University of Groningen ADPKD Messchendorp, Annemarie Lianne IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2019 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Messchendorp, A. L. (2019). ADPKD: Risk Prediction for Treatment Selection. Rijksuniversiteit Groningen. Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license. More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne- amendment. Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 18-12-2021
Transcript
University of Groningen
ADPKDMesschendorp, Annemarie Lianne
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2019
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Messchendorp, A. L. (2019). ADPKD: Risk Prediction for Treatment Selection. Rijksuniversiteit Groningen.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license.More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne-amendment.
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Figure 1. Algorithm to assess indications for tolvaptan treatment in ADPKD with lower eGFR threshold of 45 ml/min/1.73m2 and upper age threshold of 50 years (upper panel), or lower eGFR threshold of 30 ml/min/1.73m2 and upper age threshold of 55 years (lower panel) with results for adult patients from the University Medical Center Groningen, the Netherlands (n=386).
predict disease progression and is a faster and cheaper option compared to genetic
testing. Keeping this clinical experience in mind, the algorithm may be simplified as
presented in Figure 2.
Figure 2. Simplified algorithm to assess indication for tolvaptan treatment in ADPKD with eGFR threshold of 30 ml/min/1.73m2, age criteria <55 years, and results for adult patients from the University Medical Center Groningen (n=386).
A SIMPLIFIED DECISION ALGORITHM LARGELY FOCUSED ON CKD STAGE BY AGE; EXAMPLES FROM CLINICAL CARE
The hierarchical decision algorithm is based on the assumption that patients with
rapidly progressive disease will benefit the most from tolvaptan treatment and
that GFR for age, or historical changes in GFR, provide more information on rate of
disease progression than (change in) TKV or PKD gene mutation analysis. It can be
even reasoned that one might even need no other parameters than just one GFR and
age value to assess evidence of rapidly progressive disease for treatment selection.
As data was available for multiple steps in the algorithm for 386 patients with ADPKD
from the University Medical Center Groningen, we investigated if we could provide
evidence to support this hypothesis.
CKD stage by age
The first step of the decision algorithm is based on CKD stage by age. When strictly
following this algorithm, patients who are 50 or 40 years of age with a GFR of 60
ml/min/1.73m2 will both be eligible for tolvaptan treatment. In this example, the
patient of 50 years of age is probably a slower progressor and of 40 years of age a
faster progressor. Although the ERA-EDTA algorithm denotes age classes, it is better
to keep a continuous scale of GFR by age in mind in the decision to start tolvaptan
treatment. In Figure 3, the eGFR of all 386 patients from the UMCG are plotted against
age. In this figure a theoretical line is plotted: Patients below this line are defined as
fast progressors and eligible for tolvaptan and patients above this line are defined
as slow progressors and ineligible for tolvaptan. Of note, patients younger than 30
years were not taken into account, since in young patients with CKD stage 1, kidney
function may be less sensitive for assessment of disease severity, progression and
prognosis (as discussed later).
Figure 3. Estimated GFR according to age for adult patients from the University Medical Center Groningen (n=386). The dotted line represents threshold for rapidly progressive disease based on eGFR by age and was calculated with the following data points: 35 years of age with an eGFR of 90 ml/min/1.73m2, 45 years of age with an eGFR of 60 ml/min/1.73m2 and 60 years of age with an eGFR of 15 ml/min/1.73m2 (eGFR=195 – 3*age). Grey areas are sections outside the indication for tolvaptan; old situation (upper panel, eGFR<45 ml/min/1.73m2 or age>50 years), new situation (lower panel, eGFR<30 ml/min/1.73m2 or age>55 years).
