Page 1
MGH Weight Center
Partners Community Health, Inc.
Understanding and Treating ObesityLee M. Kaplan, MD, PhDMassachusetts General HospitalHarvard Medical School
[email protected]
September 14, 2010
Page 2
MGH Weight Center
• Presentation
• Q&A
Format
Page 3
MGH Weight Center
• On the left side of your screen, click the message box, “Chat with Presenter.”
• Type your question.
• Click ‘Send.”
• These questions will be addressed after the presentation.
Questions
Page 4
MGH Weight Center
Lee M. Kaplan, MD, PhDMassachusetts General HospitalHarvard Medical School
Presenter
Page 5
MGH Weight Center
Obesity
• Very common
• Growing
• Complex physiology
• Clinically heterogeneous
• Resistant to treatment
• Frustrating
• Global health priority
• Associated with cancer
Page 6
MGH Weight Center
Obesity by the Numbers
Overweight U.S. adults: 67%
U.S. adults with obesity: 33%
U.S. children with obesity: 17%
Annual U.S. health care expenditures for obesity: $ 147 billion
U.S. consumer expenditures for weight loss products: $ 50 billion
Weekly deaths from obesity complications > 6,000
Page 7
MGH Weight Center
Disproportional Increase in Severe Obesity
More than 1,000,000 U.S. adults now have a BMI >50
Sturm R. Health Aff, 2004
Page 8
MGH Weight Center
Complications of Obesity
Degenerative
Structural
Metabolic
Psychological
Neoplastic
Socioeconomic
Page 9
MGH Weight Center
Average years of life lost from obesity at age 30
BMI = 30 BMI = 40 BMI > 45
White men 1 5 11
White women 1 4 8
Black men 0 5 14
Black women 0 1 5
Obesity Shortens Life Expectancy
Page 10
MGH Weight Center
Most Common Undertreated Complications
• Obstructive sleep apnea
• Fatty liver disease
• Gastroesophageal reflux disease
• Fungal skin infections
• Nutrient deficiencies• from recurrent dieting and inadequate
nutrition during rebound weight gain
Page 11
MGH Weight Center
Feedback Regulation of Energy Metabolism
Adiposetissue
Leptin
CNS
Food intakeNutrient handling
Energy expenditure
LiverMuscle
Metabolic needs
Sensory OrgansGI Tract
Environmentalsensing
Energystores
Page 12
MGH Weight CenterMGH Weight Center
Defending a Body Energy Defending a Body Energy ““Set PointSet Point””
