22
Medical Council of India Proposed UNDER GRADUATE MEDICAL EDUCATION Undergraduate Education Working Group 2010 1 1 Final Medical Council Of India
| Date post: | 08-Apr-2018 |
| Category: |
Documents |
| Upload: | andrea-diaz |
| View: | 218 times |
| Download: | 0 times |

8/7/2019 UG-medical-education
http://slidepdf.com/reader/full/ug-medical-education 1/22
Medical Council of India
Proposed
UNDER GRADUATE MEDICAL EDUCATION
Undergraduate Education Working Group2010
1
1 Final Medical Council Of India
8/7/2019 UG-medical-education
http://slidepdf.com/reader/full/ug-medical-education 2/22
2
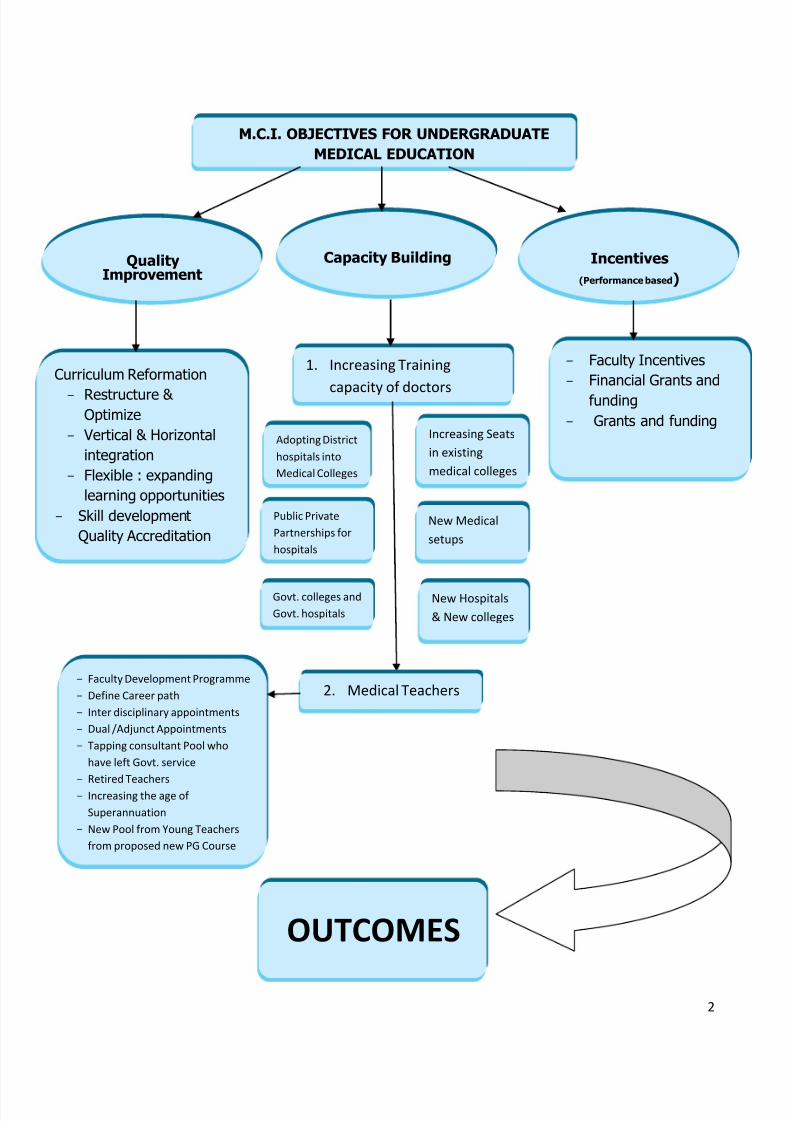
QualityImprovement
M.C.I. OBJECTIVES FOR UNDERGRADUATEMEDICAL EDUCATION
Curriculum Reformation
- Restructure & Optimize
- Vertical & Horizontalintegration
- Flexible : expandinglearning opportunities
- Skill developmentQuality Accreditation
1. Increasing Training
capacity of doctors
Capacity Building Incentives(Performance based )
- Faculty Incentives- Financial Grants and
funding- Grants and funding
Increasing Seatsin existingmedical colleges
New Medicalsetups
New Hospitals& New colleges
Adopting Districthospitals intoMedical Colleges
Public PrivatePartnerships forhospitals
Govt. colleges andGovt. hospitals
2. Medical Teachers- Faculty Development Programme- Define Career path- Inter disciplinary appointments- Dual /Adjunct Appointments- Tapping consultant Pool who
have left Govt. service- Retired Teachers- Increasing the age of
Superannuation- New Pool from Young Teachers
from proposed new PG Course
OUTCOMES

8/7/2019 UG-medical-education
http://slidepdf.com/reader/full/ug-medical-education 3/22
3
Motivating Career Pathwaysfor Students and Teachers
EXPECTED
OUTCOMES
Short Term Middle Term Long Term
Improved and RevisedCurriculum
Detailed Capacity BuildingPlan
Faculty DevelopmentProgrammes in Place
Improved Quality of Existing Colleges
Sufficient Number of Trained Teachers
- Sufficient Number of
Doctors- Improved Medical
Education- Improved Doctor: Patient
Ratio- Equitable Distribution of
Doctors in Urban-RuralAreas
Improved HealthParameters
Improved Health Care
IMPROVING QUALITY OF MEDICAL CARE
FOR PATIENTS
8/7/2019 UG-medical-education
http://slidepdf.com/reader/full/ug-medical-education 4/22
4
Medical Council of IndiaCurricular reform in Undergraduate Medical Education
INTRODUCTION
The Government of India recognises Health for All as a national goal and expects medical trainingto produce capable "Physicians of First Contact" towards meeting this goal. However, the Indianhealth care and medical education is facing systems and standards challenges.
The burden of diseases in India is still large. Even though there has been some improvement,national statistics reveal wide disparities between different states as also rural/urban areas withregard to access to basic medical services and quality health care. These are attributed tophysician shortage, both generalist and specialist, inequitable distribution of manpower andresources, and deficiencies in the quality of medical education.
India has the highest number of medical colleges in the world. This unprecedented growth hasoccurred in the past two decades in response to increasing health needs of the country. The mostsignificant challenge for regulatory bodies has been to balance the need for more medical collegeswith the maintenance of quality standards. The globalization of education and health care andIndia’s potential as destination for education and quality health care has brought the issue intosharper focus.
Curricular reform to systematically address the issues and develop strategies to strengthen themedical education and health care system is a logical next step. There is a need to create systemsand standards that establish and promote state-of-the-art medical education, so that Indianmedical graduates from all institutions are comparable to the best from anywhere in the world.
