105
Tumors of Larynx Prepared by Dr.Hiwa Asad
| Date post: | 22-Dec-2015 |
| Category: |
Documents |
| Upload: | felicia-french |
| View: | 242 times |
| Download: | 4 times |
Tumors of Larynx
Prepared by Dr.Hiwa Asad

Benign Tumors
• Ectodermal
• Mesodermal
• pseudotumours

Ectodermal Tumours
• Papilloma: single or multiple
• Adenoma
• Paraganglioma
• Neurilemmoma

• Common in adults, rare in children• Sessile or pedunculated• Usual sites anterior commissure, anterior half of
the vocal cords• Men : women ratio 2:1• Present with hoarseness• If small removed endoscopically• If large by laryngofissure• Biopsy to exclude malignancy specially if recurrent
Single papilloma
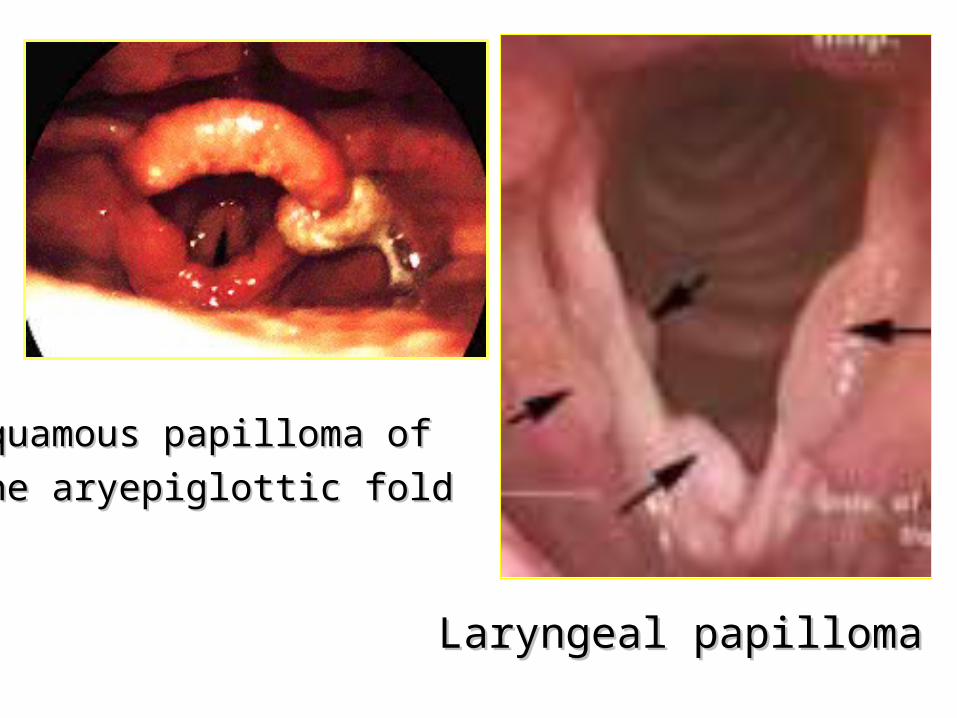
Laryngeal papillomaLaryngeal papilloma
Squamous papilloma of Squamous papilloma of
the aryepiglottic foldthe aryepiglottic fold
Multiple papillomas
• Infants and young children, rare in adults
• A virus may be responsible (HPV)
• Vocal cords are the usual site
• Hoarsness if vocal cords affected
• Dyspnoea may occur ---- tracheostomy
• Removed endoscopically by CO2 laser
• Spontaneous recovery in puberty may occur

