25
UNIPOLAR MAJOR DEPRESSION SIR MICHAEL MARMOT GROUP 1
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | shirish-tiwari |
| View: | 86 times |
| Download: | 2 times |

UNIPOLARMAJORDEPRESSION
SIR MICHAEL MARMOT GROUP
1

GROUP CONTRIBUTIONS
SHIRISH TIWARISlide Preparation and
Presentation
DR NEYANG NITIK
Data Collection from Books
DR MEENAKSHI MALIK
Data collection for Global Burden
DR ISHA SHARMA
Data Collection for NMHP
MRS SHALINI KUMARI
Data Compilation for NMHP
HEEYA MAITYWHO and Data
Compilation
SIR MICHAEL MARMOT GROUP 2
ABRAHAM LINCOLN
SIR MICHAEL MARMOT GROUP 3

WHAT IS UNIPOLAR MAJOR DEPRESSION ?
Unipolar Major Depression is a mentaldisorder characterized by pervasiveand persistent low mood that isaccompanied by low self esteem and bya loss of interest of pleasure inenjoyable activities. (3)
MANIFESTATIONS
Affects daily life for weeks or longer Interferes with social life
- Family and relationships- work and school life- Sleeping and eating habits
Implications on general health
SIR MICHAEL MARMOT GROUP 4

SIR MICHAEL MARMOT GROUP 5
HISTORY
• Hippocrates – described Melancholia with mental and physical symptoms. (3)
• Sigmund Freud – Mourning and Melancholy
CLASSIFICATION
• DSM-I, 1952 AND DSM-II, 1968. (3)
• ICD – 10 By WHO
SIR MICHAEL MARMOT GROUP 6
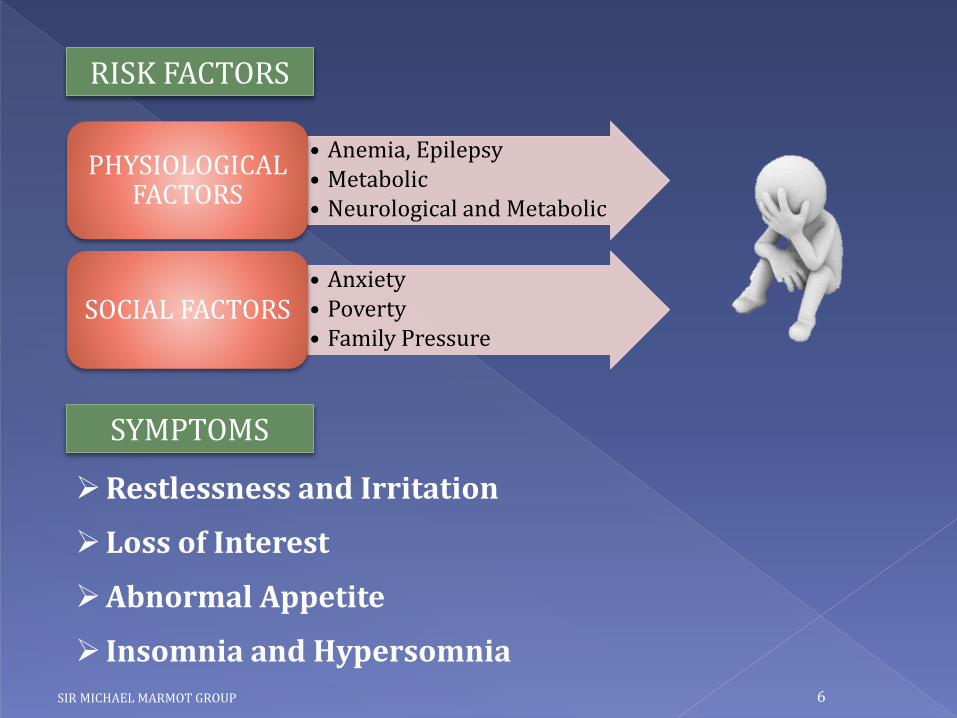
RISK FACTORS
• Anemia, Epilepsy• Metabolic• Neurological and Metabolic
PHYSIOLOGICAL FACTORS
• Anxiety• Poverty• Family Pressure
SOCIAL FACTORS
SYMPTOMS
Restlessness and Irritation
Loss of Interest
Abnormal Appetite
Insomnia and Hypersomnia