Additionally, though recent advances in medicine have been understood and adopted by medicaland other health science institutions, the same is not true for new methods and strategies inmedical education. There is an urgent need to build capacity in this area.
To address the above challenges, the Board of Governors, Medical Council of India constituted theundergraduate and postgraduate working groups in July 2010 to develop a Vision 2015 inalignment with the following mandate.
1. To evolve a roadmap for the direction of medical education in India in alignment withnational needs..
2. To evolve a broad policy regarding the emphasis, duration and curricular changes thatcould be adopted as future strategies to make medical education in India comparable toglobal standards.
3. To evolves strategies and futuristic plans so that medical education in India is innovativeand is able prepare undergraduates to be able to perform in the changing scenario ofmedical science.
4. In the light of deteriorating medical education standards in the country, to work on parallel
tracks for immediate solutions and long term improvement in a steady, phased manner.

8/7/2019 UG-medical-education
http://slidepdf.com/reader/full/ug-medical-education 5/22
8/7/2019 UG-medical-education
http://slidepdf.com/reader/full/ug-medical-education 6/22
6
MEDICAL COUNCIL OF INDIA’S MANDATE FOR MEDICAL EDUCATION
The Board of Governors, Medical Council of India constituted the undergraduate andpostgraduate working groups to develop a Vision 2015 in alignment with the followingmandate.
1. To evolve a roadmap for the direction of medical education in India.
2. To evolve a broad policy regarding the emphasis, duration and curricular changes thatcould be adopted as future strategies to make medical education in India comparable toglobal standards.
3. To evolves strategies and futuristic plans so that medical education in India is innovativeand is able to meet the demands of national needs while preparing undergraduates to beable to perform in the changing scenario of medical science.
4. In the light of deteriorating medical education standards in the country, to work on paralleltracks for immediate solutions and long term improvement in a steady, phased manner.
THE UNDERGRADUATE WORKING GROUP MANDATE
To review present statusTo rationalize and propose reforms

8/7/2019 UG-medical-education
http://slidepdf.com/reader/full/ug-medical-education 7/22
7
EXECUTIVE SUMMARY
Summary of Present Status -
1. Need for more doctors :The current doctor population ratio in India is 1:1700 when compared to a world averageof 1.5: 1000. The committee came to a consensus that targeted doctor population ratioshould be 1: 1000 by 2031. For achieving this target taking into consideration existingmedical colleges in the country, it was felt that the current intake of medical collegesand the critical mass of doctors should be doubled at least to achieve this target.
2. Improving quality of training: This is proposed as the following measures:-
I. Restructing of MBBS course - 4+1 model of training (4 years course with 6 monthselective+ 1 year internship); 1+1+2+1.
a. Converting conventional education into competency based module to develop theskill sets of the basic doctor:
b. Early clinical exposure – Clinical teaching from 1 st year onwardsc. Integrated Modular Teaching both Vertical & horizontal
INTEGRATION SCHEME
20%
60%
d. Clerkship / Student Doctor Method Of Clinical Training
e. Introduction of Electives - Examples - Bio Informatics, Tissue Processing Computer andComputer Applications, Ethics & Legal Medicine, Immunology, Genetics, Human Nutritionetc. Sports Medicine, Lab Sciences, Research Methedology, Ethics, Accident andEmergencies (A&E), Community Projects, HIV Medicine, Tissue Culture,PharmacoKinetics/Pharmacodynamics/Pharmacoeconomics, Assisted ReproductiveTechnology, Ethics and Medical Education etc.
80% CLINICAL
PARA CLINICAL
PRE CLINICAL
CLINICAL SCIENCES
BASIC SCIENCES
80%
40%
20%
8/7/2019 UG-medical-education
http://slidepdf.com/reader/full/ug-medical-education 8/22
8/7/2019 UG-medical-education
http://slidepdf.com/reader/full/ug-medical-education 9/22
9
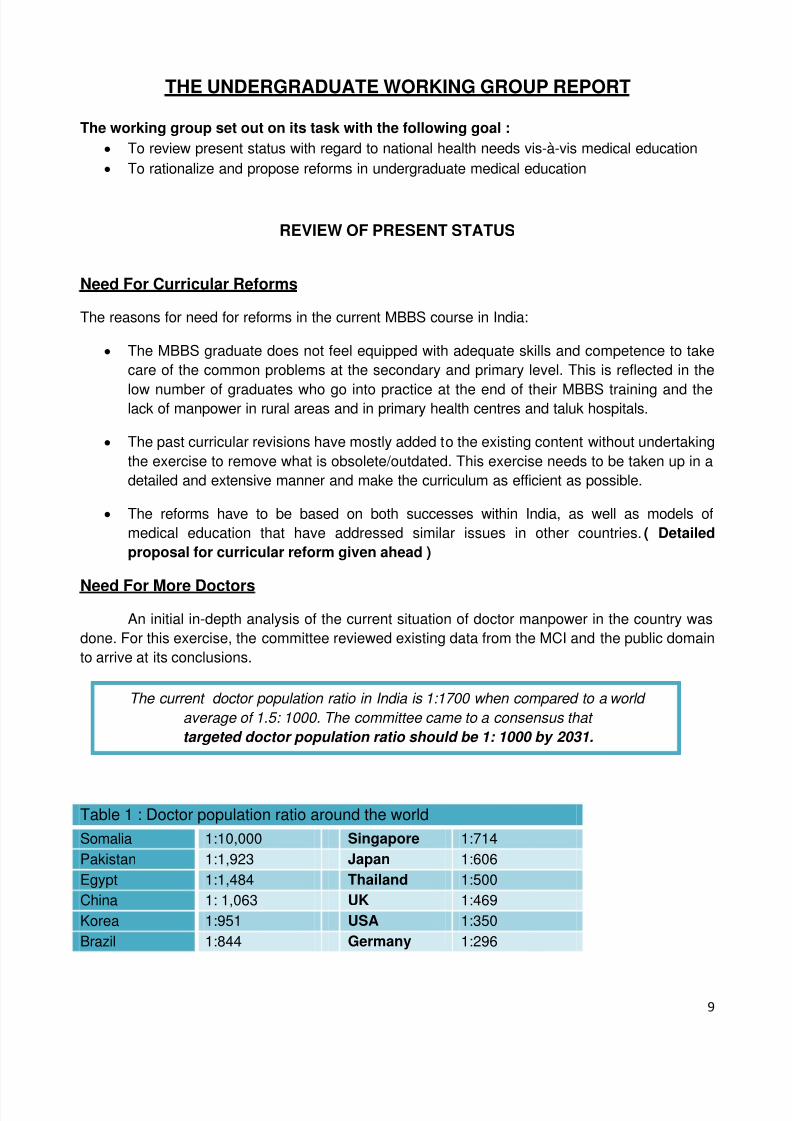
THE UNDERGRADUATE WORKING GROUP REPORT
The working group set out on its task with the following goal :To review present status with regard to national health needs vis-à-vis medical educationTo rationalize and propose reforms in undergraduate medical education
REVIEW OF PRESENT STATUS
Need For Curricular Reforms
The reasons for need for reforms in the current MBBS course in India:
The MBBS graduate does not feel equipped with adequate skills and competence to takecare of the common problems at the secondary and primary level. This is reflected in the
low number of graduates who go into practice at the end of their MBBS training and thelack of manpower in rural areas and in primary health centres and taluk hospitals.
