1
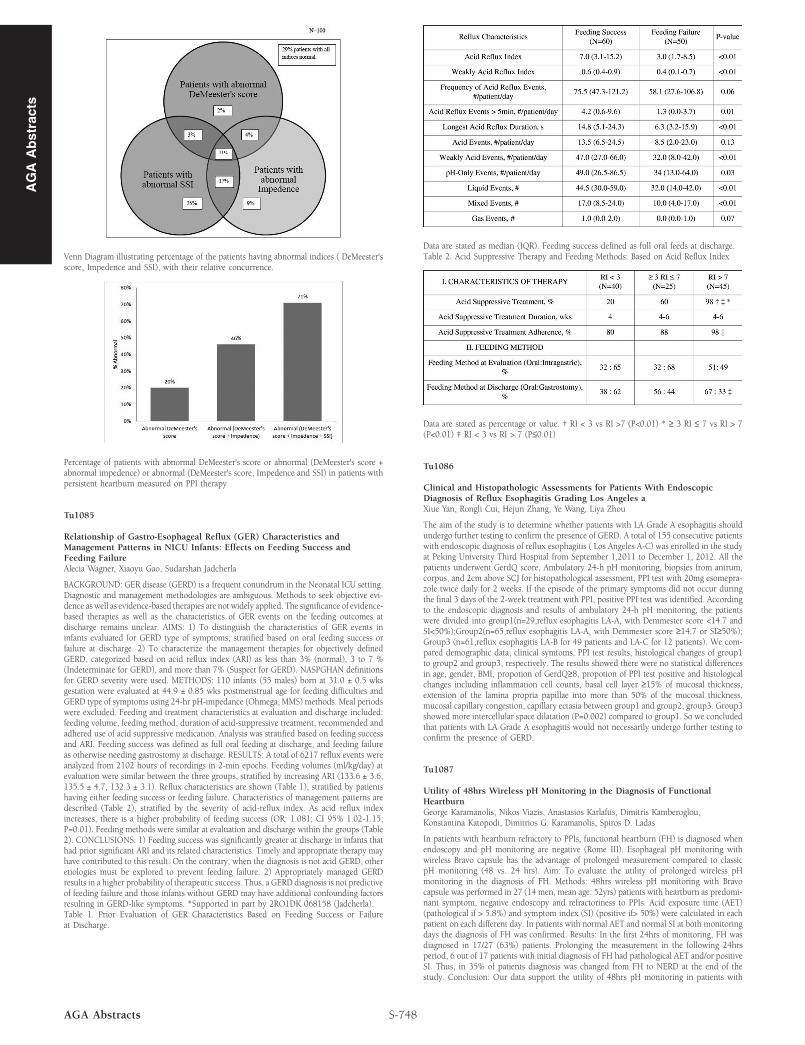
AGA Abstracts Venn Diagram illustrating percentage of the patients having abnormal indices ( DeMeester's score, Impedence and SSI), with their relative concurrence. Percentage of patients with abnormal DeMeester's score or abnormal (DeMeester's score + abnormal impedence) or abnormal (DeMeester's score, Impedence and SSI) in patients with persistent heartburn measured on PPI therapy Tu1085 Relationship of Gastro-Esophageal Reflux (GER) Characteristics and Management Patterns in NICU Infants: Effects on Feeding Success and Feeding Failure Alecia Wagner, Xiaoyu Gao, Sudarshan Jadcherla BACKGROUND: GER disease (GERD) is a frequent conundrum in the Neonatal ICU setting. Diagnostic and management methodologies are ambiguous. Methods to seek objective evi- dence as well as evidence-based therapies are not widely applied. The significance of evidence- based therapies as well as the characteristics of GER events on the feeding outcomes at discharge remains unclear. AIMS: 1) To distinguish the characteristics of GER events in infants evaluated for GERD type of symptoms, stratified based on oral feeding success or failure at discharge. 2) To characterize the management therapies for objectively defined GERD, categorized based on acid reflux index (ARI) as less than 3% (normal), 3 to 7 % (Indeterminate for GERD), and more than 7% (Suspect for GERD). NASPGHAN definitions for GERD severity were used. METHODS: 110 infants (55 males) born at 31.0 ± 0.5 wks gestation were evaluated at 44.9 ± 0.85 wks postmenstrual age for feeding difficulties and GERD type of symptoms using 24-hr pH-impedance (Ohmega, MMS) methods. Meal periods were excluded. Feeding and treatment characteristics at evaluation and discharge included: feeding volume, feeding method, duration of acid-suppressive treatment, recommended and adhered use of acid suppressive medication. Analysis was stratified based on feeding success and ARI. Feeding success was defined as full oral feeding at discharge, and feeding failure as otherwise needing gastrostomy at discharge. RESULTS: A total of 6217 reflux events were analyzed from 2102 hours of recordings in 2-min epochs. Feeding volumes (ml/kg/day) at evaluation were similar between the three groups, stratified by increasing ARI (133.6 ± 3.6, 135.5 ± 4.7, 132.3 ± 3.1). Reflux characteristics are shown (Table 1), stratified by patients having either feeding success or feeding failure. Characteristics of management patterns are described (Table 2), stratified by the severity of acid-reflux index. As acid reflux index increases, there is a higher probability of feeding success (OR: 1.081; CI 95% 1.02-1.15; P=0.01). Feeding methods were similar at evaluation and discharge within the groups (Table 2). CONCLUSIONS: 1) Feeding success was significantly greater at discharge in infants that had prior significant ARI and its related characteristics. Timely and appropriate therapy may have contributed to this result. On the contrary, when the diagnosis is not acid GERD, other etiologies must be explored to prevent feeding failure. 