65
Treatments for Suicidal Adolescents: Lessons from a Comparative Efficacy Trial Roger Kobak University of Delaware

Treatments for Suicidal Adolescents: Lessons from a
Comparative Efficacy TrialRoger Kobak
University of Delaware

Aims
• The Boundaries Between Attachment and Evidence Based Treatments
• Comparative Efficacy Trial for Suicidal Adolescents• Attachment Based Therapy for Adolescents
• Non-Directive Supportive Therapy
• Who Benefits from Attachment Based Treatments
• Initial Lessons Learned

Targets for Attachment Treatments
• Interpersonal communication—Caregiver Sensitivity• Increase attunement to attachment signals
• Caregiver-child Dyads
• Adult Attachment Bonds
• Intrapersonal communication—States of Mind• Attachment narratives
• Vulnerability—Accessing attachment needs, feelings,
• Examining expectancies for caregiver availability
• Discourse as a Window on the Mind• Coherence as Cooperative Conversation
• Stepping back--Increase reflective function

ABT Modalities and Interventions
• Dyadic Modalities—Enacting a sensitive relationship• Therapist as Coach
• Reinforcing Sensitive Responding (Dozier)
• Engineering a reparative conversation (Johnson, Diamond)
• Individual Modalities—Supporting Epistemic Space• Therapist as Attachment Figure
• Enacting a secure base script (safe haven/secure base)
• Responding sensitively to distress/help seeking behavior
• Exploring the mind of self and others• Reflective Function (Video Replay)

Bowlby (1991)
• A well known observation, which in the world of psychotherapy has perhaps been taken too much for granted without its theoretical implications being given sufficient attention, is the constant interaction of, on the one hand, patterns of communication, verbal and non-verbal, that are operating within an individual’s mind and, on the other, the patterns of communication between him and those whom he feels he can trust. (p. 294)

The Secure Cycle

IWM—Confident ExpectanciesFor Caregiver Availability
IWM of Child
Sensitive Response
Read Signals Direct Signaling ofEmotions & Motivations
Access and Reflect on Model
Repair
Update
Empathize
CHILD
CAREGIVER
Access and Reflect on Model
Repair
Update
SENSITIVELY ATTUNED DYADIC COMMUNICATION

IWM—Confident ExpectanciesFor Caregiver Availability
IWM of Child
Sensitive Response
Read Signals Direct Signaling ofEmotions & Motivations
Access and Reflect on Model
Repair
Update
Empathize
CHILD
CAREGIVER
Access and Reflect on Model
Repair
Update

IWM—Confident ExpectanciesFor Caregiver Availability
IWM of Child
Sensitive Response
Read Signals Direct Signaling ofEmotions & Motivations
Access and Reflect on Model
Repair
Update
Empathize
CHILD
CAREGIVER
Access and Reflect on Model
Repair
Update

ABT’s adapt to developmental change
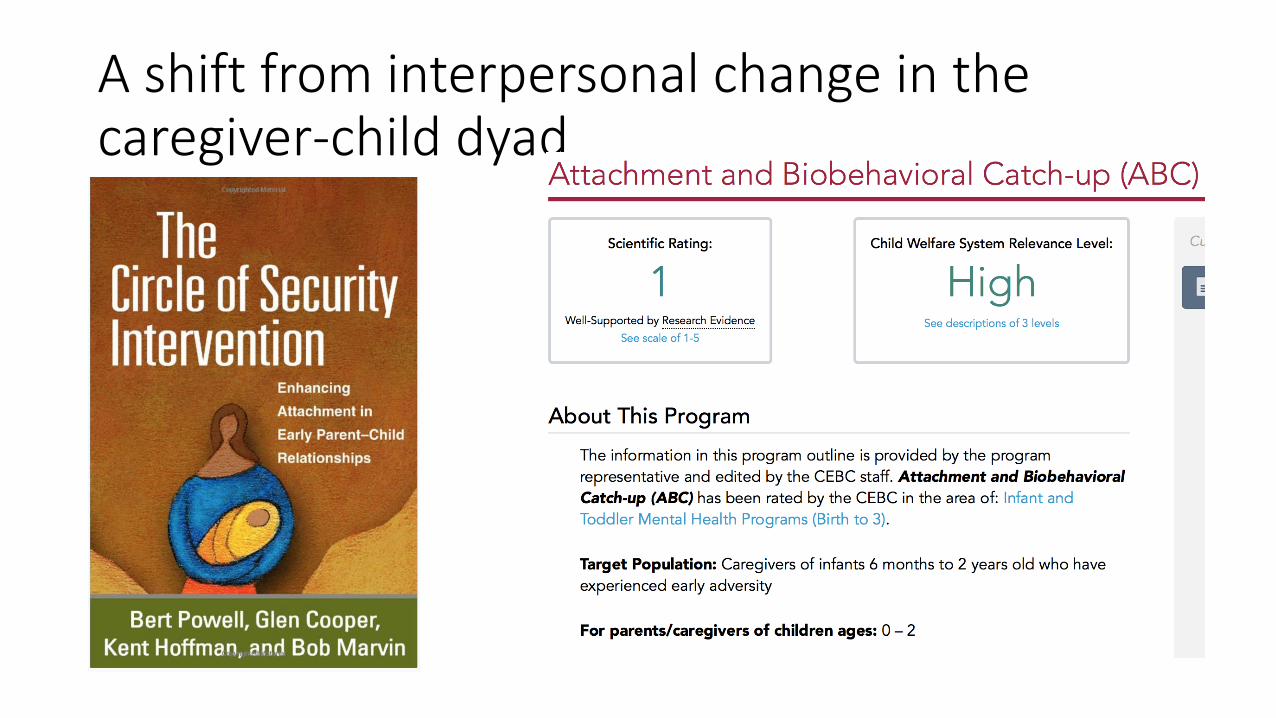
A shift from interpersonal change in the caregiver-child dyad
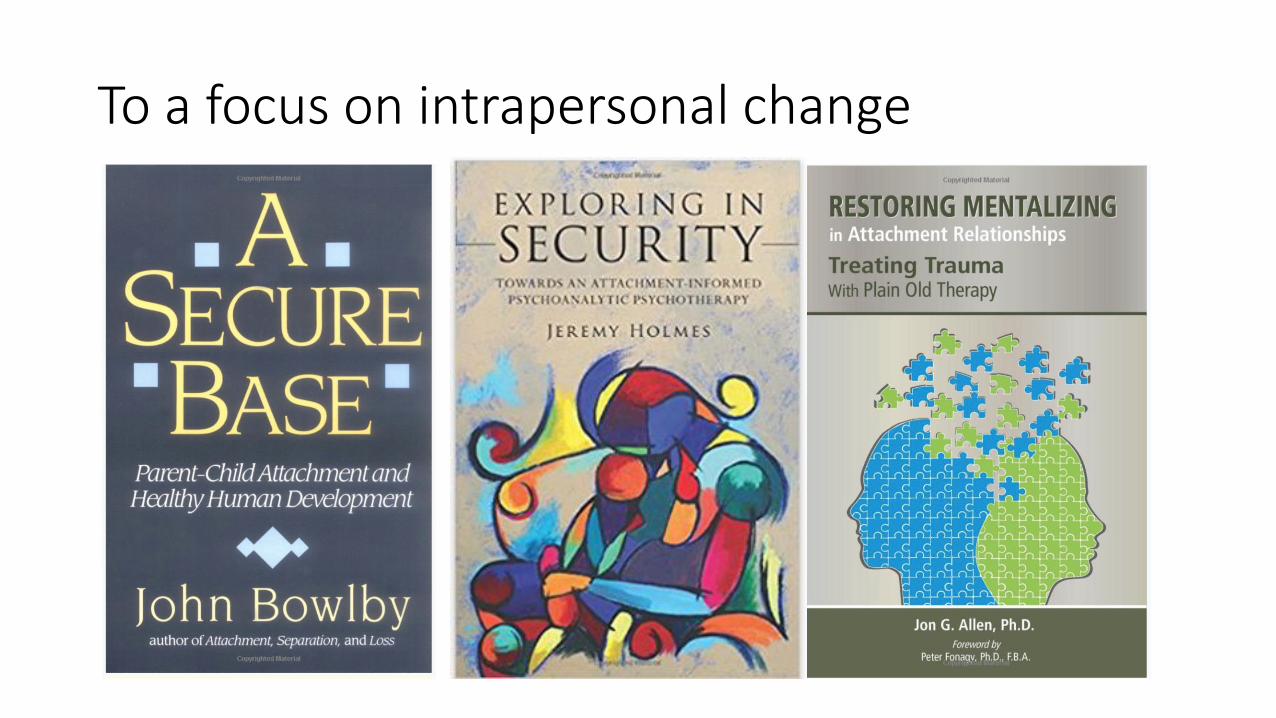
To a focus on intrapersonal change