EP
IDE
MIO
LO
GY
OF
D
EP
RE
SSIO
N
Approx. 298 MN people affected as of 2010 (4.3%) of global population. (3)
Lifetime Incidence – 3% in Japan to 17% in USA.
Population Studies – UMD twice in women compared to men. (3)
SIR MICHAEL MARMOT GROUP 7
More common in urban than rural population. (3)
8.2% - global YLDs in 2010, making it the 2nd leading cause of global disability.
11th leading cause of global burden (or DALYs) in 2010. (6)
SIR MICHAEL MARMOT GROUP 8
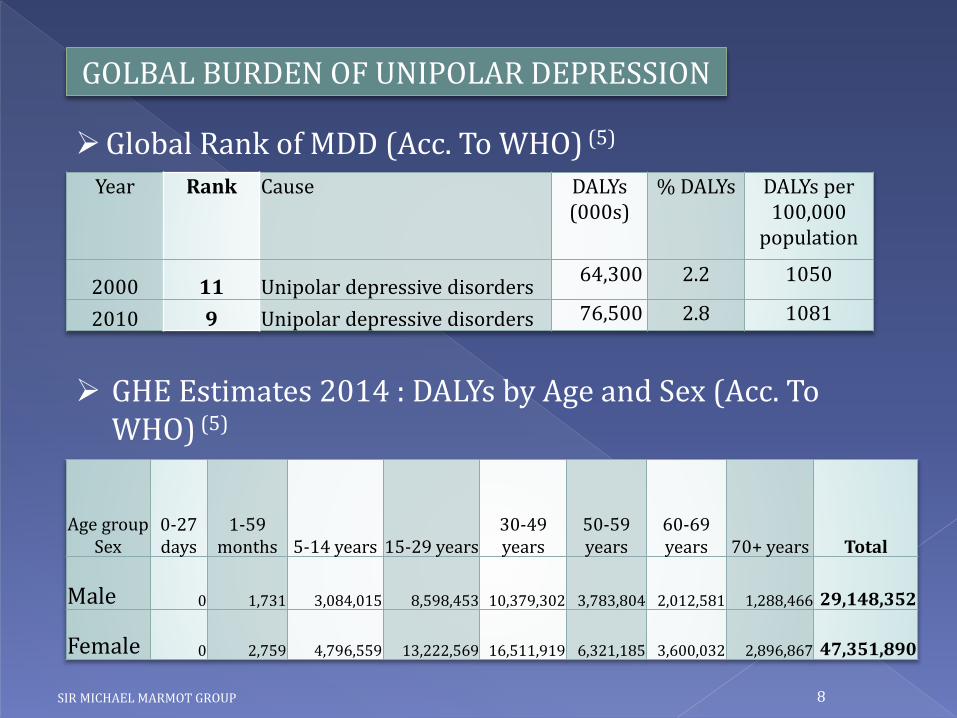
GOLBAL BURDEN OF UNIPOLAR DEPRESSION
Global Rank of MDD (Acc. To WHO) (5)
Year Rank Cause DALYs (000s)
% DALYs DALYs per 100,000
population
2000 11 Unipolar depressive disorders64,300 2.2 1050
2010 9 Unipolar depressive disorders 76,500 2.8 1081
GHE Estimates 2014 : DALYs by Age and Sex (Acc. To WHO) (5)
Age group Sex
0-27 days
1-59 months 5-14 years 15-29 years
30-49 years
50-59 years
60-69 years 70+ years Total
Male 0 1,731 3,084,015 8,598,453 10,379,302 3,783,804 2,012,581 1,288,466 29,148,352
Female 0 2,759 4,796,559 13,222,569 16,511,919 6,321,185 3,600,032 2,896,867 47,351,890