The past curricular revisions have mostly added to the existing content without undertakingthe exercise to remove what is obsolete/outdated. This exercise needs to be taken up in adetailed and extensive manner and make the curriculum as efficient as possible.
The reforms have to be based on both successes within India, as well as models ofmedical education that have addressed similar issues in other countries. ( Detailedproposal for curricular reform given ahead )
Need For More DoctorsAn initial in-depth analysis of the current situation of doctor manpower in the country was
done. For this exercise, the committee reviewed existing data from the MCI and the public domainto arrive at its conclusions.
Table 1 : Doctor population ratio around the worldSomalia 1:10,000 Singapore 1:714Pakistan 1:1,923 Japan 1:606Egypt 1:1,484 Thailand 1:500China 1: 1,063 UK 1:469Korea 1:951 USA 1:350Brazil 1:844 Germany 1:296
The current doctor population ratio in India is 1:1700 when compared to a world average of 1.5: 1000. The committee came to a consensus that targeted doctor population ratio should be 1: 1000 by 2031.
8/7/2019 UG-medical-education
http://slidepdf.com/reader/full/ug-medical-education 10/22
10
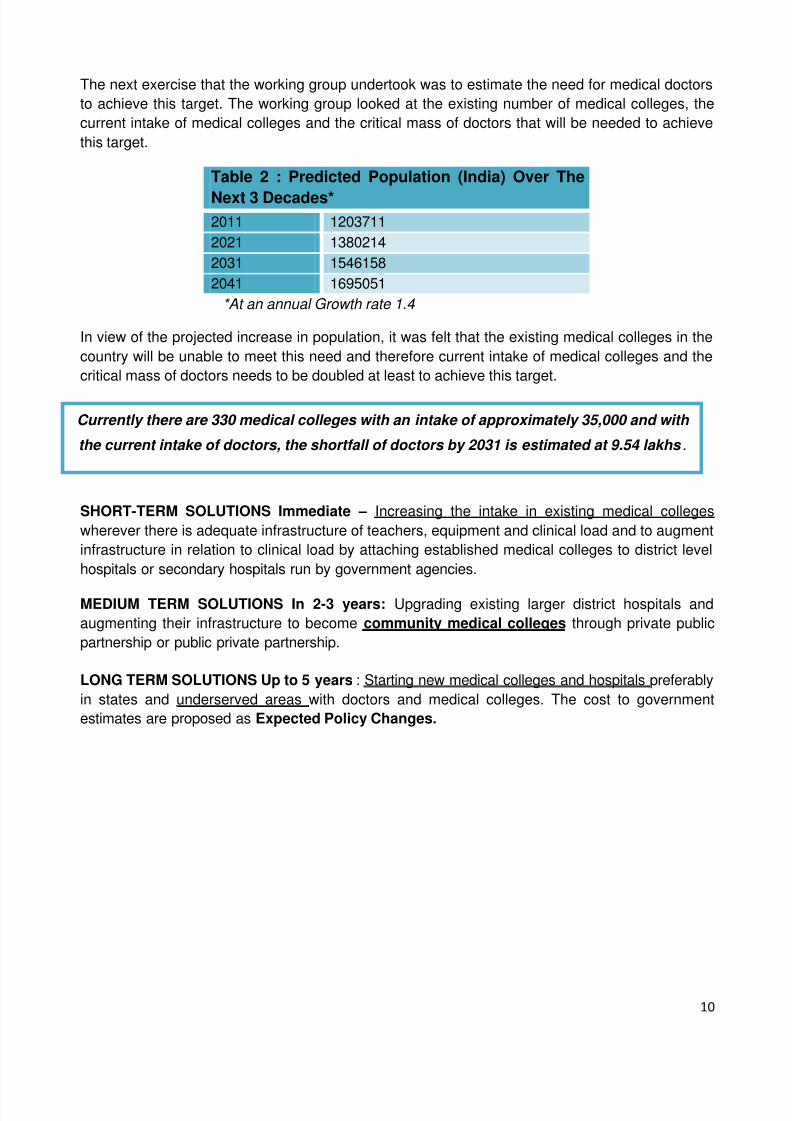
The next exercise that the working group undertook was to estimate the need for medical doctorsto achieve this target. The working group looked at the existing number of medical colleges, thecurrent intake of medical colleges and the critical mass of doctors that will be needed to achievethis target.
Table 2 : Predicted Population (India) Over The
Next 3 Decades*2011 12037112021 13802142031 15461582041 1695051
*At an annual Growth rate 1.4
In view of the projected increase in population, it was felt that the existing medical colleges in thecountry will be unable to meet this need and therefore current intake of medical colleges and thecritical mass of doctors needs to be doubled at least to achieve this target.
SHORT-TERM SOLUTIONS Immediate – Increasing the intake in existing medical collegeswherever there is adequate infrastructure of teachers, equipment and clinical load and to augmentinfrastructure in relation to clinical load by attaching established medical colleges to district levelhospitals or secondary hospitals run by government agencies.
MEDIUM TERM SOLUTIONS In 2-3 years: Upgrading existing larger district hospitals andaugmenting their infrastructure to become community medical colleges through private publicpartnership or public private partnership.
LONG TERM SOLUTIONS Up to 5 years : Starting new medical colleges and hospitals preferablyin states and underserved areas with doctors and medical colleges. The cost to governmentestimates are proposed as Expected Policy Changes.
Currently there are 330 medical colleges with an intake of approximately 35,000 and with
the current intake of doctors, the shortfall of doctors by 2031 is estimated at 9.54 lakhs .