Fuzzy Boundaries-What counts as an ABT?
• Attachment Based Treatments Aim• To improve sensitively attuned communication
• Caregiver-child or adult-adult attachment dyads
• Increase client’s capacity to access and value attachment needs
• Provide new learning to revise negative expectancies
• Attachment Informed Treatments• Incorporate client or therapist states of mind in case conceptualization
• Provide new learning in the therapeutic relationship
• Mentalization—understanding action in terms of thoughts and feelings• Mindfulness--Emotion Regulation

Adolescence—A Developmental Transition
• Adolescent ABT’s:• May continue to focus on the caregiver-child dyad
• Therapist as coach to improve cooperative communication• Parent Psychoeducation
• OR• May also focus on the adolescent’s intrapersonal functioning
• Therapist as attachment figure• May manage distress more effectively• Increase capacity to use caregivers as safe haven/secure base
• OR• May combine interpersonal and intrapersonal modalities

Attachment Meets Evidence Based Treatments

Challenges to Evaluating ABT’s as Evidence Based Treatments• Evidence Based Treatments
• DSM--Disorder Specific
• Standardized Assessment of Symptom Reduction
• RCT design Treatment as Usual or Another Active Treatment
• Standardized Treatment Manuals
• Attachment Treatments• Assume relationship disturbance implicated in psychopathology
• Focus on Enhancing Security in Close Relationships
• Trans diagnostic
• Based on developmental risk literature

Promising EBT’s for Suicidal and Depressed Adolescents• Attachment RCT’s
• Attachment Based Family Therapy (Diamond et al., 2010)• Suicidal and Depressed Adolescents 16 weeks
• Mentalization-Based Treatment for Adolescents (Rossouw & Fonagy, 2012)• Self-Harm 12 months
• Other promising Treatments for Adolescent Depression• Medication and Skills Based Treatments (SSRI’s, CBT, IPT, DBT?)
• Non-Directive Supportive Therapy was as effective as CBT and Family Therapy in Reducing Suicidality and Functional Impairment (Brent et al., 1997)
• Most RCT’s used Treatment as Usual as Control
ABFT vs NST Comparative Efficacy Trial
(2011-2017)
National Institute of Mental Health (NIMH) under Grant R01MH091059
Diamond & Kobak (Co-Principal Investigators)
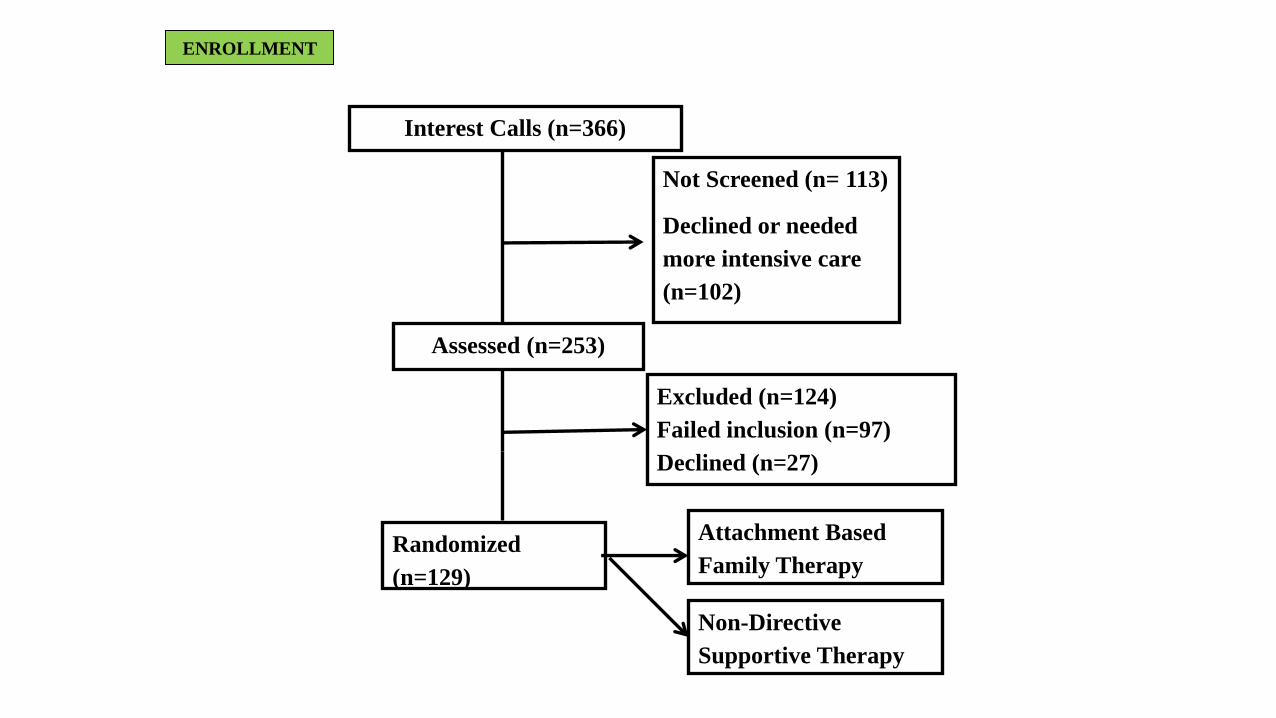
Interest Calls (n=366)
Not Screened (n= 113)
Declined or needed
more intensive care
(n=102)
Assessed (n=253)
Excluded (n=124)
Failed inclusion (n=97)
Declined (n=27)
Randomized
(n=129)
Attachment Based
Family Therapy
ENROLLMENT
Non-Directive
Supportive Therapy

