12
4.811 TUR IS – TRANSURETHRAL RESECTION IN SALINE Review of clinical evidence for bipolar resection and plasma vaporization.

4.81
1
TURIS – TRANSURETHRAL RESECTION IN SALINE
Review of clinical evidence for bipolar resection and plasma vaporization.

2
TURIS – CLINICAL BENEFITS
Safety1
· Reduced risk of TUR syndrome2
· Minimized stimulation of obturator nerve
· Extended operations times – way beyond monopolar
· Improved teaching options
Bloodless
· Reduced perioperative blood loss due to safe bipolar hemostasis
· Plasma vaporization with the PlasmaButton provides continuous hemostasis3
· Enucleation technique allows for a potentially blood-free procedure
Time-saving4
· Self-cleaning effect of loop wire through plasma activation
· Faster post-operative recovery
· Potentially decreased catheterization times
The benefits of TURis
The TURis bipolar resection system provides an outstanding versatility for the treatment of benign prostatic hyperplasia. At
the same time, it maintains all the benefits of bipolar resection in saline. As of today, more than one million successful clinical
cases have proved the safety of the TURis 2.0 system.*
Please see the references on page 9. *Data on file
8.33
38.
330
8.34
1

3
Please see the references on page 9.
TURIS – BIPOLAR PROCEDURES
Loop resection – instant ignition and continuous
activation
· Three effect options for obtaining the desired coagulation
zone
· Smooth cutting and good pathological samples
· High tissue ablation rate5
· All benefits of TURis
· Plasma vaporization enables continuous and safe
hemostasis
· Short learning curve and fast and easy set-up, just as
simple as standard resection
· Clear and unobstructed view throughout the operation as
neither tissue chips nor laser impulses impair vision
· The PlasmaButton leads to a smooth post-operative tissue
surface
· Potential for providing transurethral vaporization on a
day-case basis
· A fraction of the cost of PVP
Transurethral enucleation – a bipolar alternative
The TUEB electrode enables the fast enucleation of larger
prostates without having to invest in additional laser
technology. Transurethral Enucleation with Bipolar (TUEB)
allows for potentially blood-free procedures and a gentle
enucleation of the prostate.
Plasma vaporization – from laser to plasma vaporization
8.32
88.
339
8.33
6
4.20
54.
208
8.59
5

4
Solid Liquid Gaseous Plasma
What is plasma?
Plasma is one of the four fundamental states of matter and is created by applying energy to a gas.
Molecules are ionized, thus turning the gas into a plasma. Due to its conductivity, the plasma allows the
energy to cross at lower energy levels. This effect leads to low operating temperatures and, therefore, less
thermal spread. Tissue is vaporized by a locally confined denaturation process, while surrounding tissue-
heating effects are minor. It appears yellow due to the sodium which is dissolved in the saline and –as of
today– more than one million successful clinical cases have proved the safety of the TURis 2.0 system.
Energy Energy Energy
Molecule Free charge carriers Free radicals
What is transurethral enucleation?
This revolutionary technique for the removal of the prostate utilizes
the natural anatomy by virtually peeling the prostate tissue out of
the capsule. The TUEB electrode’s wire loop is only used to locate
the layers and coagulate any bleeding – should this occur. Once
the right layers have been located, the black runner is used to
gently peel off the prostate lobes as a whole. The lobes are then
pushed into the bladder, where they are cut and eventually
removed. TUEB potentially produces the same functional results
as the current standard treatment while reducing operating times
for large prostates and – at the same time – keeping intra-
operative blood loss to a minimum.
TURIS – TECHNOLOGY AND TECHNIQUES
4.21
3

5
TURis: The gold standard for TUR-P and TUR-B
The TURis bipolar resection system differs from monopolar resection in that the tissue effect takes place
between two electrodes that are part of the same device. The active and return electrode are within the
resectoscope, forming a bipolar electrosurgical system. Due to the conductive saline, only a very small fraction
of the current passes through the tissue, and no neutral electrode is required. In TURis, HF current is used to
create a plasma corona. After plasma ignition, cutting or vaporization can be performed.
