1 Understanding EKG’s Rhythm Recognition Review This packet is designed to be utilized in our instructor lead EKG review program for those somewhat familiar with the concept of EKG interpretation. This program will emphasize the recognition of ar rhythmias for the basic EKG provider. The participant will receive information and practice in the review of rhythms originating in the Atria, Junction, and Ventricles as well as heart blocks and pacemaker recognition. Clinical significance and general medical management will be reviewed with those rhythms requiring treatment. The participant attending this particular program should be a medical professional with a basic understanding of cardiac anatomy, physiology and electrophysiology prior to entering the course. All profe ssionals s hould re view thes e areas b efore tak ing our R hythm Re cognition Review. For more EKG practice, log onto www.Skillstat.com!
This packet is designed to be utilized in our instructor lead EKG review program for thosesomewhat familiar with the concept of EKG interpretation.
This program will emphasize the recognition of arrhythmias for the basic EKG provider. Theparticipant will receive information and practice in the review of rhythms originating in the Atria,
Junction, and Ventricles as well as heart blocks and pacemaker recognition.
Clinical significance and general medical management will be reviewed with those rhythms
requiring treatment.
The participant attending this particular program should be a medical professional with a basicunderstanding of cardiac anatomy, physiology and electrophysiology prior to entering the
course.
All professionals should review these areas before taking our Rhythm Recognition Review.
For more EKG practice, log onto www.Skillstat.com!
The heart is a hollow, four chambered organ that lies in the mediastinal cavity, betweenthe right and left lungs, just behind the sternum. The slight leftward tilt of the heartplaces about two thirds of its mass to the left of the midline of the body, and one third tothe right. The average adult heart is 5 inches long and 31/2 inches wide, or about thesize of a man’s clenched fist. The following, figure 1, shows how the heart’s borderscorrespond to other anatomical structures in the chest:
(Figure 1)
There are four main heart surfaces to consider Lateralwhen talking about the heart:
The heart is composed of striated muscle in several layers:
The pericardium is the outermost layer, composed of two parts- the fibrous pericardium is the loose fitting, fibrous sac that surrounds the heart. This sac is in directcontact with the pleura, the covering of the lungs. The serous pericardium lines theouter surface of the heart and secretes a slippery fluid, which allows easy movement of the heart during expansion and contraction.
The myocardium is the middle muscle layer, which is responsible for the major work,or pumping, of the heart, and makes up the majority of the bulk of the heart wall. Themyocardium contains contractile fibers as well as the conduction system and bloodsupply of the heart.
The endocardium is the thin layer of tissue that lines the inner chambers and thevalves of the heart.
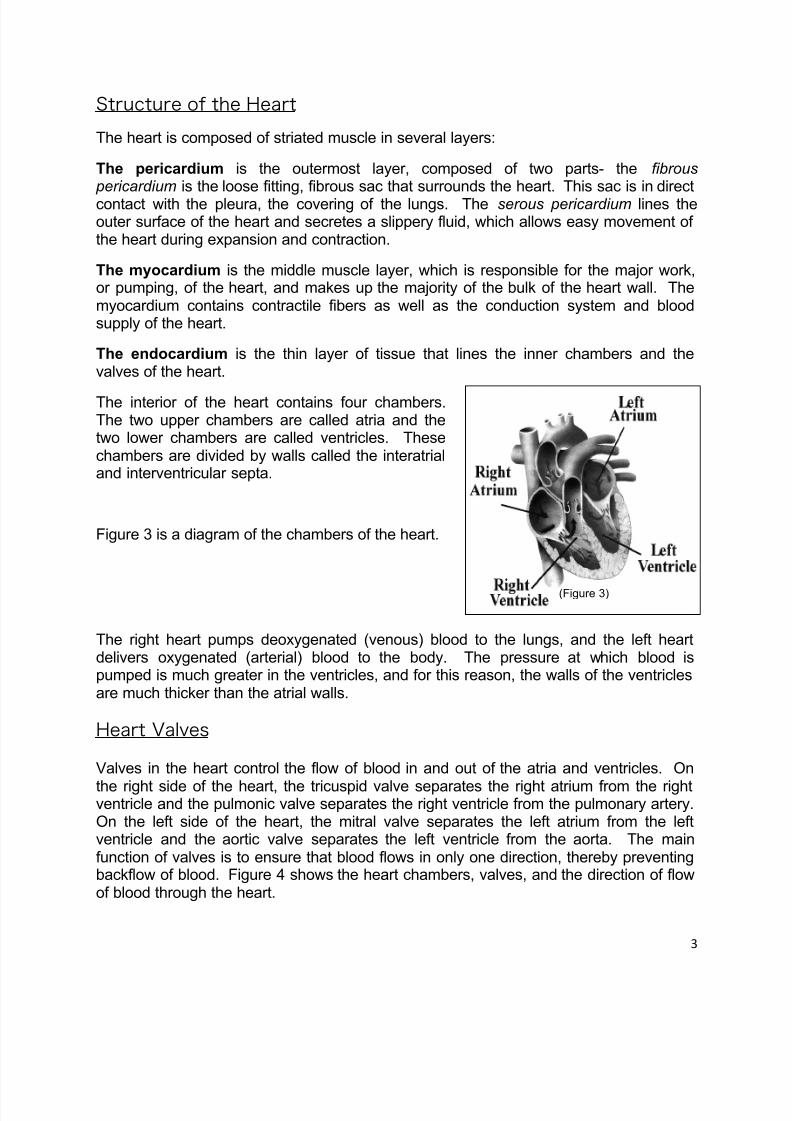
The interior of the heart contains four chambers.The two upper chambers are called atria and thetwo lower chambers are called ventricles. Thesechambers are divided by walls called the interatrialand interventricular septa.