Juvenile laryngeal papillomasJuvenile laryngeal papillomas
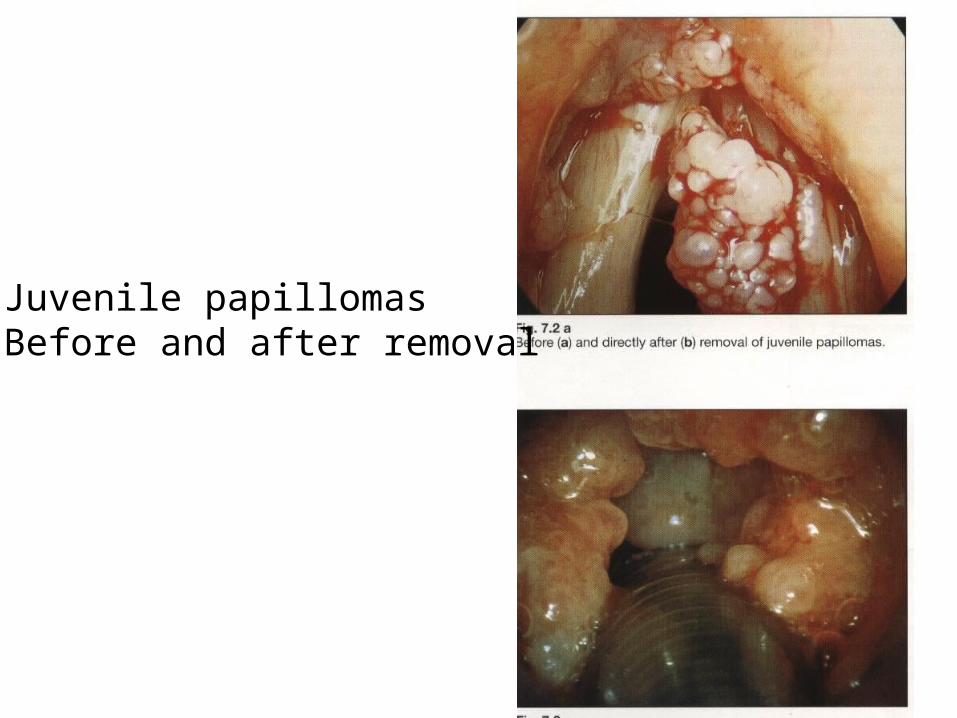
Juvenile papillomasBefore and after removal
1. Vascular neoplasms
2. Chondroma
3. Myogenic tumours
4. Fibroma
5. Lipoma
Mesodermal tumoursMesodermal tumours
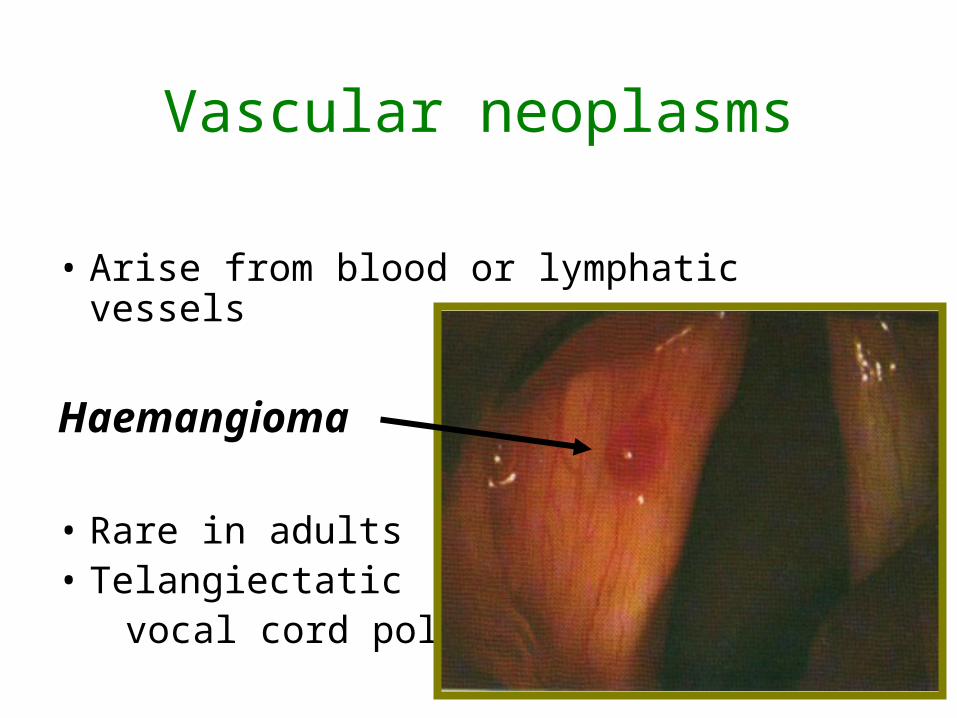
Vascular neoplasms
• Arise from blood or lymphatic vessels
Haemangioma
• Rare in adults• Telangiectatic vocal cord polyp

