epartment of Oral & Maxillofacial Surgery, Meenakshi Ammal Dental College & Hospital, Alapakkam Main Road, Maduravoyal,amil Nadu, India
eceived 28 October 2011; accepted 13 December 2011
C
AtndmrCsmdL
urdm
he term Schneiderian mucosa refers to the ectodermallyerived lining of the nasal cavity and paranasal sinuses, com-osed generally of stratified ciliated columnar cells, loosebundant lamina propria, and minor salivary glands and theiructs. This unique mucosa may give rise to three distinctistomorphologic papillomas collectively called Schneide-ian papillomas. Hyams1 has described these variants andategorized them as inverted, fungiform (exophytic, squa-ous) and oncocytic Schneiderian papilloma (cylindrical cellapilloma) based on their pattern of growth. Schneide-ian papillomas are uncommon, representing only 0.4%---4.7%f all sinonasal tumors.2---4 Oncocytic Schneiderian papillo-as are the rarest of the three morphological variants,
ccounting for only 3 per cent of all sinonasal papillomas.3,4
inonasal papillomas have a small but distinct risk ofalignant transformation.5---10 Here, we report a case
f undifferentiated carcinoma arising from oncocyticchneiderian papilloma (OSP). To the best of our knowledge,
he current patient is the fourth reported case of undiffer-ntiated carcinoma arising in OSP in English literature.
� Please cite this article as: Devadoss P, et al. Carcinoma indifer-nciado en el papiloma oncocítico Schneideriano. Una rareza. Actatorrinolaringol Esp. 2013;64:306---309.∗ Corresponding author.
75-year-old lady presented with recurrent unilateral epis-axis associated with progressive nasal blockage and rightasal purulent discharge with a foul odor of eight monthsuration. Clinical examination revealed a fleshy, polypoidass arising from right lateral nasal mucosa obstructing the
ight nostril with diffuse swelling on the right side of face.omputed tomography confirmed the presence of soft tis-ue mass in the right lateral nasal cavity and opacification ofaxillary and frontal and ethmoid sinuses (Fig. 1). No bonyestruction was noted. Incisional biopsy through Caldwelluc approach revealed it to be a case of OSP.
The patient was subjected to general anaesthetiander nasoendotracheal intubation on left side for lateralhinotomy with medial maxillectomy and frontoethmoi-ospenoidectomy. Intraoperatively, multiple polypoidalasses were found involving right lateral wall of the nasal
avity with extension into the all paranasal sinuses onhe right side. The entire tumor mass was delivered enasse and subjected to histopathological examination after
taining with hematoxylin---eosin. Other confirmatory testsike immunohistochemical analysis were not carried out for
ack of sufficient resources. The patient had an unevent-ul postoperative recovery. She was last seen six monthsost operatively and there was no recurrence noted. Theatient is being followed periodically for any evidence of
Figure 4 Transition of OSP epithelium from low-grade (1) tohn
heterogenous soft tissue density over right lateral nasal cavityand the paranasal air sinuses.
recurrence. This study followed the Declaration of Helsinkion medical protocol and ethics and the regional EthicalReview Board of Meenakshi Ammal Dental College & Hospitalapproved the study.