2020 2525 3030 3535
Body Mass Index (kg/mBody Mass Index (kg/m22))
kcal
/ 24
hou
rskc
al /
24 h
ours
20002000
25002500
30003000EnergyEnergyExpenditureExpenditure
EnergyEnergyIntakeIntake
((––) Energy Balance) Energy Balance(+) Energy Balance(+) Energy Balance
Page 13
MGH Weight CenterMGH Weight Center
BMIBMI
2020 2222 2424 2626 2828 3030 3333 3636 3939 4242 4646 5050 5555 6060
Natural Variation and Zones of OpportunityNatural Variation and Zones of Opportunity
ExcellentExcellent PoorPoor
Degree of ControlDegree of Control
Page 14
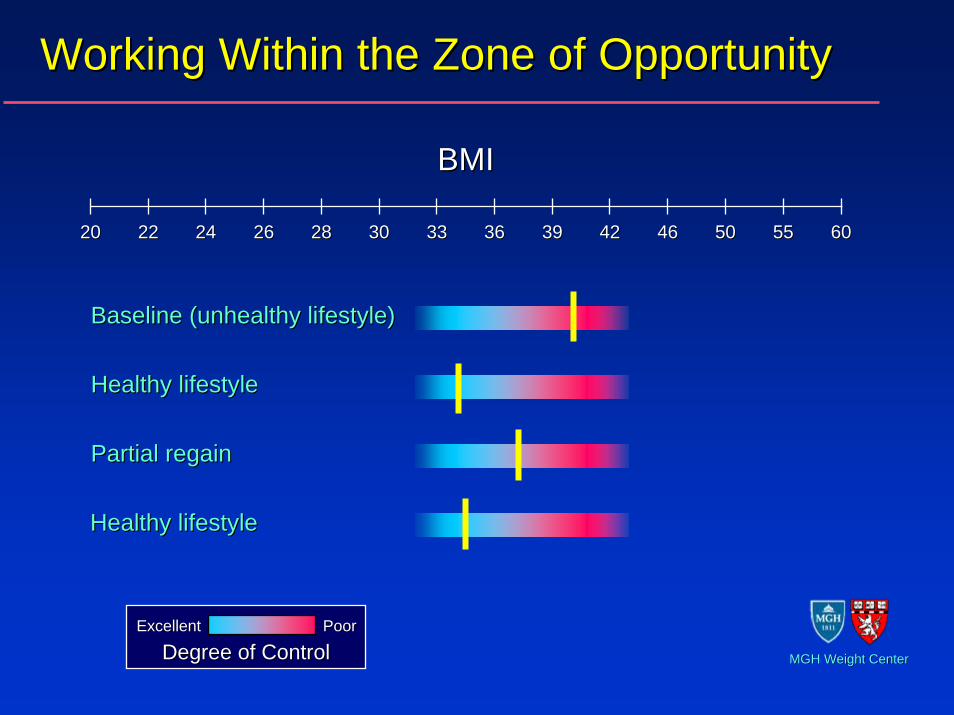
Working Within the Zone of OpportunityWorking Within the Zone of Opportunity
BMIBMI
2020 2222 2424 2626 2828 3030 3333 3636 3939 4242 4646 5050 5555 6060
Healthy lifestyleHealthy lifestyle
Partial regainPartial regain
Baseline (unhealthy lifestyle)Baseline (unhealthy lifestyle)
ExcellentExcellent PoorPoor
Degree of ControlDegree of Control
Healthy lifestyleHealthy lifestyle
MGH Weight CenterMGH Weight Center
Page 15
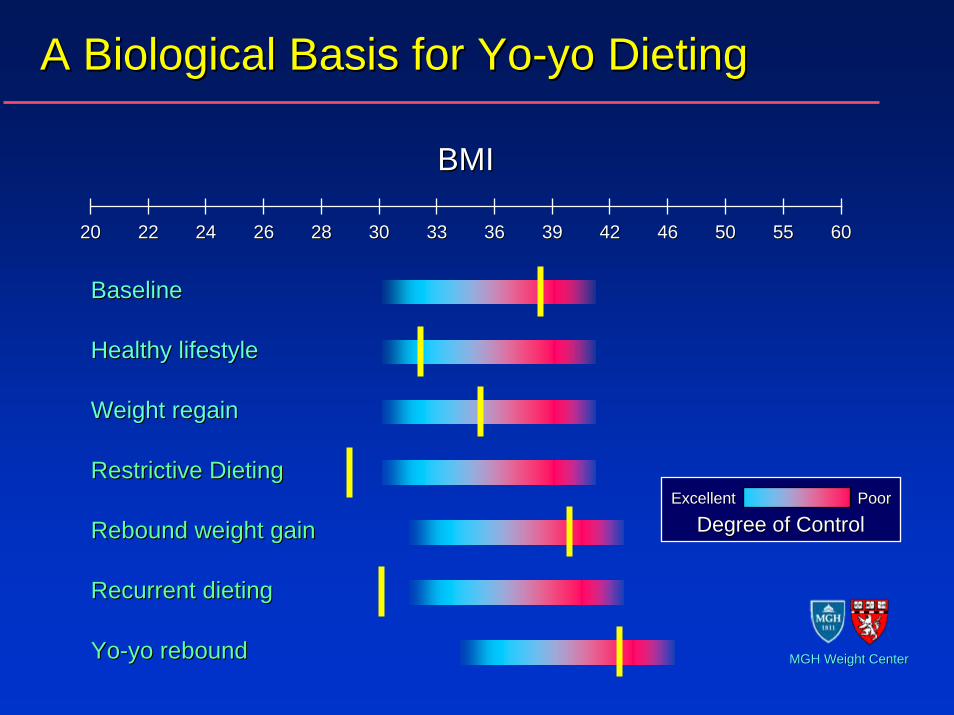
Restrictive DietingRestrictive Dieting
A Biological Basis for YoA Biological Basis for Yo--yo Dietingyo Dieting
BMIBMI
2020 2222 2424 2626 2828 3030 3333 3636 3939 4242 4646 5050 5555 6060
Healthy lifestyleHealthy lifestyle
Weight regainWeight regain
Rebound weight gainRebound weight gain
BaselineBaseline
Recurrent dietingRecurrent dieting
YoYo--yo reboundyo rebound
ExcellentExcellent PoorPoor
Degree of ControlDegree of Control
MGH Weight CenterMGH Weight Center
Page 16
MGH Weight Center
Treatment of the Patient with Obesity
Page 17
MGH Weight Center
Approach to the Patient with Obesity
• Respect the patient • Avoid pejorative language
• “Morbid,” “obese,” “recidivism”
• Understand the challenges faced by the patient• The blame game is nonproductive (no one wants this problem)• Optimize your office environment
• Physical facilities – chairs, scales, exam tables, gowns, etc.• Staff approach and attitudes
• Work to develop a therapeutic partnership• There is no quick or reliably effective therapy• Success often comes after a “trial-and-error” testing of different
approaches• Start with lifestyle but communicate that there are other