Chondroma• Arise from cartilages (Mostly cricoid)• More in men (40-70 years)
Clinical features
• Hoarsness and dyspnoea• Stridor (extention into subglottic space) • Dysphagia (extension into hypopharynx) • External swelling (cricoid ring or thyroid
cartilage)

• Indirect laryngoscopy reveals a smooth mass covered by intact mucosa
• Radiology shows calcific stippling or coarse irregular calcificatuon
• Biopsy specimens is unrepresentative, the tumour is hard and difficult to penetrate
• Surgery is the treatment of choice • Radiptherapy is of little value
Chondroma

Malignant Tumors
• 1% of all malignancies In UK
• More in men
• Predominantly of squamous pathology
• Interfere with function and emotion
• High cure rate 85%

Incidence
• Higher in urban than rural population
• Social and racial differences reflect different habits (tobacco and alcohol)

The International Union against Cancer (UICC) classified Ca larynx on anatomical bases
ClassificationClassification
20% 10% 70%

1 cm1 cm
Su
pra
glo
ttis
Su
pra
glo
ttis
EpilarynxEpilarynxSuprahyoid epiglottisSuprahyoid epiglottis
Aryepiglottic foldsAryepiglottic folds
SupraglottisSupraglottis infrahyoid epiglottis infrahyoid epiglottis
false cordsfalse cords
ventriclesventricles
Glottis Glottis True cord,ant&post comissureTrue cord,ant&post comissure
SubglottisSubglottis
UICC classification of Ca larynxUICC classification of Ca larynx

Glottis Glottis true cords true cords
anterior anterior commissure commissure
posterior posterior commissurecommissure

Aetiology • Unknown • Possibly related factors genetic and social factors male predominance racial predilection urban pollution tobacco and alcohol radiation asbestos occupational factors

Examination and diagnosis• Diagnosis will be made after consideration of:
1. History
2. Examination of the larynx
3. Examination of the neck
4. General examination of the patient
5. Radiology
6. Clinical investigations
7. Histological examination

1-Symptoms • Dysphonia progressive and unremitting• Cough and irritation in the throat (early) • Dyspnoea & stridor in advanced tumour,
specially in subglottic Ca • Pain more typical of supraglottic Ca, late and
uncommon • Referred otalgia may occur• Swelling of the neck or larynx (tumour or LN)• Haemoptysis (rare ,in lesions of the margin of
epiglottis) • Anorexia, cachexia or fetor are late symptoms• Progress of the disease

2-Examination of the larynx
examine for
• Focal abnormality • Vocal cord lesion • Mass • Mobility
examine by
• Indirect laryngoscopy (LA)• Flexible laryngoscopy (LA)• Direct laryngoscopy (GA) • Microlaryngoscopy (GA)

3-Examination of the neckA palpable neck mass could be due to:
1.Direct spread of the tumour.
2.Regional lymph nodes 2.Regional lymph nodes
metastasis. metastasis.
3.Enlarged thyroid lobe3.Enlarged thyroid lobe
which suggest which suggest invasioninvasion

4-General examination
• To identify metastasis e.g. to the liver
• To assess the overall physical status of the individual who is likely to need GA and biopsy, surgery, radiotherapy or chemotherapy