8/7/2019 UG-medical-education
http://slidepdf.com/reader/full/ug-medical-education 11/22
11
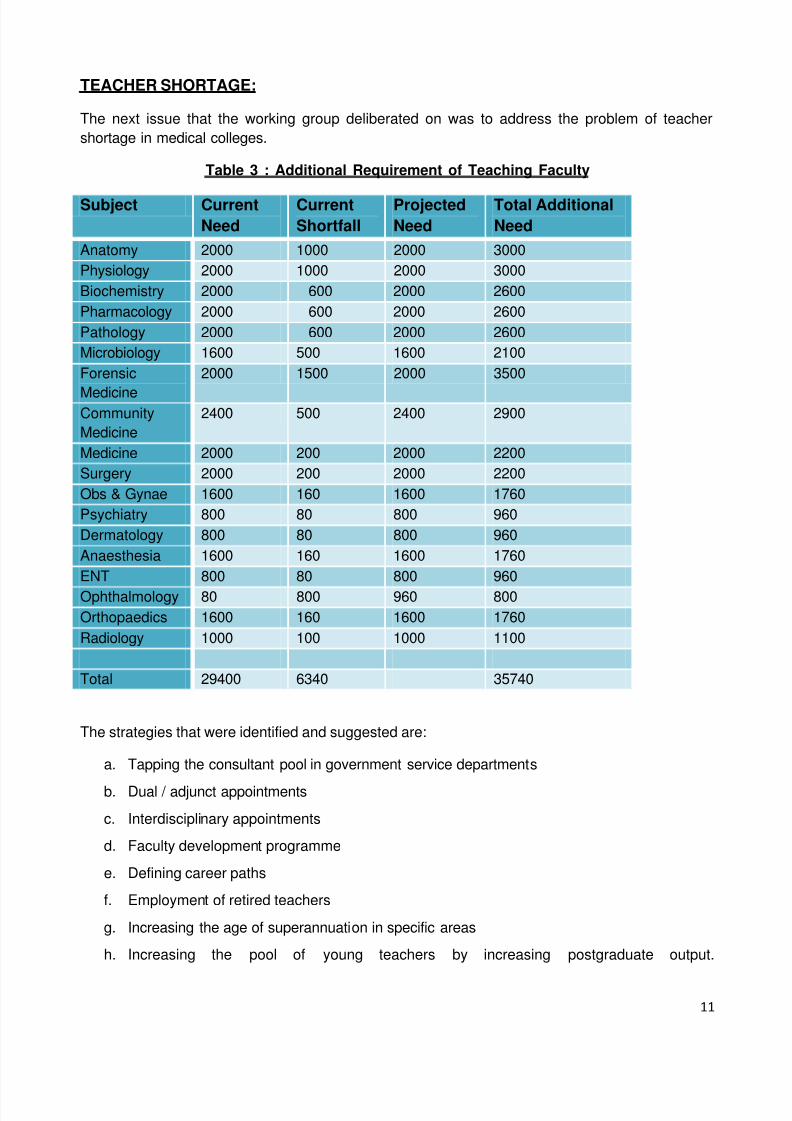
TEACHER SHORTAGE:
The next issue that the working group deliberated on was to address the problem of teachershortage in medical colleges.
Table 3 : Additional Requirement of Teaching Faculty
Subject CurrentNeed
CurrentShortfall
ProjectedNeed
Total AdditionalNeed
Anatomy 2000 1000 2000 3000Physiology 2000 1000 2000 3000Biochemistry 2000 600 2000 2600Pharmacology 2000 600 2000 2600Pathology 2000 600 2000 2600Microbiology 1600 500 1600 2100Forensic
Medicine
2000 1500 2000 3500
CommunityMedicine
2400 500 2400 2900
Medicine 2000 200 2000 2200Surgery 2000 200 2000 2200Obs & Gynae 1600 160 1600 1760Psychiatry 800 80 800 960Dermatology 800 80 800 960Anaesthesia 1600 160 1600 1760ENT 800 80 800 960Ophthalmology 80 800 960 800Orthopaedics 1600 160 1600 1760Radiology 1000 100 1000 1100
Total 29400 6340 35740
The strategies that were identified and suggested are:
a. Tapping the consultant pool in government service departments
b. Dual / adjunct appointments
c. Interdisciplinary appointments
d. Faculty development programme
e. Defining career paths
f. Employment of retired teachers
g. Increasing the age of superannuation in specific areas
h. Increasing the pool of young teachers by increasing postgraduate output.

8/7/2019 UG-medical-education
http://slidepdf.com/reader/full/ug-medical-education 12/22
12
Improving Quality of Training
The next major issue that the working group deliberated on was to improve the quality of trainingfrom what is the current existing model so that the graduates are efficient, competent andresponsive to national and international needs.
The lacunae of the CURRENT MBBS training are:a. Goal of training is not focused on providing health care to needy and disadvantaged
b. Discipline based curriculum and lack of integration between basic and laboratory scienceand clinical medicine
c. Assessment system’s focus on summative assessments at the end of each s tage, rotelearning and recall rather than competency
d. Lack of development of clinical competency
e. Majority of clinical training occurs in large teaching hospitals with insufficient practicaltraining at secondary and primary care level
f. Lack of training in family medicine
g. No mandatory service period at the end of undergraduate training and lack of linkage ofundergraduate to postgraduate training.
Strategies that have been successful in other countries :
a. Selection of students from rural and underserved backgrounds; who are motivated to workin areas of need
b. Early clinical training from I MBBS with continuity to secondary and primary care
c. Decentralisation of clinical training through clerkship model/student doctor to thesecondary and primary level;
d. Family medicine or Generalist Medical Practice as a core component of the curriculum;
e. Integrated curriculum in starting from the first yearwith- vertical and horizontal integrationbetween basic, laboratory sciences and clinical medicine;
f. Continuous assessment with specific focus on evaluating skills and competenceg. Partnerships between medical college and other health care facilities in the community
Restructuring and optimizing the current MBBS course .
