26
Ultrasound confirmation of endotracheal tube placement Dr James Wheeler BSc MBBS FACEM DDU Emergency Physician, SCGH
| Date post: | 21-Jan-2018 |
| Category: |
Health & Medicine |
| Upload: | scgh-ed-cme |
| View: | 178 times |
| Download: | 3 times |

Ultrasound confirmation of
endotracheal tube placement
Dr James Wheeler BSc MBBS FACEM DDUEmergency Physician, SCGH

Will this replace traditional
methods of ETT confirmation?
• Specifically, does this replace capnography and
auscultation
• NO!
• But no single confirmatory method is entirely reliable in
emergency situations, and in certain circumstance US
confirmation can be a very helpful adjunct

Why would you do it?
• Transtracheal ultrasound is a relatively SIMPLE technique
• FAST (~8 sec vs 18 sec for capnography1)
• May be more reliable than capnography changes in certain patient groups?
• SENSITIVE and SPECIFIC 2,3,4
• The pooled sensitivity and specificity for the detection of proper ETT placement
with US were:
• Sensitivity: 98% (95% C.I. 97-99%); Specificity: 98% (95% C.I. 95-99%);
PPV: 99.5%, NPV: 93.8%
• Does not require ventilations to assess tube placement
• May prevent gastric insufflation and delay in diagnosis of misplacement
When would you use it?
• ETCO2 unreliable or not available
• Cardiac arrest / massive PE
• Emergency blind intubation
• Patient arrives intubated and requires rapid confirmation of
ETT placement
• Any patient not responding as expected after ETT
placement prior to attempting re-intubation

How do you do it?
Direct (Transtracheal)
• Looking for evidence of direct endotracheal intubation or oesophageal intubation (a “second trachea”)
• During intubation OR Post-intubation
Indirect (Transthoracic)
• Looking at the pleural space for evidence of lung ventilation (pleural movement)
• Post-intubation

Direct: Technique
Probe:
• high frequency (6-12MHz) linear probe (but
can use lower freq micro convex or
curvilinear in obese)
Preset:
• Superficial, depth sufficient to see posterior
to trachea, focal zone at trachea
Probe placement:
• in transverse plane just above the
suprasternal notch
• i.e. beneath cricoid

Direct: Technique
Endotracheal intubation:
• One air-mucosal interface
• Hyperechoic reverberation artifacts inside trachea
OR
Oesophageal intubation:
• Dynamic opening of the oesophagus by the ETT seen on US performed during laryngoscopy
• Two air-mucosal interfaces (“two tracheas” , “double track sign”)
• Hyperechoic reverberation artifacts inside oesophagus
May also interrogate cuff position by infiltrating saline