5-Radiological examination
• Chest X-ray
• Larynx Tomography
• CT and MRI of neck and larynx

Supraglottic tumourSupraglottic tumour
TomographyTomographyAPAP LateralLateral

Axial CT shows loss of pre-epiglottic fat by carcinomatous infiltrarionAxial CT shows loss of pre-epiglottic fat by carcinomatous infiltrarion
CT scan

Epiglotic tumorEpiglotic tumor (( laryngeal Ca. supraglotic typelaryngeal Ca. supraglotic type ))
MRI

MRI
Sagittal T2 image of Sagittal T2 image of supraglottic Casupraglottic Ca
Extension involves Extension involves the epiglottis :Ethe epiglottis :E
Loss of normal Loss of normal pr-epiglottic fat plane: pr-epiglottic fat plane: solid arrowssolid arrows
Tongue base Tongue base involvement : open involvement : open arrowarrow

Axial MRI showing tumour of the Rt. VCAxial MRI showing tumour of the Rt. VC
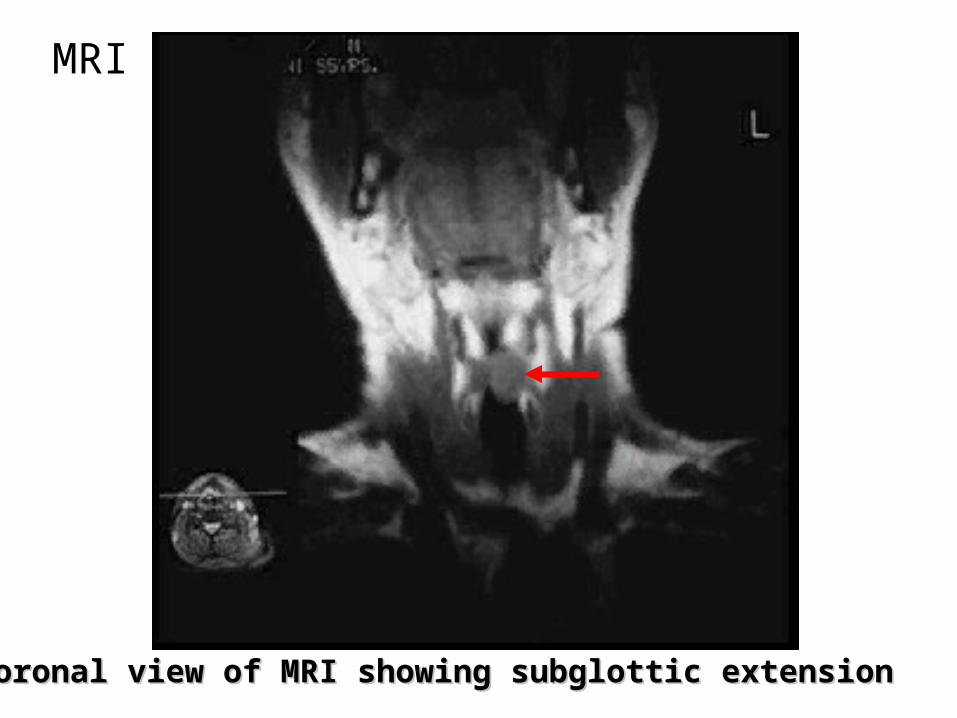
MRI
Coronal view of MRI showing subglottic extensionCoronal view of MRI showing subglottic extension

Sagittal view showing transglottic tumourSagittal view showing transglottic tumour
MRI

6-Clinical investigations
• Full hematological screen
• Biochemical profile including liver function tests and serum protein
• A urine screen for diabetes
• ECG

7-Histological examination
• Proof diagnosis of malignancy
• Type of the tumor
• Degree of differentiation

Diagnostic difficulties
• Negative biopsy
• Keratosis
• Previous radiation
• Miscellaneous conditions: chronic laryngitis, TB, Syphilis…