approaches to be considered as needed
Page 18
MGH Weight Center
Approach to the Patient with Obesity
• Demonstrate understanding of the problem• Obesity is devastating in ways that go far beyond the
medical implications• Durable weight loss is extremely difficult (or impossible)• Improved lifestyle is achievable but may not lead to
weight loss• Different people respond to different interventions very
differently• Take aim at the causes of obesity
• Food quality (even more than quantity)• Physical activity and muscle function• Mental health (stress and distress)
• Focus on important non-weight loss outcomes• Quality of life• Heath risks (cardiovascular, diabetes, cancer)
Page 19
MGH Weight Center
Approach to the Patient with Obesity
Identify and treat obesity complications• Medical• Psychological• Socioeconomic
Reduce obesity-based disparities in care• Ensure appropriate screening
• Recognize challenges to diagnosis (physical and technical limitations)
• Consider effects of obesity on treatment paradigms
Treat the obesity itself
Page 20
MGH Weight Center
Treatment of Obesity Itself
Treat underlying disorders• Drugs are common• Endocrine causes are rare
Stepwise care plan
• Lifestyle modification• Healthy diet• Regular physical activity
• Medications
• Surgery
Anticipate slow progress
Page 21
MGH Weight Center
Obesity Treatment Pyramid
Lifestyle Modification
Healthy Diet Physical Activity
Pharmacotherapy
Surgery
Page 22
MGH Weight Center
Behavioral Therapies
• Physical activity
• Problem solving
• Self-monitoring
• Stress management
• Continued contact
Predictors of Weight MaintenancePredictors of Weight Maintenance
Page 23
MGH Weight CenterMGH Weight Center
-22
-18
-14
-10
-6
-2
2
6
0 0.5 1 1.5 2 2.5 3 3.5 4
Year
Cha
nge
in W
eigh
t (kg
)
PlaceboMetforminLifestyle
Nathan D Nathan D et al.et al., , NEJMNEJM 20022002
Intensive Dietary InterventionIntensive Dietary Intervention
Diabetes Prevention ProgramDiabetes Prevention Program
Page 24
MGH Weight CenterMGH Weight Center
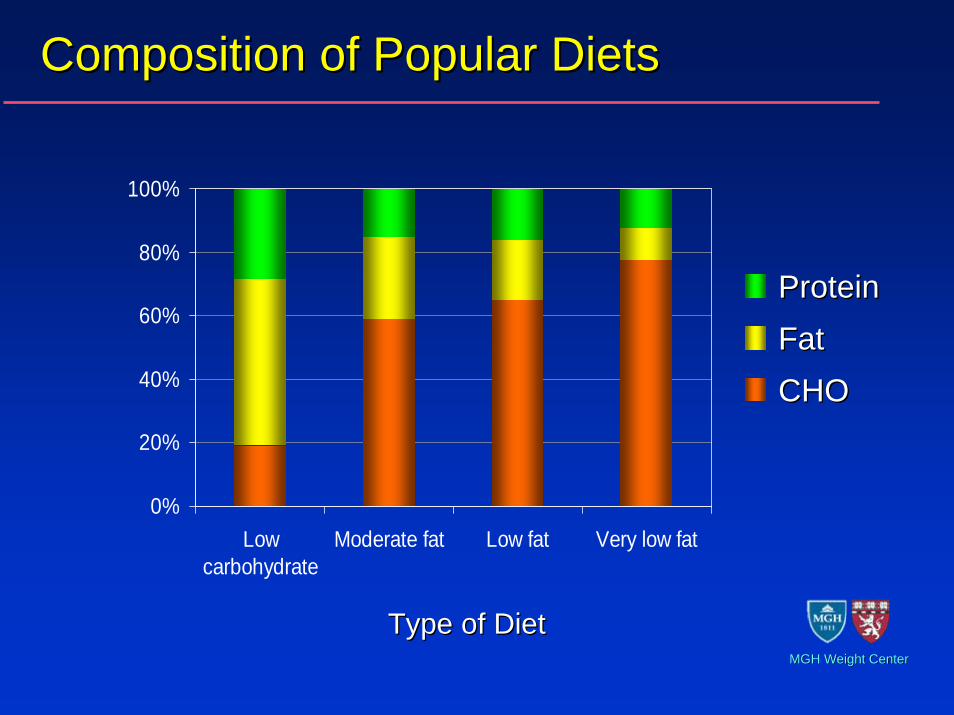
Composition of Popular DietsComposition of Popular Diets
0%
20%
40%
60%
80%
100%