The ESG-400 power curve with optimized energy output control – energy is immediately reduced after ignition
Power (W)
Time (t)
Plasma ignition
TURIS – TECHNICAL PRINCIPLE
ESG-400 – intelligent HF technology
The TURis bipolar system is powered by the ESG-400 HF generator which is equipped with various safety
features such as automated saline detection and leakage protection sensor to permanently ensure the highest
degree of safety for the user and the patient.
4.81
04.
812

6
BIPOLAR PLASMA VERSUS MONOPOLAR: REVIEW OF EVIDENCE
significantly. Irrigation and catheterization duration was
significantly longer with M-TURP (WMD: 8.75 h; 95% CI, 6.8–10.7
and WMD: 21.77 h; 95% CI, 19.22–24.32; p < 0.00001,
respectively). Inferences for hospitalization duration could not be
made. PlasmaKinetic TURP showed an improved safety profile.
Data on TUR in saline (TURis) are not yet mature to permit safe
conclusions.
Conclusions:
No clinically relevant differences in short-term efficacy
exist between the two techniques, but B-TURP is
preferable due to a more favorable safety profile (lower
TUR syndrome and clot retention rates) and shorter
irrigation and catheterization duration. Well-designed
multicentric/international RCTs with long-term follow-up
and cost analysis are still needed.
Keywords:
Benign prostatic hyperplasia, Bipolar, Electrosurgery, Meta-
analysis, PlasmaKinetic, Prostate, Randomized controlled trial,
Review, Saline, Transurethral resection of prostate
European Urology 56 (2009) 798-809
Bipolar versus Monopolar Transurethral Resection of the
Prostate: A Systematic Review and Meta-analysis of
Randomized Controlled Trials
Charalampos Mamoulakisa, Dirk T. Ubbinkb, Jean J.M.C.H. de
la Rosettea,*
Context:
Incorporation of bipolar technology in transurethral resection
(TUR) of the prostate (TURP) potentially offers advantages over
monopolar TURP (M-TURP).
Objective:
To evaluate the evidence by a meta-analysis, based on
randomized controlled trials (RCTs) comparing bipolar TURP
(B-TURP) with M-TURP for benign prostatic obstruction. Primary
end points included efficacy (maximum flow rate [Qmax],
International Prostate Symptom Score) and safety (adverse
events). Secondary end points included operation time and
duration of irrigation, catheterization, and hospitalization.
Evidence acquisition:
Based on a detailed, unrestricted strategy, the literature was
searched up to February 19, 2009, using Medline, Embase,
Science Citation Index, and the Cochrane Library to detect all
relevant RCTs. Methodological quality assessment of the trials
was based on the Dutch Cochrane Collaboration checklist.
Meta-analysis was performed using Review Manager 5.0.
Evidence synthesis:
Sixteen RCTs (1406 patients) were included. Overall trial quality
was low (eg, allocation concealment and blinding of outcome
assessors were poorly reported). No clinically relevant differences
in short-term (12-mo) efficacy were detected (Qmax: weighted mean
difference [WMD]: 0.72 ml/s; 95% confidence interval [CI],
0.08–1.35; p = 0.03). Data on follow-up of >12 mo are scarce for
B-TURP, precluding long-term efficacy evaluation. Treating 50
patients (95% CI, 33–111) and 20 patients (95% CI, 10–100) with
B-TURP results in one fewer case of TUR syndrome (risk
difference [RD]: 2.0%; 95% CI, 0.9–3.0%; p = 0.01) and one fewer
case of clot retention (RD: 5.0%; 95% CI, 1.0–10%; p = 0.03),
respectively. Operation times, transfusion rates, retention rates
after catheter removal, and urethral complications did not differ
© 2009 European Association of Urology. Published by Elsevier B.V. All rights reserved.
