University of Groningen Clearance of bronchial secretions after major surgery Leur, Johannes Peter van de IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2005 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Leur, J. P. V. D. (2005). Clearance of bronchial secretions after major surgery Groningen: s.n. Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 14-06-2018
Transcript
University of Groningen
Clearance of bronchial secretions after major surgeryLeur, Johannes Peter van de
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2005
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Leur, J. P. V. D. (2005). Clearance of bronchial secretions after major surgery Groningen: s.n.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Clearance of bronchial secretions after major surgery
The manufactures of the suction catheters and importers have sponsored the printing of this thesis and therefore are gratefully acknowledged.
UnoMedical, Denmark Medeco, The Netherlands
Cover: The Quest for meaning, by Hagen Haltern, USA ( used with permission)
Modified by: J.P. van de Leur
Printed by: Stichting Drukkerij C. Regenboog, Groningen, The Netherlands
Leur, J.P. van de Clearance of bronchial secretions after major surgery. Thesis University of Groningen, The Netherlands – With References - With summary in Dutch.
Clearance of bronchial secretions after major surgery
Proefschrift
ter verkrijging van het doctoraat in de Medische Wetenschappen
aan de Rijksuniversiteit Groningen op gezag van de
Rector Magnificus dr. F. Zwarts, in het openbaar te verdedigen op
woensdag 5 oktober 2005 om 16.15 uur
door
Johannes Peter van de Leur
geboren op 10 november 1963 te Delft
Promotores: Prof. Dr. J.H. Zwaveling Prof. Dr. J.H.B. Geertzen
Copromotor: Dr. C.P. van der Schans
Beoordelingscommissie: Prof. Dr. L.P.H.J. Aarts Prof. Dr. H.A.A.M. Gosselink Prof. Dr. H.A.M. Kertsjens
Paranimfen:
K.W. Douma R. Zorge
Contents page
Chapter 1: 3 Postoperative mucus clearance
Chapter 2: 31 Endotracheal suctioning versus minimally invasive airway suctioning
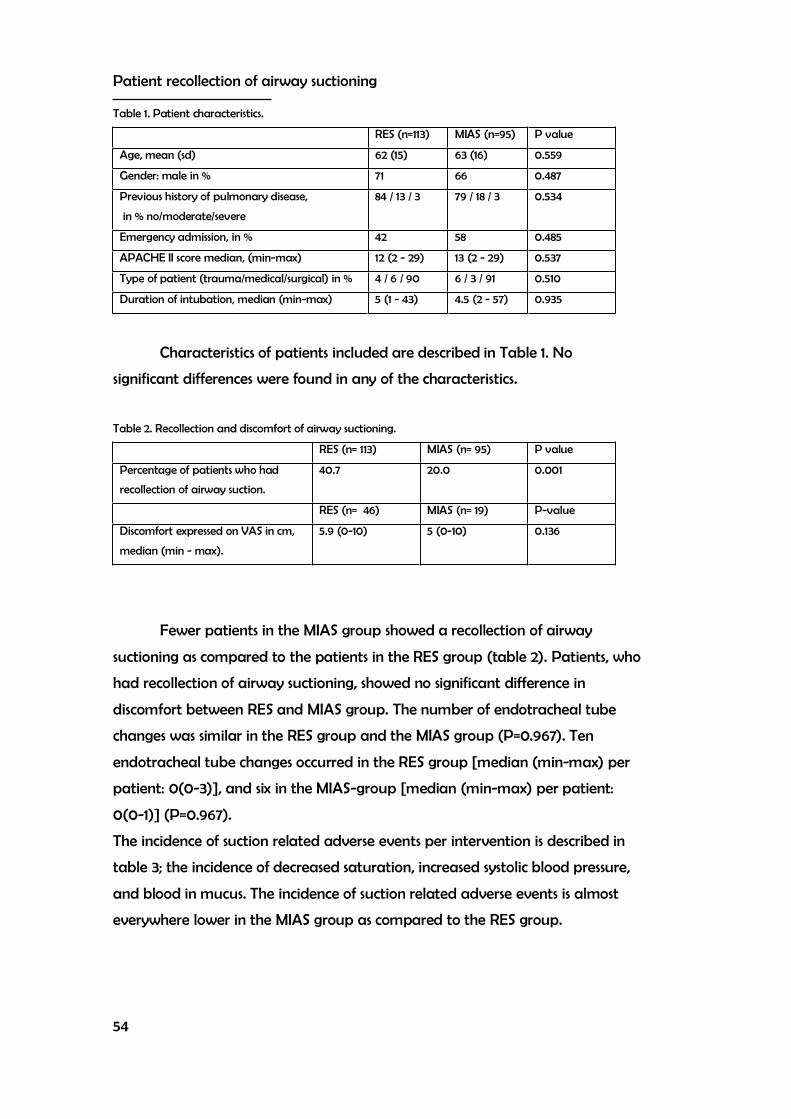
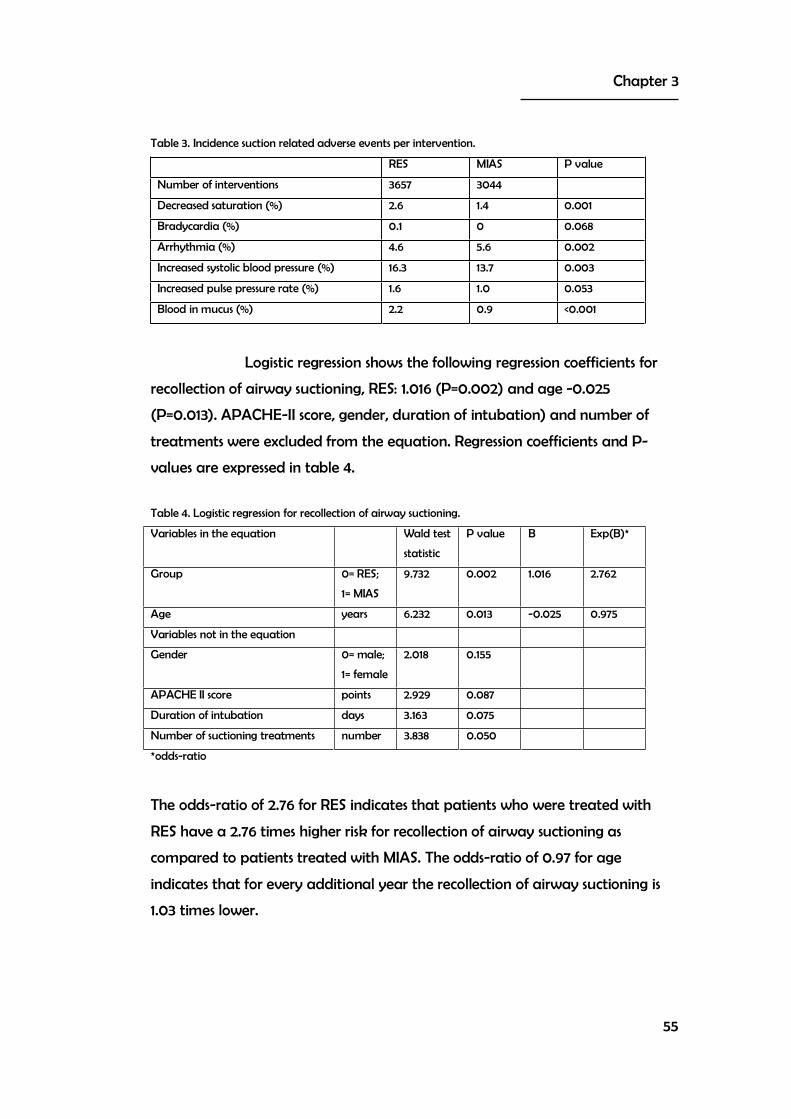
Chapter 3: 49 Patient recollection of airway suctioning: routine versus a minimally invasive procedure
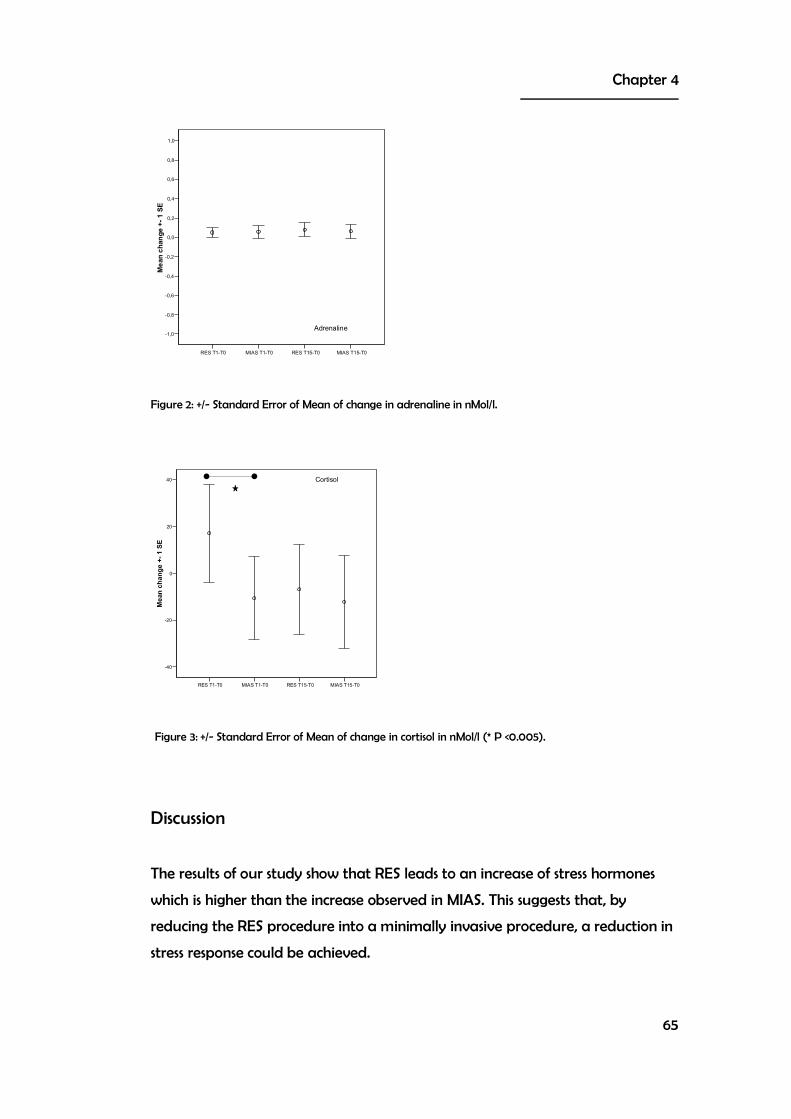
Chapter 4: 59 Stress reaction during endotracheal suctioning
Chapter 5: 69 Discomfort and factual recollection of ICU patients
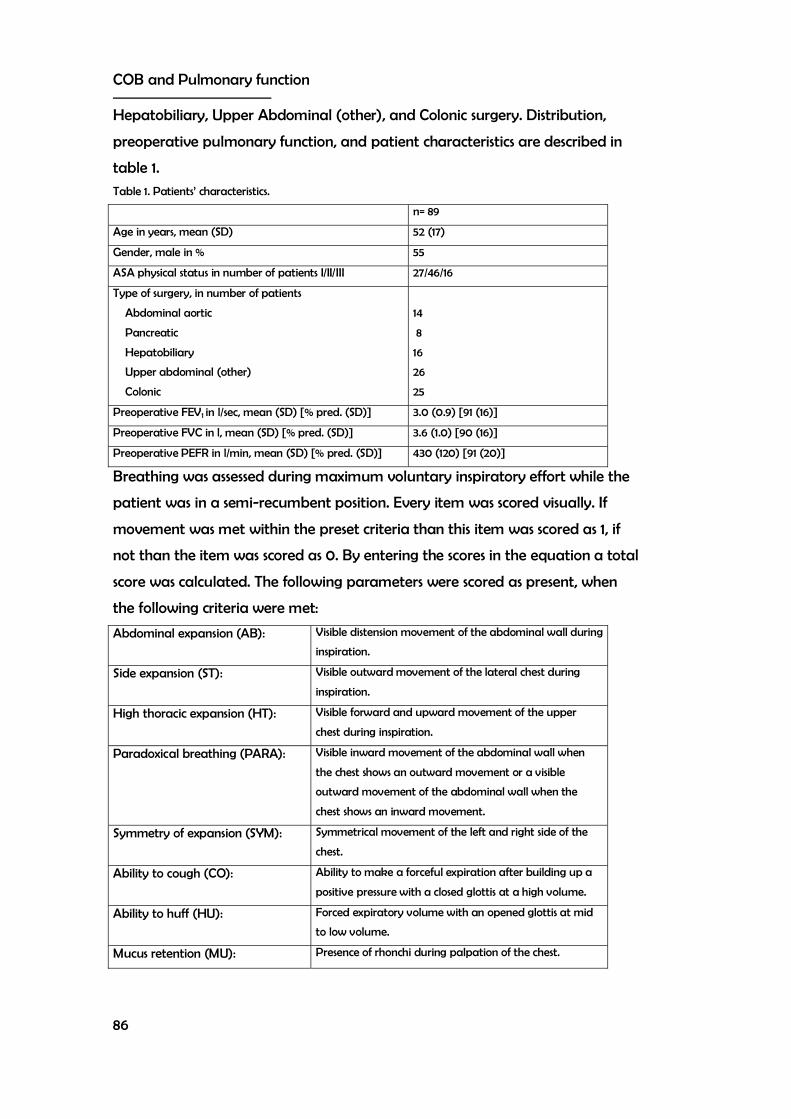
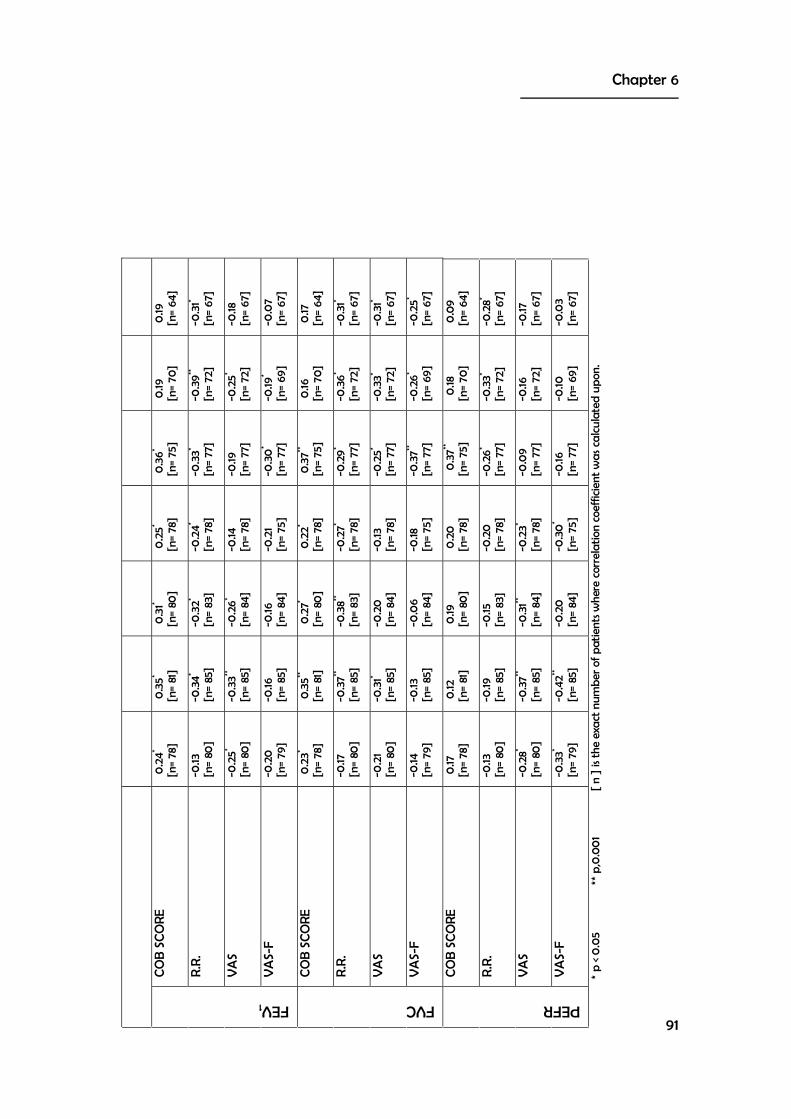
Chapter 6: 83 Are clinical observations of breathing and pulmonary function related in patients after abdominal surgery?