Lowcarbohydrate
Moderate fat Low fat Very low fat
Type of DietType of Diet
ProteinProtein
FatFat
CHOCHO
Page 25
MGH Weight CenterMGH Weight CenterFoster Foster et al.et al., , NEJMNEJM 20032003
DietDiet--induced Weight Lossinduced Weight Loss
-24
-20
-16
-12
-8
-4
0
0 3 6 9 12Time (months)
Cha
nge
in W
eigh
t (%
)
LowLow--fatfat
LowLow--carbcarb** **
Baseline Values Carried Forward AnalysisBaseline Values Carried Forward Analysis
}}
**p p < 0.05< 0.05
N.S.N.S.
Page 26
MGH Weight CenterMGH Weight Center
Medications Approved for ObesityMedications Approved for Obesity
MedicationMedication Mechanism of ActionMechanism of Action Potential Side EffectsPotential Side Effects
SibutramineSibutramine -- CCIVIV
(Meridia(Meridia™™))Adrenergic, Serotonergic,Adrenergic, Serotonergic,
DopaminergicDopaminergicHypertension, tachycardiaHypertension, tachycardia
(avoid use with SSRIs)(avoid use with SSRIs)
OrlistatOrlistat(Xenical(Xenical™™))
Lipase InhibitorLipase Inhibitor Steatorrhea, incontinenceSteatorrhea, incontinence
PhenterminePhentermine -- CCIVIV
(Adipex(Adipex™™, Ionamin, Ionamin™™))AdrenergicAdrenergic Tachycardia, hypertensionTachycardia, hypertension
Diethylpropion Diethylpropion -- CCIVIV
(Tenuate(Tenuate™™))AdrenergicAdrenergic Tachycardia, HTN, anxietyTachycardia, HTN, anxiety
Benzphetamine Benzphetamine -- CCIIIIII
(Didrex(Didrex™™))AdrenergicAdrenergic Tachycardia, HTN, anxietyTachycardia, HTN, anxiety
Phendimetrazine Phendimetrazine -- CCIIIIII
(Bontril(Bontril™™, Prelu, Prelu--22™™))AdrenergicAdrenergic Tachycardia, HTN, anxietyTachycardia, HTN, anxiety
Page 27
MGH Weight CenterMGH Weight CenterTorgenson Torgenson et alet al., ., Diabetes CareDiabetes Care 20042004
Orlistat Induces Weight LossOrlistat Induces Weight Loss
PlaceboPlacebo
OrlistatOrlistat
00 5252 104104 156156 208208--1212
--99
--66
--33
00
Time (weeks)Time (weeks)
Wei
ght C
hang
e (k
g)W
eigh
t Cha
nge
(kg)
Page 28
MGH Weight CenterMGH Weight Center
Randomization at 6 months Randomization at 6 months in those with in those with ≥≥ 5% initial weight loss5% initial weight loss
00 121222 44 66 88 1010 1414 1616 1818 2020 2222 2424MonthMonth
Bod
y W
eigh
t (lb
s.)
