23
Ulnar nerve Ulnar nerve compression compression Michael Maru Orthopaedic Postgraduate Teaching 23/04/07
| Date post: | 21-Dec-2015 |
| Category: |
Documents |
| View: | 220 times |
| Download: | 3 times |

Ulnar nerve compressionUlnar nerve compression
Michael Maru
Orthopaedic Postgraduate Teaching
23/04/07
Introduction Introduction
Second most common entrapment neuropathy M >F 5:1 Frequently bilateral Before 1959,it was thought to be posttraumatic ulnar palsy After 1959, Osborne called it tardy ulnar palsy referring to
idiopathic ulnar neuritis Feindel & Stafford in 1973 coined the term cubital tunnel
syndrome (CTS) Commonest cause of ulnar nerve compression is CTS
Relevant anatomyRelevant anatomy
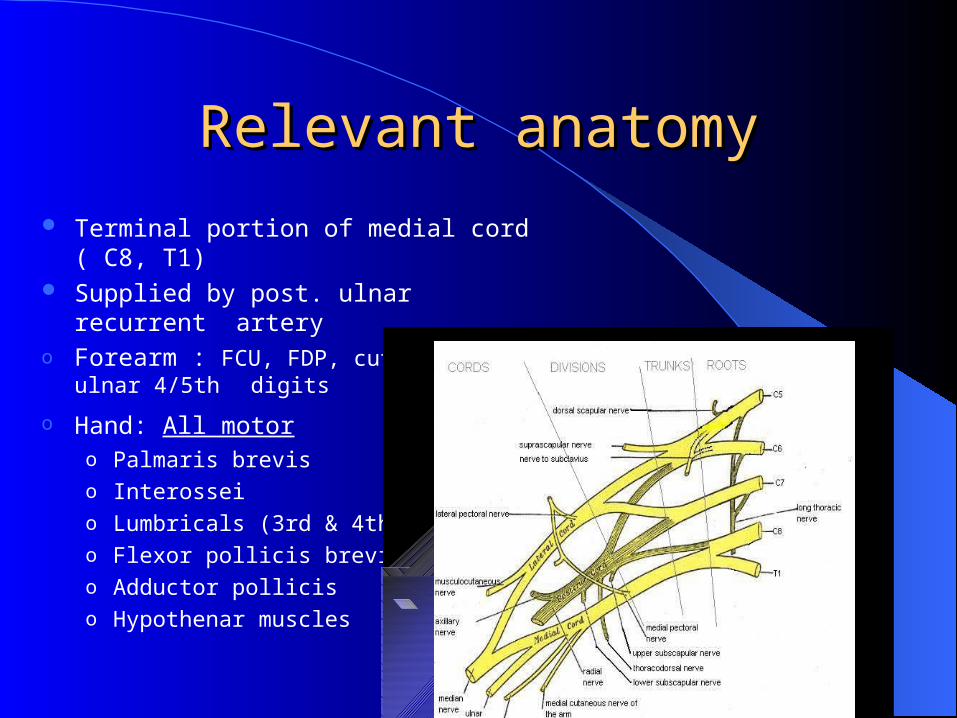
Terminal portion of medial cord ( C8, T1) Supplied by post. ulnar recurrent arteryo Forearm : FCU, FDP, cutaneous ulnar 4/5th
digits
o Hand: All motor o Palmaris brevis o Interossei o Lumbricals (3rd & 4th) o Flexor pollicis brevis o Adductor polliciso Hypothenar muscles

Branches: all distal to elbowBranches: all distal to elbow
Anatomy Anatomy Sunderland 1987;
Described internal topography of ulnar nerve Sensory and intrinsics fibres superficial Motor fibres to FCU & FDP are deeply located Hence weakness of FCU/FDP not typically seen in ulnar nerve
neuropathy
Sunderland S: Nerves and nerve injuries . 2nd ed. New York, NY: Churchhill Livingston; 1987: 728-74
“Double crush” concept Proximal compression of nerve trunk may increase
vulnerability to distal compression This is due to disruption of axonal transport

