Page 1
UNIVERSITY OF GONDAR
COLLEGE OF NATURAL AND COMPUTATIONAL SCIENCES
DEPARTMENT OF SPORT SCIENCE
PREVALENCE OF SPORT INJURY AND ITS ASSOCIATED RISK FACTORS
IN THE CASE OF WOLITA DICHA AND MEDAWOLABO UNIVERSITY
MALE VOLLEYBALL PREMIER LEAGUE CLUBS
BY
TATEK GIRMA
ADVISOR: Dr. ALEMAYEHU BELAY (ASSO. PROF.)
JUNE, 2012E.C
GONDAR, ETHIOPIA
Page 2
PREVALENCE OF SPORT INJURY AND ITS ASSOCIATED RISK FACTORS
IN THE CASE OF WOLITA DICHA AND MEDAWOLABO UNIVERSITY
MALE VOLLEYBALL PREMIER LEAGUE CLUBS
UNIVERSITY OF GONDAR
COLLEGE OF NATURAL AND COMPUTATIONAL SCIENCES
DEPARTMENT OF SPORT SCIENCE
BY
TATEK GIRMA
ADVISOR: Dr. ALEMAYEHU BELAY (ASSO. PROF.)
A THESIS SUBMITTED TO SPORT SCIENCE DEPARTMENT, UNIVERSITY OF
GONDAR, TO FULFILL THE PARTIAL REQUIREMENTS FOR THE AWARD OF
THE DEGREE OF MASTERS OF SCIENCE IN SPORT SCIENCE (VOLLEYBALL
COACHING SPECIALIZATION)
JUNE, 2012E.C
GONDAR, ETHIOPIA
Page 3
APPROVAL SHEET
UNIVERSITY OF GONDAR
POST GRADUATE STUDIES
As member of the examining board of final Msc, open defense we certify that we have read and
evaluated this thesis prepared by Tatek Girma. Entitled with “Prevalence of Sport Injury And
Its Associated Risk Factors In The Case of Wolita Dicha And Medawolabo University Male
Volleyball Premier League Clubs” and recommended that it is accepted as fulfilling the thesis
requirement for the Degree of Master of Science in volleyball coaching (coaching volleyball).
.................................... ………………… …………………….
Name of Advisor Signature Date
As member of the examining board of final Msc. open defense, we certify that we have read and
evaluated the thesis prepared by Tatek Girma. We recommend that the thesis be accepted as
fulfilling the requirement for the degree of M.sc. in volleyball coaching.
…………………….. …………………….. …………………….
Name of chairperson Signature Date
…………………….. …………………….. …………………….
Name of internal Examiner Signature Date
…………………….. …………………….. …………………….
Name of External Examiner Signature Date
Page 4
DECLARATION
I, declares that this thesis is the result of my own work and all sources or materials used for this
thesis have been duly acknowledged. This thesis is submitted to department of sport science for
the partial fulfillment Master of Science in volleyball coaching. I confidentiality declare that this
thesis has not been submitted by any other institutions or university in Ethiopia for the award of
any academic degree, diploma, or certificate.
Name: Tatek Girma
Signature: ____________
Place and Date of Submission: University of Gondar, June 2012 E.C.
This thesis has been submitted for examination by my approval as a university Advisor.
Name: ____________________________
Signature: ________________________
Date of Submission: _______________
Page 5
CERTIFICATE
This is to certify that the thesis entitled “Prevalence Of Sport Injury And Its Associated Risk
Factors In The Case Of Wolita Dicha And Medawolabo University Male Volleyball
Premier League Clubs” done by Tatek Girma for the award of Master Degree in sport science
(volleyball coaching) is an original work done by him under my supervision. The matter of
content of this thesis has not been submitted previously for the award of any Diploma,
Degree, of any university.
Alemayehu Belay (Asso pro) __________________ _________________
Name of Advisor Signature Date
Page 6
i
ORGANIZATION OF THE THESIS
This thesis focuses on the prevalence and its associated risk factors of sport injury in the study
area. The thesis paper contains five chapters. Chapter one deals with introduction, statement of
the problem, research questions, objective of the study (general and specific), significance of the
study, delimitation of the study, Limitation of the study and operational definitions of terms was
included. In chapter two, the literature review highlights essential issues that need to receive
focused attention. These include the prevalence of injuries and the body location more exposed
to injury as well as the mechanisms and causes of injuries were included with reference to
different literatures. Chapter three included an attempt to explain the methodological issues of
the study, including study area, study design, study population, sampling size and technique, data
collection tools, data analysis and the procedures of the study. Finally, chapter four and five
deals with data results and discussion, summery, conclusion and recommendations, respectively
was existing.
Page 7
ii
ACKNOWLEDGMENTS
First of all, I would like to thank the almighty God who gives me full kneecap to do all the
things what I want to do.
Then I would like to express my deepest gratitude, heartfelt thanks, and appreciation to my
Advisor Dr. Alemayehu Belay(Associat professor); who the owner of astute minds for he
gives me great technical knowledge, valuable comments, suggestions, motivational word,
consistent follow up throughout that enable to me complete the research work and vision to
conduct my research.
I really have not enough words to express my feeling to my parents for their kindly treatment in
all aspects related to my life and their shared all not only my happiness, but also my troubles,
worries, obstacles, and against; So; their advice, motivation without limits throughout my
educational life and generous financial support was an exception in my education and research;
that is why; I wish them all the best in their life. My elder by technical knowledge, constructive
idea, advice; and my Friend D/ Abebe Bancha.
My genuine appreciation and special thanks go to all Teachers of sport science apartment of
Gondar University, especially to acknowledge Dr. Mesaye, Dr. Ephrem and Dane the
informants for their cooperation and willingness to participate in this thesis.
I am grateful to many people who have assisted me in doing this research. Due to the space
limitation I cannot list all here. However, the following persons deserve special consideration
In line with this I want to acknowledge my Friends, Families and all Participants of the
research Ato/ Chernet, Dr. Abera, Dr. Haileyesus, Admasu, Shumu, Mola; Coaches and
physiotherapists of both volleyball clubs as well as players of those Tow volleyball clubs
participated in the study; for scarifying their valuable time, constant support, positive approach,
and friendly advice throughout my research; without them the study might be so difficult for the
researcher.
Eventually, to the above-mentioned people and to those who have not been mentioned, your
sacrifice and encouragement are greatly appreciated and will always be in my memory. This
thesis would not have been possible without constant support from all of you.
Page 8
iii
Table of Contents
Contents page
ORGANIZATION OF THE THESIS .............................................................................................. i
ACKNOWLEDGMENTS .............................................................................................................. ii
LIST OF TABLE .......................................................................................................................... vii
LIST OF FIGURE........................................................................................................................ viii
LIST OF ABBREVIATIONS ........................................................................................................ ix
ABSTRACT .................................................................................................................................... x
CHAPTER ONE ............................................................................................................................. 1
1. INTRODUCTION ...................................................................................................................... 1
1.1. Background of the study ...................................................................................................... 1
1.2. Statement of the Problem ..................................................................................................... 3
1.3. Research questions ............................................................................................................... 4
1.4 Objectives of the study .......................................................................................................... 4
1.4.1 General objective ............................................................................................................ 4
1.4.2. Specific objectives ......................................................................................................... 5
The following specific objectives were designed to address: .................................................. 5
1.5. Significance of the Study ..................................................................................................... 5
1.6. Delimitation (Scope) of the Study ........................................................................................ 5
1.7. Limitation of the study ......................................................................................................... 6
1.8 .Operational Definitions of terms .......................................................................................... 6
CHAPTER TWO ............................................................................................................................ 7
2. REVIEW OF RELATED LITERATURE .................................................................................. 7
2.1 Sports injury theoretical literature ......................................................................................... 7
2.2 Types of volleyball injuries ................................................................................................... 9
2.3. Injury mechanism in sport .................................................................................................. 11
2.3.1. Player contact .............................................................................................................. 12
2.3.2. Contact ......................................................................................................................... 12
2.3.3. No contact .................................................................................................................... 13
2.4. Mechanisms of volleyball injuries ..................................................................................... 13
2.4.1 .Spiking ......................................................................................................................... 13
Page 9
iv
2.4.2. Serving ......................................................................................................................... 13
2.4.3. Blocking....................................................................................................................... 14
2.4.4. Setting .......................................................................................................................... 14
2.5. Common volleyball injuries ............................................................................................... 14
2.5.1. Ankle Injuries .............................................................................................................. 14
2.5.2. Knee injury .................................................................................................................. 15
2.5.3. Shoulder injuries .......................................................................................................... 15
2.5.4. Ulnar nerve injuries ..................................................................................................... 16
2.5.5. Finger/thumb injuries .................................................................................................. 17
2.5.6. Lower Back Injuries .................................................................................................... 17
2.5.7. Lower extremity .......................................................................................................... 18
2.5.8. Upper extremity ........................................................................................................... 18
2.6. Preventive intervention measures for sports injuries ......................................................... 18
2.7. Severity of sports injuries ................................................................................................... 19
2.8. Recurrent injuries ............................................................................................................... 20
2.9. Causes of volleyball injuries .............................................................................................. 21
2.10. Major Injuries Risk Factors that influencing volleyball sport.......................................... 22
2.10.1. Intrinsic factors .......................................................................................................... 22
2.10. 1.1. Age ................................................................................................................. 22
2.10.1.2. Gender .............................................................................................................. 22
2.10.1.3. Height and weight ............................................................................................ 23
2.10.1.4 Previous injury .................................................................................................. 23
2.10.1.5. Level of fitness ................................................................................................. 24
2.10.1.6. Flexibility ......................................................................................................... 24
2.10.1.7. Physical problems ............................................................................................. 24
2.10.1.8. Warming up ...................................................................................................... 25
2.10.2. Extrinsic factors ................................................................................................... 25
2.10.2.1. Training methods .............................................................................................. 26
2.10.2.2. Level of competition ........................................................................................ 26
2.10.2.3. Playing Surface ................................................................................................. 26
2.10.2.4. Player position .................................................................................................. 27
Page 10
v
2.10.2.4.1. Centre................................................................................................................... 28
2.10.2.4.2. Hitter .................................................................................................................... 28
2.10.2.4.3. outside player ....................................................................................................... 28
2.10.2.4.4 .Setter .................................................................................................................... 28
2.10.2.4.5. Libero................................................................................................................... 29
CHAPTER THEER ...................................................................................................................... 34
3. RESEARCH METHODOLOGY.............................................................................................. 34
3.1. Study Area .......................................................................................................................... 34
3.2. Study Design ...................................................................................................................... 34
3.3. Population of the study ....................................................................................................... 35
3.4 Sample size and sampling techniques ................................................................................. 35
3.5. Sources of data ................................................................................................................... 35
3.5.1. Primary data source; .................................................................................................... 35
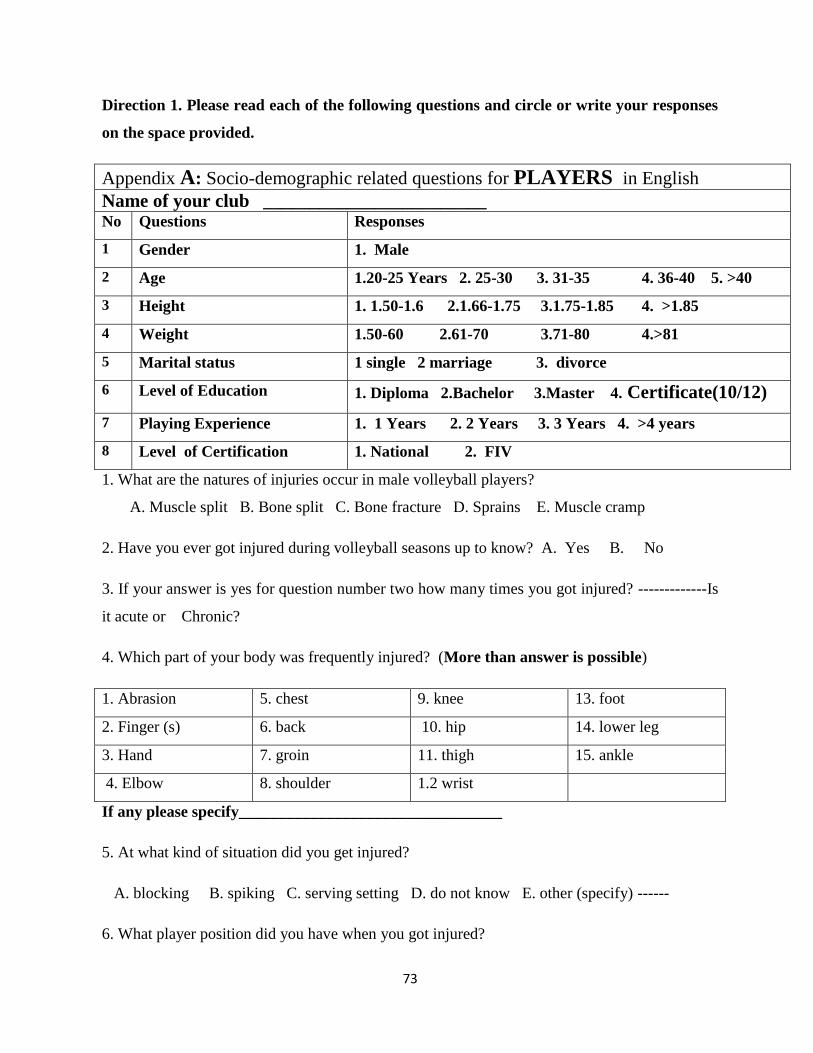
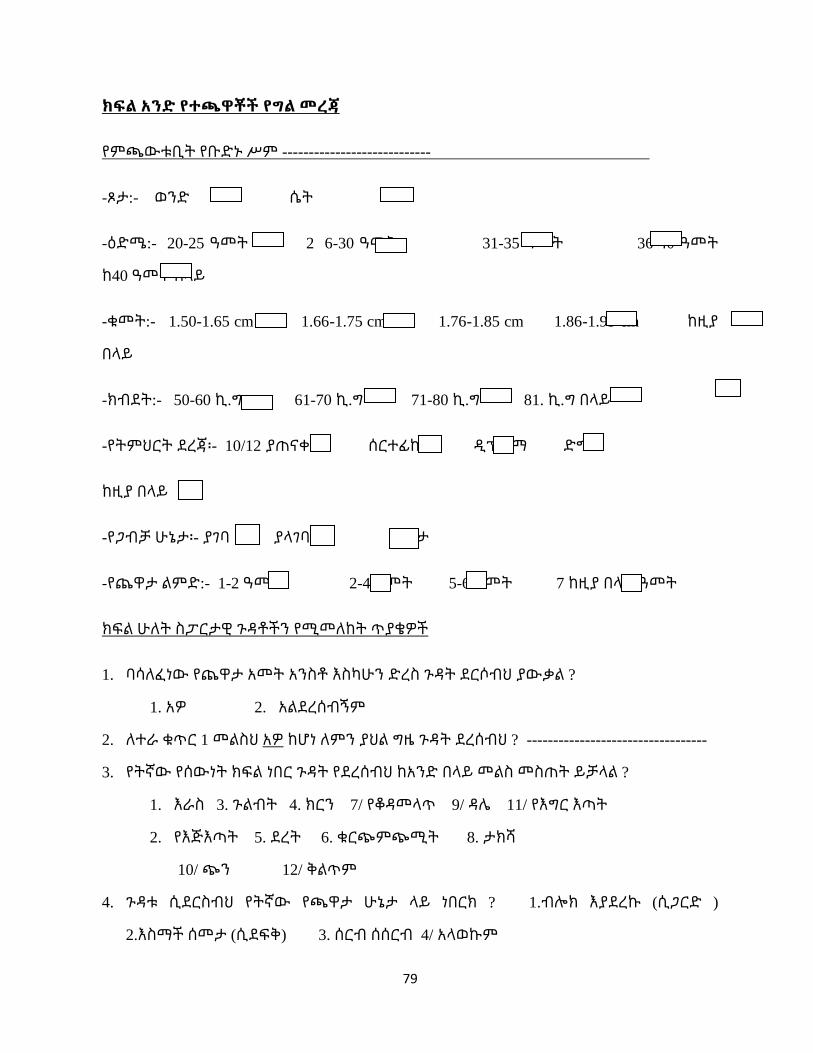
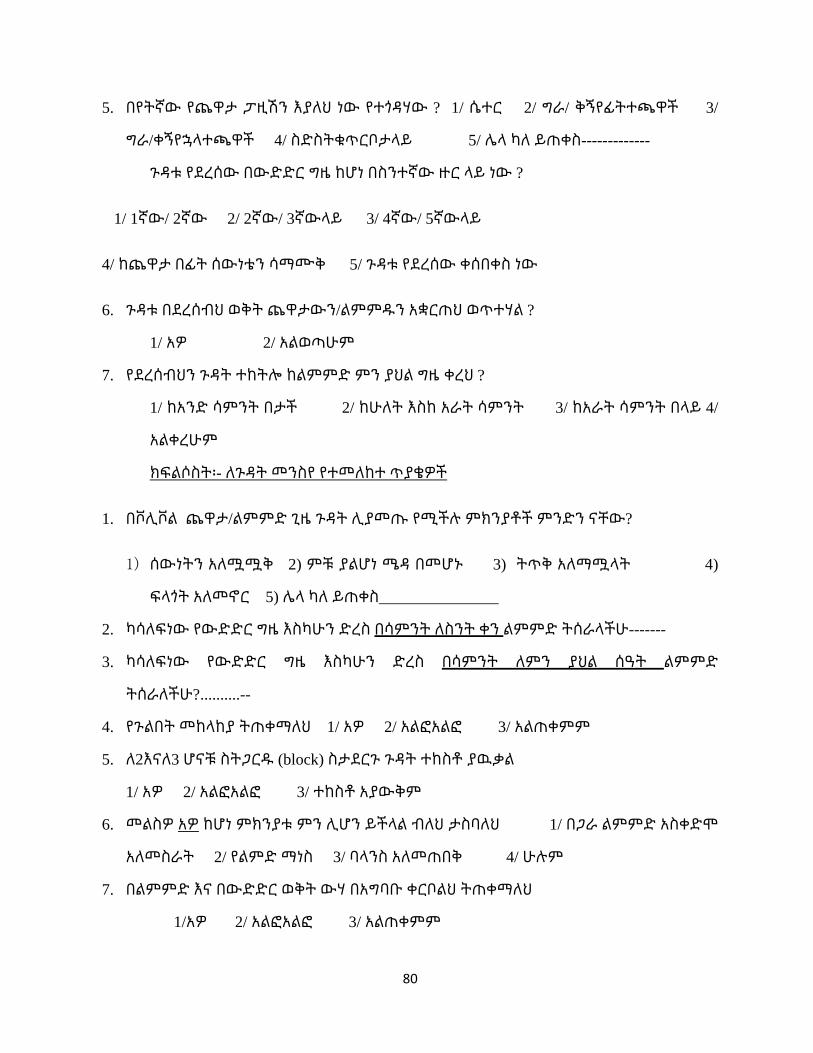
3.6. Data collection Instruments/Tools ..................................................................................... 36
3.6.1. Questionnaire ............................................................................................................... 36
3.6.2. Interview; ..................................................................................................................... 36
3.7. Data Collection Procedures ................................................................................................ 36
3.8. Methods of data analysis (statistical applications) ............................................................. 37
3.9. Ethical Consideration ......................................................................................................... 37
CHAPTER FOUR ......................................................................................................................... 38
4. RESULTS AND DISCUSSION ............................................................................................... 38
4.1 Result ................................................................................................................................... 38
4.1.1 General Characteristics of Respondents ........................................................................... 38
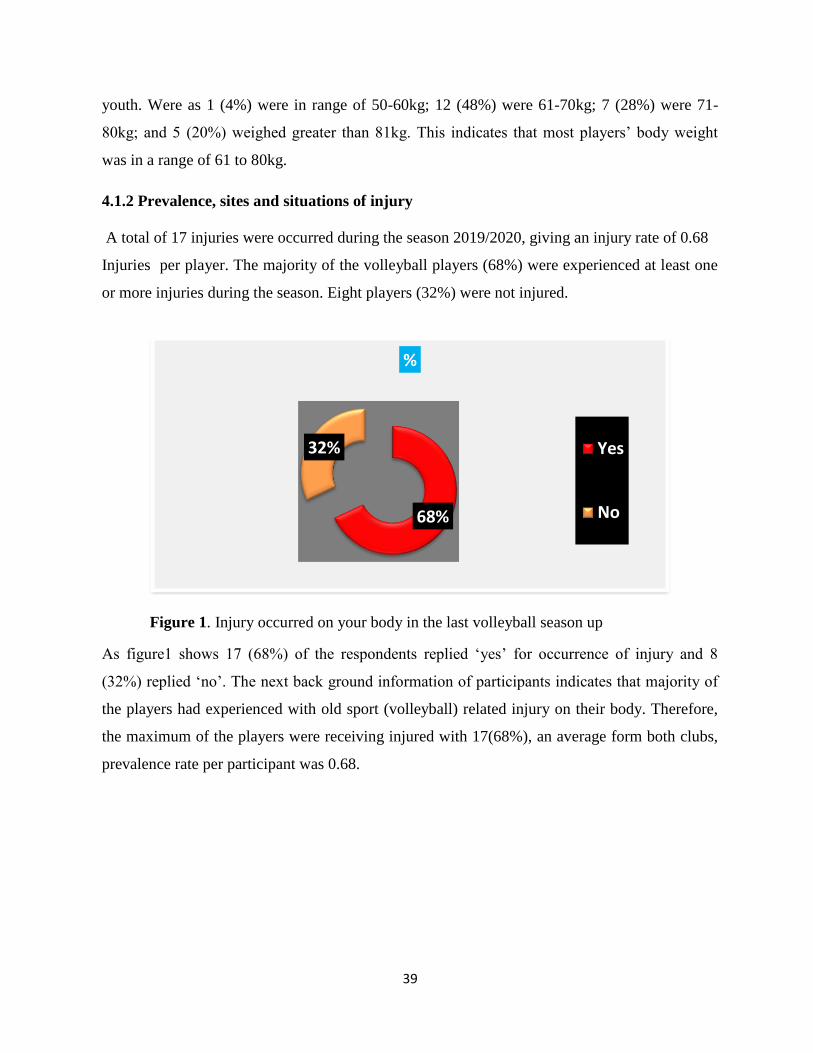
4.1.2 Prevalence, sites and situations of injury...................................................................... 39
4.1.3. General Characteristics of Coaches ............................................................................. 50
4.1.4. General Characteristics of physiotherapists ................................................................ 50
4.1.5. Interview made with coaches and physiotherapists ..................................................... 51
4.2. Discussion .......................................................................................................................... 55
4.2.1. To determines the prevalence of sport injuries related with volleyball sport. ............. 55
4.2.2. To identify types and sites of sport injuries among male volleyball players. ............. 56
Page 11
vi
4.2.3. To identify the major factors associated with the injuries sustained among the players
in a volleyball season. ............................................................................................................ 57
CHAPTER FIVE .......................................................................................................................... 59
5. SUMMARY, CONCLUSION AND RECOMMENDATIONS ............................................... 59
5.1 Summary ............................................................................................................................. 59
5.2 Conclusion ........................................................................................................................... 60
5.3 Recommendations ............................................................................................................... 61
