84
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | mithila-das-mazumder |
| View: | 116 times |
| Download: | 1 times |
ObjectivesObjectives• Introduction• Estimated burden of tuberculosis in India• Defination• Epidemiology• Pathophysiology• Immunology • Clinical Presentations• Complication and sequelae .
INTRODUCTIONINTRODUCTION
Tuberculosis is a chronic infectious disease caused by Tuberculosis is a chronic infectious disease caused by Mycobacterium tuberculosisMycobacterium tuberculosis characterized by vague characterized by vague constitutional symptoms and a protracted course of constitutional symptoms and a protracted course of illness with remissions and exacerbations.illness with remissions and exacerbations.
Tuberculosis is the reaction of tissues of the human Tuberculosis is the reaction of tissues of the human host to the presence and multiplication of host to the presence and multiplication of Mycobacterium Mycobacterium tuberculosistuberculosis..
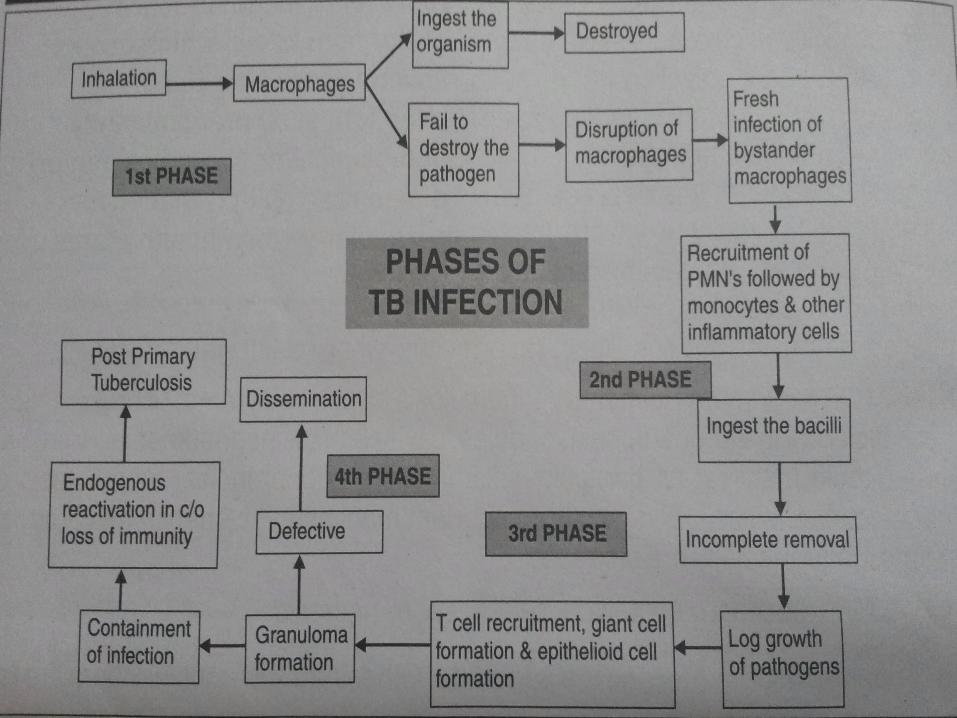
The clinical states arising from TB infection are the The clinical states arising from TB infection are the outcome between the capacity of the host to contain outcome between the capacity of the host to contain and eliminate the organism versus the capacity of the and eliminate the organism versus the capacity of the organism to multiply and proliferate. organism to multiply and proliferate.
Tuberculosis is a chronic granulomatous Tuberculosis is a chronic granulomatous inflammatory reaction of the tissues to the presence inflammatory reaction of the tissues to the presence of causative agent Mycobacterium tuberculosis,being of causative agent Mycobacterium tuberculosis,being characterized by a local aggregation of large number characterized by a local aggregation of large number of macrophages,some of which undergo striking of macrophages,some of which undergo striking structural & functional alterations in the form of their structural & functional alterations in the form of their transformation to epithelioid cells,foreign body giant transformation to epithelioid cells,foreign body giant cells & Langhancells & Langhan’s giant cells i.e. formation of ’s giant cells i.e. formation of TUBERCLE.TUBERCLE.
MAGNITUDEMAGNITUDE
1/31/3rdrd of the world of the world’s population is or has been ’s population is or has been infected with tubercle bacilli.infected with tubercle bacilli.
India accounts for one third of the word TB India accounts for one third of the word TB burdenburden
Prevalence of the disease in IndiaPrevalence of the disease in India:: 15-25 per 1000 population 15-25 per 1000 population 15 million infected, 25% sputum positive15 million infected, 25% sputum positive 3 to 4 million infected are children3 to 4 million infected are children
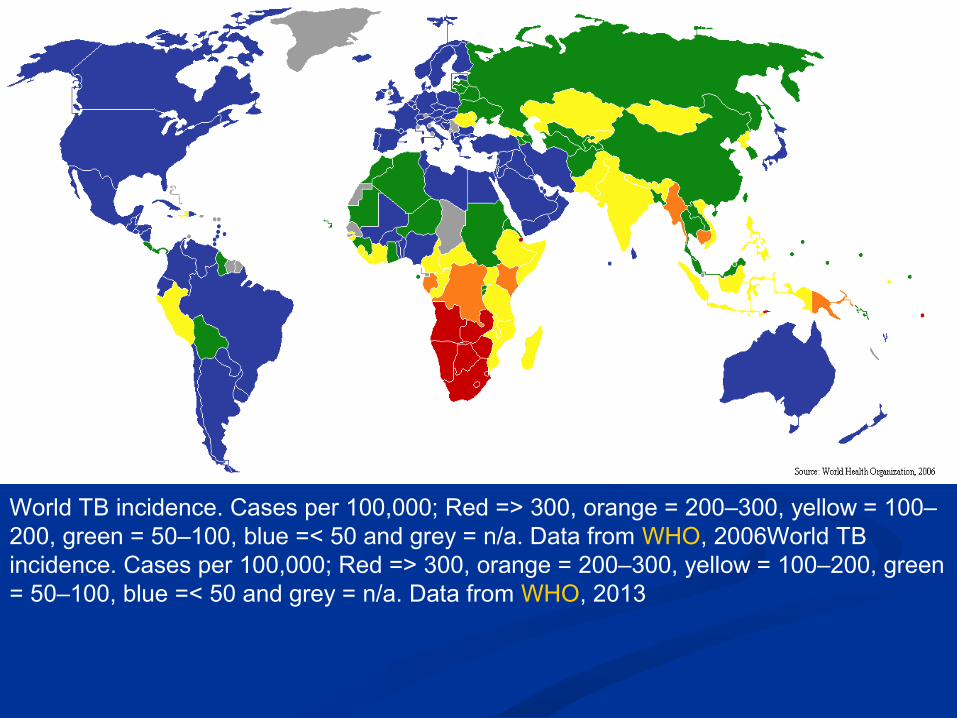
World TB incidence. Cases per 100,000; Red => 300, orange = 200–300, yellow = 100–200, green = 50–100, blue =< 50 and grey = n/a. Data from WHO, 2006World TB incidence. Cases per 100,000; Red => 300, orange = 200–300, yellow = 100–200, green = 50–100, blue =< 50 and grey = n/a. Data from WHO, 2013

EPIDEMIOLOGYEPIDEMIOLOGY
Agent : Mycobacterium tuberculosis, M. bovisAgent : Mycobacterium tuberculosis, M. bovis Reservoir : Infected patientReservoir : Infected patient Mode of infection : Droplet infection, dust, ingestion, Mode of infection : Droplet infection, dust, ingestion,
skin, mucous membrane, skinskin, mucous membrane, skin Host FactorsHost Factors
Age : all ages affected, congenital is rareAge : all ages affected, congenital is rare Sex : Girls > boys at PubertySex : Girls > boys at Puberty Malnutrition : more succeptibleMalnutrition : more succeptible Intercurrent infections : eg measles, whooping coughIntercurrent infections : eg measles, whooping cough
Environment : overcrowding, inadequate ventillation, Environment : overcrowding, inadequate ventillation, damp, insanitary and unhygenic conditionsdamp, insanitary and unhygenic conditions

ETIOLOGY
CLASSIFICATION OF MYCOBACTERIA
Typical Mycobacteria•M tuberculosis•M bovis•M bovis BCG•M africanumAtypical Mycobacteria•Photochromogens: M. Kansasii, M. marinum , M simiae•Scotochromogens: M scrofulaceum, M gordonae•Non Photochromogens : M avium , M paratuberculosis, Rapid Growers: M Fortuitum, M chelonaeNon-Cultivable Mycobacteria•M lepraeSaprophytic Mycobacteria•M butyricum•M pheli•M smegmatis

