Unilateral adrenal hyperplasia: A novel cause of surgically correctable primary hyperaldosteronism Maurizio Iacobone, MD, a Marilisa Citton, MD, a Giovanni Viel, MD, a Riccardo Boetto, MD, a Italo Bonadio, MD, a Saveria Tropea, MD, a Franco Mantero, MD, b Gian Paolo Rossi, MD, c Ambrogio Fassina, MD, d Donato Nitti, MD, a and Gennaro Favia, MD, a Padua, Italy Background. Primary hyperaldosteronism may be caused by an aldosterone-producing adenoma (APA), which is correctable by unilateral adrenalectomy or by idiopathic adrenal hyperplasia, a bilateral disease without any indication for surgery. This study sought to assess the prevalence and the results of surgery in unilateral adrenal hyperplasia (UAH). Methods. The study included 35 patients who underwent unilateral adrenalectomy because of primary hyperaldosteronism after unequivocal successful lateralization by adrenal venous sampling. Demo- graphics, biochemical evaluation, and blood pressure were assessed pre- and postoperatively. Pathology was categorized as APA (isolated adenoma), nodular (multiple micromacronodules), and diffuse UAH (gland thickening without nodules). Results. Pathology revealed 9 APAs and 23 nodular and 3 diffuse UAHs. Patients with APAs and UAHs were statistically similar regarding demographics and preoperative blood pressure levels. Bilateral adrenal involvement was evident at imaging in 10 patients (11% in APA versus 35% in UAH, P = NS). After surgery, biochemical cure of the disease was achieved in all patients; blood pressure levels normalized in 66.6% of patients and ameliorated in 22.2% in APA versus 34.6% and 50% in patients with UAH (P = NS). At a long-term follow-up, only 1 patient with nodular UAH experienced a biochemical recurrence of disease. Conclusion. UAH is not rare, sharing the same features of APA. When disease lateralization is confirmed by adrenal venous sampling, unilateral adrenalectomy achieves excellent long-term results. (Surgery 2012;152:1248-55.) From the Minimally Invasive Endocrine Surgery Unit, a Department of Surgery, Oncology and Gastroenter- ology; the Endocrinology Unit, b the Internal Medicine Unit, c and the Pathology Unit, d Department of Medi- cine, University of Padua, Padua, Italy PRIMARY HYPERALDOSTERONISM has been considered for a long time a very rare disease, but in recent years it has been reported in more than 11% of hy- pertensive patients. 1-4 Primary hyperaldosteronism is typically classi- fied into 2 main subtypes: aldosterone-producing adenoma (APA), usually considered a unilateral benign isolated adrenocortical tumor; and idio- pathic adrenal hyperplasia (IAH), usually consid- ered a bilateral disease, and they were claimed to account for more than 95% of all cases. 5 Patients with APA are considered amenable to operations because unilateral total or even partial adrenalectomy is highly successful in curing pri- mary hyperaldosteronism, with the resolution of hypokalemia in virtually all patients, cure of the hypertension in 30% to 60%, and improvement in the remaining patients. 6 Furthermore, adrenalec- tomy may counteract the deleterious effects of al- dosterone excess on the heart, kidney, and peripheral vascular system. 7 In contrast, patients with IAH are usually managed with medical treat- ment because of bilateral involvement; surgery is not indicated because usually neither the aldoster- one hypersecretion nor the hypertension is cor- rected by unilateral adrenalectomy. 8,9 Therefore, the distinction between unilateral and bilateral aldosterone hypersecretion is crucial, owing to the fact that only patients with unilateral adrenal hypersecretion may be cured by unilateral adrenalectomy. Almost all experts agree that the Accepted for publication August 20, 2012. Reprint requests: Maurizio Iacobone, MD, Minimally Invasive Endocrine Surgery Unit, Department of Surgery, Oncology and Gastroenterology, University of Padua, Via Giustiniani 2, 35128, Padova, Italy. E-mail: [email protected]. 0039-6060/$ - see front matter Ó 2012 Mosby, Inc. All rights reserved. http://dx.doi.org/10.1016/j.surg.2012.08.042 1248 SURGERY
Transcript
Accepte
ReprintEndocriand Ga35128, P
0039-60
� 2012
http://d
1248
Unilateral adrenal hyperplasia: A novelcause of surgically correctable primaryhyperaldosteronismMaurizio Iacobone, MD,a Marilisa Citton, MD,a Giovanni Viel, MD,a Riccardo Boetto, MD,a
Italo Bonadio, MD,a Saveria Tropea, MD,a Franco Mantero, MD,b Gian Paolo Rossi, MD,c
Background. Primary hyperaldosteronism may be caused by an aldosterone-producing adenoma (APA),which is correctable by unilateral adrenalectomy or by idiopathic adrenal hyperplasia, a bilateral diseasewithout any indication for surgery. This study sought to assess the prevalence and the results of surgeryin unilateral adrenal hyperplasia (UAH).Methods. The study included 35 patients who underwent unilateral adrenalectomy because of primaryhyperaldosteronism after unequivocal successful lateralization by adrenal venous sampling. Demo-graphics, biochemical evaluation, and blood pressure were assessed pre- and postoperatively. Pathologywas categorized as APA (isolated adenoma), nodular (multiple micromacronodules), and diffuse UAH(gland thickening without nodules).Results. Pathology revealed 9 APAs and 23 nodular and 3 diffuse UAHs. Patients with APAs andUAHs were statistically similar regarding demographics and preoperative blood pressure levels. Bilateraladrenal involvement was evident at imaging in 10 patients (11% in APA versus 35% in UAH, P= NS). After surgery, biochemical cure of the disease was achieved in all patients; blood pressure levelsnormalized in 66.6% of patients and ameliorated in 22.2% in APA versus 34.6% and 50% inpatients with UAH (P = NS). At a long-term follow-up, only 1 patient with nodular UAH experienced abiochemical recurrence of disease.Conclusion. UAH is not rare, sharing the same features of APA. When disease lateralization isconfirmed by adrenal venous sampling, unilateral adrenalectomy achieves excellent long-term results.(Surgery 2012;152:1248-55.)