General discussion and conclusions 97
Summary 103
Samenvatting 113
Dankwoord 121
Previous dissertations Rehabilitation Programs Research 125 of the Northern Centre for Healthcare research
Chapter 1
3
Post-operative Mucus Clearance
Johannes P. van de Leur 1 and Linda Denehy 2
1 Center for Rehabilitation, University Medical Center Groningen, The Netherlands
2 School of Physiotherapy, Faculty of Medicine, Dentistry and Health Sciences, The University of Melbourne, Australia
Summarized from a chapter published in: Therapy for Mucus-Clearance Disorders, pp 503-552
Edited by Bruce K. Rubin and Cees P. van der Schans In the series of Lung Biology in Health and Disease volume 188 Exclusive editor Claude Lefant Marcel Dekker Inc, New York 2004
Post-operative mucus clearance
4
Introduction
Post-operative pulmonary complications were identified as early as 1910 by
Pasteur [1], who thought it was due to a failure of respiratory power. In 1914,
Elliot and Dingley [2] proposed that post-operative lung collapse was the result
of occlusion of the airways by mucus. Subsequent work [3-5] reported the
findings of post-operative hypoxia and lung collapse by shallow breathing after
laparotomy. Notwithstanding subsequent advances in surgery and supportive
medications, the morbidity resulting from post-operative pulmonary
abnormalities remains a significant problem. Dilworth and White [6] found an
overall incidence of post-operative pulmonary complications of 20.5%. But in
patients with pre-existing respiratory disease characterized by chronic sputum
production and airflow obstruction on spirometry, and those who were current
smokers, the incidence of post-operative pulmonary complications were as high
as 50 and 84%. These authors concluded that mucus hypersecretion is one of the
essential determinants of post-operative pulmonary complications [6].
The proposed mechanisms for pathogenesis of post-operative pulmonary
abnormalities have altered little since early 20th century. There are still two
basic theories to explain their occurrence: regional hypoventilation and stasis of
mucus [7-10].
Regional hypoventilation
There are several physiological factors that may contribute to alveolar closure;
these relate to reductions in functional residual capacity (FRC), and an altered
relationship between functional residual capacity and closing volume.
Following upper-abdominal surgery, the functional residual capacity has been
shown to decrease to approximately 70% of pre-operative value [11,12]. As
functional residual capacity falls below closing volume, closure of dependent
small airways may occur, leading to arterial hypoxemia as perfusion of airless
lung units persists [8,11]. This altered relationship may exist regionally in the lung,
even when overall functional residual capacity exceeds overall closing volume
[11,12]. The reduction in functional residual capacity has been shown to be closely
Chapter 1
5
associated with the degree of arterial hypoxemia after surgery [11]. The
consequences of the reduction in functional residual capacity are reduced lung
compliance, altered surfactant property [11], impaired gas exchange, retention
of lung secretions, and atelectasis [8].
The precise sequence and relative contributions of each of the above
mechanisms are still unclear. It is possible that they vary between patients. In
addition, it is possible that both alveolar hypoventilation and secretion plugging
coexist to contribute to post-operative lung changes [9].
Stasis of mucus
Advocates of the mucus-blockade theory contend that the primary cause of
atelectasis is the absorption of alveolar air, distal to a mucus plug in the
proximal airway, causing eventual collapse unless fresh air enters through
collateral channels [9].
Stasis of mucus may be a result of changes in the cardio-respiratory
physiology during the post-operative period. A multi-factorial approach (figure
1) may be used to explain the rationale for the prevention of post-operative
pulmonary complications by characterizing patient categories and type of
surgery. This approach may be used for setting up treatment hypotheses of
post-operative pulmonary complications.
Post-operative mucus clearance
6
Pre-operative morbidity
Increasing age is considered in most surgical literature to be a risk factor for
developing post-operative pulmonary complications. However, the definition of
the critical age varies between studies. Many papers report that an age over 60
years increases risk after surgery [13-15], while others found that an age greater
than 70 [16,17] or 75 years [18,19] is a significant risk factor. Not all studies
analyzing risk factors found age to be important [6,20-22]. The closing capacity
of the lungs increases with age [23] and as it rises above functional residual
capacity, closure of small airways can occur. In fact, after the age of
approximately 65 years, this occurs in normal adult lungs during quiet breathing
in a seated position [23,24].
Obesity and malnutrition are frequently studied as clinical risk factors for
post-operative pulmonary complications. Weight greater than 30% of ideal has
been linked to increased risk of post-operative pulmonary complications. More
recent research defined a Body Mass Index (BMI) of greater than 25 [14] or 27
[13] as a pre-operative risk factor. In these two studies, BMI was found to be a
significant pre-operative risk factor for post-operative pulmonary complications
when analyzed using multivariate statistics. Brookes-Bunn [13] reported that a
BMI greater than 27 kg/m2 increased patient’s risk of developing post-operative
pulmonary complications by a factor of 2.8. The physiological changes
associated with obesity that may account for increased post-operative risks are
a reduction in FRC, produced mainly as a result of decreased chest wall
compliance, and a lower than normal Pa02 [24]. The reduction in FRC post-
operatively is aggravated by the use of the supine position [25].
Malnutrition has been recognized as a risk factor for more than 50 years [26],
but has not been widely addressed in recent literature. Pre-operative protein
depletion may contribute to respiratory muscle weakness, leading to a
reduction in diaphragmatic muscle mass [27], loss of periodic sighing [28],
hypoventilation, and impaired immune-system function [29].
The components of cigarette smoking have major adverse effects on
cardiovascular and respiratory function as described by Pearce and Jones [30].
The effect of smoking history on the development of post-operative pulmonary
Chapter 1
7
complications however, remains somewhat uncertain. A large body of literature
supports the inclusion of cigarette smoking as a pre-operative risk factor [6,13].
Bluman et al. [32] even reported a fourfold increase in post-operative
pulmonary complications, in current- compared with never-smokers following
elective non-cardiac surgery. In contrast, some studies report no association
between smoking and increased risk of post-operative pulmonary complications
[16,33].
Pre-existing Chronic Obstructive Pulmonary Disease (COPD) is often
considered an important risk factor for post-operative pulmonary complications
[17,20,34]. It has been suggested that mucus hyper secretion is the important
factor that increases risk in these patients [23,36]. Other predictive markers
studied extensively in COPD are pulmonary-function test indices.
Surgery
General anesthesia, irrespective of the anesthetic agents used, result in a
reduction in functional residual capacity of the magnitude of 20% [11,36,37].
Alterations in the chest wall and reduced lung volumes seem to be most
important in the etiology of functional abnormalities following anesthesia.
Carryover of these changes may occur post-operatively, when several factors
conspire to further reduce lung volumes and affect gas exchange and
mucociliary clearance [38]. However, there is no evidence that general
anesthesia per se causes post-operative pulmonary complications [29]. It is
generally agreed in literature that abdominal surgery of longer than two hours
duration carry increased risk of post-operative pulmonary complications [26],
and that those longer than 4 hours are associated with a significant risk of post-
operative pneumonia in patients following upper abdominal surgery [21]. The
risk associated with duration of surgery may reflect the complexity of the
surgical procedure itself rather than the length of anesthesia administration
[33].
The site of surgery has been identified as having a major influence on the
risk of post-operative pulmonary complications [38,39]. Patients undergoing
upper-abdominal or thoracic surgery are at a higher risk of developing
respiratory problems compared to patients who are having surgery on the lower
Post-operative mucus clearance
8
abdomen or the extremities [11,21,38,40]. In recent comparative reviews the site
of surgery has also been identified as a significant risk factor [13,14]. Celli [34] in
fact, states that the site of surgery may be the single most important risk factor.
The wide variation that exists after surgery in spirometry may be explained by
different incision sites [11,12,43,44] and operation techniques. The influence of site
of surgery as a significant risk factor is explained predominantly by alterations in
diaphragmatic function caused by surgery performed in close proximity to the
diaphragm [33,45]. Ford et al. [43] demonstrated that the diaphragmatic
contribution to tidal ventilation was reduced following upper-abdominal
surgery in 15 subjects who underwent open cholecystectomy. Blaney and Sawyer
[46] measured diaphragm displacement before and after upper-abdominal
surgery in 18 subjects, using ultrasonography, and found that mean diaphragm
displacement was reduced by 57% on the first day after surgery. Dureuil et al.
[47] reported significantly less diaphragm dysfunction in lower- compared to
upper-abdominal surgery. These authors postulated that a decrease in
diaphragmatic motion following upper-abdominal surgery might result in
diminished ventilation and expansion of the dependent lung zones. Pansard et
al. [48] found diaphragm inhibition in patients after upper-abdominal surgery
as measured by changes in diaphragmatic pressure and excursion of the chest
and abdomen. These authors suggested that inhibition of the phrenic nerve was
mainly a result of post-operative analgesia. The loss of diaphragm function also
occurs in minimally invasive surgery. Erice et al. [49] described changes in
maximum trans-diaphragmatic pressure after laparoscopic abdominal surgery.
The authors therefore, posed a second hypothesis of loss of diaphragmatic
function through stimulation of the mesenteric plexus. This hypothesis was
originally discussed by Reeve et al. [50]. However, the primary cause of post-
operative dysfunction appears to be the chest as site of surgery, which causes
reflex inhibition of the diaphragm and intercostal muscles [47,51,52]. Another
possible explanation may be increased intra-abdominal pressure because of
abdominal distension, which may limit normal diaphragmatic function [9].
Pulmonary complications following thoracic surgery relate to both the site of
incision and the removal of previous healthy lung tissue [29]. A vertical
laparotomy has been reported to increase morbidity compared to subcostal or
Chapter 1
9
transverse incisions [53]. Although median sternotomy for cardiac surgery has
been reported to have less impact on respiratory function than thoracotomy or
abdominal incisions; the effects of the cardiac surgical process may increase the
risk of developing post-operative pulmonary complications [52,54,55]. Left-
lower-lobe abnormality is a frequent finding after cardiac surgery [54,56]. The
reasons are unclear, but factors that may be of influence are diaphragmatic
dysfunction, lung trauma due to retraction, compression of the left-lower-lobe
by the heart during surgery, and pleurotomy [54].
Pain and pain control
The severity of post-surgical pain may depend on the type and site of surgery,
age of the patient and their individual response to the stress of the operation;
perhaps due to the patient's personality, previous pain experience, cultural
background, and conditioning. As in acute pain, post-operative pain is often
accompanied by changes in autonomic activity that is largely sympathetic and
may consist of hypertension, tachycardia, sweating, and decreased gut motility.
Most research measures a patient’s estimate of the severity of their pain.
Literature measuring the peri-operative incidence of post-operative pulmonary
complications and methods used in its reduction often report on a patient’s pain
by using verbal rating scales or visual analogue scales (VAS). Of these, the VAS is
the best established. Pain reduces with the natural healing process [57].
Reduction in post-operative pain intensity is essential for patient comfort but
also for reducing the incidence of severe or life-threatening post-operative
pulmonary complications. Sabanathan et al. [58] suggested that pain in the
early post-operative period may be the factor most responsible for ineffective
ventilation. More recent developments in pain management include the
introduction of post-operative pain services led by anesthetists or nurses,
recognition of the possible value of pre-emptive analgesia [59,60], use of
multimodal analgesic techniques rather than single-drug administration, more
sophisticated drug administration techniques such as patient-controlled
analgesia, and use of the epidural route on surgical wards. Perhaps in future
new developments in pain management will result in higher pulmonary
function and less pulmonary complications.
Post-operative mucus clearance
10
Ineffective cough
Leith [61] and Bouros [62] defined a cough as a complicated maneuver. An
effective cough is important for transport and expectoration of lung mucus.
Several elements contribute to the efficiency of the cough [62]. Primarily, it is
believed to be a function of peak airflow velocities in the airways. Several
elements may participate in producing the initial transient supramaximal flows
[63] that are characteristic of a cough: initial high lung volume, muscle-
generated pulmonary pressures, coordinated glottis participation, and airway
compression resulting in adequate expiratory flow.
Initial high lung volume
The initial high lung volume during cough has several effects. Greater
expiratory-muscle pressure and higher expiratory flow rate are achievable. Post
abdominal or thoracic surgery lung inspiratory volumes are reduced to initially
50% of pre-operative value [12]. This may influence the efficacy of coughing.
Muscle-generated pulmonary pressures
Adequate musculoskeletal function and pulmonary compliance must be
present for an efficient cough. Pressures generated are variable and limited by
age, gender, and physical condition [64]. In the peri-operative phase, these
pressures may be reduced [49]. Two limiting factors for the production of
pulmonary pressures must be considered in the peri-operative phase. First, the
velocity of shortening of expiratory muscles can be regarded as depending on
the rate of change of thoracic gas volume. Second, peak pressures are reached
after a substantial volume has been expired in combination with the closure of
the glottis or mouth. Higher lung volumes have an advantage in production of
peak pressures due to better muscle force-length relationship and geometry. In
the peri-operative phase, these two factors are relevant, but their effect is
limited. The abdominal muscles are more active during anesthesia in a non-
paralyzed patient. However, this activity has no significant effect on the
functional residual capacity post-surgery [65]. Some of the diaphragm muscle
function may be regained by administration of medication, such as
aminophylline [66,67].
