109
Antibiotics

Antibiotics

Antibiotics – mode of action
• Interference with of bacterial wall synthesis -
(betalactams, glycopeptides)
• Interference with DNA synthesis - (gyrase inhibitors)
• Antimetabolites - (sulfonamides, trimethoprim)
• Interference with proteosynthesis on various levels
– prevention of tRNA link (tetracycline)
– mRNA reading failure (aminoglycosides)
– Inhibition of transpeptidation (chloramphenicol)
– Inhibition of tRNA translocation (erythromycin)

Resistance
• Natural (target structure not present)
• Acquired
– Chromosomal - mutations - rare
– Extra chromosomal - plasmids - frequent
• plasmids – segments of DNA with ability of
independent replication carrying gens coding
resistence
– Transfer – conjugation of bacteria - plasmids
– Transduction by means of fags
– Transposes - plasmid/plasmid,
plasmid/chromosome and vice versa
– Transformation - DNA

Antibiotics - biochemical mechanisms of resistance
• Production of inactivating enzymes
– betalactamases - (penicillins, cefalosporins)
– acetyltransferases - (chloramphenicol)
– kinases - (aminoglycosides)
– methylases - (tetracyclines)
• Alteration of binding site - (betalactams, macrolides,
aminoglycosides)
• Reduction of antibiotic uptake - (tetracyclines)
• Alteration of dihydrofolat reductase - (sulfonamides)
• Efflux pumps - (more groups of antibiotics)
• Change in bacterial wall permeability - (betalactams)

Bacterial wall: G+ bacteria
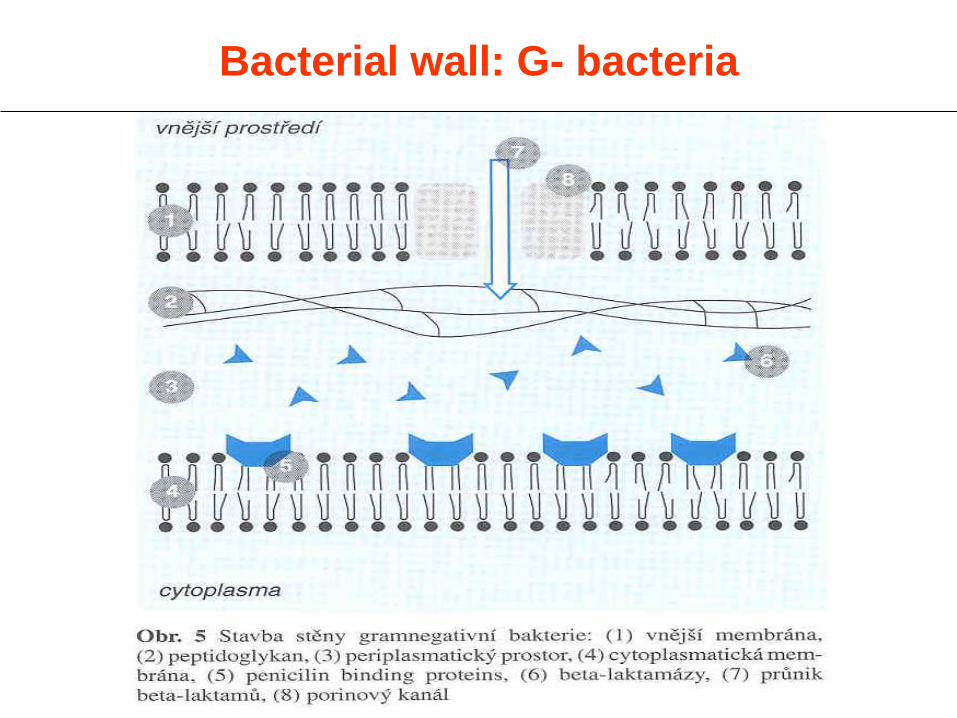
Bacterial wall: G- bacteria
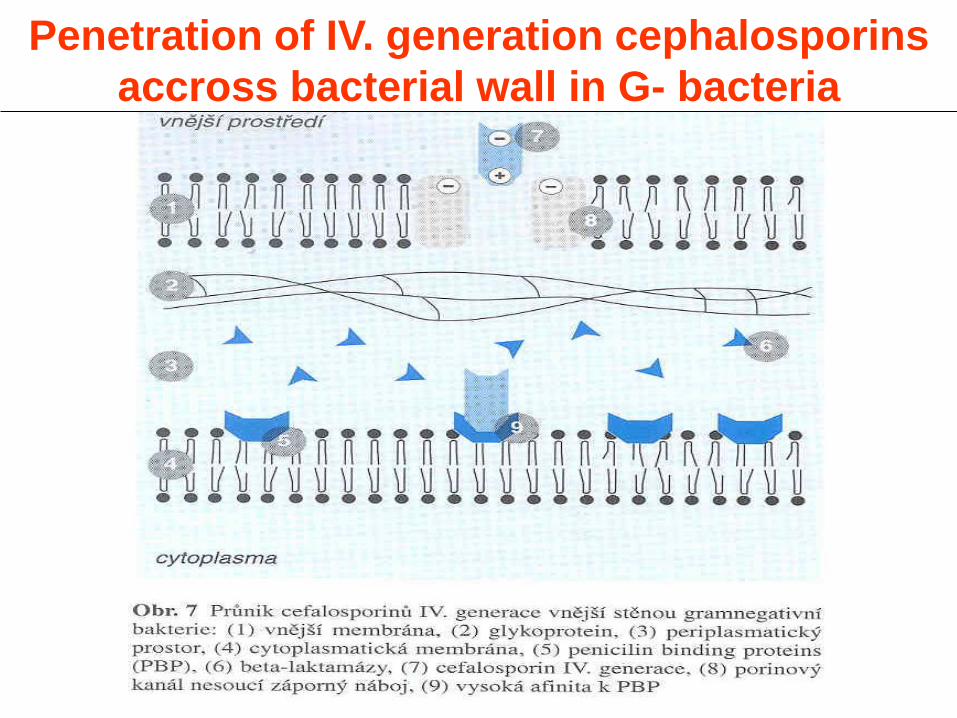
Penetration of IV. generation cephalosporins
accross bacterial wall in G- bacteria
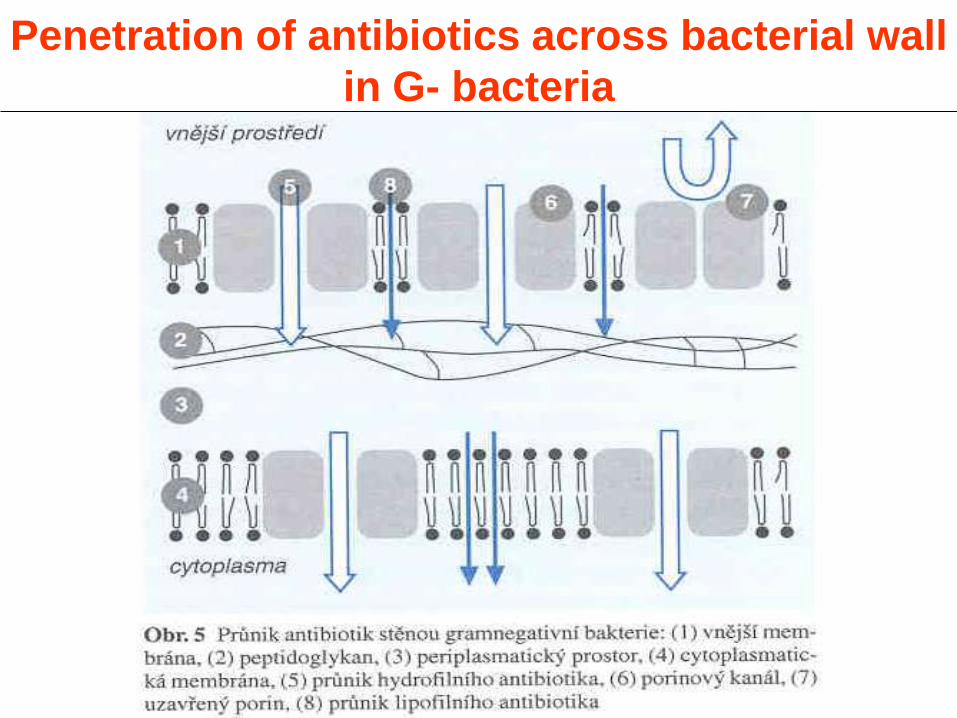
Penetration of antibiotics across bacterial wall
in G- bacteria
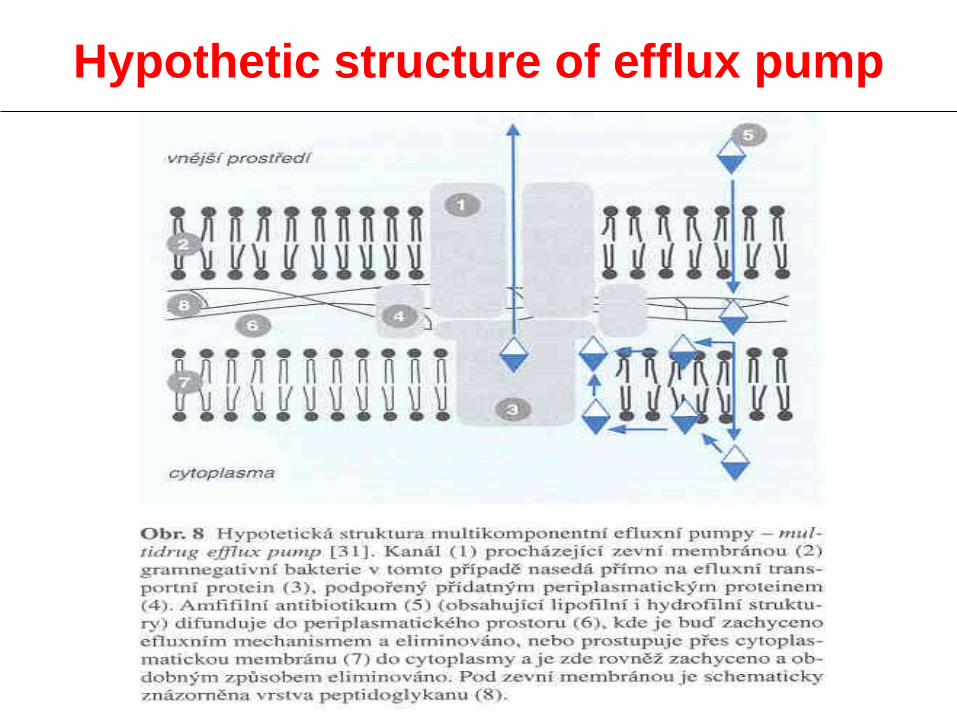
Hypothetic structure of efflux pump

Beta-lactams

1929
1941
1944
objev penicilinu
začátek používání
penicilinu
první b-laktamázy
Od objevu penicilinu k širokospektrým
b-laktamům
A. Fleming, W. Florey, E. B. Chain – 1945 Nobelova
Cena za Fyziologii a medicínu Za objev penicilinu
a jeho léčivého účinku na různé infekční choroby
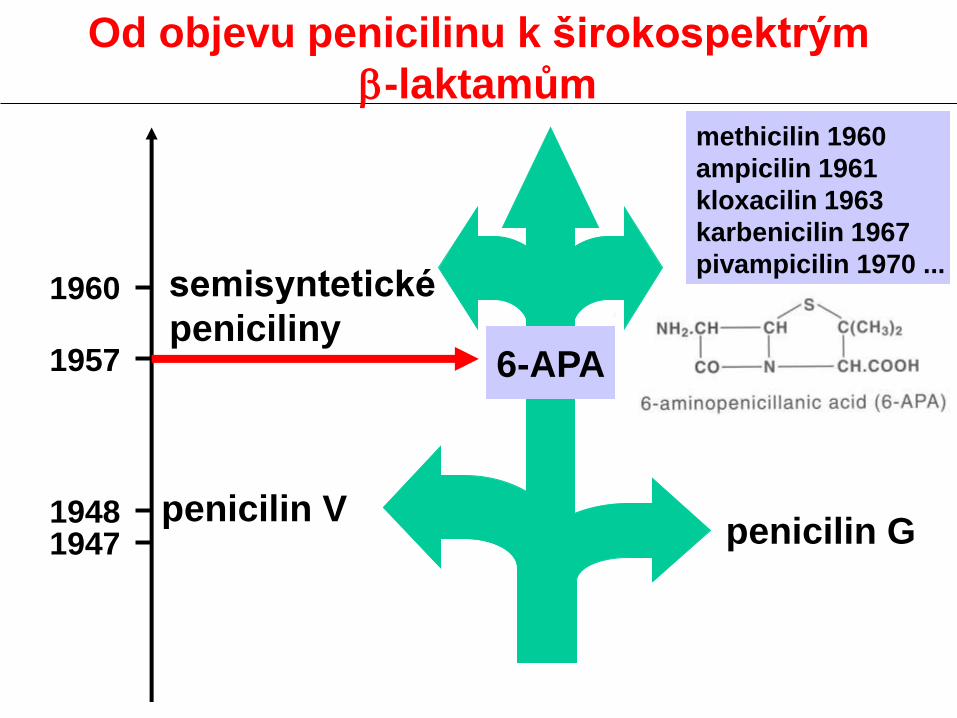
penicilin G penicilin V
semisyntetické
peniciliny 1960
1957
1948 1947
methicilin 1960
ampicilin 1961
kloxacilin 1963
karbenicilin 1967
pivampicilin 1970 ...
6-APA
Od objevu penicilinu k širokospektrým
b-laktamům