a Department of Urology, Academic Medical Center, University of Amsterdam,
Amsterdam, The Netherlands
b Department of Quality Assurance and Process Innovation and Surgery, Academic
Medical Center, University of Amsterdam, Amsterdam, The Netherlands
* Corresponding author. Department of Urology (G4-105), AMC University Hospital,
Meibergdreef 9, 1105 AZ Amsterdam, The Netherlands. Tel. +31 20 5666030;
Fax: +31 20 5669585. E-mail address: [email protected]
(J.J.M.C.H. de la Rosette).
Please see the references on page 9.

7
Summary of results
B-TURP/plasma is equally as effective as M-TURP in improving the flow rate at 12 months. (WMD: 0.72 ml/s; 95% CI, 0.08–1.35; p=0.03)
Nuhoglu 2006 (n=57)6
Lin 2006 (n=40)7
Seckiner 2006 (n=48)8
De Sio 2006 (n=70)9
Ho 2007 (n=100)10
Erturhan 2007 (n=240)11
Iori 2008 (n=53)12
Bhansali 2009 (n=67)13
Qmax at 12 months (ml/s)
0 5 10 15 20 25 30
M-TURP B-TURP
B-TURP/plasma involves significantly shorter catheterization time than M-TURP. (I2=0.98; sensitivity analysis on subgroup; p<0.00001)
M-TURP B-TURP
Yang 2004 (n=117)14
Singh 2005 (n=60)15
Seckiner 2006 (n=48)8
Kim 2006 (n=50)16
De Sio 2006 (n=70)9
Abascal 2006 (n=45)17
Nuhoglu 2006 (n=57)6
Patankar 2006 (n=103)18
Michielsen 2007 (n=238)19
Erturhan 2007 (n=240)11
Rose 2007 (n=72)20
Iori 2008 (n=53)12
Bhansali 2009 (n=64)13
Catheterization time (hours)
0 20 40 60 80 100 120
B-TURP/plasma shows significantly lower occurrence of TUR syndrome than M-TURP. (RD: 2%; 95% CI, 0–3%; p=0.01)
B-TURP/plasma shows similar long-term urethral complication to M-TURP at 12 months. (RD: 0%; 95% CI, -2–1%; p=0.58)
B-TURP/plasma shows significantly lower occurrence of clot retention M-TURP. (RD: 0%; 95% CI, 1–10%; p=0.03)
Acronyms:
WMD: weighted mean differenceCI: confidence intervalI2: heterogeneityRD: risk difference
M-TURP B-TURP
Events Patient number
Events Patient number
Yang 200414 1 59 0 58 Singh 200515 0 30 0 30De Sio 20069 3 35 0 35Abascal 200617 0 21 0 24Akcayoz 200621 0 21 0 21Patankar 200618 0 51 0 52Kim 200616 0 25 0 25Nuhoglu 20066 0 30 0 27Seckiner 20068 0 24 0 24Erturhan 200711 2 120 0 120Rose 200720 0 34 0 38Michielsen 200719 1 120 0 118Ho 200710 2 52 0 48Iori 200812 0 26 0 27Bhansali 200913 4 33 0 34
Total 13 681 0 681
M-TURP B-TURP
Events Patient number
Events Patient number
Lin 20067 1 18 0 22Patankar 200618 2 51 0 52De Sio 20069 4 35 2 35Ho 200710 2 52 3 48Michielsen 200719 6 120 4 118Erturhan 200711 17 120 2 120Iori 200812 5 26 1 27
Total 37 422 12 422
Please see the references on page 9. The figures and tables were graphically adapted by Olympus. The content has not been changed.
