Abstract A 55-year-old man who was diagnosed as having type 1 diabetes mellitus (DM) at the age of 50 years was started on insulin therapy. At 54 years old of age, he sud- denly developed complex partial seizures, which fre- quently occurred despite intensive anti-epileptic drug therapy. Neurological examination on admission revealed hyporeflexia in bilateral upper and lower extremities without any muscle rigidity, painful spasm or cerebellar ataxia. Laboratory examination showed poor glycemic control with increased glycated hemoglobin levels. Positive anti-thyroglobulin antibodies and anti-thyroid peroxidase (TPO) antibodies and slight elevation of TSH levels are consistent with subclinical hypothyroidism due to Hashimoto’s thyroiditis. A high titer of anti-glutamic acid decarboxylase (GAD) antibodies was detected in the patient’s serum and cerebrospinal fluid (CSF). Electro- encephalography showed temporal spikes, consistent with complex partial seizure. This is a very rare case pre- senting with concomitant type 1 diabetes and drug- resistant epilepsy associated with high titers of circulating and CSF anti-GAD antibodies. (Internal Medicine 44: 1174–1177, 2005) Key words: type 1 diabetes mellitus, drug-resistant epilepsy, anti-glutamic acid decarboxylase antibodies Introduction Glutamic acid decarboxylase (GAD) is the enzyme that catalyses the conversion of glutamic acid into -amino- butyric acid (GABA), one of the classical neurotransmitters with neuroinhibitory function (1). GAD is present not only in GABAnergic neurons, but also in pancreatic -cells, testis, liver, kidney, and adrenal glands (2, 3). Anti-GAD antibodies are now considered to be a marker of type 1 diabetes, since they can be found in the sera of the majority of individuals with preclinical and early phase type 1 diabetes (4, 5). Although GAD has initially been regarded as an important -cell antigen able to induce type 1 diabetes in non-obese diabetic (NOD) mice, its pathogenic role in the initiation of type 1 diabetes remains controversial (6). Anti- GAD antibodies are also detected in Stiff-person syndrome (SPS), a rare neurological disorder characterized by muscle rigidity and painful spasms, implicating their involvement in neurological diseases in central nervous system (CNS) (7). We report herein a very rare case presenting with type 1 dia- betes and drug-resistant epilepsy with a high titer of anti- GAD antibodies in serum and cerebrospinal fluid (CSF). Case Report A 50-year-old man noticed polydipsia, polyuria, and weight loss in May 1999. He was found to have hyperglyce- mia and impaired insulin secretion at another hospital, and was diagnosed as type 1 diabetes in August 1999. He also had respiratory tract infection due to bronchiectasis, and in- sulin treatment was started. His glycemic control was poor: fasting plasma glucose levels fluctuated between 50–500 mg/dl with increased glycated hemoglobin levels (HbA1c: 10–11%). He suddenly developed a complex partial seizure in August 2003, which frequently occurred thereafter, re- gardless of an intensive anti-epileptic drug therapy (Fig. 1). Internal Medicine Vol. 44, No. 11 (November 2005) 1174 Type 1 Diabetes Mellitus and Drug-resistant Epilepsy: Presence of High Titer of Anti-Glutamic Acid Decarboxylase Autoantibodies in Serum and Cerebrospinal Fluid Takanobu YOSHIMOTO, Masaru DOI, Nozomi FUKAI, Hajime IZUMIYAMA, Takehiko WAGO, Isao MINAMI, Isao UCHIMURA and Yukio HIRATA □ CASE REPORT □ From the Department of Clinical and Molecular Endocrinology Tokyo Medical and Dental University Graduate School, Tokyo Received for publication February 24, 2005; Accepted for publication July 11, 2005 Reprint requests should be addressed to Dr. Yukio Hirata, the Department of Clinical and Molecular Endocrinology, Tokyo Medical and Dental University Graduate School, 1-5-45 Yushima, Bunkyo-ku, Tokyo 113-8519