amoxicilinklavulanát 1981
1977
1973 amoxicilin
kyselina
klavulanová
Od objevu penicilinu k širokospektrým
b-laktamům
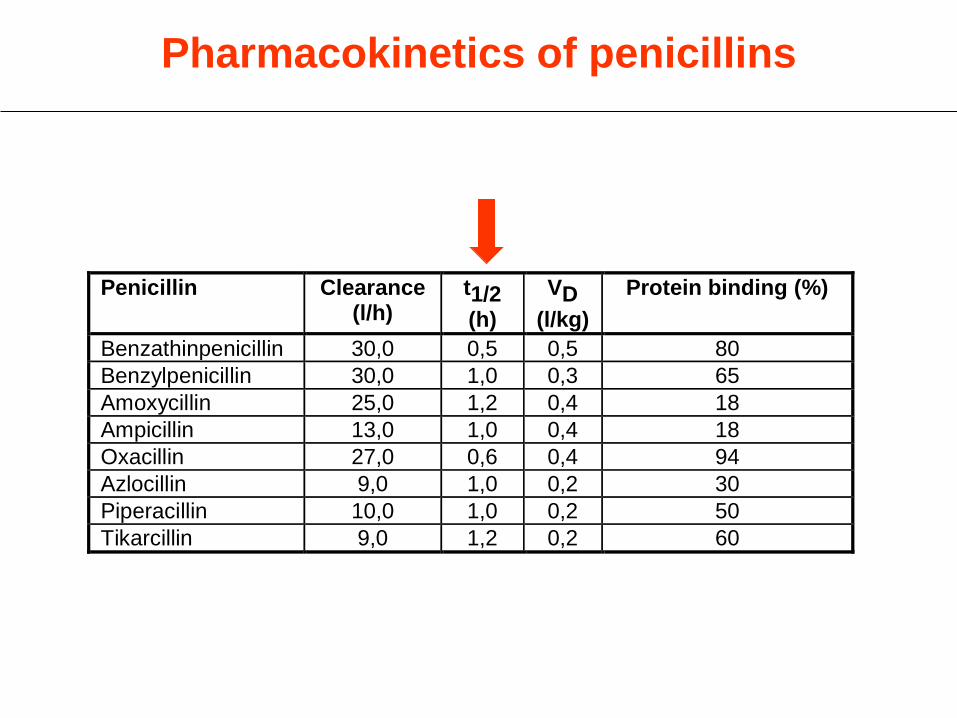
Pharmacokinetics of penicillins
Penicillin Clearance (l/h)
t1/2
(h)
VD
(l/kg)
Protein binding (%)
Benzathinpenicillin 30,0 0,5 0,5 80
Benzylpenicillin 30,0 1,0 0,3 65
Amoxycillin 25,0 1,2 0,4 18
Ampicillin 13,0 1,0 0,4 18
Oxacillin 27,0 0,6 0,4 94
Azlocillin 9,0 1,0 0,2 30
Piperacillin 10,0 1,0 0,2 50
Tikarcillin 9,0 1,2 0,2 60

Antibacterial spectrum
Standard pk Nonstandard PK Metabolic instability
G+ Cefazolin Cefradin (p.o., i.v., i.m.)
Cefalotin (deacetyl)
G(+)/- Cefuroxim Ceftriaxon (t0,5, bile)
Cefotaxim (deacetyl)
G- Ceftazidim Cefoperazon (bile)
/
anaerobes cefoxitin Cefotetan (t0,5)
/
Division of cephalosporins according to
pharmacokinetic properties (examples)
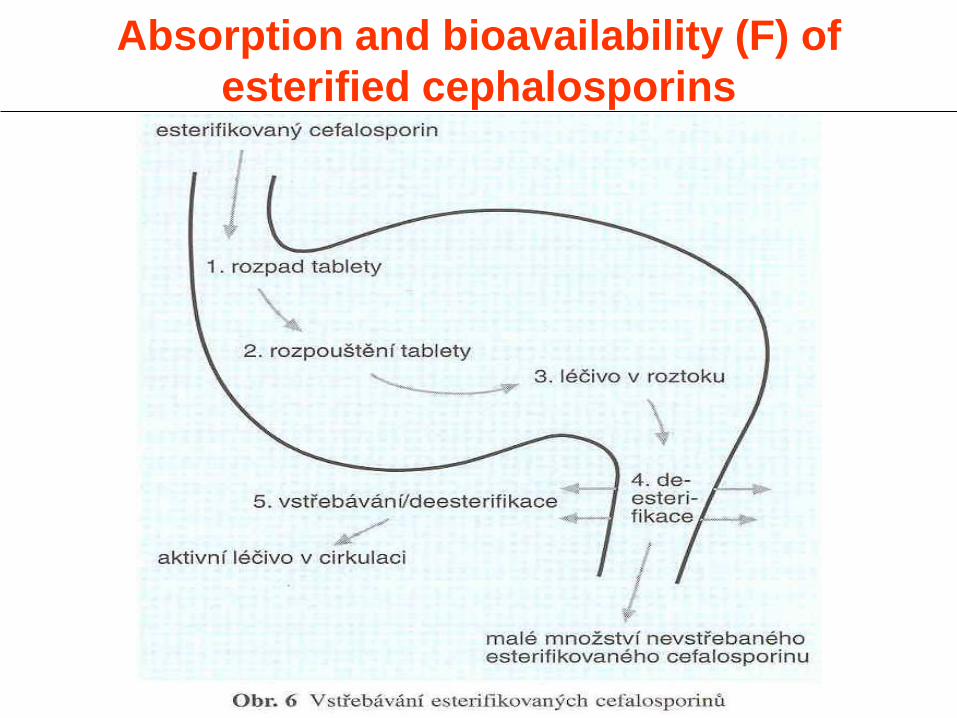
Absorption and bioavailability (F) of
esterified cephalosporins

Influence of food intake on absorption of
esterified cephalosorins
mg/l
h
After food
No food
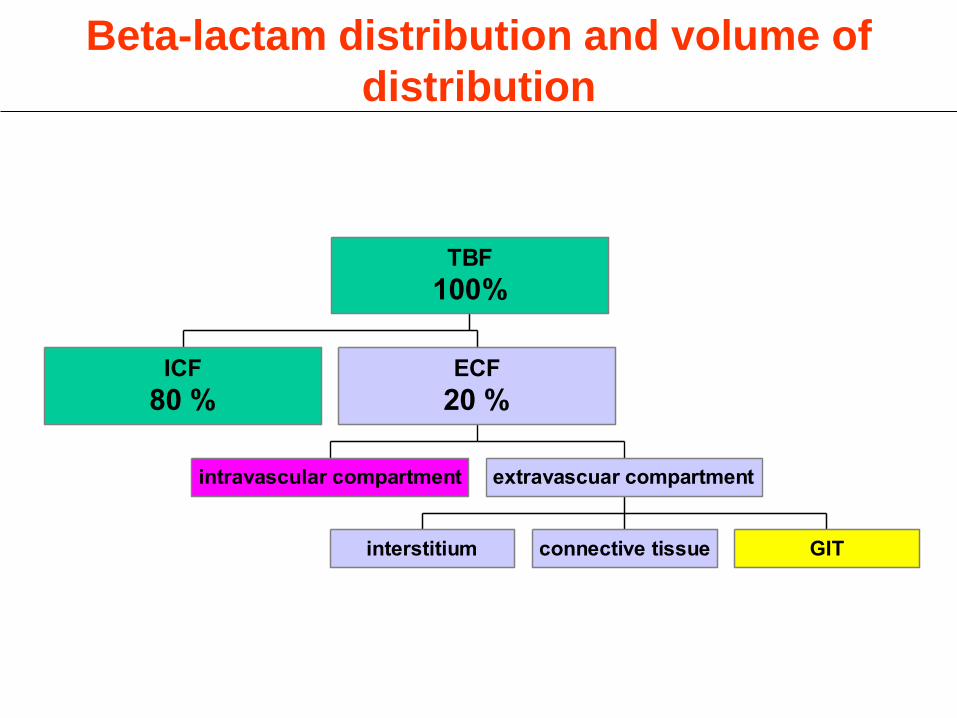
Beta-lactam distribution and volume of
distribution
ICF
80 %
intravascular compartment
interstitium connective tissue GIT
extravascuar compartment
ECF
20 %
TBF
100%

Plasma, intersticium and muscle
concentration of ceftazidim (25 mg/kg i.v.)
mg/l * mg/kg
min
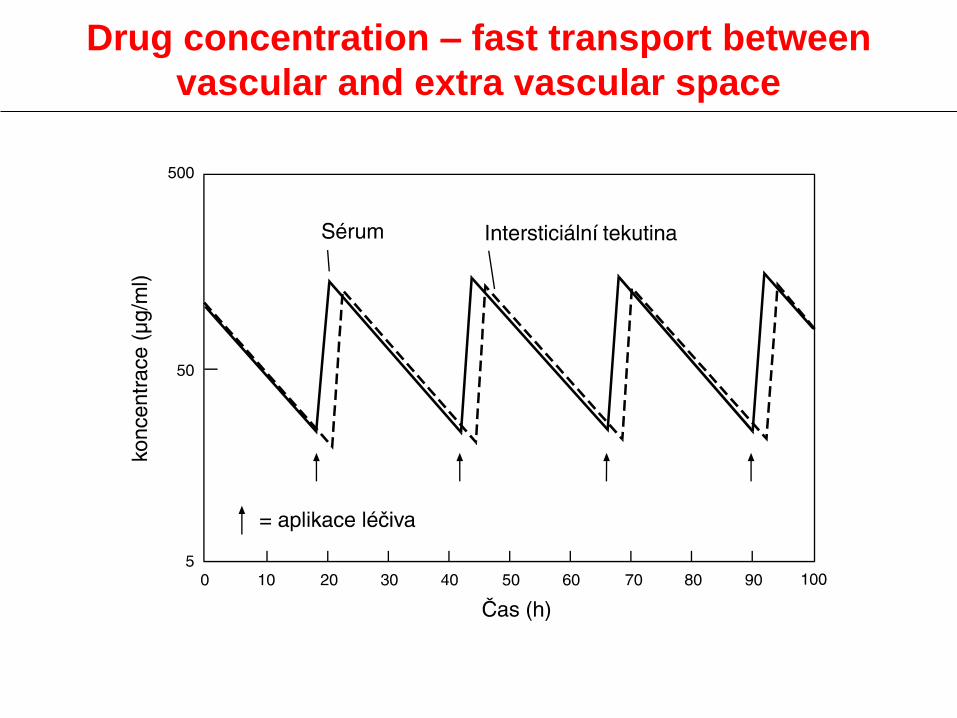
Drug concentration – fast transport between
vascular and extra vascular space