Sites of compressionSites of compression
Elbow– Arcade of Struthers – Medial epicondyle– Olecranon groove– Cubital tunnel– Anomalous anconeus
– Flexor pronator aponeurosis

Sites cont…Sites cont… Guyons canal:
Ulnar tunnel syndrome Tunnel enclosed by piso-hamate ligament Commonly due to ganglion cyst, tumour,
aneurysm or fractured hook of hamate Involvement of dorsal sensory branch
indicates compression proximal
to Guyon’s canal
Risk factorsRisk factors Trauma;
Acute, chronic or repetitive Anaesthesia and bed-ridden
patients Pressure with flexed elbow
(occupational)
Bony deformities; Arthritis (RA) Shallow groove Valgus deformity
Soft tissue masses Ulnar nerve prolapse Alcoholism Diabetes

Clinical presentationClinical presentation Paraesthesia; ring and little
finger (night) Pain ( Elbow) Weakness of grip, dropping
objects Clawing
More in distal lesions “Ulnar paradox”
Hyperextension of MCPJ (lumbricals)
Flexion of IPJ (interossei)
Intrinsic muscle wasting
Classification Classification
McGowan;Types 1: recent, mild, intermittent dysaethesia
II: persistent dysaethesia, early motor loss
III: Marked atrophy and weakness
McGowan AJ. The results of transposition of the ulnar nerve for
traumatic ulnar neuritis. J Bone Joint Surg Br, 1950;32: 293-301.
Diagnosis Diagnosis
History & Examination Ask & look for risk factors Neurological examination of upper limb
Special provocation tests Elbow flexion test: supinate, flex elbow and hyperextend
wrist Froments sign : weak adductor pollicis Wartenburg sign: little finger adopts abducted posture “Making a wish” sign: unable to cross index over middle Tinels sign: tapping along the ulnar groove causes tingling to
ring and little fingers ( +ve in 24% normal popu)

Differential diagnosisDifferential diagnosis
Cervical root lesion/myelopathy Neck & Arm pain, UMN signs
Thoracic outlet syndrome Vascular anomalies Fatigue with arm overhead
Brachial plexus abnormalities Involvement of other nerves
Investigations Investigations
Radiographs Nerve conduction studies
• Conduction velocities < 50m/s
• Identify site of compression
Electromyography• Axonal degeneration
MRIUltrasound scan
ManagementManagement Conservative
• Indicated if paraesthesia is transient• Patient education about posture• NSAIDs for nerve irritation• Physiotherapy• Elbow extension splints
Treatment of ulnar nerve palsy at the elbow with a night splintSeror-P. Laboratoire d'Electromyographie, JBJS-Br. 1993 Mar. 75(2). P 322-7.
22 patients treated with night splint preventing elbow flexion beyond 60 degrees. Improvement of symptoms in every patient including 3 who had failed surgical decompression! Conclu: Nocturnal elbow flexion aggravates symptoms
Operative managementOperative management
Indications • Failure of conservative methods
• Persistent paraesthesia
• Progressive symptoms especially motor
Options• Decompression in-situ
• Decompression with transposition
Decompression in-situDecompression in-situ
Incision 8cm proximal and 6 cm distal to medial epicondyle
Osborne ligament incised to open tunnel Open or endoscopic May be combined with medial epicondylectomy