Transcript
Abstract
A 55-year-old man who was diagnosed as having type1 diabetes mellitus (DM) at the age of 50 years wasstarted on insulin therapy. At 54 years old of age, he sud-denly developed complex partial seizures, which fre-quently occurred despite intensive anti-epileptic drugtherapy. Neurological examination on admission revealedhyporeflexia in bilateral upper and lower extremitieswithout any muscle rigidity, painful spasm or cerebellarataxia. Laboratory examination showed poor glycemiccontrol with increased glycated hemoglobin levels.Positive anti-thyroglobulin antibodies and anti-thyroidperoxidase (TPO) antibodies and slight elevation of TSHlevels are consistent with subclinical hypothyroidism dueto Hashimoto’s thyroiditis. A high titer of anti-glutamicacid decarboxylase (GAD) antibodies was detected in thepatient’s serum and cerebrospinal fluid (CSF). Electro-encephalography showed temporal spikes, consistentwith complex partial seizure. This is a very rare case pre-senting with concomitant type 1 diabetes and drug-resistant epilepsy associated with high titers ofcirculating and CSF anti-GAD antibodies.(Internal Medicine 44: 1174–1177, 2005)
Glutamic acid decarboxylase (GAD) is the enzyme that
catalyses the conversion of glutamic acid into �-amino-butyric acid (GABA), one of the classical neurotransmitterswith neuroinhibitory function (1). GAD is present not only inGABAnergic neurons, but also in pancreatic �-cells, testis,liver, kidney, and adrenal glands (2, 3).
Anti-GAD antibodies are now considered to be a markerof type 1 diabetes, since they can be found in the sera of themajority of individuals with preclinical and early phase type1 diabetes (4, 5). Although GAD has initially been regardedas an important �-cell antigen able to induce type 1 diabetesin non-obese diabetic (NOD) mice, its pathogenic role in theinitiation of type 1 diabetes remains controversial (6). Anti-GAD antibodies are also detected in Stiff-person syndrome(SPS), a rare neurological disorder characterized by musclerigidity and painful spasms, implicating their involvement inneurological diseases in central nervous system (CNS) (7).We report herein a very rare case presenting with type 1 dia-betes and drug-resistant epilepsy with a high titer of anti-GAD antibodies in serum and cerebrospinal fluid (CSF).
Case Report
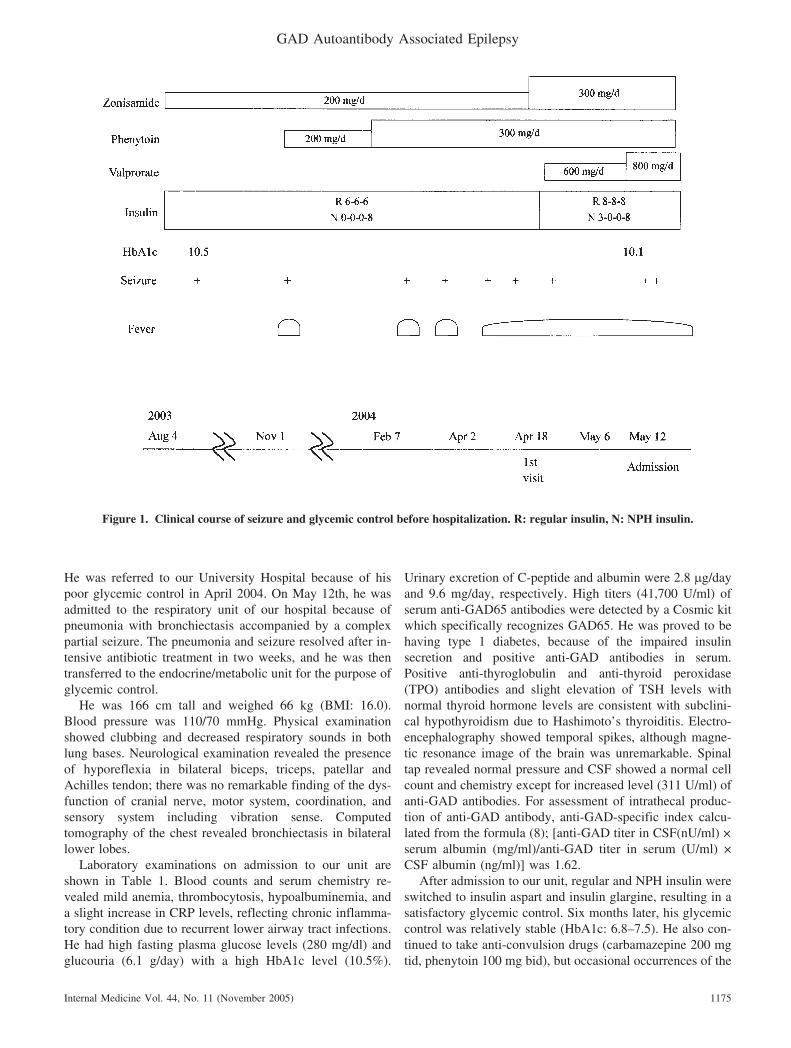
A 50-year-old man noticed polydipsia, polyuria, andweight loss in May 1999. He was found to have hyperglyce-mia and impaired insulin secretion at another hospital, andwas diagnosed as type 1 diabetes in August 1999. He alsohad respiratory tract infection due to bronchiectasis, and in-sulin treatment was started. His glycemic control was poor:fasting plasma glucose levels fluctuated between 50–500mg/dl with increased glycated hemoglobin levels (HbA1c:10–11%). He suddenly developed a complex partial seizurein August 2003, which frequently occurred thereafter, re-gardless of an intensive anti-epileptic drug therapy (Fig. 1).