Bod
y W
eigh
t (lb
s.)
Weight LossWeight Loss Weight MaintenanceWeight Maintenance230230
210210
195195
225225
220220
215215
205205
200200
PlaceboPlacebo
Sibutramine 10Sibutramine 10--20 mg/d20 mg/d
Weight Maintenance on SibutramineWeight Maintenance on Sibutramine
James James et alet al.,., LancetLancet 20002000
Page 29
MGH Weight CenterMGH Weight Center
Weight Loss from Other MedicationsWeight Loss from Other Medications
MedicationMedication Indicated UsesIndicated Uses CommentsComments
BupropionBupropion DepressionDepression Avoid in bipolar diseaseAvoid in bipolar disease
TopiramateTopiramateSeizuresSeizuresMigrainesMigraines
Mood disordersMood disorders
May produce neurological side May produce neurological side effectseffects
ZonisamideZonisamideSeizuresSeizures
Mood disordersMood disordersFew studiesFew studies
MetforminMetforminType 2 diabetesType 2 diabetes
PCOSPCOSRare liver toxicityRare liver toxicity
ExenatideExenatide Type 2 diabetesType 2 diabetes InjectableInjectable
PramlintidePramlintide Type 2 diabetesType 2 diabetes InjectableInjectable
Strategy: Aim for Double Benefits when PossibleStrategy: Aim for Double Benefits when Possible
Page 30
MGH Weight CenterMGH Weight Center
Van der Merwe T Van der Merwe T et alet al., 12th European Congress on Obesity 2003., 12th European Congress on Obesity 2003
Topiramate Induces Weight LossTopiramate Induces Weight Loss
Time (weeks)Time (weeks)
--22
--44
--66
--88
--1010
--1212
--1414
--16160 4 8 12 16 20 24 28 32 36 0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72 7640 44 48 52 56 60 64 68 72 76
+2+2
00**PlaceboPlacebo
Topiramate 96 mg/d Topiramate 96 mg/d Topiramate 192 mg/d Topiramate 192 mg/d Topiramate 256 mg/d Topiramate 256 mg/d
Wei
ght C
hang
e (%
)W
eigh
t Cha
nge
(%)
Page 31
MGH Weight CenterMGH Weight Center
Time (Months)Time (Months)
Wt Loss Wt Loss Wt MaintenanceWt Maintenance
PramlintidePramlintide(120 mcg tid) (120 mcg tid)
Aronne L Aronne L et alet al., ., JCEMJCEM 20072007
00 22 44 66 88 1010 1212--1010--99--88--77--66--55--44--33--22--1100
PlaceboPlaceboW
eigh
t Cha
nge
(kg)
Wei
ght C
hang
e (k
g)
Pramlintide Induces Weight LossPramlintide Induces Weight Loss
Page 32
MGH Weight Center
Medication-induced Weight Gain
Medications likely account for 5-10% of obesity in the U.S.