Drug concentration – slow transport between
vascular and extra vascular space

Penetration of cephalosorins across
hematoencephalic barrier in meningitis
(% of serum concentration)
cephalosporin penetration into CSF
ceftriaxon 5 - 15
cefotaxim 15 - 30
ceftazidim 20 - 40
cefuroxim 18 - 35
Penetration above 10% is clinically sufficient
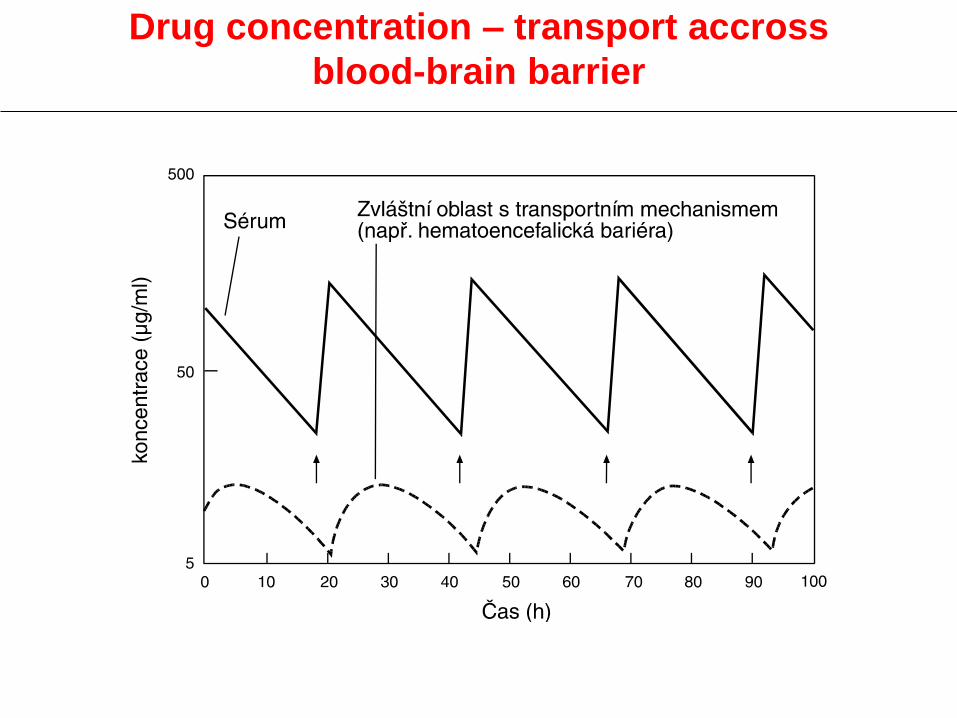
Drug concentration – transport accross
blood-brain barrier
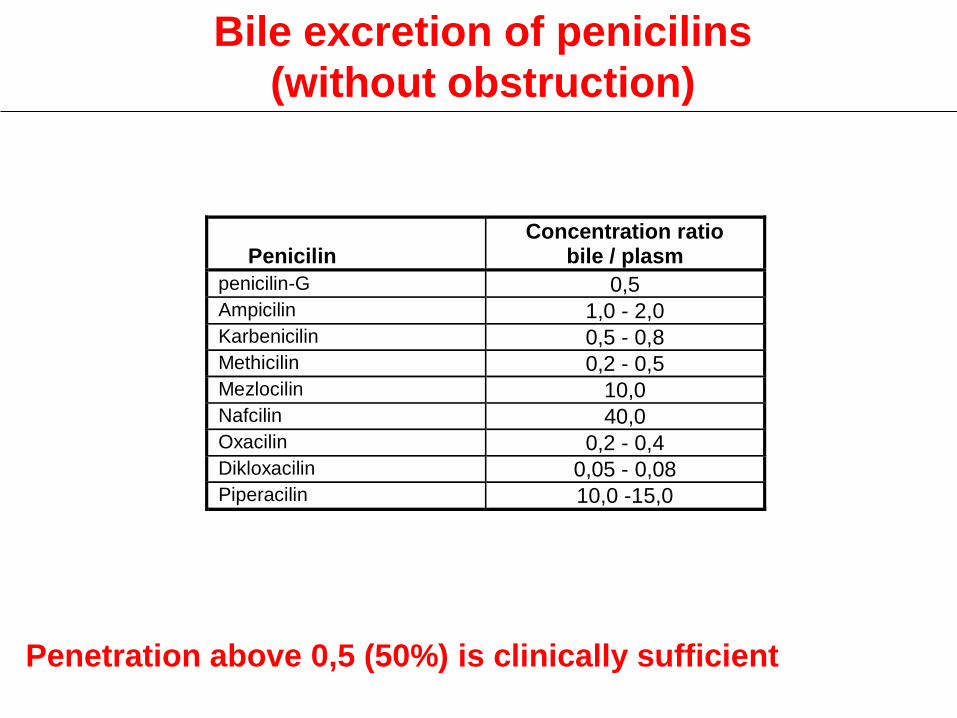
Penicilin
Concentration ratio bile / plasm
penicilin-G 0,5 Ampicilin 1,0 - 2,0 Karbenicilin 0,5 - 0,8 Methicilin 0,2 - 0,5 Mezlocilin 10,0 Nafcilin 40,0 Oxacilin 0,2 - 0,4 Dikloxacilin 0,05 - 0,08 Piperacilin 10,0 -15,0
Bile excretion of penicilins
(without obstruction)
Penetration above 0,5 (50%) is clinically sufficient
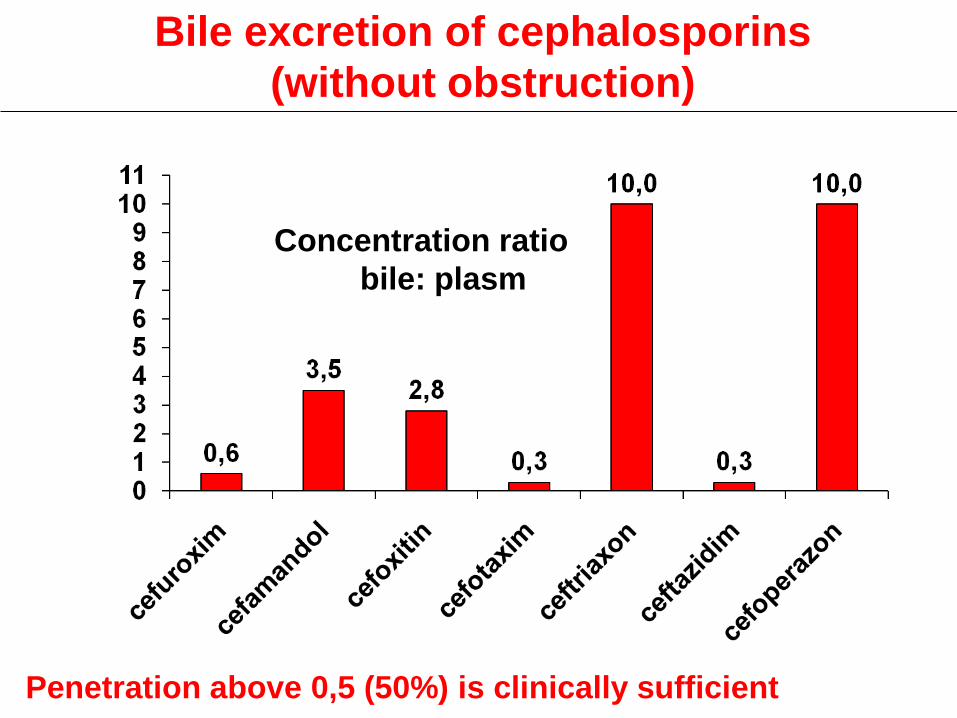
Bile excretion of cephalosporins
(without obstruction)
Concentration ratio
bile: plasm
Penetration above 0,5 (50%) is clinically sufficient
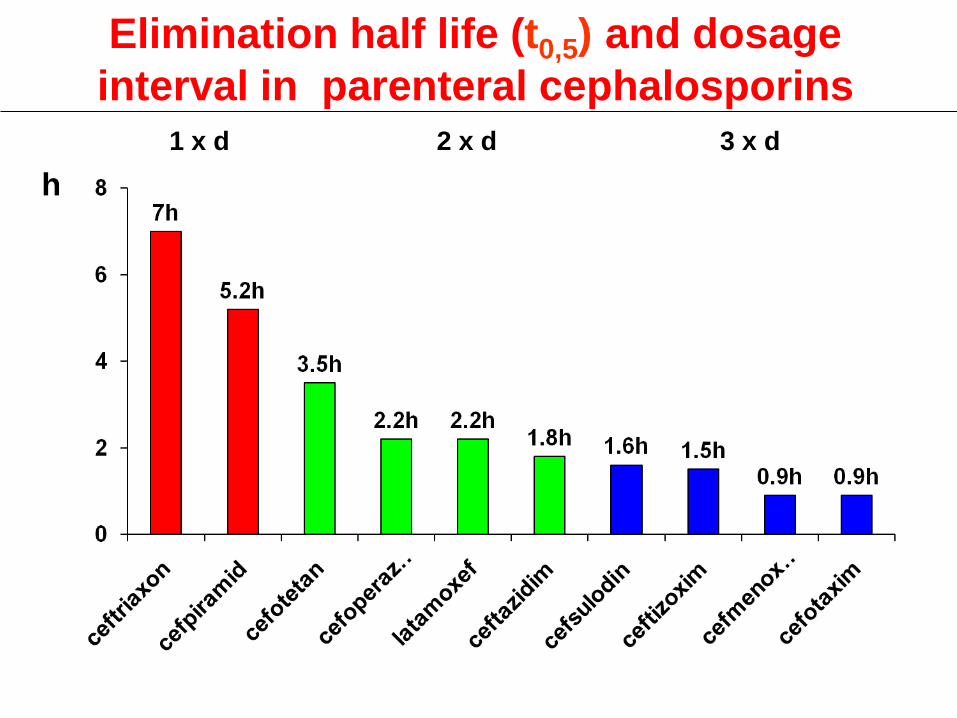
Elimination half life (t0,5) and dosage
interval in parenteral cephalosporins 1 x d 2 x d 3 x d
h h

h
2 x d 3 x d 4 x d
Elimination half life (t0,5) and dosage
interval in parenteral cephalosporins

h
3 x d 2 x d 1 x d
Elimination half life (t0,5) and dosage
interval in oral cephalosporins
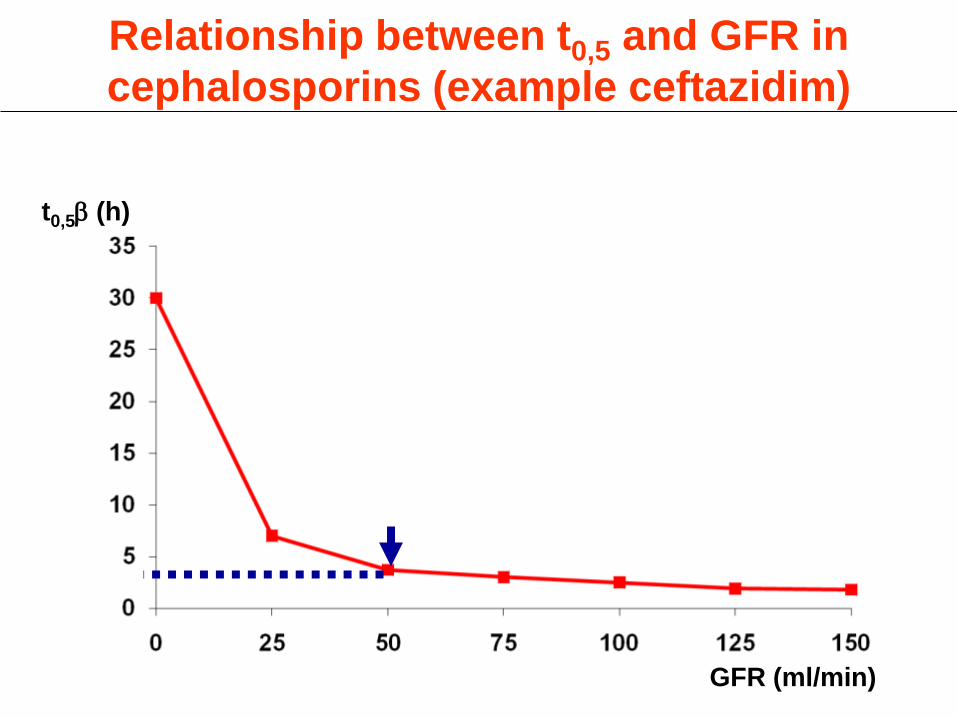
GFR (ml/min)
t0,5b (h)
Relationship between t0,5 and GFR in
cephalosporins (example ceftazidim)