Chapter 1
11
High expiratory flow is generated through the interaction of respiratory
muscle function and gravitational forces acting on the skeletal system. In the
post-operative phase, the diaphragmatic pressures are decreased by 22 ± 16%
according to a study by Pansard et al. [48]. In the post-operative phase,
expiratory flow may therefore be limited.
Coordinated glottis participation
Among the most interesting aspects of expiratory flow during a cough are those
associated with the extremely rapid collapse of intrathoracic airways when the
glottis opens. As the equal pressure point migrates upstream in the intrathoracic
airways, negative transmural pressures are applied to airways downstream
from it. The resulting dynamic compression accounts for most of the airway
volume change. In contrast, flow from the parenchyma is sustained over time,
falling relatively slowly as lung volume decreases. The timing of the rise of flow
from the parenchyma is uncertain. Effective lung clearance is not entirely
dependent on glottis closure. Further in this chapter clearing lower airways by
sharp forced expiration without glottis closure will be discussed.
Airway compression
Airway compression results in adequate expiratory flow during breathing,
airways narrowing during coughing, and dynamic compression and contraction
of smooth muscle occurring in the airway walls. This dynamic collapse of airways
contributes to increased flow velocities. Persistent coughing, however, can
precipitate wheezing and reduce expiratory flow, and may provoke asthma in
susceptible patients. As a result of anesthesia, the airway caliber is reduced. The
airway may therefore further increase in resistance and related obstruction.
Dynamic compression [68] of the intrathoracic airway is undoubtedly an
essential part of an effective cough, as compression makes it possible for the
high kinetic energy of the expiratory flow to shift material from the airway wall.
The potential kinetic energy of flowing gas may not change, except in coronary
artery surgery, when the force-velocity behavior of expiratory muscle is
changed. After abdominal surgery a decrease in maximum flow might occur.
The reductions of, for instance, peak expiratory flow rate could also be
explained by an impairment in the voluntary contraction of the abdominal
muscles or reduced motivation due to fear of pain. Cotes [69] and Nunn [70]
Post-operative mucus clearance
12
describe peak expiratory flow as having an effort-dependent element due to
many inhibiting factors, including motivation and muscular force. Therefore,
during the post-operative phase patients might be restrained in producing
maximal flows, which are needed to cough. A change in muscle force-length
relationships may also be involved.
Impaired broncho-elevation of mucus
Mucociliary clearance is a major function of the airway epithelium. The
respiratory epithelium consists of cilia, which contribute to the normal elevation
of mucus, bacteria, and debris. Gamsu et al. [71] measured clearance of
tantalum, a low radioactive powder, which adheres to airway mucus. Patients
experienced delayed clearance of the tantalum after abdominal but not after
orthopedic surgery. Pooling of tantalum powder always occurred in the region
of the lung where volume loss was evident. They concluded that impaired
mucociliary function and mucus transport are implicated in post-operative
atelectasis and that lung volume is important in mucociliary clearance. These
authors [71], and others [3,8,72], suggest that the cumulative effects of the peri-
operative process present a significant insult to mucus clearance.
Intubation and ventilation of the patient during and after surgery will influence
the internal milieu, by providing a bypass of the vocal cord and introducing
foreign substances such as anesthetic gasses. Endotracheal suctioning is an
intervention to remove accumulated mucus from the endotracheal tube,
trachea or lower airways. During intubation or endotracheal suctioning the
normal barrier is bypassed, the lower airway is opened for an intrusion of
bacteria, viruses, yeasts, and other foreign substances. Several of these post-
operative factors may contribute to the development of lower-airway infection
that in itself may contribute to impaired mucociliary transport. Impaired
mucociliary transport in intubated patients is associated with loss of cilia rather
than ultra structural abnormalities of cilia [73]. A cause of loss of cilia function
may be the mechanical trauma during endotracheal suctioning by introducing
a suction catheter in the trachea and main bronchi and applying negative
pressure. An old study by Plum and Dunning [74] described 25 tracheostomy
patients having had routinely endotracheal bronchial suctioning. They described
Chapter 1
13
extensive damage caused by this procedure. In a post-mortem follow-up of
eight of these patients, erosion of cartilage and smooth muscle surface was
found. Different types of suctioning catheters did not change the prevalence of
bronchial trauma [75]. In an animal study by Czarnik, no change in bronchial
trauma was found between intermittent and continuous suction techniques
[76]. During an endotracheal suctioning procedure, described by the American
Association for Respiratory Care, the patient is manually hyper inflated and
hyper oxygenated [77]. An increase in ciliary beat frequency with different
concentrations of oxygen at normobaric pressures has been observed in vitro by
Stanek et al. [78]. This effect might influence the efficacy of ciliary beat and
therefore impair mucus transport. In the peri-operative phase, there might be a
combination of effects on ciliary beat. Because of medical interventions during
surgery, the bronchociliary elevator can be impaired for a period ranging from 2
to 6 days post-operatively [71].
Changes in mucus production
Respiratory mucus represents the products derived from secretion of the
submucosal glands and the goblet cells. The relationship between humidity and
temperature of inspired gas and function of the airway mucosa, suggests there is
an optimal temperature and humidity above and below of which there is
impaired mucosal function. This optimal level of temperature and humidity is
core temperature and 100% relative humidity. However, existing data are only
sufficient to test this model for gas conditions below core temperature and 100%
relative humidity. The data concur with the model in that region. No studies
have yet looked at this relationship beyond 24 hours.
The main factors contributing to abnormalities in mucus clearance
during the post-operative phase are flow reduction and decreased relative
humidity. This could lead to changes in the mucus viscosity and accumulation of
mucus. In theory, if it progresses this might lead to obstruction of airways,
plugging, atelectasis, and gas exchange abnormalities.
Post-operative mucus clearance
14
Effect of mucus evacuating techniques on peri-operative respiratory
function
Rationale for mucus evacuating techniques
In 1910, Pasteur [1] described in elegant detail, several different types of post-
operative pulmonary complications. Although pulmonary treatment regimens
were not defined, Pasteur stated in his concluding words that the deficiency of
inspiratory power would occupy an important position in the search and
determination of causes of post-operative lung complications. Beecher [4]
confirmed this in laparotomy patients in 1933. The confirmation of the inhibitory
reflex was studied by Reeve et al. [50] in 1951. Several improvements have
taken place in post-operative care. Mechanical ventilation has changed from
volume controlled, to patient triggered pressure controlled. This improvement
may be responsible for a reduction in mucus production and retention. In the
1950’s endotracheal suctioning was a non-sterile procedure, with an orange
rubber tube, that was re-used after cleansing and drying at the bedside.
Nowadays endotracheal suctioning is a sterile procedure with single use,
transparent plastic catheters. This improvement may have been responsible for
a reduction in pneumonia and pulmonary infection. With respect to post-
operative lung complications after the intubation phase, breathing exercises,
concentrating on inspiratory volume and expiratory techniques, could be
essential elements in the prevention and treatment of problems of mucus
clearance. One of the earliest publications regarding increasing inspiratory effort
through breathing exercises and manual control during expiratory maneuvers
such as coughing was described by MacMahon in 1915 [79].
A review of well-recognized physiological changes of the post-operative
period provides empirical support for the role of physiotherapy treatment to
prevent or minimize hypoventilation and secretion plugging. Supporting
evidence for this role was provided almost 50 years ago [80]. Since then, several
randomized controlled trials have reported beneficial effects of prophylactic
physiotherapy in reducing the incidence of post-operative pulmonary
complications following major surgery [40,81-85]. In contrast, several other
studies report no additional benefit of prophylactic physiotherapy [56,86,87] .
Chapter 1
15
Respiratory physiotherapy may include pre-operative assessment and
education and post-operative management. Many physiotherapy techniques
may be used in treatment of patients after surgery, with the primary aims of
improving lung ventilation, clearing excess secretions, and thereby minimizing
the risk of post-operative pulmonary complications. These may include
endotracheal suctioning with or without additional airway-clearance
techniques, deep-breathing strategies, forced expiratory maneuvers and
mobilization.
Several studies suggest that pre-operative education alone may be
sufficient for patients having upper-abdominal surgery. A change in patient
management in many centers is the use of pre-admission clinics. Patients visit
the hospital as outpatients for admission details and information up to 1 to 3
weeks before surgery. They are then admitted as inpatients on the day of
surgery. If patients, undergoing upper-abdominal surgery or cardiothoracic
surgery, benefit from pre-operative physiotherapy, the physiotherapist needs to
be involved in the pre-admission of these patients. Research, particularly in
cardiac surgical patients, has shown positive peri-operative benefits from pre-
admission education [88,89]. It is essential that more research should be
performed in the identification of pre-operative risk factors, developing a risk-
factor model for clinical use and examining the efficacy of post-operative
physiotherapy in specific patient populations (especially thoracic and
esophageal surgery) using a no-treatment control group and multi-center
research if possible. More comparative research, including the use of no-
treatment control groups, is necessary to evaluate the specific continuing role of
physiotherapy for patients following major surgery. Furthermore, the
comparative efficacy of physiotherapy interventions, especially in relation to
mucus clearance, needs to be evaluated.
During the pre- and early post-operative phase patients are usually
intubated. Intubated patients have a tendency to retain mucus due to a
combination of various reasons: obstruction in mucus transport due to
ineffective cough, impaired broncho elevation of mucus (endotracheal tube,
mechanical ventilation, damaged cilia, reduced flow) and changes in mucus
Post-operative mucus clearance
16
production (increased amount or reduced viscosity). In these circumstances
endotracheal suctioning is usually performed.
In 1993, the American Association for Respiratory Care [77] described a
consensus guideline in performing endotracheal suctioning. This intervention
consists of patient preparation, the suction procedure and patient monitoring.
The patient’s preparation may include hyper oxygenation, with 100% oxygen,
longer than 30 seconds prior to the suctioning procedure. This could be
accomplished by adjustment of the mechanical ventilator or by manually
ventilating the patient with a resuscitation bag.
Manual hyperinflation as described by the American Association for
Respiratory Care [77] defined manual hyperinflation in the guideline for
endotracheal suctioning as a technique to hyperventilate with a resuscitation
bag by an increased rate and/or tidal volume. The goal of using manual
hyperinflation is to maintain oxygenation, to facilitate a sigh, to increase
expiratory flow rate [90], to increase sputum clearance [91] and to increase
inspiratory volume [91,92]. In a survey of manual hyperinflation in Australian
hospitals, Hodgson found that in 91% manual hyperinflation was used as a
physiotherapy treatment technique [93]. In a vitro setting, Maxwell et al. [90]
found that if PEEP was maintained by bag compression, a reduction in
expiratory flow rate was found. Clarke [94] suggested the increased potential of
baro-trauma during manual hyperinflation.
To increase expiratory flow manual chest wall compression can be
applied in conjunction with manual hyperinflation. In the rational on improving
expiratory flow, the technique of manual chest wall compression may be an
adjunct to the treatment rational, but in clinical practice, this technique may
oppose some problems in post-thoracic and abdominal surgery patients. To our
knowledge, data on chest wall compression with or without manual
hyperinflation has never been published.
The entire suctioning procedure, as well as the placement of a suction
catheter through an artificial airway into the lower airway, trachea and right or
left main bronchus, should be deployed as a sterile technique. Negative pressure
is applied as the catheter is being withdrawn from the airway. The duration of
each pass of a suction catheter into the artificial airway should be 10–15 seconds.
Chapter 1
17
Suction pressures should be as low as possible, to clear secretions effectively.
Indications are listed in this guideline:
coarse breath sounds or noisy breathing,
increased peak inspiratory pressures or decreased tidal volumes,
visible secretions in the airway,
changes in flow or pressure,
suspected aspiration,
clinically increased work of breathing,
deterioration of arterial blood gas values,
radiological changes consistent of mucus retention,
the need to obtain a sputum specimen,
the need to maintain patency and integrity of the artificial airway,
the need to stimulate a cough, and
presence of pulmonary atelectasis or consolidation.
Patient monitoring should consist of auscultation, interpretation of vital signs,
characteristics and ventilator parameters. These clinical “data” should be
monitored prior, during and after endotracheal suctioning to indicate and
evaluate the procedure. Evidence in literature for the indication to perform
endotracheal suctioning is not clear. The rationale for this intervention is to
maintain airway patency and reduce pulmonary complications. The assessment
for the indication to perform endotracheal suctioning should be clinically based
on objective indications and should include patient/ventilator system
interaction. Prevention of pulmonary infections and maintenance of airway
patency are cited as possible benefits. However, there are no clinical trials to
support these assumptions.
In 1976, Lefrock et al. [95] described a clinical trial of 68 patients, without
patient specifications, a prevalence of 26% infection rate. Similar prevalence
was described by Deppe et al. [96] in 1990, comparing two treatments in 84
patients. In a vitro study of 10 endotracheal tubes, Hagler [97] described that
the introduction of a suction catheter transported 60.000 colonies of bacteria to
the lower airways and the use of saline instillation transported 300.000 colonies
of bacteria to the lower airways. In theory this suggests that invading the lower
Post-operative mucus clearance
18
airways may be beneficial, but may also introduce a risk factor for pulmonary
complications.
Endotracheal suctioning may have undesired adverse effects: several
studies have reported cardiac arrhythmia [98] and oxygen desaturation [99-
101] during suctioning. Cardiac arrhythmia was seen by Stone et al. [98] during
suctioning in 26 patients post cardiac surgery. Adlkofer and Powaser [99]
reported a decrease in oxygen tension of 20 mmHg in 64 patients post cardiac
surgery. Eales [100] found a decrease in oxygen tension after suctioning of 12
mmHg. Brown et al. [101] described an oxygen desaturation of more than 4% in
a medical population of 22 patients. Several studies have reported the
discomfort of endotracheal suctioning in ICU patients [102-104]. These studies
show that endotracheal suctioning is remembered by at least 40% of the ICU
population. Evaluation of effects of endotracheal suctioning based on the
recollection and memory of patients is difficult because the recollection and
memory of this period is varied. Studies describing memories of the ICU period in
general describe a large population with no recollection, but also patients with
hallucinations or with detailed facts.