Pathology
1. Squmous cell carcinoma:
The vast majority of laryngeal malignant tumours.
• Verrucous carcinoma (Ackerman’s tumour):
A distinct variant of well differentiated squamous cell Ca is the

Glottic Ca
Origin :Origin : the free margin of the vocal cordsthe free margin of the vocal cords
Invasion & extensionInvasion & extension
anterior commissureanterior commissure
cartilage (Ossified more prone)cartilage (Ossified more prone)
arytenoid & posterior cricoarytenoid musclearytenoid & posterior cricoarytenoid muscle
vertical extension to the subglottis &/orvertical extension to the subglottis &/or supraglottis supraglottis
is more frequent than to the opposite sideis more frequent than to the opposite side

Cancer of the Lt true vocal cordCancer of the Lt true vocal cord

glottic CAglottic CA

cancer involving the true vocal cords and arytenoid. The cancer also extends onto the supraglottis

Impaired mobility :
superficial invasion of the thyroarytenoid muscle
Fixation of the vocal cords: by invasion of: - thyroarytenoid muscle - arytenoid cartilage - cricoid cartilage -cricoarytenoid joint
Glottic Ca

Supraglottic Ca
• Often involving both sides
• Seldom extend to the glottic region due to different embryological derivations and various lymphatic supplies

• thyroid cartilage
• pre-epiglottic space occur in 40% of supraglottic Ca and 70% of epiglottic Ca
• vallecula & base of the tongue
• Arytenoid
• Pyriform sinus
Supraglottic Ca
InvasionInvasion

Supraglottic CaSupraglottic Ca
Epiglottic tumpur
Tumour of Lt aryepiglottic fold
Tumour of Rt false cord

• Primary are rare
• Grow circumferentially and extensively
• Invasion of the vocal cords may lead to impairment of mobility and hoarsness
• Can spread through the cricothyroid membrane anteriorly or cricotracheal membrane posteriorly or invade the trachea caudally
Subglottic Ca

Subglottic CaSubglottic Ca

Lymph node involvement
• 18% had LN metastasis at the time of referral
Supraglottic ( 40% )
Glottic Ca ( 5% )
Subglottic Ca ( 13% )

• Few present with distant metastasis at the time of diagnosis
• 11% have distant metastasis, mostly in the lung ( 6.8% )
Distant metastasis

TNM classification
T:T: Primary tumourPrimary tumour
N: Nodal depositsN: Nodal deposits
M: MetastasisM: Metastasis

T T : : Primary tumourPrimary tumour
TXTX
T0T0
TisTis
Primary tumour can not be assesed
No evidence of primary tumour
Carcinoma insitu

T : Primary tumour
GlotticT1 limited / mobile a: one cord b: both cords
T2 extends to supra or subglottic /mobile
T3 cord fixation
T4 extends beyond
the larynx
Supra & subglottic
T1 limited / mobile cords
T2 extends to glottis/mobile
T3 cord fixation
T4 extends beyond the larynx

T1aT1a
Rt.VC Ca with normal mobilityRt.VC Ca with normal mobility
Glottic

T1bT1b Limited mobile both cordsLimited mobile both cords
Glottic

Glottic
T2 extends to supra or subglottic /mobile
large tumor on the left true vocal cord
and anterior false vocal cords (T2 Cancer)

cancer involving the true vocal cords and arytenoid.
The cancer also extends onto the supraglottis T2
Glottic

