49
AUCD Association of University Centers on Disabilities UCEDD Directors Meeting December 2, 2012 3:15‐6:15 pm 1

A U C DAssoc ia t ion of Univers i ty Centers on Disabi l i t ies
UCEDD Directors Meeting
December 2, 20123:15‐6:15 pm
1

A U C DAssoc ia t ion of Univers i ty Centers on Disabi l i t ies 2
Welcome

A U C DAssoc ia t ion of Univers i ty Centers on Disabi l i t ies
Timm Vogelsberg, PhD (MT)
Judy Struck, MD (SD)
3
Recognition

A U C DAssoc ia t ion of Univers i ty Centers on Disabi l i t ies
Native American DD Needs Assessment PCPID 2012 Report to the President Involving People w/ Most Significant Disabilities Capacity Building Tool‐kit Minority Partnerships report UCEDD Annual Report
4
UCEDD TA Updates

A U C DAssoc ia t ion of Univers i ty Centers on Disabi l i t ies
Allies in Self‐AdvocacyFinal Summit ReportPromotional videoState team progressListservOrganizational Development Mini‐grantsUpdated website www.AlliesInSelfAdvocacy.org
5
UCEDD TA Updates

A U C DAssoc ia t ion of Univers i ty Centers on Disabi l i t ies
UCEDD National Salary Survey ‐ elementsDirector & associate director $, degree, longevityUCEDD admin. home, budget, FTEUniversity Carnegie classificationSalary sourceUniversity support for UCEDD
UCEDD Evaluation Plans
6
Upcoming Requests

A U C DAssoc ia t ion of Univers i ty Centers on Disabi l i t ies 7
Self‐Advocacy Online
Amy Hewitt, PhD www.SelfAdvocacyOnline.org
A U C DAssoc ia t ion of Univers i ty Centers on Disabi l i t ies
3 major effortsAIDD/AUCD FellowshipAUCD Policy FellowshipUCEDD Leadership Institute
Wonderful opportunities for early‐mid career network members and trainees
Strongly encouraging applicants with cultural, ethnic, linguistic diversity
8
Leadership Development

A U C DAssoc ia t ion of Univers i ty Centers on Disabi l i t ies
Sue Fox, Associate UCEDD Director, IOD, NH
9
UCEDD Leadership Institute

A U C DAssoc ia t ion of Univers i ty Centers on Disabi l i t ies
Mette Pedersen, PhD, 2012‐2013 Fellow Applications due December 15 for 2013‐2014!
10
AIDD/AUCD Fellowship

A U C DAssoc ia t ion of Univers i ty Centers on Disabi l i t ies
Kristina Majewski, JD, 2012 Fellow Applications for 2013 due now!
11
AUCD Disability Policy Fellow

A U C DAssoc ia t ion of Univers i ty Centers on Disabi l i t ies
Martha Roherty, Executive Director, NASUAD www.nasuad.org
12
Partnership

A U C DAssoc ia t ion of Univers i ty Centers on Disabi l i t ies
BREAK10 minutes
Don’t miss a minute of the ACA!
13

KimMushenoAUCDDirectorofLegislativeAffairs
RachelPattersonAUCDPolicyAnalyst
Health Care Reform Update2012 AUCD Annual Meeting
UCEDD Directors

Impact of election
Affordable Care Act will not be repealed
ACA will continue to be implemented by HHS Secretary Kathleen Sebelius
Medicaid will not be block granted
Medicare will not be fundamentally altered
House bills to consolidate and cut education and employment programs will not pass
Bills to weaken the ADA will not pass
Cuts to discretionary programs will not be as severe
Still need bipartisan support to pass any bill

Public Law 111-14 Historic Legislation
Patient Protection and Affordable Health Care Act
and the
Health Care and Education Reconciliation Act
Signed into LAW on March 23, 2010
16

Purpose
• Expands coverage and access
• Transforms focus from treating sickness to preventing illness and promoting wellness
• Strengthens protections for people with disabilities who have been discriminated based on pre-existing conditions or health status
• Goal to achieve health equity and reducing health disparities
• Bending the Cost Curve over time
17

Insurance Market Reforms
18
“Guaranteed issue and renewability” –Insurance companies must not deny anyone
“Medical loss ratio” means 80‐85% of premiums must be spent on medical care, not on advertising
or CEO paychecks‐‐Or you get money back!
Regulations require insurers to justify any unreasonable rate increases

“Individual Mandate”
Everyone must share responsibility for lowering costs and covering more people
19

Expanding Coverage
Temporary high‐risk pools
Small business tax credits to cover employees
Premium subsidies (133‐400% FPL)
Employer & individual responsibility
Medicaid expansion – 133% of FPL covered
Insurance Exchanges – more coverage, increased competition, lower costs