M-TURP B-TURP
Events Patient number
Events Patient number
Urethral stricture
Nuhoglu 20066 0 26 0 24
Seckiner 20068 1 21 2 23
Erturhan 200711 2 120 2 120
Ho 200710 1 52 3 48
Total 4 219 7 215
Bladder neck contracture
Lin 20067 1 18 0 22
De Sio 20069 1 35 1 35
Nuhoglu 20066 0 26 0 24
Erturhan 200711 1 120 0 120
Iori 200812 1 26 1 27
Total 4 225 2 228
Meatal stenosis
Nuhoglu 20066 0 26 1 24
Erturhan 200711 2 120 3 120
Total 2 146 4 144
Cumul. total 10 590 13 587

8
GUIDELINE RECOMMENDATIONS
Summary B-TURP/plasma
· B-TURP is the most widely and thoroughly investigated
alternative to M-TURP.
· Available evidence to date includes 33 RCTs with 3,601
randomized patients in total.
· Three meta-analyses concluded no different efficacy and
preferred safety profile of B-TURP when compared with M-TURP
up to 12 months.
· To date, seven RCTs have mid-term follow-up duration between
18 to 60 months.
· Mid-term results of up to five years show comparable results of
B-TURP in efficacy and safety when compared with M-TURP.
· No individual RCT favors M-TURP.
Summary laser
· Only three RCTs to date provide sufficient follow-up data for 12
months.
· The longest RCT for the 80W KTP laser has a follow-up of only
12 months.
· The longest RCT for the 120W HPS laser has a 36-month
follow-up, but with inferior results in reduction of PSA level and
prostate volume when compared with TURP; the reoperation rate
was significantly higher with PVP.
· No RCTs have been published on the 180W GreenLight laser.
Please see the references on page 9. The figures and tables were graphically adapted by Olympus. The content has not been changed.
TURP/B-TURP LE GR
M-TURP is the current surgical standard procedure
for men with prostate sizes of 30–80 ml and
bothersome moderate-to-severe LUTS secondary of
BPO. M-TURP provides subjective and objective
improvement rates superior to medical or minimally
invasive treatments.
1a A
B-TURP achieves short- and midterm results
comparable with M-TURP.
1a A
B-TURP has a more favorable perioperative safety
profile compared with M-TURP.
1a A
Laser (GreenLight) LE GR
HoLEP and 532-nm laser vaporisation of the
prostate are alternatives to TURP in men with
moderate-to-sever LUTS due to BPO leading to
immediate, objective, and subjective improvements
comparable with TURP.
1a A
The intermediate-term functional results of 532-nm
laser vaporisation of the prostate are comparable
with TURP.
1b A
532-nm laser vaporization should be considered in
patients receiving anticoagulant medication or with a
high cardiovascular risk.
3 B
Level of evidence Type of evidence
1a Evidence obtained from meta-analysis of randomised trials
1b Evidence obtained from at least one randomised trial
3 Evidence obtained from well-designed nonexperimental studies, such as comparative or correlation studies and case reports
Grade Recommendation
A Based on clinical studies of good quality and consistency addressing the specific recommendations and including at least one randomised trial
B Based on well-conducted clinical studies but without randomised clinical trials
EAU guideline 201322 – Transurethral Resection of the Prostate (TURP) and Transurethral
Incision of the Prostate (TUIP)
To put it in a nutshell, B-TURP/plasma has -according to the most recent EAU 2013 guideline on prostate
treatment- equivalent clinical benefit to M-TURP referenced in multiple systematic reviews, based on RCTs.
Moreover, B-TURP/plasma is preferable due to a more favorable safety profile compared with M-TURP. Also,
B-TURP has higher level of evidence and grades of recommendation when compared with laser vaporization.

9
Please see the references on page 9.
Debate over the evidence: B-TURP/plasma has the best available evidence to date (Quotes from Mamoulakis et al. 201323).
Regarding the debate about bipolar transurethral resection of the prostate (B-TURP) versus monopolar
transurethral resection of the prostate (M-TURP), the fact is that we currently have >30 RCTs (>3500
patients) and three recent RCT-based meta-analyses [5]. Indisputably, B-TURP is presently the
most widely used and thoroughly investigated alternative to M-TURP [6].