The process of curricular change necessarily needs to start with the basic foundation of definingthe end product. In this case, the “BASIC DOCTOR” ( Annexure I )
The committee recommends the following for consideration for implementation:
A 4+1 model of training (4 years course + 1 year internship); 1+1+2+1
8/7/2019 UG-medical-education
http://slidepdf.com/reader/full/ug-medical-education 13/22
13
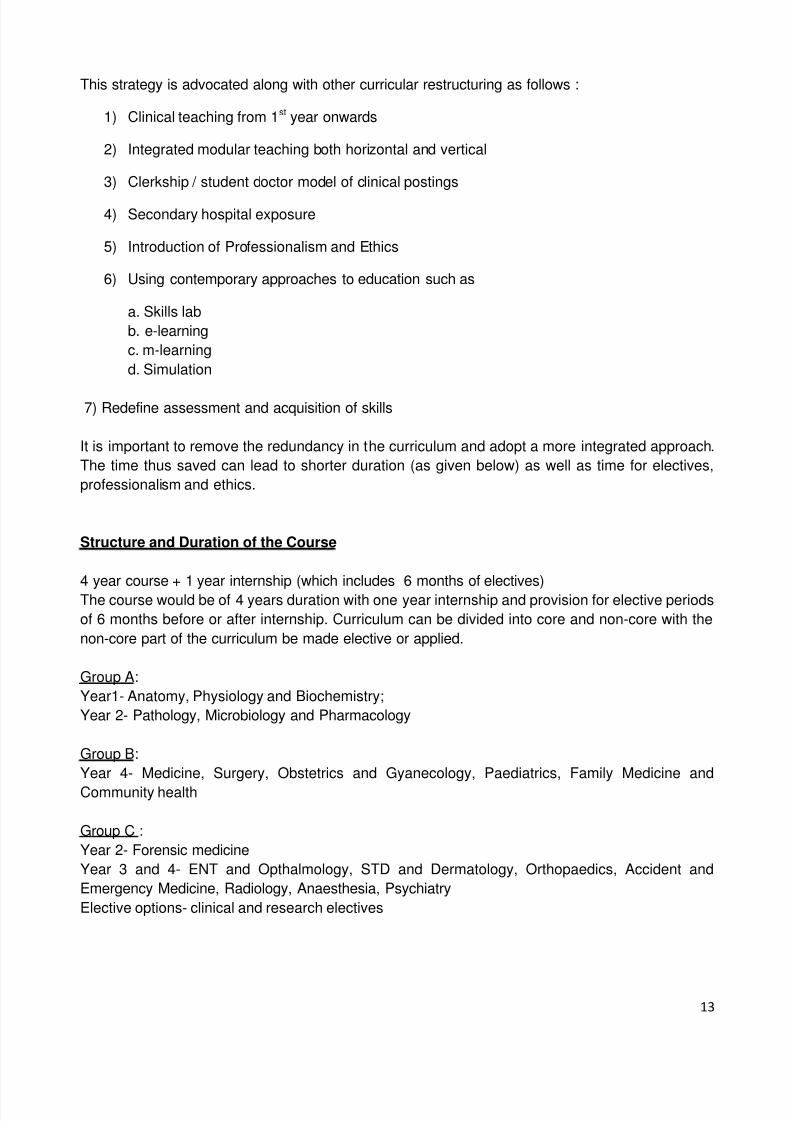
This strategy is advocated along with other curricular restructuring as follows :
1) Clinical teaching from 1 st year onwards
2) Integrated modular teaching both horizontal and vertical
3) Clerkship / student doctor model of clinical postings
4) Secondary hospital exposure
5) Introduction of Professionalism and Ethics
6) Using contemporary approaches to education such as
a. Skills labb. e-learningc. m-learningd. Simulation
7) Redefine assessment and acquisition of skills
It is important to remove the redundancy in the curriculum and adopt a more integrated approach.The time thus saved can lead to shorter duration (as given below) as well as time for electives,professionalism and ethics.
Structure and Duration of the Course
4 year course + 1 year internship (which includes 6 months of electives)The course would be of 4 years duration with one year internship and provision for elective periodsof 6 months before or after internship. Curriculum can be divided into core and non-core with thenon-core part of the curriculum be made elective or applied.
Group A:Year1- Anatomy, Physiology and Biochemistry;Year 2- Pathology, Microbiology and Pharmacology
Group B:Year 4- Medicine, Surgery, Obstetrics and Gyanecology, Paediatrics, Family Medicine andCommunity health
Group C :Year 2- Forensic medicineYear 3 and 4- ENT and Opthalmology, STD and Dermatology, Orthopaedics, Accident andEmergency Medicine, Radiology, Anaesthesia, PsychiatryElective options- clinical and research electives

8/7/2019 UG-medical-education
http://slidepdf.com/reader/full/ug-medical-education 14/22
14
Proposed timeframe in MBBS curriculum structure (to 4 years)
Table 4 : Teaching time for MBBS Curriculum
INTEGRATION SCHEME
20%
The innovative curriculum would be structured to facilitate horizontal, vertical integration betweendisciplines, the gaps between theory and practice and between hospital based medicine andcommunity medicine. Basic and laboratory sciences (integrated with their clinical relevance) wouldbe maximum in first year and will progressively decrease in second and third year as thecurriculum progresses. The essentials of basic and laboratory sciences would be taught in firstyear and built on in subsequent years.
MEDICAL ETHICS AND PROFESSIONALISMMedical professionalism forms the basis of contact between doctors and society and so it isimperative that professionalism and Ethical issues in practice should be incorporated into medicalcurriculum
Semester Weeks No. of hours ( x 40)First MBBS (1 year) 1 20 800
2 20 800Second MBBS (1 year) 3 20 800
4 20 800Third MBBS (2 years) 5 20 800
6 20 8007 20 8008 20 800
Total 160 6,400
80%
60% 88
CLINICAL
PARA CLINICAL
PRE CLINICAL
CLINICAL SCIENCES
BASIC SCIENCES
80%
40%
20%

8/7/2019 UG-medical-education
http://slidepdf.com/reader/full/ug-medical-education 15/22
15
Need to review curriculum
Similarly, certain subjects will need extra lectures from first year onwards e.g. approximately 8radiology lectures can be included in anatomy to teach students cross sectional anatomy of brain,abdomen , fetal anatomy during embryology teaching etc during first year itself. This practice isbeing already being followed by Maulana Azad Medical College, New Delhi . This model can beadopted by other colleges as well, without changing the number of lecture hours (by integration)
Forensic Medicine can be effectively taught during Gynaecology & Obstetrics (rape, assault),surgery (injuries), pharmacology (toxicology). Legal experts can be called for medico-legal issues.Forensic medicine skills can be acquired during internship such as documentation of medico-legalcases of alcoholism, suicide/homicide, rape, assault and injury cases.
Infection control section in hospital in now an important component and should be included.
Thus, both horizontal and vertical integration will be used for making the curriculum more efficient
and student friendly. Details of this are being worked out by expert committees constituted by MCIin co-ordination with undergraduate working group. ( Annexure II )
EARLY CLINICAL EXPOSURE
Most medical colleges across the world start clinical training in year I with communication,interviewing skills and basic examination skills through skills laboratories and students practicing examination on each other . In the several medical colleges the students learnt basic clinical skillsthrough half a day exposures once a week or once in two weeks with individual doctors at the level of primary care .