Internal Medicine Vol. 44, No. 11 (November 2005)1174
Type 1 Diabetes Mellitus and Drug-resistant Epilepsy:Presence of High Titer of Anti-Glutamic Acid
Decarboxylase Autoantibodies in Serumand Cerebrospinal Fluid
Takehiko WAGO, Isao MINAMI, Isao UCHIMURA and Yukio HIRATA
□ CASE REPORT □
From the Department of Clinical and Molecular Endocrinology Tokyo Medical and Dental University Graduate School, TokyoReceived for publication February 24, 2005; Accepted for publication July 11, 2005Reprint requests should be addressed to Dr. Yukio Hirata, the Department of Clinical and Molecular Endocrinology, Tokyo Medical and Dental University
Graduate School, 1-5-45 Yushima, Bunkyo-ku, Tokyo 113-8519
He was referred to our University Hospital because of hispoor glycemic control in April 2004. On May 12th, he wasadmitted to the respiratory unit of our hospital because ofpneumonia with bronchiectasis accompanied by a complexpartial seizure. The pneumonia and seizure resolved after in-tensive antibiotic treatment in two weeks, and he was thentransferred to the endocrine/metabolic unit for the purpose ofglycemic control.
He was 166 cm tall and weighed 66 kg (BMI: 16.0).Blood pressure was 110/70 mmHg. Physical examinationshowed clubbing and decreased respiratory sounds in bothlung bases. Neurological examination revealed the presenceof hyporeflexia in bilateral biceps, triceps, patellar andAchilles tendon; there was no remarkable finding of the dys-function of cranial nerve, motor system, coordination, andsensory system including vibration sense. Computedtomography of the chest revealed bronchiectasis in bilaterallower lobes.