From the Minimally Invasive Endocrine Surgery Unit,a Department of Surgery, Oncology and Gastroenter-ology; the Endocrinology Unit,b the Internal Medicine Unit,c and the Pathology Unit,d Department of Medi-cine, University of Padua, Padua, Italy
PRIMARY HYPERALDOSTERONISM has been consideredfor a long time a very rare disease, but in recentyears it has been reported in more than 11% of hy-pertensive patients.1-4
Primary hyperaldosteronism is typically classi-fied into 2 main subtypes: aldosterone-producingadenoma (APA), usually considered a unilateralbenign isolated adrenocortical tumor; and idio-pathic adrenal hyperplasia (IAH), usually consid-ered a bilateral disease, and they were claimed toaccount for more than 95% of all cases.5
d for publication August 20, 2012.
requests: Maurizio Iacobone, MD, Minimally Invasivene Surgery Unit, Department of Surgery, Oncologystroenterology, University of Padua, Via Giustiniani 2,adova, Italy. E-mail: [email protected].
60/$ - see front matter
Mosby, Inc. All rights reserved.
x.doi.org/10.1016/j.surg.2012.08.042
SURGERY
Patients with APA are considered amenable tooperations because unilateral total or even partialadrenalectomy is highly successful in curing pri-mary hyperaldosteronism, with the resolution ofhypokalemia in virtually all patients, cure of thehypertension in 30% to 60%, and improvement inthe remaining patients.6 Furthermore, adrenalec-tomy may counteract the deleterious effects of al-dosterone excess on the heart, kidney, andperipheral vascular system.7 In contrast, patientswith IAH are usually managed with medical treat-ment because of bilateral involvement; surgery isnot indicated because usually neither the aldoster-one hypersecretion nor the hypertension is cor-rected by unilateral adrenalectomy.8,9
Therefore, the distinction between unilateraland bilateral aldosterone hypersecretion is crucial,owing to the fact that only patients with unilateraladrenal hypersecretion may be cured by unilateraladrenalectomy. Almost all experts agree that the
referral diagnostic test for lateralization of aldos-terone hypersecretion is adrenal vein sampling(AVS) because the interpretation of other imagingtechniques (computerized tomography, magneticresonance imaging, adrenocortical scintigraphy) isoften equivocal or misleading.8,10
In recent years, several studies have reportednovel variants of surgically treatable primary hy-peraldosteronism; primary diffuse or nodular uni-lateral adrenal hyperplasia (UAH), previouslyconsidered a very rare disease (0.1%),5 is actuallydocumented in 8% to 70% of cases of surgicallytreated primary hyperaldosteronism,9-14 but it re-mains a controversial entity.
The aim of this study was to assess the effectiverate of APA and UAH in a series of patients withlateralized disease, according to AVS, and to com-pare the outcome after unilateral adrenalectomybased on the rate of biochemical cure of primaryhyperaldosteronism, hypokalemia, and arterialhypertension.
MATERIAL AND METHODS
The present study focused on patients whounderwent adrenalectomy after successful un-equivocal lateralization of the hypersecretion byAVS. They were selected from 111 patients surgi-cally treated because of primary hyperaldosteron-ism at the Endocrine Surgery Unit, University ofPadua, Italy, between 1990 and 2010.
Inpatient and outpatient medical records wereretrospectively reviewed, and hormonal and bio-chemical evaluations (including aldosterone/re-nin ratio [ARR] and serum potassium levels),blood pressure (BP) levels, and the number ofantihypertensive drugs were assessed before andafter surgery. Postoperative follow-up was sched-uled at 6 months after surgery and at the lastavailable medical record. Demographics, bodymass index (BMI), imaging results (including sizeand laterality of the adrenal mass, according topreoperative computerized tomography scan ormagnetic resonance imaging) and final pathology(reviewed by an expert pathologist), were alsoassessed.
All included patients underwent total unilateraladrenalectomy by laparotomic or laparoscopic ap-proach, as previously described.15
The criteria used to establish a biochemicaldiagnosis of primary hyperaldosteronism in a pa-tient with hypertension included a plasma aldos-terone concentration greater than 15 ng/dL andan ARR of more than 40 ng/dL:ng/mL/h; thesuspected diagnosis was further confirmed bysaline infusion, the captopril test, or both.1,3
AVS was performed in order to lateralize thealdosterone hypersecretion, as has been previouslydescribed.16 Successful selective catheterizationwas confirmed when the ratio between cortisolconcentration in each adrenal vein and the infe-rior vena cava was greater than 1:1. Unilateral al-dosterone hypersecretion was confirmed whenthe ratio of adrenal vein aldosterone concentra-tion to the homolateral cortisol concentration onthe side with the higher ratio over the contralateralaldosterone to cortisol ratio (AVS ratio) wasgreater than 2.16
Subjects with systolic BP of 140 mm Hg orgreater, diastolic BP of 90 mm Hg or greater, orboth, and/or on antihypertensive treatment weredefined as hypertensive. The improvement ofarterial BP was defined if the hypertensive patientspassed from one hypertension grade to anotheror if the antihypertensive drugs could be reducedto maintain the therapeutic target; cure wasdefined if BP regained normal levels after dis-continuing any medical treatment. Patients weredefined as being hypokalemic if serum potassiumlevels were below 3.4 mmol/L or in case of needof potassium supplementation; hypokalemia wasconsidered cured if serum potassium levels re-gained the normal range without potassiumsupplementation.
The BMI was calculated as body weight (kg)/height (m2) (normal values from 20 to 24.9).