The clinical training would start in first year, with a foundation course, focusing on communication,basic clinical skills and professionalism. There would be sufficient clinical exposure at the primarycare level integrated with the learning of basic and laboratory sciences. Introduction of casescenarios for classroom discussion/ case-based learning. It will be done as a co-ordinated effort bybasic science and clinical faculty.
Professionalism and ethics curriculum will be a mandatory part of the curriculum and will beintegrated throughout the MBBS Course.The foundation courses will be taken during the first andsecond year and rest of the curriculum will be taught along with the clinical subjects.
CLERKSHIP / STUDENT DOCTOR METHOD OF CLINICAL TRAINING
The need for clinical training through clerkship methodIn the first 4 ½ years students learn history and examination and clinical diagnosis. They a learn alot of theory related to investigations and management, but are not involved in the process of work,making decisions and taking responsibility. The focus of MBBS clinical skills development is on theexamination of patients that are “exam cases” for the final examination, eg. Chronic liver disease,mitral stenosis, paraplegia. These cases and not the common clinical problems that are seen ingeneral practice at the primary and secondary level. In many medical colleges, students are alsonot provided adequate practical involvement in work in internship.

8/7/2019 UG-medical-education
http://slidepdf.com/reader/full/ug-medical-education 16/22
16
In order for the MBBS course to provide sufficient skills development for competent practice, aframe shift is required in clinical training in the following ways:
a. Focus on common problems seen in outpatient and emergency settingb. Learning through clerkship method by involvement in process of care as a team member,
in investigation, management and basic proceduresc. Significant part of training to take place at primary and secondary level with compulsory
family medicine trainingd. Parts of clinical training should be core requirements and others as elective postings
Description of the clerkship method of clinical trainingIn the clerkship method students are posted to respective departments as a clerk or sub-intern.The sub-intern is below the level of intern, and takes partial patient care under responsibility as ateam member. During sub-internship, students have specific objectives of learning in relation tohistory, examination, procedural skills, management of common ambulatory and emergencyconditions. Students take care of patients under the supervision of the registrar and consultant
both in the out-patient and in-patient setting and emergency setting. Learning is by practicalinvolvement in the process of care of patients. Students have lectures, seminars and clinical casediscussions to support practical learning during clerkship.
Annexure III - Model clerkship posting
TRAINING IN SECONDARY HOSPITAL SETTING
Each medical college should be linked to the local health system including CHCs, taluk hospitalsand primary health care centres that can be used as training base for medical students.
NEWER DISCIPLINES AND REVIEW OF INFRASTRUCTURE, EQUIPMENT AND FACULTYREQUIREMENT
Family medicine or Generalist Practice of Medicine needs to be an essential undergraduatesubject taught by specialists at the level of secondary and primary care. The existing nationalinitiatives, particularly with respect to Millenium Development Goals and Health Ministry initiativeslike the RCH component of NHRM, including IMNCI and NSSK should be an integral part of thiscurriculum.
Need to review requirement of infrastructure, equipment and faculty in some subjectsKeeping in view the advances in all spheres of medicine, there is an inescapable need to reviewthe requirement of infrastructure, equipment and faculty in most of subjects due to introduction ofnewer technology and changed training needsEXAMPLES – In case of radiology, the age old dark room technology for processing of X Ray films should bereplaced by digital technology (Computed radiography/ if possible by direct digital technology).Moreover, the earlier Image intensifier systems for fluoroscopy should be replaced by radio-fluoroscopy equipment (this will enable long term storage of digitalised data which can be utilisedfor both research & training subsequently. Similarly, 60 mA X-Ray machines should be replacedby 100mA machines and CT scans should be at least 16 slices or higher. This will also necessitatechanges in infrastructure and staff accordingly which will also be required to be amended.

8/7/2019 UG-medical-education
http://slidepdf.com/reader/full/ug-medical-education 17/22
17
In Pharmacology, the training will have to be focused to clinical skills e.g. dose calculationadministering the drugs through various routes of administration, optimising the choice of drug anddose, recognising, managing and preventing adverse reactions. Experimental pharmacologypractical in animals may require to be replaced by modern techniques using videos andsimulations. The techniques relating to drugs and toxin estimations could be set up.
Considerable advances have taken place in laboratory techniques in microbiology. Sometechniques have become redundant and outdated. The undergraduate curriculum should reflectthese changes e.g. molecular diagnostic techniques.
MEDICAL TEACHERS CAPACITY BUILDING IN EDUCATION
This above strategy will not be efficiently implemented without faculty development to familiarizeteachers with this methodology of teaching. Hence, the committee strongly recommends thatLearning Facilitation Centres are set up in many parts of the country for faculty development andtraining. Each institution should be encouraged to conduct its own faculty training programme andthe completion of this training must be made mandatory. A national strategy for large scale facultydevelopment is necessary to be instituted immediately.
Specific Training Programmes will be designed to help faculty and institutions implementthe new curriculum
New programmes will be developed through multi-level system of courses and workshops, basic toadvanced, specific train-the-trainer programmes and workshops on specific topics and for specificfaculty groups. The following courses can be envisioned to begin with:
Level I – 3-day Basic Introductory CourseLevel II – 6 month Advanced (Certificate) CourseLevel III –1 Year Train-the-trainer (Diploma in ME)Level IV – 2 Year Masters’ Programme in Health Professions Education Specialized theme based courses/workshops – 5 to 10 day workshops in Medical Education and awide range of CME/CPD Programmes and Workshops.