Macrolides
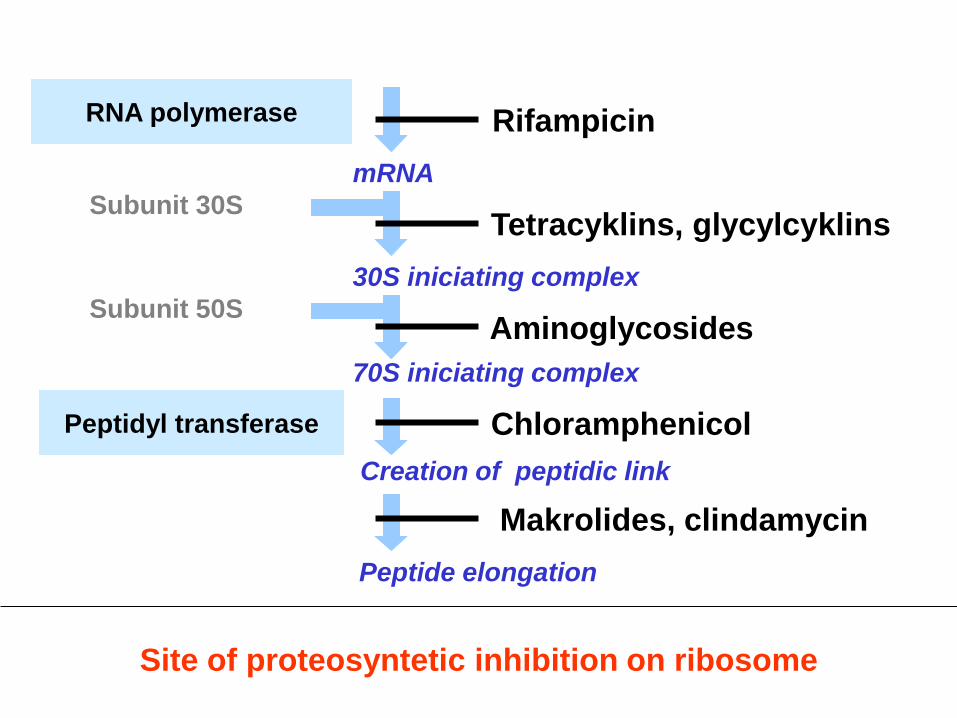
Site of proteosyntetic inhibition on ribosome
RNA polymerase
Subunit 30S
mRNA
30S iniciating complex
70S iniciating complex
Creation of peptidic link
Subunit 50S
Peptidyl transferase
Rifampicin
Aminoglycosides
Chloramphenicol
Makrolides, clindamycin
Peptide elongation
Tetracyklins, glycylcyklins
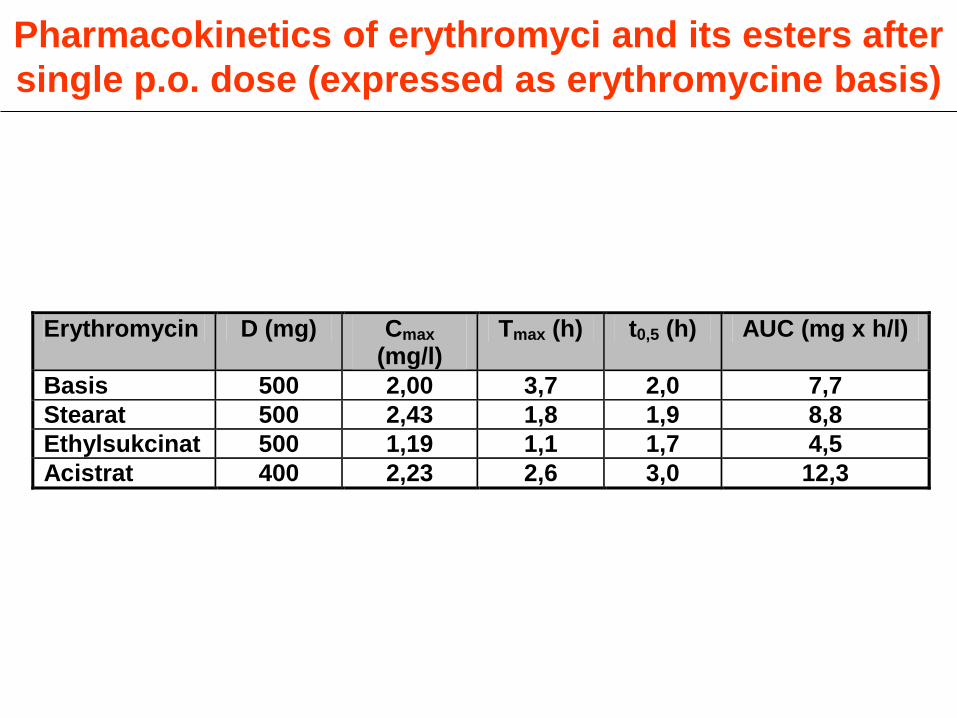
Pharmacokinetics of erythromyci and its esters after
single p.o. dose (expressed as erythromycine basis)
Erythromycin D (mg) Cmax (mg/l)
Tmax (h) t0,5 (h) AUC (mg x h/l)
Basis 500 2,00 3,7 2,0 7,7
Stearat 500 2,43 1,8 1,9 8,8
Ethylsukcinat 500 1,19 1,1 1,7 4,5
Acistrat 400 2,23 2,6 3,0 12,3
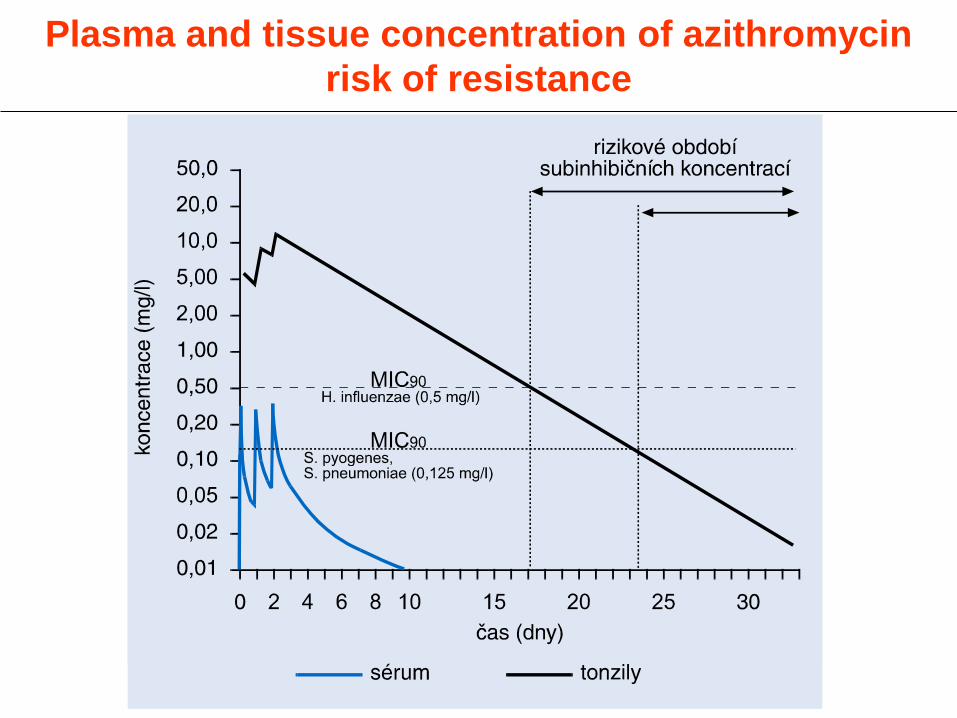
Plasma and tissue concentration of azithromycin
risk of resistance
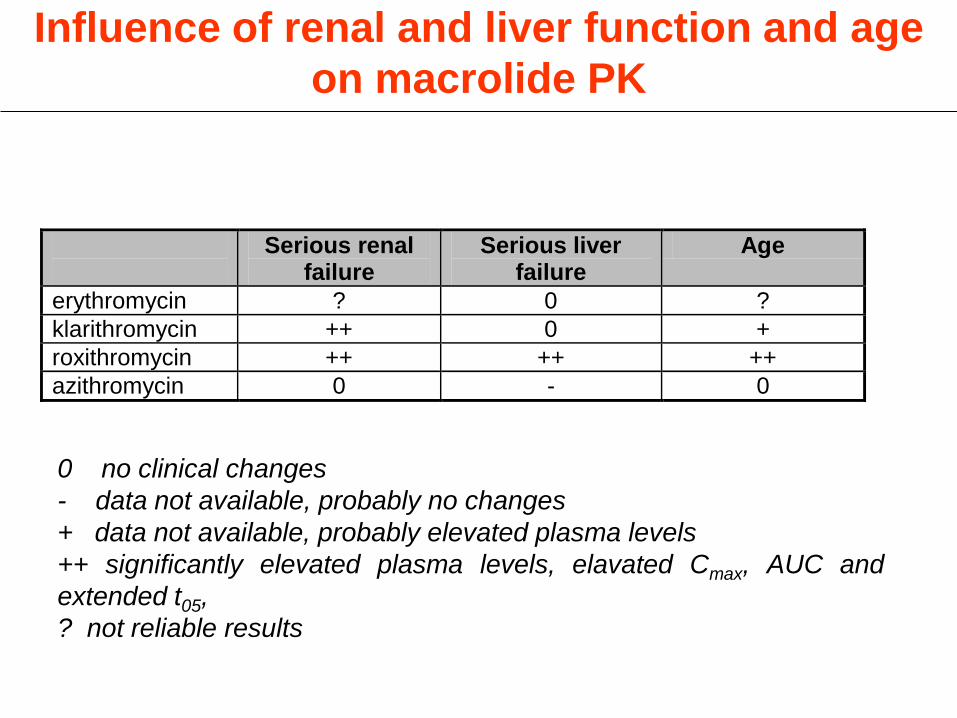
Influence of renal and liver function and age
on macrolide PK
Serious renal failure
Serious liver failure
Age
erythromycin ? 0 ?
klarithromycin ++ 0 +
roxithromycin ++ ++ ++
azithromycin 0 - 0
0 no clinical changes
- data not available, probably no changes
+ data not available, probably elevated plasma levels
++ significantly elevated plasma levels, elavated Cmax, AUC and
extended t05,
? not reliable results
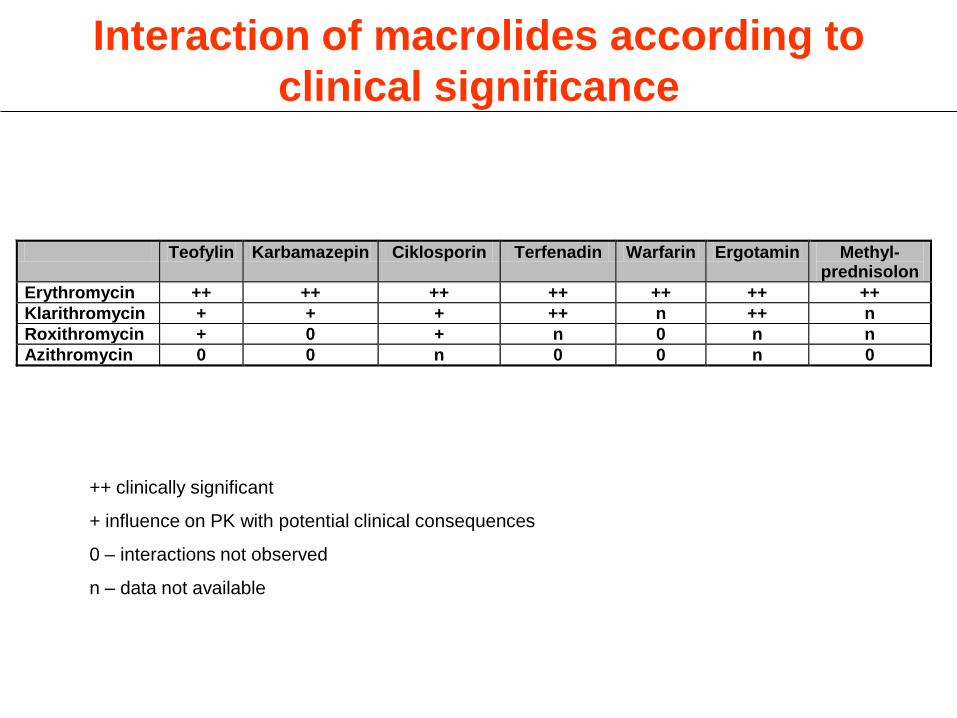
Interaction of macrolides according to
clinical significance
Teofylin Karbamazepin Ciklosporin Terfenadin Warfarin Ergotamin Methyl- prednisolon
Erythromycin ++ ++ ++ ++ ++ ++ ++
Klarithromycin + + + ++ n ++ n
Roxithromycin + 0 + n 0 n n
Azithromycin 0 0 n 0 0 n 0
++ clinically significant
+ influence on PK with potential clinical consequences
0 – interactions not observed
n – data not available

Macrolide (=drug A) interaction with other drugs
metabolised by cytochrome P 450
drugB Resulting interaction (A+B)
Teofylin Serum concentration increase (B)
ciklosporin, takrolimus, sirolimus (Enzyme inhibition)
Digoxin
Astemizol, terfenadin, loratadin
Námelové alkaloidy
Kortikosteroidy
Cisaprid
Midazolam, triazolam
Diltiazem, verapamil
Ethynil estradiol, destoden
Itrakonazol, mikonazol, ketokonazol, flukonazol
Fluoxetin, paroxetin, sertalin
Warfarin
indinavir, ritonavir Serum concentration increase (both A and B)
fenytoin, fenobarbital, karbamazepin
Omeprazol
rifabutin, rifampicin
Zidovudin Serum concentration decrease (B)
(Enzyme induction)
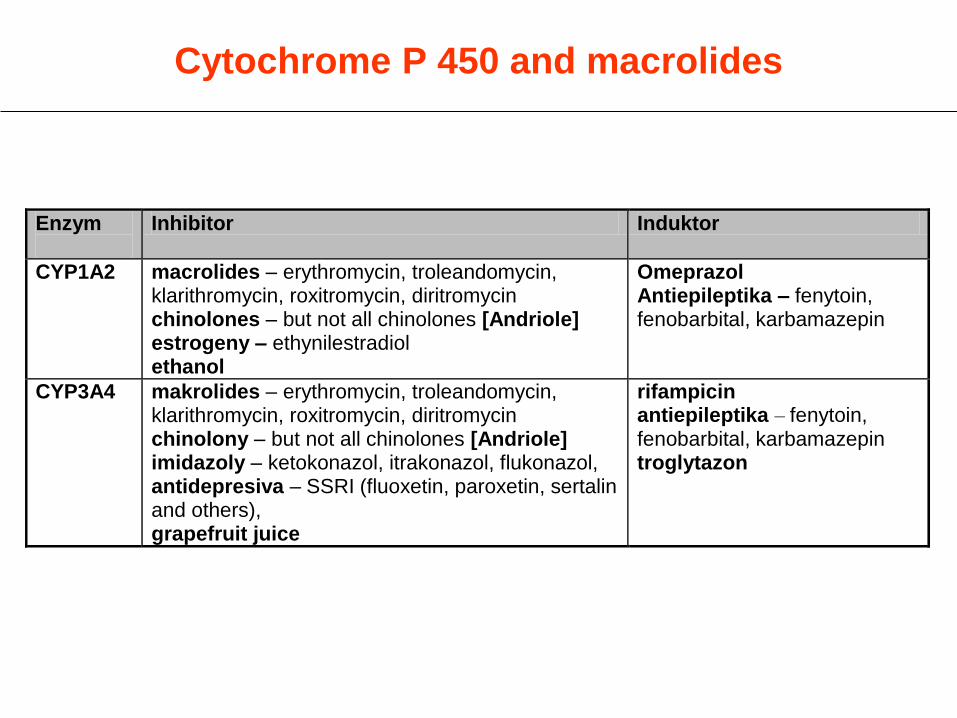
Cytochrome P 450 and macrolides
Enzym
Inhibitor Induktor
CYP1A2 macrolides – erythromycin, troleandomycin, klarithromycin, roxitromycin, diritromycin chinolones – but not all chinolones [Andriole] estrogeny – ethynilestradiol ethanol
Omeprazol Antiepileptika – fenytoin, fenobarbital, karbamazepin
CYP3A4 makrolides – erythromycin, troleandomycin, klarithromycin, roxitromycin, diritromycin chinolony – but not all chinolones [Andriole] imidazoly – ketokonazol, itrakonazol, flukonazol, antidepresiva – SSRI (fluoxetin, paroxetin, sertalin and others), grapefruit juice
rifampicin antiepileptika – fenytoin, fenobarbital, karbamazepin troglytazon
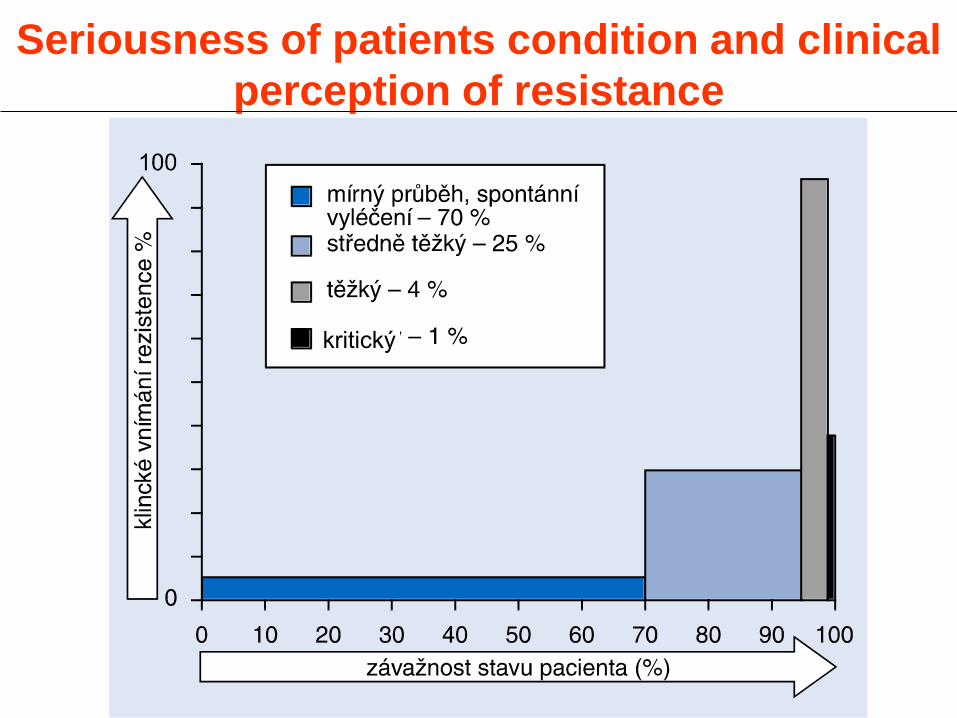
Seriousness of patients condition and clinical
perception of resistance
kritický