MORPHOLOGY OF MYCOBACTERIUM TUBERCULOSIS
• Straight or slightly curved rod.• 3 µm X 0.3 µm.• Occurring slightly in pairs or small clumps.• The size depends on condition of growth and long
filamentous club shaped and branching forms may sometimes be seen.
• Tubercle bacilli are weakly gram positive• Are ‘ACID – FAST’ & ‘ALCOHOL FAST’• Acid fastness has been ascribed to the presence of
mycolic acid in the bacillus, which resist decolourization by 20% sulphuric acid & absolute alcohol for 10 minutes.
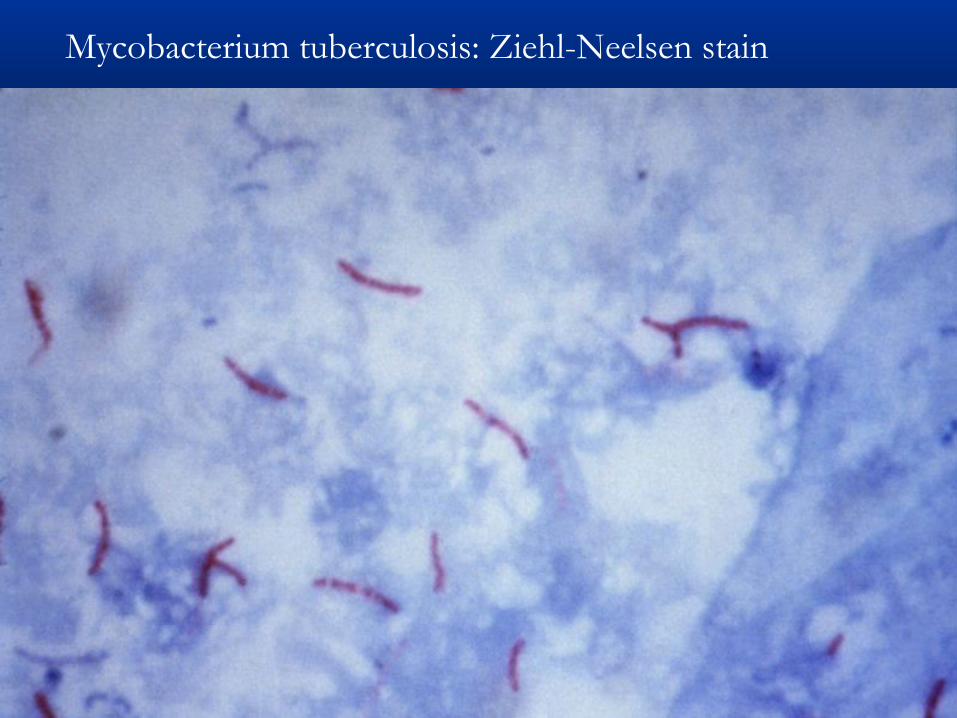
Mycobacterium tuberculosis: Ziehl-Neelsen stain
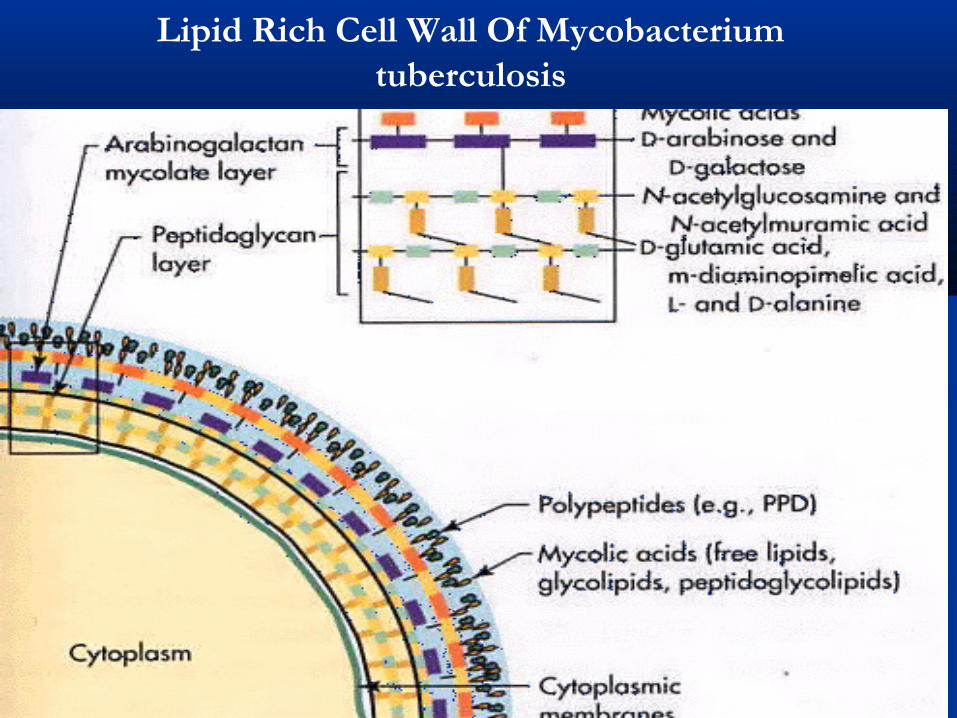
Lipid Rich Cell Wall Of Mycobacterium tuberculosis
Pathogenesis of Pediatric TB
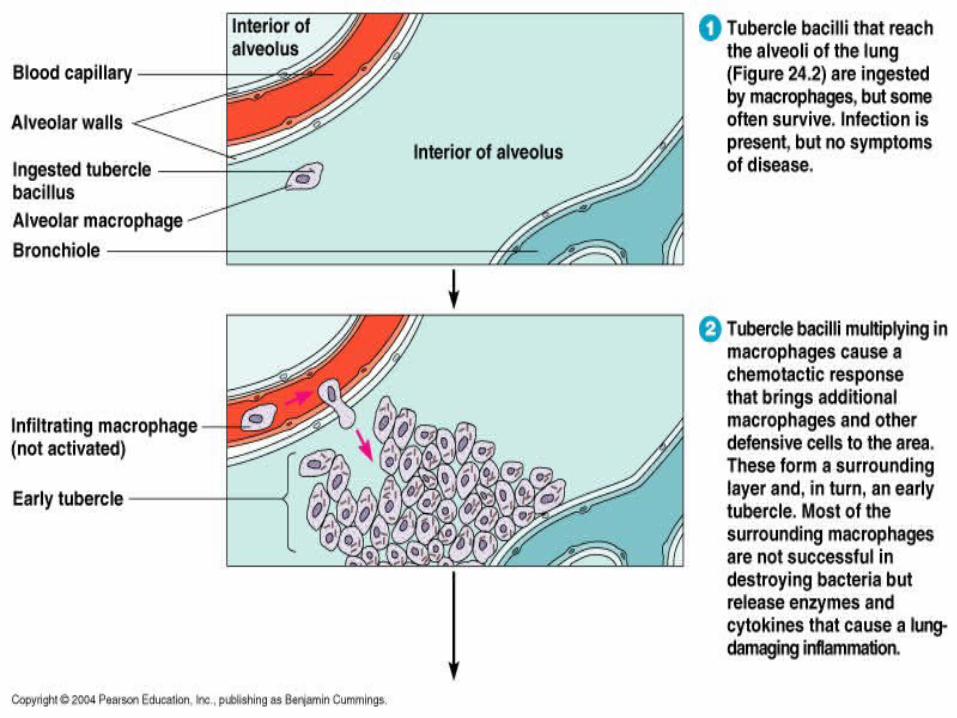
• The primary complex of tuberculosis includes the local infection of the portal of entry and the regional lymph nodes that drain the area, the lung is the portal of entry in > 98%of cases .
• The tubercule bacilli multiply within the alveoli and the alveolar ducts initially. Most of the bacilli are killed, but some survive within the inactivated macrophages which carry them through the lymphatic to the regional lymph nodes.
• When the primary infection is in the lung the hilar lymph nodes usually are involved although the upper lobe of the focus may drain in to the paratracheal nodes.
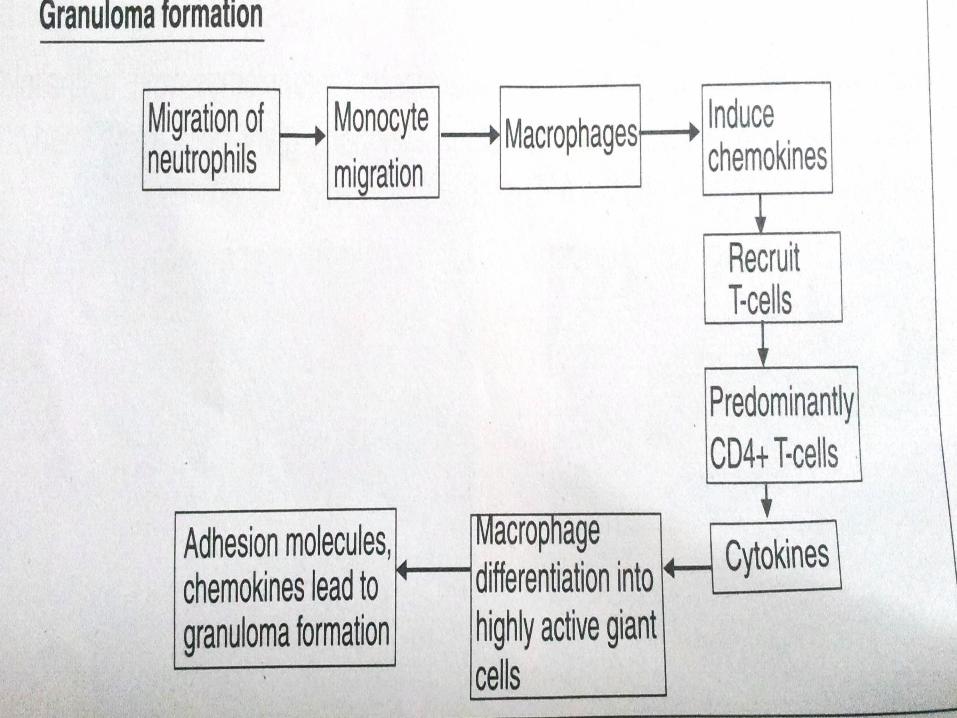
• Cell mediated immunity develops 2- 12 weeks after the initial infection , along with tissue hypersensitivity. After bacilli enters the macrophages, lymphocytes that recognizes the mycobacterial antigens proliferate and secrete lymphokines and other mediators that attract other lymphocytes and macrophages.
Certain lymphokines activate macrophages causing them to develop high concentration of lytic enzymes that enhances their mycobactericidal capacity.
• Development of specific cellular immunity prevents progression of initial infection in most individual .