Pooled results are awaited. However, it should be stressed that no individual RCT favors M-TURP in any
aspect. More than half favor B-TURP in some of the outcomes mentioned above, and the rest
show no difference. Having seven RCTs currently at hand with a follow-up >12 mo, we have
reached acceptable durations to judge the adequacy of B-TURP efficacy and safety comparability with
the predecessor in time. Regarding economic issues, we are still unable to argue decisively.
But can we ignore this ample evidence just because ‘‘the overall quality is not the best,’’ without being
prone to bias? If yes, then what can we infer from much less data on other alternatives to
M-TURP, such as lasers, for which evidence is based on fewer trials with similar methodological
limitations [2]? High-quality international multicenter RCTs are always welcomed; in the modern era of
evidence-based urology, there will always be ‘‘a plea for more.’’ Nevertheless, there comes a time when
we have to decide based on the best available evidence. This is the case for B-TURP versus
M-TURP. Definitely we can decide, and it’s about time!
10
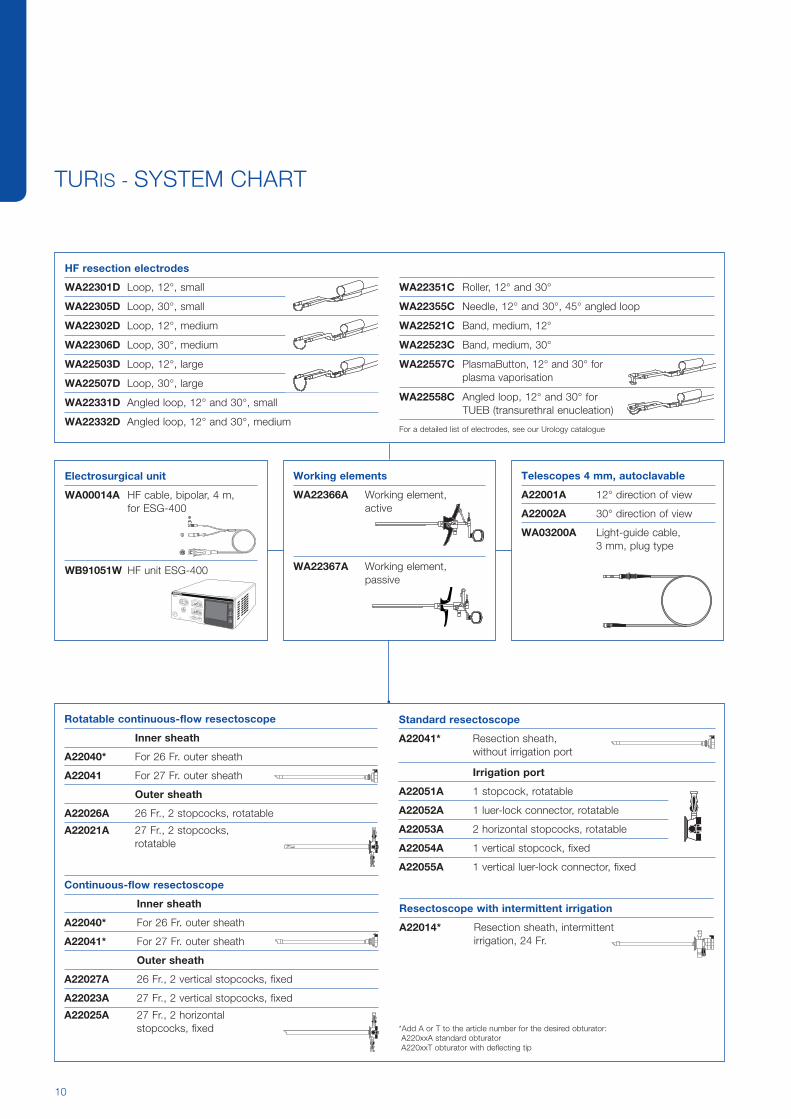
TURIS - SYSTEM CHART
Rotatable continuous-flow resectoscope
Inner sheath
A22040* For 26 Fr. outer sheath
A22041 For 27 Fr. outer sheath
Outer sheath
A22026A 26 Fr., 2 stopcocks, rotatable
A22021A 27 Fr., 2 stopcocks, rotatable
Telescopes 4 mm, autoclavable
A22001A 12° direction of view
A22002A 30° direction of view
WA03200A Light-guide cable, 3 mm, plug type
Continuous-flow resectoscope
Inner sheath
A22040* For 26 Fr. outer sheath
A22041* For 27 Fr. outer sheath
Outer sheath
A22027A 26 Fr., 2 vertical stopcocks, fixed
A22023A 27 Fr., 2 vertical stopcocks, fixed
A22025A 27 Fr., 2 horizontal stopcocks, fixed
Standard resectoscope
A22041* Resection sheath, without irrigation port
Irrigation port
A22051A 1 stopcock, rotatable