ORGANISATIONAL STRUCTURE
Level 1 Centre : EDUCATION UNIT
Number - Every Medical College
Activities/Functions :Teachers Training Programmes – Level 1
Patient Simulation Centre : Level 1
Skills Training Centre : Level 1
E-Learning/Digital Learning Resource Centre
8/7/2019 UG-medical-education
http://slidepdf.com/reader/full/ug-medical-education 18/22
18
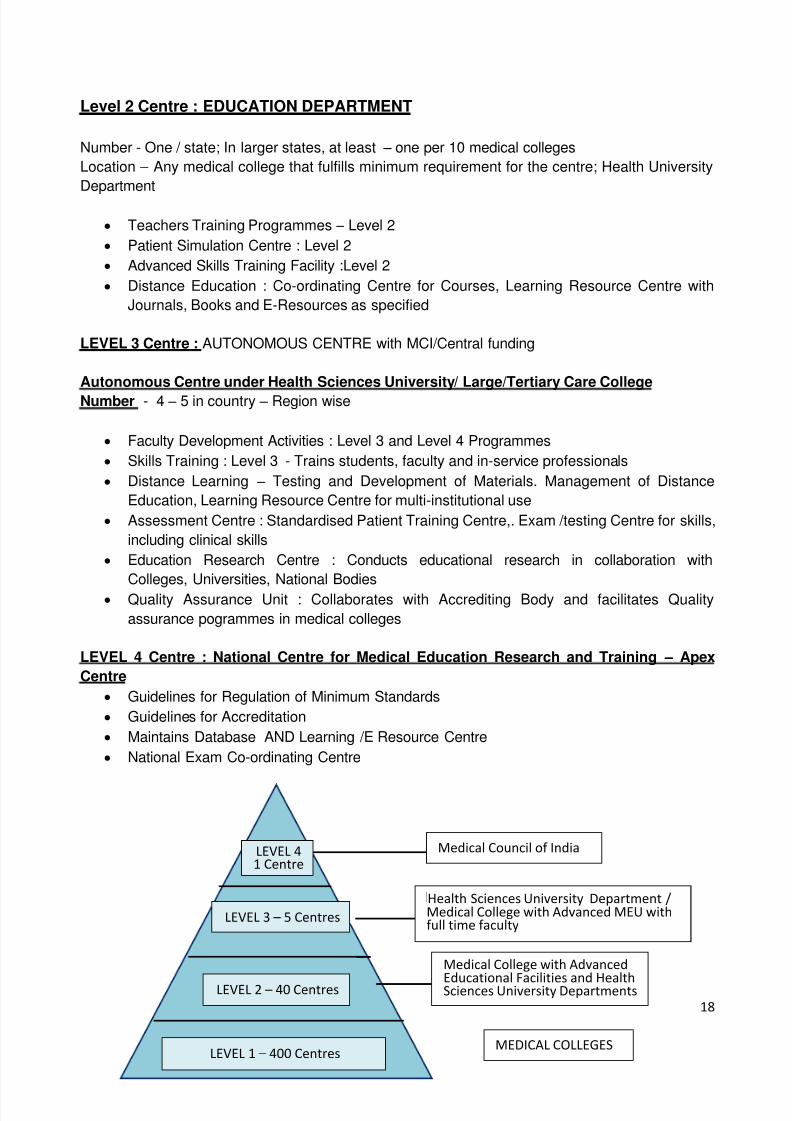
Level 2 Centre : EDUCATION DEPARTMENT
Number - One / state; In larger states, at least – one per 10 medical collegesLocation – Any medical college that fulfills minimum requirement for the centre; Health UniversityDepartment
Teachers Training Programmes – Level 2Patient Simulation Centre : Level 2Advanced Skills Training Facility :Level 2Distance Education : Co-ordinating Centre for Courses, Learning Resource Centre withJournals, Books and E-Resources as specified
LEVEL 3 Centre : AUTONOMOUS CENTRE with MCI/Central funding
Autonomous Centre under Health Sciences University/ Large/Tertiary Care CollegeNumber - 4 – 5 in country – Region wise
Faculty Development Activities : Level 3 and Level 4 ProgrammesSkills Training : Level 3 - Trains students, faculty and in-service professionalsDistance Learning – Testing and Development of Materials. Management of DistanceEducation, Learning Resource Centre for multi-institutional useAssessment Centre : Standardised Patient Training Centre,. Exam /testing Centre for skills,including clinical skillsEducation Research Centre : Conducts educational research in collaboration withColleges, Universities, National BodiesQuality Assurance Unit : Collaborates with Accrediting Body and facilitates Qualityassurance pogrammes in medical colleges
LEVEL 4 Centre : National Centre for Medical Education Research and Training – ApexCentre
Guidelines for Regulation of Minimum StandardsGuidelines for AccreditationMaintains Database AND Learning /E Resource CentreNational Exam Co-ordinating Centre
LEVEL 1– 400 Centres
LEVEL 2– 40 Centres
LEVEL 3– 5 Centres
LEVEL 41 Centre
MEDICAL COLLEGES
Medical College with Advanced
Educational Facilities and HealthSciences University Departments
Health Sciences University Department /Medical College with Advanced MEU withfull time faculty
Medical Council of India

8/7/2019 UG-medical-education
http://slidepdf.com/reader/full/ug-medical-education 19/22
19
Table 5 : Activities at Various Levels of Faculty Development Centres
S.No ACTIVITIES LEVEL 1 LEVEL 2 LEVEL 3 LEVEL 4
1. TeachersTraining
Basic Level1
Advanced Diploma/MastersProgramme
OrientationWorkshops
2 Skills Training Level 1 Level 2 Level 3 Exam Centre3 Patient
SimulationCentre
Level 1 Level 2 Level 3 Exam Centre
4 E- Learning &ResourceCentre
Yes Yes Yes CentralConsortium ofBooks/Journals/ E-Resources
5 Distance
EducationProgrammes
Co-
ordinatingCentre
Course and
MaterialDevelopment
Accreditation
5. CPD/CMEProgrammes
Can do MUST MUST Accreditation
BUDGET Establishment 1.5 croreX400
5 crore X40 20 crore X5 100 Crore X1
TOTAL - 1000 Crores
EXPECTED OUTCOMES:
1. Faculty will apply and use educational principles in their day-to-day teaching and planningof teaching to make it more student-centered.
2. Faculty will incorporate new teaching-learning methods and improve educational systemsin their own institutions.
3. Faculty will be able to conduct basic workshops in their own institutions4. Faculty with specialized skills will participate in activities of their affiliated Centre/Unit
ESTABLISHMENT OF SKILLS TRAINING CENTRES
The skills development centres will consist of:
A simulation laboratory for developing basic clinical, procedural and surgical skills.A laparoscopic training facility for acquiring basic skills in laparoscopyThe facility will be also to open to undergraduate and postgraduate students, interns andresidents, who can come for skills training accompanied by their teachers.
The courses should be tailored to meet the requirement for various levels of competence andvariety of skills.
LEVEL 1 – Basic Surgical Skills, Basic Life Support Skills, Procedural Skills, Normal LabourManagement and Conduct of Delivery. These should be a compulsory part of clinical training of allundergraduates.
Level 1 training facility is mandatory for all medical colleges.
8/7/2019 UG-medical-education
http://slidepdf.com/reader/full/ug-medical-education 20/22
20
LEVEL 2 – Advanced Life Support and Refresher Level 1 Courses, Basic Laparoscopic SkillsCourse, Neonatal and Paediatric Resuscitation Skills.
Level 2 skills training centres are desired in each medical college; however if there are financialconstraints, these could be conducted in collaboration with regional centres.
LEVEL 3 – These will be available for multi-institutional use. Course will includeMicrosurgical Skills Courses, Advanced Laparoacopic Skills Courses and Human PatientSimulators for Anaesthesia, Pharmacology, Physiology and other physiology competencies.