Expand Coverage: Medicaid
Expands Medicaideligibility for everyone up to 133 % of Federal Poverty Level (2014)
• Up to $14,600/ individual
• $29,400 /family of four
Federal share of costs to states:
• Administration lower than private insurance
• States will receive100% for newly eligible first 3 years (2014 – 2016)
• Phases down to 90% for 2020 and subsequent years
Estimated to cover 17 million more
in 2014
Efficient
more info: www.kff.org
Cost‐effective Humane

Health Insurance Exchanges
22
Exchange = = Market
If you can’t get MedicaidYou can shop in the
marketplace for insurance with government subsidies
Making Coverage Affordable
Subsidies for marketplace comes in form of Tax Credits provided for individuals/families between 133% ‐ 400% Federal Poverty
Approximately
Up to $43,000 individualUp to $88,000 family of 4
Paid by Government
directly to Insurer
Limits out of pocket costs:
Deductibles, Coinsurance, Copayments
HOW?

Essential Benefits Package for Exchanges and Medicaid
Services Everyone Expects to be Covered by their Insurance
24
Hospitalization, emergency services,
ambulance Prescription drugs and laboratory services
Rehabilitative and habilitative services
and devices
Mental health and substance use disorder services
including behavioral health treatment
Preventative and wellness services and
chronic disease management
Pediatric services including dental and vision care
Maternity and newborn care

HUGE Focus on Prevention and Wellness
Requires new plans to cover certain preventive and immunization services without deductible or co‐insurance (applies to Medicaid and Medicare)
One percent federal Medicaid share increase for States if it covers clinical preventive services
Grants to provide state incentives to Medicaid beneficiaries who successfully participate in a wellness program
$11 billion increase FY 2011 for Community Health Centers
25

Prevention and Wellness
26
• Coordination and goals
National Prevention Council
• $7 billion (FY 2010‐2015); $2 billion/yr (FY2015+)
• Sen. Coburn “prevention and public health slush fund”
Prevention and public Health Fund for
transformational sustainedinvestments
• Community Transformation Grants• Comprehensive workplace wellness programs• Education and Outreach Campaign• Oral health prevention
Numerous Prevention and wellness programs such as:

Increasing and Improving the Workforce
National Health Care Workforce Commission established
Oral Health: Grants for dental and dental hygiene
schools, residency programs, public health programs
Increases Medicaid reimbursement for
primary care physicians and pediatricians to Medicare rates (2013 and 2014)
Primary Care Training Grants for Medical Schools • training on treating individuals with disabilities priority population

Accessibility
Access Board (under the Rehab Act) establish standards for accessibility of
medical diagnostic equipment
Includes • examination tables and chairs
• mammography equipment
• x‐ray machines

Understanding Health Disparities:Data Collection
29
Requires government to collect health survey data from people with disabilities to enable better understanding of the health of people with disabilities compared to other minority groups.
Requires HHS to survey health providers to asses access to care and treatment for people with disabilities.
Requires development of recommendations for quality measures to improve the quality of health care for individuals with disabilities.

New State Incentives for Community Living
30
Community First Choice State Option• new Medicaid state plan option (beginning Oct. 2011) to provide comprehensive home and community‐based attendant services and supports for individuals who are eligible for an institutional level of care
Reforms 1915(i) State Option• Allows states to provide HCBS services without a waiver
Grants to assist states to balance their Medicaid systems in favor of community
Extends Money Follows the Person grants
CLASS Act – Community Living Assistance, Services and Supports Act

Legal ChallengeWon (mostly)
Congressional Challenges continue
31
Challenges to Health Reform

Supreme Court Decision
Court upheld the individual mandate as constitutional exercise of Congress’ power
to levy taxes
Medicaid expansion is unconstitutionally coercive of states• Power of Secretary to withhold all existing funds for state non‐compliance
Bottom line –Medicaid expansion
in ACA is now an option