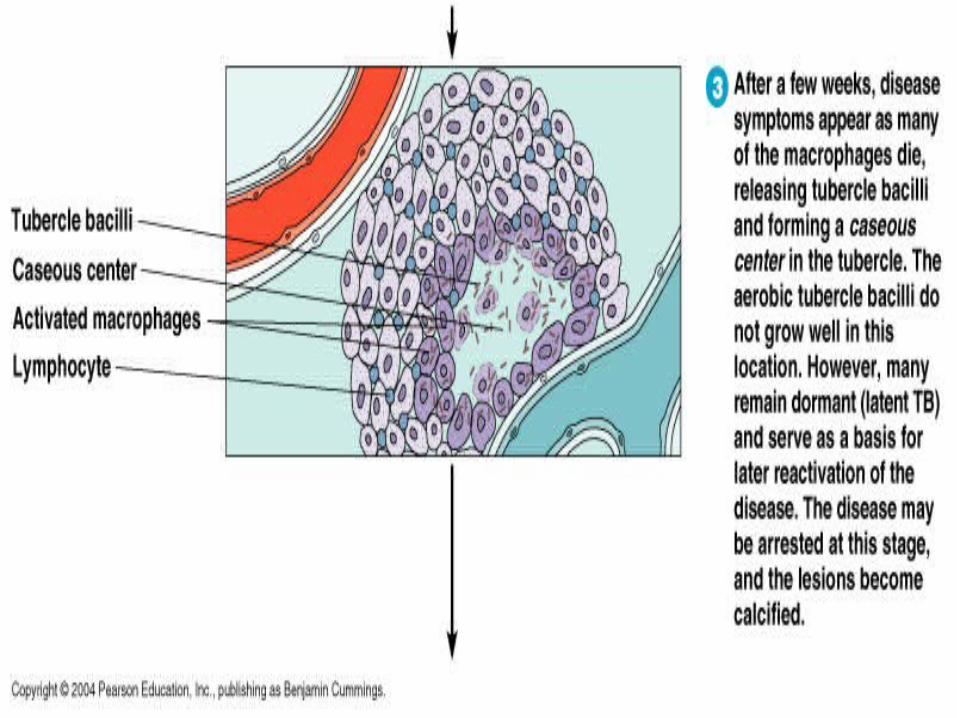
• The parenchymal portion of the primary complex often heals completely by calcification , after undergoing caseous necrosis and encapsulation. Ocassionally this portions enlarges resulting in focal pnumonitis and plueritis.
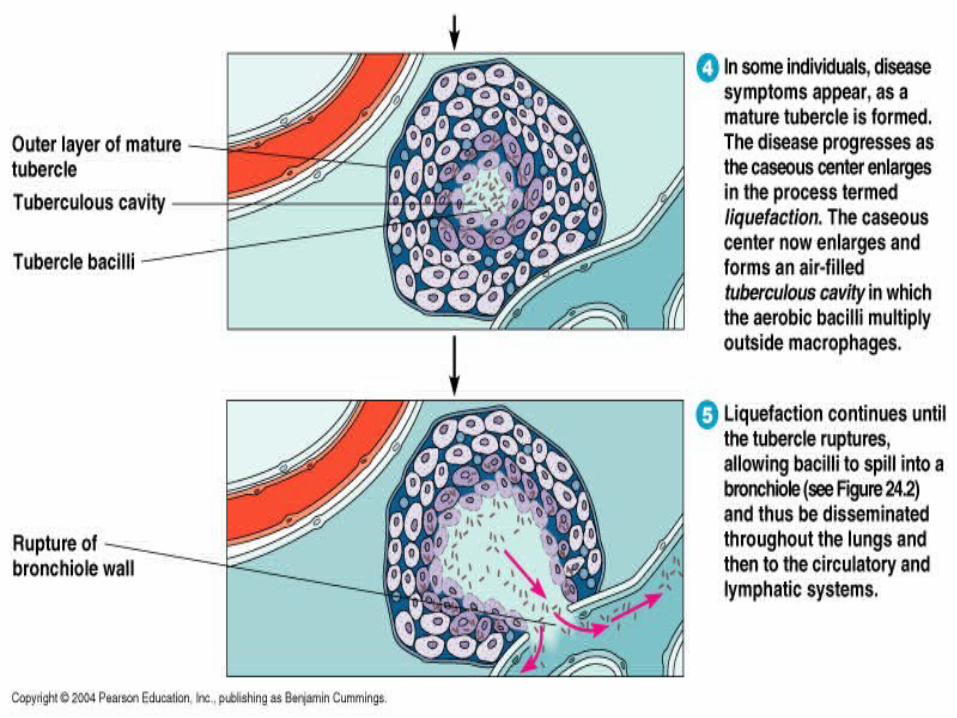
• If caseation is intense , the centre liquifies and empties in to the associated bronchus leaving a residual cavity.
• During the development of primary complex (Ghon Complex ) which is the combination of parenchymal pulmonary lesion and corresponding lymph node site , tubercle bacilli are carried to the most tissue of the body through blood and lymphatic vessels.
• Partial obstruction of the bronchus caused by external compression may cause hyperinflation in distal lung segment. Complete obstruction results in Atelectasis
The histopathological hallmark of tuberculosis is Granuloma , which is a latin term from grain / granulum . Granuloma is a focal collection of inflammatory cells in which mononuclear cells predominate. Macrophages predominate in the centre attempting to phagocytose the mycobacteria. Activated macrophages form epitheloid cells characterized by pale eosinophillic cytoplasm. This is called Epitheloid cell granuloma. Caseation necrosis is seen in the centre of the granuloma. There are two types of granuloma : Soft granuloma : These are poorly circumscribed granulomas , characterized by loose collection of neutrophils , lymphocytes, macrophages and epitheloid histiocytes with minimal fibroblastic proliferation . These lesion are more likely to contain AFB
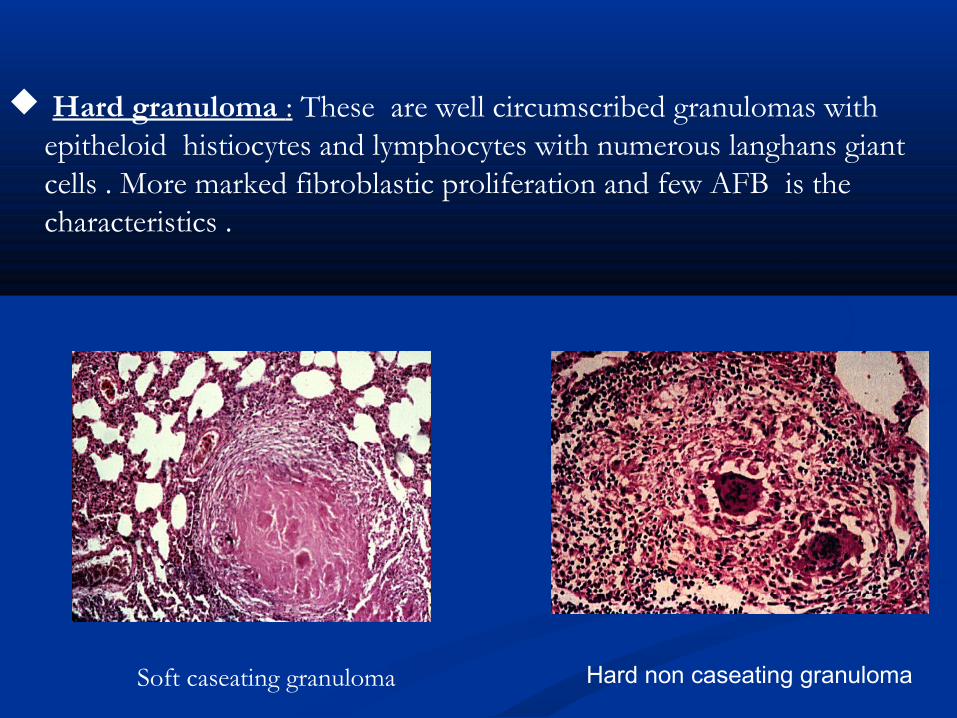
Hard granuloma : These are well circumscribed granulomas with epitheloid histiocytes and lymphocytes with numerous langhans giant cells . More marked fibroblastic proliferation and few AFB is the characteristics .
Soft caseating granuloma Hard non caseating granuloma
Pregnancy & NewbornPulmonary and particularly extrapulmonary tuberculosis other than lymphadenitis in pregnancy is associated with increased risk for prematurity , intrauterine growth retardation , low birth weight , and perinatal mortality.Congenital tuberculosis is rare because the most common result of female genital tract tuberculosis is infertility.Congenital transmission is possible from a lesion in the placenta through the umbilical vein or aspiration of amniotic fluid or hematogenous spread .
In hematogenous spread the tubercle bacilli first reach the fetal liver , where the primary focus with periportal lymph node involvement may occur. Organism pass through the liver in to the main fetal circulation and infect the other organs. The bacilli in the lung usually remain dormant until birth , when the pulmonary oxygenation and circulation increases significantly.Congenital tuberculosis may also be caused by aspiration or ingestion of infected amniotic fluid.
The micro-organism usually enters the body by inhalation through the lungs where infection is presented by a primary lesion. The infectious case (smear positive) of tuberculosis expels micro-organisms into air in tiny droplets 0.5 to 5 µm in diameter when coughing, sneezing or laughing.
These small droplets dry rapidly, become droplet nuclei carrying the micro-organism and may remain suspended in air for several hours . These droplet nuclei containing micro-organisms may be inhaled by another person who enters the room.
After inhalation, the big particles usually expelled by the secretions and cilia of the upper respiratory system while the smaller particles are settled in the lung, multiplying and causing a primary lesion from which infection may spread to other parts of the body through blood and lymphatic system
Inhalation of mycobacteria does not mean occurrence of tuberculosis, as the amount of bacilli inhaled may be not sufficient to be manifested by illness and this case is called "tuberculosis infection". Only 10% of those infected individuals may progress to a manifest disease.
The infectiousness of a person with TB disease is directly related to the number of
tubercle bacilli that he or she expels into the air. Persons who expel many tubercle
bacilli are more infectious than patients who expel few or no bacilli.
Portal of entry for tuberculosisPortal of entry for tuberculosis
Inhalation of Tubercle bacilli in >95% (M.TB)Inhalation of Tubercle bacilli in >95% (M.TB) Ingestion of milk containing Bovine Tubercle Ingestion of milk containing Bovine Tubercle
bacilli (M. bovis)bacilli (M. bovis) Contamination of superficial skin or mucous Contamination of superficial skin or mucous
membrane lesion with tubercle bacillimembrane lesion with tubercle bacilli Congenital infection occurs when mother has Congenital infection occurs when mother has
lymphohematogenous spread during pregnancy lymphohematogenous spread during pregnancy OROR tuberculous endometritis tuberculous endometritis

Latent Tuberculosis Infection (LTBI)
Persons with LTBI have M. tuberculosis in their bodies, but do not have TB disease
and cannot spread the infection to other people. A person with LTBI is not regarded
as a case of TB. The process of LTBI begins when extracellular bacilli are ingested by
macrophages and presented to other white blood cells. This triggers the immune
response in which white blood cells kill or encapsulate most of the bacilli, leading to
the formation of a granuloma. At this point, LTBI has been established.
LTBI may be detected by using the tuberculin skin test (TST) or an interferon-gamma
release assay (IGRA) .It can take 2 to 8 weeks after the initial TB infection for the
body’s immune system to be able to react to tuberculin and for the infection to be
detected by the TST or IGRA. Within weeks after infection, the immune system is
usually able to halt the multiplication of the tubercle bacilli, preventing further
progression.
Persons with LTBI have M. tuberculosis in their bodies, but do not have TB disease and cannot spread the infection to other people.
In some people, the tubercle bacilli overcome the immune system and multiply,
resulting in progression from LTBI to TB disease . Persons who have TB disease
are usually infectious and may spread the bacteria to other people. The
progression from LTBI to TB disease may occur at any time, from soon to many
years later. Body fluid or tissue from the disease site should be collected for AFB
smear and culture. Positive culture for M. tuberculosis confirms the diagnosis of
TB disease.
Persons who have TB disease may spread the bacteria to other people.
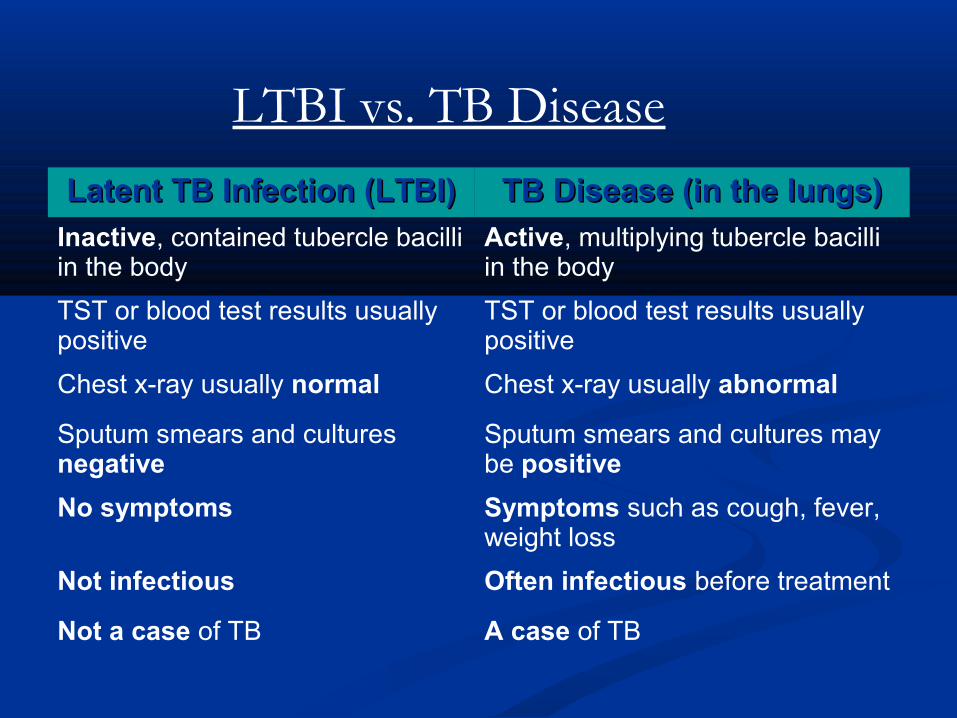
Latent TB Infection (LTBI)Latent TB Infection (LTBI) TB Disease (in the lungs)TB Disease (in the lungs)
Inactive, contained tubercle bacilli in the body
Active, multiplying tubercle bacilli in the body
TST or blood test results usually positive
TST or blood test results usually positive
Chest x-ray usually normal Chest x-ray usually abnormal
Sputum smears and cultures negative
Sputum smears and cultures may be positive
No symptoms Symptoms such as cough, fever, weight loss
Not infectious Often infectious before treatment
Not a case of TB A case of TB
LTBI vs. TB Disease