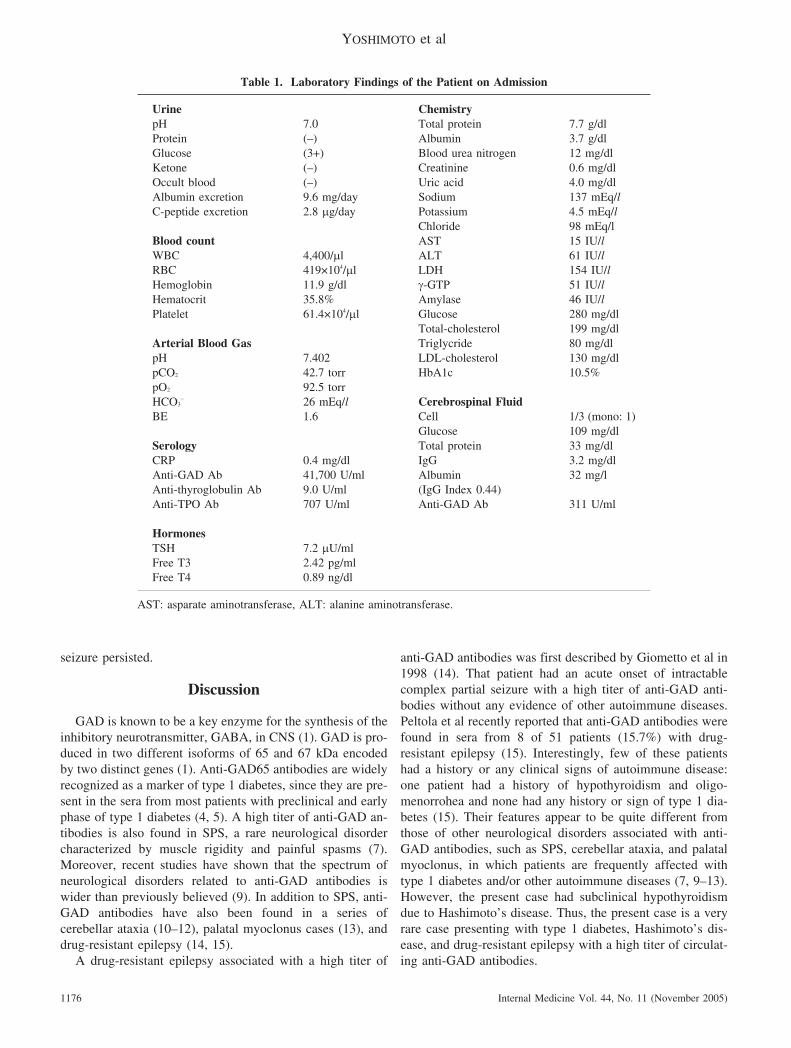
Laboratory examinations on admission to our unit areshown in Table 1. Blood counts and serum chemistry re-vealed mild anemia, thrombocytosis, hypoalbuminemia, anda slight increase in CRP levels, reflecting chronic inflamma-tory condition due to recurrent lower airway tract infections.He had high fasting plasma glucose levels (280 mg/dl) andglucouria (6.1 g/day) with a high HbA1c level (10.5%).
Urinary excretion of C-peptide and albumin were 2.8 �g/dayand 9.6 mg/day, respectively. High titers (41,700 U/ml) ofserum anti-GAD65 antibodies were detected by a Cosmic kitwhich specifically recognizes GAD65. He was proved to behaving type 1 diabetes, because of the impaired insulinsecretion and positive anti-GAD antibodies in serum.Positive anti-thyroglobulin and anti-thyroid peroxidase(TPO) antibodies and slight elevation of TSH levels withnormal thyroid hormone levels are consistent with subclini-cal hypothyroidism due to Hashimoto’s thyroiditis. Electro-encephalography showed temporal spikes, although magne-tic resonance image of the brain was unremarkable. Spinaltap revealed normal pressure and CSF showed a normal cellcount and chemistry except for increased level (311 U/ml) ofanti-GAD antibodies. For assessment of intrathecal produc-tion of anti-GAD antibody, anti-GAD-specific index calcu-lated from the formula (8); [anti-GAD titer in CSF(nU/ml) ×serum albumin (mg/ml)/anti-GAD titer in serum (U/ml) ×CSF albumin (ng/ml)] was 1.62.
After admission to our unit, regular and NPH insulin wereswitched to insulin aspart and insulin glargine, resulting in asatisfactory glycemic control. Six months later, his glycemiccontrol was relatively stable (HbA1c: 6.8–7.5). He also con-tinued to take anti-convulsion drugs (carbamazepine 200 mgtid, phenytoin 100 mg bid), but occasional occurrences of the
Internal Medicine Vol. 44, No. 11 (November 2005)
GAD Autoantibody Associated Epilepsy
1175
Figure 1. Clinical course of seizure and glycemic control before hospitalization. R: regular insulin, N: NPH insulin.
YOSHIMOTO et al
seizure persisted.