Biochemical cure of primary hyperaldosteron-ism was defined by the normalization of serumpotassium levels and ARR (<40 ng/dL:ng/mL/h),measured after washout of all interfering drugs.3
Patients who had concomitant glucocorticoid orcatecholamine hypersecretion; incomplete hormo-nal evaluation or follow-up of less than 1 year;undergoing unilateral partial adrenalectomy; orequivocal AVS interpretations because of inade-quate selective catheterization or lateralization orwithout preoperative AVS were not included in thestudy.
Statistical evaluation included the v2 for trendor the Fisher’s exact test for categorical variables,the Student’s t test and the Wilcoxon matched-paired test for continuous variables, and the Spear-man correlation test, as appropriate. P < .05 wasconsidered statistically significant.
RESULTS
The results are summarized in Tables I and II.The study included 35 patients (15 women and20 men; median age 47 years; range, 34 to 72);arterial hypertension was present in all cases; hypo-kalemia was present in 33 patients (94.3%).
Table I. Preoperative demographics, laboratory, hormonal and clinical features according to pathology in35 patients undergoing unilateral adrenalectomy for primary hyperaldosteronism after successfullateralization by adrenal venous sampling
*According to preoperative imaging techniques.Data are expressed as absolute numbers, mean ± SD or percentage in parentheses.APA, Aldosterone-producing adenoma; ARR, aldosterone/renin ratio; AVS, adrenal venous sampling; BP, blood pressure; UAH, unilateral adrenalhyperplasia.