• Children exposed to open case of tuberculosis.
• children with viral infections like measles, mumps, pertussis , varicella.
• Infants and children < 4yrs of age
• Children co infected with HIV.
• Childrens with skiin test conversion in the past 1-2 yrs.
• Childrens who are immunocompromised especially in cases of malignancy and solid organ transplantation , immunosuppressive medical treatments including anti- tumour necrosis factor, diabetes mellitus, chronic renal failure, silicosis, and malnutrition.
• Homeless childrens.

Primary tuberculous infectionPrimary tuberculous infection
Primary Focus (GhonPrimary Focus (Ghon’s focus)’s focus) at the site of first implantationat the site of first implantation usually single and Subpleuralusually single and Subpleural in most, - heals and disappears, orin most, - heals and disappears, or it heals by calcification.it heals by calcification.Primary Complex:Primary Complex: primary focus + Hilar lymphnodes + draining primary focus + Hilar lymphnodes + draining
lymphaticslymphatics complications arise more commonly from regional complications arise more commonly from regional
adenitis than from the primary focusadenitis than from the primary focus
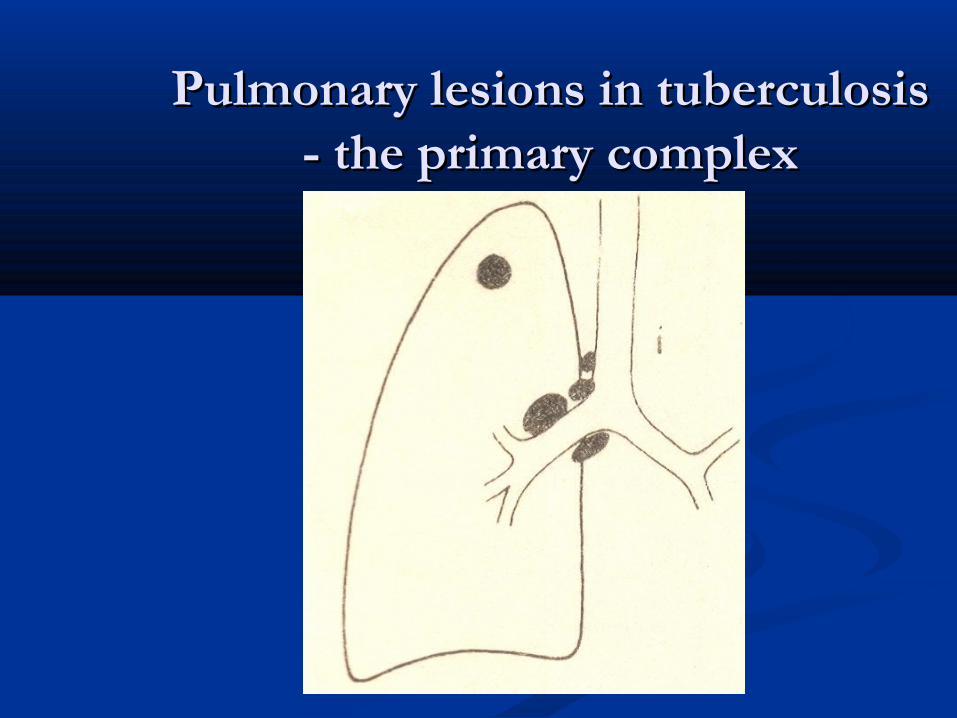
Pulmonary lesions in tuberculosisPulmonary lesions in tuberculosis- the primary complex- the primary complex
Primary infectionPrimary infection Children vs. AdultsChildren vs. Adults
In adults, In adults,
- regional lymphadenitis less marked- regional lymphadenitis less marked
- bronchial erosion less frequent- bronchial erosion less frequent
- less risk of dissemination- less risk of dissemination Thus, adult primary infection tends to be Thus, adult primary infection tends to be
more local and pulmonary.more local and pulmonary.
Progressive primary tuberculosisProgressive primary tuberculosis
Progression of TB depends on the age of the Progression of TB depends on the age of the child, number of tubercle bacilli, and host child, number of tubercle bacilli, and host resistance.resistance.
Apparently healed focus or nodes may contain Apparently healed focus or nodes may contain viable organisms for many years.viable organisms for many years.
During 1During 1stst 4-8 weeks, organisms are disseminated 4-8 weeks, organisms are disseminated in the blood stream.in the blood stream.

Progressive pulmonary diseaseProgressive pulmonary disease
Progressive primary infectionProgressive primary infection: Progression of : Progression of recently acquired pulmonary primary infection. recently acquired pulmonary primary infection.
Endogenous exacerbationEndogenous exacerbation: reactivity of : reactivity of organisms and breakdown of primary lesions organisms and breakdown of primary lesions acquired > 5 years previously.acquired > 5 years previously.
Exogenous exacerbationExogenous exacerbation: Re-infection by newly : Re-infection by newly acquired bacilli in persons with healed primary acquired bacilli in persons with healed primary lesions.lesions.
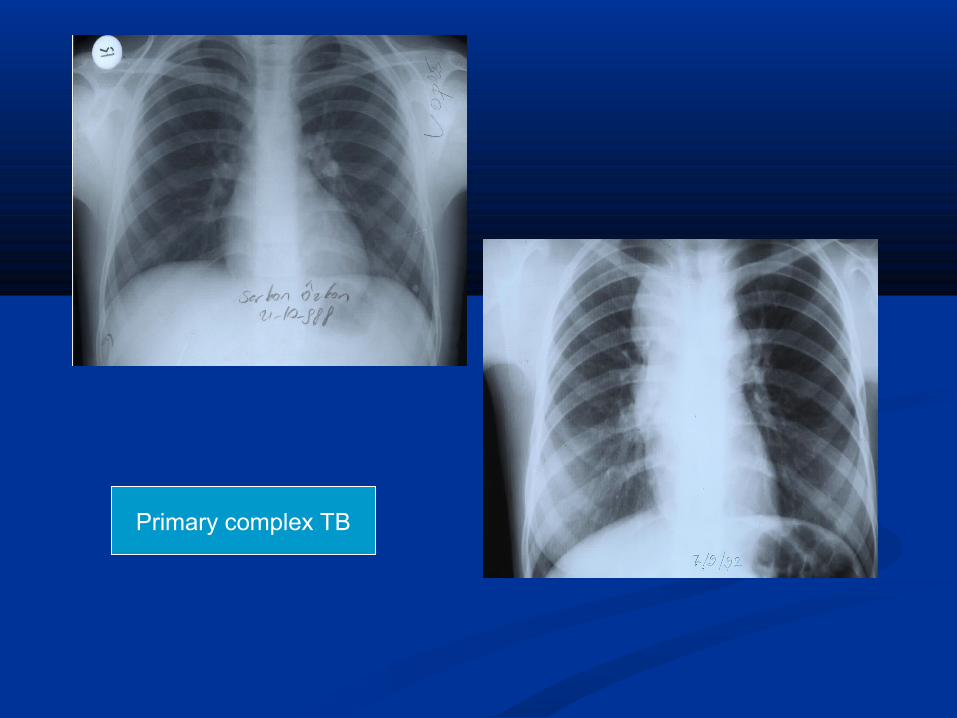
Primary complex TB
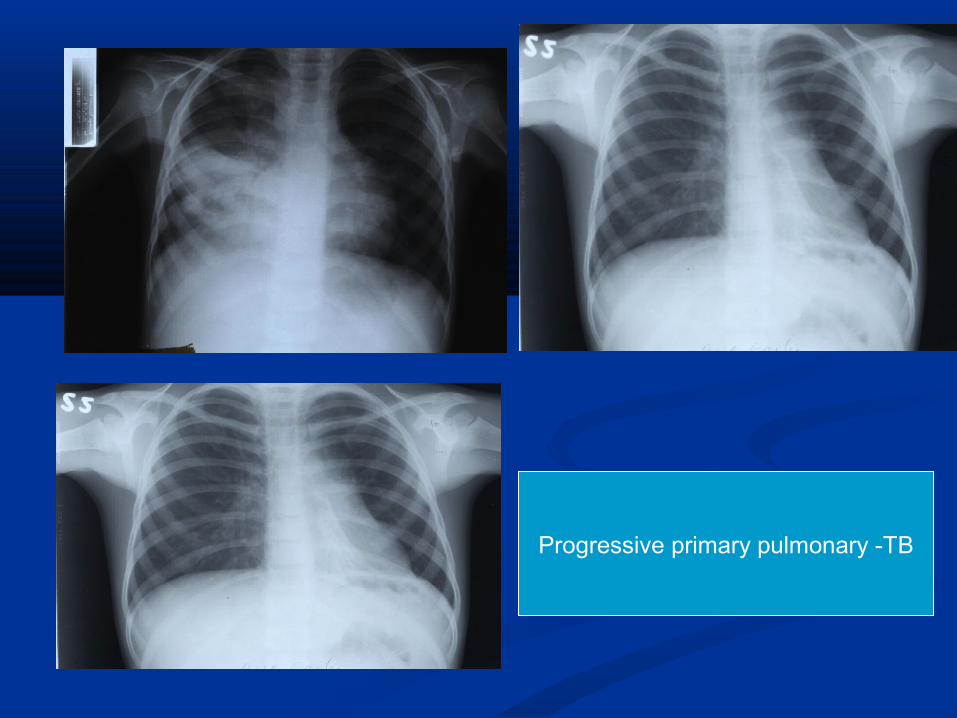
Progressive primary pulmonary -TB
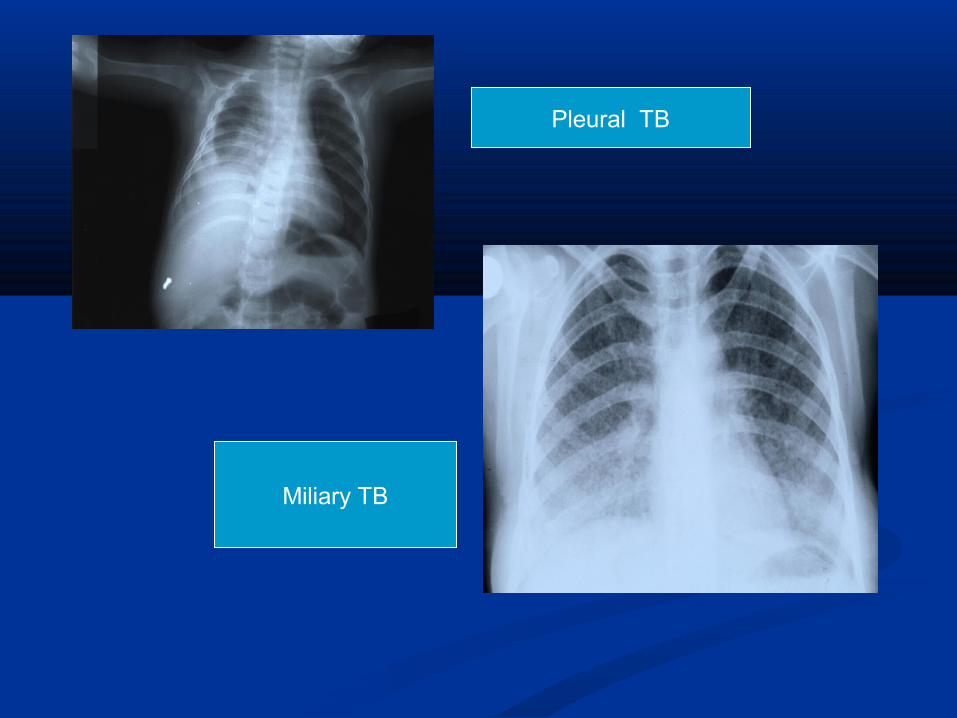
Pleural TB
Miliary TB
Complications of regional nodesComplications of regional nodes
1. Incomplete (ball-valve) bronchial obstruction, emphysema of middle & lower lobes
2. Complete bronchial obstruction, collapse of right lower lobe
3. Erosion of node into bronchus & segmental consolidation
4. Rupture of node into pericardium: tuberculous pericardial effusion
Sequelae of bronchial complicationsSequelae of bronchial complications
1. Stricture of bronchus at site of erosion
2. Cylindrical bronchiectasis in area of old collapse
3. Wedge shadow: contracture & fibrosis of segmental lesion
4. Linear scar of fibrosis following segmental lesion
42
Sites of TB Disease (2)Sites of TB Disease (2)Location Frequency
Pulmonary TB
Lungs Most TB cases are pulmonary
Extrapulmonary TB
Places other than lungs such as:• Lymph nodes• Pleura• Brain• Kidneys• Bones and joints
Found more often in:
• HIV-infected or other immunosuppressed persons
• Young children
Miliary TB Carried to all parts of body, through bloodstream
Rare
Symptoms of childhood Symptoms of childhood tuberculosistuberculosis
1.1. PulmonaryPulmonary : dry cough , low grade fever, : dry cough , low grade fever, predominantly evening rise of temperature, weight loss,predominantly evening rise of temperature, weight loss,
loss of appetite. Rarely hemoptysis can occur .loss of appetite. Rarely hemoptysis can occur .
2.2. Lymph node Lymph node : fever , lymphadenopathy (mediastinal : fever , lymphadenopathy (mediastinal lymph node) , cold abcess, cough and fever .lymph node) , cold abcess, cough and fever .
3.3. PlueraPluera : cough (non productive ) , pl ueritic chest : cough (non productive ) , pl ueritic chest
pain .pain .
4.4. Genitourinary Genitourinary : dysuria , nocturia, increased frequency,: dysuria , nocturia, increased frequency,
tenderness / swelling of testis / epididymis . Presence of tenderness / swelling of testis / epididymis . Presence of sterile pyuria should always lead to search for sterile pyuria should always lead to search for tuberculosis. tuberculosis.