• Macrolide of the ketolide group
• Mode of action, AE profile and
interactions (CYP 3A4 a CYP 2P6) –
same as other macrolides
Telithromycin
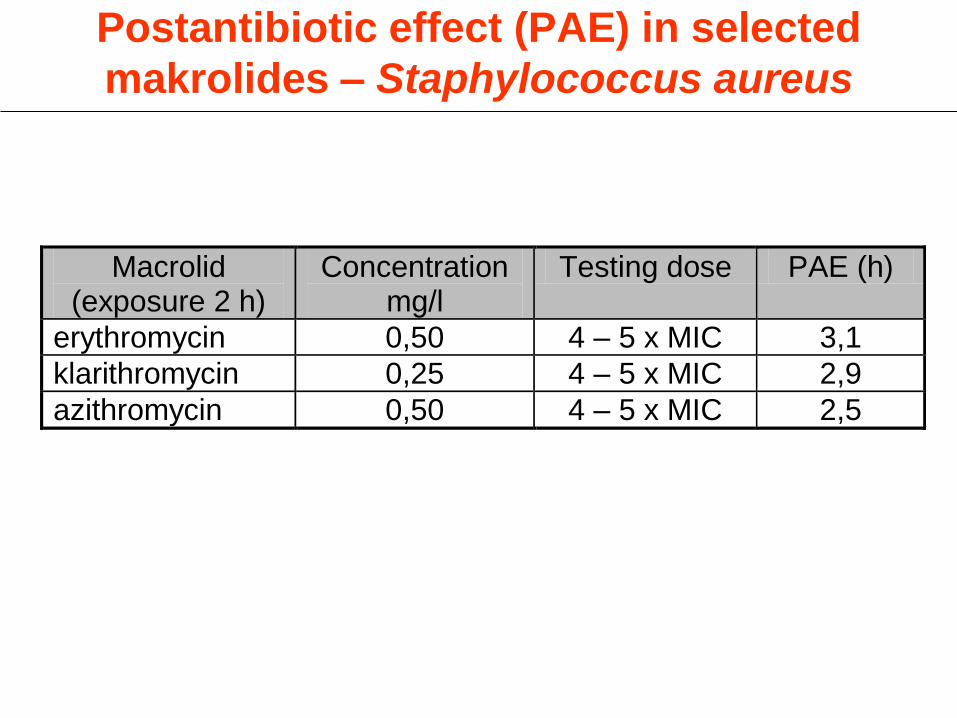
Postantibiotic effect (PAE) in selected
makrolides – Staphylococcus aureus
Macrolid (exposure 2 h)
Concentration mg/l
Testing dose PAE (h)
erythromycin 0,50 4 – 5 x MIC 3,1
klarithromycin 0,25 4 – 5 x MIC 2,9
azithromycin 0,50 4 – 5 x MIC 2,5
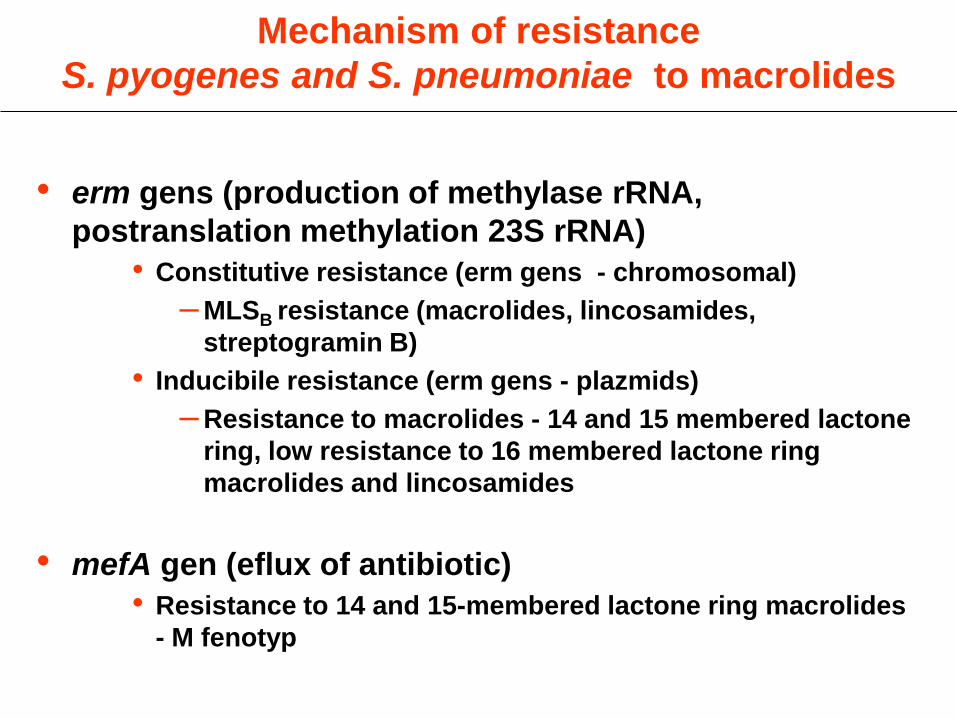
Mechanism of resistance
S. pyogenes and S. pneumoniae to macrolides
• erm gens (production of methylase rRNA,
postranslation methylation 23S rRNA)
• Constitutive resistance (erm gens - chromosomal)
– MLSB resistance (macrolides, lincosamides,
streptogramin B)
• Inducibile resistance (erm gens - plazmids)
– Resistance to macrolides - 14 and 15 membered lactone
ring, low resistance to 16 membered lactone ring
macrolides and lincosamides
• mefA gen (eflux of antibiotic)
• Resistance to 14 and 15-membered lactone ring macrolides
- M fenotyp
End of part 1
Tetracyclins
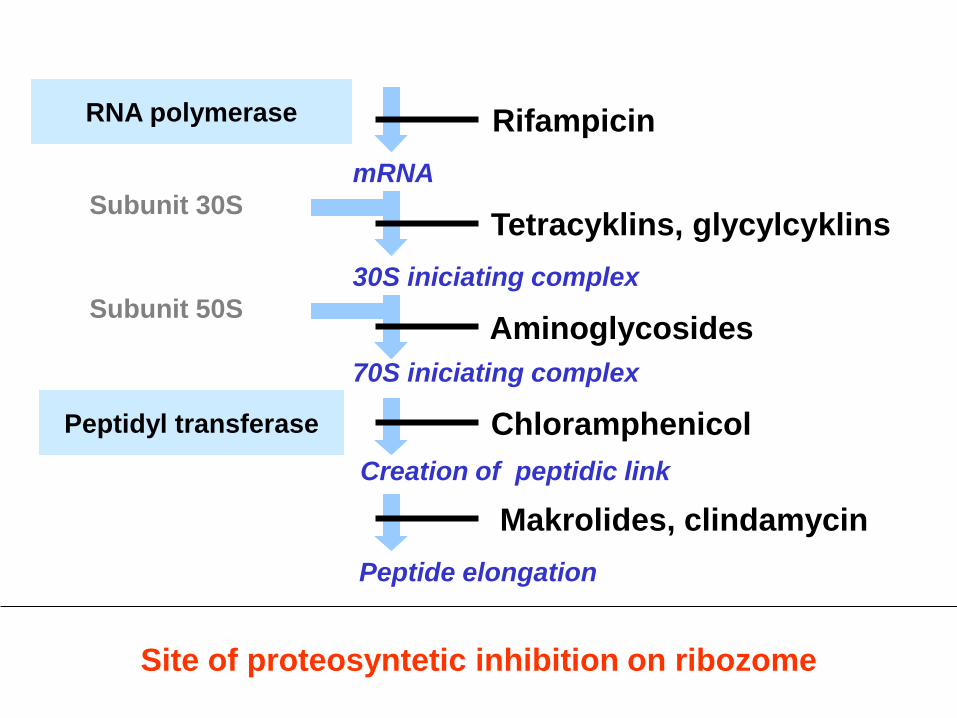
Site of proteosyntetic inhibition on ribozome
RNA polymerase
Subunit 30S
mRNA
30S iniciating complex
70S iniciating complex
Creation of peptidic link
Subunit 50S
Peptidyl transferase
Rifampicin
Aminoglycosides
Chloramphenicol
Makrolides, clindamycin
Peptide elongation
Tetracyklins, glycylcyklins

Tetracyclins - characteristics
• Broad spectrum bakteriostatic antibiotics
introduced in1949 oxyteracyclin (I. generation),
doxycyclin since1967 (II. genaration)
• Mode of action - proteosyntetic inhibitors in
bacteial cell
• Many bacteria straine resistent – result of
frequent use
• Tetracyclins inhibit tRNA-aminoacids
complex link on 30s bacterial ribosome
subunit
• Tetracyclins prevent the link aminoacyl-tRNA
on acceptor site of the mRNA complex with
ribosome
Tetracyclins - mode of action

Tetracyclins - resistance
• Plasmid resistance
• Gen for tetracycline resistance is close to
gen coding resistance to aminoglycosides,
sulfonamides a chloramphenicol
• Cross resistance with this ATBs frequent
• Decrease of accumulation or decrease
of influx resp. increase of efflux
• Limited contact of TTC with ribosome
due to ribosomal protective proteins
• Enzymatic inactivation by methylase
Tetracyclins - mechanism of resistance

Tetracyclines - pharmacokinetics
• Irregular absorption – in small intestine -
better fasting
• Protein binding +/- 80%
• Penetrate placentar barrier and into maternal
milk!
• Bile excretion - enterohepatic circulation
• Partly eliminated via kidney
Tetracycline - antimicrobial spectrum
• S. pneumoniae - frequently resistant
• H. influenzae, E. coli - frequently resistant
• Vibrio cholerae
• Chlamydia, Mycoplasms
• Shigella – if sensitive
• Ureaplasma
• Rickettsie
• Brucela, Listeria, Yersinia
• Actinomycetes
• Protozoar infection (amoeba, malaria-schizonts)

Average resistance to selected antibiotics
S. pneumoniae
Resistance (%)

Average resistance to selected antibiotics
S. pyogenes
Resistance (%)
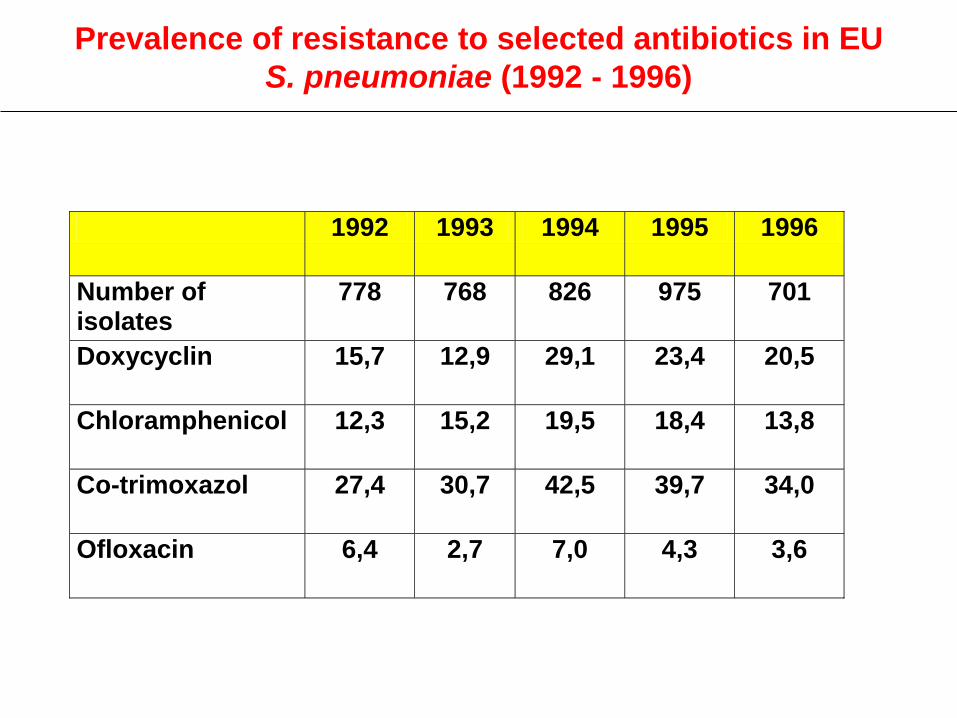
1992 1993 1994 1995 1996
Number of isolates
778 768 826 975 701
Doxycyclin 15,7 12,9 29,1 23,4 20,5
Chloramphenicol 12,3 15,2 19,5 18,4 13,8
Co-trimoxazol 27,4 30,7 42,5 39,7 34,0
Ofloxacin 6,4 2,7 7,0 4,3 3,6
Prevalence of resistance to selected antibiotics in EU
S. pneumoniae (1992 - 1996)

Average resistance to selected antibiotics
H. influenzae
Resinstance (%)

1992 1993 1994 1995
Number of isolates/bla+
702/12,3% 1130/14,4% 1065/15,5% 1456/16,8%
Chloramphenikol 4,1 2,5 2,5 2,1
Co-trimoxazol 13,5 8,6 20,5 18,9
Average resistence to selected antibiotics in EU
H. Influenzae (1992 - 1995)

Tetracyclines – ADR and KI
• ADR
– GI - frequent, alter compliance,
pseudomembranous colitis rare
– Most serious - toxic liver damage
– Exfoliative dermatitis
– Fotosenzibilisation - fotodermatitis
• KI
– pregnancy a lactation
– children until 8 years – dental abnormities
– alcohol

Tetracyclines - interactions
• Pharmacokinetic on the level of absorption - antacids,
Ca, Mg, Zn, Al and other salts, milk and milk products
– decrease of absorption (chelats)
• Coumarin anticoagulation drugs – increase of
bleeding
• OHA - hypoglycemia
• Interaction with cytochrome P450 - metabolism of
tetracycline accelerated = decrease of therapeutic
concentration
• Combining with beta-lactams = decrease in efficacy!