SIR MICHAEL MARMOT GROUP 9
COMPARISON OF DALYs
Globally, Prevalence of MDD more in women than men (2012)
0
5,000,000
10,000,000
15,000,000
20,000,000
25,000,000
30,000,000
35,000,000
40,000,000
45,000,000
50,000,000
0-27 days 1-59months
5-14 years 15-29years
30-49years
50-59years
60-69years
70+ years Total
Male
Female
SIR MICHAEL MARMOT GROUP 10
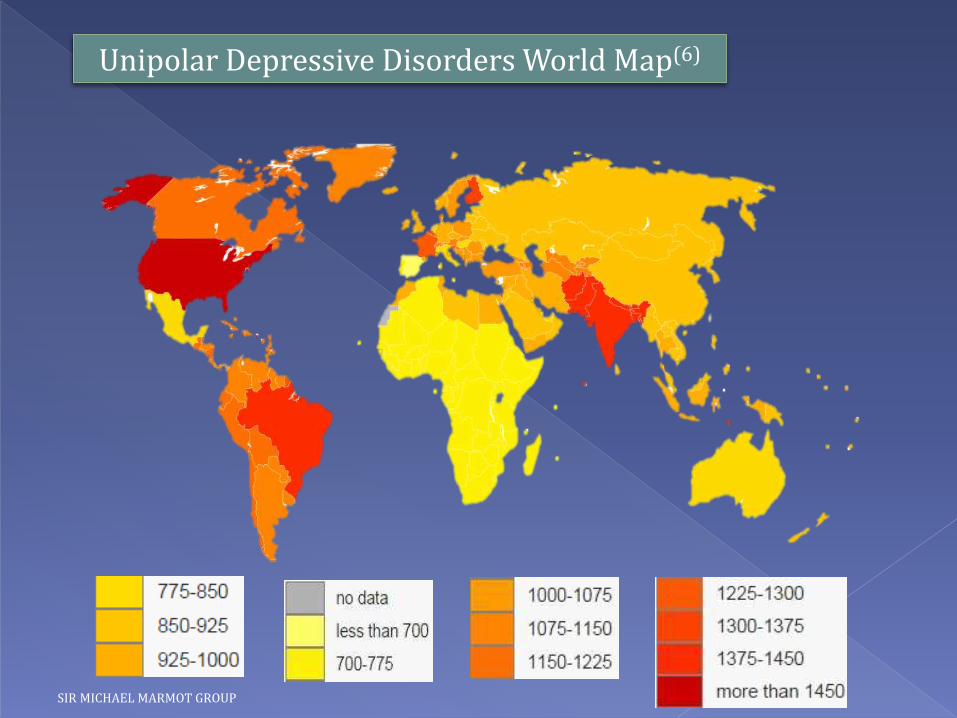
Unipolar Depressive Disorders World Map(6)

SIR MICHAEL MARMOT GROUP 11
GBD OF DEPRESSION IN INDIA
Global Health Estimates – DALYs – By sex and age groups (2012).(5)
0
1000
2000
3000
4000
5000
6000
7000
8000
DALYs 0-4years
DALYs 5-14years
DALYs 15-29years
DALYs 30-59years
DALYs 60-69years
DALYs 70+years
All Ages
MALE 0.3 587.6 1543.5 2282.9 267 134 4815.3
FEMALE 0.4 876.9 2288.9 3474.2 458.1 269.2 7367.7
Po
pu
lati
on
('0
00
)
SIR MICHAEL MARMOT GROUP 12
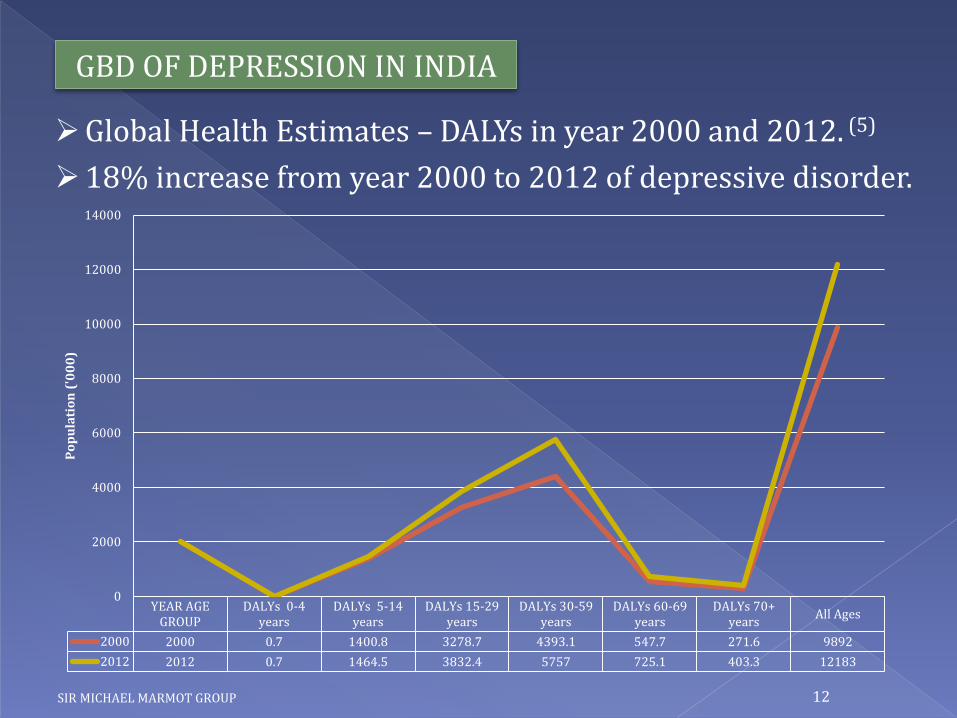
GBD OF DEPRESSION IN INDIA
Global Health Estimates – DALYs in year 2000 and 2012. (5)
18% increase from year 2000 to 2012 of depressive disorder.
YEAR AGEGROUP
DALYs 0-4years
DALYs 5-14years
DALYs 15-29years
DALYs 30-59years
DALYs 60-69years
DALYs 70+years
All Ages
2000 2000 0.7 1400.8 3278.7 4393.1 547.7 271.6 9892
2012 2012 0.7 1464.5 3832.4 5757 725.1 403.3 12183
0
2000
4000
6000
8000
10000
12000
14000
Po
pu
lati
on
('0
00
)