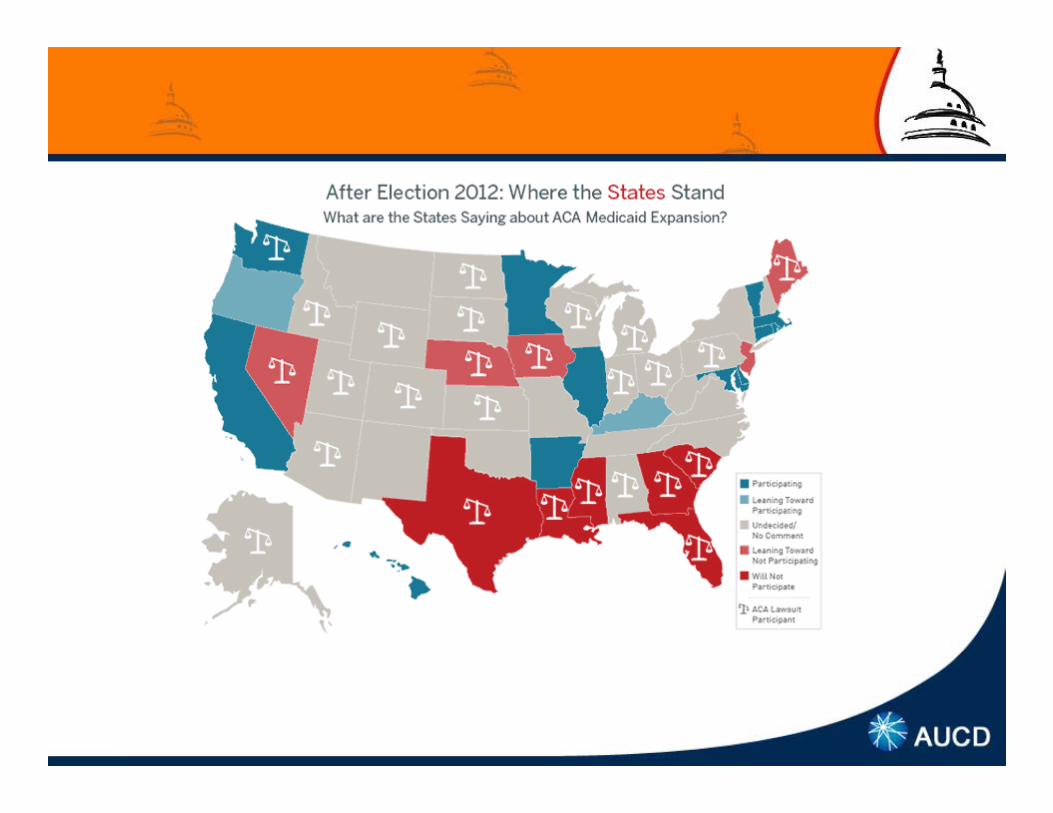
Medicaid expansion
4 Republican governors do not plan to join in the
expansion16 yes
No deadline for states to decide on joining the expansion and
they can drop out at any time
Partial expansion? • E.g. limit enrollment to people with income up to 100 percent of the FPL rather than 133 %
Will Congress slash Medicaid
budget?

Cutting Medicaid
Block grants off the table, but
Per Capita Caps still under discussion
Limitations on Medicaid provider taxes
Blended match rate
Limit federal reimbursement for certain expenses

Election Impact - Exchanges
States must have Exchanges ready by Jan. 2013
States took “wait and see approach” – now not ready
Secretary extended deadline for application from Nov. 16 to Dec. 14 (if partnership Feb. 15)
Two new Rules on Exchanges to come out soon
Election Impact


Managed Long-Term Services and Supports
Source: AARP, On the Verge: The Transformation of LTSS
As of February 2012

MLTSS – Power Tools
Benefits ConcernsRebalancing Fast implementation
Primary and Coordinated Care
Limited experience from states or MCOs
Cost containment Mandatory or passive enrollment Consumer protection
Lack of quality measures

MLTSS – Where UCEDDs are Needed
Quality measures focused on long term quality‐of‐life outcomes

Duals Demos

Duals Demos
Benefits Concerns
Medicare‐Medicaid coordination
Demonstration overreach
Care coordination Passive enrollment
Cost containment Consumer protection
Rebalancing Need for evaluation
Lack of experience from states or MCOs

Duals Demos – Where UCEDDs are Needed
Public Engagement
Monitoring and Evaluation

What you can do
Speak up and advocate for the
Affordable Care Act
Volunteer your expertise to help plan
Coordinate with state partners• National Academy for State Health Policy
• National Association of Insurance Commissioners
• National Association of State Medicaid Directors

Resources
AUCD Health Reform HUB: http://www.aucd.org/healthreformhub• Text of the law• Detailed summaries and analyses
• Implementation resources• Archived webinars on 4 topics
US Dept. of Health and Human Services:
http://www.healthcare.gov/
Kaiser Family Foundation:
http://www.kff.org/
45

46
Questions?
Thank You

A U C DAssoc ia t ion of Univers i ty Centers on Disabi l i t ies
Is your state considering any of the following: Managed Long Term Services & Supports (MLTSS) Dual eligibility demonstrations Expanding Medicaid Setting up healthcare exchanges
How are these issues being addressed in your state (task force, etc.)? How are experts being chosen to advise the process? How did you, or can you, get involved? Do you use AUCD’s Health Care Hub?
What else would be helpful to include?
How else can AUCD assist through TA?
47
Table Discussions

A U C DAssoc ia t ion of Univers i ty Centers on Disabi l i t ies 48
Implications for TA

A U C DAssoc ia t ion of Univers i ty Centers on Disabi l i t ies 49

















