18
U07-1845 #844043110 • 54 y.o. male • Deceased donor renal transplant April 18/06 (APCKD) • Creat 120 170 515 • Being treated for CMV • Rejection?
| Date post: | 30-Dec-2015 |
| Category: |
Documents |
| Upload: | jaquelyn-porter |
| View: | 66 times |
| Download: | 0 times |

U07-1845
#844043110
• 54 y.o. male
• Deceased donor renal transplant April 18/06 (APCKD)
• Creat 120 170 515
• Being treated for CMV
• Rejection?
• 54 yrs old male
• Status post deceased donor renal transplant (April 2006) baseline SCr 100-120
• He had ESRD secondary to APCKD.
• CMV D /R, EBV D/ R, Mismatch HLA antigens
• Medications: – Cellcept,Tacrolimus, prednisone
• Past history:– Legally blind (retinitis pigmentosa), – HTN– Dyslipidemia

• 2-3 weeks ago developed leukopenia, Cellcept dose decreased
• No change in U/O
• Jan 13 2007 CMV PCR 23,950 copies/ml (peak 55,000 copies/ml)
• 18 Jan started on Gancyclovir, 26 Jan SCr 140 next day 178 then 2 days 515
• Hb 105 plate 203 WBC 5.5 LDH normal Bilirubib 11
• U/A: +3 protein , +1 Hb

• Doppler u/s: no diastolic flow, patent renal vein
• U/S: no hydronephrosis
• Renal scan: severely impaired perfusion

IF• IgG- Negative.• IgA- Negative.• IgM- Mild to moderate mesangial staining. Moderate vascular
staining.• C3- Moderate vascular staining including peritubular
capillaries.• C1q- Negative.• Kappa- Negative.• Lambda- Mild vascular staining. • Fibrinogen- Moderate interstitial staining. Moderate staining
of thrombi in peritubular capillaries and glomerular capillaries.• Albumin- Negative.

IgM

C3

C3

lambda

fibrinogen

fibrinogen

fibrinogen

IF
• C4d: Moderate linear peritubular capillary staining. Mild to moderate endothelial staining in small arteries.
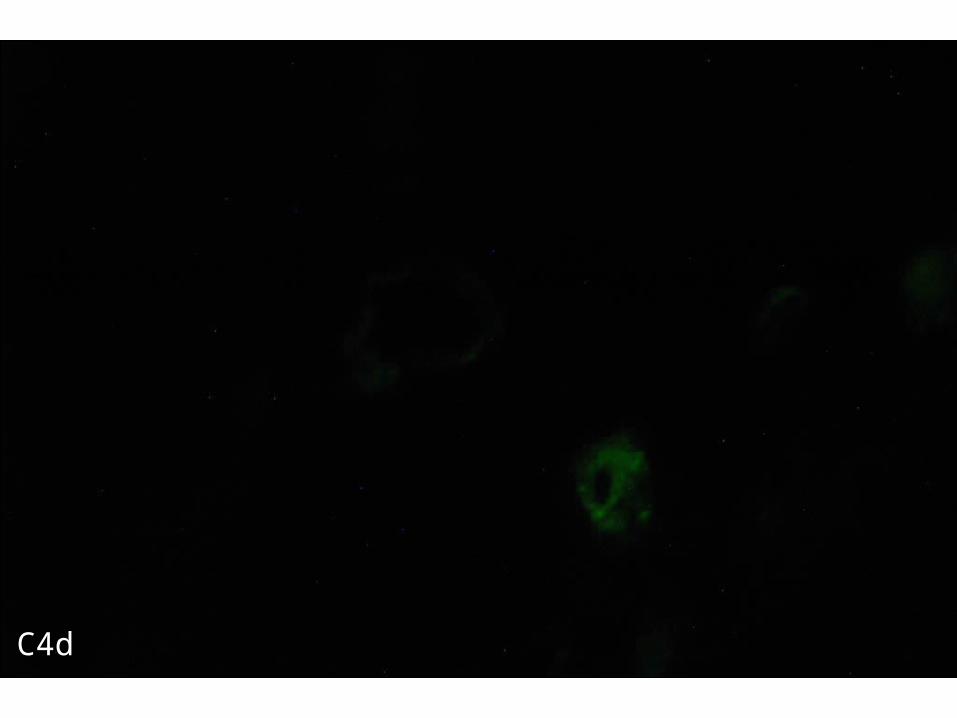
C4d

C4d

C4d
EM
• Is pending

DiagnosisRenal Biopsy:• Probable antibody-mediated rejection with
thrombotic microangiopathy manifested – in glomeruli with extensive glomerular capillary
thrombosis
– and congestion and thrombosis in peritubular capillaries.
• No evidence of T-cell mediated rejection.• Banff scores:
– G0 CG0 I0 CI0 T0 CT0 V0 CV1 AH0 MM0 PTC0













![ÈÅÛ «B Regular Class A ]cB ] ]d]! 7 Advanced Class C...Regular class B ¥î«c Â#Ý e8 2) 4) 7) 8) >| 11) 13) 14) 7VC '¨H 'v U0 6õ X '¨H ( U0 6õ X H H M+á0 Fø < Ø](https://static.documents.pub/doc/80x56/5f2e2d45e9473b38f5248d42/-b-regular-class-a-cb-d-7-advanced-class-c-regular-class-b-c.jpg)