The use of additional specific airway-clearance techniques, like postural
drainage and percussion etc., may have limited value because of post-operative
pain and incision site. Patients with suppurative lung disease are at high risk of
developing post-operative pulmonary complications. These patients should be
assessed and treated by a physiotherapist in the immediate pre-operative
period, with the aim of reducing secretion volume. In these patients, it may be
necessary to delay surgical intervention to mid-morning in order to allow
clearance of secretions prior to anesthesia [105]. Close post-operative monitoring
is essential and effective analgesia is vital (even after minor procedures) to
enable patients to perform airway-clearance techniques [105]. The addition of
humidified supplemental oxygen may also be of benefit to this patient group,
both intra- and post-operatively [105,106], because reduced humidification
alters ciliary function [107]. Nebulized saline, and in some cases bronchodilators,
following surgery may be helpful in improving secretion clearance [106]. In
general however, the use of airway-clearance techniques is less common
following surgery for patients without suppurative lung disease.
Chapter 1
19
After the intubation phase patients need to maintain sufficient lung
volume to avoid pulmonary complications. To maintain sufficient lung volume
deep-breathing exercises could be used to increase the level of breathing above
closing capacity, a level where airways collapse. Deep-breathing strategies
aiming to improve lung volume are performed from functional residual
capacity to total lung capacity. They are aimed at increasing lung volume,
redistributing ventilation, improving gas exchange, increasing thoracic
movement, and helping in secretion mobilization [108]. These have been the
mainstay of physiotherapy for this patient group. The exercises commonly used
are directed at thoracic expansion exercises, diaphragmatic breathing and
sustained maximal inspiration.
Most deep-breathing exercises may also be used in combination with
gravity-assisted drainage and forced expiratory maneuvers. Variations in
inspiratory flow are thought to alter the distribution of ventilation [108]. To
improve ventilation to dependant lung regions, which are the most affected
following major surgery, a slow inspiratory flow is recommended. As lung
volume increases, the influence of flow on distribution of ventilation is reduced
[108]. Based on a study by Ferris and Pollard, the number of maximal
sequential breaths needed for physiological effects is thought to be five,
performed once every waking hour [109]. The time spent on breathing exercises
and respiratory maneuvers described as most beneficial is reported to be
approximately 20 minutes [84]. Blaney and Sawyer [46] studied diaphragmatic
motion using ultrasonography in 18 patients following upper-abdominal surgery.
The authors compared three breathing strategies with the patients sitting,
receiving verbal instruction to take only deep breaths, and coached in
diaphragmatic breathing and thoracic expansion exercises pre- and post-
operatively. Results showed a significant increase in diaphragmatic excursion
following surgery when the two tactile, or “hands-on”, breathing techniques
were compared with verbal instruction alone [46]. The addition of a 3-second
breath hold at total lung capacity has been recommended [110,111]. A sustained
maximal inspiration mimics a sigh or yawn and aims to increase
transpulmonary pressure [111]. It may also allow time for alveoli with slow time
constants to fill. Redistribution of gas into areas of low lung compliance utilizing
Post-operative mucus clearance
20
collateral ventilation pathways and lung interdependence may re-expand
collapsed alveoli [110,112]. If regional ventilation is reduced as a result of
secretion plugging, the re-expansion of collapsed alveoli may allow air to move
behind the secretions and assist their removal using forced expiration techniques
[113,114].
Incentive spirometry was developed to stimulate the patient to perform
deep-breathing exercises under supervision or independently. Various inspiration
devices have been invented to stimulate the patient visually to increase the
total lung capacity, either by marking the inspired volume in liters (or ml), or by
transporting one or more balls on inspired flow. Thruvol (Argyle Sherwood
Medical, USA) Coach (DHD, USA), and Airlife (Allegiance, USA) are examples of
incentive spirometers used in clinical situations. Different devices all aim to
stimulate the patient to increase inspiration and breathe better and avoid
pulmonary complications. Incentive spirometry volumes underestimate the
maximum inspiratory capacity. The incentive spirometers with a low flow rate
tend to use less work of breathing compared to the flow activated incentive
spirometers.
Many conflicting articles have been written about its physiological effects
[115-120] or absence of them [121-123]. Other benefits such as cost-effectiveness
have been described by Hall et al. [14] and refuted by Denehy et al. [124] and
others [125,126]. The use of incentive spirometry has been evaluated in different
patient categories such as those undergoing cardiac surgery and in a pediatric
population [127,128]. Many questions regarding its effectiveness remain
unanswered. The patient category most likely to benefit from this tool are high-
risk patients, after thoracic or upper-abdominal surgery [121,129]. In a recent
well-designed study, it was reported that the addition of incentive spirometry to
physiotherapy, including deep-breathing exercises and early mobilization, in 67
patients did not significantly alter the incidence of post-operative pulmonary
complications following thoracic and esophageal surgery [130].
Evidence supporting their efficacy in achieving these aims is scant [131-
133] and often conflicting. However, O'Donohue [134] and Celli [33] both stress
the importance of regular maximal inspirations in a prophylactic peri-operative
treatment regimen, whereas others question the need to include breathing
Chapter 1
21
exercises at all [56,135]. The effects of breathing exercises, in isolation, in aiding
secretion clearance, have not been studied. The efficacy of deep-breathing
strategies in clinical practice for reducing post-operative morbidity has been
studied by several authors. Different methods of post-operative prophylaxis
have been compared. It seems apparent from these studies that different
breathing strategies may be equally effective in thoracic patients [123,136,137]
and in abdominal patients [24,44,56,86] and that some form of deep breathing
is better than no intervention [33,81,84] in minimizing the incidence of post-
operative pulmonary complications.
With respect to expiratory techniques, like huffing and coughing, little
research exists that compares the efficacy of mucus-mobilizing techniques in the
post-operative phase. Forced expiration is one technique used for mobilizing
and expectorating excess bronchial secretions [114]. The technique incorporates
one or two forced expirations (huffs) and breathing control. Extensive
information outlining the definition and efficacy of this technique has been
published [114,138]. Much of this research was performed in medical patients
with copious secretions. The specific role of the forced expiratory technique in the
management of patients after surgery has not been studied. Many studies
support its efficacy in clearing excess secretions. However, teaching the correct
performance of the huff from mid-to-low lung volume with the glottis open
may be best done pre-operatively. Coughing with wound support should be
encouraged as part of any prophylactic treatment regimen following major
surgery.
The cardiovascular and respiratory effects of immobility and bed-rest
have been well documented [131,139-141]. These include reduced lung volumes
and capacities, especially functional residual capacity; reduced Pa02; decreased
V02 max, cardiac output, and stroke volume; increased heart rate; and
orthostatic intolerance [139]. A model of the interaction between pulmonary,
cardiac and muscular function was described by Wasserman [142].
The goal of ambulation of post-operative patients is exercise at a level
sufficient to increase minute ventilation and cardiac output, within safe
physiological limits [140]. Given the previously described physiological changes
associated with major surgery, a technique that can increase ventilation may
Post-operative mucus clearance
22
improve outcome in this patient group. Effective analgesia is necessary in order
to actively ambulate patients [58]. It has long been recognized that body
position affects respiratory parameters [143,144]. Adoption of the upright
position and increased tidal volumes may aid in recruitment of alveoli in
dependent lung zones, improve ventilation/perfusion (V/Q) matching, and
promote secretion evacuation [140,145].
Several studies have examined the efficacy of this technique in isolation.
Dull and Dull [146] and Jenkins et al. [147] advocate early ambulation in the
respiratory prophylaxis of patients following coronary artery surgery. No
additional benefits of breathing exercises or incentive spirometry were found in
either study. Hallböök et al. [136] reported similar results in patients following
cholecystectomy. Wolff et al. [148] studied the effects of exercise
hyperventilation compared with eucapnic hyperventilation using radioactive
isotopes in normal subjects. The authors reported a significant improvement in
secretion evacuation with exercise hyperventilation.
Summarizing, post-operative mucus clearance techniques should be used
to target high-risk patients (increasing age, history of respiratory disease,
morbidly obesity, cardiothoracic or upper-abdominal surgery) as the literature
to date suggests. The type, dosage, and frequency of post-operative
physiotherapy techniques in the Intensive Care Units utilized in different
countries (and within the same country) also vary significantly [149,150]. Within
Europe large differences occur between the work field of physiotherapists [149].
It seems that many methods of treatment may be effective for prophylaxis, and
the specific method used will ultimately depend on individual patients’ needs,
available resources [33], and, to some extent, the training and experience of the
physiotherapist.
Outcome measures used to test the efficacy of techniques used by
physiotherapists vary considerably, as does the definition of the same outcome
across numerous studies. Reassessment after surgery may be required to assess
post-operative risk factors (pain levels, ambulation). Ambulation should be
encouraged as soon as possible following surgery. Patients may need respiratory
physiotherapy management for 1 or 2 days after surgery.
Chapter 1
23
Post-operative mucus clearance in patients after high-abdominal and thoracic
surgery is daily routine. Our daily routine needs to be evaluated especially
during and after the intubated phase. Evidence based literature describes little
indications on endotracheal suctioning. The following questions were to be
answered:
1: Is an on-demand procedure of minimally invasive airway
suctioning bio-equivalent in ICU outcome compared to routine
procedure of endotracheal suctioning without its undesirable side
effects?
2: What is the difference in recollection during routine endotracheal
suctioning and minimally invasive airway suctioning?
3: What is the difference in stress-hormonal response in ICU patients
to the two procedures of airway suctioning; routine endotracheal
suctioning and minimally invasive airway suctioning?
4: What is the discomfort and memory of facts recalled by patients
post ICU stay?
5: Is the clinical observation of breathing and pain predictive for the
decline of pulmonary function in post surgical patients?
Reference list
1. Pasteur W: Active lobar collapse of the lung. Lancet 1910, 1080-1083. 2. Elliot TR, Dingley LA: Massive collapse of the lungs following abdominal operations.
Lancet 1914, 1305-1309. 3. Haldane J, Meakins J, Priestly J: The effects of shallow breathing. Journal of Physiology
1919, 52, 433-453. 4. Beecher H: The measured effect of laparotomy on the respiration. Journal of Clinical
Investigation 1933, 12: 639-658. 5. Dripps R: Post-operative atelectasis and pneumonia. Annals of Surgery 1946, 124, 94-
110. 6. Dilworth JP, White RJ: Post-operative chest infection after upper abdominal surgery: an
important problem for smokers. Respiratory Medicine 1992, 86: 205-210. 7. Bartlett RH: Pulmonary pathophysiology in surgical patients. Surgical Clinics North
America 1980, 60: 1323-1338. 8. Fairshter RD, Williams JHJ: Pulmonary physiology in the post-operative period. Critical
Care Clinics 1987, 3: 287-306. 9. Marini JJ: Post-operative atelectasis: pathophysiology, clinical importance and principle
of management. Respiratory Care 1984, 29: 516-528. 10. Pierce AK, Robertson J: Pulmonary complications of general surgery. Annual Review
Medicine 1977, 28: 211-221. 11. Ali J, Weisel RD, Layug AB, Kripke BJ, Hechtman HB: Consequences of post-operative
alterations in respiratory mechanics. American Journal Surgery 1974, 128: 376-382. 12. Craig DB: Post-operative recovery of pulmonary function. Anesthesia and Analgesia
1981, 60: 46-52.
Post-operative mucus clearance
24
13. Brooks-Brunn J: Predictors of post-operative pulmonary complications following abdominal surgery. Chest 1997, 111: 564-571.
14. Hall JC, Tarala RA, Hall JL, Mander J: A multivariate analysis of the risk of pulmonary complications after laparotomy. Chest 1991, 99: 923-927.
15. Jackson CV: Pre-operative pulmonary evaluation [see comments]. Archives of Internal Medicine 1988, 148: 2120-2127.
16. Calligaro KD, Azurin DJ, Dougherty MJ, Dandora R, Bajgier SM, Simper S: Pulmonary risk factors of elective abdominal aortic surgery. Journal of Vascular Surgery 1993, 18: 914-920.
17. Kroenke K, Lawrence VA, Theroux JF, Tuley MR, Hilsenbeck S: Post-operative complications after thoracic and major abdominal surgery in patients with and without obstructive lung disease. Chest 1993, 104: 1445-1451.
18. Cullen DJ, Apolone G, Greenfield S, Guadagnoli E, Cleary P: ASA Physical Status and age predict morbidity after three surgical procedures [see comments]. Annals of Surgery 1994, 220: 3-9.
19. Mendes-da CP, Lurquin P: Gastrointestinal surgery in the aged. British Journal of Surgery 1993, 80: 329.
20. Williams-Russo P, Charlson ME, MacKenzie CR, Gold JP, Shires GT: Predicting post-operative pulmonary complications. Is it a real problem? Archives of Internal Medicine 1992, 152: 1209-1213.
21. Garibaldi RA, Britt MR, Coleman ML, Reading JC, Pace NL: Risk factors for post-operative pneumonia. American Journal of Medicine 1981, 70: 677-680.
22. Wightman JA: A prospective survey of the incidence of post-operative pulmonary complications. British Journal of Surgery 1968, 55: 85-91.
23. Leblanc P, Ruff F, Milic EJ: Effects of age and body position on "airway closure" in man. Journal of Applied Physiology 1970, 28: 448-451.
24. Jenkins S. Pre-operative and post-operative physiotherapy; are they necessary? Pryor J. Respiratory Care. 7, 147-168. 1991. London, Longman Group.
25. Ridley S. Surgery for adults. Pryor J. and Webber B. Physiotherapy for respiratory and cardiac problems. 295-327. 1998. London, Churchill Livingstone.
26. Windsor JA, Hill GL: Risk factors for post-operative pneumonia. The importance of protein depletion. Annals of Surgery 1988, 208: 209-214.
27. Arora NS, Gal TJ: Cough dynamics during progressive expiratory muscle weakness in healthy curarized subjects. Journal of Applied Physiology 1981, 51: 494-498.
28. Rosenbaum S, Askanazi J, Hyman A, Silverberg P, Milic-Emili J, Kinney JM. Respiratory patterns in profound nutritional depletion. Anesthesiology 1982, 51 S 36.
29. Luce JM: Clinical risk factors for post-operative pulmonary complications. Respiratory Care 1984, 29, 484-491.
30. Pearce AC, Jones RM: Smoking and anesthesia: pre-operative abstinence and peri-operative morbidity. Anesthesiology 1984, 61: 576-584.
31. Kocabas A, Kara K, Ozgur G, Sonmez H, Burgut R: Value of pre-operative spirometry to predict post-operative pulmonary complications. Respiratory Medicine 1996, 90: 25-33.
32. Bluman LG, Mosca L, Newman N, Simon DG: Pre-operative smoking habits and post-operative pulmonary complications [see comments]. Chest 1998, 113: 883-889.