Referral Sources (253 Assessed)
• Emergency Rooms 118
• Inpatient Psychiatric Hospital 36
• Primary Care 31
• Schools 30
• Outpatient Therapist 29

Inclusion
• SIQ > 31 (clinical cut off range)
• BDI > 21 (moderate depression)
• Parent willing to participate
• Suicidal issues manageable on outpatient

Baseline
Week 4
Week 8
Week 12
Week 16
Week 24
Week 32
Week 40
Week 52
Timeline
In Therapy Post-Treatment

Random Assignment to Two Active Treatments (N = 129)
• A Promising Attachment Treatment (16 weeks)• Attachment Based Family Therapy (Diamond et al., 2010)
• Versus
• Another promising Treatment (16 weeks)• Non-Directive Supportive Therapy (Brent et al. 1997)
• with Parent Enhanced Psychoeducation

ABFT—Five Treatment Tasks
1) Relational Reframe
2) Alliance with the Adolescent
3) Alliance with the Parent
4) Attachment Task
5) Promoting Competency Task
Non-Directive Supportive Therapy (PE)
• Family Safety Planning
• Client Centered Individual Therapy• Reflective listening
• Empathic responding
• Encouragement
• Exploration of client experience and feelings
• Four parent psycho-educational sessions
• A mentalization treatment?
• An ”attachment-informed” treatment?

Heterogeneity Among those Treated

Adolescent Population
White N = 37 28.7%
Black/African American N = 63 48.8%
Other N = 29 22.5%
Hispanic N = 20 15.5%
Male N = 21 16.3%
Female N = 108 83.7%
Two-Parent Household N = 45 34.9%
DEMOGRAPHICS
Family Yearly Household Income
$0 - $9,999 N = 15; 11.6%
$10,000 - $19,999 N = 15; 11.6%
$20,000 - $29,999 N = 11; 8.5%
$30,000 - $39,999 N = 21; 16.3%
$40,000 - $49,000 N = 12; 9.3%
$50,000 - $59,999 N = 10; 7.8%
$60,000 - $69,999 N = 5; 3.9%
$70,000 - $79,999 N = 5; 3.9%
$80,000 - $89,999 N = 9; 7.0%
$90,000 - $99,999 N = 11; 8.5%
$100,000 or Higher N = 14; 10.9%

Symptom Severity—Suicide Ideation
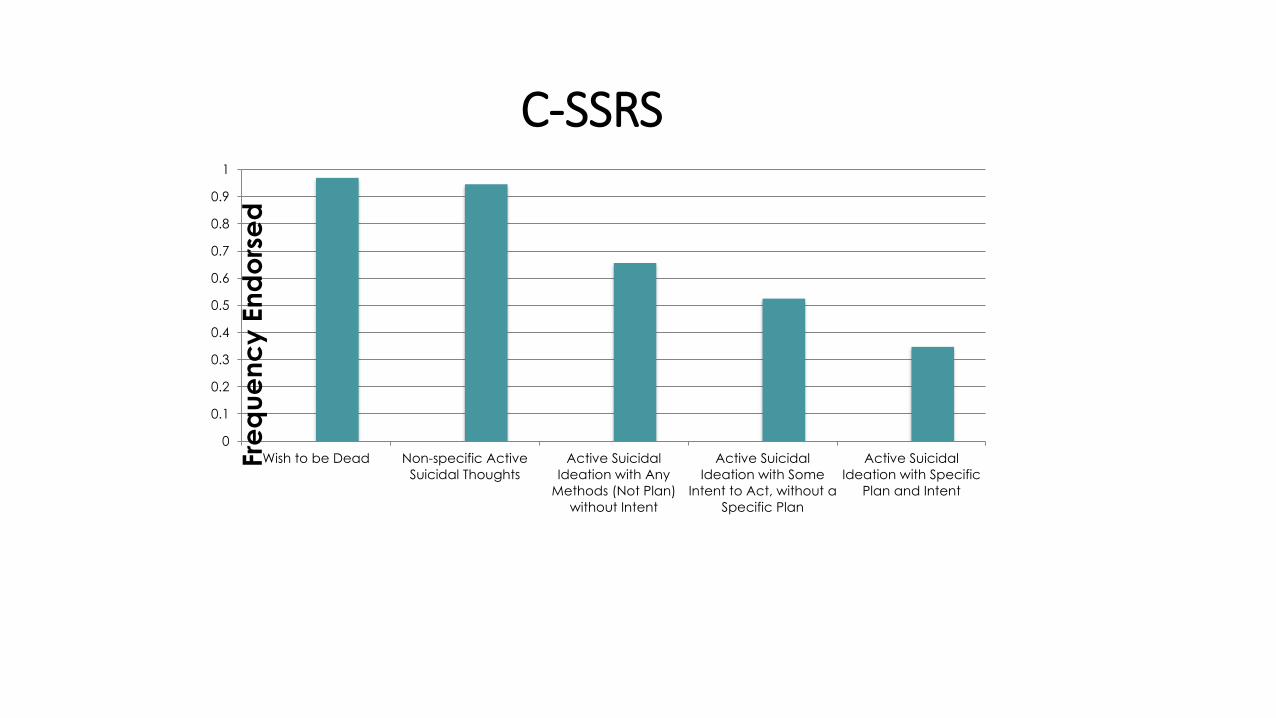
C-SSRS
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Wish to be Dead Non-specific Active
Suicidal Thoughts
Active Suicidal
Ideation with Any
Methods (Not Plan)
without Intent
Active Suicidal
Ideation with Some
Intent to Act, without a
Specific Plan
Active Suicidal
Ideation with Specific
Plan and Intent
Fre
qu
en
cy
En
do
rse
d

Adolescent BDISymptom Severity--Depression

• 51 (39.5%) patients had a history of
attempted suicide
• Of those, 26 made more than one
attempt
• 56.6% (N = 73) engaged in NSSI
ATTEMPTORS and
SELF-HARM