5.3.1 Recommendations for solution ..................................................................................... 61
5.3.1.1. To Coach................................................................................................................... 61
5.3.1.2. To clubs players ........................................................................................................ 62
5.3.1.3. Recommendations for future researchers ................................................................. 63
REFERENCE ................................................................................................................................ 64
APPENDIX ................................................................................................................................... 72
Page 12
vii
LIST OF TABLE
Table 1 Frequency of injury occurrence ....................................................................................... 40
Table 2 Respondent‟s response on injury occurrence related with body part .............................. 40
Table 3 Response on injury occurrence during double and triple block....................................... 42
Table 4 Type of injury occurred during double and triple block ................................................. 42
Table 5 . Did you withdraw without completing the training and match play at the time of
injured? ......................................................................................................................................... 44
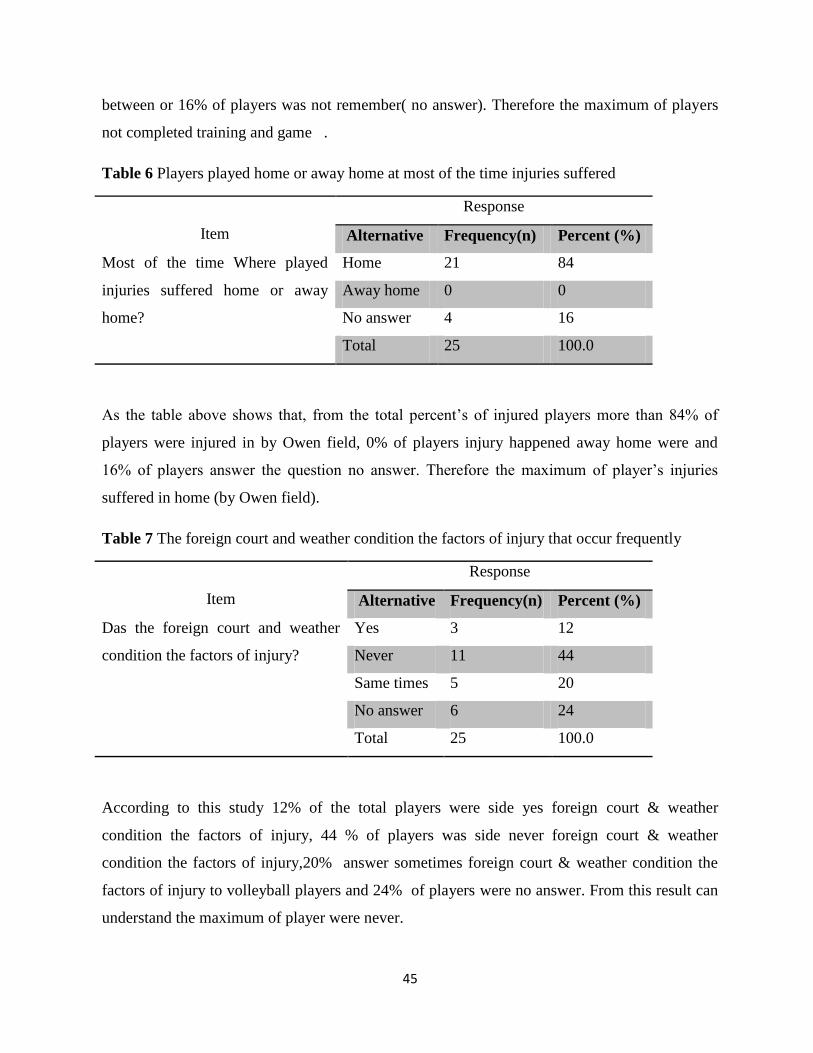
Table 6 Players played home or away home at most of the time injuries suffered ...................... 45
Table 7 The foreign court and weather condition the factors of injury that occur frequently ...... 45
Table 8 able8. Amount of absent players following to injury from training ................................ 46
Table 9 What are the natures of injuries occur in male volleyball?.............................................. 48
Table 10 Cultural dance and emotional jumping celebration that contribution to injuries ......... 50
Table 11 Relation b/n injury occurrence during different skills ................................................... 52
Table 12 Cultural dance and emotional jumping celebration that contribution to injuries after
scoring ........................................................................................................................................... 53
Table 13 Association of injury occurrence with upper or lower extremity ................................. 53
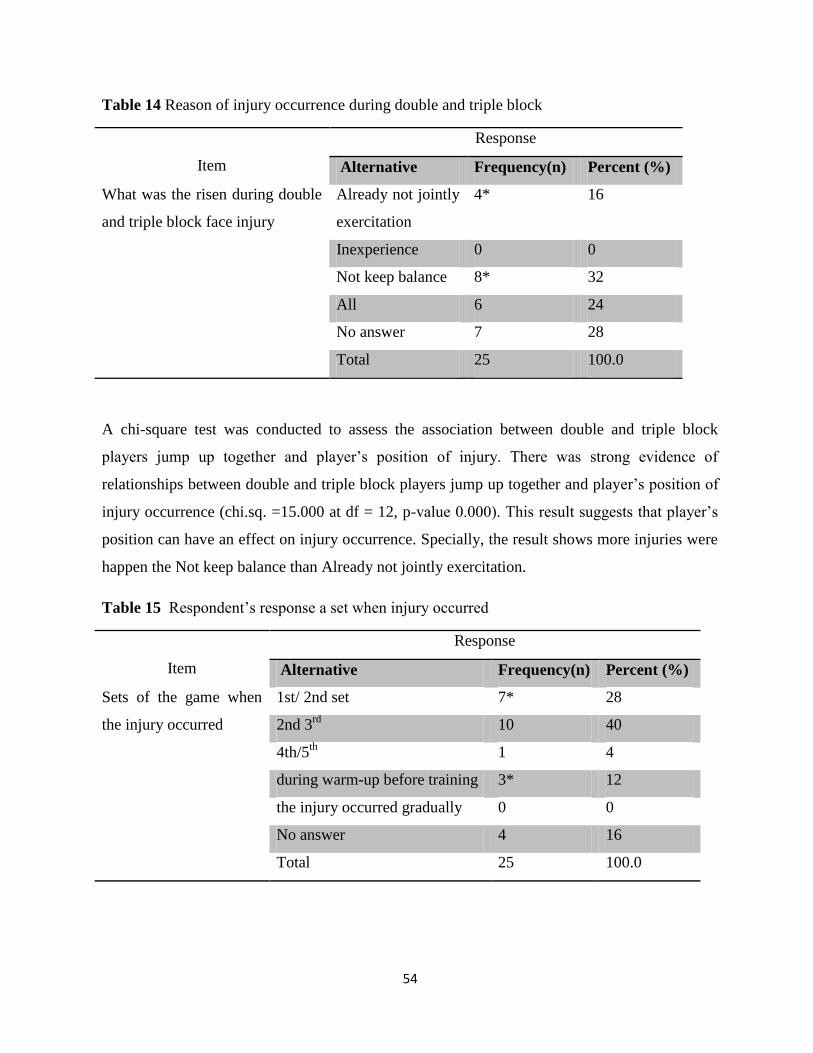
Table 14 Reason of injury occurrence during double and triple block ......................................... 54
Table 15 Respondent‟s response a set when injury occurred ...................................................... 54
Page 13
viii
LIST OF FIGURE
Figure 1. Injury occurred on your body in the last volleyball season up ...................................... 39
Figure 2 Situation at which injury occurred. ................................................................................ 41
Figure 3Position at where did you got injured .............................................................................. 43
Figure 4 At which set did you get injured, when the injury occurred in game? ........................... 44
Figure 5 What are the main causes of volleyball injuries in the players? ..................................... 46
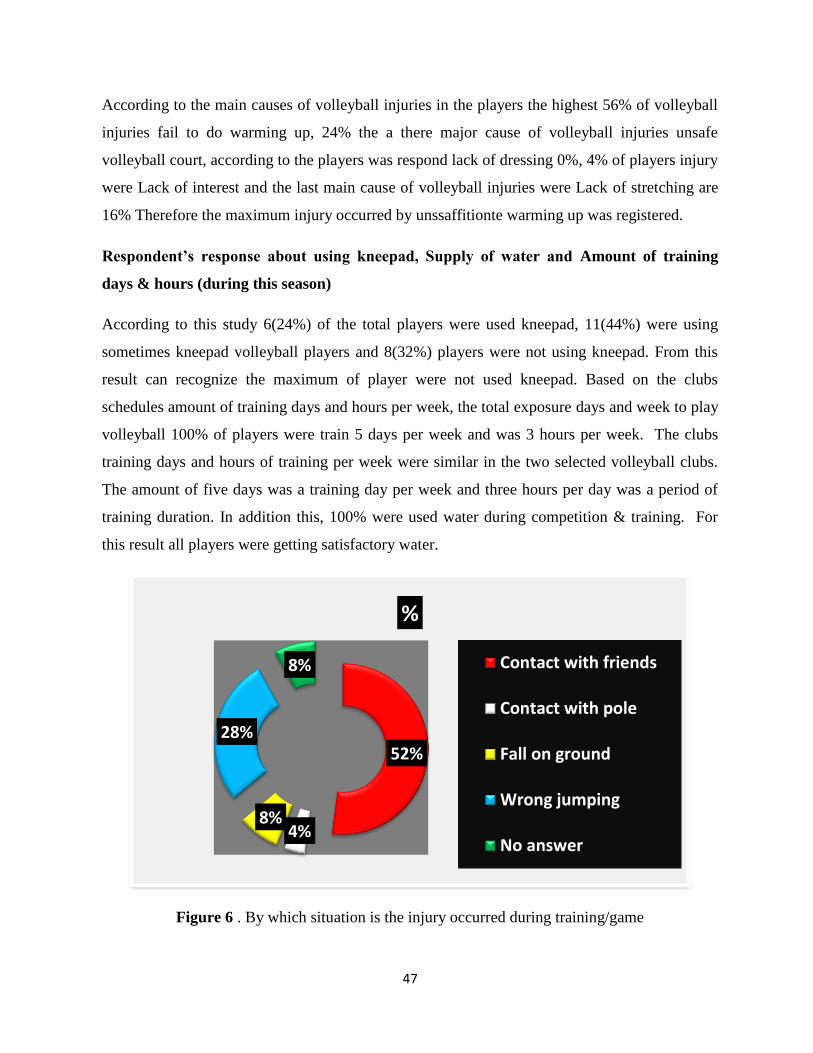
Figure 6 . By which situation is the injury occurred during training/game .................................. 47
Figure 7 Physiotherapy services get access at the time of injured ................................................ 49
Page 14
ix
LIST OF ABBREVIATIONS
AS Ankle sprain
WDC Wolaita Dicha Club
USA United States of America
EFV Ethiopian Federation of Volleyball
MWUC Medawolabo University Club
FIVB International Federation of Volleyball
CAVB Confederation African de Volleyball
YMCA International Young Men‟s Christian Association
SNNPR South Nation Nationality People Region
Page 15
x
ABSTRACT
Although physical activity brings a range of lifelong health benefits, it may also lead to injuries
that pose a significant threat to health and hinders sport performance. The aim of this study is to
investigate prevalence of sport injury and its associated risk factors in the case of Wolaita Dicha
and Madda Walabo University male volleyball premier league clubs. a descriptive survey
design; qualitative and quantitative research approach was employed. To achieve the desired
purpose 26 male volleyball players aged 20 to 35 were selected from both clubs by census; 2
coaches and 2 physiotherapists were selected by purposive sampling technique. Relevant data
were gathered through self-developed questionnaire and semi-structured interview. Data were
scientifically and systematically analyzed and interpreted. Results revealed that sustained
volleyball related injury frequency of prevalence was 68%, which had incidence of 2.06 per
injured player. Ankle, shoulder and Hand figure injuries were the most common injuries
sustained volleyball players. Sprain, dislocation and muscle cramp were the common types of
injuries in the players. Inadequate warm-up and stretching, poor execution of techniques, and
contact with other player were common causes of injury. The study also showed that most of
injuries occurred during block; in terms of position that left/right front position players got most
of injuries followed by the center back. Awareness programs highlighting prevention strategies
and physiotherapy intervention are required for coaches and in the prevention of volleyball
injuries. Players’ safety attention should be prior to wining intention. Similar study in a large
size population should be conducted.
Key words: injuries, prevalence, volleyball, clubs,
Page 16
1
CHAPTER ONE
1. INTRODUCTION
This chapter deals with the background information regarding sport injuries in general and
volleyball injuries specifically in Wolita Dicha and Medawolabo University Male Volleyball
Premier League Clubs and also includes the Statement of the problem, Research questions, the
objectives (General and Specific), Significance of the study and Delimitation of the study,
Limitation of the study and Definition of Operational Terms.
1.1. Background of the study
Volleyball is one of the most widely played sports in addition to football and basketball. It has
become a very popular sport globally over the last 30 years. The International Federation of
Volleyball (FIVB) represents about 150 million players in approximately 170 countries
(Stasinopoulos, 2004). It is played at different levels of competition, and organizations, starting
from youth to the professional level. Considering the popularity of the sport, there is a lack of
information about volleyball injuries and their mechanisms ( Bahr & Bahr, 1997).
The Volleyball World Championship was started in 1974 for men by the FIVB and is now run
every four years. Three years later, the women‟s version was added to the championship. The
Volleyball World Cup is another event established in 1965 for men and in 1973 for women. It
was established in order to fill the gap between the world volleyball championships and the
Olympic Games. The leading teams in the Volleyball World Cup are automatically entered into
the Olympic Games. The Volleyball World league is also an important event that was created in
1990 for men and organized by the FIVB. The final games are usually played in Poland. It
includes 12 teams participating in the final games from 5 continents. Volleyball currently has a
good status sports program in billions of people across the globe join in; watching, listening to
and reading about the greatest global celebration of sport. When athletes come together from
around the world to compete in the games, they are fulfilling their dreams and competing at the
highest level played in all continents, with its own playing concept and identity. Volleyball it
was subsequently spread to other parts of the world during the World War I by the American
troops. Since, it is not a very vigorous sport; women also took interest in the sport and started
playing Volleyball (Seminati and Minetti, 2013).
Page 17
2
According to Abdelnour (2008), in Africa Confederation African de Volleyball (CAVB) is the
volleyball controlling body located in Cairo, Egypt. It includes 36 African countries and
organizes five different volleyball activities in Africa such as: African volleyball championship,
African volleyball championship under 21, 20, 19, and 18 years old. Egypt, Tunisia, Algeria,
Cameroon, and Kenya are the top volleyball teams in Africa. The African performances
internationally are still slow according to the above researcher regarding studies volleyball in
Africa.
In Ethiopia the sport volleyball has grown fast and its popularity has increased despite other
sports, Volleyball has been one of the most popular sports in Ethiopia since the 1970s. The
country participated in continental competition both in the men and women‟s category until the
late 1990s. These days, volleyball no longer enjoys popularity among Ethiopian sports fans.
According to the writer (personal communication), explores the issue to report this, though
experts look frustrated by the lack of international competitions for the national team, EVF
seems busy with projects at the lower level.
Volleyball requires a variety of physical attributes and specific playing skills therefore
participants need to train and prepare to meet at least a minimum set of physical, physiological
and psychological requirements to cope with the demands of the game and to reduce the risk of
the injuries. Volleyball playing largely involves, jumping, stretching, twisting, diving, spiking
and turning movements that increases the vulnerability of the players to greater risk of injuries
(Seminati and Minetti, 2013). Research showed that early mobilization in ankle sprain (AS)
shows better outcomes than immobilization or restoring ankle sprain(Seminati and Minetti,
2013). In addition, physiotherapy management results to fewer residual symptom and improve
the range of motion and early return to sport. The physiotherapy treatment in ankle sprain (AS)
will focus on reducing pain, swilling and restoring the ankle motion as well that can be achieved
through applying ice bath with specific exercise (Jibuike O, 2003).In the epidemiological
studies, injury occurs in training or matches, interrupt or hampered play effect of injuries
.Special treatment is required in order to continue the game, or if the injury has made playing
impossible. Beach volleyball is being studied by researchers and sports professionals from
different fields of study (Seminati and Minetti, 2013).
Page 18
3
Literature has experienced exponential growth over the last 20 years, when beach volleyball
sport was incorporated to the Olympic program in 1996 (Jimenez-Olmedo JM, 2015). Injuries
in sport are common due to contact with player, ground, objects and other reasons such as
pressure, overuse and falls. Weakness is also a common cause of injuries. For example, Physical
weakness due to a previous injury, may lead to an injury in the same area. Preventing or treating
the injury can be achieved through science and research. According to (Hawkins D, 2001) in
dealing with injury, there are factors to be considered like knowing the injury extension, the
mechanisms, and the preventative strategies. Physiotherapy is a branch of rehabilitation that
deals with musculoskeletal injuries. Therefore, physiotherapy intervention is very important in
injuries in general. Spinal cord injuries, sport injuries and work related injuries are in need of
proper physiotherapy rehabilitation after the injuries have been sustained (Frontera WR, 2003).
Therefore, the immediate physiotherapy rehabilitation helps in fast recovery and getting patients
back to the normal body activities. A worker can have the ability to get back to his work quickly
to save athletes. Physiotherapy can help in protecting the damaged tissues which will help
healing in the inflammatory stage and pain control. In addition, it helps in muscle flexibility,
strength, and balances especially during activities with assistive devices like walking with
walker, crutches and using tape or splint. Flexibility to the muscles aids in improving the
normal range of motion into the joint which will encourage the joint to return to the normal
activity (Frontera WR, 2003). Ankle, shoulder and knee injuries are common injuries in
volleyball which need physiotherapy care. That is why; this study aims to investigate the
prevalence and associated risk factors of sport injury; in the case of Wolaita Dicha and
Medawolabo University male VB premier league clubs.
1.2. Statement of the Problem
Volleyball is recognized as one of the most widely played sports in world level and it is the
sport of choice for many in Ethiopian. It has been recognized as both recreational and
professional sports that have a positive effect of health and social benefits nature. But, sport
involves a risk of injury. Injuries in volleyball are quite frequent as mentioned by different
scholars (Verhagen, 2004). It is supposed that an increase in the frequency, intensity and
duration of training might lead to an increased rate of injury. Volleyball is technically heavy
game with many dynamic movements from that Volleyball game has relatively low rates of
Page 19
4
injury compared to other sports, but injury rates are on the rise according to a recent study (Bere
et al., & Bahr, 2015; Eerkes, 2012). Since volleyball is a non-contact game, where trainees
from the opposing teams are separated by the net, it may be expected that the incidence of
injuries is low. But, the opposite is true. Its heavy shuffling, fast movement, forceful jumping,
blocking, spiking and improper landing as well as game‟s position is inevitable to introduce an
injuries to players (Bere et al., 2015).
Given literature reported sport injury status there is a shortage of data about sports injuries
among professional volleyball sports players in Ethiopian. Only one study in northern parts of
Ethiopian volleyball players had been reported (Abeje, Alemayehu & Ephrem, 2016). In the
study area, there are a number of male and female athlete projects of volleyball players and only
two premier league clubs. Given this there is no study done to assess the Prevalence of sport
related injuries and its associated risk factors in the selected clubs: Wolaita Dicha and
Medawolabo University Male Volleyball Premiere League Clubs. Therefore the purpose of this
study was to examine the prevalence, types, their causes and anatomical location of the
volleyball injuries occurred among players in two clubs.
1.3. Research questions
In this study following research questions were formulated:
What is the prevalence of sport injuries that occurred in male volleyball players?
What are the anatomical locations of players most frequently affected by sport injuries in
volleyball?
What are the major factors associated with the volleyball injuries sustained among the
players?
1.4 Objectives of the study
1.4.1 General objective
The General Objective Of The Study Was To Investigate The Prevalence Of Sport Injury And
Its Associated Risk Factors In The Case Of Wolaita Dicha And Medawolabo University Male
Volleyball Premiere League Clubs In The Study Area.
Page 20
5
1.4.2. Specific objectives
The following specific objectives were designed to address:
To determine the prevalence of sport injuries related with volleyball sport
To identify types and sites of sport injuries among male volleyball players.
To identify the major factors associated with the injuries sustained among the players in a
volleyball season.
1.5. Significance of the Study
The study has the following expected significances.
This study help to provide meaningful experiences to the physical educationist, coaches,
projects, clubs and Volleyball expertise to consider such information in appropriate
training method so as to minimize occurrence of injury.
The findings of this study important to provide information on what expected from
athletes, coach, physiotherapy and communities for young generation.
It also helpful for trainees to know the site, various cause of injury and used as a
reference for the scientific community.
This study might be creating awareness for coaches and athletes to do the proper
warming up and stretching activities to minimize the incidence of injury and indicate
how to improve sport safety.
The result of the study is believed to serves as stepping stone or helps as basic reference
for those who began to conduct further investigation.
1.6. Delimitation (Scope) of the Study
This study is confined in its scope to Wolaita Dicha club on SNNPR in Wolaita Zone and
Medawolabo University club in Oromia Region Bale Zone Robe Taiwan. Additionally, the
study also is delimited only to investigate the prevalence of sport injury and its associated risk
factors in volleyball sport. So to this affect, the study delimited only to Wolaita Dicha and
Medawolabo University male premier league volleyball clubs.
Page 21
6
1.7. Limitation of the study
To undertake this study the researcher was limited by the following obstacles:-
The Prevalence, site of injured body part and causes were not recorded in the clubs area,
due to this the data collected through questionnaire and interview were analyzed.
Players might be forgetting minor and major injuries in volleyball players. Because of
the major and minor injuries, there are it is easy for the player to rehabilitation for the
physiotherapist to normal body. And both clubs are too far away from learning center.
The shortage of review literatures
Willingness for answers from respondents
1.8 .Operational Definitions of terms
Sport: Is an activity involving physical exertion and skill in which an individual or a team
competes against another or others for entertainment.
Project: a piece of planned work an activity that is finished over period of time and intended to
achieve a particular purpose (Cambridge dictionary).
Club: a group of people how meet regularly to pursue an interest in a competitive collegiate
activity at the state, regional and national level.
Prevalence: Total number of existing cases at a particular point in time. Whereas incidence
total number of new cases over a particular time period. The definition of prevalence and
incidence of /volleyball injuries has been designed in different sources of literature in different
ways (Nelso et al., 2007).
Cause: A circumstance, fact, or influence that contributes to a result (English oxford living
dictionaries)
Injury:is damage to the body caused by external force.
Page 22
7
CHAPTER TWO
2. REVIEW OF RELATED LITERATURE
This chapter attempts to provide a review of the related literature directed specifically at
Volleyball injuries. The literature will concentrate on some important areas related to the study
such as the prevalence of volleyball injuries, what type of volleyball injuries which frequently
occur? Which body parts are mostly affected? and nature of the volleyball injuries and cause of
injury mechanisms intervening volleyball training and competition. In addition, it reviews
literature on injury prevention and it highlights the gaps in the literature regarding volleyball
injuries. The chapter will include discussion of some specific injuries which are common in
volleyball. It will also show the players‟ positions and the common actions performed by the
players in volleyball.