33. Celli BR: Peri-operative respiratory care of the patient undergoing upper abdominal surgery. Clinics in Chest Medicine 1993, 14: 253-261.
34. Ephgrave KS, Kleiman WR, Pfaller M, Booth B, Werkmeister L, Young S: Post-operative pneumonia: a prospective study of risk factors and morbidity. Surgery 1993, 114: 815-819.
35. Gracey DR, Divertie MB, Didier EP: Pre-operative pulmonary preparation of patients with chronic obstructive pulmonary disease: a prospective study. Chest 1979, 76: 123-129.
36. Richardson J, Sabanathan S: Prevention of respiratory complications after abdominal surgery. Thorax 1997, 52 Suppl 3: S35-S40.
37. Juno J, Marsh HM, Knopp TJ, Rehder K: Closing capacity in awake and anesthetized-paralyzed man. Journal of Applied Physiololgy 1978, 44: 238-244.
38. Tisi GM: Pre-operative evaluation of pulmonary function. Validity, indications, and benefits. American Review Respiratory Disease 1979, 119: 293-310.
39. McKeague H, Cunningham AJ: Post-operative respiratory dysfunction: is the site of surgery crucial? [editorial; comment]. British Journal of Anaesthesiology 1997, 79: 415-416.
Chapter 1
25
40. Celli BR, Rodriguez KS, Snider GL: A controlled trial of intermittent positive pressure breathing, incentive spirometry, and deep breathing exercises in preventing pulmonary complications after abdominal surgery. American Review Respiratory Disease 1984, 130: 12-15.
41. Cain HD, Stevens PM, Adaniya R: Pre-operative pulmonary function and complications after cardiovascular surgery. Chest 1979, 76: 130-135.
42. Seymour DG, Pringle R: Post-operative complications in the elderly surgical patient. Gerontology 1983, 29: 262-270.
43. Ford GT, Rosenal TW, Clergue F, Whitelaw WA: Respiratory physiology in upper abdominal surgery. Clinics of Chest Medicine 1993, 14: 237-252.
44. Johnson WC: Post-operative ventilatory performance: dependence upon surgical incision. American Surgeon 1975, 41: 615-619.
45. Latimer RG, Dickman M, Day WC, Gunn ML, Schmidt CD: Ventilatory patterns and pulmonary complications after upper abdominal surgery determined by pre-operative and post-operative computerized spirometry and blood gas analysis. American Journal of Surgery 1971, 122: 622-632.
46. Blaney F, Sawyer T: Sonographic measurement of diaphragmatic motion after upper abdominal surgery: A comparison of three breathing manoeuvres. Physiotherapy Theory and Practice 1997, 13, 207-2115.
47. Dureuil B, Cantineau JP, Desmonts JM: Effects of upper or lower abdominal surgery on diaphragmatic function. British Journal of Anaesthesiology 1987, 59: 1230-1235.
48. Pansard JL, Mankikian B, Bertrand M, Kieffer E, Clergue F, Viars P: Effects of thoracic extradural block on diaphragmatic electrical activity and contractility after upper abdominal surgery. Anesthesiology 1993, 78: 63-71.
49. Erice F, Fox GS, Salib YM, Romano E, Meakins JL, Magder SA: Diaphragmatic function before and after laparoscopic cholecystectomy. Anesthesiology 1993, 79: 966-975.
50. Reeve EB, Nanson EM, Rundle FF: Observation on inhibitory reflexes during abdominal surgery. Clinical Science 1951, 10: 65-87.
51. Estenne M, Yernault JC, De-Smet JM, De-Troyer A: Phrenic and diaphragm function after coronary artery bypass grafting. Thorax 1985, 40: 293-299.
52. Locke TJ, Griffiths TL, Mould H, Gibson GJ: Rib cage mechanics after median sternotomy. Thorax 1990, 45: 465-468.
53. Vaughan RW, Wise L: Choice of abdominal operative incision in the obese patient: a study using blood gas measurements. Annals of Surgery 1975, 181: 829-835.
55. Vargas FS, Cukier A, Terra FM, Hueb W, Teixeira LR, Light RW: Influence of atelectasis on pulmonary function after coronary artery bypass grafting. Chest 1993, 104: 434-437.
56. Stiller K, Montarello J, Wallace M, Daff M, Grant R, Jenkins S: Efficacy of breathing and coughing exercises in the prevention of pulmonary complications after coronary artery surgery [see comments]. Chest 1994, 105: 741-747.
57. Dodson M: The management of post-operative pain. Dodson M. Current topics in anaesthesia. Issue 8. 1985. London, Edward Arnold Ltd.
58. Sabanathan S, Shah R, Tsiamis A, Richardson J: Oesophagogastrectomy in the elderly high risk patients: role of effective regional analgesia and early mobilisation. Journal Cardiovascular Surgery Torino 1999, 40: 153-156.
strength in the elderly. Correlates and reference values. Cardiovascular Health Study Research Group. American Journal Respiratory and Critical Care Medicine 1994, 149: 430-438.
Post-operative mucus clearance
26
65. Hewlett AM, Hulands GH, Nunn JF, Heath JR: Functional residual capacity during anaesthesia. II. Spontaneous respiration. British Journal of Anaesthesiology 1974, 46: 486-494.
66. Siafakas NM, Stoubou A, Stathopoulou M, Haviaras V, Tzanakis N, Bouros D: Effect of aminophylline on respiratory muscle strength after upper abdominal surgery: a double blind study [see comments]. Thorax 1993, 48: 693-697.
67. Celli B: Respiratory muscle strength after upper abdominal surgery [editorial; comment]. Thorax 1993, 48: 683-684.
69. Cotes JE: Maximal flow rates. Cotes J.E. Lung function: assessment and application in medicine. 5, 114-121. 1993. London, Blackwell.
70. Nunn JF: Measurement of ventilatory capacity. Nunn JF.Applied Respiratory Physiology. 1993. London Butterworth
71. Gamsu G, Singer MM, Vincent HH, Berry S, Nadel JA: Post-operative impairment of mucous transport in the lung. American Review Respiratory Diseases 1976, 114: 673-679.
72. Wahba RW: Peri-operative functional residual capacity [see comments]. Canadian Journal of Anaesthesiology 1991, 38: 384-400.
73. Konrad F, Schiener R, Marx T, Georgieff M: Ultrastructure and mucociliary transport of bronchial respiratory epithelium in intubated patients. Intensive Care Med 1995, 21: 482-489.
74. Plum F, Dunning MF: Technique for minimizing trauma to the tracheobronchial tree after tracheotomy. New England Journal of Medicine 1956, 254: 193-200.
75. Jung RC, Gottlieb LS: Comparison of tracheobronchial suction catheters in humans. Visualization by fiberoptic bronchoscopy. Chest 1976, 69: 179-181.
76. Czarnik RE, Stone KS, Everhart CCJ, Preusser BA: Differential effects of continuous versus intermittent suction on tracheal tissue. Heart and Lung 1991, 20: 144-151.
77. Branson RD, Campbell RS, Chatburn RL, Covington J: Endotracheal suctioning of mechanically ventilated adults and children with artificial airways. American Association Respiratory Care Clinical Practice Guideline. Respiratory Care 1993, 38: 500-504.
78. Stanek A, Brambrink AM, Latorre F, Bender B, Kleemann PP: Effects of normobaric oxygen on ciliary beat frequency of human respiratory epithelium. British Journal of Anaesthesiology 1998, 80: 660-664.
79. MacMahon C: Breathing and Physical exercises for use in wounds in the pleura, lung and diaphragm. Lancet 1915, 2: 769-770.
80. Thoren L. Post-operative pulmonary complication: observation on their prevention by means of physiotherapy. Acta Chirurca Scandinavia 1954, CVII, 193-205.
81. Chumillas S, Ponce JL, Delgado F, Viciano V, Mateu M: Prevention of post-operative pulmonary complications through respiratory rehabilitation: a controlled clinical study. Archives Physical Medicine Rehabilitation 1998, 79: 5-9.
82. Fagevik OM, Hahn I, Nordgren S, Lonroth H, Lundholm K: Randomized controlled trial of prophylactic chest physiotherapy in major abdominal surgery. British Journal of Surgery 1997, 84: 1535-1538.
83. Bartlett RH, Gazzaniga AB, Geraghty TR: Respiratory maneuvers to prevent post-operative pulmonary complications. A critical review. Journal American Medical Association 1973, 224: 1017-1021.
84. Morran CG, Finlay IG, Mathieson M, McKay AJ, Wilson N, McArdle CS: Randomized controlled trial of physiotherapy for post-operative pulmonary complications. British Journal of Anaesthesiology 1983, 55: 1113-1117.
85. Roukema JA, Carol EJ, Prins JG: The prevention of pulmonary complications after upper abdominal surgery in patients with noncompromised pulmonary status. Archives of Surgery 1988, 123: 30-34.
86. Stiller K, Crawford R., McInnes M., Montarello J., Hall B. The incidence of pulmonary complications in patients not receiving phrophylactic chest physiotherapy after cardiac surgery: a randomized clinical trial. Physiotherapy Theory and Practice 1995, 11, 205-208.
87. Laszlo G, Archer GG, Darrell JH, Dawson JM, Fletcher CM: The diagnosis and prophylaxis of pulmonary complications of surgical operation. British Journal of Surgery 1973, 60: 129-134.
Chapter 1
27
88. Rice VH, Mullin MH, Jarosz P: Preadmission self-instruction effects on postadmission and post-operative indicators in CABG patients: partial replication and extension. Research Nurse Health 1992, 15: 253-259.
89. Recker D: Patient perception of pre-operative cardiac surgical teaching done pre- and postadmission. Critical Care Nurse 1994, 14: 52-58.
90. Maxwell LJ, Ellis ER: The effect on expiratory flow rate of maintaining bag compression during manual hyperinflation. Australian Journal of Physiotherapy 2004, 50: 47-49.
91. Berney S, Denehy L, Pretto J: Head-down tilt and manual hyperinflation enhance sputum clearance in patients who are intubated and ventilated. Australian Journal of Physiotherapy 2004, 50: 9-14.
92. McCarren B, Chow CM: Manual hyperinflation: a description of the technique. Australian Journal of Physiotherapy 1996, 42: 203-208.
93. Hodgson C, Carroll S, Denehy L: A survey of manual hyperinflation in Australian hospitals. Australian Journal of Physiotherapy 1999, 45: 185-193.
94. Clarke RC, Kelly BE, Convery PN, Fee JP: Ventilatory characteristics in mechanically ventilated patients during manual hyperventilation for chest physiotherapy. Anaesthesia 1999, 54: 936-940.
95. LeFrock JL, Klainer AS, Wu WH, Turndorf H: Transient bacteremia associated with nasotracheal suctioning. Journal American Medical Association 1976, 236: 1610-1611.
96. Deppe SA, Kelly JW, Thoi LL, Chudy JH, Longfield RN, Ducey JP et al.: Incidence of colonization, nosocomial pneumonia, and mortality in critically ill patients using a Trach Care closed-suction system versus an open-suction system: prospective, randomized study. Critical Care Medicine 1990, 18: 1389-1393.
97. Hagler DA, Traver GA. Endotracheal saline and suction catheters: sources of lower airway contamination. American Journal of Critical Care 1994, 3:444-447.
98. Stone KS, Preusser BA, Groch KF, Karl JI, Gonyon DS: The effect of lung hyperinflation and endotracheal suctioning on cardiopulmonary hemodynamics (see comments). Nursing Research 1991, 40: 76-80.
99. Adlkofer RM, Powaser M: The effect of endotracheal suctioning on arterial blood gasses in patients after cardiac surgery. Heart and Lung 1978, 7: 1011-1014.
100. Eales CJ: The effects of suctioning and ambubagging on the partial pressure of oxygen and carbon dioxide in arterial blood. South African Journal of Physiotherapy 1989, 45: 53-55.
101. Brown SE, Stansbury DW, Merrill EJ: Prevention of suctioning-related arterial oxygen desaturation. Comparison of off-ventilator and on-ventilator suctioning. Chest 1983, 84: 621-627.
102. Turner JS, Briggs SJ, Springhorn HE, Potgieter PD: Patients' recollection of intensive care unit experience. Critical Care Medicine 1990, 18: 966-968.
103. Turner JS, Messervy SJ, Davies LA: Recollection of intensive care unit admission in the United Kingdom. Critical Care Medicine 1992, 20: 1363.
104. Rose D, Roeggla M, Behringer W, Roeggla G, Frass M: Erinnerungreste beatmeter Patienten nach Aufenthalt an der Intensivestation. Wiener Klinische Wochenschrift 1999, 111: 148-152.
105. Weeks AM, Buckland MR: Anaesthesia for adults with cystic fibrosis. Anaesthesia and Intensive Care 1995, 23: 332-338.
106. Walsh TS, Young CH: Anaesthesia and cystic fibrosis. Anaesthesia 1995, 50: 614-622. 107. Branson RD, Campbell RS, Davis K, Porembka DT: Anaesthesia circuits, humidity
output, and mucociliary structure and function. Anaesthesia and Intensive Care 1998, 26: 178-183.
108. Tucker B, Jenkins S: The effect of breathing exercises with body positioning on regional ventilation. Australian Journal of Physiotherapy 1996, 42, 219-227.
109. Ferris B, Pollard D. Effect of deep and quiet breathing on pulmonary compliance in man. Journal of Clinical Investigation 1960, 39, 143-149.
110. Terry PB, Traystman RJ, Newball HH, Batra G, Menkes HA: Collateral ventilation in man. New England Journal of Medicine 1978, 298: 10-15.
111. Bakow ED: Sustained maximal inspiration: A rational for its use. Respiratory Care 1977, 22, 379-382.
112. O'Donohue WJJ: Post-operative pulmonary complications. When are preventive and therapeutic measures necessary? Postgraduate Medicine 1992, 91: 167-175.
Post-operative mucus clearance
28
113. Menkes HA, Traystman RJ: Collateral ventilation. American Review Respiratory Diseases 1977, 116: 287-309.
114. Pryor J: The forced expiration technique. Pryor J. Respiratory Care. [7], 79-99. 1991. London, Churchill Livingstone.
115. Hall JC, Tarala RA, Tapper J, Hall JL: Prevention of respiratory complications after abdominal surgery: a randomised clinical trial [see comments]. British Medical Journal 1996, 312: 148-152.
116. Chuter TA, Weissman C, Starker PM, Gump FE: Effect of incentive spirometry on diaphragmatic function after surgery. Surgery 1989, 105: 488-493.