Table II. Postoperative (6 months of follow-up) laboratory, hormonal, and clinical features according topathology in 35 patients undergoing unilateral adrenalectomy for primary hyperaldosteronism aftersuccessful lateralization by adrenal venous sampling
Data are expressed as absolute numbers, mean ± SD or percentage in parentheses.APA, Aldosterone-producing adenoma; ARR, aldosterone/renin ratio; BP, blood pressure; UAH, unilateral adrenal hyperplasia.
SurgeryDecember 2012
1250 Iacobone et al
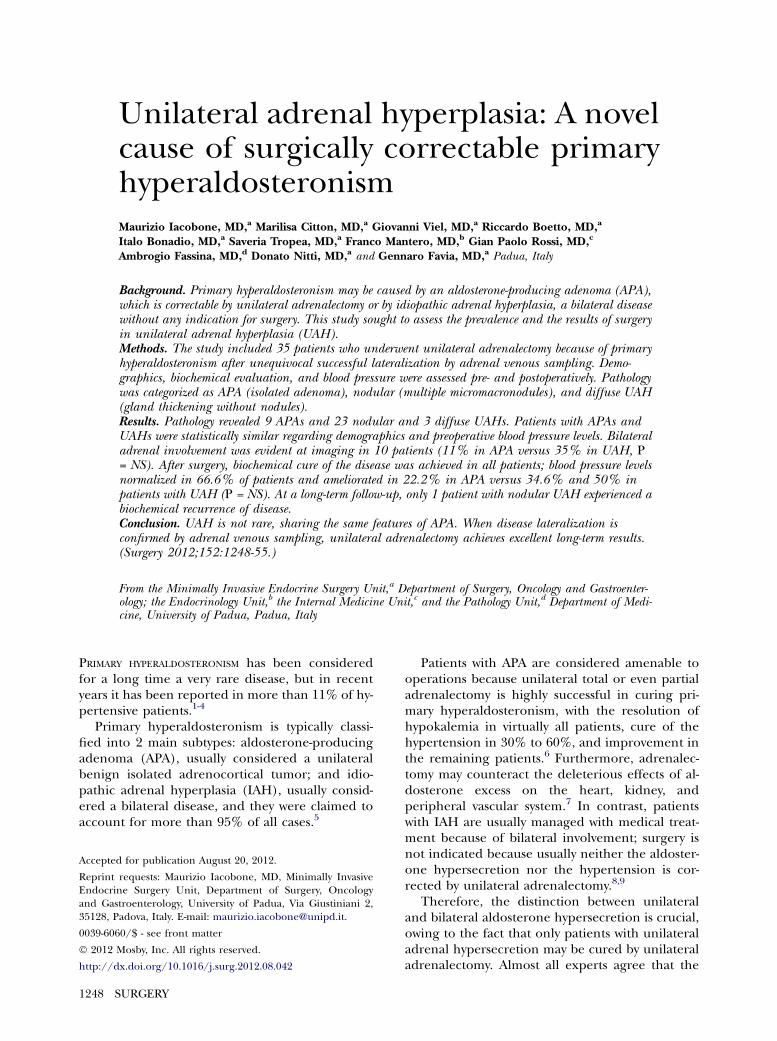
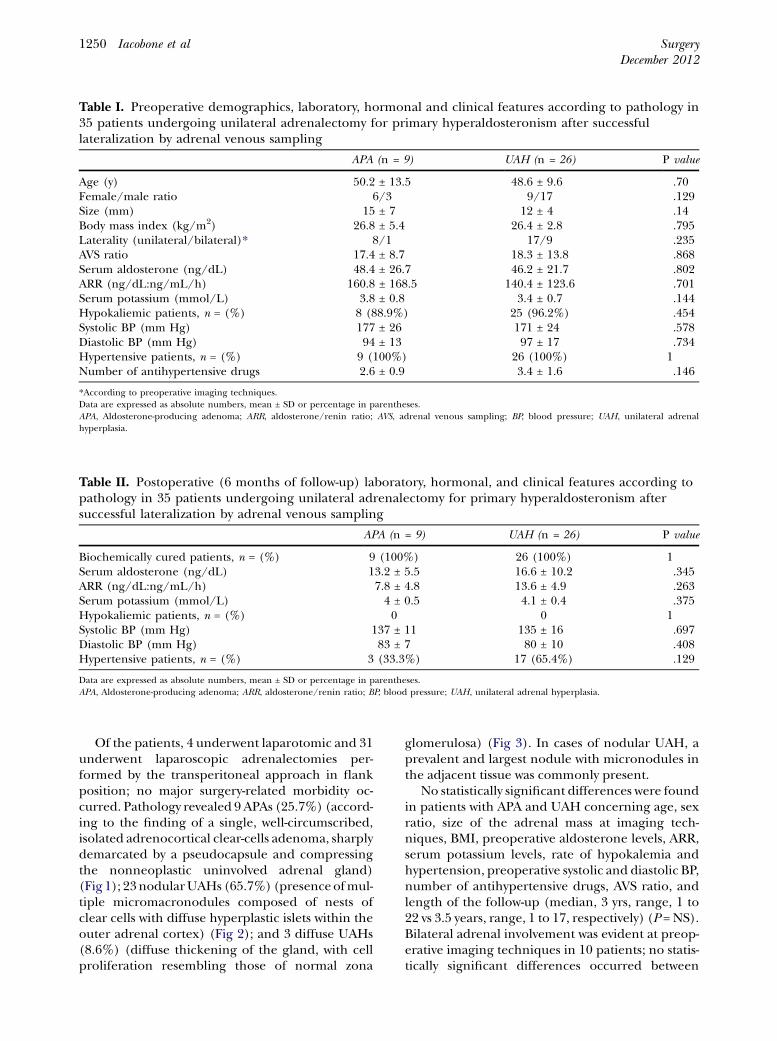
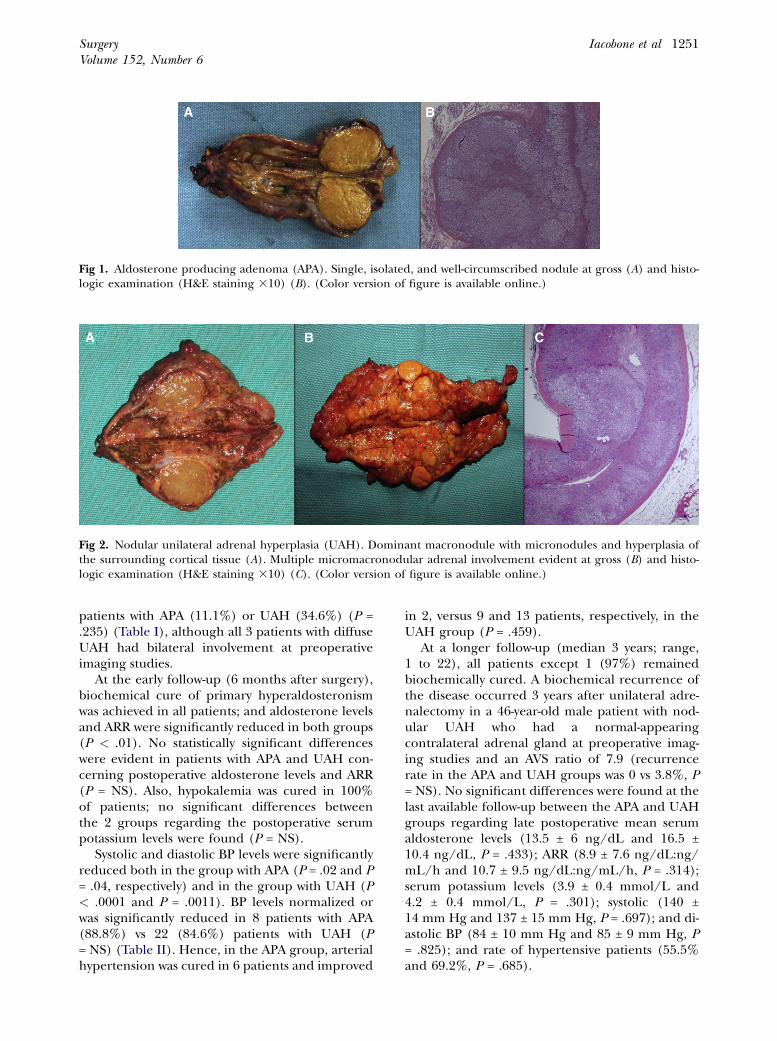
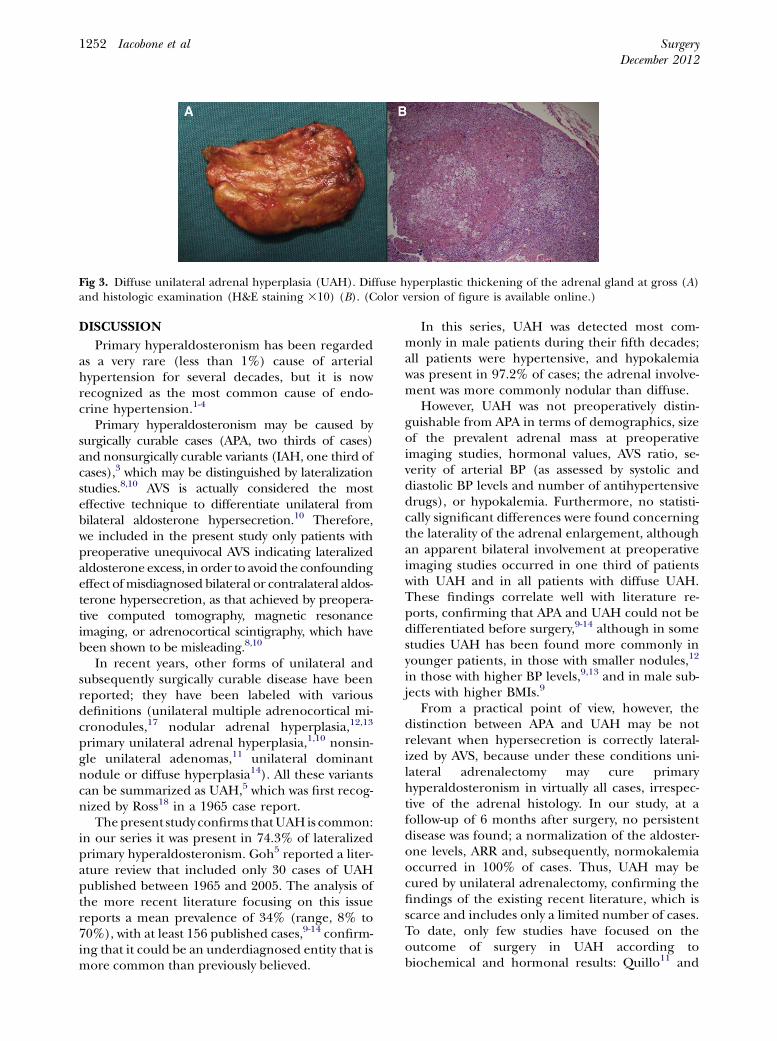
Of the patients, 4 underwent laparotomic and 31underwent laparoscopic adrenalectomies per-formed by the transperitoneal approach in flankposition; no major surgery-related morbidity oc-curred. Pathology revealed 9 APAs (25.7%) (accord-ing to the finding of a single, well-circumscribed,isolated adrenocortical clear-cells adenoma, sharplydemarcated by a pseudocapsule and compressingthe nonneoplastic uninvolved adrenal gland)(Fig 1); 23nodularUAHs (65.7%) (presenceofmul-tiple micromacronodules composed of nests ofclear cells with diffuse hyperplastic islets within theouter adrenal cortex) (Fig 2); and 3 diffuse UAHs(8.6%) (diffuse thickening of the gland, with cellproliferation resembling those of normal zona
glomerulosa) (Fig 3). In cases of nodular UAH, aprevalent and largest nodule with micronodules inthe adjacent tissue was commonly present.