5. Skeletal TB (POTTS SPINE ) : fever , backache is commonly seen. Paresis or plegia depending upon duration of development is a cause of concern. Joint pain / cold abcess formation is also commonly seen.
6. CNS TB : fever , malaise , anorexia , iritability , later on as the diesease preogress neurological symptoms develop like progressive headache, lethargy , impaired cognition , memory disturbance, confusion and then stupor – coma with or with out neurological deficit. Features of meningitis may be present.
8. Abdominal : peritonotis followed by ileo-caecal , ano rectal and
mesentric lymph nodes infection. In peritoneal tuberculosis TB
fever , ascitis , pain , anorexia , / weight loss are common.
8. Pericardial : fever , dyspnoea , tachycardia , neck vein distension edema , hepatomegaly , paradoxical pulse , pericardial rub.
9.Disseminated and miliary Koch’s : This is a haematogenous spread and amongst one of the serious manifestations of tuberculosis . patients are cachetic and present with fever , weight loss and multi organ symptoms . Bone marrow involvement now a days frequently seen.


Miliary tuberculosisMiliary tuberculosis
most common within 1most common within 1stst 3 to 6 months after 3 to 6 months after infectioninfection
due to heavy hematogenous spread of tubercle due to heavy hematogenous spread of tubercle bacillibacilli
Onset: Insidious, with Onset: Insidious, with Fever and weight lossFever and weight loss Palpable liver and/or spleenPalpable liver and/or spleen Tachypnoea with normal chest findingsTachypnoea with normal chest findings
Miliary tuberculosisMiliary tuberculosis
Hematogenous dissemination leads to progressive Hematogenous dissemination leads to progressive development of small lesions throughout the body, development of small lesions throughout the body, with tubercles in the with tubercles in the
lung, spleen, liver, lung, spleen, liver, bone marrow, heart, pancreasbone marrow, heart, pancreas brain, choroid, skinbrain, choroid, skin Radiologic diagnosisRadiologic diagnosis:: ““Snow stormSnow storm”” appearance appearance
(Multiple small lung nodules 1mm size and above in (Multiple small lung nodules 1mm size and above in both lung fields).both lung fields).

Miliary TBMiliary TB
Cutaneous TuberculosisCutaneous Tuberculosis 1.1. Associated with primary complexAssociated with primary complex
(Direct inoculation into Traumatized Area)(Direct inoculation into Traumatized Area) - Painless nodule, leading to non healing ulcer with regional - Painless nodule, leading to non healing ulcer with regional
lymphadenitislymphadenitis - Scrofuloderma over ruptured caseous lymph node- Scrofuloderma over ruptured caseous lymph node2.2. Associated with Hematogenous disseminationAssociated with Hematogenous dissemination - Papulonecrotic tuberculids- Papulonecrotic tuberculids papules with soft centers on trunk, thighs and facepapules with soft centers on trunk, thighs and face - Tuberculosis verrucosa cutis- Tuberculosis verrucosa cutis Large tuberculids on arms and legsLarge tuberculids on arms and legs3.3. Associated with hypersensitivity to tuberculinAssociated with hypersensitivity to tuberculin - Erythema nodosum- Erythema nodosum painful indurated nodules on shins, elbows, forearms thatpainful indurated nodules on shins, elbows, forearms that subside in 2-3 weekssubside in 2-3 weeks
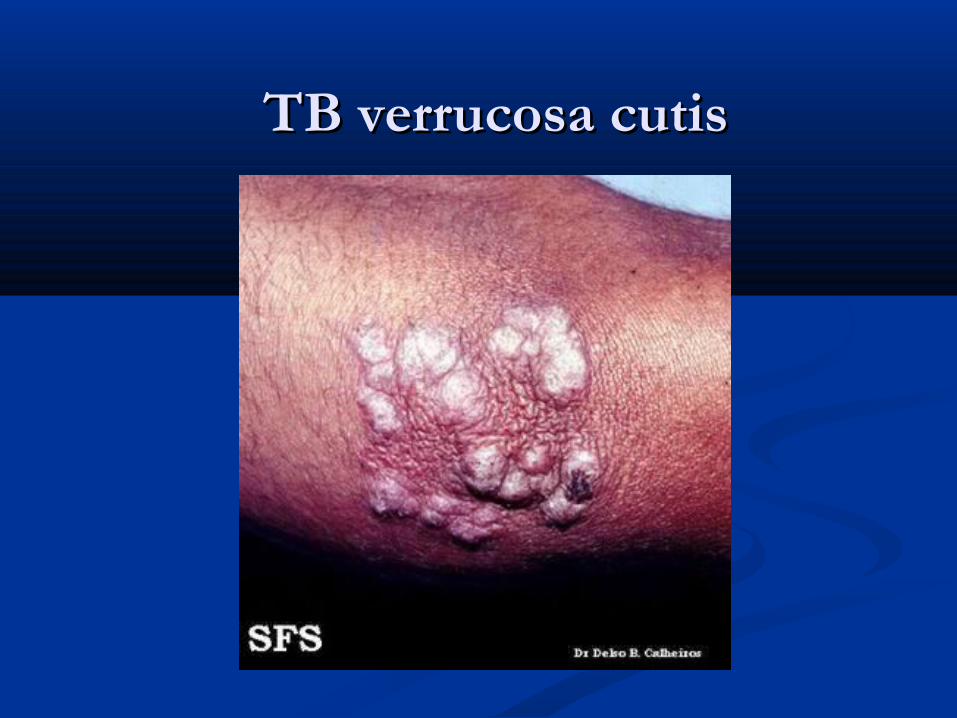
TB verrucosa cutis TB verrucosa cutis