On histological examination, the multiple polypoidlesions showed a central core of connective tissue com-posed of multilayered columnar type of epithelium. Theepithelium was thrown into numerous papillary projectionsexhibiting both endophytic and exophytic growth patternsindicative of OSP (Fig. 2). The epithelium was made oftall columnar cells with small dark nuclei and eosinophilicgranular cytoplasm. Connective tissue stroma is myxoma-tous and edematous showing minimal chronic inflammatorycell infiltrate predominantly of lymphocytes and plasmacells. The specimen also showed malignant cells arrangedin sheets, islands and in papillary pattern. The tumor cells
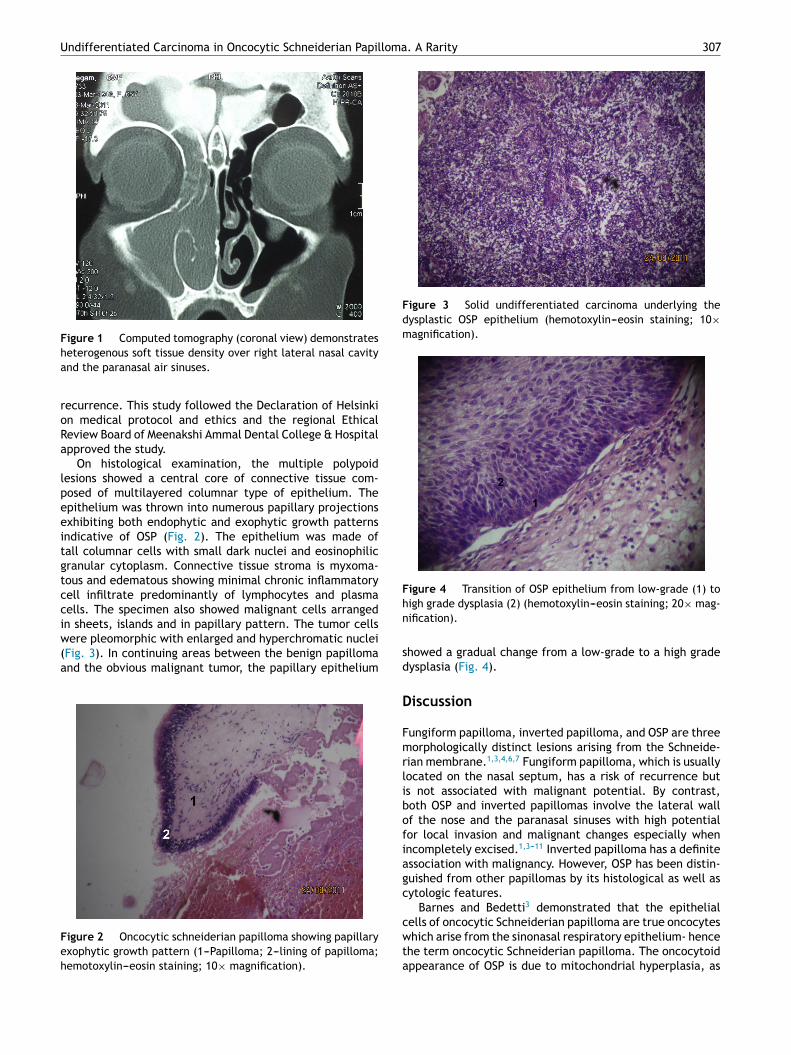
were pleomorphic with enlarged and hyperchromatic nuclei(Fig. 3). In continuing areas between the benign papillomaand the obvious malignant tumor, the papillary epithelium
howed a gradual change from a low-grade to a high gradeysplasia (Fig. 4).
iscussion
ungiform papilloma, inverted papilloma, and OSP are threeorphologically distinct lesions arising from the Schneide-
ian membrane.1,3,4,6,7 Fungiform papilloma, which is usuallyocated on the nasal septum, has a risk of recurrence buts not associated with malignant potential. By contrast,oth OSP and inverted papillomas involve the lateral wallf the nose and the paranasal sinuses with high potentialor local invasion and malignant changes especially whenncompletely excised.1,3---11 Inverted papilloma has a definitessociation with malignancy. However, OSP has been distin-uished from other papillomas by its histological as well asytologic features.
Barnes and Bedetti3 demonstrated that the epithelial
ells of oncocytic Schneiderian papilloma are true oncocyteshich arise from the sinonasal respiratory epithelium- hence
he term oncocytic Schneiderian papilloma. The oncocytoidppearance of OSP is due to mitochondrial hyperplasia, as
3
ta
btitoOoTcsseaSd
etmeesdn
gogwTsccn
iolicw1c1tp1acacrediTiic
wmuoYfadti
ciloohntp
nOtiltwat
tlpian
C
T
R
08
hey are in oncocytes of varied tissues, such as oncocytoma,nd Hurthle cell or Warthin’s tumor.