Page 33
MGH Weight CenterMGH Weight Center
Treatment of MedicationTreatment of Medication--induced Obesity induced Obesity
CategoryCategory Common Weight Gain Common Weight Gain Promoting MedicationsPromoting Medications
Potential Alternatives that Potential Alternatives that Promote Less Weight GainPromote Less Weight Gain
SSRIsSSRIsCelexaCelexa™™, Lexapro, Lexapro™™
PaxilPaxil™™ProzacProzac™™, Zoloft, Zoloft™™
BupropionBupropion
Mood stabilizersMood stabilizersOlanzapine (ZyprexaOlanzapine (Zyprexa™™) ) Clozapine (ClozarilClozapine (Clozaril™™))
RisperidoneRisperidone
Topiramate, ZonisamideTopiramate, ZonisamideGeodonGeodon™™
AnticonvulsantsAnticonvulsants ValproateValproatePhenytoinPhenytoin
TopiramateTopiramate
Insulinotropic Insulinotropic agentsagents
Insulin, SulfonylureasInsulin, SulfonylureasThiazolidinedionesThiazolidinediones
PramlintidePramlintideExenatideExenatide
SteroidsSteroids CorticosteroidsCorticosteroidsImmunosuppressantsImmunosuppressants
TNFTNFαα blockersblockers
Strategy: Replace Weight Gain Promoting MedicationsStrategy: Replace Weight Gain Promoting Medications
Page 34
MGH Weight Center
Wadden T Wadden T et alet al., ., NEJMNEJM 20052005
Behavior Therapy Augments Sibutramine
Sibutramine and behavioral therapy
Sibutramine alone
Wei
ght C
hang
e (k
g)
Time (weeks)
Page 35
MGH Weight Center
5-year
1-5
1-5
50-70
Weight Loss (% of patients):
Comprehensive, behavior-based(diet and exercise)
Medications(sibutramine, orlistat, phentermine)
Surgery(gastric bypass, gastroplasty)
6-month
60-75
70-90
80-90
Efficacy of Current Therapies
Page 36
MGH Weight Center
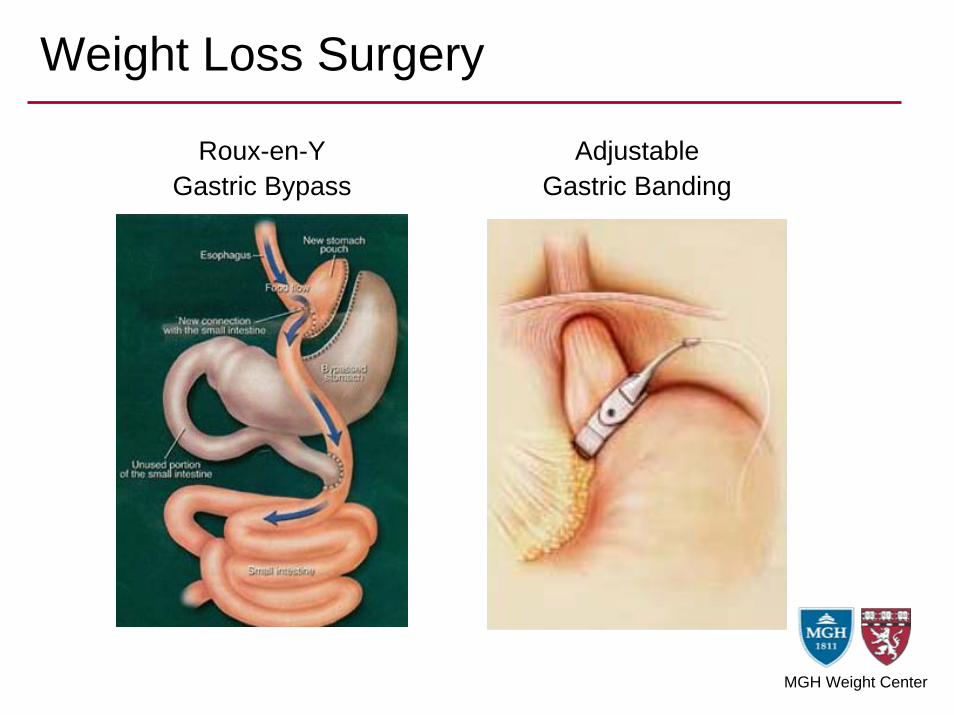
Weight Loss Surgery
Roux-en-YGastric Bypass
AdjustableGastric Banding
Page 37
MGH Weight CenterMGH Weight Center
Effectiveness of Obesity TreatmentsEffectiveness of Obesity Treatments
-50
-40
-30
-20
-10
0
0 2 4 6 8 10
Time After Surgery (years)
Per
cent
Tot
al W
eigh
t Los
s Lifestyle &Medications
GastricBanding
GastricBypass
Swedish Obesity SubjectsSwedish Obesity SubjectsDiabetes Prevention ProgramDiabetes Prevention Program
Page 38
MGH Weight Center
Outcomes of Gastric Bypass
Disorder % Improved % ResolvedDiabetes mellitus 100 82Gastroesophageal reflux 96 72Hypercholesterolemia 96 63Peripheral edema 96 41Obstructive sleep apnea 93 74Hypertension 88 70Osteoarthritis 88 41Gout 86 72Hypertriglyceridemia 86 57Urinary incontinence 83 44Asthma 82 13Depression 55 8