In Figure 4 the eGFR of all 386 patients from the UMCG are again plotted against age
including the theoretical threshold line. In this figure patients are marked according to
a confirmed eGFR decline ≥ or < 3.0 ml/min/1.73m2 over a period of five years. Table
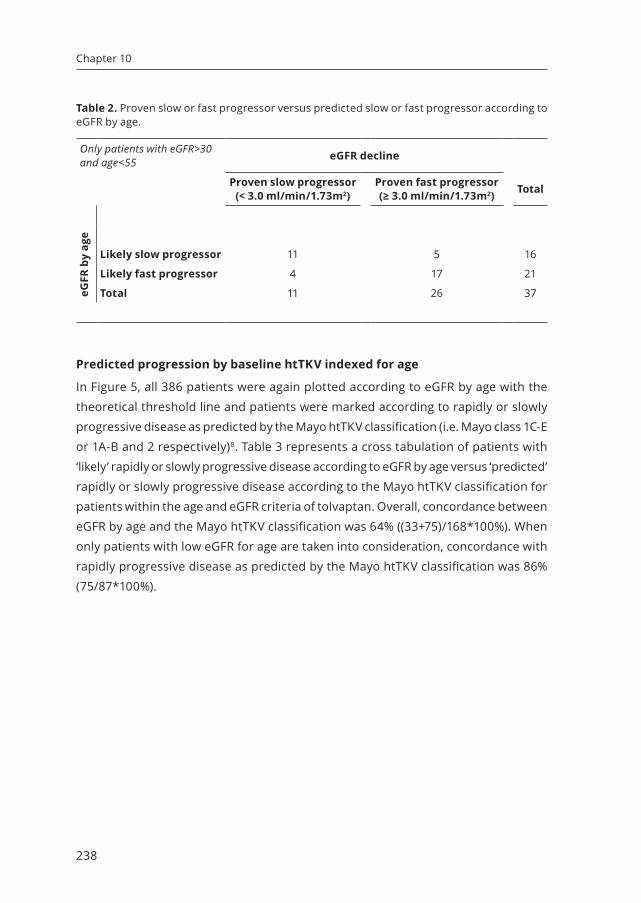
2 represents a cross tabulation of patients with ‘likely’ rapidly or slowly progressive
disease according to eGFR by age versus ‘proven’ rapidly or slowly progressive
disease according to eGFR decline for patients within the age and eGFR criteria
of tolvaptan. Overall, concordance between eGFR by age and eGFR decline was
76% ((11+17)/37*100%). When only patients with low eGFR for age are taken into
consideration, concordance with rapidly progressive disease as determined by eGFR
decline was 81% (17/21*100%).
Figure 4. Rapidly or slowly progressive ADPKD based on eGFR decline versus eGFR by age. The dotted line represents threshold for rapidly progressive disease based on eGFR by age and was calculated with the following data points: 35 years of age with an eGFR of 90 ml/min/1.73m2, 45 years of age with an eGFR of 60 ml/min/1.73m2 and 60 years of age with an eGFR of 15 ml/min/1.73m2 (eGFR=195 – 3*age). Grey areas are sections outside the indication for tolvaptan (eGFR<30 ml/min/1.73m2 or age>55 years).
Figure 5. Rapidly or slowly progressive ADPKD based on Mayo htTKV class versus eGFR by age. The dotted line represents threshold for rapidly progressive disease based on eGFR by age and was calculated with the following data points: 35 years of age with an eGFR of 90 ml/min/1.73m2, 45 years of age with an eGFR of 60 ml/min/1.73m2 and 60 years of age with an eGFR of 15 ml/min/1.73m2 (eGFR=195 – 3*age). Grey areas are sections outside the indication for tolvaptan (eGFR<30 ml/min/1.73m2 or age>55 years).
Table 3. Predicted slow or fast progressor according to Mayo htTKV class versus eGFR by age.
Only patients with eGFR>30 and age<55 Mayo htTKV class
well as clinical parameters9. When clinical parameters are not available, the ‘Genetic
Risk Score’ can be used, which is a score based on sex and genotype only. A genetic
score ≥2 points, which incorporates the presence of a truncating PKD1 mutation,
predicted end stage kidney disease onset before age 65 years with a sensitivity of
73.8%, a specificity of 74.3%, a positive predictive value of 80.4%, and an negative
predictive value of 66.6%. In Figure 6 patients are plotted according to eGFR by age
with the theoretical threshold line and marked as slowly or rapidly progressive disease
predicted by the Genetic Risk Score (i.e. <2 or ≥ 2 respectively). Table 4 represents
a cross tabulation of patients with ‘likely’ rapidly or slowly progressive disease
according to eGFR by age versus ‘predicted’ rapidly or slowly progressive disease
according to the Genetic Risk Score for patients within the age and eGFR criteria of
tolvaptan. Overall, concordance between eGFR by age and the Genetic Risk Score
was 60% ((40+36)/126*100%). When only patients with low eGFR for age are taken
into consideration, concordance with rapidly progressive disease as predicted by the
Genetic Risk Score was 57% (36/63*100%).