Direct: US Anatomy

Direct: Tracheal Intubation



Direct - Oesophageal Intubation






Indirect
• Looking at the pleural space for evidence of lung
ventilation (pleural movement)
• Differential pleural movement may indicate RMS
intubation
• Requires ventilation
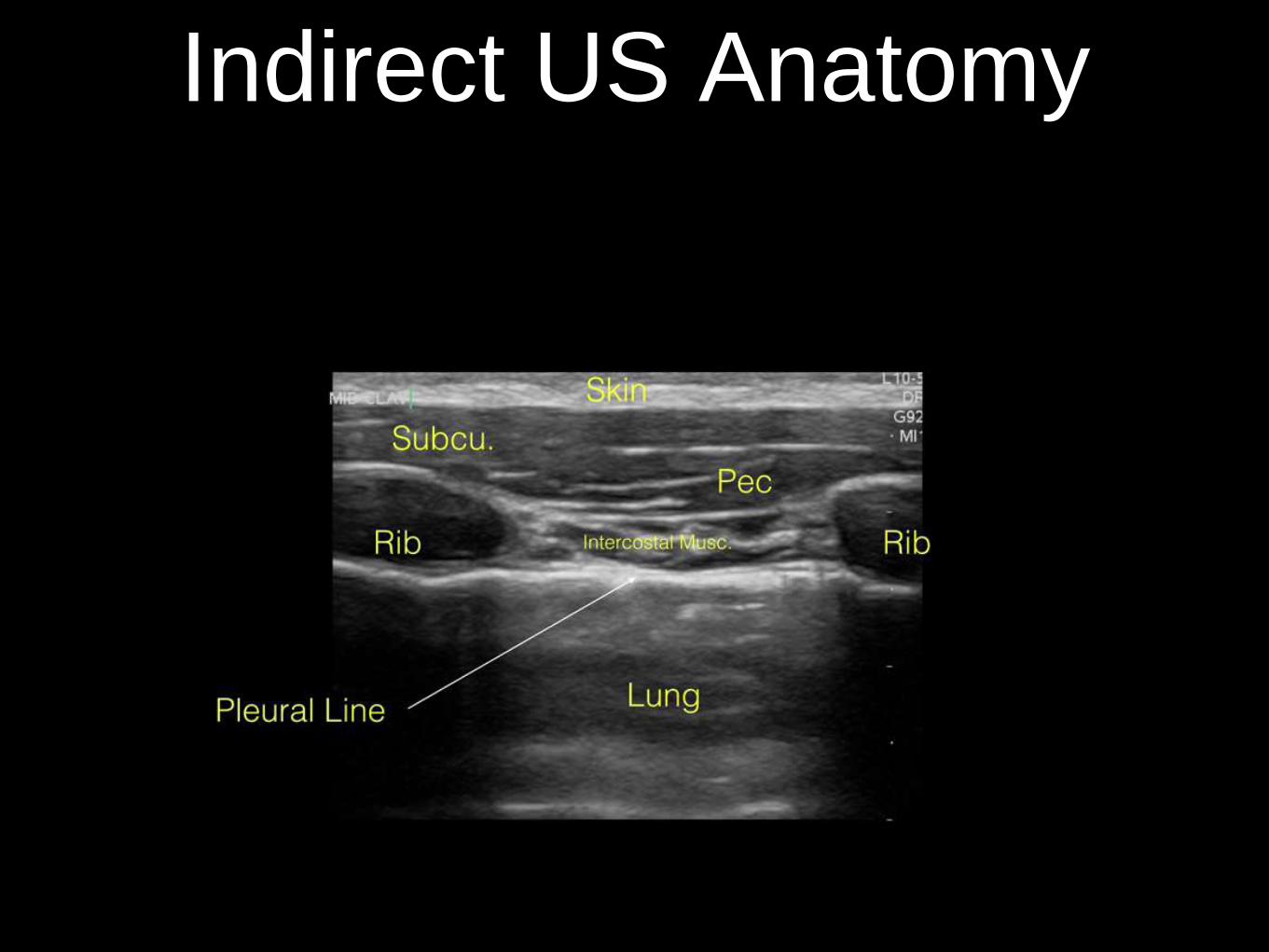
Indirect US Anatomy
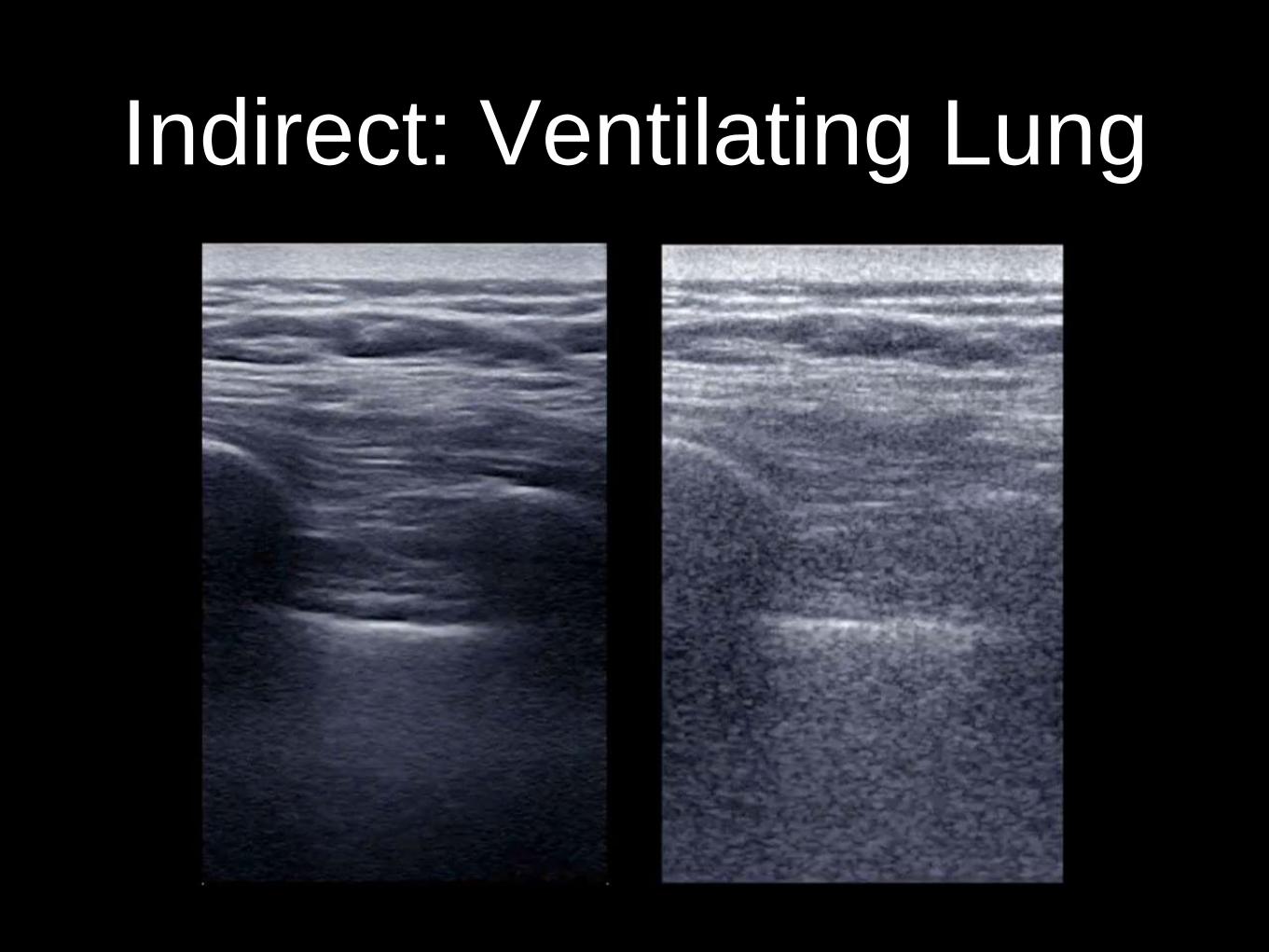
Indirect: Ventilating Lung

Indirect: Non-Ventilating Lung

Indirect: Pneumothorax

Indirect: PTX Lung Point

Pitfalls?
• Requires access to US machine
• No single confirmatory method is entirely reliable (esp. in
emergency situations)
• Operator dependent
• Surgical emphysema can obscure view
• Can’t identify supraglottic airway
• Pneumothorax (for indirect)

References
1. Reliability of Ultrasonography in Confirming Endotracheal Tube
Placement in an Emergency Setting. Vimal Koshy, Thomas et al.
Indian J Crit Care Med. 2017 May; 21(5): 257–261.
2. Transtracheal ultrasound for verification of endotracheal tube
placement: a systematic review and meta-analysis. Das SK1, Choupoo
NS, Haldar R, Lahkar A. Can J Anaesth. 2015 Apr;62(4):413-23
3. Ultrasonography for confirmation of endotracheal tube placement: A
systematic review and meta-analysis. Eric H.Chou et al. Resuscitation,
Volume 90, May 2015, 97-103
4. Can Transtracheal Ultrasonography Be Used to Verify Endotracheal
Tube Placement? Gottlieb M, Bailitz J .Ann Emerg Med. 2015 Oct;
66(4): 394-5

