Discussion
GAD is known to be a key enzyme for the synthesis of theinhibitory neurotransmitter, GABA, in CNS (1). GAD is pro-duced in two different isoforms of 65 and 67 kDa encodedby two distinct genes (1). Anti-GAD65 antibodies are widelyrecognized as a marker of type 1 diabetes, since they are pre-sent in the sera from most patients with preclinical and earlyphase of type 1 diabetes (4, 5). A high titer of anti-GAD an-tibodies is also found in SPS, a rare neurological disordercharacterized by muscle rigidity and painful spasms (7).Moreover, recent studies have shown that the spectrum ofneurological disorders related to anti-GAD antibodies iswider than previously believed (9). In addition to SPS, anti-GAD antibodies have also been found in a series ofcerebellar ataxia (10–12), palatal myoclonus cases (13), anddrug-resistant epilepsy (14, 15).
A drug-resistant epilepsy associated with a high titer of
anti-GAD antibodies was first described by Giometto et al in1998 (14). That patient had an acute onset of intractablecomplex partial seizure with a high titer of anti-GAD anti-bodies without any evidence of other autoimmune diseases.Peltola et al recently reported that anti-GAD antibodies werefound in sera from 8 of 51 patients (15.7%) with drug-resistant epilepsy (15). Interestingly, few of these patientshad a history or any clinical signs of autoimmune disease:one patient had a history of hypothyroidism and oligo-menorrohea and none had any history or sign of type 1 dia-betes (15). Their features appear to be quite different fromthose of other neurological disorders associated with anti-GAD antibodies, such as SPS, cerebellar ataxia, and palatalmyoclonus, in which patients are frequently affected withtype 1 diabetes and/or other autoimmune diseases (7, 9–13).However, the present case had subclinical hypothyroidismdue to Hashimoto’s disease. Thus, the present case is a veryrare case presenting with type 1 diabetes, Hashimoto’s dis-ease, and drug-resistant epilepsy with a high titer of circulat-ing anti-GAD antibodies.
Internal Medicine Vol. 44, No. 11 (November 2005)1176
Table 1. Laboratory Findings of the Patient on Admission
The role of anti-GAD antibodies in neurological diseasesis still elusive due to the lack of experimental animal models(9). It has been postulated that the humoral immune responseto GAD could lead to functional impairment of GABAnergicsynaptic transmission in SPS and cellebellar ataxia, possiblydue to the reduction by anti-GAD antibodies of GABA syn-thesis and/or the interference with exocytosis of GABA (16,17). Therefore, it can be speculated that the autoimmunityagainst GAD may in part contribute to the development ofdrug-resistant epilepsy as in the present case.
It is of interest to consider the mechanism how anti-GADautoimmunity can initiate two distinct clinical manifestationsas observed in the present case. Since anti-GAD antibodiesare unable to cross the blood-brain barrier (18), theintrathecal-produced anti-GAD antibodies not from systemiccirculation, are essential for the impairment of CNS. In thepresent case, anti-GAD-specific IgG index (1.62), an assess-ment index for intrathecal production of anti-GAD antibody(8), was greater than 1.0, thus lending a strong support for itsintrathecal production (8, 19). In addition, it has been shownthat the characteristics of anti-GAD antibodies are differentbetween type 1 diabetes and SPS: anti-GAD65 antibodies intype 1 diabetes may recognize conformational epitopes in themiddle and C-terminus of the protein, whereas in SPS theyrecognize both the linear and conformational epitopes at N-terminus and C-terminus of GAD65 molecules (9, 18, 20,and 21). Although we have not examined the characteristicof anti-GAD antibodies in the present case, it is possible toassume that the variation of polyclonal properties of anti-GAD antibodies in different cases might account for the ini-tiation of different clinical manifestations.
In conclusion, we herein presented a very rare case ofdrug-resistant epilepsy accompanied with detection of anti-GAD antibodies in his CSF and type 1 diabetes. It is impor-tant to measure anti-GAD antibodies in CSF in case of type1 diabetes whenever accompanied by neurological disorders,such as seizure, ataxia, rigidity, or painful spasms.
References
1) Soghomonian J, Martin DL. Two isoforms of glutamate decarboxylase:why? Trends Biochem Sci 19: 500–505, 1998.
2) Reetz A, Solimena M, Matteoli M, Folli F, Takei K, De Camilli P.GABA and pancreatic beta-cells: colocalization of glutamic aciddecarboxylase (GAD) and GABA with synaptic-like microvesicles sug-gests their role in GABA storage and secretion. EMBO J 10: 1275–1284, 1991.