2.1 Sports injury theoretical literature
Volleyball is practiced by approximately 800 million people with diverse characteristics,
including different age groups. Sports injuries have become one of the most common injuries in
contemporary volleyball players together with soccer and basket is at the first places in the ball-
related sports causing injuries. Injuries in volleyball are quite frequent (Verhagen, 2004).
The term „sports injury‟ is used to refer to a variety of musculoskeletal damage caused by sports
participation. Recently, studies have provided some „consensus‟ helping to standardize the
definition and classification of injuries improving the comparability between studies, settings,
sports facilities, injury measurement systems, and also between different time-points. There are
general definitions, such as injuries are considered disorders of the musculoskeletal system or
concussions and specific definitions, such as injuries requiring medical attention (i.e. any injury
that leads to health care utilization) or injuries leading to time loss (i.e. injuries that hamper the
ability to fully participate in sports for at least one training session or competition).
A theoretical definition of an injury is often difficult because of its dependence on context
(Fuller, 2010). Generally, sports injuries are considered as all types of injury occurring during
sporting activities (Roald Bahr & Krosshaug, 2005). An injury occurs when the stress that falls
upon a tissue exceeds the tissue‟s ability to absorb the stress acutely or chronically (McBain et
Page 23
8
al., 2012b). Two broadly acceptable injury definitions are based on medical treatment, which
includes injuries requiring any treatment from a physician, and loss-of-time, which includes
injuries that result in loss of time from training or competitions (Brooks & Fuller, 2006). Every
day, a lot of people all over the world participate in games and sports activities or competitions.
Participation in sports improves physical fitness and overall health and wellness. Games and
sports training can also result in injuries, some slight, minimal, minor, or some serious and still
other in lifelong medical problem (Kordi et al., 2011). Sport injuries result from acute trauma or
repetitive stress associated with athletic activities. Sports injuries can affect bones or soft tissue
(ligaments, muscles, tendons).
There are numerous sports injuries happened in the field of sports. It is very important for all
coaches, trainers and players to know the causes symptoms, prevention and treatment for all
these common injuries in order to avoid most of these types of injuries, also to update the poor
training methods. In many cases, these types of injuries are due to overuse of a part of the body
when participating in a certain activity. Additionally sport injuries occur while participating in
organized sports, competitions, training sessions, or organized fitness activities. Common high
injury risk sport are, for example football, soccer, basketball, cricket, volleyball, tennis as well
as contact sports as a whole (Frisch et al., 2009).
sports injuries are considered as all types of injury occurring during sporting activities (Roald
Bahr & Krosshaug, 2005). An injury occurs when the stress that falls upon a tissue exceeds the
tissue‟s ability to absorb the stress acutely or chronically (McBain et al., 2012a). Although
variations in definitions and methodologies may create significant differences in the results and
conclusions obtained from studies of sports injuries, there is still lack of consistency in the
definition of sports injuries (Fuller et al., 2006). There are only few consensus statements on
injury definitions in the studies on sports injuries. These consensus statements are concerning
team sports such as football Fuller et al. (2006), rugby Fuller et al. (2007). Consensus
statements can be used as the basis of definitions for studies in other team sports based on injury
occurrences. Generally, as Fuller et al. (2006), states that injury is “Any physical complaint
sustained by a player that results from a match or training irrespective of the need for medical
attention or time loss from volleyball activities. An injury that results in a player receiving
Page 24
9
medical attention is referred to as a medical-attention injury and an injury that results is a player
being unable to take a full part in future volleyball training or match play as a time-loss injury
2.2 Types of volleyball injuries
There are a number of studies concerning the prevalence and incidence of volleyball injuries.
Review evidence recognized that moderately higher injury rate for overuse shoulder injuries
compared to the backspin. The review identified playing hours, age, biomechanical and
anatomical features of a volleyball technique as the main risk factors for overuse upper limb
injuries (Seminati & Minetti, 2013).
The definition of prevalence and incidence of volleyball injuries has been designed in different
sources of literature in different ways. Incidence can refer to the number of injuries per hours.
The injury incidence in volleyball has been estimated to be between 1.7 and 4.2 per 1000 hours
of play and is the furthermost common source of sports injuries (Stasinopoulos, 2004). Studies
have proven that volleyball injuries in the United States Volleyball Association (USVBA) are
estimated around 2.3 per 1000 hours (Nelson, et al., 2007). Various studies have indicated that
injuries in volleyball are quite common and that they occur in games more often than in training
(Agel et al., 2007; Augustsson et al., 2005). There is still debate on the concept of injury
prevalence. in a study conducted among United States high school sport athletics, where it was
found that Ankle Injuries (AI) during training are much higher than in games. Overuse and
acute injuries appear to be equally as common in volleyball as in other sports (Augustsson et al.,
2005).
In the national collegiate athletic association, the injury prevalence of the lower extremity
reaches up to 55% and 20 % for the upper extremity (Agel et al., 2007). The data on volleyball
injuries showed that there is an increase in the injury rate with the level of participation from
school to colleges to clubs. In addition, older studies used to show lower rates of injuries than
the recent studies. The incidence of injury in volleyball is nearly equivalent to those observed in
ice hockey and soccer (Seminati & Minetti, 2013).
A study done among volleyball players of Iran, fingers and chronic tendon injury were reported
as the most prevalent and most common type of injuries. Weight, seated height, torso width at
Page 25
10
umbilicus, torso circumferences at hip are the determinants for injuries prevalence, sprain,
dislocation and tendon and muscle chronic injuries. Significant relationship was observed
between injuries prevalence and types of injuries with games‟ position. Fingers, ankle, knee and
shoulder injuries were also described as the highest prevalent injuries (Fattahi, Sadeghi, &
Ameli, 2011).Another study conducted in Denmark identified spiking and blocking as causes
for most injuries. Acute injuries to fingers and ankles or overuse injuries to shoulders and knees
were reported frequently. Shoulder injuries seemed to be more serious problem in females
(Svantesson, 2006).
Moreover, a study carried out among USA high school students revealed that in all sports
except girls‟ volleyball, ankle injury rates were higher in competition than during training and
most ankle injuries were diagnosed as ligament sprains within complete tears (Belay, Tamirat,
& Science, 2016). A study in Greek among male volleyball players pointed out injury
occurrence is dependent on age and juniors had lower rate than seniors. Acute injuries were
significantly more common than overuse syndrome and the ankle was the most common injured
anatomical location. Besides, outside hitters, universals and setters faced different injury rates
and the “incorrect sprawls” and “stepping on others‟ feet” were the most common injury
factors(Sole, Kavanaugh, & Stone, 2017). Furthermore, a study involved elite Swedish
volleyball players described that anatomical positions including ankle, followed by the knee and
the back where the majority of the injuries were located.
These most injuries were occurred during training and substantial proportion of injuries had a
gradual on set. Specific court related blocking and during spiking were described as causes for
injuries (Svantesson, 2006). Another study conducted by involving five Norwegian sports
revealed that knee was the anatomical position where overuse injuries had occurred greatly in
volleyball (Hassan, Student, & Cape, 2008).Across types of injuries, the ankle was the most
commonly injured region, followed by the lower back, knee, shoulder and fingers. Of the ankle
injuries, 79% were recurrences, and the relative risk of injury was higher for previously injured
ankles compared with non-injured ankles(Seminati & Minetti, 2013). A study conducted at
2001 Beach Volleyball World Championships reported that knee, ankle, and finger injuries
accounted for more than half of all acute time-loss injuries. Low back pain, knee pain, and
shoulder problems were reported as the three most common overuse conditions(Hassan et al.,
Page 26
11
2008). Most volleyball injuries are related to blocking or spiking, both of which involve vertical
jumps. The most common acute injuries include ankle and thumb sprains, and common overuse
injuries include patellar and shoulder tendinitis, suprascapular neuropathy, and low-back injury.
Symptoms will usually resolve with conservative treatment, which may include activity
modification, such as reduced jump training or jumping on a sand surface, and technical
instruction (Miranda, Mas, Lopez, Perez, & Micheo, 2015). African continent to assess the
status of injuries experienced at professional or amateur levels even though researchers believe
that the injury prevalence in Africa could be higher than the cases observed in the developed
countries. But there was no related research in Ethiopia in this case (Saavedra, 2003). One of
the most important reasons for collecting data on the prevalence of sport injuries was to provide
a guide for injury-prevention and improve sport safety. Volleyball injury is needs to be directed
to injuries occurring as a result of participation in volleyball.
Due to injury, players restricted from participation for one or more days from training and
games, clubs loose points from games. If this problem will not be resolved, the players can‟t
play permanently, will be affect with chronic injury and the clubs will also getting the least rank
with volleyball competition. Considerable researches have been done abroad in sport injury
related to volleyball sport. However as per the knowledge of the researcher there was no
research that conducted in Ethiopia to assess the prevalence and associated factors of volleyball
injuries occurred on professional volleyball players. In Ethiopia, a study conducted among
volleyball players of public universities reported higher injuries prevalence among female
players than male players. Strain, ankle, finger and thumb dislocation injuries were the most
frequent. Injuries were more frequently occurred during match than during team training.
Blocking, setting, executing wrong technique, and stepping on other‟s foot were the causes of
injuries. Lower and upper extremities injuries were required more time to recover (Desalegn &
Zenebe, 2016).
2.3. Injury mechanism in sport
Injuries in volleyball are most commonly attributed to jumping, landing, hitting, and blocking
movements, with the majority of acute and overuse injuries occurring from jumping.
Additionally, more injuries occur during hitting and blocking tasks than passing and setting in
Page 27
12
volleyball (Eerkes, 2012). As the above researcher the ankle is the most commonly injured
joint, but the knee, shoulder, lower back and fingers also vulnerable.
There are a number of studies concerning the prevalence and incidence of volleyball injuries.
The definition of prevalence and incidence of volleyball injuries has been designed in different
sources of literature in different ways. Various studies have indicated that injuries in volleyball
are quite common and that they occur in games more often than in training (Agel et al., 2007;
Bahr & Bahr, 1997; Stasinopoulos, 2004; Verhagen et al., 2004). There is still debate on the
mentioned fact, according to Nelson et al., (2007), in a study conducted among United States
high school sport athletics, where it was found that Ankle Injuries (AI) during training are much
higher than in games. Overuse and acute injuries appear to be equally as common in volleyball
as in other sports (Verhagen et al., 2004). According to (Bere et al., 2015; Desalegn et al., 2016;
Kordi et al., 2011; Verhagen et al., 2004), in volleyball games or training sprain, strain, Ankle,
knee, shoulder, lower back, and finger are common injuries. According to Agel et al., (2007),
injuries in volleyball occur in three way, which are: -
2.3.1. Player contact
Player contact: Player contact means that the injury occurs due to attachment with another
player from the same team or the opposite team. It can be due to a player stepping onto another
player‟s foot or knee. Ankle Injury (AI) is one of the most common types of injury which
occurs during player contact. According to Nelson et al., (2007), player contact in volleyball is
the most common mechanism for Ankle Injury (AI). A typical situation is collision during a
forward move by the attacking player towards the defensive line, which represents a basic and
necessary move of all back and wing players to develop the attack.
2.3.2. Contact
It mostly occurs due to hitting/striking other objects while playing, like balls, and floor. In case
of injury due to ball contact (mostly in spiking and blocking), fingers are the common injured
body parts. The most common mechanism for Ankle Injury (AI) is forced suspiration, which
occurs when blocking player's foot lands on the opponent spike‟s foot that has crossed the net
line (in the conflict zone"). A study done in the Netherlands by Verhagen et al., (2004) found
that 75% to 78% of all players with an Ankle Sprain (AS) experienced previous Ankle Sprain
Page 28
13
(AS) rehabilitation, including proprioceptive training. Ankle orthoses or taping has been found
to assist in active rehabilitation of Ankle Sprain (AS).Functional instability is the most common
complication after Ankle Sprain (AS) and it occurs in15-60% of athletes who had ankle sprains
(Seminati & Minetti, 2013). Soda, Amorism, & Sacco, (2007), stated that functional instability
is a result of muscles‟ imbalance due to mechanical, motor, and sensory factors which occur
after Ankle Sprain (AS) in muscles.
2.3.3. No contact
It can occur due to stressful movement or heavy loading after landing. As a result landing after
Jumping on a single leg. A severe knee, ankle, and shoulder injury usually occurs in a non-
contact mechanism.
2.4. Mechanisms of volleyball injuries
In volleyball, there are major actions player‟s needs to perform while playing. During those
actions, and due to the fast speed in action, the risk of being injured is increasing. The major
actions during volleyball are as follows:
2.4.1 .Spiking
This is when a high amount of topspin is applied to the ball to direct the ball in a short
horizontal direction into the opposite team‟s zone. The spike effect increases with the ball high,
which means that the higher setting to the ball, will give better fast spiking. In spiking, overhead
arm swing is performed with the body in the air, which means that there is no closed chain
support (Jacobson & Benson, 2001). It requires quick timing and adjustment to the ball.
2.4.2. Serving
Is the action of sending the ball into the opposite team‟s zone after winning one point. The aim
while serving is to score and make it more difficult for the opposite team receiving the ball
(Masumura et al., 2007). The fast serve is also known as “spikes serve” and it is an effective
technique to use while serving, due to the high speed of the ball.•
Page 29
14
2.4.3. Blocking
Blocking is a defensive action to keep the other team from spiking successfully into the
blocking team‟s zone. Most ankle and knee injuries in volleyball occur while blocking (Nelson
et al, 2007). Similar to spiking, blocking depends on the vertical jump which involves ankle
force to Dorsi flexion, followed by knee and hip extension force to increase the jumping
(Hughes & Watkins, 2008). That requires strong knee and ankle extensor muscles.
2.4.4. Setting
Is the action of passing the ball to the teammate before spiking over the net? Most
musculoskeletal injuries (MSI) in volleyball occur due to landing which follows blocking and
spiking or jumping before blocking or spiking. . According to Salci, Kentel, Heycan, Akin, &
Korkusuz (2004), 68% of the MSI occur due to the above-mentioned movements in volleyball.
2.5. Common volleyball injuries
The most common injuries in volleyball are acute injuries of fingers and ankles, and overuse
injuries of the knee, shoulder and lower back (Bere et al., 2015; Verhagen et al., 2004). The
burden of injuries in volleyball is significant, with overuse injuries being more common and
resulting in as much athletic impairment as acute injuries. When compared to other Olympic
sporting events, volleyball has a relatively low incidence/ of time loss injuries (Bere et al.,
2015). In this aspect commonly location injuries are as shown below.
2.5.1. Ankle Injuries
Ankle injuries are the most common acute injury affecting volleyball players. Ankle Injuries
(AI) accounts for 15-60% of acute injuries in volleyball (Reeser et al., 2006; Augustson et al.,
2005; Verhagen et al., 2004; Nelson et al., 2007) and According to Bahr & Bahr (1997),
previous studies indicated that an Ankle Sprain (AS) is the most common type of injury in
volleyball, accounting for one-quarter to one-half of the overall quantity of acute injuries.
According to Verhagen et al. (2004), reported that frequently ankle sprains account for up to
half of all reported volleyball injuries Furthermore, Ankle Sprain (AS) They commonly occurs
near the net during jumping and landing is performed, fxecution of the blocking and spiking
actions, with contact with another player being sustained. 19% of these types of injuries occur
Page 30
15
due to landing on a team mate‟s foot, which is considered as a technical error. But, the previous
ankle injuries are still the main risk factors. Suda, Amorim, & Sacco, (2007), stated that
functional instability is a result of muscles‟ imbalance due to mechanical, motor, and sensory
factors which occur after Ankle Sprain (AS) in muscles such as invertor and evertor muscles as
well as peroneus longus, tibialis anterior, and gastrocenemius . In addition to previous injury,
the other common risk factor for ankle injury is poor dynamic balance (Plisky, Rauh, Kaminski,
& Underwood, 2006).
2.5.2. Knee injury
Knee injuries in volleyball can be divided into two primary categories of acute and overuse.
While repetitive jump landing sequence jumper‟s knee is the most common overuse knee
diagnosis and it affects male athletes‟ disproportionately more than female athletes. This is
theorized to be due to an increased jumping ability and therefore greater load on the extensor
mechanisms of the knee. Knee injuries are reported as acute injuries in most of the cases. That
is due to the high ability to generate strength while vertical jumping. The quadriceps produces
high strength to help in muscle imbalance between knee extensors and flexors. These will cause
overload of the tendons of the knee joint. Gisslen, Gyulai, Soderman, & Alfred son (2005),
found that knee sprains and meniscus tears account for approximately 15% of acute injuries.
Furthermore, Gisslen et al., (2005), stated that patellar tendonitis (jumper's knee) accounts for
up to 80% of overuse injuries. According to Malliaras, Cook, & Kent, (2006), tendon
abnormality accompanied with pain is known as patellar tendinopathy. Patellar tendinopathy
may present in 25 per cent of volleyball players. It is quite difficult to treat and can stay with the
volleyball player even after quitting from volleyball in a later stage or age. There is a strong
association between the Patellar Tendinopathy injury and the jump height accompanied with
low range in ankle Dorsi Flexion (DF) during jumping and landing same as the number of years
participating in volleyball.
2.5.3. Shoulder injuries
The shoulder joint is called the shoulder complex because it contains different joints such as the
Acromioclavicular Joint, Sternoclavicular Joint, Scapulothoracic Articulation, and
Glenohumeral Joint. Injuries to the shoulder seem to be the most frequently reported overuse
Page 31
16
injuries(Augustsson et al., 2005). Spiking and serving in volleyball are common actions while
playing and they apply high stress on the shoulder joint. According to Ozbek, Bamac, Budak,
Yenigun, & Colak(2006), serving and spiking are the most asymmetrical, powerful movements
which require strenuous unilateral action on the upper extremity (UE). Overhead movements
such as overhead serving and spiking, may increase the risk of impingement. The increased
force occurring at ball contact while the arm is in maximal abduction, may increase the risk of
impingement. The most common specific diagnosis of shoulder problem amongst volleyball
athletes is subacromial or rotator cuff impingement. Shoulder injuries amongst volleyball
players are predominately overuse in nature and have been found to effect up to 8.06 % of
Ethiopian public universities players, 32% of British, and 24% of American elite volleyball
players (Desalegn et al., 2016; Mjaanes & Briner, 2005). Similar to other overhead throwing
sports, volleyball athletes with overuse shoulder complaints have been found to have significant
bilateral range of motion and strength differences causes for shoulder injures (Reeser et al.,
2010). Finally, spiking during attacking is the most common action resulting in shoulder injury
due to the ball acceleration in mid-air without closed kinematic chain support. It can lead to
shoulder complex syndrome in the form of pain such as bursitis, involvement of supraspinatus,
biceps tendinitis, and instability of the shoulder.
2.5.4. Ulnar nerve injuries
Ulnar nerve injury is a common type of injury in volleyball. It can occur due to different causes
such as compression, traction, and friction. According to Ozbek et al., (2006), in most
Ulnarnerve cases, there are two abnormalities which usually appear. Firstly, compression occurs
due to hypertrophy of the surrounding soft tissues. This hypertrophy occurs due to subluxation
or dislocation of the nerve as a result of developmental laxity of the soft tissues which holds
theulnar nerve in its groove inside the cubical tunnel. Secondly, traction of the valgus force,
which occurs while throwing, is the reason for performing ulnar nerve injury. All the above-
mentioned situations occur when the repetitive flexion and extension occur in the elbow joint
while playing volleyball. When the nerve is unstable, it is easy to irritate or inflame it,
especially when the shoulder is in abduction and wrist and fingers are in extension.
The Ulnar nerve arises from the medial cord of the brachial plexus through the medial head of
the triceps. It goes behind the medial epicedial of the homers and through the cubical tunnel
Page 32
17
distally until it enters the palm of the hand. Any disorder to the nerve may appear in the form of
pain at any point of the mentioned route. According to Hyde &Gengenbach (2007), ulnar nerve
injuries occur as 25% of athletics injuries and that is due to the involvement of the hand in those
sports. In Netherland, 42% of ulnar nerve injuries in adult athletes reported success treatment
without surgical treatment (Eygendaal & Safran, 2006).
The Majority of the injuries that occurred in the current study were not due to contact with
another player. That is similar to the study conducted by Seminati & Minetti, (2013), which
found that most of the injuries in volleyball were associated with no contact with other player/s.
According to Agel et al., (2007), most injuries occurred in the ankle is due to contact. In this
study, Injuries occurred in the ankle were steps on other‟s foot at the center line or conflict zone
which is 45.16% (28/62).
2.5.5. Finger/thumb injuries
Volleyball activities, such as blocking, setting, and receiving are the most mechanisms of
injuries occur when the ball forcefully strikes the fingertip. Common finger injuries include
fractures, dislocations, and tendon and ligament tears. If you are unable to bend the finger,
consultation with your sports medicine professional or athletic trainer is important. Treatment
can vary significantly depending on the injury. Injuries to the finger/ thumb seem to be the most
frequently reported overuse injuries (Bere et al., 2015). According to Desalegn et al. (2016), the
finger injuries used to be one of serious injuries among university volleyball players in Ethiopia
and it counts 29.03% of the total number of injuries. In addition, finger injuries count 11.54% of
the total volleyball injuries in club players of the Amahara region (Abeje et al., 2016). Hard
ball and fast velocity ball in volleyball are common actions while playing and they apply high
stress on the finger tips.
2.5.6. Lower Back Injuries
According to Seminati and Minetti (2013), reported that trunk and back injuries effect 17% of
volleyball players, with professional athletes having higher injury prevalence than recreational
volleyball players. The most commonly reported injury is lower back muscle strain, an overuse
condition caused by repetitive overload of the lower back musculature. Similar to overuse
shoulder injuries, positions associated with a high frequency of attacking (e.g. outside hitters
Page 33
18
and middle blockers) are at a greater risk. Potentially, the best way to reduce stress in the
lumbar spine musculature is through the adjustment of volleyball spiking technique. Attacking
and serving volleyball athletes perform extension and rotation of the lumbar and thoracic spine.
Athletes with lumbar discomfort should look to reduce their extension while increasing their
thoracic rotational range.
2.5.7. Lower extremity
Lower extremity refers to injuries which are located in lower body appendages such as Ankle,
knees, feet, and joint structures. In the national collegiate athletic association, the injury
prevalence of the lower extremity reaches up to 55% and 20 % for the upper extremity (Agel et
al., 2007). The data on volleyball injuries showed that there is an increase in the injury rate with
the level of participation from school to colleges to clubs. In addition, older studies used to
show lower rates of injuries than the recent studies (Caine, 1996). Similar studies found Lower
extremities injuries conducted by Bahr and Bahr (1997), the ankle 54% was the most commonly
injured region. In addition knee sustained 8% of total injuries.
2.5.8. Upper extremity
The upper extremities commonly include the shoulder, wrist, finger/thumb, hands, elbow, and
trunk as well as joint structures. Acute injuries to the upper body appendages are frequent and
different studies present numbers ranging from 7% - 50% of total injuries. Shoulder injuries
have also been reported to be frequent in volleyball and handball. (Olsen, Myklebust,
Engebretsen, Holme, & Bahr, 2003).