SIR MICHAEL MARMOT GROUP 13
WORLD HEALTH ORGANISATION
mhGAP – Mental Health Gap Action Plan.(8)
-“Scaling up care for mental, neurological and substance disorder”
- It was endorsed by 55th World Health Assembly in 2002.
- Mental Health : Evidence and Research Team (MER)
- Mental Health Atlas
- WHO-AIMS (Assessment Instrument for Mental Health Systems)
- WHO-MIND (Mental Health in Development)
SIR MICHAEL MARMOT GROUP 14
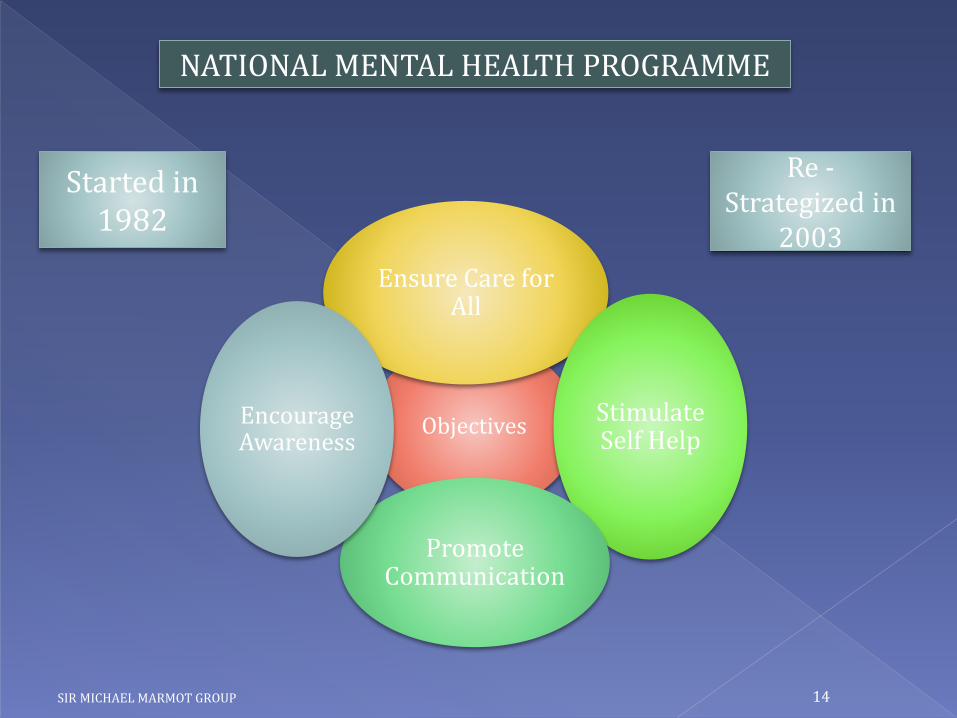
Objectives
Ensure Care for All
Stimulate Self Help
Promote Communication
Encourage Awareness
NATIONAL MENTAL HEALTH PROGRAMME
Started in 1982
Re -Strategized in
2003