C-DISC Diagnoses (115 completed)
Depressive Disorders
Positive
Major Depressive Episode(Past Year)
46 (40.0%)
Major Depressive Episode(Past Month)
31 (27.2%)
Anxiety Disorders (Past Year)
Positive
Social Phobia 28 (24.3%)
Separation Anxiety Disorder 15 (13%)
Panic Disorder 12 (10.4%)
Agoraphobia 30 (26.1%)
Generalized Anxiety Disorder 10 (8.7%)
Post-Traumatic Stress Disorder
9 (7.8%)

Top Three Reasons Reported for Suicide
•Pressure to achieve
•My parents don’t understand me
•Poor grades

Retention Data
• 106 full completion
• 118 got 10 or more sessions.
• 2 withdrawn • psychosis
• Medical hospitalization
• Number of sessions attended• about 13 in both treatments
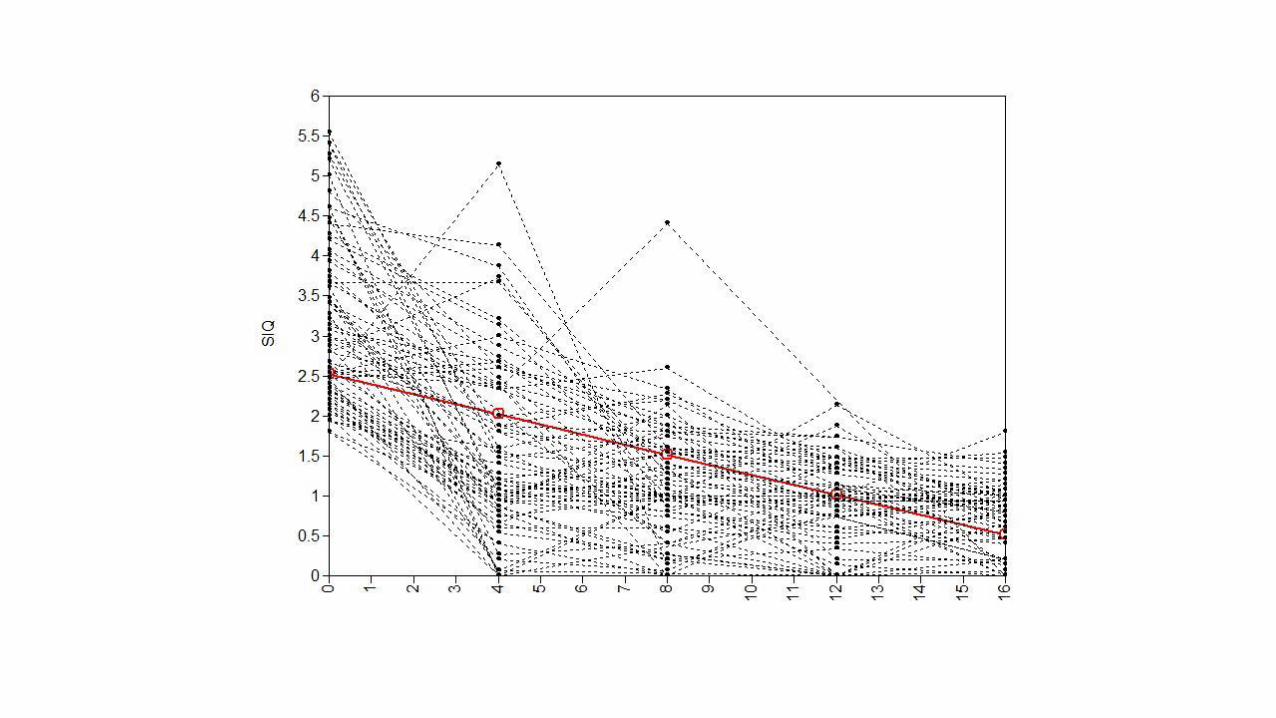
Comparing ABFT and NST Treatment Effects(Primary Outcomes)
• Suicide Ideation Questionnaire (SIQ)
• Beck Depression Inventory BDI
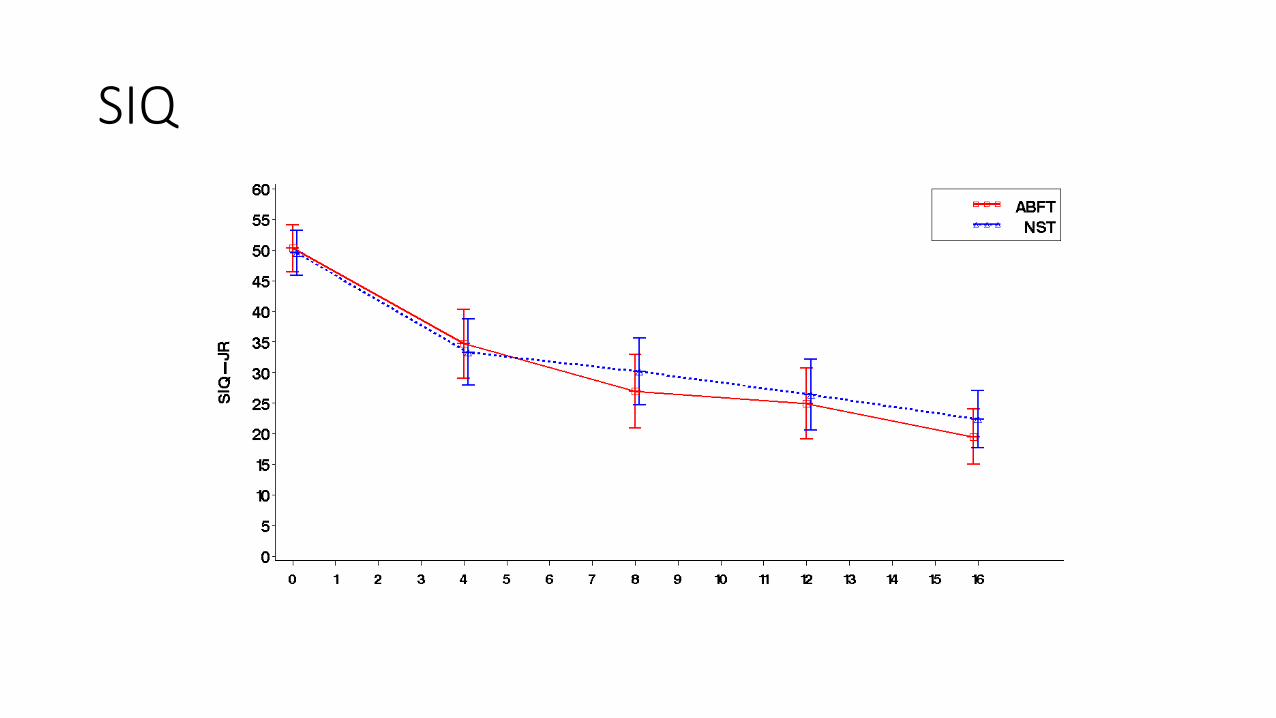
SIQ
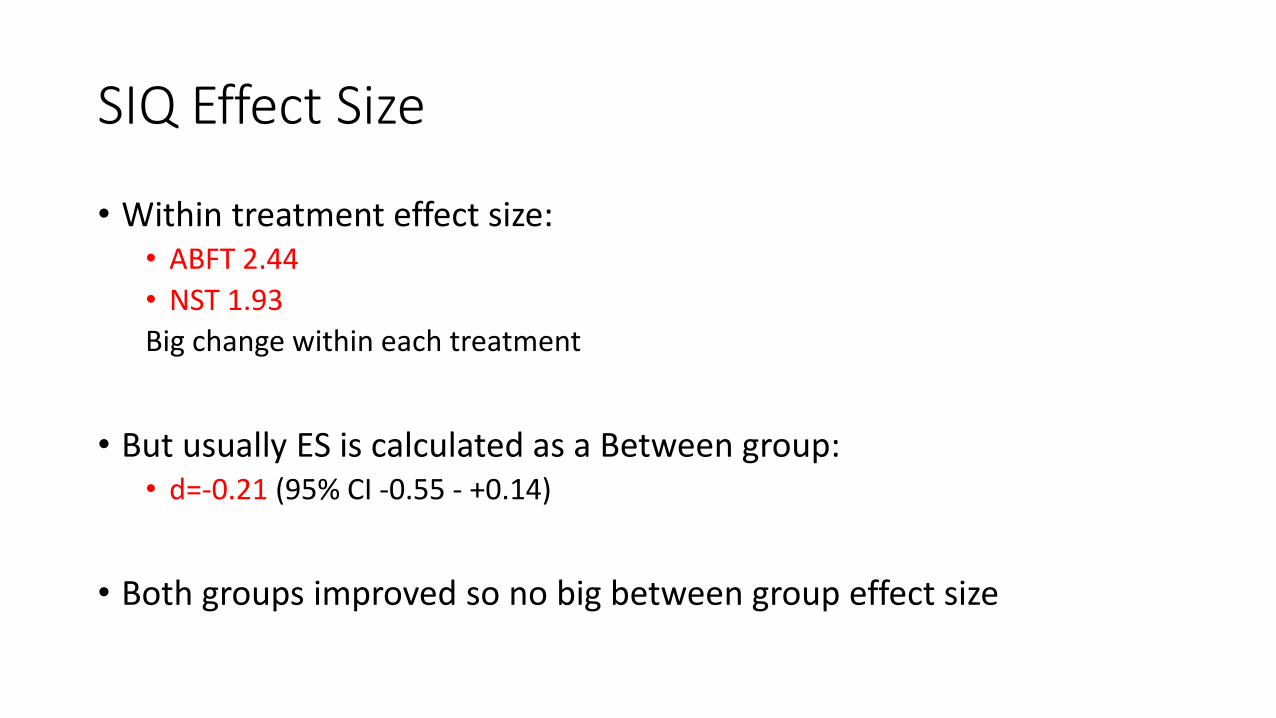
SIQ Effect Size
• Within treatment effect size: • ABFT 2.44
• NST 1.93
Big change within each treatment
• But usually ES is calculated as a Between group: • d=-0.21 (95% CI -0.55 - +0.14)
• Both groups improved so no big between group effect size