117. Weiner P, Man A, Weiner M, Rabner M, Waizman J, Magadle R et al.: The effect of incentive spirometry and inspiratory muscle training on pulmonary function after lung resection. Journal of Thoracic Cardiovascular Surgery 1997, 113: 552-557.
119. Minschaert M, Vincent JL, Ros AM, Kahn RJ: Influence of incentive spirometry on pulmonary volumes after laparotomy. Acta Anaesthesiology Belgica 1982, 33: 203-209.
120. Parker A, Verne S: Incentive spirometry versus routine chest physiotherapy [letter; comment]. Lancet 1991, 337: 1350.
121. Crowe JM, Bradley CA: The effectiveness of incentive spirometry with physical therapy for high-risk patients after coronary artery bypass surgery. Physical Therapy 1997, 77: 260-268.
122. Oikkonen M, Karjalainen K, Kahara V, Kuosa R, Schavikin L: Comparison of incentive spirometry and intermittent positive pressure breathing after coronary artery bypass graft. Chest 1991, 99: 60-65.
123. Schwieger I, Gamulin Z, Forster A, Meyer P, Gemperle M, Suter PM: Absence of benefit of incentive spirometry in low-risk patients undergoing elective cholecystectomy. A controlled randomized study. Chest 1986, 89: 652-656.
124. Denehy L, Ntoumenopoulos G, Maclellan DG: The cost-efficiency of incentive spirometry after abdominal surgery [letter; comment]. Australian New Zealand Journal of Surgery 1994, 64: 637-639.
125. Ayres SM: Magnitude of use and costs of in-hospital respiratory therapy. American Review Respiratory Diseases 1980, 122: 11-13.
126. Kester L, Stoller JK: Ordering respiratory care services for hospitalized patients: practices of overuse and underuse. Cleveland Clinical Journal of Medicine 1992, 59: 581-585.
127. Krastins I, Corey ML, McLeod A, Edmonds J, Levison H, Moes F: An evaluation of incentive spirometry in the management of pulmonary complications after cardiac surgery in a pediatric population. Critical Care Medicine 1982, 10: 525-528.
128. Gale GD, Sanders DE: Incentive spirometry: its value after cardiac surgery. Canadian Anaesthesiological Society Journal 1980, 27: 475-480.
129. Hall JC, Tapper J, Tarala R: The cost-efficiency of incentive spirometry after abdominal surgery [see comments]. Australian New Zealand Journal of Surgery 1993, 63: 356-359.
130. Gosselink R, Schrever K, Cops P, Witvrouwen H, De Leyn P, Troosters T et al.: Incentive spirometry does not enhance recovery after thoracic surgery. Critical Care Medicine 2000, 28: 679-683.
131. Dean E, Ross J: Discordance between cardiopulmonary physiology and physical therapy. Toward a rational basis for practice [see comments]. Chest 1992, 101: 1694-1698.
132. Sampson MG, Smaldone GC: Voluntary induced alterations in regional ventilation in normal humans. Journal of Applied Physiology 1984, 56: 196-201.
133. Roussos CS, Fixley M, Genest J, Cosio M, Kelly S, Martin RR: Voluntary factors influencing the distribution of inspired gas. Am Rev Respir Dis 1977, 116: 457-467.
134. O'Donohue WJJ: Prevention and treatment of post-operative atelectasis. Can it and will it be adequately studied? [editorial]. Chest 1985, 87: 1-2.
135. Jenkins SC, Soutar SA, Forsyth A, Keates JR, Moxham J: Lung function after coronary artery surgery using the internal mammary artery and the saphenous vein. Thorax 1989, 44: 209-211.
136. Hallböök T, Lindblad B, Lindroth B, Wolff T: Prophylaxis against pulmonary complications in patients undergoing gall-bladder surgery. A comparison between early mobilization, physiotherapy with and without bronchodilatation. Annals Chirurg Gynaecology 1984, 73: 55-58.
Chapter 1
29
137. Denehy L, Carroll S, Groves V, MacLellan D: The physiological and clinical outcome of using mask CPAP in the management of patients following abdominal surgery. European Respiratory Journal 1996, 9 Supp, 444s.
138. Webber B, Pryor J: Physiotherapy techniques. 138-145. Pryor J. and Webber B. Physiotherapy for respiratory and cardiac problems. 1998. London, Churchill Livingstone.
139. Dean E: Mobilization and exercise. 265-296. Frownfelter D. and Dean E. Principles and Practice of Cardiopulmonary Physical Therapy. 1987. New York, Mosby.
140. Ross J, Dean E: Integrating physiological principles into the comprehensive management of cardiopulmonary dysfunction. Physical Therapy 1989, 69: 255-259.
141. Winslow EH: Cardiovascular consequences of bed rest. Heart and Lung 1985, 14: 236-246.
142. Wasserman: Principles of exercise testing and interpretation. 1-63 Wasserman K, Hansen JE, Sue DY, Caraburi R, Whipp R. 3rd ed. 1999. Baltimore, Lippincott, Williams& Wilkins.
143. Wahba RW, Beique F, Kleiman SJ: Cardiopulmonary function and laparoscopic cholecystectomy. Canadian Anaesthesia 1995 Jan; 42(1): 51-63.
144. Crosbie W, Sim D: The effect of postural modification on some aspects of pulmonary function following surgery of the abdomen. Physiotherapy 1986, 72, 487-492.
145. Jenkins S, Soutar SA, Gray B, Evans J, Moxham J: The acute effects of respiratory manoeuvers in post-operative patients. Physiotherapy Practice 1988, 4, 63-68.
146. Dull JL, Dull WL: Are maximal inspiratory breathing exercises or incentive spirometry better than early mobilization after cardiopulmonary bypass? Physical Therapy 1983, 63: 655-659.
147. Jenkins SC, Soutar SA, Loukota JM, Johnson LC, Moxham J: Physiotherapy after coronary artery surgery: are breathing exercises necessary? Thorax 1989, 44: 634-639.
148. Wolff RK, Dolovich MB, Obminski G, Newhouse MT: Effects of exercise and eucapnic hyperventilation on bronchial clearance in man. Journal of Applied Physiology 1977, 43: 46-50.
149. Norrenberg M, Vincent JL: A profile of European intensive care unit physiotherapists. European Society of Intensive Care Medicine. Intensive Care Medicine 2000, 26: 988-994.
150. Jones AYM, Hutching RC, Oh TE: Chest physiotherapy on Intensive Care Units in Australia, the UK and Hong Kong. Physiotherapy Theory and Practice 1992, 8: 39-44.
Post-operative mucus clearance
30
Chapter 2
31
Endotracheal suctioning versus
minimally invasive airway suctioning in
intubated patients: a prospective
randomised controlled trial
Johannes P. van de Leur 1, Jan Harm Zwaveling 2, Bert G. Loef 3,
Cees P. van der Schans 1, 4.
1 Center for Rehabilitation, University Medical Center Groningen, The Netherlands
2 Department of General Surgery and Intensive Care, University Medical Center Groningen, The Netherlands
3 Department of Cardio-Thoracic Surgery and Intensive Care, University Medical Center Groningen, The Netherlands
4 University for Professional Education, Hanzehogeschool, Groningen, The Netherlands
Published in: Intensive Care Medicine: 2003, 29, 3, 426-432
RES versus MIAS
32
Abstract
Study Objective:
Endotracheal suctioning in intubated patients is routinely applied in most ICUs but may have negative side effects. We hypothesized that on-demand minimally invasive suctioning would have fewer side effects than routine deep endotracheal suctioning, and would be comparable in duration of intubation, length of stay in the ICU, and ICU mortality.
Design:
Randomised prospective clinical trial.
Setting:
Two ICUs at the University Medical Center Groningen, the Netherlands.
Patients:
Three hundred and eighty-three patients requiring endotracheal intubation for more than 24 hours.
Interventions:
Routine endotracheal suctioning (n=197) using a 49 cm suction catheter was compared with on-demand minimally invasive airway suctioning (n=186) using a suction catheter only 29 cm long.
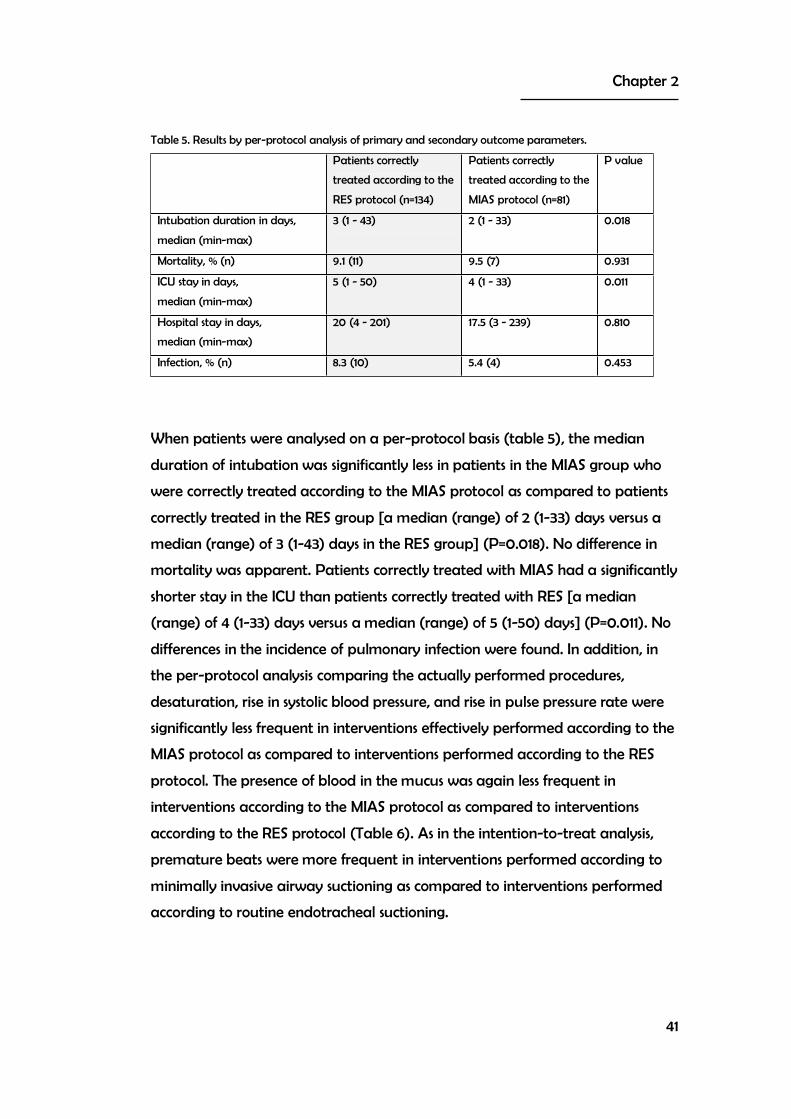
Measurements and results:
No differences were found between the routine endotracheal suctioning group and the minimally invasive airway suctioning group in duration of intubation [median (range) 4 (1-75) versus 5 (1-101) days], ICU-stay [median (range) 8 (1-133) versus 7 (1-221) days], ICU mortality (15% versus 17%), and incidence of pulmonary infections (14% versus 13%). Suction-related adverse events occurred more frequently with RES interventions than with MIAS interventions; decreased saturation: 2.7% versus 2.0% (P=0.010); increased systolic blood pressure 24.5% versus 16.8% (P<0.001); increased pulse pressure rate 1.4% versus 0.9% (P=0.007); blood in mucus 3.3% versus 0.9% (P<0.001).
Conclusions:
This study demonstrated that minimally invasive airway suctioning in intubated ICU-patients had fewer side effects than routine deep endotracheal suctioning, without being inferior in terms of duration on intubation, length of stay, and mortality.
Group allocation to either routine endotracheal suctioning (RES) or minimally
invasive airway suctioning (MIAS) was obtained by block randomisation with
sealed envelopes. The Medical Ethics Committee of the hospital approved the
study protocol and waived informed consent.
Twenty-four hours after randomisation, all patients no longer requiring
intubation, or who presented contra-indications or specific indications for
endotracheal suction, including pulmonary oedema, pulmonary haemorrhage
or atelectasis, were withdrawn from the study. All other patients were included
in the final phase of the trial and were kept in the treatment arm they had
been allocated to 24 hours earlier for the entire period that they required
intubation. According to their clinical requirements, patients received sedation
and partial ventilatory support with a heated humidifier. A proper level of
sedation was achieved with a continuous infusion of midazolam (range 1-4
mg/h) and fentanil (range 50-150 μg/h). Patients’ body positions were routinely
changed by nurses. The RES and MIAS procedures were performed supine, and
both are sterile procedures.
RES was defined according to the American Association Respiratory Care
guideline [1]. With a minimum frequency of three times a day, the patient was
disconnected from the ventilator after a short course of pre-oxygenation with
100% oxygen. Manual hyperinflation was performed before a 49-cm (19.3-inch)
CH12 catheter (Maersk Medical, Denmark) was introduced into the
endotracheal tube and the airway. Then negative pressure (200-400 mmHg)
was applied for a maximum duration of 3 seconds. Manual hyperinflation was
Chapter 2
35
applied between suctioning cycles and sterile normal saline (10 ml) was instilled
into the endotracheal tube if considered necessary by the nurse. After three
cycles of hyperinflation, saline, and suctioning, the patient was reconnected to
the ventilator. The nurse decided whether additional (i.e., in excess of three
times a day) RES was needed on clinical grounds (audible or visible mucus
retention in the tube, when mucus induced repetitive coughing, or in case of an
acute decrease of oxygen saturation (below 90%)).
MIAS was defined as follows; when considered clinically indicated
(audible or visible retention of mucus in the endotracheal tube, repetitive
coughing, or otherwise unexplained decreased oxygen saturation), the patient
was disconnected from the ventilator without pre-oxygenation with 100%
oxygen. Subsequently, a 29-cm (11.4-inch) CH12 suction catheter (Maersk
Medical) was introduced into the endotracheal tube to which a negative
pressure (200–400 mmHg) was applied for a maximum duration of 3 seconds.
Manual hyperinflation was avoided. No saline was instilled. The length of the
catheter was chosen to exclude the possibility of the airway being touched by
the catheter: it was too short to pass beyond the tip of the endotracheal tube.
The suctioning procedure could be repeated if necessary, after which the patient
was reconnected to the ventilator.
RES and MIAS groups were compared for possible differences in the
primary outcome parameter: duration of intubation. The secondary outcome
parameters of the study were mortality, length of stay in the ICU, incidence of
pulmonary infection, and incidence of suction-related adverse events.