3) Erdo SL, Wolff JR. Gamma-aminobutyric acid outside the mammalianbrain. J Neurochem 54: 363–372, 1990.
4) Atkinson MA, Maclaren NK. The pathogenesis of insulin-dependent
diabetes mellitus. N Engl J Med 331: 1428–1436, 1994.5) Seissler J, Amann J, Mauch L, et al. Prevalence of autoantibodies to the
65- and 67-kD isoforms of glutamate decarboxylase in insulin-dependent diabetes mellitus. J Clin Invest 92: 1394–1399, 1993.
6) Jun HS, Khil LY, Yoon JW. Role of glutamic acid decarboxylase in thepathogenesis of type 1 diabetes. Cell Mol Life Sci 59: 1892–1901,2002.
7) Solimena M, Folli F, Aparisi R, Pozza G, De Camilli P. Autoantibodiesto GABA-ergic neurons and pancreatic beta cells in stiff-man syn-drome. N Engl J Med 322: 1555–1560, 1990.
8) Dalakas MC, Li M, Fujii M, Jacobowitz DM. Stiff person syndrome:quantification, specificity, and intrathecal synthesis of GAD65 antibod-ies. Neurology 57: 780–784, 2001.
9) Vianello M, Tavolato B, Giometto B. Glutamic acid decarboxylaseautoantibodies and neurological disorders. Neurol Sci 23: 145–151,2002.
10) Honnorat J, Saiz A, Giometto B, et al. Cerebellar ataxia with anti-glutamic acid decarboxylase antibodies: study of 14 patients. ArchNeurol 58: 225–230, 2001.
11) Saiz A, Arpa J, Sagasta A, et al. Autoantibodies to glutamic aciddecarboxylase in three patients with cerebellar ataxia, late-onset insu-lin-dependent diabetes mellitus, and polyendocrine autoimmunity.Neurology 49: 1026–1030, 1997.
12) Iwasaki H, Sato R, Shichiri M, Hirata Y. A patient with type 1 diabetesmellitus and cerebellar ataxia associated with high titer of circulatinganti-glutamic acid decarboxylase antibodies. Endocr J 48: 261–268,2001.
13) Nemni R, Braghi S, Natali-Sora MG, et al. Autoantibodies to glutamicacid decarboxylase in palatal myoclonus and epilepsy. Ann Neurol 36:665–667, 1994.
14) Giometto B, Nicolao P, Macucci M, Tavolato B, Foxon R, BottazzoGF. Temporal-lobe epilepsy associated with glutamic-acid-decarboxy-lase autoantibodies. Lancet 352: 457, 1998.
15) Peltola J, Kulmala P, Isojarvi J, et al. Autoantibodies to glutamic aciddecarboxylase in patients with therapy-resistant epilepsy. Neurology55: 46–50, 2000.
16) Mitoma H, Song SY, Ishida K, Yamakuni T, Kobayashi T, MizusawaH. Presynaptic impairment of cerebellar inhibitory synapses by anautoantibody to glutamate decarboxylase. J Neurol Sci 175: 40–44,2000.
17) Dinkel K, Meinck HM, Jury KM, Karges W, Richter W. Inhibition ofgamma-aminobutyric acid synthesis by glutamic acid decarboxylaseautoantibodies in stiff-man syndrome. Ann Neurol 44: 194–201, 1998.
18) Ellis TM, Atkinson MA. The clinical significance of an autoimmuneresponse against glutamic acid decarboxylase. Nat Med 2: 148–153,1996.
19) Link H, Tibbling G. Principles of albumin and IgG analysis in neuro-logical disorders III. Evaluation of IgG synthesis within the centralnervous system in multiple sclerosis. Scand J Clin Lab Invest 37: 397–401, 1997.
20) Bjork E, Velloso LA, Kampe O, Karlsson FA. GAD autoantibodies inIDDM, stiff-man syndrome, and autoimmune polyendocrine syndrometype I recognize different epitopes. Diabetes 43: 161–165, 1994.
21) Daw K, Ujihara N, Atkinson M, Powers AC. Glutamic aciddecarboxylase autoantibodies in stiff-man syndrome and insulin-dependent diabetes mellitus exhibit similarities and differences inepitope recognition. J Immunol 156: 818–825, 1996.