SIQ Response Rate (< 12)
12.1 11.5
26.524.5
14.3
25 24.5
32.7
0
5
10
15
20
25
30
35
Wk 4 Wk 8 Wk 12 Wk 16
NST
ABFT
p =0.72 p=0.08 p=0.82 p=0.35

BDI
ABFT= 15.4NST = 15.6
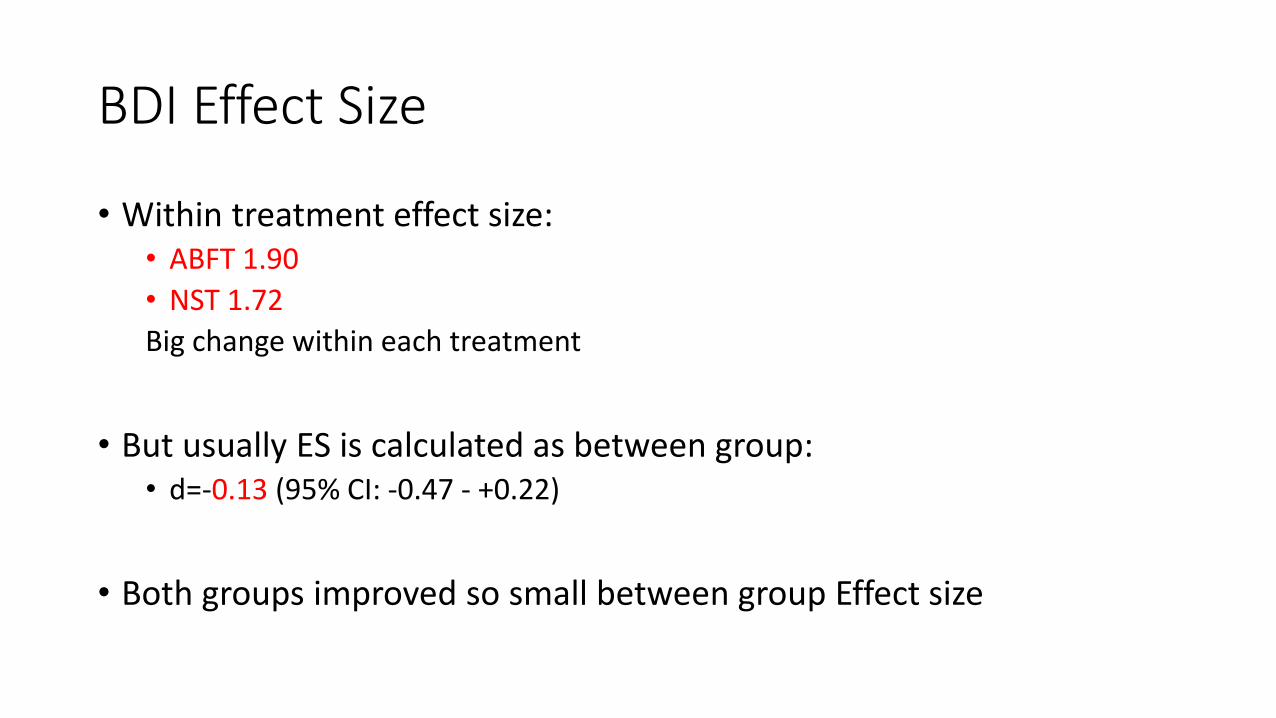
BDI Effect Size
• Within treatment effect size: • ABFT 1.90
• NST 1.72
Big change within each treatment
• But usually ES is calculated as between group: • d=-0.13 (95% CI: -0.47 - +0.22)
• Both groups improved so small between group Effect size