Pulmonary infection was defined using the Clinical Pulmonary Infection Score as
described by Pugin [6]. A score 7 was considered as proof of pulmonary
infection. The CPIS score included body temperature, leucocytes, X-ray findings,
aspect of the mucus, and microbiological findings. The total score range was
between 0-12. Suction-related adverse events were defined as any of the
following occurring within 10 minutes after suctioning: 1) a decrease in oxygen
saturation measured by transcutaneous pulse-oxymetry of 5% or greater; 2)
bradycardia of 40 beats per minute or less; 3) the occurrence of any new
sustained cardiac arrhythmia; 4) the occurrence of more than 3 premature
beats per minute; 5) a rise in systolic blood pressure of 10% or more above
RES versus MIAS
36
baseline level; 6) an increase in pulse pressure rate (mean arterial blood
pressure times heart rate) of 30% or more above baseline level; 7) the visual
presence of new blood in the aspirated mucus. Data for the registration of
adverse events were collected from the Marquette Medical Systems monitor
using version 9A software. Vital signs (oxygen saturation, heart rate, systolic
blood pressure, mean blood pressure) were measured at 1-minute intervals from
the 2-minute period preceding the suctioning intervention until 10 minute after.
To evaluate cost effectiveness, the net cost of the materials used in the two
suctioning protocols and the mean time invested in carrying out one
intervention for each protocol was calculated for 45 treatments for each of the
interventions. The costs were extrapolated to the total number of interventions
and to an annual basis.
Patients allocated to MIAS were permitted treatment with RES if one of
the following conditions was present after clinical observation by nurses and
confirmation by medical staff: 1) an acute and persistent (> 1 minute) decrease in
oxygen saturation below 90% for which no other cause than mucus retention
could be found; 2) unilateral hypoventilation indicating unilateral bronchus
obstruction; 3) persistent coughing causing asynchronised breathing on the
ventilator and evident distress. RES in MIAS-allocated patients had to be
approved by the physician on call. The patient was kept in the same treatment
arm and MIAS was restarted after the event. All events were recorded and
retrospectively analyzed. All protocol deviations (too low treatment frequency
in the RES group and RES treatment in MIAS-allocated patients) were
recorded.
Statistical analysis
Sample size calculation was based upon the assumption of bio-equivalence
between both treatment arms, duration of intubation being the primary
outcome parameter. We have used duration of intubation data from the 2
years previous to the start of the study. Because the distribution of the mean
number of days with intubation was skewed to the right, a log transformation
was performed to calculate sample size. A difference of 2 days or less was
considered to be acceptable for bio-equivalence. The alpha was set at 0.05 and
Chapter 2
37
the beta at 0.20. The minimum number of patients per group required to fulfil
these criteria was 166.
Data in the RES and MIAS groups were compared with chi-square tests
for proportions, with the Students t-test for continuous data, and with a Mann-
Whitney U-test for ordinal variables and in case of skewed distribution of the
data. All analyses were performed on an intention-to-treat as well as a per-
protocol basis.
Results
During the study period (September 1998-July 2000), 2,795 patients were
admitted to the ICUs participating in the study. Of these patients, 2,254 were
randomised to receive either RES or MIAS on admission. Finally, 383 patients
(197 receiving RES and 186 receiving MIAS) could be included into the study
since they still needed intubation 24 hours after admission and had no other
reasons for exclusion. The reasons for non-randomisation and exclusion are listed
in table 1.
Table 1. Reasons for exclusion.
Patient selection
Admitted 2795
Not randomised < 18 years Not intubated Intubated at other hospital Non-regular tube type Closed suction system Lung transplant Missed randomisation within 24 hours Died before randomisation Other reasons
223 119 4428109442242
541
Randomised 2254 Not included Intubation < 24 hours Pulmonary oedema Atelectasis as admission diagnosis Pulmonary haemorrhage
1857 770
1871
Included 383
Patient characteristics and demographic data are presented in table 2. No
significant differences between the patients in RES and MIAS groups were
found. The median (min-max) number of suctioning treatments per patient in
the RES group was 9 (0-453) and in the MIAS group 11 (0-638) (P=0.405).
RES versus MIAS
38
Table 2. Patient characteristics and demographic data.
RES MIAS P value
Number of patients 197 186
Gender % m / f 72 / 28 71 / 29 0.988
Age in years, mean (SD) 61 (16) 62 (16) 0.636
Apache II score, median (min - max.) 12 (2 - 29) 13 (2 - 30) 0.229
* The number of interventions is higher in the RES group in the per-protocol analysis (8555) as compared to the intention-to-treat analysis (7827) because some interventions in the MIAS-allocated patients were actually performed according to the RES protocol.# For the same reason the number of interventions in the MIAS group is lower in the per-protocol analysis (6631) as compared to the intention to treat analysis (7395).
Discussion
The results of our study show that MIAS was associated with fewer suction-
related adverse events and at least was equal in terms of duration of
intubation, mortality and pulmonary infection incidence compared with RES.
The pathophysiologic mechanism underlying suction related adverse events was
probably multifactorial. Hypoxia based on alveolar derecruitment may had
been a common denominator. Oxygen desaturation would have been most
prominent in patients with low functional residual capacities, elevated mean
airway pressures, and high levels of PEEP. The use of large-bore suction
catheters and high levels of negative pressure applied to the airway would have
increased the likelihood of oxygen desaturation. Mucosal bleeding may have
been the effect of direct damage due to catheter introduced into the airway,
but could have been also related to the negative pressure applied and to the
technique of suctioning.
The MIAS procedure which we evaluated in this study was likely to be
less effective in removing secretions from the lower airways as compared to the
standard procedure. This was supported by the fact that the main reasons for
treating MIAS-allocated patients with suctioning according to RES protocol
were signs of mucus retention and decreased saturation. However, this
Chapter 2
43
appeared to have no effect on mortality, duration of intubation, and ICU stay.
This suggested that, in general, the minimally invasive procedure is sufficient.
However, in specific patients with large amounts of secretions in the lower
airways the more rigorous conventional procedure may still be required.
The incidence of most suction-related adverse events in the MIAS group is lower
than in the RES group. RES is a more invasive procedure and may induce stress,
which may contribute to increased systolic blood pressure and pulse pressure
rates, which indeed occurred more frequently in the RES group than in the MIAS
group. Previously, smaller studies found circumstantial evidence for induced
stress due to suctioning [2,7]. Suctioning in the lower airways probably also
explained the higher incidence of clinically detected blood in aspirated mucus in
the conventional RES group than in the MIAS group. Although we had no
indication that systematic differences in negative pressure between both
suctioning procedures occurred, this may theoretically explain the differences in
the incidence of blood in the aspirated mucus.
Unlike all other suction-related adverse events, the incidence of suction-
related arrhythmia was higher in the MIAS group than in the conventional RES
group. Our study does not offer any clues whythis should be so.
Suction-related adverse events appeared to have no effect on duration
of intubation, ICU mortality, ICU stay, hospital stay, and first day of pulmonary
infection, as there was no difference between the two groups in the intention-
to-treat analysis. Suction-related adverse events could therefore be less
detrimental for the patient than expected; alternatively the incidence of
suction-related adverse events may have been too low to have measurable
long-term effects.
In the per-protocol analysis differences were found in other parameters:
duration of intubation and ICU stay were longer in the RES group than in the
MIAS group. Differences in outcome between the per-protocol analysis and the
intention-to-treat analysis were probably due to selection bias. The number of
patients in whom a protocol deviation occurred, and who, consequently, were
excluded from the per-protocol analysis, was much higher in the MIAS group
than in the RES group. Since both groups excluded patients with a longer
duration of intubation and ICU stay, selection bias would explain why the
RES versus MIAS
44
duration of intubation and ICU stay was significantly higher in the RES group
than in the MIAS group.
No difference in incidence of pulmonary infection between the two
groups was found, although our study was not primarily designed to investigate
the difference in pulmonary infection between RES and MIAS. LeFrock [8]
found in a group of 68 patients that 12% developed bacteraemia after
endotracheal suctioning. This was probably caused by transport of bacteria
from the upper to the lower airways. Hagler [9] confirms transport of bacteria
due to suctioning. In an in vitro study, this author found that insertion of a
suction catheter in an endotracheal tube and instillation of normal saline
dislodges considerable amounts of viable bacterial colonies from endotracheal
tubes that could potentially be transported to the lower airways. Suctioning
according to the RES procedure, but not the MIAS procedure, included deep
suctioning and instillation of saline. Since we found no difference in the incidence
of pulmonary infections between the groups, the clinical relevance of Hagler’s
and LeFrock’s findings was probably limited.
Cost effectiveness was in favour of the MIAS intervention because fewer
sterile-paper covers and less saline was used and less time was invested by
nursing staff and/or respiratory physiotherapists. Cost savings when using the
MIAS intervention are limited due to the small difference in materials used and
time invested. Additional expenses (antibiotics and use of hospital resources)
were not taken into account due to the fact that there were no differences in
infection rates, duration of ventilation, ICU stay or hospital stay.
The incidence of suction-related adverse events in the group receiving RES was
lower than we expected. Many publications have focused on adverse effects
related to endotracheal suctioning and suggested that adverse events arise
frequently. Previous studies [3-5, 10-12] described suction-related decreases of
oxygen tension and desaturation. However, the incidence of desaturation was
not reported in these studies. The results of our study showed for the first time
that the incidence of suction-related decreased saturation was low (2.7% in the
RES group and 2% in the MIAS group). The incidence of oxygen desaturation
was significantly lower in the MIAS groups as compared to the RES group. This
difference could be explained by the fact that the minimal number of cycles
Chapter 2
45
during suctioning according to RES was three cycles while in case of MIAS this
was only one. The whole minimally invasive airway suctioning procedure was
therefore shorter as compared to the routine endotracheal suctioning
procedure. However, the incidence difference of oxygen desaturation was only
0.7%. We considered this difference as less clinically relevant.
The incidence of suction-related arrhythmia, 6.6% in our study, was much lower
than in a previous study by Stone et al. [13], who reported an incidence of
arrhythmia of 81% in patients after open-heart surgery. It must be noted that
Stone’s study included only 26 patients and that the estimation of the incidence
of arrhythmia was therefore less reliable than ours, which was based on 197
patients and 7,800 RES interventions.
Obviously, the results of our study can only be applied to the type of
patients included (i.e., without ARDS or atelectasis as admission diagnosis). The
reason for excluding patients with ARDS was that we considered that these
patients require a constant positive pressure from the mechanical ventilator to
maintain adequate oxygenation. It was therefore considered unfavourable to
disconnect these patients from the mechanical ventilator for suctioning (either
RES or MIAS). Patients with an atelectasis, at the time of admission, were
excluded because in our opinion they required selective deep suctioning in order
to remove accumulated mucus. We believed that inclusion in this study would
have denied these patients optimal treatment for their disease or condition. We
were well aware of the fact that exclusion of this type of patient may have
reduced the number of suction-related adverse events in our study population,
underestimating the general risk of this procedure.
It should be formally mentioned that for our study a modified (i.e., non-
standard) catheter was used for the MIAS group, which by itself precludes
immediate general adoption of a minimally invasive airway suctioning strategy.
A further potential limitation of our study was the substantial number of
protocol deviations. One or more protocol deviations occurred in 32% of the
patients in the RES group and in 56.5% of the patients in the MIAS group.
However, the number of protocol deviations per patient was low: in 68.3% of
the patients in the MIAS group, less than 10% of the interventions were contrary
to the protocol. To summarise, protocol deviations were common on a patient
RES versus MIAS
46
level, but the number of deviations per patient was low. In the conventional
RES group this proportion was 81.2%. The most frequently reported reason
(94%) for a protocol deviation in the RES group was “no indication for
suctioning”. The minimum suctioning frequency of three times per day was not
met in these patients. The most important reason (69%) for protocol deviations
in the MIAS group was visible or audible presence of mucus. In these cases RES
was used instead of the prescribed MIAS. It appeared that the nursing staff
considered MIAS as inadequate and preferred the RES intervention. MIAS could
have resulted in a greater accumulation of secretions if it had been applied
without deviations (RES instead of MIAS). Potentially, this accumulation of
secretions could have resulted in a higher incidence of pulmonary infections in
the MIAS group. However, this is not supported by the per protocol analysis. In
contrast, it has also been suggested that deep suctioning, like in case of RES, is a
risk factor for the development of infections. This could theoretically have
contributed to a higher incidence of pulmonary infections in case of suctioning
according to RES than according to MIAS, but no differences were found.
The results of our study suggest that the use of minimally invasive airway
suctioning instead of routine endotracheal deep suctioning in patients with a
ventilation duration of more than 24 hours, caused a lower incidence of suction-
related adverse events, and was equivalent in terms of duration of intubation,
ICU mortality, pulmonary infection incidence, duration of ICU stay, and hospital
stay. However, suction-related adverse events were generally mild, even with
deep suctioning, if proper precautions were taken. As a consequence, our data
do not support the general adoption of a MIAS strategy for mechanically
ventilated ICU-patients; they merely question the added benefit of repeated
deep suctioning. Further studies are needed to investigate whether the
reduction of the duration of intubation and stay in the ICU, observed in the
MIAS group with a per-protocol analysis, is borne out in a proper intention-to
treat format.
Chapter 2
47
Reference list
1 Branson RD, Campbell RS, Chatburn RL, Covington J: Endotracheal suctioning of mechanically ventilated adults and children with artificial airways. American Association Respiratory Care Clinical Practice Guideline. Respiratory Care (1993) 38: 500-504.
2 Stone KS, Talaganis SA, Preusser B, Gonyon DS: Effect of lung hyperinflation and endotracheal suctioning on heart rate and rhythm in patients after coronary artery bypass graft surgery. Heart and Lung (1991) 20: 443-450.
3 Adlkofer RM, Powaser M: The effect of endotracheal suctioning on arterial blood gases in patients after cardiac surgery. Heart and Lung (1978) 7: 1011-1014.
4 Eales CJ. The effects of suctioning and ambubagging on the partial pressure of oxygen and carbon dioxide in arterial blood. South African Journal of Physiotherapy (1989) 45: 53-55.
5 Brown SE, Stansbury DW, Merrill EJ: Prevention of suctioning-related arterial oxygen desaturation. Comparison of off-ventilator and on-ventilator suctioning. Chest (1983) 83: 621-627.
6 Pugin J, Auckenthaler R, Mili N, Janssens JP, Daniel P, Sutter P: Diagnosis of ventilator associated pneumonia by bacteriologic analysis of bronchoscopic and non-bronchoscopic "blind" bronchoalveolar lavage fluid. American Review of Respiratory Disease (1991) 143: 1121-1129.
7 Clark AP, Winslow EH, Tyler DO, White KM: Effects of endotracheal suctioning on mixed venous oxygen saturation and heart rate in critically ill adults. Heart and Lung (1990) 19: 552-557.