Figure 6. Rapidly or slowly progressive ADPKD based on Genetic Risk Score compared to eGFR by age. The dotted line represents threshold for rapidly progressive disease based on eGFR by age and was calculated with the following data points: 35 years of age with an eGFR of 90 ml/min/1.73m2, 45 years of age with an eGFR of 60 ml/min/1.73m2 and 60 years of age with an eGFR of 15 ml/min/1.73m2 (eGFR=195 – 3*age). Grey areas are sections outside the indication for tolvaptan (eGFR<30 ml/min/1.73m2 or age>55 years).
Figure 7. Simplified algorithm focused on CKD stage by age to assess indication for tolvaptan treatment in ADPKD with eGFR threshold of 30 ml/min/1.73m2 and age criteria <55 years.
CONCLUSION
Now clinical experience with tolvaptan as treatment of ADPKD has been acquired, and
with the results of a recent large clinical trial, the recommendations when to initiate
tolvaptan treatment need to be updated. We reason that the eGFR threshold can be
lowered from 45 to 30 ml/min/1.73m2, and that the age threshold can be increased
from 50 to 55 years. In addition, we provided an updated and simplified decision
algorithm to assess whether tolvaptan treatment is warranted in patients with ADPKD.
It is important to emphasize that these are only recommendations to help caregivers
in the decision to initiate tolvaptan treatment and not rules that are set in stone. The
previous recommendations by the ERA-EDTA unfortunately have led to exclusion of
patients from reimbursement of tolvaptan from health care insurances because they
were not officially eligible for treatment. The decision to initiate treatment requires
the consideration of many factors besides eligibility, like patients motivation and
1. Torres VE, Chapman AB, Devuyst O, et al. Tolvaptan in patients with autosomal dominant polycystic kidney disease. N Engl J Med. 2012;367(25):2407-2418.
2. Gansevoort RT, Arici M, Benzing T, et al. Recommendations for the use of tolvaptan in autosomal dominant polycystic kidney disease: A position statement on behalf of the ERA-EDTA working groups on inherited kidney disorders and european renal best practice. Nephrol Dial Transplant. 2016;31(3):337-348.
3. Torres VE, Chapman AB, Devuyst O, et al. Tolvaptan in later-stage autosomal dominant polycystic kidney disease. N Engl J Med. 2017;377(20):1930-1942.
4. Shemesh O, Golbetz H, Kriss JP, Myers BD. Limitations of creatinine as a filtration marker in glomerulopathic patients. Kidney Int. 1985;28(5):830-838.
5. Watkins PB, Lewis JH, Kaplowitz N, et al. Clinical pattern of tolvaptan-associated liver injury in subjects with autosomal dominant polycystic kidney disease: Analysis of clinical trials database. Drug Saf. 2015;38(11):1103-1113.
6. Spithoven EM, Kramer A, Meijer E, et al. Renal replacement therapy for autosomal dominant polycystic kidney disease (ADPKD) in europe: Prevalence and survival--an analysis of data from the ERA-EDTA registry. Nephrol Dial Transplant. 2014;29 Suppl 4:iv15-25.
7. Messchendorp AL, Meijer E, Boertien WE, et al. Urinary biomarkers to identify autosomal dominant polycystic kidney disease patients with a high likelihood of disease progression. Kidney International Reports. 2017.
8. Irazabal MV, Rangel LJ, Bergstralh EJ, et al. Imaging classification of autosomal dominant polycystic kidney disease: A simple model for selecting patients for clinical trials. J Am Soc Nephrol. 2015;26(1):160-172.
9. Cornec-Le Gall E, Audrezet MP, Rousseau A, et al. The PROPKD score: A new algorithm to predict renal survival in autosomal dominant polycystic kidney disease. J Am Soc Nephrol. 2016;27(3):942-951.