A22052A 1 luer-lock connector, rotatable
A22053A 2 horizontal stopcocks, rotatable
A22054A 1 vertical stopcock, fixed
A22055A 1 vertical luer-lock connector, fixed
Artikel-NR.
ILL-Name:
Maßstab:
Datum Erstellung:
Datum Änderung: von: von: Artikel-Bezeichnung:
Lubert 13.12.01
A22014A/T.ILL
Resectoscope with intermittent irrigation
A22014* Resection sheath, intermittent irrigation, 24 Fr.
*Add A or T to the article number for the desired obturator: A220xxA standard obturator A220xxT obturator with deflecting tip
HF resection electrodes
WA22301D Loop, 12°, small
WA22305D Loop, 30°, small
WA22302D Loop, 12°, medium
WA22306D Loop, 30°, medium
WA22503D Loop, 12°, large
WA22507D Loop, 30°, large
WA22331D Angled loop, 12° and 30°, small
WA22332D Angled loop, 12° and 30°, medium For a detailed list of electrodes, see our Urology catalogue
WA22351C Roller, 12° and 30°
WA22355C Needle, 12° and 30°, 45° angled loop
WA22521C Band, medium, 12°
WA22523C Band, medium, 30°
WA22557C PlasmaButton, 12° and 30° for plasma vaporisation
WA22558C Angled loop, 12° and 30° for TUEB (transurethral enucleation)
Working elements
WA22366A Working element, active
WA22367A Working element, passive
Artikel-NR.
ILL-Name:
Maßstab:
DatumErstellung:
DatumÄnderung:
von: von:
Artikel-Bezeichnung:
Sperlich
15.3.06
WA22367A_fly.eps
Artikel-NR.
ILL-Name:
Maßstab:
DatumErstellung:
DatumÄnderung:
von: von:
Artikel-Bezeichnung:
Lubert
15.3.06
WA22366A.eps
Artikel-NR.
ILL-Name:
Maßstab:
DatumErstellung:
DatumÄnderung:von: von:Artikel-Bezeichnung:
Lubert21.9.01
A22026A.ILL
Artikel-NR.
ILL-Name:
Maßstab:
DatumErstellung:
DatumÄnderung:von: von:Artikel-Bezeichnung:
Lubert13.12.01
A22040A.ILL
Artikel-NR.
ILL-Name:
Maßstab:
DatumErstellung:
DatumÄnderung:von: von:Artikel-Bezeichnung:
Lubert13.12.01
A22040A.ILL
Artikel-NR.
ILL-Name:
Maßstab:
DatumErstellung:
DatumÄnderung:von: von:Artikel-Bezeichnung:
Lubert26.9.01
A22041A.ILL
Artikel-NR.