Antimetabolites
• Sulfonamides and trimethoprim block two
subsequent processes of nucleic acid synthesis
• Sulfonamides compete with PABA for
dihydropteroate syntetase necessary for
dihydrofolic acid synthesis
• Trimethoprim is competitive inhibitor of
dihydrofolatreductase preventing conversion to
tetrahydrofolic acid
Antimetabolites – mode of action

• In sulfonamides: plasmid encoded
dihydropteroate synthetase with low affinity to
sulfonamide (but preserved to PABA)
• In trimethoprim: bypass of metabolic pathway
dihyhydrofolat reductase has then low affinity
to trimethoprim
Antimetabolits – mechanisms of rezistance
• Gastrointestinal – nausea, vomitus
• Dermal – from mild up to toxic epidermal
necrolysis
• Hematological dosorders
• Caution: asthma, serious allergic disorders and
liver function disorders
• Contraindications: pregnancy, brest feeding,
immature neonates
Antimetabolites - AE, contraindications

• Frequent PK interactions – binding site
competition in plasma proteins (oral
hypoglycemic agents, anticoagulating agents)
• Antacids decrease antibacterial efficacy
• NSAID (aspirin) in combination with
sulfonamides = crystaluria
• Sulfonamides and TMP are fenytoin
metabolism inhibitors (t0,5 extension by 40%)
Antimetabolites – interactions
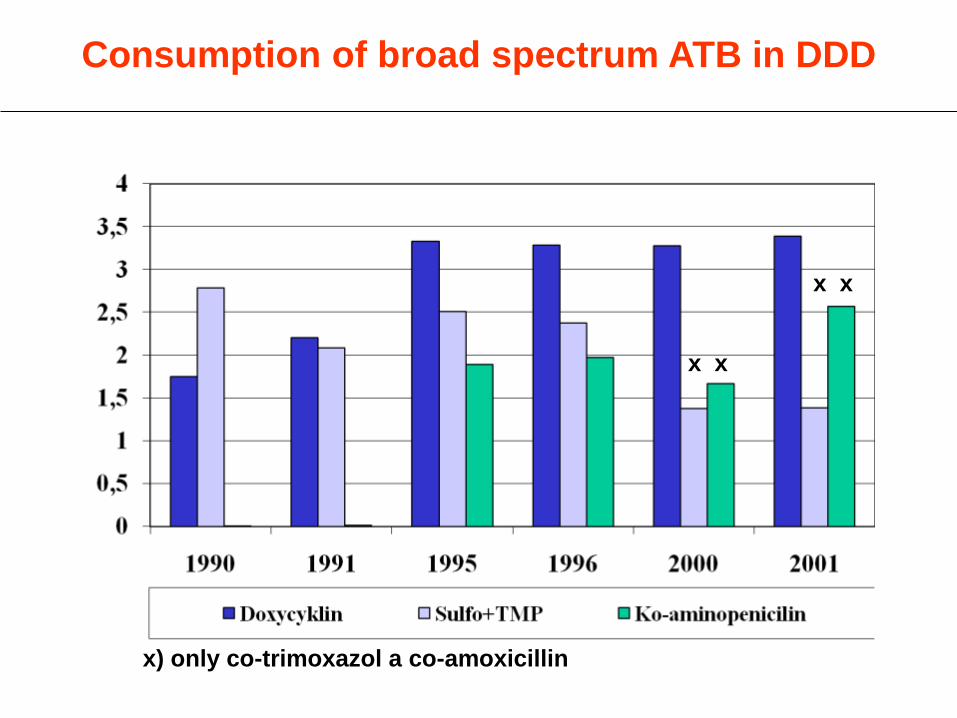
Consumption of broad spectrum ATB in DDD
x x
x x
x) only co-trimoxazol a co-amoxicillin
Amphenicols

Chloramphenicol - characteristics
• First synthetic ATB (1947)
• Broad spectrum bacteriostatic ATB
• Proteosynthetic inhibitor on 50S subunit
• Prevents incorporation of amino Ac into
newly synthesized peptides
• Spectrum: H. influenzae, N. meningitidis,
Bacteroides
• Indication – salmonella infections,
H. influenzae meningitis, sepsis including
anaerobic
Chloramphenicol - AE/IT
• Blood disorders
– Early: reversible, dose dependent, given by
means of Mode of action
– Delayed: irreversible - idiosyncrasy - aplastic
anemia with lethal outcome
• Grey children syndrome – alteration of
detoxicatoin (glucuronidation)
• Interaction – cytochrome P450
– OHA (PAD), phenytoin, warfarin – incerase of
plasma levels

Aminoglycosides

Aminoglycosides – characteristics (1)
• Broad spectrum bactericidal ATBs
• Mode of action – proteosynthetic
inhibition
• No oral absorptions - only parenteral
application possible
• Renal elimination - in RI dose
adjustment needed
• Do not penetrate BBB
Aminoglycosides – characteristics (2)
• Significant post antibiotic effect (PAE)
• Single daily dose = decrease of toxicity
• Toxicity depends more on length of
exposure then on height of dose
Aminoglycosides – mode of action
• Proteosynthetic inhibitor on 30S
ribosome subunit
• Alteration of recognition
codon/anticodon = wrong reading mRNA
= synthesis of incorrect bacterial
proteins
Aminoglycosides - resistance
• Inactivation of aminoglycoside by means of
microbial enzymes - 9 enzymes (plasmid encoded
resistance) netilmycin and amicacin are not
metabolized
• Metabolite does not interfere with proteosyntesis
• Alteration of penetration across bacterial wall –
prevented by means of combination with
penicillin or vancomycin
• Mutation of 30S subunit (streptomycin)

Aminoglycosides - antibacterial spectrum
• G- including P. aeruginosa
• Poor H. influenzae, Mycoplasms
• G+ less or not effective
• No effect (Bacteroides)
• Some AMG act as antituberculotics
(streptomycin)

Aminoglycosides - compounds
• Amicacin, gentamycin, tobramycin,
netilmycin, isepamycin
• Streptomycin, kanamycin
(antituberculotics)
• Neomycin (topical use in surgery - lavage)
• Spectinomycin (single dose - gonorrhea)
Aminoglycosides - AE
• Nephrotoxicity (reversible)
• Ototoxicity (irreversible)
• Neurotoxicity
• Curare-like effect (streptomycin)
• Worsening of AE - diuretics, dehydratation
• AE – depend on plasma level
• Plasma level estimation frequently necessary

Glycopeptides
Glycopeptides – mode of action (1)
Basic component of peptidoglycan: N-acetyl-
glukosaminmuramyl-pentapeptid.
• Transglycosilase, transpeptidase and D,D-
carboxypeptidase are responsible for building of
macromolecular structure .
• Transglycosilase connects muramyl parts
• Transpeptidase connects transversal links by means
of cleaving end alanin on both ends of the chain
• D,D - karboxypeptidase cleavs end D - ala and acts
as regulator
• Inhibit peptidoglycan growth (early phase of cell wall
synthesis of G+ microbes: conjugation with new
components of bacterial wall).
• Beta-lactams: late phase of synthesis – creation of
transversal links
• Beta-lactams act by means of PBP, glycopeptides on
substrate
• PAE vanco 1 - 2 h, teico 2 - 10 h
• Glycopeptides are active only against G+ (c.f. MoA)
• Combination with b-lact., Ag., Chino., Rif. possible
Glycopeptides – mode of action (2)
Most frequent: enterococci - Van A, B, C
• Van A: inducible van and teico - genetic
alteration, D - ala replaced by. D - lactate or D -
butyrate, gen transferred by means of
conjugation
• Van B: only in van. In genetically equipped
bacteria. Induced by low concentration of van.
Non plasmid.
• Van C: Chromosomal, only in van, insignificant
Glycopeptides - resistance
Fluorochinolones
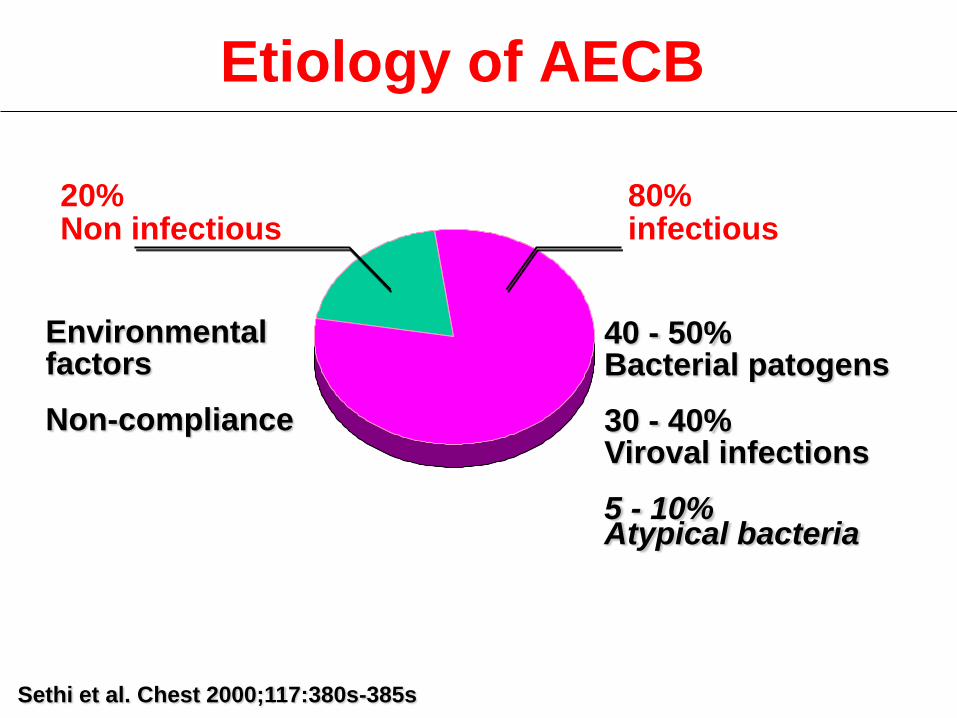
Etiology of AECB
Sethi et al. Chest 2000;117:380s-385s
80% infectious
20% Non infectious
40 - 50% Bacterial patogens 30 - 40% Viroval infections 5 - 10% Atypical bacteria
Environmental factors Non-compliance

Chinolones and fluorochinolones optimum
structure - optimum antimicrobial activity
1. Substitution on N1 (best cyclopropyl)
2. Double link between C2 and C3
3. On C3 carboxyl group
4. On C4 keto group
5. On C6 fluorine atom
6. On C7 substitution, most frequently piperazin,
resp. N4´ methyl piperazin (G-) or pyrolidin (G+)
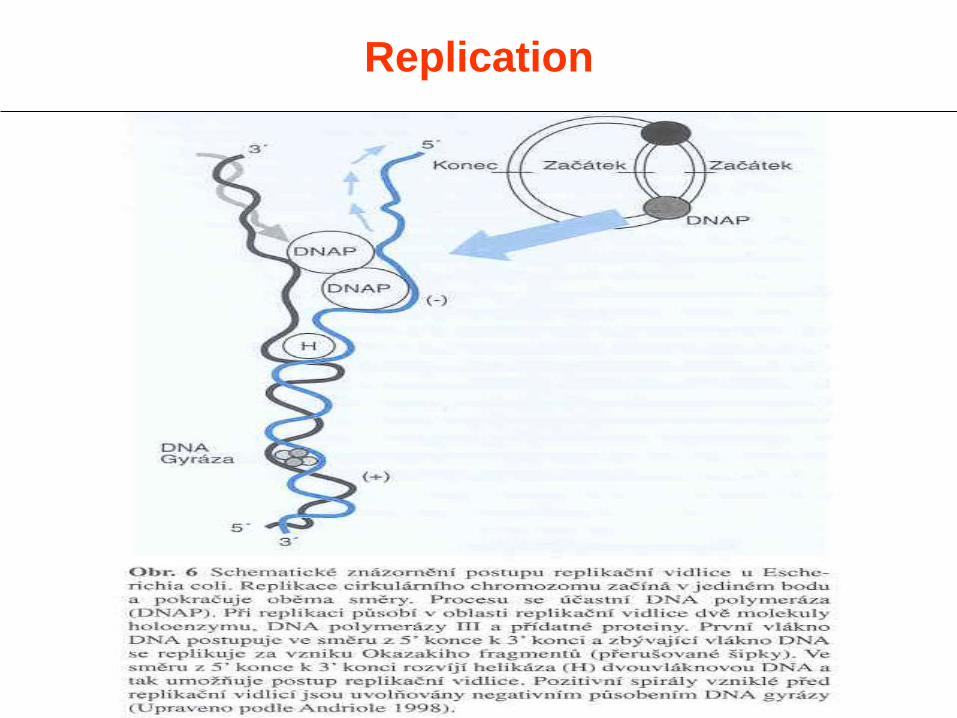
Replication

Classification of chinolones (Andriole 1998)
Nonfluorinated (I)
Fluorinated (II)
Fluorinated (III)
Fluorinated broad
spectrum (IV)
nalidixic ac. pipemidic ac. oxolinic ac. rosoxacin
norfloxacin ciprofloxacin ofloxacin pefloxacin enoxacin lomefloxacin fleroxacin rufloxacin
levofloxacin gatifloxacin sparfloxacin grepafloxacin temafloxacin
gemifloxacin sitafloxacin moxifloxacin clinafloxacin trovafloxacin alatrofloxacin*
*prodrug of trovafloxacin

Absorption - Cmax and
bioavailability (F) of fluorochinolones Chinolon Dose (mg) Cmax (mg/l) F (%)
norfloxacin ciprofloxacin ofloxacin pefloxacin enoxacin lomefloxacin fleroxacin rufloxacin levofloxacin sparfloxacin grepaflpxacin trovafloxacin gatifloxacin clinafloxacin gemifloxacin moxifloxacin
400 500 400 400 400 400 400 400 500 400 400 300 400 400 600 400
1,5 2,5 4,0 3,2 2,3 3,5 4,3 3,2 5,1 1,6 1,3 3,6 3,3 2,4 3,9 2,5
45 85 95 95 88 95 92 50 99 90 72 88 96 90 95 89
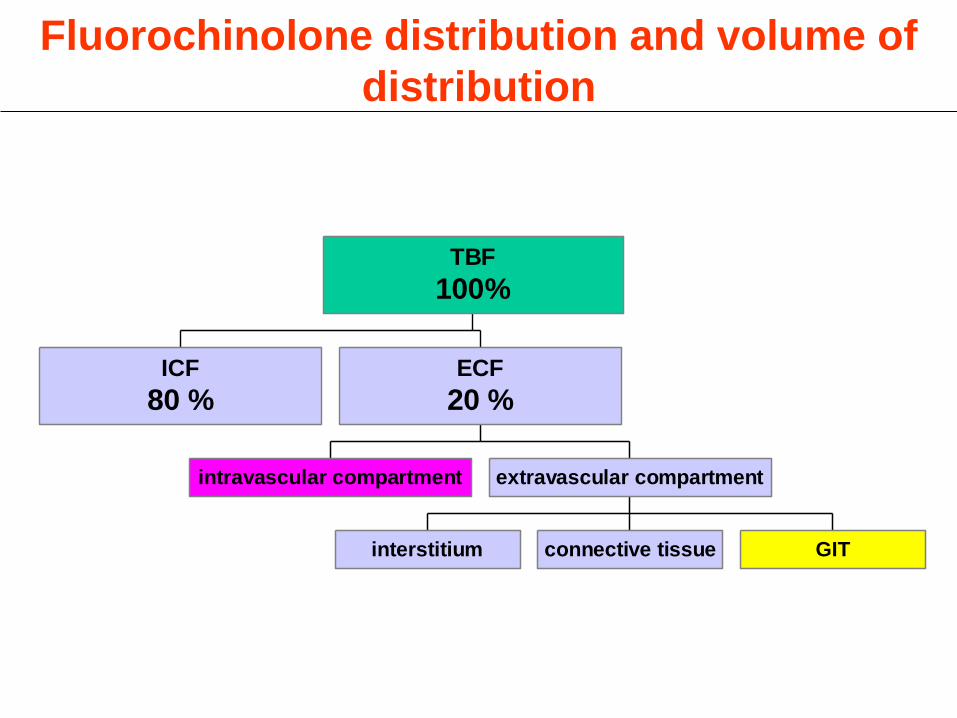
Fluorochinolone distribution and volume of
distribution
ICF
80 %
intravascular compartment
interstitium connective tissue GIT
extravascular compartment
ECF
20 %
TBF
100%