No statistically significant differences were foundin patients with APA and UAH concerning age, sexratio, size of the adrenal mass at imaging tech-niques, BMI, preoperative aldosterone levels, ARR,serum potassium levels, rate of hypokalemia andhypertension, preoperative systolic and diastolic BP,number of antihypertensive drugs, AVS ratio, andlength of the follow-up (median, 3 yrs, range, 1 to22 vs 3.5 years, range, 1 to 17, respectively) (P = NS).Bilateral adrenal involvement was evident at preop-erative imaging techniques in 10 patients; no statis-tically significant differences occurred between
Fig 1. Aldosterone producing adenoma (APA). Single, isolated, and well-circumscribed nodule at gross (A) and histo-logic examination (H&E staining 310) (B). (Color version of figure is available online.)
Fig 2. Nodular unilateral adrenal hyperplasia (UAH). Dominant macronodule with micronodules and hyperplasia ofthe surrounding cortical tissue (A). Multiple micromacronodular adrenal involvement evident at gross (B) and histo-logic examination (H&E staining 310) (C). (Color version of figure is available online.)
SurgeryVolume 152, Number 6
Iacobone et al 1251
patients with APA (11.1%) or UAH (34.6%) (P =.235) (Table I), although all 3 patients with diffuseUAH had bilateral involvement at preoperativeimaging studies.
At the early follow-up (6 months after surgery),biochemical cure of primary hyperaldosteronismwas achieved in all patients; and aldosterone levelsand ARR were significantly reduced in both groups(P < .01). No statistically significant differenceswere evident in patients with APA and UAH con-cerning postoperative aldosterone levels and ARR(P = NS). Also, hypokalemia was cured in 100%of patients; no significant differences betweenthe 2 groups regarding the postoperative serumpotassium levels were found (P = NS).
Systolic and diastolic BP levels were significantlyreduced both in the group with APA (P = .02 and P= .04, respectively) and in the group with UAH (P< .0001 and P = .0011). BP levels normalized orwas significantly reduced in 8 patients with APA(88.8%) vs 22 (84.6%) patients with UAH (P= NS) (Table II). Hence, in the APA group, arterialhypertension was cured in 6 patients and improved
in 2, versus 9 and 13 patients, respectively, in theUAH group (P = .459).
At a longer follow-up (median 3 years; range,1 to 22), all patients except 1 (97%) remainedbiochemically cured. A biochemical recurrence ofthe disease occurred 3 years after unilateral adre-nalectomy in a 46-year-old male patient with nod-ular UAH who had a normal-appearingcontralateral adrenal gland at preoperative imag-ing studies and an AVS ratio of 7.9 (recurrencerate in the APA and UAH groups was 0 vs 3.8%, P= NS). No significant differences were found at thelast available follow-up between the APA and UAHgroups regarding late postoperative mean serumaldosterone levels (13.5 ± 6 ng/dL and 16.5 ±10.4 ng/dL, P = .433); ARR (8.9 ± 7.6 ng/dL:ng/mL/h and 10.7 ± 9.5 ng/dL:ng/mL/h, P = .314);serum potassium levels (3.9 ± 0.4 mmol/L and4.2 ± 0.4 mmol/L, P = .301); systolic (140 ±14 mm Hg and 137 ± 15 mm Hg, P = .697); and di-astolic BP (84 ± 10 mm Hg and 85 ± 9 mm Hg, P= .825); and rate of hypertensive patients (55.5%and 69.2%, P = .685).
Fig 3. Diffuse unilateral adrenal hyperplasia (UAH). Diffuse hyperplastic thickening of the adrenal gland at gross (A)and histologic examination (H&E staining 310) (B). (Color version of figure is available online.)