ILL-Name:
Maßstab:
DatumErstellung:
DatumÄnderung:von: von:Artikel-Bezeichnung:
Lubert21.9.01
A22027A.ILL
MONOPOLAR 1
MONOPOLAR 2
NEUTRAL
FCQM
UNIVERSAL
BIPOLAR
ESG-400
SELECTPROCEDURE
FOOTSWITCH
MENU
Electrosurgical unit
WA00014A HF cable, bipolar, 4 m, for ESG-400
WB91051W HF unit ESG-400
Artikel-NR.
ILL-Name:
Maßstab:
DatumErstellung:
DatumÄnderung:von: von:Artikel-Bezeichnung:
Lubert27.9.01
A22051A.ILL

11
REFERENCES
6 Nuhoglu B, Ayyildiz A, Karagüzel E, et al. Plasmakinetic prostate resection in the treatment of benign prostate hyperplasia: results of one-year follow-up. Int J Urol 2006; 13:21–4.
7 Lin MS, Wu JC, Hsieh HL, et al. Comparison between monopolar and bipolar TURP in treating benign prostatic hyperplasia: one-year report. Mid-Taiwan J Med 2006; 11:143–8.
8 Seckiner I, Yesilli C, Akduman B, et al. A prospective randomized study for comparing bipolar plasmakinetic resection of the prostate with standard TURP. Urol Int 2006; 76:139–43.
9 de Sio M, Autorino R, Quarto G, et al. Gyrus bipolar versus standard monopolar transurethral resection of the prostate: a randomized prospective trial. Urology 2006; 67:69–72.
10 Ho HSS, Yip SKH, Lim KB, et al. A prospective randomized study comparing monopolar and bipolar transurethral resection of prostate using transurethral resection in saline (TURIS) system. Eur Urol 2007; 52:517–24.
11 Erturhan S, Erbagci A, Seckiner I, et al. Plasmakinetic resection of the prostate versus standard transurethral resection of the prostate: a prospective randomized trial with 1-year follow-up. Prostate Cancer Prostatic Dis 2007; 10:97–100.
12 Iori F, Franco G, Leonardo C, et al. Bipolar transurethral resection of prostate: clinical and urodynamic evaluation. Urology 2008; 71: 252–5.
13 Bhansali M, Patankar S, Dobhada S, et al. Management of large (>60 g) prostate gland: PlasmaKinetic Superpulse (bipolar) versus conventional (monopolar) transurethral resection of the prostate. J Endourol 2009; 23:141–6.
14 Yang S, Lin WC, Chang HK, et al. Gyrus plasmasect: is it better than monopolar transurethral resection of prostate? Urol Int 2004; 73: 258–61.
15 Singh H, Desai MR, Shrivastav P, et al. Bipolar versus monopolar transurethral resection of prostate: randomized controlled study. J Endourol 2005; 19:333–8.
16 Kim JY, Moon KH, Yoon CJ, et al. Bipolar transurethral resection of the prostate: A comparative study with monopolar transurethral resection. Korean J Urol 2006; 47:493–7.
17 Abascal Junquera JM, Cecchini Rosell L, Salvador Lacambra C, et al. Bipolar versus monopolar transurethral resection of the prostate: preoperative analysis of the results. Actas Urol Esp 2006; 30:661–6.
References of page 7:
References of page 2:
References of page 3: References of page 8:
References of page 9:
1 Puppo P, Bertolotto F, Introini C, et al. Bipolar transurethral resection in saline (TURis): outcome and complication rates after the first 1000 cases. J Endourol. 2009 Jul; 23(7):1145-9
2 Michielsen DP, Debacker T, De Boe V, et al. Bipolar transurethral resection in saline--an alternative surgical treatment for bladder outlet obstruction? J Urol. 2007 Nov; 178(5):2035-9
3 Geavlete B, Stanescu F, Moldoveanu C, et al. Continuous vs conventional bipolar plasma vaporisation of the prostate and standard monopolar resection: a prospective, randomised comparison of a new technological advance. BJU Int. 2013 Jun 13.