Subglottic
limited / mobile cords
T1T1
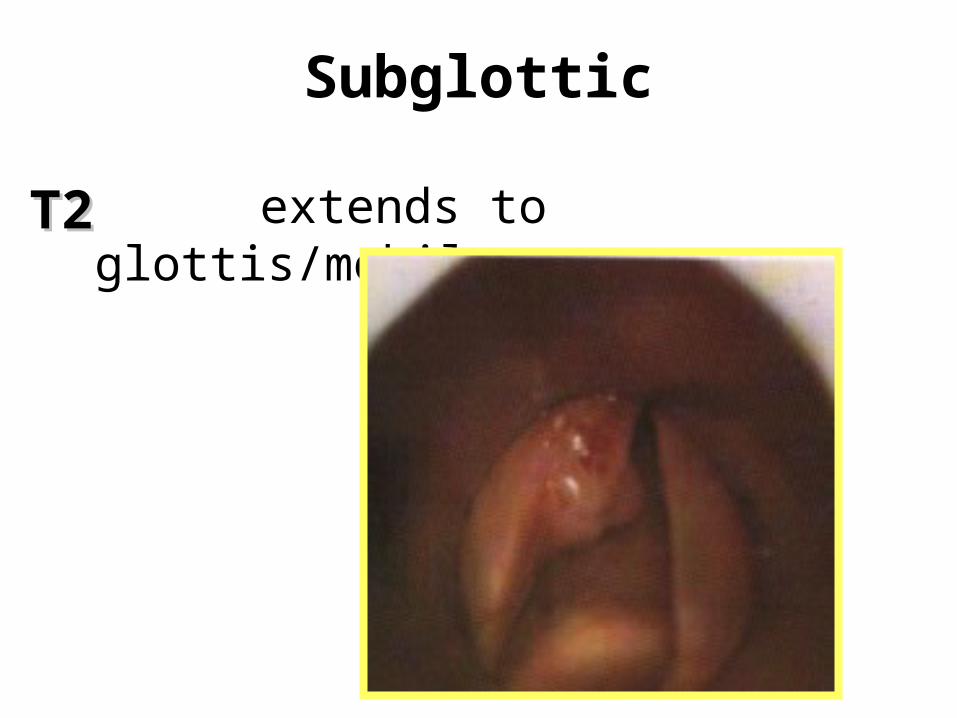
Subglottic
extends to glottis/mobileT2T2

Lt false cord Lt false cord tumourtumour
SupraglotticSupraglottic
T1T1 limited / mobile cords

T2T2
SupraglotticSupraglottic
Ca of the Rt. aryepiglottic foldCa of the Rt. aryepiglottic fold
Extends to glottisExtends to glottis
Moblie cordsMoblie cords

cord fixation
SupraglotticSupraglottic
T3T3
Ca of the Lt. arytenoidCa of the Lt. arytenoid

N: Nodal deposits
N1 ipsilateral movable
N2 contra or bilateral movable
N3 Fixed
No LN depositsNo LN depositsN0N0

M: Metastasis
M0 no metastasis
M1 metastasis
Stage 0 : Tis, N0 , M0Stage 1 : T1, N0 , M0Stage 2 : T2, N0 , M0Stage 3 : T3, N0 , M0 T1-T3, N1 , M0
Stage 4 : T4, N0/N1 , M0 Any T, N2/N3 , M0 Any T, Any N , M1
Staging

RehabilitationRehabilitation
TreatmentTreatment
curativecurative
No treatmentNo treatment PalliationPalliation

No treatment
• Those presenting in extremis
• who are no longer conscious of pain or distress
• Disseminated tumours cause their death without the primary tumour or regional disease causing symptoms
• 7-8% recieve no treatment

Palliation • The attempt to suppress the Ca and its
symptoms without expectation or intent to cure
• Palliation is used in late stages
• Includes: pain relief tracheostomy other surgery radiotherapy chemotherapy

Pain relief
• Pain is not common in Ca larynx
• combination methods including analgesics, radiation, surgery, and chemotherapy used for pain relief

Tracheostomy
• To relieve airway obstruction
It often provide a dilemma, as it just delay the inevitable death in a patient with incurable cancer

Other surgeries
Total laryngectomy
For pain control occasionally
Radical neck dissection
may remove a fungating or painful local lesion

Radiotherapy
• Commonly used for palliation• Can be applied locally and selectively• Radioactive implants of gold are useful for
local treatment

Chemotherapy
• No Ca larynx has been cured by drugs• Complete regression is rare• Partial response in 20%• In no way can be compared to
radiotherapy or surgery• Rather it is an alternative to analgesics• Has significant side effects and leads to
more suffering