FCH Dose (mg) Binding (%) VD (l)
norfloxacin ciprofloxacin ofloxacin pefloxacin enoxacin lomefloxacin fleroxacin rufloxacin levofloxacin sparfloxacin grepaflpxacin trovafloxacin gatifloxacin clinafloxacin gemifloxacin moxifloxacin
400 500 400 400 400 400 400 400 500 400 400 300 400 400 600 400
14 35 25 30 40 10 23 70 35 45 50 70 20 55 70 48
225 195 102 112 175 133 110 149 101 350 560 84
118 150
* 250
Distribution of fluorochinolones (VD) and
protrin binding (plasma albumin)

Concentration of norfloxacine in plasma,
interstitial fluid and tissue (15 mg/kg i.v.)
mg/l * mg/kg
min
tissue
interstitial fluid
plasma
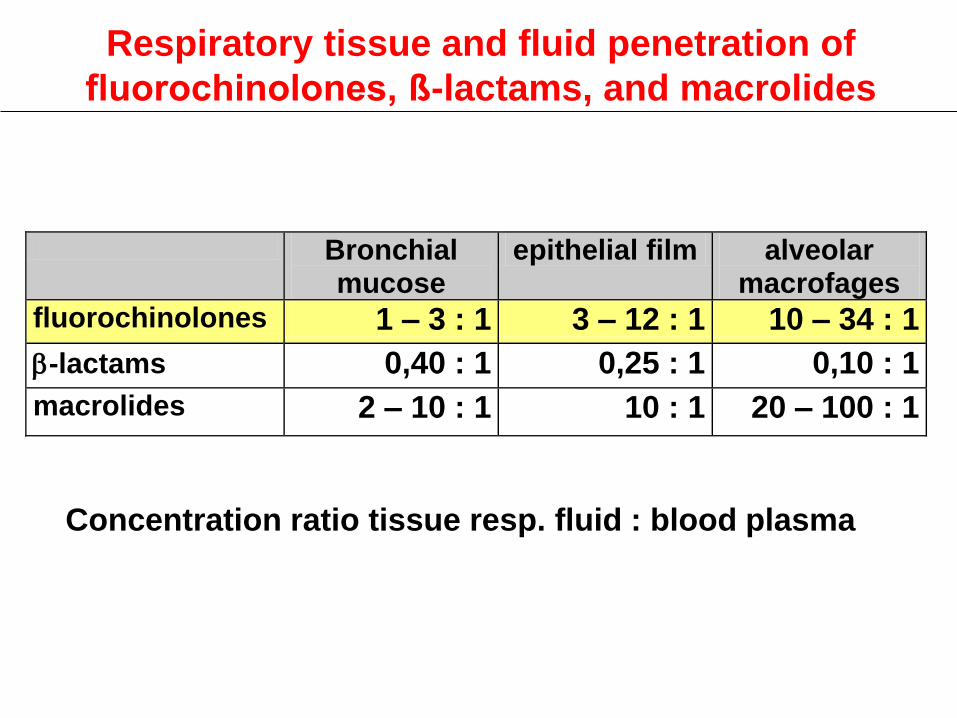
Bronchial mucose
epithelial film alveolar macrofages
fluorochinolones 1 – 3 : 1 3 – 12 : 1 10 – 34 : 1
b-lactams 0,40 : 1 0,25 : 1 0,10 : 1
macrolides 2 – 10 : 1 10 : 1 20 – 100 : 1
Respiratory tissue and fluid penetration of
fluorochinolones, ß-lactams, and macrolides
Concentration ratio tissue resp. fluid : blood plasma

Penetration, cumulation, localization
and efflux of the antibiotic from the cell
Antibiotics Penetration Cumulation Localization Efflux
aminoglycosides slow (days) very slow lysozomes very slow
b-laktams weak není cytosol fast
fluorochinolones fast 4 – 8 x cytosol fast
macrolides slow up to 100 x lysozomes cytosol
slow
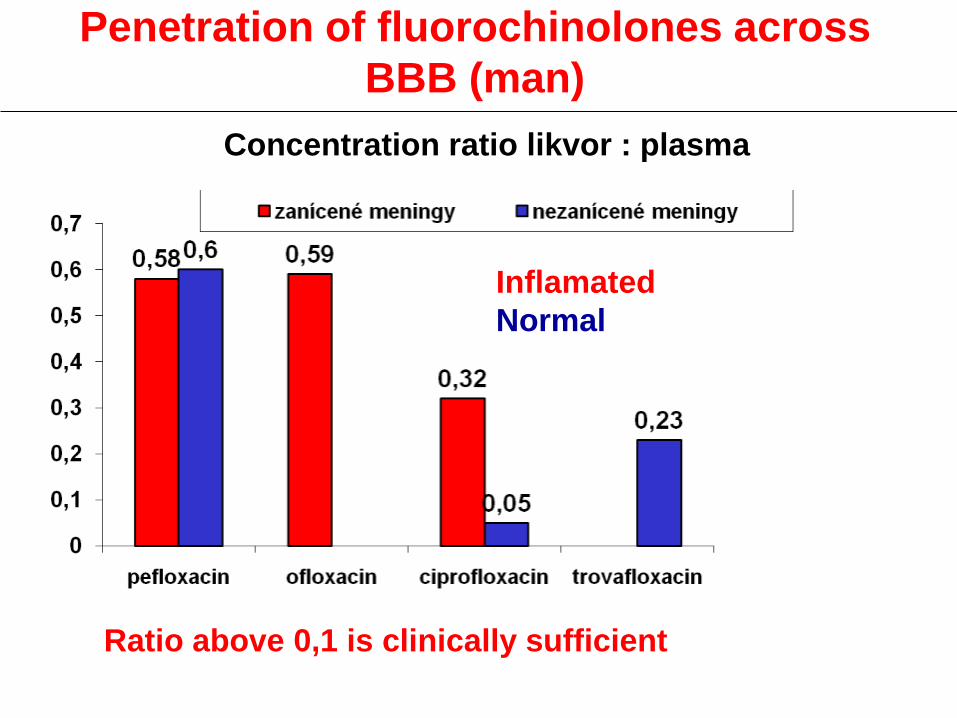
Penetration of fluorochinolones across
BBB (man)
Ratio above 0,1 is clinically sufficient
Concentration ratio likvor : plasma
Inflamated
Normal

Penetration of fluorochinolones across
BBB (model)
Concentration ratio likvor : plasma
Ratio above 0,1 is clinically sufficient
Inflamated
Normal

Bile excretion of fluorochinolones
(without obstruction)
Concentration ratio bile : plasma
Ratio above 0,5 is clinically sufficient

Elimination pathways of fluorochinolones
• Kidney
–ofloxacin, levofloxacin, lomefloxacin,
fleroxacin, rufloxacin, clinafloxacin,
gatifloxacin
• Liver
–pefloxacin, grepafloxacin
• Kidney + liver
–trovafloxacin, enoxacin, norfloxacin
• Kidney + liver + GIT
–ciprofloxacin, sparfloxacin
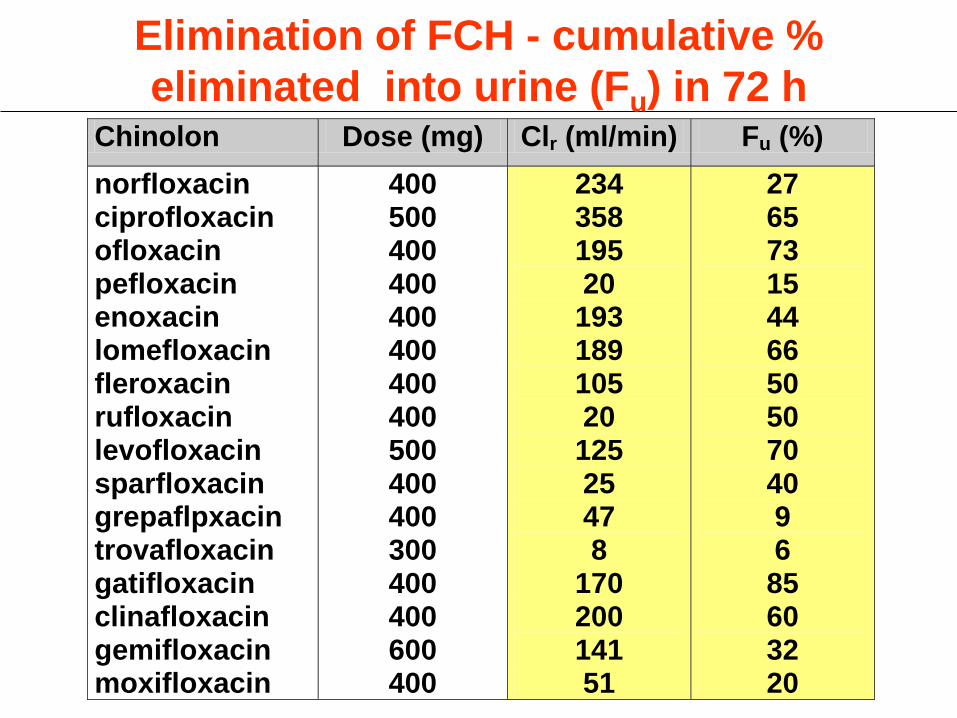
Chinolon Dose (mg) Clr (ml/min) Fu (%)
norfloxacin ciprofloxacin ofloxacin pefloxacin enoxacin lomefloxacin fleroxacin rufloxacin levofloxacin sparfloxacin grepaflpxacin trovafloxacin gatifloxacin clinafloxacin gemifloxacin moxifloxacin
400 500 400 400 400 400 400 400 500 400 400 300 400 400 600 400
234 358 195 20
193 189 105 20
125 25 47 8
170 200 141 51
27 65 73 15 44 66 50 50 70 40 9 6
85 60 32 20
Elimination of FCH - cumulative %
eliminated into urine (Fu) in 72 h
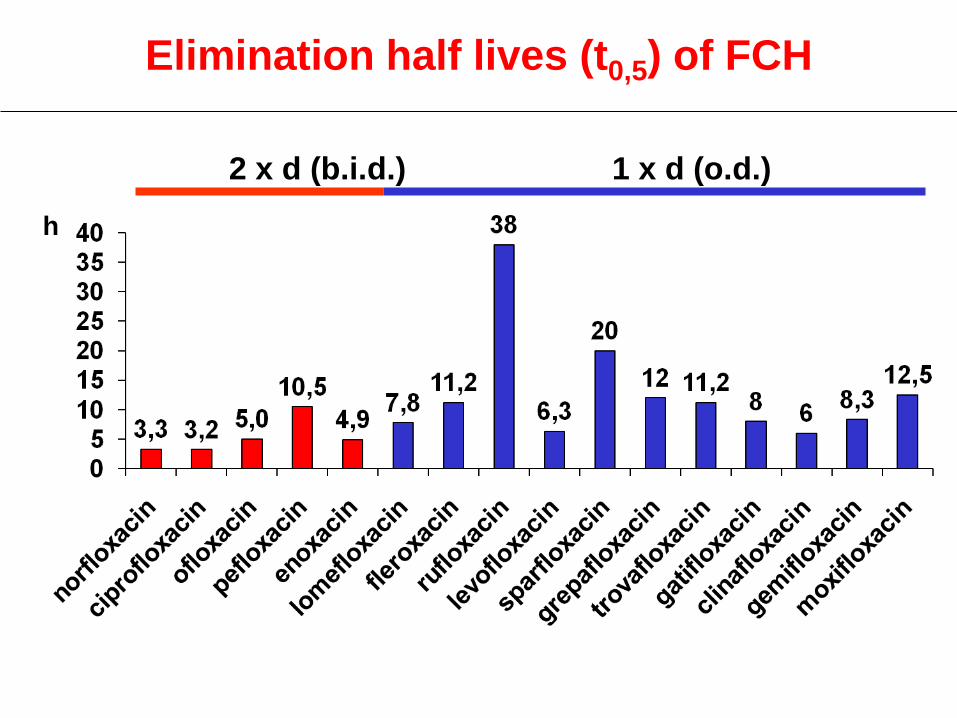
Elimination half lives (t0,5) of FCH
h
2 x d (b.i.d.) 1 x d (o.d.)
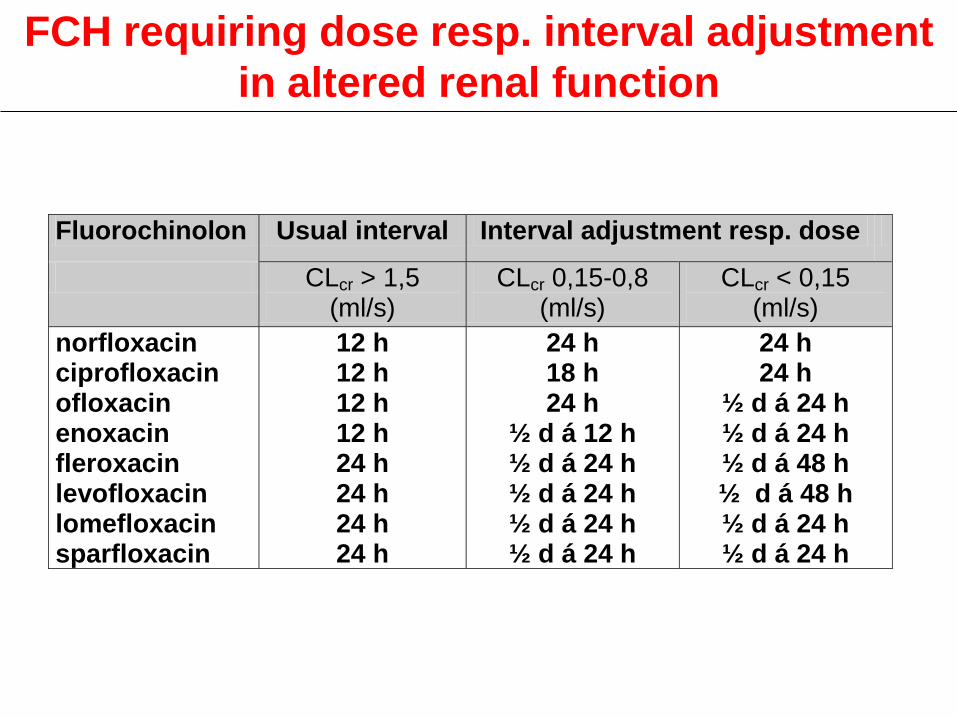
FCH requiring dose resp. interval adjustment
in altered renal function
Fluorochinolon Usual interval Interval adjustment resp. dose
CLcr > 1,5 (ml/s)
CLcr 0,15-0,8 (ml/s)
CLcr < 0,15 (ml/s)
norfloxacin ciprofloxacin ofloxacin enoxacin fleroxacin levofloxacin lomefloxacin sparfloxacin
12 h 12 h 12 h 12 h 24 h 24 h 24 h 24 h
24 h 18 h 24 h
½ d á 12 h ½ d á 24 h ½ d á 24 h ½ d á 24 h ½ d á 24 h
24 h 24 h
½ d á 24 h ½ d á 24 h ½ d á 48 h ½ d á 48 h ½ d á 24 h ½ d á 24 h
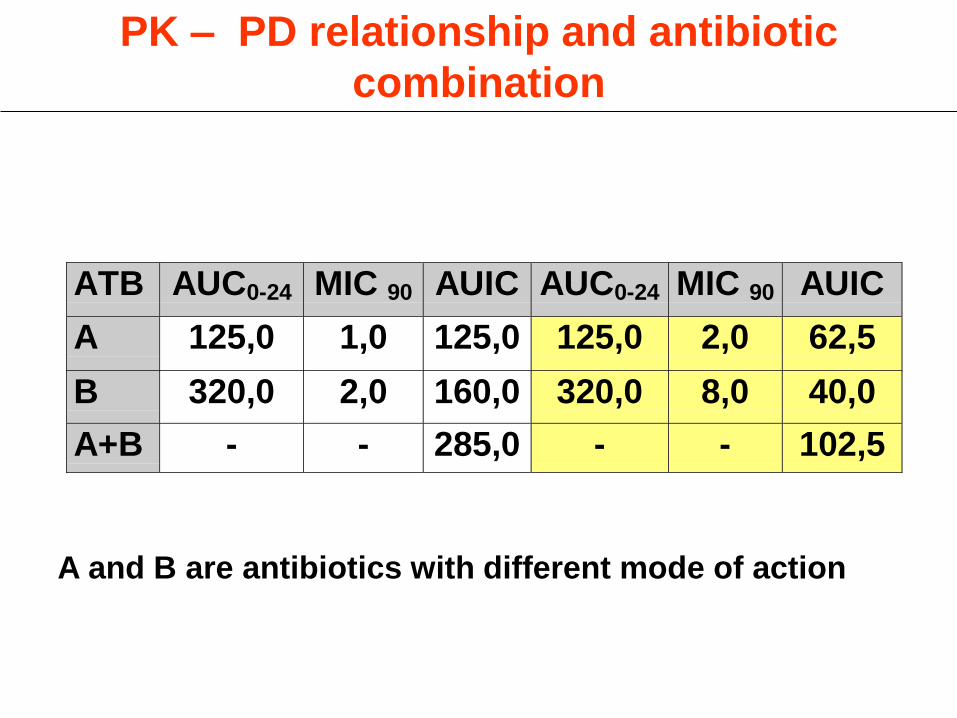
ATB AUC0-24 MIC 90 AUIC AUC0-24 MIC 90 AUIC
A 125,0 1,0 125,0 125,0 2,0 62,5
B 320,0 2,0 160,0 320,0 8,0 40,0
A+B - - 285,0 - - 102,5
PK – PD relationship and antibiotic
combination
A and B are antibiotics with different mode of action