BDI Response Rate (< 9)
15.5
11.8
18.4
34
7.1
19.2
35.9
40
0
5
10
15
20
25
30
35
40
45
Wk 4 Wk 8 Wk 12 Wk 16
NST
ABFT
p =0.16 p=0.29 p=0.048 p=0.52
Who Benefits?
Moderators of Primary Outcomes

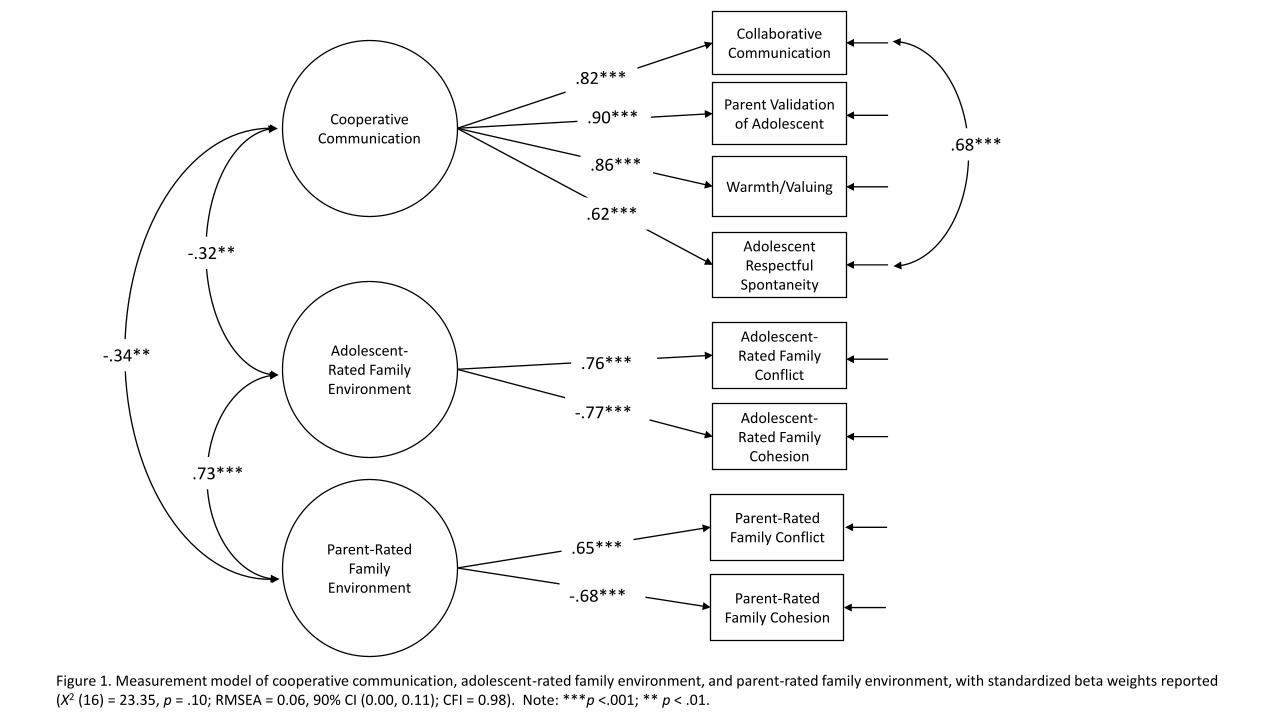
Relationship Disturbance and Treatment Response
Adolescent-Rated Family Environment
Parent-Rated Family
Environment
Collaborative Communication
Parent Validation of Adolescent
Warmth/Valuing
Adolescent Respectful
Spontaneity
Adolescent-Rated Family
Conflict
Adolescent-Rated Family
Cohesion
Parent-Rated Family Conflict
Parent-Rated Family Cohesion
Cooperative Communication
.82***
.90***
.86***
.62***
.76***
-.77***
.65***
-.68***
.68***
-.32**
.73***
-.34**
Figure 1. Measurement model of cooperative communication, adolescent-rated family environment, and parent-rated family environment, with standardized beta weights reported (Χ2 (16) = 23.35, p = .10; RMSEA = 0.06, 90% CI (0.00, 0.11); CFI = 0.98). Note: ***p <.001; ** p < .01.

15
20
25
30
35
40
Week 1 Week 16
BD
I Sco
re
High CooperativeCommunication atBaseline
Low CooperativeCommunication atBaseline
Figure 2. Rates of change in depressive symptoms over the course of 16 weeks of treatment.
Treatment Non-Responders—Major Depression and Optimism as Predictors