Oncocytic Schneiderian papilloma are equally distributedetween the sexes, and the majority of patients are morehan 50 years of age at the time of diagnosis.1---8 Theres no sex predilection, unlike in inverted and fungiformypes which occur predominantly in males. Unilateral nasalbstruction is the most common presenting symptom forSP. Intermittent epistaxis and pain are also reported. Rhin-rrhea, sinusitis and allergic symptoms are rarely described.he duration of symptoms is usually months to years. Allases known to date have been unilateral.8,12,13 A grosshaggy or papillary configuration is most typical. However,mooth, edematous, polypoid lesions are not uncommon asvidenced in our patient. Routine sinus radiographs revealbnormalities confined to the ipsilateral sinonasal passages.inus opacification associated with an intranasal soft tissueensity is the predominant finding.
The radiographic findings vary with the extent of the dis-ase. Early on, there may be only a soft tissue density withinhe nasal cavity and/or paranasal sinuses.12---17 Later, withore extensive disease, unilateral opacification and thick-
ning of one or more of the sinuses are common, as arexpansion and displacement of adjacent structures. Pres-ure erosion of bone may also be apparent, and must beistinguished from osseous invasion associated with malig-ancy.
Grossly, OCP appears as a fleshy pink papilloma orray polypoidal growth. The classic histologic descriptionf OCP is the presence of both exophytic and invertedrowth patterns, composed of multilayers of columnar cellsith eosinophilic cytoplasm and small uniform dark nuclei.he epithelial cells of OCP are true oncocytes from theinonasal respiratory epithelium and hence the term onco-ytic Schneiderian papilloma was used. The epitheliumharacteristically contains small cysts filled with mucin oreutrophils (microabscess).1,3
Although the clinical behavior of OSP parallels that ofnverted papilloma, it appears to have a higher frequencyf association with malignancy (10% to 17%) compared to theater (5% to 10%).1---7,9---11 Fortunately, the incidence of OSPs much lower than that of inverted papilloma. Of the 178ases of OSP previously reported in the English literaturehich constitute 3% to 10% of Schneiderian papillomas, only3 cases were found to be associated witharcinoma.1,2,5,8---10 But Maitra et al.11 study reported6 cases of malignancies arising in OSP. Hyams1 reportedhe first case of OSP (which he named cylindrical cellapilloma) associated with invasive carcinoma among0 cases of OSP. Barnes and Bedetti3 described a casessociated with mucoepidermoid carcinoma among sixases of OSP. However, the relationship between carcinomand the epithelium of OSP is unclear. The evidence thatarcinomas can arise in an OSP came when Ward et al.9
eported two cases of OSP, associated with poorly differ-ntiated squamous cell carcinoma in one case, but poorlyifferentiated nonkeratinizing carcinoma and papillaryntermediate (transitional) cell carcinoma in the other.
heir study is the first to document dysplastic epithelium
n OSP, which they claimed can be the site of origin fornvasive carcinoma. Kapadia et al.10 reported nine cases ofarcinoma in OSP, among which six cases were associated
P. Devadoss et al.
ith squamous cell carcinoma, two cases with high gradeucoepidermoid carcinoma, and one case with sinonasal
ndifferentiated carcinoma. This was the first reported casef undifferentiated carcinoma arising from OSP. Moreover,ang and Abraham2 also reported a case of sinonasal undif-erentiated carcinoma. Using morphological, histochemicalnd immunohistochemical analysis, they were able toemonstrate the malignancy associated with the OSP. Thehird case of sinonasal undifferentiated carcinoma arisingn OSP was reported by Maitra et al.11
In our case, the oncocytic features of this papilloma werelearly demonstrated histomorphologically. It is of utmostmportance to determine the origin of carcinoma in papil-oma. It could be either arising from within the papillomar merely a coexisting disease. In our case, the epitheliumf papilloma showed areas of transition from low-grade toigh-grade dysplasia, thereby validating the origin of carci-oma from within the OSP. The malignancy associated withhis OSP resembles an undifferentiated carcinoma histomor-hologically.
This article emphasizes the association of OSP with malig-ancy and not on discussing the modalities of treatment ofSP. In our case, carcinoma was present in a small propor-ion of each papilloma and could easily have been missedf only a few tissue sections were taken. Moreover, if suchesions (as this case) were to be treated by a conserva-ive approach, that is, polypectomy, foci of malignant cellsill be undoubtedly left behind. Hence, the authors suggest
more radical approach at a time when there is minimalumor burden.