Curative treatment
• Radiotherapy
• Surgery
• Chemotherapy
• Radiation is most effective where the tissues are well oxygenated.
• So it is most valuable in small lesions and when the vascular supply is undamaged, where it has not preceded by surgery
• Radiation is more applicable on the oxygenated periphery, while surgery could deal with the mass
RadiotherapyRadiotherapy

• Selection of cases:1. When cure is likely with preservation of function.2. When surgery is contraindicated or refused.
Chemotherapy before radiation increases the response.
RadiotherapyRadiotherapy

• Contraindicaitons
1. Active perichondritis
2. Cartilage invasion
3. Previous radiotherapy
RadiotherapyRadiotherapy

• Interstitial radiation
radioactive gold-198 grains can be inserted using a special gun in a pattern which can give a very high dose localized to nodes or nodules in the neck, with little damage to normal structures
RadiotherapyRadiotherapy

• Radiation reactions
1. Erythema or moist desquamation of the skin, may progress to necrosis
2. Perichondritis
3. Mucositis (Painful erythematous reaction)
reactions are minimized by the avoidance of smoking and alcohol.
RadiotherapyRadiotherapy

Recurrence after radiotherapyRecurrence after radiotherapy
Surgery
• Microlaryngeal Surgery
• Laser Surgery
• ExcisionalExcisional Surgery
Microendolaryngeal and laser surgery
• Carcinoma in situ can by treated by microsurgical excision and laser makes this easier
• Certain localized supraglottic lesions may be excised using a laser
Carbon dioxide laser is used

• Used with or without radiotherapy• Has risk of loss of voice, and protection of the
airway• Is more effective than radiotherapy in large
tumours and when there are secondary deposits in LN in the neck
• Partial resection of the larynx may maintain a near normal funcion with high cure rate
• Used after failure of radiotherapy
Excisional surgery

Selection of treatment

1. Keratosis & Carcinoma in situ in the glottis and supraglottis
2. Small tumours in the marginal zones (suprahyoid epiglottis, aryepiglottic folds, false cords)
Microendoscopic removal with or without laser

1. T1 & T2 lesions (Supraglottis and glottis )
2. T3 glottis
3. Subglottic tumours
4. Small or subclinical nodes
Radiotherapy

1. Supraglottic lesions arising from the base of the epiglottis and the false cords .
2. T2 lesions as alternative to radiotherapy
3. T3 & T4
4. Subglottic lesion as alternative to radiotherapy
5. Secondary nodal deposits
6. Other malignancies apart from squamous type all are treated by laryngectomy
Surgery
• This is to avoid tracheostomy when there is airway obstruction in laryngeal Ca
• Peristomal recurrence is more in those with tracheostomy who undergone laryngectomy
Emergency laryngectomy
Surgical techniques
• Vertical partial resectionVertical partial resection
• Horizontal partial resectionHorizontal partial resection
• Total resectionTotal resection
-With or without neck dissection-With or without neck dissection

Skin incision for laryngofissureSkin incision for laryngofissureRunning over the midportion of thyroid cartilage between st.cl.mastoid Running over the midportion of thyroid cartilage between st.cl.mastoid
musclesmuscles

Skin incisionSkin incision
Thyroid cartilageThyroid cartilage
Cricoid cartilageCricoid cartilage
cordectomycordectomy

Exposure of thyroid cartilage & cricothyroid membrane in the midlineExposure of thyroid cartilage & cricothyroid membrane in the midline
cordectomycordectomy

The perichondrium is exposed retracting the strap musclesThe perichondrium is exposed retracting the strap muscles
cordectomycordectomy