4 Fagerström T, Nyman CR, Hahn RG. Complications and clinical outcome 18 months after bipolar and monopolar transurethral resection of the prostate. J Endourol. 2011 Jun; 25(6):1043-9
5 Fagerström T, Nyman CR, Hahn RG. Degree of vaporization in bipolar and monopolar resection. J Endourol. 2012 Nov; 26(11):1473-7
22 Oelke M, Bachmann A, Descazeaud A, et al. EAU Guidelines on the Treatment and Follow-up of Non-neurogenic Male Lower Urinary Tract Symptoms Including Benign Prostatic Obstruction. European Urology 64, 2013; 118-140.
23 Mamoulakis C, Schulze M, Skolarikos A, et al. Best Available Evidence in 2012 on Bipolar Versus Monopolar Transurethral Resection of the Prostate for Benign Prostatic Obstruction: It’s About Time to Decide! Eur Urol 2013; 63:679–80.
[2] Bachmann A, Muir GH, Wyler SF, et al. Surgical benign prostatic hyperplasia trials: the future is now! Eur Urol 2013; 63:677–9.
[5] Mamoulakis C, Sofras F, de la Rosette J, et al. Bipolar versus monopolar transurethral resection of the prostate for lower urinary tract symptoms secondary to benign prostatic obstruction. Cochrane Collaboration, John Wiley & Sons; 2012. http://dx.doi.org/10.1002/14651858.CD009629.
[6] Oelke M, Bachmann A, Descazeaud A, et al. members of the European Association of Urology Guidelines Office. Guidelines on the management of male lower urinary tract symptoms (LUTS), incl., (BPO) BPO. Paper presented at: 27th European Association of Urology Annual Congress; February 24–28, 2012; Paris, France.
18 Patankar S, Jamkar A, Dobhada S, et al. PlasmaKinetic Superpulse transurethral resection versus conventional transurethral resection of prostate. J Endourol 2006; 20:215–9.
19 Michielsen DP, Debacker T, De Boe V, et al. Bipolar transurethral resection in saline-an alternative surgical treatment for bladder outlet obstruction? J Urol 2007; 178:2035–9.
20 Rose A, Suttor S, Goebell PJ, et al. Transurethral resection of bladder tumors and prostate enlargement in physiological saline solution (TURIS). A prospective study [in German]. Urologe A 2007; 46:1148–50.
21 Akcayoz M, Kaygisiz O, Akdemir O, et al. Comparison of transurethral resection and plasmakinetic transurethral resection applications with regard to fluid absorption amounts in benign prostate hyperplasia. Urol Int 2006; 77: 143–7.

E0
4921
39
· 2.
00
0 ·
04/
14 ·
PR
TURIS – TRANSURETHRAL RESECTION IN SALINE
Specifications, design, and accessories are subject to change without any notice or obligation on the part of the manufacturer.
Postbox 10 49 08, 20034 Hamburg, GermanyWendenstrasse 14–18, 20097 Hamburg, GermanyPhone: +49 40 23773-0, Fax: +49 40 237765www.olympus-europa.com





![[XLS] 7-10... · Web view1 0 0 0 2 0 0 0 3 0 0 0 4 0 0 0 5 0 0 0 6 0 0 0 7 0 0 0 8 0 0 0 9 0 0 0 10 0 0 0 11 0 0 0 12 0 0 0 13 0 0 0 14 0 0 0 15 0 0 0 16 0 0 0 17 0 0 0 18 0 0 0 19](https://static.documents.pub/doc/80x56/5ae8a6607f8b9a29049069b5/xls-7-10web-view1-0-0-0-2-0-0-0-3-0-0-0-4-0-0-0-5-0-0-0-6-0-0-0-7-0-0-0-8-0.jpg)