Life Orientation Test
0
0.5
1
1.5
2
2.5
3
Responders Non Responders
SIQ
BDI
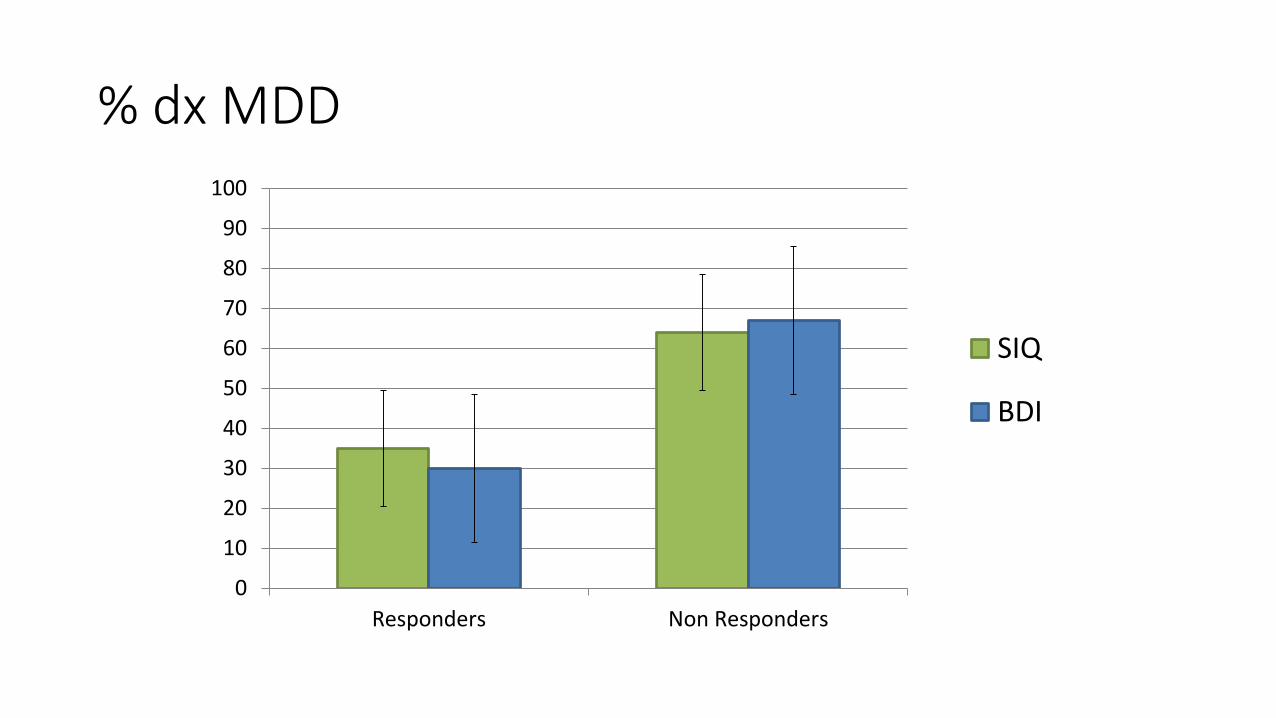
% dx MDD
0
10
20
30
40
50
60
70
80
90
100
Responders Non Responders
SIQ
BDI
Comparing ABFT and NST Treatment Effects(Secondary Outcomes)
• Adult Attachment Interview
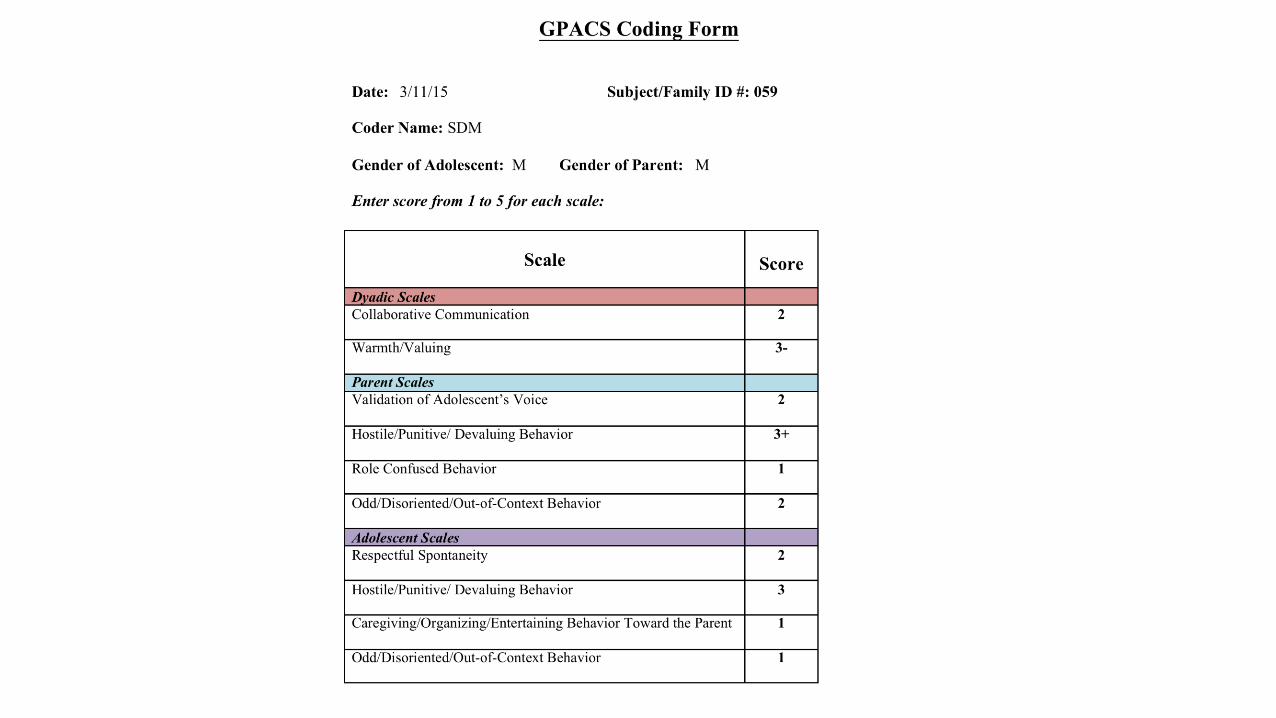
• Goal-Corrected Partnership Attachment Coding System (GPACS)
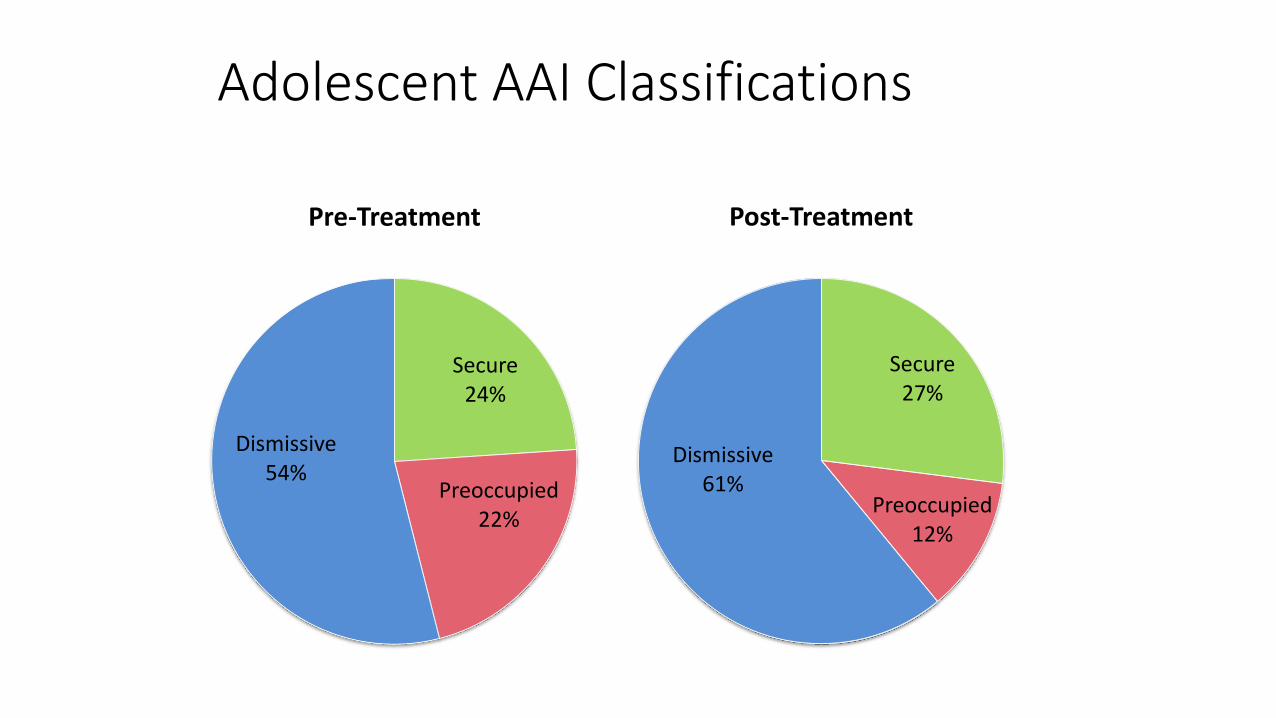
Adolescent AAI Classifications
Secure24%
Preoccupied22%
Dismissive54%
Pre-Treatment
Secure27%
Preoccupied12%
Dismissive61%
Post-Treatment