SurgeryDecember 2012
1252 Iacobone et al
DISCUSSION
Primary hyperaldosteronism has been regardedas a very rare (less than 1%) cause of arterialhypertension for several decades, but it is nowrecognized as the most common cause of endo-crine hypertension.1-4
Primary hyperaldosteronism may be caused bysurgically curable cases (APA, two thirds of cases)and nonsurgically curable variants (IAH, one third ofcases),3 which may be distinguished by lateralizationstudies.8,10 AVS is actually considered the mosteffective technique to differentiate unilateral frombilateral aldosterone hypersecretion.10 Therefore,we included in the present study only patients withpreoperative unequivocal AVS indicating lateralizedaldosterone excess, in order to avoid the confoundingeffect ofmisdiagnosed bilateral or contralateral aldos-terone hypersecretion, as that achieved by preopera-tive computed tomography, magnetic resonanceimaging, or adrenocortical scintigraphy, which havebeen shown to be misleading.8,10
In recent years, other forms of unilateral andsubsequently surgically curable disease have beenreported; they have been labeled with variousdefinitions (unilateral multiple adrenocortical mi-cronodules,17 nodular adrenal hyperplasia,12,13
primary unilateral adrenal hyperplasia,1,10 nonsin-gle unilateral adenomas,11 unilateral dominantnodule or diffuse hyperplasia14). All these variantscan be summarized as UAH,5 which was first recog-nized by Ross18 in a 1965 case report.
Thepresent study confirms thatUAHis common:in our series it was present in 74.3% of lateralizedprimary hyperaldosteronism. Goh5 reported a liter-ature review that included only 30 cases of UAHpublished between 1965 and 2005. The analysis ofthe more recent literature focusing on this issuereports a mean prevalence of 34% (range, 8% to70%), with at least 156 published cases,9-14 confirm-ing that it could be an underdiagnosed entity that ismore common than previously believed.
In this series, UAH was detected most com-monly in male patients during their fifth decades;all patients were hypertensive, and hypokalemiawas present in 97.2% of cases; the adrenal involve-ment was more commonly nodular than diffuse.
However, UAH was not preoperatively distin-guishable from APA in terms of demographics, sizeof the prevalent adrenal mass at preoperativeimaging studies, hormonal values, AVS ratio, se-verity of arterial BP (as assessed by systolic anddiastolic BP levels and number of antihypertensivedrugs), or hypokalemia. Furthermore, no statisti-cally significant differences were found concerningthe laterality of the adrenal enlargement, althoughan apparent bilateral involvement at preoperativeimaging studies occurred in one third of patientswith UAH and in all patients with diffuse UAH.These findings correlate well with literature re-ports, confirming that APA and UAH could not bedifferentiated before surgery,9-14 although in somestudies UAH has been found more commonly inyounger patients, in those with smaller nodules,12
in those with higher BP levels,9,13 and in male sub-jects with higher BMIs.9
From a practical point of view, however, thedistinction between APA and UAH may be notrelevant when hypersecretion is correctly lateral-ized by AVS, because under these conditions uni-lateral adrenalectomy may cure primaryhyperaldosteronism in virtually all cases, irrespec-tive of the adrenal histology. In our study, at afollow-up of 6 months after surgery, no persistentdisease was found; a normalization of the aldoster-one levels, ARR and, subsequently, normokalemiaoccurred in 100% of cases. Thus, UAH may becured by unilateral adrenalectomy, confirming thefindings of the existing recent literature, which isscarce and includes only a limited number of cases.To date, only few studies have focused on theoutcome of surgery in UAH according tobiochemical and hormonal results: Quillo11 and
SurgeryVolume 152, Number 6
Iacobone et al 1253
Hennings14 found a biochemical cure of primaryhyperaldosteronism in 100% of cases in a seriesof 35 and 21 UAH patients, respectively.
In our series, the outcomes of BP levels werealso similar: BP levels normalized or significantlyreduced in 88.8% of APA patients and in 84.6% ofUAH patients, concordantly with other authorswho evaluated only postoperative BP and con-firmed a normalization or amelioration in 80%of cases at a mean follow-up of 2 years.13 Althoughimportant, resolution of hypertension is by itselfinsufficient to assess cure of primary hyperaldoste-ronism, given the multitude of other factors thatmay contribute to persistently elevated BP.6 There-fore, BP alone can be used only as a surrogate andnot as the gold standard for determining cure. Fur-thermore, hypertension represents only one of thedeleterious effects of aldosterone excess7; for thisreason we defined the unequivocal cure of primaryhyperaldosteronism as biochemical normalizationof ARR and serum potassium levels, and not onlyaccording to BP outcomes. Thus, we did not in-clude in the analysis patients without completepostoperative hormonal evaluation or inadequatefollow-up.
In our series, no differences were found be-tween APA and UAH outcomes according to therate of cure aldosterone, ARR, and serum potas-sium levels at an overall median follow-up of 3years (range, 1 to 22 years). Only 1 patient suffer-ing from nodular UAH with unequivocal laterali-zation at AVS and a normal-appearingcontralateral adrenal gland at preoperative imag-ing studies experienced a biochemical recurrenceof primary hyperaldosteronism 3 years after sur-gery. This finding could further confirm that UAHmight represent a unilateral disease with lowrecurrence rates after unilateral surgery. However,a prolonged follow-up is required to verify whetherthese patients relapse, because cases of initial cureafter unilateral adrenalectomy have been reportedalso in bilateral IAH; in fact, metachronous hyper-plasia may develop at the contralateral adrenalglands at varying times.5 Consequently, the medianfollow-up of 3.5 years in the patients with UAH inthe present series might not be adequate to con-sider them definitively cured, although no recur-rent disease was found in a UAH patient up to17 years after surgery.
Walz12 reported a relapse in the contralateraladrenal glands of UAH patients 5 and 14 years af-ter initial surgery, but it was unclear whether pre-operative lateralization was performed by AVS.Hennings14 reported 2 recurrences in nodularUAH; it is interesting that in 1 of these patients,
relapse was caused by recurrent ipsilateral nodulardisease in the remnant after subtotal adrenalec-tomy. The same outcomes have been reported byIshidoya,19 who noted persistent primary hyperal-dosteronism because of ipsilateral involvement af-ter partial adrenalectomy in 7% of cases.