2.6. Preventive intervention measures for sports injuries
Due to the physical and psychological consequences of injuries and its associated financial
costs, injury prevention is a top priority. According to Van Mechelen et al. (1992), emphasized
that without knowledge of the incidence, and mechanism of injury, it is not possible to
effectively prevent sports injuries. Therefore, the “sequence of prevention” was introduced,
describing necessary steps in injury prevention. Firstly, the model emphasizes that the injury
problem in terms of incidence and severity measures is identified. Secondly, risk factors and
injury mechanisms must be identified. Thirdly, preventive measures, based on information from
Page 34
19
the first and second steps, are implemented. Finally, the first step is repeated to conclude on the
effectiveness of preventive measures.
The essence of injury prevention in volleyball is to minimize absenteeism from participation in
matches due to risk factors and maximize player‟s internal drive. It is generally accepted that
basic physical preparation during training is essential to meet the increased demands and
dynamics of the current game. Precedence should be set on preventing injuries caused by pre-
mature fatigue, insufficient regeneration or athletic mismatching for players with regard to
endurance, strength, flexibility and speed. The same issues strongly feel that formulation of
structured and supervised athletic conditioning program that address individually adapted
endurance training, functional weight training, dynamic mobilization and agility drills, should
form the basis of volleyball training programs (Luig and Henke, 2010).
To achieve basic strength and power training, use of bench press and squats and specific power
training with heavier and lighter balls (Van den Tillar and Marques, 2013). Training program
should include fast accelerations with stops and short sprints with directional change (Buchheit,
2013). There is less evidence available for prevention of overuse problems to the lower back
and shoulder, but it is suggested that preventive measures should focus on load reduction
(limiting the number of spikes and jump serves) and correction of technique, as well as any
underlying imbalances of strength and flexibility through an appropriate training program.
2.7. Severity of sports injuries
As Fuller et al. (2010) views the definition of severity of an injury as the number of days the
athletes will not be able to undertake their normal training program or competition. As (Clarsen,
2015), defined injury severity as the number of days that have elapsed from the date of injury to
the date of the players‟ return to full participation in team training and availability for team
selection. All injuries that result in the athlete being unable to undertake his or her normal
training program or being unable to compete at least the day after injury are classified as time-
loss injuries (Junge et al., 2008). Other literature state different durations and classifications,
like Orchard and Seward (2002), who categorized severity of injuries according to the number
of games missed due to the sustained injury. Increasing participation in physical activity and
sports has also increased the incidence of sports injuries (Parkkari, Kujala, & Kannus, 2001).
Page 35
20
Injury severity can be categorized into three classifications. It is classified as major, moderate,
and minor injury. The classification depends on the time that the injury takes to recover.
According to Hawkins and Fuller (1998), stated that the minor or slight injuries take two to
three days to recover while the moderate take four to seven days to recover and the major
injuries usually take more than four weeks. Other literature stated different durations and
classification, like (Orchard & Seward, 2002), who classified the severity of injuries according
to the number of games missed due to the injury. According to (Bere et al., 2015; Kordi et al.,
2011), Injuries were classified according to a time loss definition five grades of severity:
However, in accordance with the majority of previous studies, this study across all age and sex
groups, most injuries were slight to severe with subsequent time loss from training of 0 to >28
days.
Injury severity was classified according to a time loss definition. Slight injuries were those
causing absence from 0 days from training and competition as a result of time loss; Minimal
injuries were those causing absence from (1-3 days) from training and competitions; Mild
injuries were those causing absence from (4-7 days) from training and competitions; Moderate
injuries were those causing absence from (8- 28 days) from training and competitions; Severe
injuries were those causing absence > 28 days from training and competitions. In this study
severity of injury was similar classification of in accordance (Bere et al., 2015; Kordi et al.,
2011). Generally, the above authorities tend to agree that injuries should be grouped and that
there is a close alignment with the nature of sport, circumstances and current environment and
situation in which it is being conducted. This, tied together with intrinsic and extrinsic risk
factors, would greatly influence injury mechanism and severity outcomes which a well
informed coach should be aware of so that injury risk during matches and competitions could be
effectively reduced.
2.8. Recurrent injuries
The definition of recurrent injuries includes both the definition of an injury and the definition of
a recurrence (Brooks, Fuller, Kemp, & Reddin, 2006). Recurrent injury can be defined as an
injury of the same type and same site as an index injury occurring after athlete has returned to
full participation from the index injury (Fuller, Bahr, Dick, & Meeuwisse, 2007). Furthermore
recurrent injury can be referred as an „early recurrence‟, „late recurrence‟ or „delayed
Page 36
21
recurrence‟ according to the time recurrence occur after the index injury, which is within 2
months, 12 months or more than 12 months respectively (Fuller et al., 2006). Recurrent injuries
are usually described as acute injuries that occur multiple times; still they sometimes can be
mixed up with chronic overuse injuries.
2.9. Causes of volleyball injuries
The performance of prevention exercises also effects injury prevalence. According to
(Augustsson et al. (2006) and Verhagen et al. (2004), prevention programmes have gained
attention in recent years due to its direct impact in reducing the prevalence of injuries in sports.
The performance of prevention exercises pre-season and during season was higher in the study
of Augustsson et al., (2006). In this study the injury prevalence is higher and the performance of
preventative exercises is lower. Prevention programme supervision can reduce injury
occurrence in cases where the trainer is experienced in sport-specific injuries and have the
knowledge of designing training programmes to achieve high performance and prevent injuries
Kraemer, et al, (2002).
The performance of preventative exercises with supervision (51.75%) in this study was higher
than without supervision (48.25%). It is different from the study by Augustsson et al., (2006),
which shows increased performance without supervision (58%). According to Seminati &
Minetti (2013), proper preventative exercises need enough experience by the coach. Therefore,
performing preventive exercise without supervision is one of the risk factors to the Ethiopian
public Universities Volleyball Players. Results show that the training schedule of the
Universities volleyball club is limited to 2 or 3 times per week for less than 3 hours per session.
In the study by Augustsson et al., (2006) more time was spent on training which enhances the
players experience in performing this kind of exercises, leading to better physical performance
and experience (Kraemer et al., 2002).
The majority of the players (60.53%) made use of technique drill training followed by strength
training incorporated in their prevention programme. Players in the left and right front row were
significantly more prone to be injured during spiking
Page 37
22
2.10. Major Injuries Risk Factors that influencing volleyball sport
In sport, the cause of sports injuries is multi-factorial, involving both intrinsic (player-related)
and extrinsic (environment-related) risk factors related to injuries. Intrinsic factors are Age,
gender, previous injury; body size, muscles strength, and postural stability are some of the
intrinsic factors associated with injuries. Extrinsic factors associated with the injuries are type of
sport, exposure time, and trainees‟ position, level of competition, sport equipment, training
conditions, training technique, and playing surface. Identifying risk factors is a crucial step in
injury prevention.
2.10.1. Intrinsic factors
It is directly related with biomechanics anatomy of an athlete. In further analysis it comprises
Fitness of psychological condition, Age experience training local capacities………
2.10. 1.1. Age
Age has been seen to be a causative risk factor associated with injury prevalence and exposure
time. Together with experience both factors have been reported to increase injury risk. Research
findings by Murphy et al. (2003), and (Verhagen et al., 2004), indicate a degree of relationship
between old age and injury occurrence for lower body appendages as old players have more
exposure hours than young players. To this end, however, risk factor studies have shown the
multiplicity of incongruous results on the effect that age has on injury. Risk of injuries generally
increases with age across most studies when looking at specific sports. Even though some
studies have shown the reverse or not found any association between age and injury. The
association between age and injury prevalence is related to the exposure time. In volleyball, it
seems to be a risk factor for injuries; older athletes have more exposure time in sport (Verhagen
et al., 2004). For younger athletes, exposure time in sport is less; therefore the injuries risks are
decreased. But still findings are different depends on each study conditions.
2.10.1.2. Gender
Some studies showed that females accounts higher injury prevalence in volleyball (Augustsson
et al., 2006; Verhagen et al., 2004). However the relation between sex and injury is still
unclear. Another Study by Seminati & Minetti (2013), have however shown that males accounts
Page 38
23
higher injury prevalence in volleyball. In some cases the high injury prevalence for males are
due to the higher participation among males. Augustsson, et al. (2006), related the gender factor
to the participation rate and the level of competition showing that males are participated more in
training activities than females.
According to Augustsson et al., (2006), found that there is no significant association between
gender and other term such as age and exposure time. To this effect, injury outcome will be
different during play or practice. However, a number of researchers have debated on the
relationship between sex and injury occurrence during training and match situation that are
related to proximal and distal aspects (Bahr and Holme, 2007).
2.10.1.3. Height and weight
Body size used to be measured by height, weight, muscles and fat content in the body. The
relationship between bone tissue, lean muscle, weight, height and fat mass, has received some
attention as a potentially modifiable risk factor on sport injury risk (Emery, 2003). The
relationship between body size and injury is not clear. Some studies showed association
between the body size and injury. For example, in soccer some studies showed increase injury
risk in males with greater height but no association found for females. In running sports speed is
related to Height and weight. In volleyball, the height and weight relation are connected to
jumping and stability. Players with heavier weight are prone to injuries (Wang & Cochrane,
2001). Malliaras et al., (2006), found relationship between players having a waste greater than
83 cm and tendon pattelar pathology. That is due to the mechanical affect in performing
volleyball actions.
2.10.1.4 Previous injury
Previous injury is an intrinsic factor associated with ankle injuries in volleyball. Evidence is
provided in the literature that previous injuries combined with inadequate rehabilitation are risk
factors for re-injury of the same type and location in adults, especially in the ankle. Studies
showed that most of the ankle injuries which occurred is related to players having had previous
ankle injuries (Augustsson et al., 2006; Malliaras, Cook, & Kent, 2006). Recurrences of
previous injury usually happen in volleyball (Bahr & Bahr, 1997). Proper rehabilitation and use
of protective device reduces the possibility of injury recurrence in volleyball. According to
Page 39
24
(Bahr & Bahr, 1997; Nelson et al., 2007) the use of ankle brace and taping reduced the ankle
injuries of the volleyball players in United States of America (USA) and Norway.
2.10.1.5. Level of fitness
High level of fitness is associated with injury prevention (Augusts son et al., 2006). As
mentioned repetitive jumping in volleyball requires high level of fitness. To increase fitness, a
proper training program is required. Coaches used to make use of gradual progressive polymeric
training to increase the player‟s fitness. Increase in duration and intensity in the training
program is recommended. In volleyball, the hamstring & quadriceps muscles are used in
jumping and landing. Therefore, stretching those muscles will help in better performance and
injury reeducation. Injuries in the ankle are related to ankle flexibility. A study by Milliaras et
al., (2006), showed that players with less than 45 degree of ankle flexion are more prone to
patellar tendinopathy. Warm up before exercising increases the blood flow and blood supply to
the tissues.
2.10.1.6. Flexibility
There is a positive relationship between flexibility and health. In sport, flexibility of muscles
and soft tissues around the joint reduces the chance of injuries occurrence, increase range of
motion also decrease the stiffness of muscle and improve the trainees performance (McNair &
Stanley, 1996).Flexibility assessment during exercises and rehabilitation stages is highly
recommended to the volleyball players. Flexibility can be improved or monitored through the
use of stretching exercises. In volleyball, the hamstring & quadriceps muscles are used in
jumping and landing. Therefore, stretching those muscles will help in better performance and
injury reduction. Injuries in the ankle are related to ankle flexibility. A study by Malliaras et al.
(2006), showed that players with less than 45 degree of ankle flexion are more prone to patellar
tendinopathy.
2.10.1.7. Physical problems
Studies assert that physical activity is the most important recreational, preventive remedial
Instrument, which is useful for competitors. The main aim of physical conditioning preparation
Page 40
25
to maintain an athlete present physical conditioning should across though two important
phenomena these are:
The general physical conditioning
The special type of conditioning.
In physical preparation an Athlete to maintain or to improve athletics performance and to avoid
risk of injury should have the quality of speed, strength, skill, mobility and endurance. But the
absence of all the mentioned Athlete quality will lead to a minor or server injury during training
or match condition.
2.10.1.8. Warming up
The importance of proper warming up before any vigorous exercise or competition is highly
recommended by different scholars. Warming up is an important requirement for an effective
Preparedness of the general organic, co-coordinative readiness and psychological readiness. We
can think that if an athlete pass across through the main specific warming up he has a chance of
minimize or avoiding injuries during training or competition condition. Anyone who wants to
engage in any strenuous physical activity is advised to do proper warming up. It is a well-
established fact that considerable amount of warming up enhances the performance and the
result of an athlete and it reduces athletics injuries.
The warm up is through to minimize the risk of in adequate blood flow to the heart and during
the few seconds of heavy exercises because it gives the heart time to adjust from being at rest to
undergoing sudden strenuous activity. Sudden exertion can caused can caused heart attack even
among athletes in good professional positions. An less the heart is given time to warm up the
coronary arteries dilate allowing more blood to flow through them it lead to the heart injuries.
2.10.2. Extrinsic factors
Environmental or Extrinsic related risk factors may be the external conditions that
circumstances, which are natural or manmade it includes different variables such as, in sport
world the type of climate, the playground, sport equipments, spectators, player exposure,
playing and player position, duration in match, coaching-related factors, type of sport, level of
Page 41
26
competition, training conditions, lack of co-ordination, rules and foul play facilities have a great
contribution for the occurrence of injuries in competition and other athletics activities.
Understanding the etiology of risk factors and mechanisms of injuries in volleyball is an
important base of preventive measures.
2.10.2.1. Training methods
Proper methods for trainings are important to avoid injuries. Therefore inadequate warm up can
cause muscles strain and due to the applying an over load stretching on the muscle. Increase in
the load gradually is the proper and safe way to perform it. Prevention program supervision can
reduce injury occurrence in cases where the trainer is experienced in sport-specific injuries and
have the knowledge of designing training program to achieve high performance and prevent
injuries (Kraemer et al., 2002). According to (Augustsson et al., 2006), stated that there is a
need to investigate the effect of supervision and training techniques in the prevention of
volleyball injuries. It‟s important for the coach or players to decide the purpose of the training.
Is it strength training or resistance training. Furthermore, some studies showed a positive
relationship between strength training and jumper‟sknee (Lian, Refsnes, Engebretsen, & Bahr,
2003).
2.10.2.2. Level of competition
According to Augustsson et al. (2006), related the increase of overuse injuries to participation in
other sport activities due to the increase in training hours. On the other hand, there is positive
association between level of training, level of competition and skill level. Furthermore, it‟s
possible that younger players with less period of participation in sport are more prone to
injuries. As (Agel et al., 2007), shows that an increase in the level of participation in volleyball
helps in develop skills of jumping and landing. Agel at al., (2006), showed that there is a need
for players to learn the proper landing techniques to avoid knee flexion and ankle injury.
2.10.2.3. Playing Surface
The type of playing surface is related to safety while playing. Indoor volleyball courts increases
the risk of injury due to hard surfaces, falling or hitting the floor. One of the safety requirements
in playing volleyball is to check the surface. Water or sand on the playing surface may cause
Page 42
27
sliding and falling. On the basis of his research into jumper's knee, Ferretti et al. (1992),
recommends wooden parquet floors or synthetic floors with similar elastic properties to
minimize the risk of jumper's knee in players. Training and playing on hard surfaces such as
concrete should be avoided. It‟s clear that in beach volleyball the nature of the sand prevent the
players from injuries during falling.
A study by Bahr and Reeser (2003), conducted on beach volleyball players and the nature of the
surface in beach volleyball found that more physical strength and more stability is needed by
players than with indoor court surfaces. According to Abdelnour (2008), players who train on
hard surfaces are more prone to jumper‟s knee. According to Smith (2006), the ability to
transfer position during playing is more difficult on the sand as compared to hard court
volleyball. In addition, the vertical jumping requires more energy in beach volleyball and cause
more stress on the back muscles.
2.10.2.4. Player position
In volleyball, there is a relationship between player position and injury occurrence. The player
position is linked to the action that the player will be performing in that specific position.
According to studies by ( Agel et al., 2007; Desalegn et al., 2016; Verhagen et al., 2004),
volleyball players near the net are more prone to injuries than any other position. That is due to
the blocking and spiking that the player performs. According to (Desalegn et al., 2016), 52.94%
of musculoskeletal injuries (MSI) occur in volleyball due to landing and jumping which follows
blocking and spiking. According to Desalegn et al. (2016), found that 47.06% male and 35.71%
female volleyball injuries occur in the right and left front row. In the same study the setter
position accounts for 32.14% male and 17.65% female, 26.47% female and 25% male occur to
players in the back line position. In addition to jumping, spiking requires strong fast shoulder
vertical overhead movements. because of the quick changing situations of attack and defense
injury easily occur (Kumar, 2018).
In spiking, the player used to do different actions such as, jumping in high level above the net
and hit the ball. During that there are different mechanisms occurring in the shoulder, wrist, and
elbow muscles in the upper extremity to hit the ball. For jumping, lower extremity muscles
mainly hamstring and quadriceps take the burden in producing forces. In blocking, the same
Page 43
28
mechanism occurs to the lower extremity. According to Abdelnour (2008), Volleyball players
are distributed on the playground into different positions.
2.10.2.4.1. Centre
The centre is located along the center of the net. His/her main mission is blocking and attacking
the ball. The centre‟s actions require quick movement in blocking and attacking. According to
(Desalegn et al., 2016; Kumar, 2018), 25% male, 26.47% female and 11.23% players
respectively of the MSI occur due to the above-mentioned movements in volleyball.
2.10.2.4.2. Hitter
A hitter is attacking and blocking over the net on the right and left side. A hitter can also receive
the ball. In hitting and blocking, vertical jumping is required, risking the body joints into
injuries. For example, jumping characterized by a quick eccentric action to the musculature
involves the quadriceps. Therefore, injuries on the knee joint are common in this position.
According to Abdelnour (2008), result (51.3%) of the total number of injured players were in
the left and right front row.
2.10.2.4.3. outside player
This outside player is in the back row, where they are normally not involved in the net duels
typically leading to ankle sprains. Also, even if they are not involved in blocking actions by the
net, they had a greater proportion of finger and thumb injuries, which may be explained by a
high frequency of overhand defensive actions in the back row. Outside player displayed a
relatively large proportion of shoulder injuries. This is logical, as they are the main attackers.
The extremely mobile shoulder joint allows hitters to swing high for a spike, which over time
may cause shoulder overuse problems. In addition outside players more prone to finger and
thumb injuries are common (Bere et al., 2015).
2.10.2.4.4 .Setter
The setter usually does not receive the ball but hits the ball after the receiver sets it up in a good
position for the hitter to spike the ball. Setter is the hardest to perfect and get to the highest of
levels because of the most stressful position due to their responsibilities. The setter needs to
Page 44
29
deliver a ball that is expected at the point that the hitter/attacker wants it. According to the
researchers Abdelnour (2008), 12.6% of the players were prone to injuries in the setter position
and the other studies 32.14% for male and 17.6% of female were injuries (Desalegn et al.,
2016).
2.10.2.4.5. Libero
The Libero is the player who is in the back court. The Libero‟s mission is to defend the received
ball from the opposite team and the Libero is not allowed to serve or attack. Liberos, in contrast,
had the lowest injury risk and a lower proportion of ankle sprains than other player functions, a
finding supported by previous studies among club players (Beneka et al., 2009).
2.10.2.5. Athletic Trainer (Sports Therapist)
Athletic trainers work with team physicians, coaches, and other sports professionals to prevent
and treat illness and injuries related to sports and exercise.
2.10.2.6. Biomechanics’/Kinesiology’s
A Biomechanic/Kinesiologist seeks to apply the laws of physics to physical activity, exercise,
and sports. Biomechanics study injury to muscles, bones, and joints under certain conditions.
They analyze body mechanics and attempt to improve athletic performance. Biomechanics are
typically employed in research settings and clinical sites, but future growth appears to be in
industrial ergonomic settings. The minimal requirement is a master‟s degree.
2.10.2.7. Exercise Physiologist
Exercise physiologists study the acute and chronic physiological responses of physical activity.
Their goal is to improve health, fitness, and performance. Traditionally, exercise physiologists
worked only with athletes. However, today‟s exercise physiologists also work in commercial,
clinical, and other professional settings for the general population. At a minimum, an
undergraduate degree is required to be an exercise physiologist. Certification can be obtained
from the American College of Sports Medicine.
Page 45
30
2.10.2.8. Fitness Instructor/Personal Trainer
Fitness instructors, or personal trainers, typically work one-on-one with clients either in the
client‟s home, the trainer‟s office, or a fitness facility. Personal trainers are generally employed
as freelance contractors paid by the hour or per session. It is recommended that a personal
trainer have a strong background in anatomy and kinesiology at a minimum, and preferably an
undergraduate degree in a science-related area. In addition, personal trainers must obtain the
American College of Sports Medicine Certified Personal Trainer certification.
2.10.2.9. Massage Therapist (Therapeutic Massage Therapist)
Massage therapists relieve muscle tension, spasms, inflammation, fluid retention, aches,
stiffness, and pain by applying structured pressure, tension, motion, or vibration to the soft
tissues of the body. Other benefits of massage include improved circulation (blood and lymph),
general flexibility, range of motion, and increased tissue elasticity. Massage can aid in the
healing of injuries by limiting scar formation. On completion of a massage therapy training
program, a massage therapist can seek certification through state examinations. A national
certification examination is offered by the National Certification Board for Therapeutic
Massage and Body Certification. Massage therapists may work as faculty in a sports/
rehabilitation medicine or fitness/spa facility. They commonly act as support for professional
athletes or teams.
2.10.2.10. Sports Medicine Physician/Medical Doctor
Sports medicine physicians are highly trained in the diagnosis and treatment of sports-related
injuries. Most professional teams employ sports medicine physicians, whereas other physicians
are employed by clinics or hospitals. A physician interested in sports medicine normally seeks
specialized training in sports medicine, orthopedics, cardiology, or other areas. Each field has
three to five years of internship and residency training, in addition to one to two more years of
fellowship training.
2.10.2.11. Sport Psychologist
Sport psychologists study the psychological factors associated with participation and
performance in sports, exercise, and other types of physical activity. Specifically, a sport
Page 46
31
psychologist helps athletes use psychological principles to achieve optimal mental health and
athletic performance. In most cases, a college undergraduate degree is the principal requirement
for entry into this profession. In addition to obtaining a degree in psychology, one should
acquire national certification. Strength and Conditioning Coach Strength and conditioning
coaches develop and monitor training plans for athletes. Their goal is to improve and enhance
an athlete‟s power and performance. High school, college, and professional athletic teams often
require the services of strength and conditioning coach.
2.10.2.12. Balanced Competition
In order to reduce the risk of injury, it is important to keep competitions balanced.
Consideration should be given to the age, size, sex, strength and skill of the athletes.
2.10.2.13. Coaches
Coaches are responsible for the design of safe and effective training programs. All coaches
should be educated in the general principles of sport and fitness and understand volleyball and
its potential injury risks. As much as possible, coaches should prevent players from attempting
skill or competition levels for which their maturity, strength or other attributes are insufficient.
A coach should be an educator, psychologist, injury prevention and first aider and provide a role
model for good sportsmanship and fair play (Cassell, 2001). It is important that coaches
undertake regular training to update their knowledge of injury prevention, first aid, and
rehabilitation principles and are kept informed on developments in knowledge about training
players in volleyball skills.