Duration of PAE* (h)
Antibiotics Staphylo-coccus spp.
Entero-bacteriaceae
Pseudomonas
Penicilins – 2 0,5 – 2 0,5
Cefalosporins – 2 0,5 – 2 0,5
Aminoglykosides 2 – 4 2 – 6 2 – 6
Macrolides 3 – 6 3,5 – 6 –
Fluorochinolones 2 – 4 2 – 6 2 – 6
*Extention of suppression of bacterial growth after short
Exposure to antibiotics in vitro

Number of patients needed to record rare B
type AE*
Incidence 1 2 3
1 : 100 300 480 650
1 : 200 600 900 1 300
1 : 1 000 3 000 4 800 6 500
1 : 2 000 6 000 9 600 13 000
1 : 10 000 30 000 48 000 65 000
* AE type A given by pharmacological – predictable
AE type B are rare – non predictable

AE of fluorochinolones highest dose without
fototoxicity (mg/kg)*
(log conc..)
*experimental data Andriole, 1998
18
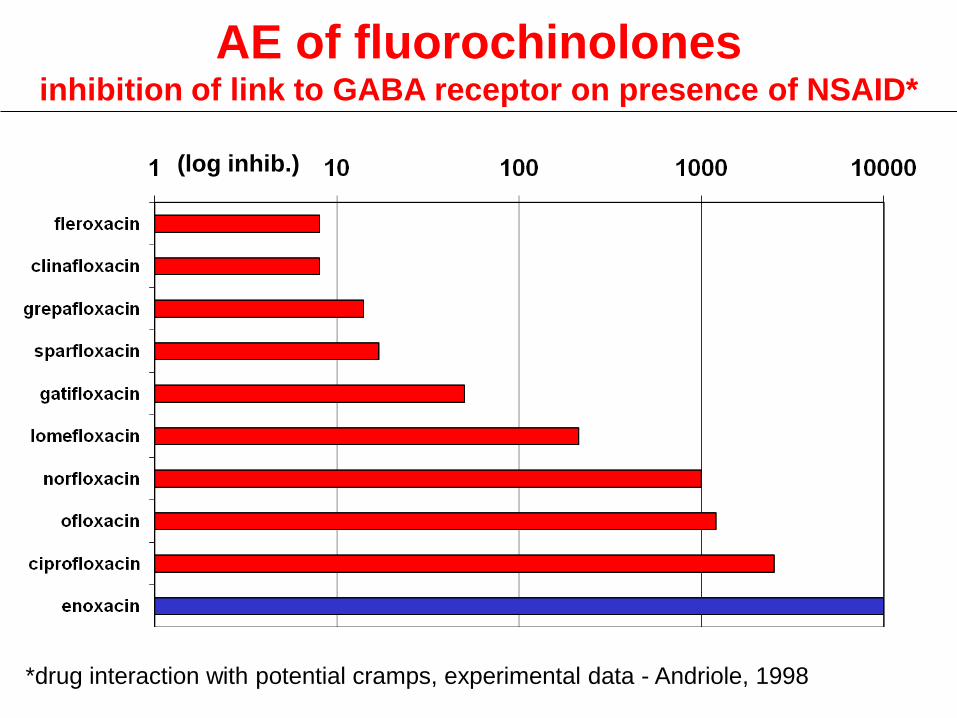
AE of fluorochinolones inhibition of link to GABA receptor on presence of NSAID*
(log inhib.)
*drug interaction with potential cramps, experimental data - Andriole, 1998

• Hepatotoxicity - trovafloxacin (B)
• Elongation of QT interval - grepafloxacin (?)
• Temafloxacine syndrom - temafloxacin (B),
• Hypoglycemia - clinafloxacin (B)
• Phototoxicity - sparfloxacin (A)
• Artropathy in exp. Animals - all ch. (A)
Some AE of chinolones
• Elongation of QT interval : without relation to
P450 mainly in predisposed, incidence 3,7: 1M,
improper combination with e.g. cisapride,
astemizole and terfenadine
• Temafloxacine sy.: hemolytic - uremic syndrome
probably immune reaction, incidence 1: 1000
• Artropathy: probably based on generation of
chelates, mainly uptake of Mg++ creation of
radicals alteration of chondrocytes
Some AE of chinolones

Interaction of chinolones
Concomitant medication (B)
Result of interaction (A+B)
antacids containing Mg, Al
sucralfat, Bi Decreased of bioavailability
Fe, Ca of chinolone (A)
H2 antihistamines*
*metabolised by cytochrome P450
Responsibility for interactions is attributed to piperazin on C6,
Methylation of piperazin results decrease of interactions
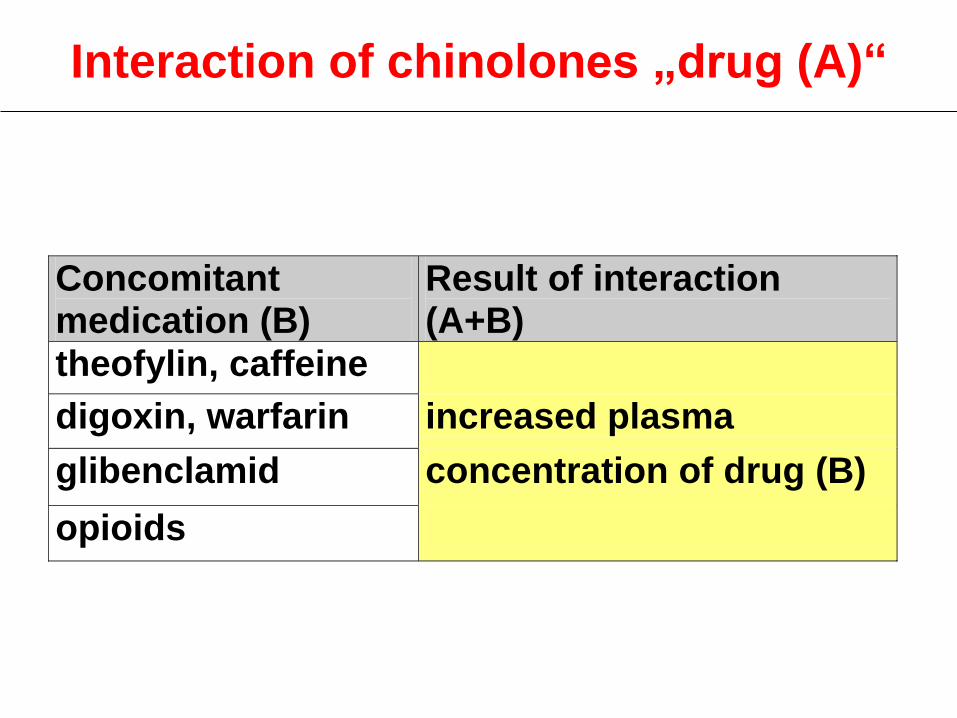
Interaction of chinolones „drug (A)“
Concomitant medication (B)
Result of interaction (A+B)
theofylin, caffeine
digoxin, warfarin increased plasma
glibenclamid concentration of drug (B)
opioids

Interaction of chinolones: influence on enzyme
activity of various isoforms of cytochrome P450
Isoform Inhibitor Inducer
CYP1A2 chinolones: pipemidic ac., enoxacin, grepafloxacin, pefloxacin, ciprofloxacin, ofloxacin
rifampicin
14C macrolides: erythromycin, klarithromycin, roxirthromycin, dirithromycin
CYP3A4 chinolony rifampicin
14C macrolides imidazoly: ketokonazol, itrakonazol, flukonazol
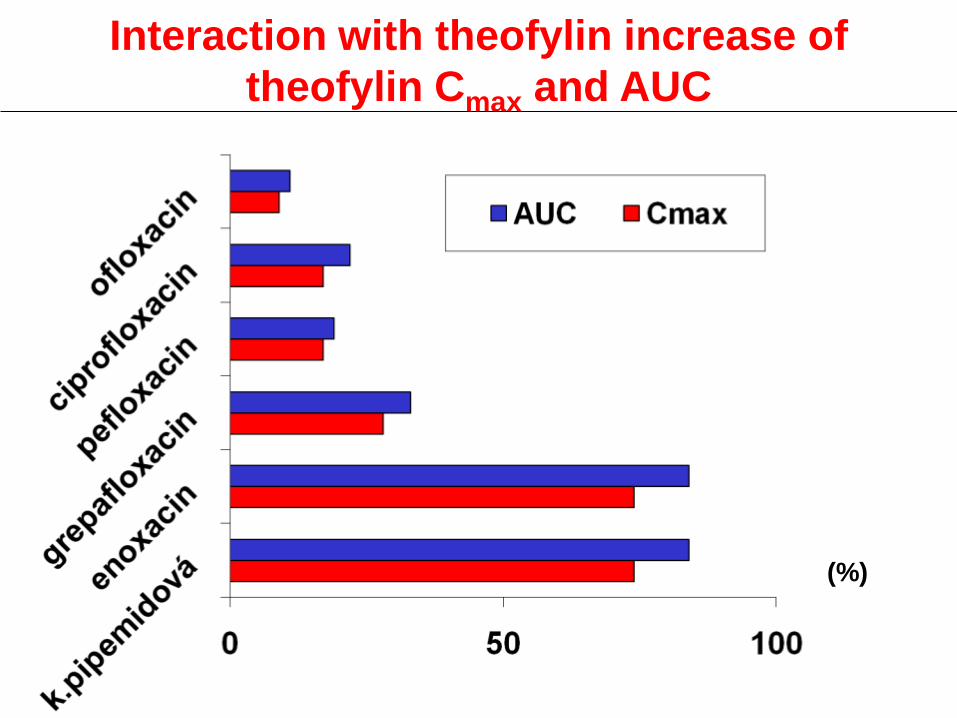
Interaction with theofylin increase of
theofylin Cmax and AUC
(%)

• Oxazolidinon – proteosyntetic inhibitor (binds
on 23s subunit 50s – prevents 70s complex
necessary for translation
• Bioavailability p.o. – 100%
Linezolid
Linezolid
• Selective proteosyntetic inhibitor a non-
selective MAO inhibitor - oxazolidin
• Indication G+ infection, including serious
nosocomial
• G+ including MRSA and VRE a PNC/ERY
resistant streptococci
• In mixed G+/G- infection combination
necessary
• Non cross resistance VRSA and MRSA
• No activity in atypical microorganisms
• Recommended only by ATB centers
• KI cf. interaction with iMAO

