For these reasons, some concerns about the roleof less than total unilateral adrenalectomy shouldbe raised. Partial adrenalectomy is sometimesperformed in patients with evidence of singleAPA at preoperative imaging studies.12 However,as demonstrated in this series, UAH may be morecommon than expected, and APA cannot be pre-dicted accurately before surgery. Subsequently,partial adrenalectomy in cases of unsuspectedUAH may theoretically achieve an incomplete re-moval of abnormal adrenal tissue. Recently it hasbeen confirmed that aldosterone hypersecretionis not localized exclusively in the adenoma cellsbut also in the adjacent hyperplastic or micronod-ular tissue, or both,20 leading to the recommenda-tion of total unilateral adrenalectomy also inlateralized primary hyperaldosteronism, irrespec-tive of preoperative findings.8,11
In this study, we did not perform any immuno-histochemical or aldosterone extraction examina-tion aimed at localizing the hormonalhypersecretion from individual nodules or sur-rounding hyperplastic cortex in UAH; thus, wecannot confirm multiple sites of excess aldoster-one secretion within these adrenal glands. Fur-thermore, because of the high degree of homologybetween the 11-beta-hydroxylase and thealdosterone-synthase in humans, the developmentof specific antibodies for the latter has beenchallenging. Therefore, to date, the only toolavailable for proving aldosterone production couldbe the in situ hybridization, which, however, is nota technique for routine clinical use.21 Therefore,the distinction between APA and UAH has beenhampered by the lack of established criteria and di-agnostic tools. Finally, another possible limitationof this study is the relatively small number of in-cluded patients, which suggests that further studiesincluding a larger number of cases with confirma-tion of the site of aldosterone hypersecretionmight be needed to confirm the results of the pre-sent series.
In conclusion, UAH might be more commonthan anticipated, representing the 74.3% of cases inlateralized primary hyperaldosteronism in our se-ries. It is preoperatively indistinguishable from APAbecause it could share the same features, although itmay present as a bilateral disease at preoperativeimaging techniques in one third of cases. However,
SurgeryDecember 2012
1254 Iacobone et al
when AVS is successful in lateralizing the disease,unilateral adrenalectomy may achieve excellentresults in term of biochemical cure and BP control,regardless of the results of pathology. Recurrencesof the disease are rare, although a prolonged follow-up is required. Some concerns exist in cases ofpartial unilateral adrenalectomy because theoreti-cally it may lead to a persistent or recurrent primaryhyperaldosteronism.
The authors thank Dr Marco Scarpa for assistance instatistical analysis and Dr Sasa Sekulovic for help in dataextraction.
REFERENCES
1. Rossi GP. Prevalence and diagnosis of primary aldosteron-ism. Curr Hypertens Rep 2010;12:342-8.
2. Kempers MJ, Lenders JW, van Outheusden L, van der WiltGJ, Schultze Kool LJ, Hermus AR, et al. Systematic review:diagnostic procedures to differentiate unilateral from bilat-eral adrenal abnormality in primary aldosteronism. AnnIntern Med 2009;151:329-37.
3. Rossi GP, Bernini G, Caliumi C, Desideri G, Fabris B, FerriC, et al. A prospective study of the prevalence of primaryaldosteronism in 1,125 hypertensive patients. J Am Coll Car-diol 2006;48:2293-300.
4. Mulatero P, Stowasser M, Loh KC, Fardella CE, Gordon RD,Mosso L, et al. Increased diagnosis of primary aldosteron-ism, including surgically correctable forms, in centersfrom five continents. J Clin Endocrinol Metab 2004;89:1045-50.
5. Goh BK, Tan YH, Chang KT, Eng PH, Yip SK, Cheng CW.Primary hyperaldosteronism secondary to unilateral adre-nal hyperplasia: an unusual cause of surgically correctablehypertension: a review of 30 cases. World J Surg 2007;31:72-9.
6. Lumachi F, Ermani M, Basso SM, Armanini D, Iacobone M,Favia G. Long-term results of adrenalectomy in patientswith aldosterone-producing adenomas: multivariate analysisof factors affecting unresolved hypertension and review ofthe literature. Am Surg 2005;71:864-9.
7. Rossi GP, Bolognesi M, Rizzoni D, Seccia TM, Piva A, PorteriE, et al. Vascular remodelling and duration of hypertensionpredict outcome of adrenalectomy in primary aldosteron-ism patients. Hypertension 2008;51:1366-71.
8. Funder JW, Carey RM, Fardella C, Gomez-Sanchez CE, Man-tero F, Stowasser M, et al. Case detection, diagnosis, andtreatment of patients with primary aldosteronism: an endo-crine society clinical practice guideline. J Clin EndocrinolMetab 2008;93:3266-81.
9. Tresallet C, Salepcioglu H, Godiris-Petis G, Hoang C, GirerdX, Menegaux F. Clinical outcome after laparoscopic adre-nalectomy for primary hyperaldosteronism: the role ofpathology. Surgery 2010;148:129-34.
10. Young WF, Stanson AW, Thompson GB, Grant CS, Far-ley DR, van Heerden JA. Role for adrenal venoussampling in primary aldosteronism. Surgery 2004;136:1227-35.
11. Quillo AR, Grant CS, Thompson GB, Farley DR, RichardsML, Young WF. Primary aldosteronism: results of adrenalec-tomy for nonsingle adenoma. J Am Coll Surg 2010;213:106-12.
12. Walz MK, Gwosdz R, Levin SL, Alesina PF, Suttorp AC, MetzKA, et al. Retroperitoneoscopic adrenalectomy in Conn’ssyndrome caused by adrenal adenomas or nodular hyper-plasia. World J Surg 2008;32:847-53.
13. Novitsky Y, Kercher K, Rosen M, Cobb WS, Jyothinagaram S,Heniford BT. Clinical outcomes of laparoscopic adrenalec-tomy for lateralizing nodular hyperplasia. Surgery 2005;138:1009-17.
14. Hennings J, Andreasson S, Botling J, H€agg A, Sundin A,Hellman P. Long-term effects of surgical correction of adre-nal hyperplasia and adenoma causing primary aldosteron-ism. Langenbecks Arch Surg 2010;395:133-7.