Page 39
MGH Weight Center
Complications of Gastric Bypass
Need for re-operation 5 %Major wound infections 2 %Anastomotic ulcer/obstruction 5 %Persistent dumping syndrome 3 %Micronutrient deficiency 22 %Steatohepatitis 3 %Symptomatic gallstones 2 %Venous thrombosis 2 %Anastomotic leak 0.7 %Overall major morbidity 10 %Overall mortality 0.3 %
Page 40
MGH Weight Center
Surgery Decreases Long-term Mortality
• 15850 gastric bypass patients and matched controls (Utah)
• 7.1 year mean follow-up
• Gastric bypass group exhibited overall 40% reduction in mortality
• Specific-cause mortality after gastric bypass• 56% reduction from CAD• 92% reduction from type 2 diabetes• 60% reduction from cancer• 58% increase for accidents or suicide
Adams et al., NEJM 2007
Page 41
MGH Weight Center
Indications for Weight Loss Surgery
1. BMI > 35 in association with major medical complications of obesity
ORBMI > 40
(more stringent BMI criteria for adolescents)
2. Failure of other approaches to long-term weight loss
Page 42
MGH Weight Center
Contraindications to Surgery
• End-stage lung disease
• Unstable cardiovascular disease
• Multiorgan failure
• Gastric varices
• Uncontrolled psychiatric disorder
• Ongoing substance abuse
• Age > 75 or < 15 years
• Noncompliant patient
Page 43
MGH Weight Center
• Embrace modest weight loss• Focus on what is achievable – and sustainable• Understand biological limits • Be clear about what treatment can and cannot do
• Understand that one size does not fit all
• Cherish non-weight outcomes• Recognize all successes of therapy
• Go slow, gain the patient’s confidence, and try different approaches (“Pac-Man”)
• Focus more on what you can offer more than how the patient behaves
Practical Guidance
Page 44
MGH Weight Center
Practical Guidance
• Be realistic
• Be optimistic
• Be encouraging
• Be there
Page 45
MGH Weight Center
Partners Community Health, Inc.
Understanding and Treating ObesityLee M. Kaplan, MD, PhDMassachusetts General HospitalHarvard Medical School
[email protected]
September 14, 2010
Page 46
MGH Weight Center
October• Employee Engagement
• 10/7 at 12:15pm
• Health Literacy & Patient Education in PC• 10/14 at 12:15pm
• Program and Course Informationwww.massgeneral.org/stoecklecenter/pec/course_catalog
Upcoming Webinars, Programs, Services
Page 47
MGH Weight Center
• Today’s session - available online.
• Evaluations
Thank you for your participation!
Wrap-Up