Volleyball coaches should undertake a variety of training at various levels. These range from
the Level 0 coaching course, as a base, to elite level coaching courses provided through
Volleyball Victoria. The intensity and educational expectations increase with the level of the
course. Projects, Clubs and associations should encourage and support coaches to become
accredited and to continuously upgrade their knowledge and skills (Cassell, 2001).
2.10.2.14. Nutrition and hydration
For athletes, nutrition and supplement use is a common way to augment a steady training
program. Arguments that have gone on for years about the best diet for optimal athletic
Page 47
32
performance will likely continue for years, as well. Big questions in sports nutrition are what to
eat and when to eat, as well as eating during training versus eating before competition.
Specifically, they review the current scientific data related to athletes‟ nutrient, energy, and
fluid needs, assessment of body composition, strategies for weight change, the use of
supplements, and nutrition recommendations for vegetarian athletes. See Section Three,
Annotated Primary Source Documents for a reprint of the ADA/CDA position stand on
nutrition for athletes.
Outline
Injuries Are Not an Act of God
Volleyball is recognized as one of the most widely played sports in world level and it is the
sport of choice for many countries. With the increase in the number of people involved in sport
and in the number of people from different countries meeting in sport, sport became a
significant part of the developed countries and communities. It has been recognized as both
recreational and professional sports that have a positive effect of health and social benefits
nature. Whereas Injuries those occur in sport fall into one of two groups: The etiology of sports
injuries is multi-factorial, involving both internal and external risk factors. Internal risk factors
refer internal to the athlete (e.g. age, sex, injury history, biomechanics), whereas external risk
factors act on the athlete from outside (e.g. environment, sports equipment, sports rules). Some
of these risk factors may be modified (e.g. workload, equipment), whereas other are non-
modifiable (e.g. sex, age). Injuries have consequences on sports involvement and performance,
but may also lead to experiencing negative psychological responses (frustration, anger), daily
living activity consequences (sleep disturbances, study issues), as well as feelings of loneliness,
self-blame or self-criticism, high competence-based self-esteem and increase in training load
and training intensity, while at the same time decreasing sleep volume, emerged as risk factors
for injury.
In addition, the increased participation in sports increases the exposure to risk factors associated
with the occurrences of sports injuries. Agel et al., (2007) showed that there is increased injury
prevalence in general, and in volleyball specifically, during games more than during training
sessions. Ankle ligament sprain, knee internal derangement, muscle strains of the shoulder and
Page 48
33
upper leg muscle strains are the most common injury types which occur during games and
training sessions. There is still a lack of information about injuries in volleyball and the
mechanism of injury (Bahr & Bahr, 1997). Better surveillance systems are required in sport to
ascertain information on common injuries like AS (Nelson et al., 2007). As highlighted in this
review of the literature, a fair amount of research on sports injuries in Ethiopia, a study
conducted among volleyball players of public universities reported higher injuries prevalence
among female players than male players. Strain, ankle and finger dislocation injuries were the
most frequent.
Injuries were more frequently occurred during match than during team training. Blocking,
setting, executing wrong technique, and stepping on other‟s foot were the causes of injuries.
Lower and upper extremities injuries were required more time to recover (Desalegn & Zenebe,
2016). Volleyball injury is needs to be directed to injuries occurring as a result of participation
in volleyball. Due to injury, players restricted from participation for one or more days from
training and games, clubs loose points from games. If this problem will not be resolved, the
players can‟t play permanently, will be affect with chronic injury and the clubs will also getting
the least rank with volleyball competition. Considerable researches have been done abroad in
sport injury related to volleyball sport. However as per the knowledge of the researcher there
was no research that conducted in Ethiopia or Wolita Dicha and Medawolabo University to
assess the prevalence and associated factors of volleyball injuries occurred on professional
volleyball players.
Page 49
34
CHAPTER THEER
3. RESEARCH METHODOLOGY
This chapter discusses about methodology utilized in the study and presents the overall research
design, research settings and the study‟s multiple data collection tools used to collect sufficient
data. The chapter included as well, designs, population of the study, sample and, sampling
techniques and, procedures that was used. The data analysis and presentation methods were
presented.
3.1. Study Area
This study was conducted in SNNPR and Oromia regions Wolita Dicha and Madda Walabo
University male premier league clubs respectively. Geographically the study wolita Sodo town
is located 315 km away from the capital city Addis Ababa. With elevation of 1600m to 2100m
above sea level and it has average annual temperature of 200C. Whereas, Madda Walabo
University is located in Bale Zone, Robe town, about 430 km away from Addis Ababa, 17.5oC
average annual temperature, 2492m elevated above sea level. Specifically it is found in Wolaita
1048 km and Medawolabo 1163 km far away from Gondar town in Amhara region of Ethiopia.
3.2. Study Design
To bring the intended result of this study by using relevant design, the researcher will employ a
cross-sectional survey design of the research. According to Bell, (2005), it is more appropriate
for small samples. Both qualitative and quantitative design is most commonly used type in the
non-experimental approach. Therefore, the researcher chose this kind of design to bring about
the desired effect of the study due to the study aim is to know the prevalence of sport injuries
and its associated risk factors. For qualitative, the focus will be in explaining and knowing facts
as is the case in this study, which is the research design chosen to answer the research question.
Looking to the questionnaires, it consists of quantitative variables as the normal situation in the
quantitative design. For this reason the researcher used quantitative and qualitative design to
analyze data which was collected from different informants through questionnaires and
interview.
Page 50
35
3.3. Population of the study
The study population consisted of all volleyball clubs players, 2 physiotherapists and 2 head
coaches of male volleyball clubs found in the selected sampled clubs. This study could include
two Volleyball Club‟s current membership stands at 26 members. The WDC team consists of
13 members. The MWUC team currently registered 13 members. Therefore, all 26volleyball
clubs athletes, 2 physiotherapists and the 2 head coaches, total of all 30 participants from both
clubs were included for this study.
3.4 Sample size and sampling techniques
The 26 players from both clubs were selected by census, the two coaches and the two
physiotherapists (one from each club) were selected by purposive sampling technique.
3.5. Sources of data
Statistical data may be classified into two basic types of data: primary (original) data &
secondary data. Data was gathered from participants that are claiming to have adequate
proximity to the study area. In this study the two clubs participated to gain pertinent information
for the study. The researcher used a primary data type that collects information directly from the
sample (representative of my study population) of respondents. To get primary data the
researcher administered open and close ended questions for clubs players; interview for both
club coaches and physiotherapists. Therefore, coaches, physiotherapists and clubs players were
the primary source of data in this study.
3.5.1. Primary data source; to get primary data the researcher was administer open and close
ended questions for coaches, physiotherapists and clubs players. The questionnaires were
prepared in English and Amharic version. The English version questionnaire was translated in
Amharic language. Moreover, Coaches and physiotherapists are going to be interviewed
regarding the prevalence of sport injury of volleyball players. To triangulate the data obtained
through the questionnaires and interview methods were employed. Generally, coaches,
physiotherapists and clubs players were the primary source of data in this study.
Page 51
36
3.6. Data collection Instruments/Tools
For this study, the researcher was used primary source of data .The primary aim of this study
were find out the prevalence and its associated risk factors of sport injury in the case of
Wolaita Dicha and Medawolabo university male volleyball premier league clubs . It is
best follows the descriptive methods. To collect the desired information or data the researcher
were questionnaires and interview was used as instrument for collecting the required primary
data.
3.6.1. Questionnaire; the survey was probably the best method to collect information from a
group of people, which is too large for direct observation. Surveys are also a great tool to see
the views and attitudes of a numerically large population (Babble, 2006). The questionnaire
provides the researcher with an increased likelihood of boating complete and precise
information [Zikmund, 2003]. The questionnaire will comprise of issues that relate to the basic
questions or emphasis on the prevalence and its associated risk factors of sport injury of
volleyball clubs. A structured questionnaire was used to collect quantitative data through a
census survey involved all target population from the study area. Data was collected on the
demographic characteristics and driving factors by preparing close and open ended items
questions.
3.6.2. Interview; at the beginning of the study, a set of information were prepared to gather
information regarding the baseline data of coaches as well as physiotherapists. Interview was
conducted in a face –to-face means. Semi-structured interview was used in order to strength
and cross check the respondents answers. Based on that, a schedule of the planned interviews
was made containing all the necessary needed information about the interview participants. The
interviews questions were designed to assess the different prevalence and its associated risk
factors that might have an impact on players‟ of sport injury. Within the interviews, open ended
questions were used to gain the needed data. Amharic language and tape recorder/ phone were
used to record the information from the participants
3.7. Data Collection Procedures
This study also all the necessary data was collected above and related points to identify the
prevalence and its associated risk factors on among volleyball clubs players was used the
Page 52
37
following actions. Moreover, information related to the prevalence injuries such as, anatomical
location, cause of injury, playing position at a time of injury, severity and situations related to
the injury occurrence was recorded
First, Permission was also sought from the University of Gondar sport science department. The
researcher announces the consent form for the administrative of youth and sport office and
coaches. The coaches of clubs, physiotherapists and players were informed face to face for the
purpose and procedures of the study. This instrument consists of questions and interview
contained to identify the prevalence and its associated risk factors among volleyball clubs
players. After that all baseline data were collected by distributing a structured questionnaire to
the respondents and interview was provided in order to get additional information from coaches
and physiotherapists. The procedure was performed by the researcher and his colleagues.
3.8. Methods of data analysis (statistical applications)
After Completed data was captured on injury record form, data entered into the Social Sciences
software (SPSS) version 20 in preparation for analysis. Descriptive statistics (frequencies and
percentage) was used to analyze the data. The results are displayed using table and graphs.
Injury prevalence was calculated as the number of injuries reported per number of volleyball
trainees. Variables having p-value of less than 0.05 has been considered as significantly
associated with the dependent variable (Chi-Square Tests).
3.9. Ethical Consideration
The current study was subject to certain ethical issues and approval form has properly addressed
before the study got underway. Written consent was given from University of Gondar sport
science department for ethical approval. Furthermore After having letters of permission the
researcher conducted administrative of youth and sport office, coaches, physiotherapists and
players for their kindly permission. Then after made an agreement with the concerned
participants, the aim of the study was explained to the relevant administrative bodies, coaches,
physiotherapists and the volleyball players. The volleyball players were assured that all the
information collected from the study would be kept confidential and anonymous. The aim of
both letters was to reassure participants that their participation in the research is voluntary and
that they were free to withdraw from it at any point and for any reason.
Page 53
38
CHAPTER FOUR
4. RESULTS AND DISCUSSION
The main aim of this study was to investigate the prevalence of sport injury and its associated
risk factors in the case of Wolaita Dicha and Madda Walabo university male volleyball premier
league clubs. This chapter includes data analysis, presentation, interpretation, results and
discussions of the study data.
4.1 Result
In order to make all the collected data suitable for the analysis, all questionnaires were screened
to be complete. All returned incomplete questionnaires were therefore considered as errors and
removed from the survey data. A total of 26 volleyball players were included in the study.
However, 25 players participated and completed the questionnaire; one player was not volunteer
to responded and participate in questionnaire. Hence, a total of 25 complete questionnaires were
used for this research for data analysis. The questions and possible answers were corresponded
in the order of the actual questionnaire. This represented a response rate of 96.15% which could
be taken as higher response rate. The response rate among the Wolita Dicha club, 100% (13/13)
was higher compared to the Medda Walabo University volleyball players, 92.31% (12/13).
4.1.1 General Characteristics of Respondents
The demographic information‟s of volleyball players are presented in table 2. A total of 25
volleyball players were expected to participate in the study, so all players participated and
completed the questionnaires. From the total players 2 (8%) were; 1.50-1.65m tall were taller
than 1.95 meters. This implies that most players were categorized as 1.86-1.95m body height.
From the total respondents 5 (20%) were married; 19 (76%) were single and 1 (4%) didn‟t
reply. This implies that most of the respondents were single. And 13 (52%) completed
secondary education; 7 (28%) held diploma; 4 (16%) held degree and 1 (4%) was above degree
level. This implies that most of the players completed their secondary education only. In
addition to educational status 10 (40%) had 1-2 years‟ experience; 7 (28%) had 3-4 years; 5
(20%) had 5-6 years; and 3 (12%) players had 7 and more than years of experience in playing
volleyball. In age category of 5 (20%) was in age range of 26-35. This indicates that the players
are in age range of 20 to 35 years of age and 80% most of them were 20 to 25 years of age,
Page 54
39
youth. Were as 1 (4%) were in range of 50-60kg; 12 (48%) were 61-70kg; 7 (28%) were 71-
80kg; and 5 (20%) weighed greater than 81kg. This indicates that most players‟ body weight
was in a range of 61 to 80kg.
4.1.2 Prevalence, sites and situations of injury
A total of 17 injuries were occurred during the season 2019/2020, giving an injury rate of 0.68
Injuries per player. The majority of the volleyball players (68%) were experienced at least one
or more injuries during the season. Eight players (32%) were not injured.
Figure 1. Injury occurred on your body in the last volleyball season up
As figure1 shows 17 (68%) of the respondents replied „yes‟ for occurrence of injury and 8
(32%) replied „no‟. The next back ground information of participants indicates that majority of
the players had experienced with old sport (volleyball) related injury on their body. Therefore,
the maximum of the players were receiving injured with 17(68%), an average form both clubs,
prevalence rate per participant was 0.68.
68%
32%
%
Yes
No
Page 55
40
Table 1 Frequency of injury occurrence
Item
Response
`Alternative Frequency(n) Percent (%)
How many times you’re
injured
No injury 8 32
1-3 11 44
more than 3 6 24
Total 25 100.0
Table1 shows that from total respondents volleyball players experienced one or more injuries
during the season, 11 (44%) were injured 1-3 times; 6 (24%) experienced injure more than 3
times and 8 (32%) didn‟t experience injury volleyball players occurred during the season. This
implies that majority of the injured players experienced injury more than 3 times.
Table 2 Respondent‟s response on injury occurrence related with body part
Item
Response
Body parts injured Frequency(n) Percent (%)
Which part of your body was
injured?
Hand Finger (s) 6 17
Ankle 11 31
Knee 5 14
Thigh 1 3
Leg finger 1 3
Shoulder 6 17
Elbow 2 6
Abrade 3 9
Total 35 100.0
As table2 shows injuries in reference to body parts, ankle injury occurred at the highest rate
31% (11/35), followed by fingers and Shoulder injury 17% (6/35) each, knee injury 14% (5/35),
Abrade 9% (3/35). In addition 12% (4/35) of the injuries were in other body rather than the
Page 56
41
mentioned ones. Generally from the total injury the lower limb injuries located was greater than
the upper limb injuries.
This indicates that, Ankle injury was commonly occurred at the highest charge, Hand Finger
and Shoulder sit almost correspondingly an injured in the volleyball players and more
frequently injured body parts. So that, the prevalence rate per injured players was 2.06.
Figure 2 Situation at which injury occurred.
As the figure above shows that, In this research indicate that the main mechanism that
accounted for the greatest percentage of or 40% of players were injured due to blocking, 28% of
injury happened with spiking, due to serving setting 0% or no one players injured in serving
setting and 16% of players answer the question I do not know and no answer( this both I do not
know and no answer was the same present all of the given answers ) Therefore the maximum
injury occurred by blocking injury was registered and the minimum of in both clubs volleyball
players serving setting injury was registered. (Generally, in this study more injuries were
happened because of blocking the ball).
40%
28%
16%
16%
%
blocking
spiking
I do not know
no answer
Page 57
42
Table 3 Response on injury occurrence during double and triple block.
Item
Response
Alternative Frequency(n) Percent (%)
Does your team have face injury during
double and triple block at the net?
Yes 9 36
Never 9 36
Same times 7 28
No answer 0 0
Total 25 100.0
As shown in table above, according to game have face injury during double and triple block
players jump up together at the net to block were occurred as follows; yes and never injury was
face at the same rate of 36% from total of players, 28%of players same times Face injury during
double and triple block and 0% of players were no answer.
Table 4 Type of injury occurred during double and triple block
Item
Response
Alternative Frequency(n) Percent (%)
If your answer is yes what was
the reason?
Already not jointly
exercitation
4* 16
Inexperience 0 0
Not keep balance 8* 32
All 6 24
No answer 7 28
Total 25 100.0
As shown in table above, according to body parts were occurred injury by what is the reason as
follows; during tiring and much not keep balance injury was occurred at the highest level of
32%, already not jointly exercitation 16% reason injured in the volleyball players,0% of
volleyball players was injure inexperience, 24% of volleyball players was side all and finally no
answer the above reason of volleyball players 28%. Therefore special the maximum injury
reason occurred by not keep balance.
Page 58
43
Figure 3Position at where did you got injured
As the figure above shows that, most of players injuries 48% were occurred on the left/right
front row position, The second highest percentages of injuries occurring among the player‟s
12% were on the Center back or most of a time receiver positions,8% Setter positions of the
court, 8% injuries happened on the positions of right /left front row and final 24% of players
was side no answers. That kind of situation can have an effect on injury occurrence. Generally,
the result shows more injury were occurred when a player playing in the left/right front row
position than other positions.
8%
48%
8%
12%
24%
%
Setter
Left/Right front row
Right/Left front row
Center back
No answers
Page 59
44
Figure 4 At which set did you get injured, when the injury occurred in game?
The above figure4, shows that 28% injured on first and second set, 40 % players injured in the
2nd
and 3rd set, 4% players injured in fourth and fifth set, 12% players injured during warming
up before the game, 0% player injured gradually and lastly 16% of players was respond no
answer. Therefore the maximum of injury were occurred in the 2nd
and 3rd set.
Table 5 . Did you withdraw without completing the training and match play at the time of
injured?
Item
Response
Alternative Frequency(n) Percent (%)
Did you withdraw at the time
of injured
Yes 14 56
No 7 28
No answer 4 16
Total 25 100.0
The table above show that 56% of the injured players were withdraw without completed
training and match, 28% were completed at the time training and match and few and few
28%
40%
4%
12%
0%
16%
%
1st/2nd set
2nd/3rd set
4th/5th set
During warm-up beforetrainingInjury occurredgraduallyNo answer
Page 60
45
between or 16% of players was not remember( no answer). Therefore the maximum of players
not completed training and game .
Table 6 Players played home or away home at most of the time injuries suffered
Item
Response
Alternative Frequency(n) Percent (%)
Most of the time Where played
injuries suffered home or away
home?
Home 21 84
Away home 0 0
No answer 4 16
Total 25 100.0
As the table above shows that, from the total percent‟s of injured players more than 84% of
players were injured in by Owen field, 0% of players injury happened away home were and
16% of players answer the question no answer. Therefore the maximum of player‟s injuries
suffered in home (by Owen field).
Table 7 The foreign court and weather condition the factors of injury that occur frequently
Item
Response
Alternative Frequency(n) Percent (%)
Das the foreign court and weather
condition the factors of injury?
Yes 3 12
Never 11 44
Same times 5 20
No answer 6 24
Total 25 100.0
According to this study 12% of the total players were side yes foreign court & weather
condition the factors of injury, 44 % of players was side never foreign court & weather
condition the factors of injury,20% answer sometimes foreign court & weather condition the
factors of injury to volleyball players and 24% of players were no answer. From this result can
understand the maximum of player were never.
Page 61
46
Table 8 able8. Amount of absent players following to injury from training
Item
Response
Alternative Frequency(n) Percent (%)
Amount of absent on
training following the
injury.
Absence less than 1 week 6 24
Absence 2-4 weeks 7 28
Absence more than4 week 2 8
No absence 6 24
No answer 4 16
Total 25 100.0
The above table shows that, 28% of players were absence 2-4 weeks to injury happened on the
training, the same percent or 24% of the players were not absence and absence less than 1 week
injury followed from the training, 8% of players were absence more than 4 weeks and 16% of
the players was side no answer. Specially, the result shows that more injury absence was
occurred 2-4 weeks.
Figure 5 What are the main causes of volleyball injuries in the players?
56% 24%
0% 4%
16%
%
Fail to do warming up
Unsafe volleyball court
Lack of dressing
Lack of interst
Lack of stretching
Page 62
47
According to the main causes of volleyball injuries in the players the highest 56% of volleyball
injuries fail to do warming up, 24% the a there major cause of volleyball injuries unsafe
volleyball court, according to the players was respond lack of dressing 0%, 4% of players injury
were Lack of interest and the last main cause of volleyball injuries were Lack of stretching are
16% Therefore the maximum injury occurred by unssaffitionte warming up was registered.
Respondent’s response about using kneepad, Supply of water and Amount of training
days & hours (during this season)
According to this study 6(24%) of the total players were used kneepad, 11(44%) were using
sometimes kneepad volleyball players and 8(32%) players were not using kneepad. From this
result can recognize the maximum of player were not used kneepad. Based on the clubs
schedules amount of training days and hours per week, the total exposure days and week to play
volleyball 100% of players were train 5 days per week and was 3 hours per week. The clubs
training days and hours of training per week were similar in the two selected volleyball clubs.
The amount of five days was a training day per week and three hours per day was a period of
training duration. In addition this, 100% were used water during competition & training. For
this result all players were getting satisfactory water.
Figure 6 . By which situation is the injury occurred during training/game
52%
4% 8%
28%
8%
%
Contact with friends
Contact with pole
Fall on ground
Wrong jumping
No answer
Page 63
48
According to the study result 52% of injuries were happened due to contact with friends, 4% of
injuries were happened due to contact with pole, 8 % of injury were occurred fall on ground,
28% of players injury was wrong landing and final 8% of players side no answer. Based on the
above table contact with friends were the highest causative factors for both clubs during the
study period. Generally, the maximum percentages or 54% of injuries were happened because
of contact with friend and wrong landing.
Table 9 What are the natures of injuries occur in male volleyball?
Concerning the severity of injuries, results of this study figuer7, above indicated that the natures
of injuries occur in male volleyball the main causes of volleyball injuries in the highest rate
84%(21/25) of volleyball injuries Sprains, 12%(3/25) of players were Muscle cramp,
additionally in terms of degree of severity 4%(1/25) the a there nature of volleyball injuries
Bone fracture and Muscle split and Bone split according to the players was respond 0%, of
volleyball injuries. The study showed that a significant difference in injury severity between the
two categories. Therefore the maximum natures of injury occurred by Sprains was registered.
0% 0% 4%
84%
12%
%
Muscle split
Bone split
Bone fracture
Sprains
Muscle cramp
Page 64
49
Figure 7 Physiotherapy services get access at the time of injured
Item
Response
Alternative Frequency(n) Percent (%)
Did you get access of physiotherapy
services?
Always 13 52
Sometimes 9 36
Never 3 12
Total 25 100.0
As the above table shows that, answer the questions 52 % of player were always get access of
physiotherapy services at the time of injured, 36 % of player were sometimes get access of
physiotherapy services at the time of injured and the rest 12 % of player were never get access
of physiotherapy services at the time of injured. Therefore the maximum of players were always
or 52% of players get access of physiotherapy services at the time of injured.
In another quotation what was the reason not getting access of physiotherapy services players
said not getting physiotherapy treatments was due to absent of physiotherapist and lack of
financial problem to fulfill the treatment materials.