SIR MICHAEL MARMOT GROUP 15
NATIONAL MENTAL HEALTH PROGRAMME
HOSPITAL BASED APPROACH
COMMUNITY BASED
APPROACH
10th 5 Year plan(2002-07)
DMHP-Country wise
Strengthening Central & State Mental Health Authorities
Increased Psychiatry content in Medical curriculum
Research & Training
11th 5 Year plan(2007-12)
DMHP with added components
Modernization of state run hospitals
Up gradation of psychiatric wing
IEC Man power
development
12th 5 Year plan(2012-17)
Integration of different components of NMHP to that of NRHM

SIR MICHAEL MARMOT GROUP 16
• 0.05% of total Health Budget – For Mental Health
• The 11th FYP of 2005 had an allocation of Rs.1000 crore for the NMHP
• Sum of 70 crore has been made available for 2008-09 for the further implementation of NMHP but this only constitutes 2.5% of the total health budget.
BUDGET ALLOCATION

SIR MICHAEL MARMOT GROUP 17
S. No. Resources Present Status (2011) Required Status
1 Psychiatrist 3000 11,500
2 Clinical Psychologist 500 17,250
3 Psychiatrist Social Workers
400 23,000
4 Psychiatrist Nurses 900 9,000
5 Number of Beds 300 30,000
• 7% of population suffers from mental disorders
• Point Prevalence - 10 to 20 per 1000 of the population
• <1 Psychiatrist for every FOUR lakh population.
MANPOWER RESOURCE IN INDIA

SIR MICHAEL MARMOT GROUP 18
SHORTCOMINGS OF NMHP
• Lack of manpower resources
• Lack of proper and effective monitoring and guidelines.
• Inadequate data about Health Status
• Poor feasibility of policies and implementation.
• No indicators to assess mental health
SIR MICHAEL MARMOT GROUP 19
RECOMMENDATIONS FOR NMHP
• Strengthening manpower
• Proactive role of State Government in the implementation of programmes.
• Preventive measures should be taken
• Manpower should be trained with Public Mental Health.
• Integrated with NRHM
• NGO works should be encouraged.
• Social Initiatives should be given preference

SIR MICHAEL MARMOT GROUP 20
Psychotherapy – Effective at preventing new onset of depression.
- Interpersonal Therapy
- Cognitive Behavioral Therapy
- Significant in severe cases of disorders.
- Mostly given with psychotherapy.
- E.g.:- SSRIs, Bupropion, Venlafaxine, etc.
- Significant decline in suicide rates.(3)
TREATMENT

SIR MICHAEL MARMOT GROUP 21
S. No. Low Resourced Setting High Resourced Setting
1 Routine screening for detection High-risk or routine screening with confirmation of diagnosis by skilled clinician
2 Psycho-education Psycho-education
3 Generic antidepressants Choice of antidepressants
4 Problem-solving treatment Choice of brief psychological treatments
CONCLUSION
• Mass awareness through education and promotion.
• Removal of Social taboos and stigmas (FAITH-HEALERS)
• People with illness should be joined to mainstream.
PACKAGE CARE FOR DEPRESSION.
SIR MICHAEL MARMOT GROUP 22
Sir Isaac Newton John Stuart Mill Abraham Lincoln
Robin Williams Mike Tyson

SIR MICHAEL MARMOT GROUP 23
IMPORTANT FACTS
World Mental Health Day – 10th October
Theme for 2014 – “Living with Schizophrenia”
SIR MICHAEL MARMOT GROUP 24
REFERENCES
1) The Hindu Newspaper - http://tinyurl.com/pzby9ow
2) National Crime Records Bureau – Suicides in India, 2013
3) Wikipedia - http://tinyurl.com/lealaug
4) http://obad.ca/information_depression#criteria
5) WHO Data on Global Health Estimates.
6) GBD Data on Depressive Disorder
7) Medscape - http://www.medscape.com/viewarticle/813896
8) WHO - http://www.who.int/mental_health/mhgap/en/
9) WHO - http://www.who.int/mental_health/maternal-child/en/
10)MOHFW - http://tinyurl.com/qgvu6ev
SIR MICHAEL MARMOT GROUP 25
“Depression begins with disappointment. When disappointment festers in our soul, it leads to discouragement.”- Joyce Meyer

![SOCIO-DEMOGRAPHIC CORRELATES OF UNIPOLAR MAJOR DEPRESSION … · depression is segregated based on ethnicity, and the prevalence for Malay elderly is 6.5% [5].Additionally, a south](https://static.documents.pub/doc/80x56/5f0d7b1a7e708231d43a91d6/socio-demographic-correlates-of-unipolar-major-depression-depression-is-segregated.jpg)