Erythema nodosumErythema nodosum
Tuberculosis of superficial Tuberculosis of superficial lymph nodes (scrofula)lymph nodes (scrofula)
Tonsillar / submandibular Tonsillar / submandibular
(Spread from paratracheal nodes)(Spread from paratracheal nodes) Supraclavicular Supraclavicular
(From primary lesion in upper lobe)(From primary lesion in upper lobe) Axillary / epitrochlear Axillary / epitrochlear
(From skin lesion on hand)(From skin lesion on hand) Inguinal Inguinal
(From ulcer on sole of foot)(From ulcer on sole of foot)
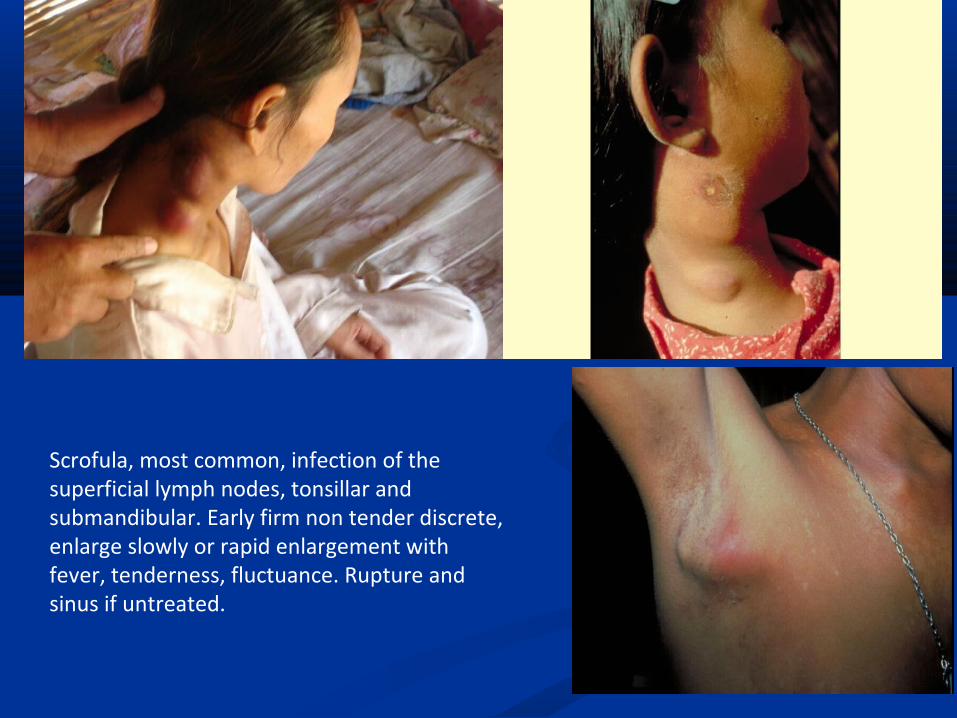
Scrofula, most common, infection of the superficial lymph nodes, tonsillar and submandibular. Early firm non tender discrete, enlarge slowly or rapid enlargement with fever, tenderness, fluctuance. Rupture and sinus if untreated.
• The nodes usually enlarge gradually in the early stage of the lymph node disease the lymph nodes are discrete , firm , matted , nontender , often fixed to the under lying skin . It is usually unilateral , but bilateral involvement may also occur because of the cross over drainage pattern of the lymphatics.
• Systemic signs and symptoms other than low grade fever are usually absent . The tuberculin skin test is usually reactive. But the chest radiograph is also normal in 70% of cases .
• Lymph node TB may require surgical removal , due to the rupture of the capsule of lymph node resulting in the formation of the draining sinus tract. The tuberculosis lymph adenitis can usually by fine needle aspiration of the node . It responds to ATT .
Although the lymph nodes do not return to the normal size for months or even years.
Differential diagnosis for TB lymphadenitis are : • Non Tuberculous Mycobacteria (NTM)• Cat scratch disease ( BARTONELLA HENSELAE)• Tularemia• Brucellosis • Toxoplasmosis• Tumor• Branchial cyst• Cystic hygroma • Pyogenic infection.

Ocular TuberculosisOcular Tuberculosis
Primary tuberculous conjunctivitisPrimary tuberculous conjunctivitis (after trauma) (after trauma)
Yellowish – gray nodules on palpebral conjunctiva Yellowish – gray nodules on palpebral conjunctiva with preauricular adenopathywith preauricular adenopathy
Phlyctenular conjunctivitisPhlyctenular conjunctivitis (Hypersensitivity) (Hypersensitivity)
Nodules on limbus recurring in crops for weeksNodules on limbus recurring in crops for weeks
Tubercles of choroidTubercles of choroid (with miliary TB) (with miliary TB)
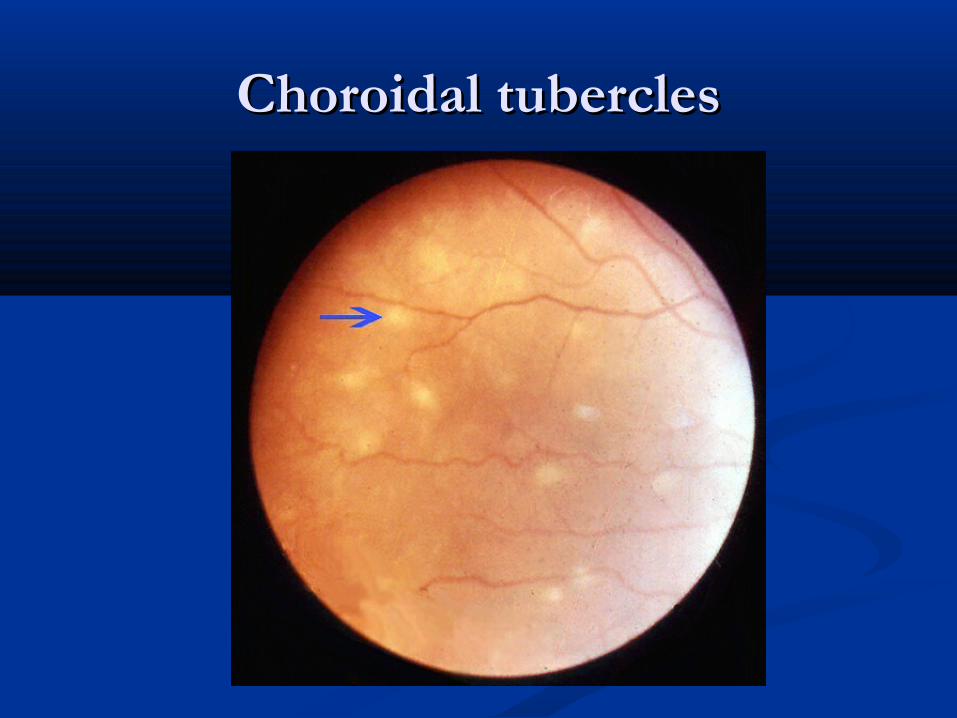
Choroidal tuberclesChoroidal tubercles
GI and Abdominal TBGI and Abdominal TB
Hematogenous spread from lungs or swallowing Hematogenous spread from lungs or swallowing of infected sputum. of infected sputum.
Painless ulcer in gingivolabial sulcus with Painless ulcer in gingivolabial sulcus with submental or submandibular adenopathysubmental or submandibular adenopathy
Ulcer on tonsilUlcer on tonsil Esophageal diverticulum secondary to rupture of Esophageal diverticulum secondary to rupture of
mediastinal nodes into lumenmediastinal nodes into lumen
Tuberculous toxemiaTuberculous toxemia Present with colicky abdominal pain, vomiting and Present with colicky abdominal pain, vomiting and
constipation. constipation. Abdomen feels doughy. Abdomen feels doughy. Rolled up omentum and enlarged lymph nodes may Rolled up omentum and enlarged lymph nodes may
appear as irregular nodular masses with ascitesappear as irregular nodular masses with ascites Tuberculous enteritisTuberculous enteritis Ulcers, mesenteric adenitis, peritonitisUlcers, mesenteric adenitis, peritonitis Adhesions, subacute intestinal obstruction,Adhesions, subacute intestinal obstruction, HepatosplenomegalyHepatosplenomegaly

• Tuberculous peritonitis: which occurs in young men and adolescence rare in children arises from the subclinical or haematogenous dissemination .
Localised peritonitis is caused by direct extension from abdominal lymphnode ,intestinal focus/ genitourinay tuberculosis.
• Abdominal pain / tenderness , ascites , anorexia , low grade fever are the typical manifestations. The tuberculin test is usually reactive.
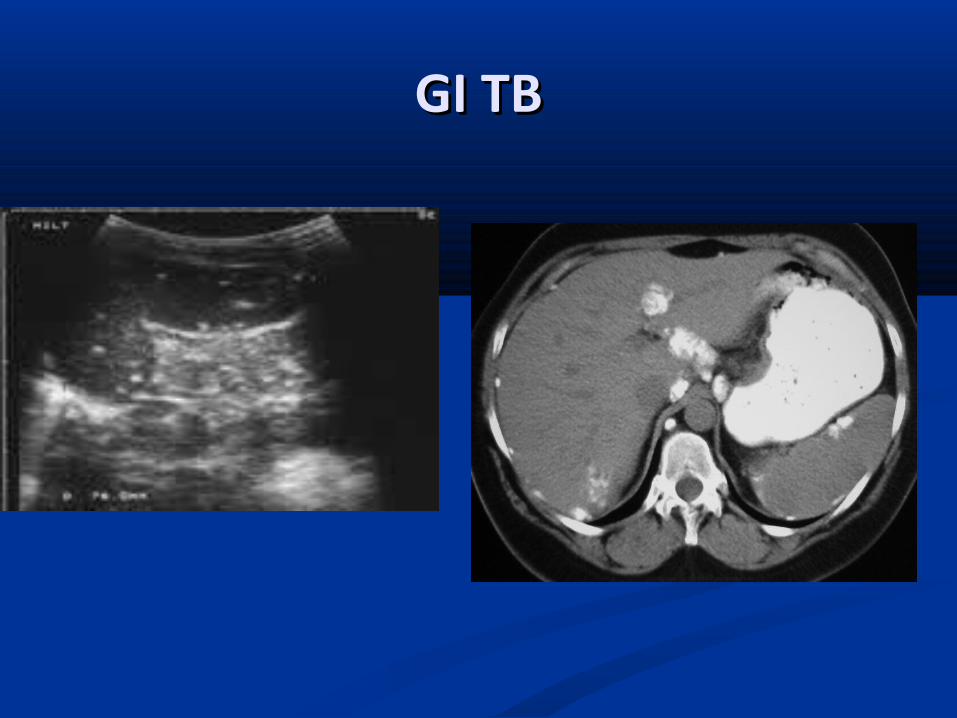
GI TBGI TB