The purpose of this case report in highlighting this sub-ype of sinonasal papilloma in general and OSP, in particularies in its rarity, tendency to be misdiagnosed as ordinaryolyp, well-differentiated adenocarcinoma, or rhinosporid-osis and the necessity of advocating an extensive operativepproach due to its high recurrence rate, local destructive-ess and a relatively high malignant potential.
onflict of Interest
he authors have no conflict of interest to declare.
eferences
1. Hyams VJ. Papillomas of the nasal cavity and paranasal sinuses:a clinicopathological study of 315 cases. Ann Otol Rhinol Laryn-gol. 1971;80:192---206.
2. Yang YJ, Abraham JL. Undifferentiated carcinoma arising inoncocytic Schneiderian (cylindrical cell) papilloma. J Oral Max-illofac Surg. 1997;55:289---94.
3. Barnes L, Bedetti C. Oncocytic Schneiderian papilloma: a reap-praisal of cylindrical cell papilloma of the sinonasal tract. HumPathol. 1984;15:344---51.
4. Cunningham MJ, Brantley S, Barnes L, Schramm Jr VL. Onco-cytic Schneiderian papilloma in a young adult: a rare diagnosis.Otolaryngol Head Neck Surg. 1987;97:47---51.
5. Kaufman MR, Brandwein MS, Lawson W. Sinonasal papillo-mas: clinicopathologic review of 40 patients with inverted
and oncocytic Schneiderian papillomas. Laryngoscope.2002;112:1372---7.
6. Christensen WN, Smith RRL. Schneiderian papillomas: a clinico-pathologic study of 67 cases. Hum Pathol. 1986;17:393---400.
Undifferentiated Carcinoma in Oncocytic Schneiderian Papil
7. Philips PP, Gustafson RO, Facer GW. The clinical behaviourof inverting papilloma of the nose and the paranasal sinuses:report of 112 cases and review of the literature. Laryngoscope.1990;100:463.
8. Pérez-Ordónez B. Hamartomas, papillomas and adenocarcino-mas of the sinonasal tract and nasopharynx. J Clin Pathol.2009;62:1085---95.
9. Ward BE, Fechner RE, Mills SE. Carcinoma arising in onco-cytic Schneiderian papilloma. Am J Surg Pathol. 1990;14:364---9.
10. Kapadia CSB, Barnes L, Pelzman K, Mirani N, Heffner DK, BedettiC. Carcinoma ex oncocytic Schneiderian (cylindrical cell) papil-
loma. Am J Otolaryngol. 1993;14:332---8.
11. Maitra A, Baskin LB, Lee EL. Malignancies arising in oncocyticSchneiderian papillomas: a report of 2 cases and review of theliterature. Arch Pathol Lab Med. 2001;125:1365---7.
1
. A Rarity 309
2. Cheng TY, Ueng SH, Chen YL, Chang KP, Chen TM. OncocyticSchneiderian papilloma found in a recurrent chronic paranasalsinusitis. Chang Gung Med J. 2006;29:336---41.
3. Chrysovergis A, Paschalidis J, Michaels L, Bibas A. Nasopharyn-geal cylindrical cell papilloma. J Laryngol Otol. 2011;125:86---8.
4. Fechner RE. Pathologic quiz case 2. Cylindrical cell papil-loma with invasive, nonkeratinising squamous carcinoma. ArchOtolaryngol. 1981;107:454---5, 457.
5. Shikowitz MJ. Pathologic quiz case 1. Cylindrical cell papillomaof the maxillary sinus. Arch Otolaryngol. 1984;110:486---8.
6. Batsakis JG, Suárez P. Schneiderian papillomas and carcinomas:a review. Adv Anat Pathol. 2001;8:53---64.
7. Pérez Fernández CA, Lacosta Nicolás JL, López Preciado J,Sánchez del Hoyo A. Malignant oncocytic papilloma. An infre-quent type of sinonasal papilloma. An Otorrinolaringol IberoAm. 2004;31:379---86.