Assessing Parent-Teen Communication
• Goal-Corrected Partnership Attachment Coding System (Lyons-Ruth)• Cooperative Problem Solving
• Hostility
• Role Confusion
• Disorganization
Questions
• Is there change in Secondary Outcomes?• Change in Adolescent AAI (States of Mind, Expectancies)—Reduction in Preoccupation
• Reductions in Self-Report Avoidance with Mothers and Fathers
• Improvement in communication-Improvement in Cooperative Communication
• Are there Treatment Differences in Secondary Outcomes?• No
• Are there Moderators of Treatment Efficacy for Secondary Outcomes• Factors that specifically link Relationship Disturbance to Suicidality
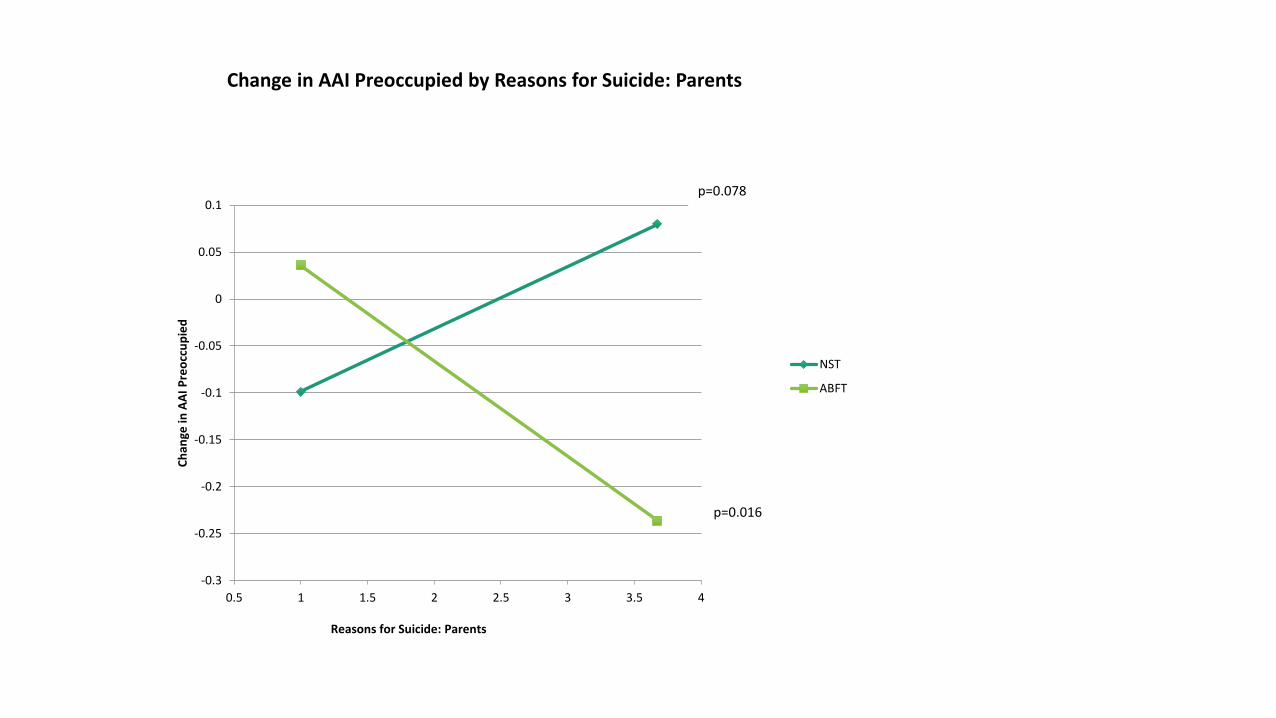
• Reasons for Suicide Scale
Reasons for Suicide
• ”Please rate how much the following common reasons for suicide contribute to your thoughts about suicide” (scale 1-6)
• Parents• Overly controlling or critical parents• My parents don’t care about me• My parents don’t understand me
• School Problems• Peer Problems• Abuse• Loss• LGBT issues
-0.3
-0.25
-0.2
-0.15
-0.1
-0.05
0
0.05
0.1
0.5 1 1.5 2 2.5 3 3.5 4
Ch
ange
in A
AI
Pre
occ
up
ied
Reasons for Suicide: Parents
Change in AAI Preoccupied by Reasons for Suicide: Parents
NST
ABFT
p=0.078
p=0.016

Summary
• Suicidal or depressed symptoms = attachment problems for all adolescents
• Adolescents in less cooperative dyads responded better to both treatments
• More depressed (MDD) and less optimistic (-LOT) individuals are less likely to benefit from ABFT and NST• Should assess and address treatment expectancies
• Should consider CBT for depression
• Individual therapy vs. family therapy• Remarkably few treatment differences in symptom reduction
• ABFT if parents are perceived as reason for suicide

Lessons Learned
• Non-Directive Supportive Therapy “Works” (Plain Old Therapy and Mentalization)
• Comparative efficacy designs generally struggle to show treatment superiority
• Some suicidal adolescents benefit from ABFT and NST treatments but some benefit more than others and some do not benefit at all
• After establishing that an ABFT “works” begin to ask whether an ABT is best (compared to other active treatments) for a particular adolescent

Future Directions for ABT’s
Use Assessments To Guide Treatment Recommendations and Planning
Assess for Co-Morbid PsychopathologyNSSI and AttemptersPessimism-Optimism
Symptom Severity as a prognostic indicator of Probability of Treatment Benefit
Assessments of Relationship Disturbance as a Gateway to ABT’s

Defining and Assessing Relationship DisturbanceAssessments of Relationship Disturbance are needed to
1) Establish norms for clinical intervention2) Guide recommendations for ABT3) Evaluate the efficacy of ABT’s 4) Test attachment as mechanism for symptom reduction
Assessments of Interpersonal Communication should IncludeDimensional measures that are sensitive to changeUse of brief observationsIntensive longitudinal designs using self-report
Assessments of Intrapersonal Communication should includeExpectancies for Caregiver Availability and Responsiveness (Secure Base Script)Access to and Integration of Attachment Narratives (Emotion Regulation)Reflective capacity and meaning making

Thank you!
University of Delaware• Caroline Abbott• Abby Zisk• Nadia Bounoua
The College of New Jersey
• Joanna Herres
Drexel University
–Guy Diamond
– Stephanie Krauthamer-Ewing
– Suzanne Levy

