Figure 3 is a diagram of the chambers of the heart.
(Figure 3)
The right heart pumps deoxygenated (venous) blood to the lungs, and the left heartdelivers oxygenated (arterial) blood to the body. The pressure at which blood ispumped is much greater in the ventricles, and for this reason, the walls of the ventriclesare much thicker than the atrial walls.
Heart Valves
Valves in the heart control the flow of blood in and out of the atria and ventricles. On
the right side of the heart, the tricuspid valve separates the right atrium from the rightventricle and the pulmonic valve separates the right ventricle from the pulmonary artery.On the left side of the heart, the mitral valve separates the left atrium from the leftventricle and the aortic valve separates the left ventricle from the aorta. The mainfunction of valves is to ensure that blood flows in only one direction, thereby preventingbackflow of blood. Figure 4 shows the heart chambers, valves, and the direction of flowof blood through the heart.
Blood flow through the heart begins in theheart’s right side and is unidirectional.Unoxygenated blood enters the right atrium
via the superior vena cava, inferior venacava and coronary sinus.
When the right atrium contracts, bloodpasses through the tricuspid valve to theright ventricle. From the right ventricle,blood is ejected through the pulmonic valve to the pulmonary artery , which carries bloodto the lungs, where the blood releasesexcess carbon dioxide and picks upoxygen.
(Figure 4)
Oxygenated blood returns to the heart via the pulmonary veins to the left atrium. Whenthe left atrium contracts: blood is ejected through the mitral valve to the left ventricle,then from the left ventricle through the aortic valve to the aorta, for distribution throughthe body.
A recap of the flow of blood through the heart and lungs:
• The Superior Vena Cava/Inferior Vena Cava transports blood to the Right Atrium
• The Right Atrium transports blood through the Tricuspid Valve to the RightVentricle
• The Right Ventricle transports blood through the Pulmonic Valve to the lungs andthe Pulmonic Veins
• Blood returns via the Vena Cava to the Left Atrium
• The Left Atrium transports blood through the Mitral Valve to the Left Ventricle
• The Left Ventricle transports blood through the Aortic Valve to the Aorta
• The Aorta transports blood to the Coronary Arteries of the heart and the SystemicCirculation
The heart is supplied with blood by the right and left coronary arteries, which arise fromthe aorta.
The Right Coronary Artery (RCA) travels down the right side of the heart and curvesaround the interior wall. It also supplies blood to the posterior wall via the posterior descending artery in most people. Therefore, occlusion of the right coronary arteryresults in inferior wall or posterior wall myocardial infarction. The RCA also suppliesblood to the following heart structures:
• SA node in 50% of the population
• AV node in 90% of the population
• Right Atrium and Right Ventricle
• Inferior Wall of the Left Ventricle
• Posterior Wall of the Left Ventricle
The Left Coronary Artery has two branches: the Left Anterior Descending (LAD)Branch, which supplies the anterior wall of the heart, and the Circumflex (Cx), whichtravels down the lateral wall of the heart. Occlusion of the LAD results in anterior wallMI and occlusion of the Circumflex results in a lateral wall myocardial infarction.
The LAD also supplies blood to the following heart structures:
• Anterior wall of the Left Ventricle
• Interventricular septum
• Right Bundle Branch
• Anterior fascicle of the left bundle branch
The Circumflex also supplies the following heart structures:
• SA Node in 50% of the population
• AV Node in 50% of the population
• Left Atrium
• Lateral wall of the left ventricle
• Posterior wall of the left ventricle in 10% of the population
The heart is composed of electrical (pacemaker) cells and myocardial (working) cells.
The electrical cells are responsible for the generation and conduction of impulses, whilethe myocardial cells are responsible for the response to those impulses-contraction.
The electrical cells are arranged alon the conduction pathways in the heart and possessthree properties:
• Automaticity - the ability of a cell to generate and discharge electrical impulses
• Excitability - the ability to respond to electrical impulses
• Conductivity - the ability to transmit electrical impulses between cells
The myocardial cells form the layers of the atrial and ventricular walls and possess twoproperties:
• Contractility - the ability of a cell to shorten and lengthen in response to stimuli
• Extensibility - the ability of the cell to stretch
Depolarization and Repolarization
The electrical impulses generated by heart cells are created by the flow of positivelycharged ions back and forth across the cardiac cell membrane. This flow of ions results
in depolarization (electrical activation), contraction, and repolarization (recovery) of thecell. Sodium (the primary extracellular ion) and potassium (the primary intracellular ion)are the electrolytes responsible for regulating electrical charges.
In the resting state, potassium is inside the cell, and the inside of the cell membrane isnegatively charged, while sodium is outside, and the outside of the cell membrane ispositively charged. (see figure 6)
Once an electrical impulse is generated, sodium quickly moves into the cell andpotassium moves out, changing the electrical charge inside the cell to positive. The cellis then considered depolarized.
As soon as depolarization is complete, repolarization begins, with potassium movinginto the cell and sodium moving out, until repolarization is complete and the cell is backat its resting charge of negative on the inside and positive on the outside.
Depolarization of one cell stimulates the depolarization of adjacent ones, creating a“domino effect” which produces the electrical current that is detected by skin electrodesand translated to waveforms on ECG graph paper.