Decompression with Decompression with transpositiontransposition
May be indicated in:• Recurrence of symptoms after simple neurolysis
• Acute fracture ORIF ( prominent metalware)
• Elbow arthroplasty (scarring)
• Ulnar nerve repair
• Cubital valgus
• Arthritis with osteophytes formation
• Recurrent dislocation of nerve
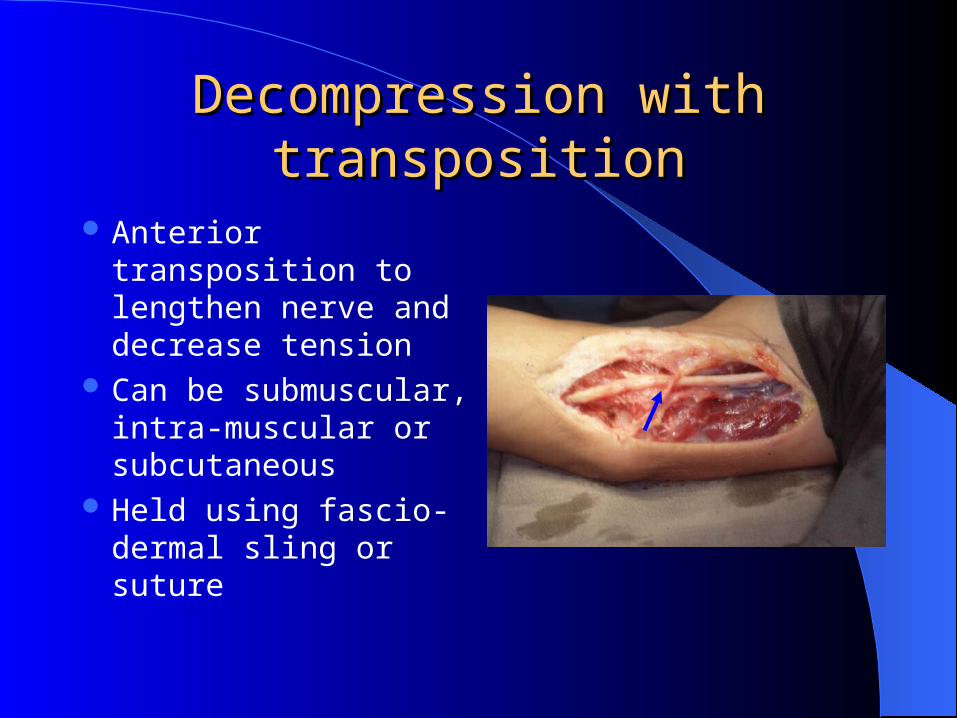
Decompression with Decompression with transpositiontransposition
Anterior transposition to lengthen nerve and decrease tension
Can be submuscular, intra-muscular or subcutaneous
Held using fascio-dermal sling or suture
Transposition or not?Transposition or not? Cochrane Review; 5 RCTs, same conclusion
Simple decompression or subcutaneous anterior transposition of the ulnar nerve for cubital tunnel syndrome
NABHAN A et al ; The Journal of hand surgery 2005, vol. 30, pp. 521-524
Prospective randomised study; 66 patients, 32 had simple decompression, 34 had transposition. At 9 months , no significant difference in pain, sensory or motor deficits. Recommended simple decompression
Randomized, prospective study comparing ulnar neurolysis in situ with submuscular transpositionBiggs M, Curtis J; Neurosurgery 2006, Vol 58, issue 2, pg 296-304
RCT, 44 patients, 21 had neurolysis, 23 had transposition. Both procedures equally effective in objective neurological improvement. However, higher wound complications.in transposition group.Conclusion; Neurolysis in situ for idiopathic symptomatic ulnar nerve compression

Endoscopic or open?Endoscopic or open?
Endoscopic method becoming popular Thought to be less invasive, quick rehab No reported RCT Tsu-Min Tsai et al (1999)
85 elbows in 76 patients F/U of 32 months 42% excellent, 45% good, 11% fair,2% poor
Tsai TM, Chen IC, Majd ME: Cubital tunnel release with endoscopic assistance: results of a new technique. J Hand Surg [Am] 1999 Jan; 24(1): 21-9

Decompression at the wristDecompression at the wrist Zigzag incision Pisohamate ligament opened Identify and remove the cause Usually ganglion cyst (Sedon)
beware aneurysm!
Hence the need for appropriate
investigation before operating

Conclusion Conclusion
Commonest site of ulnar nerve compression is at the cubital tunnel in the elbow
Decompression in-situ (neurolysis) is recommended for idiopathic ulnar nerve neuropathy
Transposition should be considered in recurrent cases, arthritis and cubital valgus
Endoscopic release is the future trend.

Thank you
?

