2) Appropriately managed GERD results in a higher probability of therapeutic success. Thus, a GERD diagnosis is not predictive of feeding failure and those infants without GERD may have additional confounding factors resulting in GERD-like symptoms. *Supported in part by 2RO1DK 068158 (Jadcherla). Table 1. Prior Evaluation of GER Characteristics Based on Feeding Success or Failure at Discharge. S-748 AGA Abstracts Data are stated as median (IQR). Feeding success defined as full oral feeds at discharge. Table 2. Acid Suppressive Therapy and Feeding Methods: Based on Acid Reflux Index Data are stated as percentage or value. † RI < 3 vs RI >7 (P<0.01) * ≥ 3 RI ≤ 7 vs RI > 7 (P<0.01) ‡ RI < 3 vs RI > 7 (P≤0.01) Tu1086 Clinical and Histopathologic Assessments for Patients With Endoscopic Diagnosis of Reflux Esophagitis Grading Los Angeles a Xiue Yan, Rongli Cui, Hejun Zhang, Ye Wang, Liya Zhou The aim of the study is to determine whether patients with LA Grade A esophagitis should undergo further testing to confirm the presence of GERD. A total of 155 consecutive patients with endoscopic diagnosis of reflux esophagitis ( Los Angeles A-C) was enrolled in the study at Peking University Third Hospital from September 1,2011 to December 1, 2012. All the patients underwent GerdQ score, Ambulatory 24-h pH monitoring, biopsies from antrum, corpus, and 2cm above SCJ for histopathological assessment, PPI test with 20mg esomepra- zole twice daily for 2 weeks. If the episode of the primary symptoms did not occur during the final 3 days of the 2-week treatment with PPI, positive PPI test was identified. According to the endoscopic diagnosis and results of ambulatory 24-h pH monitoring, the patients were divided into group1(n=29,reflux esophagitis LA-A, with Demmester score <14.7 and SI<50%);Group2(n=65,reflux esophagitis LA-A, with Demmester score ≥14.7 or SI≥50%); Group3 (n=61,reflux esophagitis LA-B for 49 patients and LA-C for 12 patients). We com- pared demographic data, clinical symtoms, PPI test results, histological changes of group1 to group2 and group3, respectively. The results showed there were no statistical differences in age, gender, BMI, propotion of GerdQ≥8, propotion of PPI test positive and histological changes including inflammation cell counts, basal cell layer ≥15% of mucosal thickness, extension of the lamina propria papillae into more than 50% of the mucosal thickness, mucosal capillary congestion, capillary ectasia between group1 and group2, group3. Group3 showed more intercellular space dilatation (P=0.002) compared to group1. So we concluded that patients with LA Grade A esophagitis would not necessarily undergo further testing to confirm the presence of GERD. Tu1087 Utility of 48hrs Wireless pH Monitoring in the Diagnosis of Functional Heartburn George Karamanolis, Nikos Viazis, Anastasios Karlaftis, Dimitris Kamberoglou, Konstantina Katopodi, Dimitrios G. Karamanolis, Spiros D. Ladas In patients with heartburn refractory to PPIs, functional heartburn (FH) is diagnosed when endoscopy and pH monitoring are negative (Rome III). Esophageal pH monitoring with wireless Bravo capsule has the advantage of prolonged measurement compared to classic pH monitoring (48 vs. 24 hrs). Aim: To evaluate the utility of prolonged wireless pH monitoring in the diagnosis of FH. Methods: 48hrs wireless pH monitoring with Bravo capsule was performed in 27 (14 men, mean age: 52yrs) patients with heartburn as predomi- nant symptom, negative endoscopy and refractoriness to PPIs. Acid exposure time (AET) (pathological if > 5.8%) and symptom index (SI) (positive if> 50%) were calculated in each patient on each different day. In patients with normal AET and normal SI at both monitoring days the diagnosis of FH was confirmed. Results: In the first 24hrs of monitoring, FH was diagnosed in 17/27 (63%) patients. Prolonging the measurement in the following 24hrs period, 6 out of 17 patients with initial diagnosis of FH had pathological AET and/or positive SI. Thus, in 35% of patients diagnosis was changed from FH to NERD at the end of the study. Conclusion: Our data support the utility of 48hrs pH monitoring in patients with