Respondents’ response on rehabilitation exercise at the period of injured
From the total injured players illustrate that, 88%(22/25) of the injured volleyball players were
doing rehabilitation exercise to recovering by self supporting, 8%(2/25) of volleyball Players
injured also sometimes works recovering self supporting rehabilitation exercises and 4%(1/25)
of Players were no answer. Players also gave responses the questions of what type of exercise
you done. From this 96% of injured players were doing jogging, bicycle, rope jump & strength
exercise pushup, pull-up, box, the rest 4% of the total inured players were not doing instead of
lack of information about the types and necessary of rehabilitation exercises.
Page 65
50
Table 10 Cultural dance and emotional jumping celebration that contribution to injuries
After scoring
Item
Response
Alternative Frequency(n) Percent (%)
Is there contribute cultural dance
and emotional celebration to
injuries?
Yes 8 32
Sometimes 11 44
Never 6 24
No answer 0 0
Total 25 100.0
As the above table shows that “yes”8(32%) of players Cultural dance and emotional jumping
celebration that contribution to injuries, 11(44%) of players were Sometimes, 6(24%) was side
never and 0% of player were no answer cultural dance and emotional jumping celebration that
contribution to injuries. From this result can understand the maximum of player were
Sometimes.
Demographic Characteristics of Coaches and Physiotherapist
4.1.3. General Characteristics of Coaches
The demographic characteristics of coaches that the coaches in both clubs were Male, married;
held degree in their education, and both had FIVB coaching qualification. In addition, the WDC
coach was 47 years old, with 7 years of playing experience and 16 years of coaching
experience. Whereas, the MWUC coach was 63 years old with 5 years of playing and coaching
experience. This indicates that both coaches were qualified and experienced in volleyball sport.
4.1.4. General Characteristics of physiotherapists
Demographic characteristics of physiotherapist that the physiotherapists in both clubs were
male, married and experienced. In addition, the WDC physiotherapist had had more than 29
years of experience as a traditional physiotherapist and. whereas; the MWUC coach had had 5
years‟ experience. This indicates that both coaches were qualified and experienced in volleyball
sport. However both of the didn‟t study and qualify physiotherapeutic science.
Page 66
51
4.1.5. Interview made with coaches and physiotherapists
Coach‟s and physiotherapist services: -The clubs have their own volleyball court in your team?
And Players train & play at safe volleyball court? In addition, did you see injury on your
player‟s competition or training? And Is a clubs having a physiotherapist? As wile as Players
doing rehabilitation Exercises?
In addition to data collected through questionnaire, to get in depth and relevant information
semi-structured interview was conducted to the coaches and physiotherapists in each club.
According to the views of the coaches and physiotherapists, there were sustained injuries in
their team players. Both acute and chronic injuries were observed during match and training.
Physiotherapists further described most frequent and common injuries in volleyball like, sprain
at knee, shoulder, ankle and fingers, dislocation of joints. Least frequently strain of hamstring
and fracture one per year occurred. For those fractures they prescribed referral to hospitals.
Concerning the causes of injury in volleyball the two coaches mentioned: Failure to keep
balance during landing, inharmonious execution during double block, being emotional and
using excessive force, missing the ball during smash, body contact with teammate, and
inadequate warm-up and stretching, Ignoring attention for post-match cooling down exercise
and stretching after matches most of the time the big problems are not done starching exercises
after matches why because of first one the referee after billowing the whistle all spectators
direct inter to field and the second one all players not understand more the uses of starching.
The physiotherapists stressed that some players had played being injured because of intention
for not missing the game, this aggravated the injury. Most of the time winning is their first
temptation and safety of players comes next, so it may make players more susceptible to injury.
All interviewees agreed that unsafe court, age of players, training methodology, life style, and
weather condition were not common causes of injury.
They also said that celebration and dance after scoring a point could prone players to injury but
in such a situation the onset of injury was rare. They also added that Playing courts were
suitable and safe for training and playing; the Ethiopian volleyball federation approved and
accepted the courts. The coaches further replied and supported by physiotherapists idea that
Players were physically fit and not aged, so lack of fitness might not be cause for injury,
however, comparative lack of experience in continental and international matches had put
players to psychological injury instead of physical
Page 67
52
Associations of Injury Occurrence and Different Variables
Table 11 Relation b/n injury occurrence during different skills
Item
Response
Alternative Frequency(n) Percent (%)
Kind of situation players
get injured.
Blocking 10* 40
Spiking 7* 28
serving setting 0 0
I do not know 4 16
No answer 4 16
Total 25 100.0
Chi-Square Tests
Chi-square(X2) Df P-value
Pearson Chi-Square 12.000 9 0.000
A chi-square test was conducted to assess the association between weight of players and type of
situation getting in injury. There was strong evidence of relationships between weight of players
and type of situation getting in injury (chi.sq. =12.0 at df = 9, p-value 0.000). This result
suggests that kind of situation can have an effect on weight of players. Specially, the result
shows more injury were happened when a player playing in blocking than spiking.
Page 68
53
Table 12 Cultural dance and emotional jumping celebration that contribution to injuries after
scoring
Item
Response
Alternative Frequency(n) Percent (%)
Is there contribute cultural dance
and emotional celebration to
injuries?
Yes 8 32
Sometimes 11 44
Never 6 24
No answer 0 0
Total 25 100.0
A chi-square test was conducted to assess the association between cultural dance and emotional
jumping celebration and injury. There was strong evidence of relationships between cultural
dance and emotional jumping celebration and injury occurrence (chi.sq. = 12.00 at df = 9, p-
value 0.000). This result suggests that kind of situation can have an effect on injury Occurrence.
Specially, the result shows more injury were happened when a player playing in sometimes than
yes.
Table 13 Association of injury occurrence with upper or lower extremity
Item
Response
Alternative Frequency(n) Percent (%)
Which anatomy part
commonly/repeatedly offence
injury?
Hand Finger (s) 5* 20
Ankle 11** 44
Knee 3** 12
Shoulder 6 24
Leg finger 0 0
Total 25 100.0
A chi-square test was conducted to assess the association between location extremity (lower or
upper) and injury. There was strong evidence of relationships between location extremity (upper
or lower) and injury occurrence (chi.sq. = 15.00 at df = 12, p-value 0.001). This result suggests
that kind of situation can have an effect on injury Occurrence. Specially, the result shows more
injury were happened when a player playing in upper extremity than lower (lower or upper).
Page 69
54
Table 14 Reason of injury occurrence during double and triple block
Item
Response
Alternative Frequency(n) Percent (%)
What was the risen during double
and triple block face injury
Already not jointly
exercitation
4* 16
Inexperience 0 0
Not keep balance 8* 32
All 6 24
No answer 7 28
Total 25 100.0
A chi-square test was conducted to assess the association between double and triple block
players jump up together and player‟s position of injury. There was strong evidence of
relationships between double and triple block players jump up together and player‟s position of
injury occurrence (chi.sq. =15.000 at df = 12, p-value 0.000). This result suggests that player‟s
position can have an effect on injury occurrence. Specially, the result shows more injuries were
happen the Not keep balance than Already not jointly exercitation.
Table 15 Respondent‟s response a set when injury occurred
Item
Response
Alternative Frequency(n) Percent (%)
Sets of the game when
the injury occurred
1st/ 2nd set 7* 28
2nd 3rd
10 40
4th/5th
1 4
during warm-up before training 3* 12
the injury occurred gradually 0 0
No answer 4 16
Total 25 100.0
Page 70
55
A chi-square test was conducted to assess the associated between game sets and age injury
occurrence. There was an evidence of relation between game sets and age injury occurrence
(chi.sq.= 6.000 at df= 4, p- 0.001). This result suggests that game sets have an effect of injury
occurrence. Especially the result shows more injuries were happen the 2nd 3rd
set than1st/ 2nd
set of the game.
4.2. Discussion
The ultimate aim of the study was to assess the prevalence of injuries experienced by volleyball
players in Wolaita Dicha and Medawolabo University male volleyball clubs that participate in
primer league of Ethiopian. This chapter will show how the objectives of the study have been
achieved and will discuss all the aspects related to the prevalence of the volleyball injuries at the
two Volleyball Clubs as well as the sites and causes of injuries. The chapter will compare the
findings with other studies in the same field. The total response rate in the study was 96.15%
from a sample of 26 players. That was high response rate which supports the validity of the
study even though the small sample size limits the generalization potential of the study.
Whereas the response rate of coaches and physiotherapists was 100%.
4.2.1. To determines the prevalence of sport injuries related with volleyball sport.
The first objective of the study was to determine the prevalence of volleyball injuries
experienced among the two Volleyball club Players in a volleyball season. In volleyball, there
are challenges facing studies in injury prevalence. According to Augustsson et al., (2006), some
players may be absent due to an injury, while others continue with the same injury and others
forget minor injury. According to data analysis and results obtained from respondents were a
total of 17 injuries which was happened on the players from the total participant of 25 players.
In this study, showed that more than half of the participants had sustained volleyball related
injury and the frequency of prevalence of injury in volleyball was 68%, which was 0.68 per
participant and 2.06 per injured player.
The injury incidence of the current study was higher than the study conducted by Bahr & Bahr
(1997), which had an incidence of 1.7 injuries per player. Traditionally, volleyball has been a
safer sport when compared to football, wrestling, gymnastics, and basketball in the high school
population. In a retrospective study, Vanderlei et al. (2013) reported an injury rate of 0.23 per
Page 71
56
participant and 1.19 per injured participant in young volleyball players in Brazil. This finding
was higher than that of a previous study by Augustsson et al., (2006), 52%, Bahr and Reeser,
(2003), 43% of the players experienced one or more injury, but the results of this study was less
than the study of Hassan (2008), he indicates 88.1%, and Abjeie Kumilachew,(2016), 80% of
the volleyball players experienced one or more injuries in the season. This current study finding
showed less injury prevalence than the previous study.
Results of this study showed that most common sustained injuries in volleyball were observed
in lower extremities like, ankle, In addition, shoulder finger and knee injuries took the next rate
in volleyball. This result agrees with Zetou E. et al (2006) that most commonly affected areas
involved talocrural joint, hand, knee, shin and shoulders Volleyball players sustained typical
sport-related injuries: muscles, joints and ligaments injuries, sprains and dislocations as well as
soft tissue bruises. Findings of the study showed that the most frequent injury was on the ankle
followed by shoulder injury and the least frequent injury was back. This current study finding is
consistent with Augustsson et al., (2006) that majority of injuries pertaining to training and
match times, occurred at the ankle, which was similar to the study of.
It is further supported by other studies which report that ankle injuries are the most common
acute injury which occurs in volleyball ((Reeser et al., 2006; Augustsson et al., 2005; Verhagen
et al., 2004). This finding is contrasting with a study by Bahr & Reeser (2003), which found that
most of the injuries with gradual onset occurred in the back. This difference might be due to
population difference that in the previous study the participants were beach volleyball players.
There were a total of 17 volleyball players‟ injuries (68%) which occurred in the season. The
Injury prevalence was higher in the study area. Based on the respondent‟s injury prevalence was
higher in the injuries and the causes of injuries. Because of Fail to do warming up, Unsafe
volleyball court, Lack of interest, Lack of stretching, Already not jointly exercitation, blocking,
spiking and during landing not keep balance techniques.
4.2.2. To identify types and sites of sport injuries among male volleyball players.
Results of this study showed that most common sustained injuries in volleyball were observed
in lower extremities like, ankle, knee. In addition, shoulder and finger injuries took the next rate
in volleyball. This result agrees with Zetou E. et al (2006) that most commonly affected areas
Page 72
57
involved talocrural joint, hand, knee, shin and shoulders Volleyball players sustained typical
sport-related injuries: muscles, joints and ligaments injuries, sprains and dislocations as well as
soft tissue bruises. Findings of the study showed that the most frequent injury was on the ankle
followed by knee injury and the least frequent injury was back. This current study finding is
consistent with Augustsson et al., (2006) that majority of injuries pertaining to training and
match times, occurred at the ankle, which was similar to the study of. It is further supported by
other studies which report that ankle injuries are the most common acute injury which occurs in
volleyball ((Reeser et al., 2006; Augustsson et al., 2005; Verhagen et al., 2004).
This finding is contrasting with a study by Bahr & Reeser (2003), which found that most of the
injuries with gradual onset occurred in the back. This difference might be due to population
difference that in the previous study the participants were beach volleyball players. In this
study, results showed that most of volleyball players experience ankle, shoulder and finger
sprains. Acute ankle sprain was the most common encountered injury. Contact with another
player or contact with the floor was the main cause of injury (Angel J, 2007). Some others
encounter muscle cramps and shoulder joint dislocation; other types of injuries were not
common in volleyball.
4.2.3. To identify the major factors associated with the injuries sustained among the
players in a volleyball season.
The third research question of the study was to identify the intrinsic and extrinsic factors
associated with the injuries the research revealed various factors as a cause of injuries related to
volleyball. Failure to keep balance during landing, inharmonious execution during double block,
being emotional and using excessive force, missing the ball during smash, body contact with
teammate, and inadequate warm-up and stretching, Ignoring attention for post-match cooling
down exercise and stretching after matches. Among these, inadequate warm-up and poor
execution of techniques, contact with other player were common ones. The result is also similar
to to Agel et al., (2007), injuries in volleyball occur by contact with player, The study also
revealed that it was during block that most of injuries occurred and the next vulnerable situation
for onset of sport injuries was spiking. It coincides with Elżbieta (2005) research involving Plus
League volleyball players‟ revealed significant correlation between the average rate of
Page 73
58
block/attack jump reach and the occurrence of sport-specific injuries. The players who sustained
sport injuries were characterized by higher parameters of block and attack jump.
Results of current study clearly showed in terms of position that left/right front position players
got most of injuries followed by the center back. The front row positions (outside hitter, middle
blocker, opposite hitter) were injured more often than the back row (libero, setter) or players
that played both positions. In terms of position played in the court, (Angel J, 2007) reported that
front row players suffered more injuries. There is not a significant association of player position
and increase number of injuries, although most acute injuries occur during net play and a large
number of our subjects had been playing a specific position from early in their careers. Early
court position specialization may lead to an increase risk of acute injury as well as long term
increase risk of overuse injury (DiFiori JP, 2014).
Generally, the result shows more injury were occurred when a player Playing in the left and
right front row positions of court because of players wants to cover all spaces and repetitive
actions and dual purposes on the front row players. Augustsson et al., (2006), expressed their
concern that an increase in the ratio of injury among volleyball players might be attributed to an
increase in frequency, intensity and duration of the injury, which lead to a need to increase the
prevalence of treatments. Early physiotherapy intervention helps in reducing and preventing the
injury recurrence because physiotherapy provides treatment to achieve soft tissue damage
rehabilitation. Better injury mechanism examination help in develop injury prevention program.
Page 74
59
CHAPTER FIVE
5. SUMMARY, CONCLUSION AND RECOMMENDATIONS
This Chapter provides an epigrammatic summary of the major issues established in the study.
The Chapter ends by making some realistic suggestions and recommendations. In addition,
major issues to be addressed in future research in volleyball.
5.1 Summary
The aim of this study was to determine the prevalence of volleyball injuries sustained on
volleyball players that participate in training period & mach, the study focus on to identify the
causes, anatomical sites, mechanisms, severity and that were commonly lying on your front to
injury during volleyball activities. The study also put out to recognize position of players and
situations at a time of injury prevalence. It was dissimilar factors recorded by the investigator
watching needs for fulfillment in the clubs.
To reach the mentioned plan the following research questions were developed:
What is the prevalence of sport injuries that occurred in male volleyball players?
What are the major types of sport injury and which part of the players‟ body most
frequently affected?
What are the major factors associated with the volleyball injuries sustained among the
players?
To investigator this study old data obtained through the questionnaires and interview methods
tape recorder/phone were used to record the information from the informants. Taken as a
whole, respective study result also showed that the prevalence of injury was highly affected
anatomical location among the injured players were the ankle, shoulder, hand fingers and knee.
According to the results; it is experimental that ankle, shoulder, hand fingers and knee injuries
are the common anatomical location with the highest prevalence of injuries nonstop in
volleyball players in both volleyball clubs. All the above injuries take place during any
volleyball tearing and mach‟s.
Page 75
60
Thus injuries were result from Fail to do warming up, contact with friend, wrong jumping,
unsafe volleyball court, Lack of stretching, fall on ground, contact with pole and lack of
interest.
The most common injury position in volleyball was the front row position. In addition, the
study showed that the most applicable instrument to injury in volleyball is blocking and spiking.
The study concluded that slight severity of injuries was more experience on volleyball players.
Finally, the study showed that all players have gotten physiotherapy service, enough water
supply and sport facility in all volleyball activities. (In training & games). And both clubs have
standard playground or field certified by Ethiopia Volley ball Federation as convenient for
playing and training.
5.2 Conclusion
Sport injury occurrence is an evitable episode sport training and as well as in competition. In at
hand study the injury occurrence linked with training and game was assessed. The study also set
out to identify the intrinsic and extrinsic factors associated with the injuries experienced among
the players in a volleyball season. Based on the results obtained and discussion made, the
following conclusions were drawn:
In objective the overall injury prevalence rates during volleyball training and competition in
both clubs was found high 68% and injury incidence was 2.06 injuries per one player per
season.
Among different causes for injury in training and competition of volleyball, inadequate
warm-up and stretching, poor execution of techniques, and contact with other player were
common ones.
The most common sustained injuries in volleyball players were observed in lower
extremities of the body like, ankle and knee; in addition, shoulder and finger injuries took
the next rate.
Result of this current study also showed that Sprain, joint dislocation and muscle cramps
were most frequently occurring types of injuries in volleyball players.
In terms of playing position on the court, the left and right front row players were most
vulnerable and injured frequently.
Page 76
61
From the different situations and actions that may contribute to injury, blocking and spiking
were the highest.
During volleyball match, injury occurs almost in all sets, but in the 4th and 5th sets least
injury occurred; following injuries majority of the injured players withdrew from the match.
Majority of injured players had missed training sessions for some days to four weeks
When got injured during training and match, players had always got access for
physiotherapy service and most of them had done therapeutic exercises.
5.3 Recommendations
Based on the result and conclusions of the study, the following recommendations are
forwarded: All the prevalence injuries and their causes have been recorded & mentioned. By
considering the major findings and conclusions of the study, it is important to state the
following points as a recommendation and to investigate more the researcher raises some
crucial points to the issue of sport injury prevalence among volleyball clubs players.
5.3.1 Recommendations for solution
5.3.1.1. To Coach
In the present study ankle shoulder and finger injuries were identified as the most occurred
injuries. Wrong landing (not keeping balance) have face injury during double and triple
block was identified as the cause of the injury. Literature shows that wrong landing, contact
with friends and fall on ground respectively were the cause of injury. If the players instruct
properly how to land, how to limit the load and how to correctly ground on floor the
occurrence of injury will be minimized. Therefore I recommend the coach to give the
correct landing skill, load limit, the way how to ground to prevent wrist injuries and correct
landing technique (keeping balance) to the players so that the occurrence of injury during
training and competitions will be lessened.
In the preset study the players were not exposed to well prepare warming up and starching
exercises. Literatures show warming up and starching exercises are one of the injury
preventing mechanisms to the players. If the players exposed for well-prepared warming up
and starching exercise that based on the daily training objectives the occurrence of injury
will be decrease. Therefore I recommend the coach to let the players exposed for well-
Page 77
62
prepared warming up and starching exercises before they enter to the main part and after
training and competition.
The location of injury and causative factors were identified according to players function
and their mechanisms. Based on this result I recommend coaches‟ preventive measure
should be focused on ankle, shoulder and hand finger injuries. And Coaches should give
prior safety attention for their players rather than won (CUP) intention the match.
The injured all sites, causes and prevalence‟s of volleyball injuries were not documented in
the clubs due to these players can‟t know and supervision the frequency of injured body part
and causes. Therefore, I would recommend Medical teams, couches and others recording the
players injured anatomy sites (body part), causes and prevalence‟s. Why because, accessible
to all athletes at each National Sports, are warranted to reduce the unhealthy behavior,
injury risk and help athletes return to sports safely following injury. These medical teams
should be aware of the multiple consequences of injury in adolescent elite athletes.
The outcomes of this study must be made available to government, coaches, managers,
stakeholders and players in the form of seminars or workshops. And for national federation
of volleyball why because of >60% of players selected for national team. So the
government and other stakeholders should actively participate in the sector or clubs.
For injury prevention and management team approach is required, Awareness programs
about physiotherapeutic intervention in volleyball injuries are required for the coaches,
physiotherapists and players. Offering scientific and significant help and treatment is
fundamental for effective prevention and management of injury; hence, the clubs should
include qualified and professional physiotherapists in their group.( thus the volleyball clubs
should have medical team).
5.3.1.2. To clubs players
In the preset study observation result the players always not work convincing warming up
and at the end stretching exercise. Literatures show warming up and stretching exercises
have its own physiological importance to minimize injury occurrence. If the players did
warming up and stretching exercise that based on their daily training objectives the
occurrence of injury to them will be decrease. Therefore I recommend the players to start
Page 78
63
their daily training and competition after and before doing warming up and stretching
exercise that prepare themselves to the next activities.
In this study Wrong landing (not keeping balance) have face injury during double and triple
block was identified as the cause of the injury. Literature shows that wrong landing, contact
with friends and fall on ground respectively were the cause of injury. If the players instruct
properly how to land, how to limit the load and how to correctly ground on floor the
occurrence of injury will be minimized. Therefore I recommend the players to give the
correct landing skill work with yours teammates jointly training (exercitation) in different
time to skill keeping balance during training (before competitions) to deduced injury.
5.3.1.3. Recommendations for future researchers
This study conducted with cross-sectional survey, but other researchers would study with
longitudinal design to determine if changes over time become perceptible.
Finally, the researcher would like to recommend further studies, Other researcher may
conduct a study in individuals or groups to carry out deeper and wider research work on
similar issue in females‟ population and in other levels of volleyball leagues in the country;
I recommend to use large sample size and in year duration so that better result will be
reported.
Generally, Injuries Are Not an Act of God the impact of this problem may lead male athlete‟s
fails to make part in any training and competition at same time this raped dependent of injury
may have serious impact on male athlete‟s life and their athletic career in particular that means
no body benefited from athletes injure. Therefore, keeping in mind researcher design to pursue
his studies.
Page 79
64
REFERENCE
Aagaard, H., &Scavenius, U. (1996).Injuries in elite volleyball.Scandinavian Journal of
Medicine and Science in Sports, 6(4):228-32.
Abdelnour, H. (2008). Prevalence and pattern of injuries among players at the university of the
Western Cape volleyball club.
Abeje, k., Alemayehu, B., & Ephrem, T. (2016). Prevalence and its associated risk factors of
sport injury in the case of male Volleyball premier League clubs residing in Amhara
Region.
Agel, J., Palmieri-Smith, R. M., Dick, R., Wojtys, E. M., & Marshall, S. W. (2007). Descriptive
epidemiology of collegiate women's volleyball injuries: National Collegiate Athletic
Association Injury Surveillance System, 1988–1989 through 2003–2004. Journal of
athletic training, 42(2), 295.
Augustsson, S., Augustsson, J., Thomee, R., & Svantesson, U. (2006). Injuries and preventive
actions in elite Swedish volleyball. Scandinavian journal of medicine & science in
sports, 16(6), 433-440.