Renal tuberculosisRenal tuberculosis
Tubercles in glomeruli lead to shedding of Tubercles in glomeruli lead to shedding of tubercle bacilli into tubules tubercle bacilli into tubules
Caseous mass / Cavity between cortex and Caseous mass / Cavity between cortex and pyramidspyramids
TB of bladder (Tuberculous cystitis)TB of bladder (Tuberculous cystitis) SymptomsSymptoms: dysuria, hematuria, : dysuria, hematuria,
pyuria with TB bacillipyuria with TB bacilli
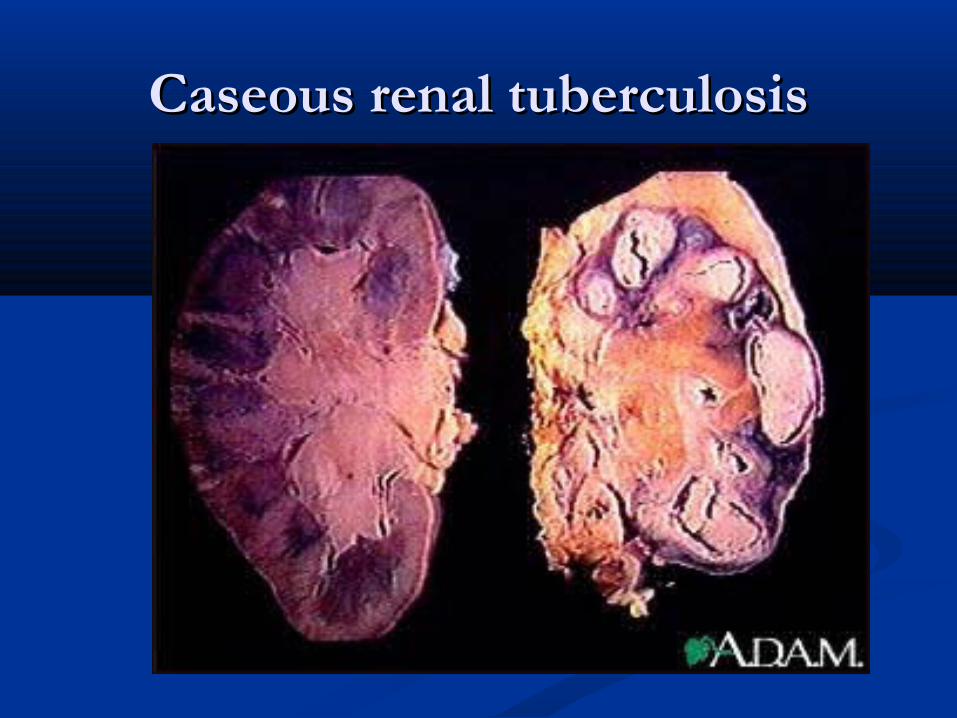
Caseous renal tuberculosisCaseous renal tuberculosis
Skeletal tuberculosisSkeletal tuberculosis Bones involved in order of frequencyBones involved in order of frequency: : Vertebrae > knee > hip > elbowVertebrae > knee > hip > elbow Upper extremities and non-weight-bearing bonesUpper extremities and non-weight-bearing bones (skull, clavicle) rarely involved(skull, clavicle) rarely involved Tuberculous spondylitisTuberculous spondylitis most commonly most commonly Thoracic / Lumbar / Both (Decreasing frequency)Thoracic / Lumbar / Both (Decreasing frequency) X-ray findingsX-ray findings: : Narrowing of disc space, Collapse of vertebral Narrowing of disc space, Collapse of vertebral
bodybody Extensive destruction with kyphosis (Pott disease)Extensive destruction with kyphosis (Pott disease) ComplicationsComplications:Para vertebral abscess (Pott abscess):Para vertebral abscess (Pott abscess) Psoas Abscess. Paraplegia, Quadriplegia (cervical)Psoas Abscess. Paraplegia, Quadriplegia (cervical)
HistoryHistory
Presentation depends on the following: Presentation depends on the following: Stage of disease Stage of disease Site Site Presence of complications such as neurologic deficits, abscesses, Presence of complications such as neurologic deficits, abscesses,
or sinus tractsor sinus tracts
The reported average duration of symptoms at the time of The reported average duration of symptoms at the time of diagnosis is 3-4 months. diagnosis is 3-4 months.
Back pain is the earliest and most common symptom. Back pain is the earliest and most common symptom. Patients have usually had back pain for weeks prior to Patients have usually had back pain for weeks prior to
presentation. presentation. Pain can be spinal or radicular.Pain can be spinal or radicular.
Constitutional symptoms include fever and weight loss. Constitutional symptoms include fever and weight loss.
Neurologic abnormalities occur in 50% of cases and can Neurologic abnormalities occur in 50% of cases and can include spinal cord compression with paraplegia, paresis, include spinal cord compression with paraplegia, paresis, impaired sensation, nerve root pain, or cauda equina impaired sensation, nerve root pain, or cauda equina syndrome. syndrome.
Cervical spine tuberculosis is a less common presentation is Cervical spine tuberculosis is a less common presentation is characterized by pain and stiffness. characterized by pain and stiffness.
Patients with lower cervical spine disease can present Patients with lower cervical spine disease can present with dysphagia or stridor. with dysphagia or stridor. Symptoms can also include torticollis, hoarseness, and Symptoms can also include torticollis, hoarseness, and neurologic deficits.neurologic deficits.
The clinical presentation of spinal tuberculosis in patients The clinical presentation of spinal tuberculosis in patients infected with the human immunodeficiency virus (HIV) is infected with the human immunodeficiency virus (HIV) is similar to that of patients who are HIV negative; however, similar to that of patients who are HIV negative; however, the relative proportion of individuals who are HIV positive the relative proportion of individuals who are HIV positive seems to be higher. seems to be higher.
Osseous Clinical manifestationsOsseous Clinical manifestations
TB osteitisTB osteitis Synovitis/epiphysitis, destructive arthritis, fusion Synovitis/epiphysitis, destructive arthritis, fusion
in deformed positionsin deformed positions Abscesses may track through tissues (psoas)Abscesses may track through tissues (psoas)
TB arthritis (PonchetTB arthritis (Ponchet’s Disease)’s Disease) 1-5% children if TB untreated1-5% children if TB untreated Knee/hip/elbow/dacylitisKnee/hip/elbow/dacylitis Thick, inflammatory synovium, invades articular Thick, inflammatory synovium, invades articular
surface, with erosion and fibrosis jointsurface, with erosion and fibrosis joint

PottPott’s Disease’s Disease
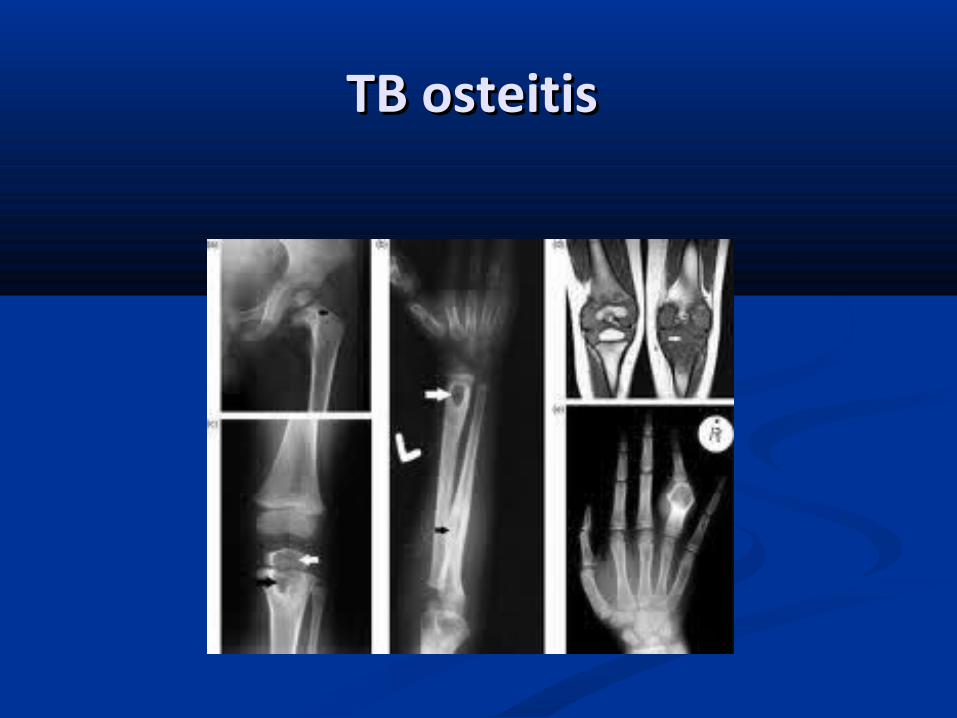
TB osteitis TB osteitis
Genital tuberculosisGenital tuberculosis
Uncommon before pubertyUncommon before puberty Usually due to lympho-hematogenous spreadUsually due to lympho-hematogenous spread Occasionally by direct extension from Occasionally by direct extension from
adjacent lesion of bone, gut, or urinary tractadjacent lesion of bone, gut, or urinary tract

Genital tuberculosisGenital tuberculosis
SalpingitisSalpingitis EndometritisEndometritis OophoritisOophoritis Cervicitis Cervicitis Infertility is commonest sequel Infertility is commonest sequel in malesin males:: Primary tuberculosis of penis after circumcision Primary tuberculosis of penis after circumcision
with inguinal adenopathywith inguinal adenopathy Epididymitis / Epididymo – orchitis in early Epididymitis / Epididymo – orchitis in early
childhoodchildhood