Elevation of the edges of external perichondriumElevation of the edges of external perichondrium
cordectomycordectomy
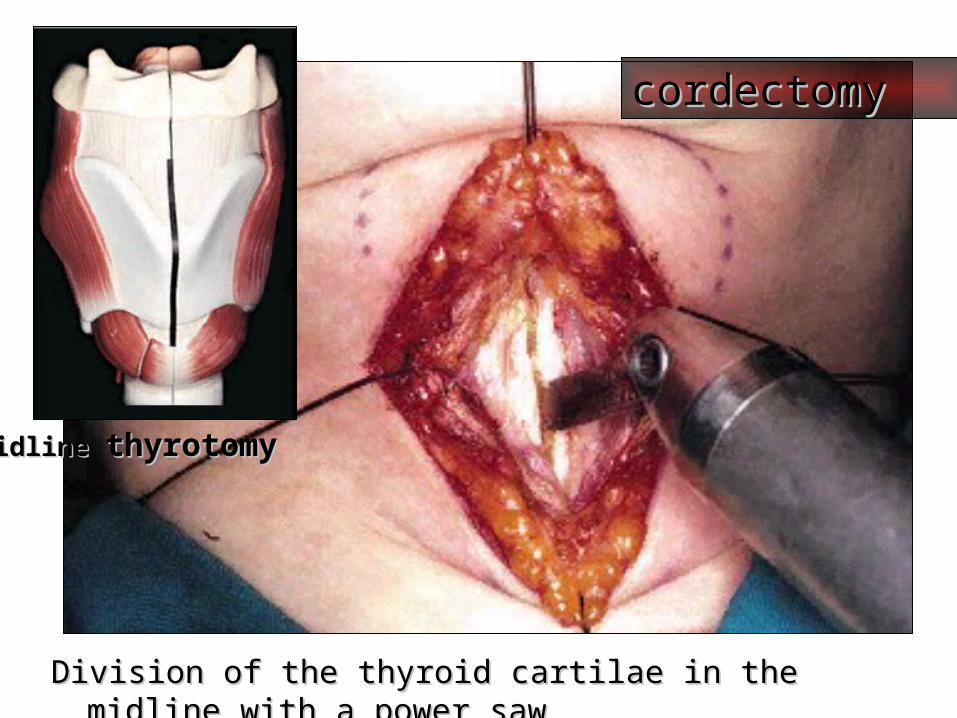
Midline Midline thyrotomythyrotomy
Division of the thyroid cartilae in the midline with a power sawDivision of the thyroid cartilae in the midline with a power saw
cordectomycordectomy

Thyroid alae retractedThyroid alae retracted
Endolarynx inspectedEndolarynx inspected
Extent of the tumour assesedExtent of the tumour assesed
VC removed from ventricle to VC removed from ventricle to
subglottis, lateral boundary of subglottis, lateral boundary of
resection is the internal perichondrium resection is the internal perichondrium
of tyroid ala of tyroid ala
cordectomycordectomy

Tumour of the Rt. VC is seen by retraction of thyroid laminaTumour of the Rt. VC is seen by retraction of thyroid lamina
Rt.VC tumourRt.VC tumour
cordectomycordectomy

Retraction of supraglottic larynxRetraction of supraglottic larynx
Rt.VC tumourRt.VC tumour
cordectomycordectomy

Line of incisionLine of incision
Excision with scissorsExcision with scissors
cordectomycordectomy

Reapproximated thyroid cartilageReapproximated thyroid cartilage
cordectomycordectomy

Suturing of the perichondriumSuturing of the perichondrium
cordectomycordectomy

Suturing of sternohyoid Suturing of sternohyoid
cordectomycordectomy

Suturing of platysmaSuturing of platysma
cordectomycordectomy
Closure of skinClosure of skin
cordectomycordectomy

The surgical specimenThe surgical specimen 1 year after surgery1 year after surgery
cordectomycordectomy

Management of LN metastasis
1. Observation for limited cancers
2. Palpable LN at presentation—Neck disection with/without Radiotherapy.
3. Prophylactic treatment—Neck dissection or radiotherapy.
4. Treatment of postoperative and post- irradiation LN

Thanks

