15. Henry JF, Sebag F, Iacobone M, Hubbard J, Maweja S. Les-sons learned from 274 laparoscopic adrenalectomies. AnnChir 2002;127:512-9.
16. Rossi GP, Sacchetto A, Chiesura-Corona M, De Toni R, Gal-lina M, Feltrin GP, et al. Identification of the etiology of pri-mary aldosteronism with adrenal vein sampling in patientswith equivocal computed tomography and magnetic reso-nance findings: results in 104 consecutive cases. J Clin En-docrinol Metab 2001;86:1083-90.
17. Omura M, Sasano H, Fujiwara T, Yamaguchi K, Nishikawa T.Unique cases of unilateral hyperaldosteronemia due to mul-tiple adrenocortical micronodules, which can only be de-tected by selective adrenal venous sampling. Metabolism2002;51:350-5.
18. Ross EJ. Conn’s syndrome due to adrenal hyperplasia withhypertrophy of zona glomerulosa, relieved by unilateral ad-renalectomy. Am J Med 1965;39:994-1002.
19. Ishidoya S, Ito A, Sakai K, Satoh M, Chiba Y, Sato F, et al.Laparoscopic partial versus total adrenalectomy for aldos-terone producing adenoma. J Urol 2005;174:40-3.
20. Shigematsu K, Yamaguchi N, Nakagaki T, Sakai H. A case ofunilateral adrenal hyperplasia being difficult to distinguishfrom aldosterone-producing adenoma. Exp Clin Endocri-nol Diabetes 2009;117:124-8.
21. Lenzini L, Seccia TM, Aldighieri E, Belloni AS, Bernante P,Giuliani L, et al. Heterogeneity of aldosterone-producingadenomas revealed by a whole transcriptome analysis. Hy-pertension 2007;50:1106-13.
DISCUSSION
Dr William Young (Rochester, MN): I have two questions.Your presentation was very clear. Despite that, I didn’tunderstand some of the data.
Finally, 26% of your 35 patients that went to surgeryhad a solitary unilateral aldosterone-producing ade-noma, which I think is rather low. As you probablyknow, Mayo Clinic summarized their experience andpublished it last year. In a group of 167 patients, 79%had a unilateral aldosterone-producing adenoma.
So my first question relates to that difference. How doyou explain the difference? Do you think that there wassome selection bias?
The second question relates to the main differencebetween the 2 studies concerning your multinodulardisease. I think it’s a problem since you didn’t do,apparently, immunohistochemistry for aldosterone syn-thase, knowing whether these multiple nodules areproducing aldosterone or not. It may be the case ofjust 1 secreting nodule, and maybe most of yourpatients could have a solitary aldosterone-producingadenoma.
SurgeryVolume 152, Number 6
Iacobone et al 1255
So the question is: Why do you think there’s adifference? Why do you think that only 26% of yourpatients had APA?
Dr Marilisa Citton (Padua, Italy): Do you mean thedifferences in aldosterone-producing adenomas be-tween our and your patients?
Dr William Young (Rochester, MN): Right. Most serieswould have a much higher percentage of aldosterone-producing adenomas.
Dr Marilisa Citton (Padua, Italy): In our series, we re-viewed the pathology. We selected only patients with un-equivocal lateralization at AVS. So we considered ahighly selected group of patients. We think that a unilat-eral hyperplasia can be confounded with a unilateralaldosterone-producing adenoma, especially with thenodular form, when there is a bigger nodule and othersmaller nodules in the surrounding tissue.
I argue that we have a higher number of unilateraladrenal hyperplasias because of the selection of patientsand the analysis of our pathologists.
Dr William Young (Rochester, MN): So just to clarify,do you think that it is the selection based on adrenal ve-nous sampling that led to this difference?
DrChrisRaeburn (Aurora, CO): I think she’s saying thatit’s a combination of their selection for this group. Thenperhaps they considered patients that had small nodulesaround the main nodule as being hyperplasia, whereasother studieswouldhave classified that as a single adenoma.
Dr Marilisa Citton (Padua, Italy): In the present studyimmunohistochemistry was not used; to date, it is a tech-nique that is still not feasible for the routine clinicalpractice.
Dr Quan Yang Duh (San Francisco, CA): I have somesimilar concerns, as Dr Young has. My question is about
your adrenal vein sampling and your definition of whatis a unilateral secretion. When you do these AVS, thereare 2 types of hypersecretions. Sometimes you will seeone side elevated, the other side decreased, comparedwith the peripheral value. Occasionally, you will see bilat-eral elevated levels compared with peripheral, but oneside significantly more than the other side. And I justwonder what is your definition of positive adrenal veinsampling?
Dr Marilisa Citton (Padua, Italy): We selected the pa-tients with unequivocal lateralization of hypersecretionof aldosterone, and we used a lateralization index higherthan 2. When the lateralization was equivocal, these pa-tients were excluded.
Dr Quan Yang Duh (San Francisco, CA): Maybe I canask the question another way. Concerning the gland thatwas not removed, was the aldosterone-to-cortisol ratio onthis side lower than the inferior vena cava, at AVS?
Dr Marilisa Citton (Padua, Italy): No, in most casesthe hypersecretion was exclusively unilateral.
Dr Chris Raeburn (Aurora, CO): I noticed that yousaid that the difference in the aldosterone-to-renin ratioswere not different between the APA and hyperplasiagroups, but it seemed that there was some trend towardhigher aldosterone levels in that group. With longerfollow-up, is it possible that you really have just takenout 1 gland in bilateral adrenal hyperplasia?
About the postoperative values for aldosterone andrenin in the APA, the ratio was quite low; but in thehyperplasia group, it was a little higher.
Dr Marilisa Citton (Padua, Italy): There were not sta-tistically significant differences between the 2 groupsabout any value. They were indistinguishable beforeand after surgery.