CNS ManifestationsCNS Manifestations Rich focus, vessels infiltrated by exudateRich focus, vessels infiltrated by exudate
Inflamation/infarctionInflamation/infarction Brain stem: CN III,VI,VII dysfunctionBrain stem: CN III,VI,VII dysfunction Basilar cisterns obstructed: hydrocephalus Basilar cisterns obstructed: hydrocephalus
TB meningitisTB meningitis Children < 4 yrs age, most common in 3-6 month of primary infectionChildren < 4 yrs age, most common in 3-6 month of primary infection Gradual onset, rapid in infants HydrocephalusGradual onset, rapid in infants Hydrocephalus Tuberculomas (20-37%)Tuberculomas (20-37%) Mortality (<10% w/ Rx) Morbidity high (MR, Sz, hemiparesis)Mortality (<10% w/ Rx) Morbidity high (MR, Sz, hemiparesis) TST – in 40%, CXR nl 50% TST – in 40%, CXR nl 50% CSF: cell # 10-100, glucose low, protein highCSF: cell # 10-100, glucose low, protein high
TuberculomaTuberculoma Most common in < 10yrs ageMost common in < 10yrs age Infratentorial: headaches, Seizures, increased ICPInfratentorial: headaches, Seizures, increased ICP
Tuberculous meningitisTuberculous meningitisTB meningitis seen in 1/300 Primary infectionsTB meningitis seen in 1/300 Primary infectionsPathophysiology:Pathophysiology:Rupture of a subcortical caseous focus (RichRupture of a subcortical caseous focus (Rich’s) into the ’s) into the
subarachnoid space.subarachnoid space.Inflammatory exudates form about base of brain and along Inflammatory exudates form about base of brain and along
cerebral vessels as they pass over hemispheres.cerebral vessels as they pass over hemispheres.Raised intracranial pressure due to increased secretion of Raised intracranial pressure due to increased secretion of
CSF CSF Adhesions along base and roof of 4Adhesions along base and roof of 4 thth ventricles lead to ventricles lead to
obstruction to CSF flow and hydrocephalus,obstruction to CSF flow and hydrocephalus,involvement of cranial nerves III VI VII and optic chiasma.involvement of cranial nerves III VI VII and optic chiasma.Cerebral endarteritis narrows lumen, reduces blood flow, Cerebral endarteritis narrows lumen, reduces blood flow,
leads to cerebral thrombosis and infarction. leads to cerebral thrombosis and infarction.
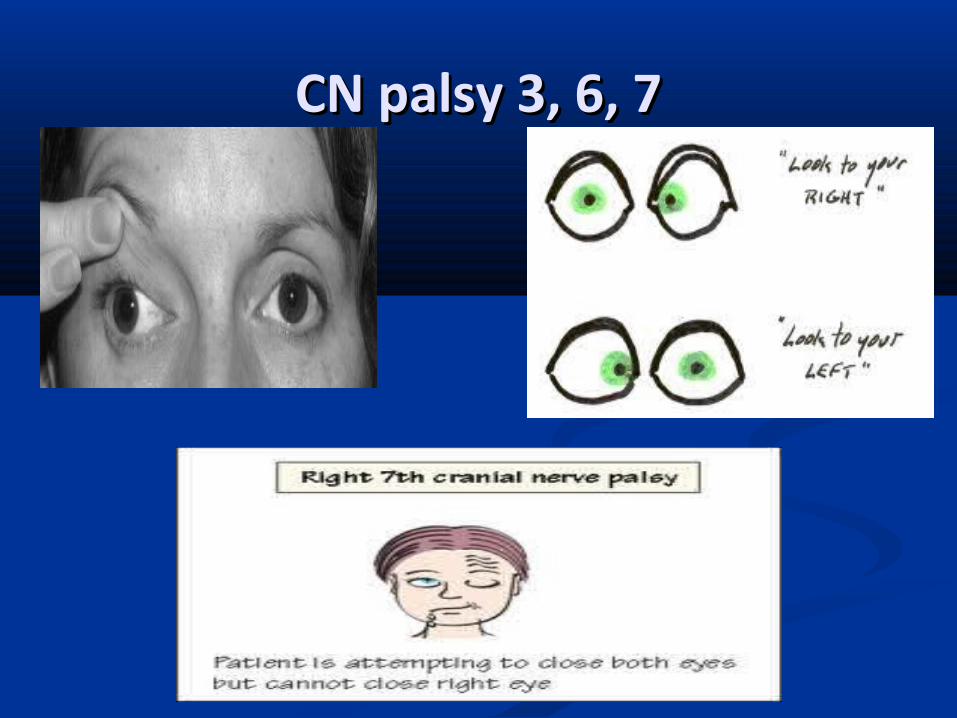
CN palsy 3, 6, 7CN palsy 3, 6, 7

Stages of TB meningitisStages of TB meningitis
Stage I Irritability, anorexia, headache, drowsiness,Stage I Irritability, anorexia, headache, drowsiness,
vomiting, fever, malaise.vomiting, fever, malaise.
Stage II : Focal neurological signs, cranial nerve palsies Stage II : Focal neurological signs, cranial nerve palsies Seizures, squint, lethargy, positive Kernig and Seizures, squint, lethargy, positive Kernig and Brudzinki sign. Brudzinki sign.
Stage III : Loss of consciousness, hemiplegia, Coma, Stage III : Loss of consciousness, hemiplegia, Coma, Papilloedema, Decerebrate rigidity and eventually Papilloedema, Decerebrate rigidity and eventually death.death.
Complications of TB meningitisComplications of TB meningitis
HydrocephalusHydrocephalusSubdural effusionSubdural effusionLate: Hemiplegia / ParaplegiaLate: Hemiplegia / Paraplegia Intellectual impairmentIntellectual impairment BlindnessBlindness DeafnessDeafness Intracranial calcifications leading to Intracranial calcifications leading to hypothalamic and pituitary dysfunctionhypothalamic and pituitary dysfunction - Growth failure- Growth failure - Diabetes insipidus- Diabetes insipidus - Failure of development of secondary sexual - Failure of development of secondary sexual characteristicscharacteristics

Diagnosis of TB meningitisDiagnosis of TB meningitis Signs of meningeal irritationSigns of meningeal irritation X-ray chestX-ray chest CT scan – basal exudates, inflammatory granulomas etcCT scan – basal exudates, inflammatory granulomas etc Tuberculin testingTuberculin testing Retinoscopy for choroidal tuberclesRetinoscopy for choroidal tubercles Lumbar punctureLumbar puncture Elevated CSF pressure(30 – 40cm h2o)Elevated CSF pressure(30 – 40cm h2o)
Cobweb Coagulum/ pellicle on standing Cobweb Coagulum/ pellicle on standing 100 – 500 WBCs / cu.mm100 – 500 WBCs / cu.mm
protein are elevated (400 – 5000 mg/dl) protein are elevated (400 – 5000 mg/dl) secondarily to hydrocephalus and spinal block. secondarily to hydrocephalus and spinal block.
Low / Normal sugar< 40mg/dlLow / Normal sugar< 40mg/dl AFB smear & cultureAFB smear & culture
Prognosis in TB meningitisPrognosis in TB meningitis
100% mortality in 3-4 weeks without treatment100% mortality in 3-4 weeks without treatment
100% survival with treatment started in Stage I100% survival with treatment started in Stage I
75% survival with treatment started in Stage II75% survival with treatment started in Stage II
Stage III – variable survival, all will have sequelaeStage III – variable survival, all will have sequelae

Tuberculoma : A tumour like mass arising from the aggregation of caseous tubercles clinically presenting as a brain tumour.•Lesions are most often singular but may be multiple.Tuberculoma in children are located infratentorial located at the base of the brain near Cerebellum. •Clinical presentation is similar to neurocysticercosis.
• Tuberculoma rings are usually large . On CT or MRI of the brain the lesion often has a thick irregular wall , ring enhancing lesion and associated with severe perilesional edema.
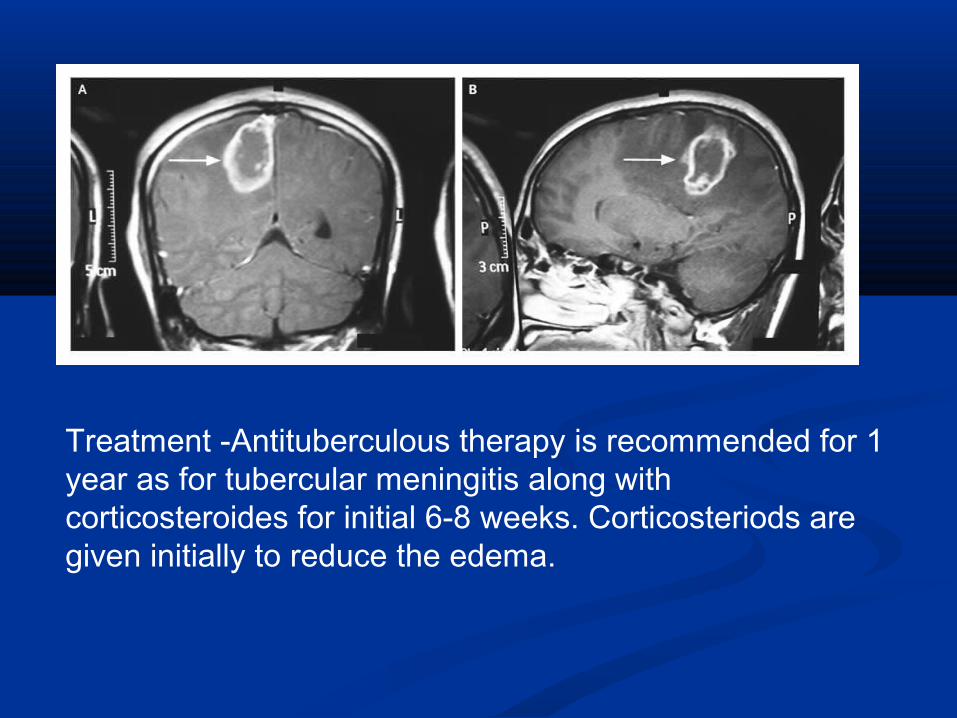
Treatment -Antituberculous therapy is recommended for 1 year as for tubercular meningitis along with corticosteroides for initial 6-8 weeks. Corticosteriods are given initially to reduce the edema.
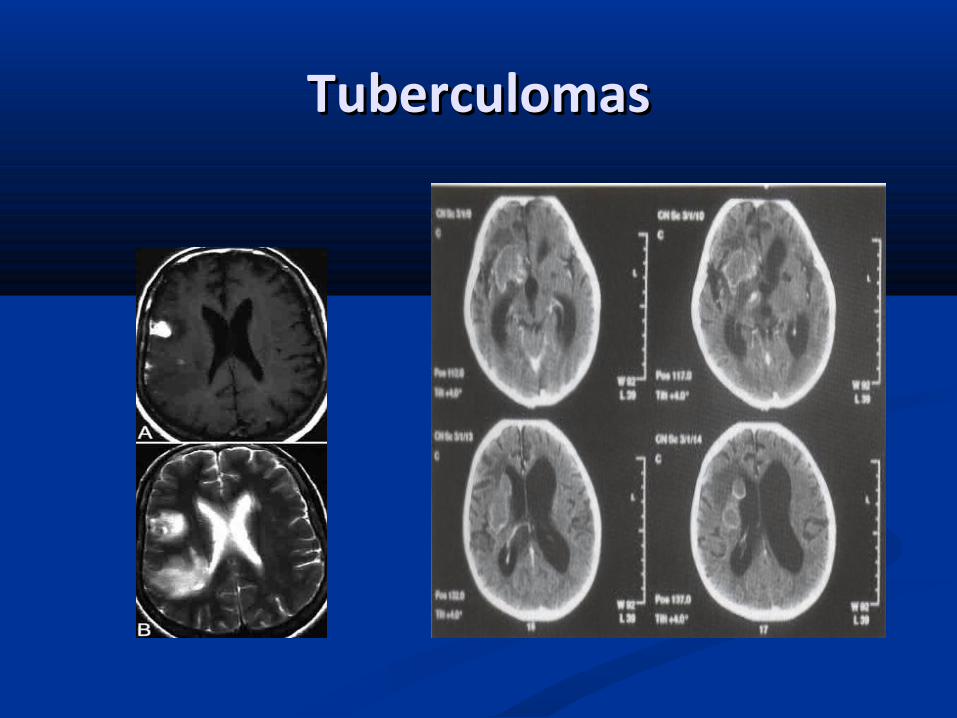
TuberculomasTuberculomas

ReferencesReferences
NelsonNelson’’s textbook of paediatricss textbook of paediatrics Pediatric tuberculosis , by Vimlesh sethPediatric tuberculosis , by Vimlesh seth IAP Textbook IAP Textbook Essentials of tuberculosis in children by kabra skEssentials of tuberculosis in children by kabra sk Internet Internet