Augustsson, S., Augustsson, J., Thomee, R., &Svantesson, U. (2006).Injuries and preventive
action in elite Swedish volleyball.Scandinavian Journal of Medicine and Science in
Sports, 16:433-440.
Augustsson, S., Augustsson, J., Thomee, R., and Svantesson, U. (2005), Injuries and preventive
action in elite Swedish volleyball. “Scandinavian Journal Medicine and Science in
Sports”, 16: 433-440.
Babble E. (2006). Practice of Social Research (11th edition), Cengage Learning.
Bahr, R., & Bahr, I. (1997). Incidence of acute volleyball injuries: a prospective cohort study of
injury mechanisms and risk factors. Scandinavian journal of medicine & science in
sports, 7(3), 166-171.
Bahr, R., & Krosshaug, T. (2005). Understanding injury mechanisms: a key component of
preventing injuries in sport. British journal of sports medicine, 39(6), 324-329.
Page 80
65
Bahr, R., & Reeser, J. (2003). Federation Internationale de Volleyball. Injuries among world-
class professional beach volleyball players. The Federation Internationale de Volleyball
beach volleyball injury study. Am J Sports Med, 31(1), 119-125.
Bahr, R., & Reeser, J. C. (2003). Injuries among world-class professional beach volleyball
players: Federation Internationale de Volleyball beach volleyball injury study. The
American journal of sports medicine, 31(1), 119-125.
Bailasha, N., & Rintaugu, E. (2007). Etiological factors, pattern and time of injury during inter-
collegiate soccer competition. Paper presented at the joint congress 2007 seagames and
ASEAN paragames scientific congress and the 5th Bangkok ASPASP international
congress on sports psychology.
Belay, A., Tami rat, E., & Science, C. (2016). Nature and Science 2016; 14(9)
http://www.sciencepub.net/nature, 14(9), 51–63.
Beneka, A., Malliou, P., Gioftsidou, A., Tsigganos, G., Zetou, H., & Godolias, G. (2009). Injury
incidence rate, severity and diagnosis in male volleyball players. Sport Sciences for
Health, 5(3), 93-99.
Bere, T., Kruczynski, J., Veintimilla, N., Hamu, Y., & Bahr, R. (2015). Injury risk is low among
world-class volleyball players: 4-year data from the FIVB Injury Surveillance System.
Br J Sports Med, 49(17), 1132-1137.
Brooks, J. H., & Fuller, C. W. (2006). The influence of methodological issues on the results and
conclusions from epidemiological studies of sports injuries. Sports medicine, 36(6), 459-
Brooks, J. H., Fuller, C. W., Kemp, S. P., & Reddin, D. B. (2006). Incidence, risk, and
prevention of hamstring muscle injuries in professional rugby union. The American
journal of sports medicine, 34(8), 1297-1306.
Buchheit, M. (2013). Should we be Recommending Repeated Sprints to Improve Repeated-
Sprint Performance? “Sports Medicine”, 42: 169-172.
Caine, D., Caine, C., & Lindner, K. (1996). Epidemiology of Sports Injuries: Champaign IL:
Human Kinetics.
Caine, e. a. (1996). Epidemiology of Sports Injuries: Champaign IL: Human Kinetics.
Page 81
66
Cassell, E. (2001). Spiking injuries out of volleyball: a review of injury countermeasures:
Monash University Accident Research Centre.
Clarsen, B. (2015). Overuse injuries in sport: development, validation and application of a new
surveillance method.
Desalegn, E. T., Zenebe, M. D., & Wusen, M. E. (2016). Prevalence of volleyball-related
musculoskeletal injuries among university players:A search for Ethiopian public
universities. International Journal of Physical Education, Sports and Health, 3(3), 608-
Eerkes, D. (2012). Academic integrity handbook for instructors and teaching assistants:
Edmonton, AB: University of Alberta.
Eerkes, K. (2012). Volleyball injuries. Current sports medicine reports, 11(5), 251-256.
Emery, C. A. (2003). Risk factors for injury in child and adolescent sport: a systematic review
of the literature. Clinical Journal of Sport Medicine, 13(4), 256-268.
Eygendaal, D., & Safran, M. (2006).Postero-medial elbow problems in the adult athlete.
Fattahi, A., Sadeghi, H., & Ameli, M. (2011). Relationship between injury types and
prevalence with some anthropometric properties of male elite volleyball players of Iran.
World Applied Sciences Journal, 15(5), 667-672.
Ferretti, A., Papandrea, P., Conteduca, F., & Mariani, P. P. (1992). Knee ligament injuries in
volleyball players. The American journal of sports medicine, 20(2), 203-207.
Frisch, A., Seil, R., Urhausen, A., Croisier, J., Lair, M. & Theisen, D. (2009). Analysis of
sexspecific injury patterns and risk factors in young high level athletes. Scandinavian
journal of medicine & science in sports, 19(6), 834-841.
Frontera, W. R. (2003). Rehabilitation of sports injuries: scientific basis: Wiley Online Library.
Fuller, C. (2010). Injury definitions. Sports injury research, 43-53.
Fuller, C. W., Bahr, R., Dick, R. W., & Meeuwisse, W. H. (2007). A framework for recording
recurrences, reinjuries, and exacerbations in injury surveillance. Clinical Journal of
Sport Medicine, 17(3), 197-200.
Page 82
67
Fuller, C. W., Ekstrand, J., Junge, A., Andersen, T. E., Bahr, R., Dvorak, J., . . . Meeuwisse, W.
H. (2006). Consensus statement on injury definitions and data collection procedures in
studies of football (soccer) injuries. Scandinavian journal of medicine & science in
sports, 16(2), 83-92.
Gisslen, K., Gyulai, C., Soderman, K., & Alfredson, H. (2005). High prevalence of jumper‟s
knee and sonographic changes in Swedish elite junior volleyball players compared to
matched controls. British Journal of Sports Medicine, 39(5): 298-301.
Hassan, B., Student, A., & Cape, W. (2008). Prevalence and pattern of injuries among players at
the University of the Western cape Volleyball, (November).
Hawkins, R. D., & Fuller, C. W. (1998). An examination of the frequency and severity of
injuries and incidents at three levels of professional football. British journal of sports
medicine, 32(4), 326-332.
Hawkins D, Metheny J. Overuse injuries in youth sports: biomechanical considerations.
Medicine & Science in Sports & Exercise. 2001; 33(10):1701-7.
Hughes, G., & Watkins, J. (2008). Lower limb coordination and stiffness during landing from
volleyball block jumps. Research in Sports Medicine, 16(2), 138-154.
Hyde, E., & Gengenbach, S. (2007). Conservative Management of Sports Injuries. Toronto:
Jones & Bartlett Publishers.
Jacobson, R. P., & Benson, C. J. (2001). Amateur volleyball attackers competing despite
shoulder pain: analysis of play habits, anthropometric data, and specific pathologies.
Physical Therapy in Sport, 2(3), 112-122.
Jibuike, O., Paul-Taylor, G., Maulvi, S., Richmond, P., & Fairclough, J. (2003). Management of
soft tissue knee injuries in an accident and emergency department: the effect of the
introduction of a physiotherapy practitioner. Emergency Medicine Journal, 20(1), 37-39.
Jimenez-Olmedo JM, Penichet-Tomás A. Injuries and pathologies in beach volleyball players:
A systematic review. 2015.
Page 83
68
Junge, A., Engebretsen, L., Alonso, J. M., Renström, P., Mountjoy, M., Aubry, M., & Dvorak,
J. (2008). Injury surveillance in multi-sport events: the International Olympic
Committee approach. British journal of sports medicine, 42(6), 413-421.
Kordi, R., Hemmati, F., Heidarian, H., & Ziaee, V. (2011). Comparison of the incidence, nature
and cause of injuries sustained on dirt field and artificial turf field by amateur football
players. Sports Medicine, Arthroscopy, Rehabilitation, Therapy & Technology, 3(1), 3.
Kraemer, J., Adams, K., Cafarelli, E., Dudley, G., Dooly, C., Feigenbaum, M., Fleck, J.,
Francklin, B., Fry, C., Hoffman, R., Newton, U., Potteiger, J., Stone, H., Ratamess, A.,
& Triplett-McBride, T. (2002). American College of Sport Medicine Position Stand.
MedicalScience and Sports Exercise, 34: 364-380.
KUMAR, K. S. (2018). A RETROSPECTIVE STUDY OF INJURIES PREVALENCE IN
COMPETITIVE VOLLEYBALL PLAYERS.
Lian. O., Refsnes, P., Engebretsen, L., Bahr, R. (2003). Performance characteristics of Injuries
and preventive actions in elite Swedish volleyball players with patellar tendinopathy.
American Journal of Sports Medicine, 31: 408–413.
Luig, P. and Henke, T. (2010). “Preventing injuries in volleydball: Safety in sports”. EU
sponsored project (2003-2008). Germany. Arag Sports Insurance.
Malliaras, P., Cook, J. L., & Kent, P. (2006). Reduced ankle dorsiflexion range may increase
the risk of patellar tendon injury among volleyball players. Journal of science and
medicine in sport, 9(4), 304-309.
Masumura, M., Marquez, W. Q., Koyama, H., & Michiyoshi, A. (2007). A BIOMECHANICAL
ANALYSIS OF SERVE MOTION FOR EL TE MALE VOLLEYBALL PLAYERS IN
OFFICIAL GAMES. Journal of Biomechanics, 40, S744.
McBain, K., Shrier, I., Shultz, R., Meeuwisse, W. H., Klügl, M., Garza, D., & Matheson, G. O.
(2012a). Prevention of sport injury II: a systematic review of clinical science research.
Br J Sports Med, 46(3), 174-179.
McBain, K., Shrier, I., Shultz, R., Meeuwisse, W. H., Klügl, M., Garza, D., & Matheson, G. O.
(2012b). Prevention of sports injury I: a systematic review of applied biomechanics and
physiology outcomes research. Br J Sports Med, 46(3), 169-173.
Page 84
69
McNair, P. J., & Stanley, S. N. (1996). Effect of passive stretching and jogging on the series
elastic muscle stiffness and range of motion of the ankle joint. British journal of sports
medicine, 30(4), 313-317.
Milliaras, P & Kent, P. (2006). Reduced ankle dorsiflexion range may increase the risk of
patellar tendon injury among volleyball players. Journal of Science and Medicine in
Sport, 9: 304-309.
Miranda, G. E., Mas, M., Lopez, D., Perez, C., & Micheo, W. (2015). Epidemiology of
Volleyball Related Injuries in the Young Athlete ClinMed, 1–3.
Mjaanes, J., & Briner, W. (2005). Trends in shoulder injuries among elite volleyball players in
the USA. Br J Sports Med, 39(6), 373-408.
Murphy, D. F., Connolly, D.A. and Beynon, B.D. (2003). Risk factors for lower extremity
injury: a review of the literature. “British Journal Sport Medicine”, 37: 13-29.
Nelson, A. J., Collins, C. L., Yard, E. E., Fields, S. K., & Comstock, R. D. (2007). Ankle
injuries among United States high school sports athletes, 2005–2006. Journal of athletic
training, 42(3), 381.
Olsen, O., Myklebust, G., Engebretsen, L., Holme, I., & Bahr, R. (2003). Relationship between
floor type and risk of ACL injury in team handball. Scandinavian journal of medicine &
science in sports, 13(5), 299-304.
Orchard, J., & Seward, H. (2002). Epidemiology of injuries in the Australian Football League,
seasons 1997–2000. British journal of sports medicine, 36(1), 39-44.
Ozbek, A., Bamac, B., Budak, F., Yenigun, N., & Colak, T. (2006). Nerve conduction study of
ulnar nerve in volleyball players. Scandinavian Journal of Medicine and Science in
Sport, 16(3): 197-200.
Parkkari, J., Kujala, U. M., & Kannus, P. (2001). Is it possible to prevent sports injuries? Sports
medicine, 31(14), 985-995.
Plisky, P. J., Rauh, M. J., Kaminski, T. W., & Underwood, F. B. (2006). Star Excursion Balance
Test as a predictor of lower extremity injury in high school basketball players. Journal of
Orthopaedic & Sports Physical Therapy, 36(12), 911-919.
Page 85
70
Reeser, J. C., Joy, E. A., Porucznik, C. A., Berg, R. L., Colliver, E. B., & Willick, S. E. (2010).
Risk factors for volleyball-related shoulder pain and dysfunction. Pm&r, 2(1), 27-36.
Reeser, J. C., Verhagen, E., Briner, W. W., Askeland, T., & Bahr, R. (2006). Strategies for the
prevention of volleyball related injuries. British journal of sports medicine, 40(7), 594-
600.
Salci, Y., Kentel, B., Heycan, C., & Akin, S. (2004). Comparison of landing maneuvers
between male and female college volleyball players. Clinical biomechanics, 19(6): 622-
628.
Seminati, E., & Minetti, A. E. (2013). Overuse in volleyball training/practice: A review on
shoulder and spine-related injuries. European journal of sport science, 13(6), 732-743.
Seminati, E., & Minetti, A. E. (2013). European Journal of Sport Science Overuse in volleyball
training / practice : A review on shoulder and spine-related injuries, (November).
Smith, R. (2006). Movement in the sand: Training implications for beach volleyball. Strength
and Conditioning Journal, 28(5), 19.
Sole, C., Kavanaugh, A., & Stone, M. (2017). Injuries in Collegiate Women‟s Volleyball: A
Four-Year Retrospective Analysis. Sports, 5(2), 26.
Solgård, L., Nielsen, A. B., Møller-Madsen, B., Jacobsen, B. W., Yde, J., & Jensen, J. (1995).
Volleyball injuries presenting in casualty: a prospective study. British journal of sports
medicine, 29(3), 200-204.
Stasinopoulos, D. (2004). Comparison of three preventive methods in order to reduce the
incidence of ankle inversion sprains among female volleyball players. British journal of
sports medicine, 38(2), 182-185.
Suda, E., Amorim, C., Sacco, I. (2007). Influence of ankle functional instability on the
ankleelectromyography during landing after volleyball blocking. Journal of
Electromyography andKinesiology, doi:10.1016/j.jelekin.2007.10.007
Svantesson, U. (2006). Injuries and preventive actions in elite Swedish volleyball ´ 2 , 433–440.
Page 86
71
Van den Tillar, R., and Marques, M. C. (2013). Effect of different training workload on
overhead throwing performance with different weighted balls. “Journal of Strength and
Conditioning Research”, 27: 1196-1201.
Van Mechelen, W., Hlobil, H., & Kemper, H. C. (1992). Incidence, severity, aetiology and
prevention of sports injuries. Sports medicine, 14(2), 82-99.
Verhagen, E., Van der Beek, A. J., Bouter, L. M., Bahr, R., & Van Mechelen, W. (2004). A one
season prospective cohort study of volleyball injuries. British journal of sports medicine,
38(4), 477-481.
Wang, H., & Cochrane, T. (2001). A descriptive epidemiological study of shoulder injury in top
level English male volleyball players. International journal of sports medicine, 22(02),
159-163.
Zetou E, Malliou P, Lola A, Tsigganos G, Godolias G. Factors related to the incidence of
injuries‟ appearance to volleyball players. J Back Musculoskeletal Reh 2006;19:129-34.
Zikmund,W.G(2003). Business research methods (7th edition), Masson, Ohio: Thompson.
Page 87
72
APPENDIX
UNIVERSITY OF GONDAR
COLLEGE OF NATURAL AND COMPUTITIONA SCIENCE
DEPARTMENT OF SPORTS SCIENCE
This is the Questionnaire prepared to collect relevant data from volleyball players,
physiotherapists and coaches concerning “Prevalence of Sport Injury and its Associated
Risk factors in the case of Wolaita Dicha and Medawolabo University male volleyball
premier league clubs.”
Dear Players,
This questionnaire is designed to collect desired information for research purpose only. As
mentioned above its objective is to investigate the ” prevalence of sport injury and its
associated risk factors in the case of Wolaita Dicha and Medawolabo University male
volleyball premier league clubs”.
This data, after effective collection, will help the researcher to make pertinent analysis which
indicates the source of the problem understudy so as to make awareness on stakeholders and
victims of the volleyball injuries. Therefore, you are highly esteemed respondent extremely
important for the purpose of the study and to give genuine data for this study. Your response
will be kept strictly confidential. Thus, I would politely request you to read the questions
carefully and respond to each question appropriately. You do not write your name. Your
participation will be helpful in producing useful results. Finally, thank you very much in
advance for your humble participation in this research.
Prepped by: Tatek Girma
Advisor: DrAlemayehu Belay (Associat professor)
. March. 2012 E.C
Gondar Ethiopia
Page 88
73
Direction 1. Please read each of the following questions and circle or write your responses
on the space provided.
Appendix A: Socio-demographic related questions for PLAYERS in English
Name of your club ________________________ No Questions Responses
1 Gender 1. Male
2 Age 1.20-25 Years 2. 25-30 3. 31-35 4. 36-40 5. >40
3 Height 1. 1.50-1.6 2.1.66-1.75 3.1.75-1.85 4. >1.85
4 Weight 1.50-60 2.61-70 3.71-80 4.>81
5 Marital status 1 single 2 marriage 3. divorce
6 Level of Education 1. Diploma 2.Bachelor 3.Master 4. Certificate(10/12)
7 Playing Experience 1. 1 Years 2. 2 Years 3. 3 Years 4. >4 years
8 Level of Certification 1. National 2. FIV
1. What are the natures of injuries occur in male volleyball players?
A. Muscle split B. Bone split C. Bone fracture D. Sprains E. Muscle cramp
2. Have you ever got injured during volleyball seasons up to know? A. Yes B. No
3. If your answer is yes for question number two how many times you got injured? -------------Is
it acute or Chronic?
4. Which part of your body was frequently injured? (More than answer is possible)
1. Abrasion 5. chest 9. knee 13. foot
2. Finger (s) 6. back 10. hip 14. lower leg
3. Hand 7. groin 11. thigh 15. ankle
4. Elbow 8. shoulder 1.2 wrist
If any please specify_________________________________
5. At what kind of situation did you get injured?
A. blocking B. spiking C. serving setting D. do not know E. other (specify) ------
6. What player position did you have when you got injured?
Page 89
74
A/ setter B/ left/right front row C/ left/right back row D/ receiver E/ other (specify) --
7. At which point did you get injured, when the injury occurred in game?
A/ 1st/ 2
nd set B. 2
nd /3
rd set C/ 4
th /5
th D/ during warm-up before match E/ the
injury occurred gradually F/ No answers
8. Did you complete the training match play at the time of injured? A/ yes B/ no
9. How many times per week do you train volleyball (during this season)? ____________
10. How many hours per week do you train volleyball (during this season)? _____________
11. What was the amount of absence from subsequent training session (s) following the injury?
A/ absence less than 1 week B/ absence 2-4 weeks
C/ absence more than 4 weeks D/ no absence
Part 3 questionnaires that will assess causes of injuries
1. What are the main causes of volleyball injuries in the players? A. Fail to do warming up
B. Unsafe volleyball court C. Lack of dressing D. Lack of interest E. Lack of stretching
2. Do you use kneepad during training and playing? A. Yes B. No C. Sometimes
3. Is supply of water during training and competition? A. Yes B. Sometimes C. No
4. By which situation is the injury occurred during training game
A. Contact with friends B. Contact with pole C. Fall on ground
D. wrong jumping E. contact with opponent players F. No answer
5. Does your team have face injury during double and triple block players jump up together at
the net to block? A. Yes B. Never C. Same times D. No answer
6. If your answer is yes what is the reason? A. Already not jointly exercitation
B. Inexperience C. Not keep balance D. All E. No answer
7. Where most of the time injuries suffered are home or away home played?
Page 90
75
A. Home B. Away home C. No answer
8. Is there the ferine court and weather condition the factors of injury that occur frequently?
A. Yes B. Never C. Same times D. No answer
9. Are you think over the cultural dance and emotional jumping celebration after scoring that
contribute to injuries? A. Yes B. Same times C. Never D. No answer
Part 4 questionnaires that will assess treatments of injuries
1. How often do you get access of physiotherapy services at the time of injury?
A. always B.sometimes C.never
2. If your answer is never what is the reason was?
A. Financial problems to fulfill the necessary materials
B. Lack of physiotherapist C. I have no idea
3. When injury is occurred who gives first aid? A. Coach B. Physiotherapists
4. Do you do rehabilitation exercise at the period of injured? A. Yes B. No
5. If your answer Q4 is „Yes‟, what type of exercise do you do?
6. If your answer Q4 is „No‟, for number 5th
question why?
7. What do you think should be done additional to avoid volleyball injuries? (Elaborate)
Appendix B: Socio-demographic related questions for Coaches in English
Name of your club ________________________ No Questions Responses
1 Gender 1.Male 2.Femae
2 Age 1. > 30 Years 2. 30-40 3. 40-50 4. Older Than 50
3 Field of Study 1. Physical Education and Sport Sciences 2. Other study Fields
4 Level of Education 1. Diploma 2.Bachelor 3.Master 4.PhD
5 Coaching Experience year 1. < 5 Years 2. 5-10 Years 3. Higher Than 10 Years
6 Level Coaching Certification 1. Level I 2. Level II 3. Level III 4. FIV
1. Is there coaching work experience in others team? For how long?
Page 91
76
2. How long years of coaching volleyball experience in this club?
3. Does the club have its own volleyball court? A. Yes B. No
4. Which court type do you have?
A. Soil B. Natural grass C. Asphalt D. Other
5. Are players trained and play at safe playing court? A.Yes B. No
6. Did you see incidence of injury on your players? A.Yes B. No
7. When injury is occurred mostly?
A. During training B. during match, C. Both during training and match
8. Does your team have face injury because of using improper equipment?
A. Yes B. No
9. How much the injury affects player‟s performance? A. Highly B. Middle C. Low
10. Is imbalance diet is factoring for injury your club? A. Yes B. No
11. Does the players‟ injury have psychological impact? A. Yes B. No
12. Is none-flexible plays more injured than flexible player? A. Agree B. Disagree
13. Is dehydration is the cause for injury in your club? A. Yes B. No
14. Which type of injuries that are facing during training?
A. Dislocation B. Fracture C.Muscle tear
15. Does a club have physiotherapists? A. Yes B. No
16. If your answer for question number 13 is „No‟, what is the reason?
17. If your answer for number 13 questions is „No‟, by which mechanisms the injured get player
treatment?