Level 3 is to be offered only in regional skill training centres and above.
Interns should have a mandatory Level I Certification before they get their Licensure degree
A detailed document regarding the training programmes, minimum activities, infrastructure andequipment requirement at each level, minimum faculty and staff with budget is attached as
Annexure IV
RESEARCH METHODOLOGYThere should be a workshop on learning the nuances of research in terms of principles, collection,organization and analysis of data to prepare a budding faculty member for guiding thethesis/research work in their subsequent work profile. The minimum duration of the exposure tothese techniques should be at least 3 days.A mandatory course on epidemiology for at least 2 days should also be incorporated into thecapacity building.
IMPARTING COMPUTER SKILLSThese would include power point presentations, hosting a web page , excel sheet maintenanceand a basic training in SPSS software.The above courses/workshops on Research methodology and computer skills will need to beorganized by the individual institutes themselves.
LIBRARY AND DISTANCE LEARNING CENTRE
In all centres, this facility will be utilized by teachers who attend course and programmes ar thesecentres. It will be equipped with books, journals, a variety of electronic resources includinginteractive multimedia and self assessment packages for students. The advanced centre facilitywill also be made available to instiutions affiliated to the University at nominal rates.
KEY AGENCIES FOR EXPECTED POLICY CHANGES – MCI, Planning Commission and Ministry of Health, GOI .
8/7/2019 UG-medical-education
http://slidepdf.com/reader/full/ug-medical-education 21/22
21
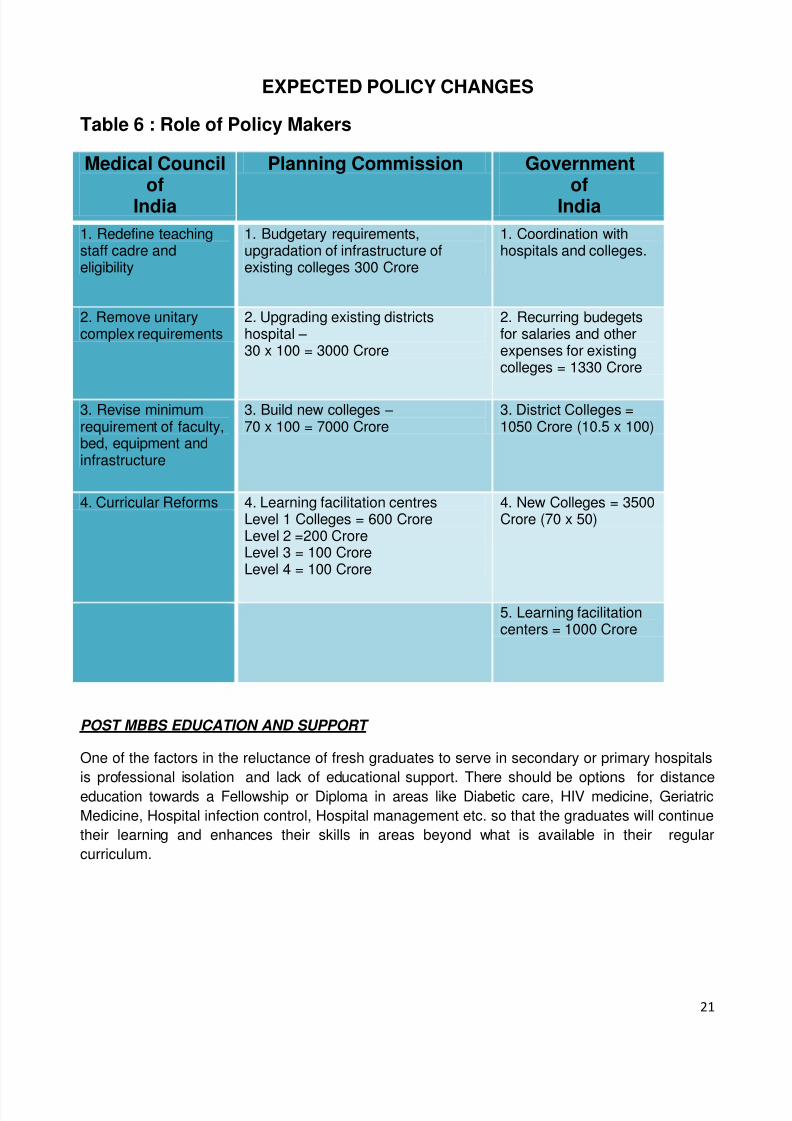
EXPECTED POLICY CHANGES
Table 6 : Role of Policy Makers
Medical Councilof
India
Planning Commission Governmentof
India1. Redefine teachingstaff cadre andeligibility
1. Budgetary requirements,upgradation of infrastructure ofexisting colleges 300 Crore
1. Coordination withhospitals and colleges.
2. Remove unitarycomplex requirements
2. Upgrading existing districtshospital – 30 x 100 = 3000 Crore
2. Recurring budegetsfor salaries and otherexpenses for existingcolleges = 1330 Crore
3. Revise minimumrequirement of faculty,bed, equipment andinfrastructure
3. Build new colleges – 70 x 100 = 7000 Crore
3. District Colleges =1050 Crore (10.5 x 100)
4. Curricular Reforms 4. Learning facilitation centresLevel 1 Colleges = 600 CroreLevel 2 =200 CroreLevel 3 = 100 CroreLevel 4 = 100 Crore
4. New Colleges = 3500Crore (70 x 50)
5. Learning facilitationcenters = 1000 Crore
POST MBBS EDUCATION AND SUPPORT
One of the factors in the reluctance of fresh graduates to serve in secondary or primary hospitalsis professional isolation and lack of educational support. There should be options for distanceeducation towards a Fellowship or Diploma in areas like Diabetic care, HIV medicine, GeriatricMedicine, Hospital infection control, Hospital management etc. so that the graduates will continuetheir learning and enhances their skills in areas beyond what is available in their regularcurriculum.

8/7/2019 UG-medical-education
http://slidepdf.com/reader/full/ug-medical-education 22/22
22
CONCLUDING REMARKS
Thus the working group is of the opinion with an improved
and revised curriculum and detailed capacity building offaculty, increased manpower can be produced which is
equal to world standards, provided the necessary
infrastructure and faculty development programmes are put
in place.
The group also feels that this will result in the improved
quality of the existing colleges, sufficient number of
teachers and will create motivating career pathways for
both students and teachers.
This should result in better alignment of medical education
with health needs and an overall improvement in the
healthcare of our country with improved health parameters.

















