused thus far, it may take more time to prompt a favorableresponse. The present patient's visual impairment was so se-vere that wehad to relieve the mass effect morequickly.
Therefore, we chose to administer HDMPT.Our patient hadan extremely favorable response to this plan of action.Questions remain regarding the necessity of HDMPTin thiscase, because previous reports have discussed the efficacy ofa replacement dose or high doses of corticosteroid for pitui-tary mass reduction. However, considering that our patient'ssymptomsand MRIfindings relapsed upon tapering the doseof prednisolone to 25 mg daily, there appears to be a greatlikelihood that our patient would not have had an adequateresponse to high dose prednisolone, such as 50 mg/day.The effect of corticosteroid treatment on pituitary functionremains uncertain. Somepatients have experienced improve-ment in pituitary function following corticosteroid therapy(8, 9). It has been suggested that corticosteroids may im-prove pituitary function in the early stages of this disease,when the pituitary has become edematous, inflamed, and en-larged (10). On the other hand, when pituitary tissue has
been destroyed and replaced by fibrosis, corticosteroids maynot induce an adequate response (ll, 12). In our patient,
endocrinological examination 6 months after the start of ster-oid therapy revealed normalization of response of TSHandACTHlevels to provocative testing. Webelieve that the im-provement of pituitary function in this patient can be attrib-uted to successful steroid therapy. However, this is notdefinitive since some patients demonstrate spontaneous re-mission without therapy (13).In summary, we have reported a case of LHywith grossvisual disturbance whose neurological symptomsand MRIfindings improved remarkably 3 days after the start ofHDMPT,and whose pituitary function recovered 6 monthsafter the start of corticosteroid therapy. This case report
172 Internal Medicine Vol. 42, No. 2 (February 2003)
Lymphocytic Hypophysitis and Pulse
suggests that methylprednisolone pulse therapy was effectivefor mass reduction of severe LHyand could allow patients toavoid useless surgery.
Psychiatry 67: 398-402, 1999.4) O'Dwyer DT, Clifton V, Hall A, Smith R, Robinson PJ, Crock PA.
Pituitary autoantibodies in lymphocytic hypophysitis target bothgamma- and alpha-enolase -A link with pregnancy? Arch PhysiolBiochem 110: 94-98, 2002.
5) Saiwai S, Inoue Y, Ishihara T, et al. Lymphocytic adenohypophysitis:skull radiographs and MRI. Neuroradiology 40: 1 14-120, 1998.6) Honegger J, Fahlbusch R, BornemannA, et al. Lymphocytic and
granulomatous hypophysitis: experience with nine cases. Neurosurgery40: 713-722, 1997 (see discussion, 722-723).7) Takao T, Nanamiya W, Matsumoto R, Asaba K, Okabayashi T,
Hashimoto K. Antipituitary antibodies in patients with lymphocytichypophysitis. Horm Res 55: 288-292, 2001.8) Beressi N, Cohen R, Beressi JP, et al. Pseudotumoral lymphocytichypophysitis successfully treated by corticosteroid alone: first case re-port. Neurosurgery 35: 505-508, 1994 (see discussion, 508).
9) Shimon I, Berezin M, Hadani M, Tadmor R, Gross D, Karasik A. A pi-tuitary mass and hypopituitarism: improvement after corticosteroid
therapy. Isr J Med Sci 33: 58-62, 1997.10) Nishioka H, Ito H, Fukushima C. Recurrent lymphocytic hypophysitis:
case report. Neurosurgery 41: 684-686, 1997 (see discussion, 686-687).
ll) Reusch JE, Kleinschmidt-DeMasters BK, Lillehei KO, Rappe D,Gutierrez-Hartmann A. Preoperative diagnosis of lymphocytic hy-pophysitis (adenohypophysitis) unresponsive to short course dexa-
methasone: case report. Neurosurgery 30: 268-272, 1992.12) Nishioka H, Ito H, Miki T, Akada K. A case of lymphocytic
hypophysitis with massive fibrosis and the role of surgical intervention.Surg Neurol 42: 74-78, 1994.
13) Ozawa Y, Shishiba Y. Recovery from lymphocytic hypophysitis asso-ciated with painless thyroiditis: clinical implications of circulating