18. What do you think should be done to avoid volleyball injuries? (Elaborate)
Page 92
77
Appendix C: Socio-demographic related questions for physiotherapists in English
Name of your club ________________________ No Questions Responses
1 Gender 1.Male 2.Femae
2 Age 1. > 30 Years 2. 30-40 3. 40-50 4. Older Than 50
3 Field of Study 1. Physical Education and Sport Sciences 2. Other study Fields
4 Level of Education 1. Diploma 2.Bachelor 3.Master 4. certificate
5 Physiotherapists Experience 1. < 5 Years 2. 5-10 Years 3. Higher Than 10 Years
6 Level of Certification 1. National 2. FIV
1. Is there physiotherapists work experience in others team? For how long?
2. How long years of physiotherapists volleyball experience in this club?
3. What kind of injuries occurred in volleyball male athletes? ____________________
4. Have you met any athlete have got injured? A. Yes B. No
5. What kind of medical treatment you give for injures male athletes? ______
6. Do you think athletes life style is the problems of injures? A. Yes B. No
7. If your answer is yes for the yes questions why? __________
8. Do you think male volleyball players injures because of their training?
A. Yes B. No
9. What are the problems and challenges of injury in volleyball male players? _______
10. Is adequate medical equipment and conducive classroom for conducting
Proper medication? A. Yes B. No
11. Do you think medical service is enough? A. Yes B. No
12. If your answer is no for the yes questions what kind injures you face? _______
13. In your medical treatments did athletes rehabilitate or not? A. Yes B. No
14. What are problems and challenges athletes were not rehabilitate? _______
15. Does volleyball players have enough sport wear? A. Yes B. No
Page 93
78
Appendix I
ጎንደር ዩኒቨርስቲ
የተፈጥሮ ቀመርና ሳይንስ ኮሌጅ ስፓርት ሳይንስ ትም/ክፍል
የድህረምረቃ ፕሮግራም የጥናት መጠይቅ ለቮልቮል ተጫዋቾች፣ አሰልጣኖች እና
የወጌሻ ባለሙያ
የተከበራቹ ተጫዋቾች፣አሰልጣኖች እና የወጌሻ ባለሙያ
የመጠይቁ አላማ፡-
ይህ መጠይቅ የተዘጋጀበትን ዋና አላማ በደቡብ ክልል በወላታ ዞን በሶዶ ከተማ ና አሮምያ ክልል በባለ ዞን
በሮበ ከተማ በመዳዎላቦ ዩኒቨርስቲ ባሉት የወንዶች ቮልቮል ፒርምርሊጊ ክለብ ውስጥ በሚጫዎቱ ከለቦች
ላይ የሚደርሱ ስፓርታዊ ጉዳቶች ማለትም የሚጎዳው የሰውነት ክፍል፣ ጉዳት አይነት፣ ብዛትና
መንስኤዎቹን ለማዎቅና የጥናቱን ውጤት መሰረት በማድረግ ለችግሮች የመፍትሄ ሀሳብ ለመጠቆም
ሲሆን የጥናቱ ዋና ምክንያት በጎንደር ዩኒቨርስቲ ስፓርት ሳይንስ የድህረ ምረቃ ትምህርት የመጨረሻ
አመት የመመረቂያ ጹሁፍ ለማሟላት ነው፡፡በዚህ መጠይቅ ላይ ላሉ ጥያቄዎች የሚሰጡት መልስ ከላይ
ለተጠቀሰው አላማ ብቻ የሚውል ሲሆን የእርስዎ ሙሉ ትብብር ለአላማው መሳካት በጣም አስፈላጊ
በመሆኑ ቀና ትብብረዎን ከአክብሮት ጋር በትህትና አጠይቃለሁ፡፡
የተከበራቹ በቅድሚያ አመሰግናለሁ ! ማሳሰብያ፡-
መጠይቁን በሚሞሉበት ግዜ ሰምዎን ና አድራሻዎን መጻፍ አስፈላጊ አይደለም፡፡
የእርስዎ ሁሉንም ጥያቄዎች መሙላት ወሳኝነት ስላለው እባክዎ ሁሉንም ጥያቄዎች በትክክል
መሙላተዎትን እንዳይረሱ፡፡
ምርጫ ለቀረበላቸው ጥያቄዎች የራየት ምልክት/ የክብ ምልክት በመጠቀም
ይመልሱ
ቀጥሎ በጽሁፍ ለሚመለሱ ጥያቄዎች አጭርና ግልጽ መልስ ይፃፉ
ታጠቅ ግርማ(በስፓርትሳይንስየማስተርስተመራቂተማሪ)
ስ. ቁ 09 00 40 36 60/09 16 13 09 57
Email address: [email protected]
ጎንደርዩኒቨርስቲ
2019/2020 G.C
Page 94
79
ክፍል አንድ የተጫዋቾች የግል መረጃ
የምጫውቱቢት የቡድኑ ሥም ----------------------------
-ጾታ:- ወንድ ሴት
-ዕድሜ:- 20-25 ዓመት 2 6-30 ዓመት 31-35 ዓመት 36-40 ዓመት
ከ40 ዓመት በላይ
-ቁመት:- 1.50-1.65 cm 1.66-1.75 cm 1.76-1.85 cm 1.86-1.95 cm ከዚያ
በላይ
-ክብደት:- 50-60 ኪ.ግ 61-70 ኪ.ግ 71-80 ኪ.ግ 81. ኪ.ግ በላይ
-የትምህርት ደረጃ፡- 10/12 ያጠናቀቀ ሰርተፊኬት ዲፕሎማ ድግሪ
ከዚያ በላይ
-የጋብቻ ሁኔታ፡- ያገባ ያላገባ የፈታ
-የጨዋታ ልምድ:- 1-2 ዓመት 2-4 ዓመት 5-6 ዓመት 7 ከዚያ በላይ ዓመት
ክፍል ሁለት ስፓርታዊ ጉዳቶችን የሚመለከት ጥያቄዎች
1. ባሳለፈነው የጨዋታ አመት አንስቶ እስካሁን ድረስ ጉዳት ደርሶብህ ያውቃል ?
1. አዎ 2. አልደረሰብኝም
2. ለተራ ቁጥር 1 መልስህ አዎ ከሆነ ለምን ያህል ግዜ ጉዳት ደረሰብህ ? ----------------------------------
3. የትኛው የሰውነት ክፍል ነበር ጉዳት የደረሰብህ ከአንድ በላይ መልስ መስጠት ይቻላል ?
1. እራስ 3. ጉልብት 4. ክርን 7/ የቆዳመላጥ 9/ ዳሌ 11/ የእግር እጣት
2. የእጅእጣት 5. ደረት 6. ቁርጭምጭሚት 8. ታክሻ
10/ ጭን 12/ ቅልጥም
4. ጉዳቱ ሲደርስብህ የትኛው የጫዋታ ሁኔታ ላይ ነበርክ ? 1.ብሎክ እያደረኩ (ሲጋርድ )
2.እስማች ሰመታ (ሲደፍቅ) 3. ሰርብ ሰሰርብ 4/ አላወኩም
Page 95
80
5. በየትኛው የጨዋታ ፓዚሽን እያለህ ነው የተጎዳሃው ? 1/ ሴተር 2/ ግራ/ ቅኝየፊትተጫዋች 3/
ግራ/ቀኝየኋላተጫዋች 4/ ስድስትቁጥርቦታላይ 5/ ሌላ ካለ ይጠቀስ-------------
ጉዳቱ የደረሰው በውድድር ግዜ ከሆነ በስንተኛው ዙር ላይ ነው ?
1/ 1ኛው/ 2ኛው 2/ 2ኛው/ 3ኛውላይ 3/ 4ኛው/ 5ኛውላይ
4/ ከጨዋታ በፊት ሰውነቴን ሳማሙቅ 5/ ጉዳቱ የደረሰው ቀሰበቀስ ነው
6. ጉዳቱ በደረሰብህ ወቅት ጨዋታውን/ልምምዱን አቋርጠህ ወጥተሃል ?
1/ አዎ 2/ አልወጣሁም
7. የደረሰብህን ጉዳት ተከትሎ ከልምምድ ምን ያህል ግዜ ቀረህ ?
1/ ከአንድ ሳምንት በታች 2/ ከሁለት እስከ አራት ሳምንት 3/ ከአራት ሳምንት በላይ 4/
አልቀረሁም
ክፍልሶስት፡- ለጉዳት መንስየ የተመለከተ ጥያቄዎች
1. በቮሊቮል ጨዋታ/ልምምድ ጊዜ ጉዳት ሊያመጡ የሚችሉ ምክንያቶች ምንድን ናቸው?
1) ሰውነትን አለሟሟቅ 2) ምቹ ያልሆነ ሜዳ በመሆኑ 3) ትጥቅ አለማሟላት 4)
ፍላጎት አለመኖር 5) ሌላ ካለ ይጠቀስ_______________
2. ካሳለፍነው የውድድር ግዜ እስካሁን ድረስ በሳምንት ለስንት ቀን ልምምድ ትሰራላችሁ-------
3. ካሳለፍነው የውድድር ግዜ እስካሁን ድረስ በሳምንት ለምን ያህል ሰዓት ልምምድ
ትሰራለችሁ?..........--
4. የጉልበት መከላከያ ትጠቀማለህ 1/ አዎ 2/ አልፎአልፎ 3/ አልጠቀምም
5. ለ2እናለ3 ሆናቹ ስትጋርዱ (block) ስታደርጉ ጉዳት ተከስቶ ያዉቃል
1/ አዎ 2/ አልፎአልፎ 3/ ተከስቶ አያውቅም
6. መልስዎ አዎ ከሆነ ምክንያቱ ምን ሊሆን ይችላል ብለህ ታስባለህ 1/ በጋራ ልምምድ አስቀድሞ
አለመስራት 2/ የልምድ ማነስ 3/ ባላንስ አለመጠበቅ 4/ ሁሉም
7. በልምምድ እና በውድድር ወቅት ውሃ በአግባቡ ቀርቦልህ ትጠቀማለህ
1/አዎ 2/ አልፎአልፎ 3/ አልጠቀምም
Page 96
81
8. ጉዳቱ የደረሰው በልምምድ /ጨዋታ ግዜ ከሚከተሉት በየትኛው ሁኔታ ነው
1/ ከጓደኛ ጋር ግጭት 2/ ከፓል ጋር ግጭት 3/ መሬት ላይ በመውደቅ 4/
በዝላይ ግዜ በአንድ ዕግር ተመልሶ በማረፍ 5/ ሌላ ካለ ይጠቀስ--------------------------
9. የተለመደ/ተደጋጋሚ የሚደርሱ ጉዳቶች የትኛዉን የአካልህን ክፍል በብዛት ያጠቃሉ ?
1/ ትከሻ 2/ቁርጭምት 3/ ጉልበት 4/ የእጅ ጣት 5/ የእግር ጣት
10. አብዛኛዉን ግዜ የሚያጋጥምህ ጉዳት ምን አይነት ነው
1/ የአጥንት መሰንጠቅ 2/ የአጥንት ስብራት 3/ የጡንቻ መሰንጠቅ 4/ የጡንቻ መሸማቀቅ
5/ ወለምታ
11. ብዙን ግዜ በሀገር ውስጥ ስትጫወት ነው ወይስ ከሀገር ዉጭ ስትጫወት ነዉ ጉዳት የደረሰብህ ?
1/ በአገር ዉስጥ 2/ ከሀገር ዉጭ
12. ከአሀር ዉጭ ስትጫወት ከሆነ ምክንያቱ ምንድነዉ ብለህ ታስባለህ ?-------------------------------
13. ከሀገር ዉጭ ስትጫወት ሜዳው የጉዳት መንሰኤ ሆኖብህ ያዉቃል ?
1/አዎ 2/ አልፎአልፎ 3/ አልሆነብኝም
14. ከሀገር ዉጭ ስትጫወት የአየር ንብረቱ የጉዳት መንሰኤ ሆኖብህ ያዉቃል ?
1/አዎ 2/ አልፎአልፎ 3/ አልሆነብኝም
15. ከነጥብ ቦሃላ የምታደደርገዉ የደስታ አገላለጽ በመዚለል ሆነ በባህል ጭፈራ የጉዳት መንስኤ
(ምክንያት ሆኖብህ ያዉቃል) 1/ አዎ 2/ አልፎአልፎ 3/ አልሆነብኝም
ክፍልአራት፡ስፓርታዊ ህክምናን የተመለከተ ጥያቄ
1. ጉዳቱ በረደሰብህ ወቅት ህክምና አግኝተህ ነበር ? 1/ሁልግዜ 2/ አልፎአልፎ 3/ አላገኘሁም
2. መልሰህ አላገኘሁም ከሆነምክንያቱ ምን ይሆን ?
1. የህክምና ቁሳቁሶችን ለሟሟላት የገንዘብ እጥረት
2. የህክምና ባለ ሙያ (ወጌሽ) አለመኖር 3. ምንም ሃሳብ የለኝም
3.ጉዳቱ በደረሰብህ ግዜ የህክምና አገልግሎት ወድያውኑ የሰጠህ ማን ነበር
-------------------------------------------------------------------
4.ከጉዳትህ እንድታገግም የተለያዩ የማገገምያ እንቅስቃሴዎችን ትሰራ ነበር
Page 97
82
1/ አዎ እሰራ ነበር 2/ አልሰራም
5.ለተራ ቁጥር 4 መልስህ አዎ ከሆነ ምን አይነት ስፓርታዊ እንቅስቃሴዎችን ነበር የምትሰራው
---------------------------------------------------------------------------------------
6.ለተራ ቁጥር 4 መልስህ አልሰራም ከሆነ ለምን---------------------------------------------------------------
---------------------------------------------------------------------------------------------------------
ክፍል 2፡- የአሰልጣኞች የግል መረጃ
የምያስለጥነኑት የቡድኑ ሥም ------------------------------------------
-ጾታ:- ወንድ ሴት
-ዕድሜ:- 20-25 ዓመት 26-30 ዓመት 31-35 ዓመት 36-40 ዓመት ከ40
ዓመት በላይ
-ቁመት:- 1.50-1.65 cm 1.66-1.75 cm 1.76-1.85 cm 1.86-1.95 cm ከዚያ
በላይ
-ክብደት:- 50-60 ኪ.ግ 61-70 ኪ.ግ 71-80 ኪ.ግ 81. ኪ.ግ በላይ
-የትምህርት ደረጃ፡- 10/12 ያጠናቀቀ ሰርተፊኬት ዲፕሎማ ድግሪ ከዚያ በላይ
-የጋብቻ ሁኔታ፡- ያገባ ያላገባ የፈታ
-የጨዋታ ልምድ:- 1-2 ዓመት 2-4 ዓመት 5-6 ዓመት 7 ከዚያ በላይ
ዓመት
-የአሰልጣኝነት ደረጃ :- ደረጃ አንድ ደረጃ ሁለት ደረጃ C FIFA በ ልምድ
-በዚህ ክለብ ዉስጥ ለምን ያህል ዓመት የማሰልጠኝ ልምድ አሎት ?----------------------------
-በሌላ ክለብ የአሰልጣኝነት ልምድ አሎት ? ለምን ያህል ዓመት ?
Page 98
83
ክፍልሁለት፡- አጠቃላይ ጥያቄ
1. ክለቡ የራሱ የሆነ የቮሊቮል ሜዳ አለው? 1/ አዎ 2/ የለውም
2. የጨዋታ ሜዳችሁ ምን አይነት ነው? 1.አፈር 2/ የተፈጥሮ ሳር 3/ አሰፋልት 4/ ሌላ ከሆነ ይጠቀስ
3. ተጫዋቶች ልምምድ የሚሰሩበት እና ውድድር የሚያካሂዱበት ሜዳ ምቹ ነው? 1/አዎ 2/ አይደለም
4. ተጫዋቶች ጉዳት ሲያጋጥማቸው ተመልክተሃል? 1/ አዎ 2/ አላጋጠመኝም
5. በየትኛው ግዜ ነበር ጉዳቱ የደረሰባቸው? 1/ በልምምድ ወቅት 2/ በውድድር ወቅት 3/ በሁለቱም
6. የክለብህ ተጫዋቾች በቂ የሆነ የዕስፖርት ትጥቅ አላቸዉ ?
1/ አዎ 2/ የለዉም 3/ ሙሉ በሙሉ ባይባልም
7. የተጫዋቿች ትጥቅ ለጉዳት መንሰኤ የሆነባቸው አጋጣሚ አለ ? 1/ አዎ 2/ አላጋጠማቸዉም
መልሱ አዎ ከሆነ ለምሳሌ ቢጠቅሱ -----------------------------
8. ከነጥብ ቦሃላ ደስታን ለመግለጽ በሚል ተገቢ ያልሆነ ዝላይ, የባህል ጭፈራና የተለያዩ ምልክቶች
ለጉዳት መንስኤ ሆነዉ ያዉቃሉ (አጋልጧቸው ያዉቃል)? 1/ አዎ 2/ አላጋጠማቸዉም
9. የዕርሶ የአሰለጣጠን ዘይቤ (ስልት) ለጉዳት ያጋልጣቸዉ ይሆን ብለዉ ያስባሉ? 1/ አዎ 2/ በፍጹም
10. ከአገር ዉጭ ከሆነ ምክንያቱ ምንድነዉ ብለዉ ያስባሉ?
1/ የተጋጣሚያቹ ችሎታ/ልምድ መብለጥ 2/ ለሚዳዉ አዲስ መሆን
11. የእርሶ ክለብ ተጫዋቾች ዕድሜ በአማካኝ ከስንት እስከ ስንት ይሆናሉ ?-------------------
12. የተጫዋቾች ዕድሜ የጉዳት መንስኤ ሆኖበት ያዉቃል ? ስያንስ/ሲበዛ -----------------------
13. በጫወታም ሆነ በልምምድ ሰዓት ተጫዋቾች ጉዳት እንዳያጋጥማቸው ምን አይነት ጥንቃቄ
እንዲወስዱ ይመክሯቸዋል? ---------------------------------------------------------------
14. ክለቡ የራሱ የሆነ ሀኪም/ወጌሻ አለዉ? 1/ አዎ 2/ የለዉም
15. መልስህ የለውም ከሆነ ምክያቱ ምንድን ነው? -------------------------------------------
16. ለተራቁጥር 6 መልስህ የለውም ከሆነ ተጫዋቾች ጉዳት ሲደርስባቸው ህክምና የሚያገኙት እንዴት
ነው?
Page 99
84
የምሰሩበት የቡድኑ ሥም
-ጾታ፡- ወንድ ሴት
-የወገሻ ልምድ 1-2 ዓመት 2-4 ዓመት 5-6 ዓመት 7 ከዚያ በላይ ዓመት
- የወገሻ ደረጃ ፡- ደረጃ አንድ ደረጃ ሁለት ደረጃ C FIFA በልምድ
-በዚህ ክለብ ዉስጥ ለምን ያህል ዓመት የወገሻነት ልምድ አሎት ?----------------------------
-በሌላ ክለብ የወገሻነት ልምድ አሎት ? ለምን ያህል ዓመት ?
ክፍል ሶስት፡- አጠቃላይ ጥያቄ
1.በተጫዋቾች በልምምድ/በትሬንግ ሆነ በጫዋታ ሰዓት ጉዳት ስያጋጥማቸዉ አይተዋል/አጋጥሞታል?
1/ አዎ 2/ አላየዉም
2.ካጋጠሞት በብዛት በወንዶች የክለብ ተጫዋቾች ምን አይነት ጉዳት ይከሰታል ?
1/ አስቸጋሪ/ሀይለኛ (acute injuries) 2/ ልማደኛ /ስር የሰደደ (chromicinjuries) 3/ ሁለቱም
3.የተጫዋቾች የአኖኖር ዘይቤ ለጉዳት መከሰት ችግር ነዉ ብለዉ ያስባሉ? 1/ አዎ 2/ አላስብም መልሶ
አዎን ከሆነ እንዴት ?
4.የተጫዋቾች የጉዳት መንሰኤ የልምምድ/የትሬንግ ችግር ብለዉ ያስባሉ ? 1/ አዎ 2/ አላስብም
5.ለተጫዋቾች ጉዳት የአሰልጣኙ የአሰለጣጠን ዘዴ ለጉዳት መንሰኤ ነዉ ብለዉ ያስባሉ ?
1/ አዎ 2/ አይደለም አዎ ከሆነ እንዴት
6.ለተጫዋቾች ጉዳት የአሰልጣኙ አቅም/ቸወሎታ ማነስ ለጉዳት ይዳርጋቸዋል ብለዉ ያስባሉ? 1/ አዎ 2/
አላስብም
1. በዋናነት ለተጫዋቾች ጉዳት ችግሩ ምንድነዉ ብለዉ ያስባሉ ?------------------------
2. በቂ የሆነ የመጀመርያ እርዳት መስጫ መሳሪያና ለእርዳታ አመች የሆኑ የህክምና ክፍሎች አላቹሁ ? --
Page 100
85
3. ጉዳት ደርሶባቸው በምትረዱአቸዉ ግዜ የተለመደ/ተደጋጋሚ የሚደርስባቸዉ ጉዳቶች የትኖቹ ናቸዉ?
1/ የጉልበት መጎዳት 2/ የትከሻ ጉዳት 3/ የቁርጭምጭሚት 4/ የጣት 5/ ወለምታ
4. ከነዚህ ዉስጥ ብዙን ግዜ የምትቸገሩባቸዉ የትኖቹ የጉዳት አይነቶች ነቸዉ ?-----------------------
5. አብዛኛዉ ግዜ ተጫዋቾች የሚያጋጥማቸዉ ጉዳት ምን አይነት ነዉ ?
1/ የሀጥንት ስብራት 2/ የአጥንት መሰንጠቅ 3/ የጡንቻ መሰንጠቅ 4/ ወለምታ
6. ብዙን ግዜ ብሎም በተለምዶ በሯጮችና በእግርኳስ ተጫዋቾች ላይ የጡንቻ መሸማቀቅ ያጋጥማል ፡፡
በቮሊቮል ተጫዋቾች የጡንቻ መሸማቀቅ ያገጥማል ? 1/ አዎ 2/ አያጋጥምም
7. ብዙን ግዜ ተጫዋቾች ጉዳት ያጋጠማቸዉ ሀገር ዉስጥ ስትጫወቱ ነዉ/ከሀገር ዉጭ ?
ከሀገር ዉጭ ከሆነ ምንድነዉ ችግሩ ብለዉ ያስባሉ -------------------------
8. አብዛኛዉን ጊዜ የተጫዋቾች ጉዳት የሚመዘገበዉ በምን አይነት ሜዳ ላይ ነዉ ?
1/ አስፓልት 2/ አፈር 3/ ጂሚናዚየም 4/ አርቴ ፊሻል ሳር
9. የተጫዋቾች ዕድሜ የጉዳት መንሰኤ ሊሆን ይችላል ብለዉ ያስባሉ ? ሲያንስ/ሲበዛ
10. ደስታን ለመግለጽ የሚጠቀሙበቸዉ ባህላዊ ጭፈራዎች ለጉዳት መንሰኤ ነዉ ብለዉ ያምናሉ 1/ አዎ
2/ አላምንም
11. በናተ ደረጃ የህክምና/ የመጀመሪያ እርዳታዉ በቂ ነዉ ብለዉ ያስባሉ 1/ አዎ 2/ አይ
አይ ከሆነ ምክንያ
12. እርሶ የጉዳቱ መጠን ተመልክተዉ ወይንም አረጋግጠዉ ተጫዋቹ እንዳይገባ ወስነዉ ሳለ ተጫዋቹ
ልጫወት ያለበት ግዜ አለ (አሰልጣኙ ወሳኝ ጫወታ ሆኖ በማደንደዘዧም ቡሆን ይግባና ይጫወት
ብለዉ ዉሳኔዉን የተቃረኑበት ጊዜ አለ)?
1/ አዎ ከሆነ ተጫዋቹ ከጫወታ ቦሃላ ለከፋ ጉዳት ወይንም ለተጨማሪ ጉዳት አልተጋለጠም