8 LeFrock JL, Klainer AS, Wu WH, Turndorf H: Transient bacteremia associated with nasotracheal suctioning. Journal of American Medical Association (1976) 236: 1610-1611.
9 Hagler DA, Traver GA: Endotracheal saline and suction catheters: sources of lower airway contamination. American Journal of Critical Care (1994) 3: 444-447.
10 Boutros AR: Arterial blood oxygenation during and after endotracheal suctioning in the apneic patient. Anesthesiology (1970) 32: 114-118.
11 Berman IR, Stahl WM: Prevention of hypoxic complications during endotracheal suctioning. Surgery (1968) 63: 586-587.
12 Ritz R: Hypoxemia and arrhythmias due to endotracheal suction. Schweizerische Medizinische Wochenschrift (1973) 103: 1017-1021.
13 Stone KS, Bell SD, Preusser BA: The effect of repeated endotracheal suctioning on arterial blood pressure. Applied Nursing Research (1991) 4: 152-158.
RES versus MIAS
48
Chapter 3
49
Patient recollection of airway suctioning
in the ICU: routine versus a minimally
invasive procedure
Johannes P. van de Leur 1, Jan Harm Zwaveling 2, Bert G. Loef 3,
Cees P. van der Schans 1,4.
1 Centre for Rehabilitation,University Medical Center Groningen, The Netherlands
2 Department of General Surgery and Intensive Care, University Medical Center Groningen, The Netherlands
3 Department of Cardio-Thoracic Surgery and Intensive Care University Medical Center Groningen, The Netherlands
4 University for Professional Education, Hanzehogeschool, Groningen, The Netherlands
Published in: Intensive Care Medicine 2003, 29, 3, 433-436
Patient recollection of airway suctioning
50
Abstract
Study Objective:
Many patients have an unpleasant recollection of routine endotracheal suctioning after discharge from the Intensive Care Unit (ICU). We hypothesized that through minimally invasive airway suctioning discomfort and stress may be prevented, resulting in less recollection.
Design:
A prospective randomized clinical trial.
Setting:
Two ICUs at the University Hospital of Groningen, the Netherlands.
Patients and Participants:
Adult patients with an intubation period exceeding 24 hours were included.
Interventions:
Patients received either routine endotracheal suctioning (RES) or minimally invasive airway suctioning (MIAS) during the duration of intubation.
Measurements and results:
Within 3 days after ICU discharge all patients were interviewed, regarding recollection and discomfort of suctioning. The level of discomfort was quantified on a visual analogue scale (VAS). We analyzed data from 208 patients (RES: n=113, MIAS: n=95). A significantly lower prevalence of recollection of airway suctioning was found in the MIAS group (20%) compared to the RES group (41%) (P=0.001). No significant difference in level of discomfort was found between the RES and the MIAS group (P=0.136).
Conclusions:
Minimally Invasive Airway Suctioning results in a lower prevalence of recollection of airway suction than in Routine Endotracheal Suctioning, but not in discomfort.
Logistic regression shows the following regression coefficients for
recollection of airway suctioning, RES: 1.016 (P=0.002) and age -0.025
(P=0.013). APACHE-II score, gender, duration of intubation) and number of
treatments were excluded from the equation. Regression coefficients and P-
values are expressed in table 4.
Table 4. Logistic regression for recollection of airway suctioning.
Variables in the equation Wald test
statistic
P value B Exp(B)*
Group 0= RES;
1= MIAS
9.732 0.002 1.016 2.762
Age years 6.232 0.013 -0.025 0.975
Variables not in the equation
Gender 0= male;
1= female
2.018 0.155
APACHE II score points 2.929 0.087
Duration of intubation days 3.163 0.075
Number of suctioning treatments number 3.838 0.050
*odds-ratio
The odds-ratio of 2.76 for RES indicates that patients who were treated with
RES have a 2.76 times higher risk for recollection of airway suctioning as
compared to patients treated with MIAS. The odds-ratio of 0.97 for age
indicates that for every additional year the recollection of airway suctioning is
1.03 times lower.
Patient recollection of airway suctioning
56
Discussion
The results of our study show that the prevalence of recollection of airway
suctioning is considerably lower when endotracheal suctioning was done
according to a minimally invasive protocol as compared to conventional
endotracheal suctioning. Of the mainly surgical patients in our study discharged
from an ICU, 40.7% have a recollection of endotracheal suctioning, which they
experienced as unpleasant. This is in agreement with two other studies by
Turner. Turner found in a group of 68 ventilated, mainly medical, patients [2] a
prevalence (95% Confidence Interval) of recollection of endotracheal suctioning
of 44% (32-57%), and in 26 mainly surgical patients [6] a prevalence of
recollection of endotracheal suctioning of 47% (26-70%). The estimate of the
prevalence of recollection of conventional endotracheal suctioning in our study
extends the results of Turners’ studies to a larger population producing higher
reliability.
General recollection of ICU stay is reported to range between 35% and
66% [7,8], and may be dependant on the use of medication like
benzodiazepines [9] and propofol [10]. These types of medication are used
routinely in our ICU’s. A considerable number of patients were not able to
answer the questions, but they were distributed equally over both treatment
protocols, therefore creating no bias.
MIAS results in a lower incidence of recollection of endotracheal
suctioning compared to RES. We also found that in the MIAS group a lower
incidence of increased systolic blood pressure, which may indicate that the
patients in the MIAS group experienced less stress. MIAS is designed to clean only
the length of the endotracheal tube due to the identical length of tube and
suction catheter. No physical contact can be made between the suction tube
and the trachea or main bronchi. This procedure then probably induces less
stress in the patient. The design of our study does not allow a distinction
between the separate components of the endotracheal suctioning procedure
such as airway manipulation, saline instillation, and manual hyperinflation. The
duration of intervention is shorter in MIAS than in RES, which also may have
contributed to a lower prevalence of recollection of suctioning. MIAS causes
Chapter 3
57
fewer physical stimuli, and is shorter, resulting in less stress during the intubation
period. Less stress may explain the lower number of patients having recollection
of airway suctioning in case of MIAS. Our study also shows that elderly patients
tend to have a lower risk of recollection of airway suction. This can be explained
by the general decline in memory with age [11]. Other variables like APACHE-II
score, gender, duration of intubation, and number of treatments did not show
to be a significant factor in recollection. This may be due to level of sedation of
patients or the bias created by selection in this study.
The level of discomfort, expressed by a visual analogue scale in
centimetres, is not significantly different between RES and MIAS. We would
expect a lower level of discomfort in MIAS, due to the no-physical airway
contact and the shorter duration of MIAS. Potential explanations for equal
levels of discomfort found in both treatments imply that the patient is
disconnected from the mechanical ventilator, resulting in loss of positive pressure
and a disturbance in their breathing pattern. A second explanation may be the
fact that patients were addressed by the nursing staff to inform them about the
treatment. This may have resulted in a change in daily rhythm and waking
them from their sleep.
Conclusions
Minimally invasive airway suctioning results in a lower prevalence of recollection
of airway suction than routine endotracheal suctioning. Presumably, this
difference is due to fewer physical stimuli and a shorter procedure during the
MIAS treatment. Furthermore, when patients have a recollection of airway
suctioning, this recollection is a moderately distressful experience.
Patient recollection of airway suctioning
58
Reference List
1 Laitinen H: Patients' experience of confusion in the intensive care unit following cardiac surgery. Intensive and Critical Care Nursing (1996) 12: 79-83.
2 Turner JS, Briggs SJ, Springhorn HE, Potgieter PD: Patients' recollection of intensive care unit experience. Critical Care Medicine (1990) 18: 966-968.
3 Rose D, Roeggla M, Behringer W, Roeggla G, Frass M: Erinnerungreste beatmeter Patienten nach Aufenthalt an der Intensivestation. Wiener klinische Wochenschrift (1999) 111: 148-152.
4 Branson RD, Campbell RS, Chatburn RL, Covington J: Endotracheal suctioning of mechanically ventilated adults and children with artificial airways. International Anesthesiology Clinics (1996) 34: 73-80.
5 Stone KS, Bell SD, Preusser BA: The effect of repeated endotracheal suctioning on arterial blood pressure. Applied Nursing Research (1991) 4: 152-158.
6 Turner JS, Messervy SJ, Davies LA: Recollection of intensive care unit admission in the United Kingdom. Critical Care Medicine (1992) 20: 1363.
7 Rundshagen I, Schnabel K, Wegner, Schulte am Esch J: Incidence of recall, nightmare, and hallucination during analgosedation in intensive care. Intensive Care Medicine (2002) 28: 38-43.
8 Daffurn K, Bishop G, Hilman K, Bauman A: Problems following discharge after intensive care. Intensive and Critical Care Nursing (1994) 10: 244-251.
9 Tomaz C, Dickinson AH, McGaugh JL, Souza SM, Viana MB, Graeff FG: Localization in the amygdala of the amnestic action of diazepam on emotional memory. Behaviour and Brain Research (1993) 58: 99-105.
10 Sung YF, Tillette T, Freniere S, Powell RW: Retrograde amnesia, anterograde amnesia and impairment recall by using either thiopentone or propofol as induction and maintenance agents. Benno B, Fitch W, Millar K, editors. Memory and awareness in anaesthesia. Amsterdam: Swets & Zeitlinger, (1990): 176-180.
11 Jolles J, Boxtel MPJ van, Ponds RWHM, Metsemakers JFM, Houx PJ: The Maastricht Aging Study (MAAS): The longitudinal perspective of cognitive aging. Tijdschrift voor Gerontologie en Geriatrie (1998) 29: 120-129.
Chapter 4
59
Stressreaction during endotracheal
suctioning
Johannes P. van de Leur 1,2, Cees P. van der Schans 3, Bert G. Loef 4,
Ido P. Kema 5, Jan H.B. Geertzen 1,2, Jan H. Zwaveling 6.
1 Center for Rehabilitation, University Medical Center Groningen, The Netherlands 2 Northern Center for Health Care Research, University Medical Center Groningen, The Netherlands 3 Hanze University, Center for Research and Development in Health Care and in Nursing, Groningen, The Netherlands 4 Department of Cardio-Thoracic Surgery, University Medical Center Groningen, The Netherlands
5 Departments of Pathology and Laboratory Medicine, University Medical Center Groningen, and University Groningen, The Netherlands 6 Department of Intensive Care, University Hospital Maastricht, The Netherlands
Submitted.
Stressreaction
60
Abstract
Introduction
Routine endotracheal suctioning (RES) was shown to increase systolic blood pressure and
increase pulse-pressure rate suggestive of stress. This study was designed to test the hypothesis
that minimally invasive airway suctioning (MIAS) evokes a less pronounced stress response than
RES.
Patients and methods
Intubated stable ICU patients were eligible for participation in this study. Exclusion criteria were
noradrenaline or adrenaline infusion for the last 24 hours, the use of steroids and age under 55
or over 80 years. All patients underwent one episode of RES and one episode of MIAS, in
random order. Arterial blood samples were collected prior to (T0), 1 minute after (T1) and 15
minutes after the suctioning procedure (T15) via an arterial access. After a washout period of
three hours the second intervention, either MIAS or RES, was performed. Blood samples were
analyzed for noradrenaline, adrenaline and cortisol levels.
Results
In this study, 16 patients were included. Baseline levels of noradrenaline, adrenaline and cortisol
were elevated. With RES there were significantly greater noradrenaline and cortisol levels at T1
compared with MIAS. Adrenaline levels were not significantly influenced in either group.
Conclusions
RES caused a significant increase in noradrenaline and cortisol response compared to the MIAS
intervention, which suggests that RES leads to higher stress levels. Therefore, RES may be a more
stressful intervention than MIAS.
Keywords: Stress - Endotracheal suctioning - Intensive care
Chapter 4
61
Introduction
Endotracheal suctioning for removal of bronchial secretions in intubated
patients may be a hazardous procedure. It is performed to maintain airway
patency and is believed to prevent pulmonary infections, although evidence for
this is lacking. Many complications of endotracheal suctioning have been
described including cardiac arrhythmia [1] and oxygen desaturation [2-4]. In a
previous study, we found that routine endotracheal suctioning (RES) increases
pulse-pressure rate and increases systolic blood pressure suggestive of
considerable stress [5]. Elevations in pulse-pressure rate and blood pressure were
less pronounced with a new technique, described as “Minimally Invasive Airway
Suctioning” (MIAS). With MIAS only the endotracheal tube is suctioned with a
short catheter and contact with bronchial epithelium is avoided. The present
study was designed to test the hypothesis that MIAS results in a less pronounced
stress response than RES.
Patients and methods
Stable patients on a cardio-thoracic or general-surgical Intensive Care Unit
(ICU) in our University Medical Center were considered for randomisation in this
study. Exclusion criteria were noradrenaline or adrenaline infusion for the last
24 hours, the use of steroids and age under 55 or over 80 years. The narrow
range of age was chosen to limit variety in hormonal response during the study.
All patients underwent a RES and a MIAS treatment. Treatment order was
obtained with sealed envelopes. The Medical Ethics Committee of the hospital
approved the study protocol. Patients’ relatives gave informed consent to
participate in the study. RES and MIAS procedures were performed in a supine
position.
RES was defined according to the American Association of Respiratory Care
guideline [6]. The patient was disconnected from the ventilator. Manual
hyperinflation was performed before a 49 cm (19.3 inch), CH12, catheter
Stressreaction
62
(Maersk Medical, Denmark) was introduced into the endotracheal tube.
Subsequently a negative pressure (200 mmHg) was applied for a maximum
duration of three seconds. Manual hyperinflation was applied between
suctioning cycles and sterile normal saline (10 ml) was instilled into the
endotracheal tube. After three cycles of hyperinflation, saline and suctioning,
the patient was reconnected to the ventilator.
MIAS was performed as follows: the patient was disconnected from the
ventilator. Subsequently, a 29 cm (11.4 inch), CH12, suction catheter (Maersk
Medical, Denmark) was introduced into the endotracheal tube to which a
negative pressure (200 mmHg) was applied for a maximum duration of three
seconds. The patient was reconnected to the ventilator. Manual hyperinflation
was avoided. No saline was instilled. The length of the catheter was chosen to
exclude the possibility of the airway being touched by the catheter: it was too
short to pass beyond the tip of the endotracheal tube.
Arterial blood samples were collected via an arterial access prior to (baseline,
T0), 1 minute after (T1) and 15 minutes after (T15) starting RES or MIAS. After a
washout period of three hours the second intervention, MIAS or RES, was
performed. Blood samples were then collected at the identical time intervals.
Blood samples of 10 ml were analyzed for noradrenaline, adrenaline and
cortisol. Blood samples for nor- and adrenaline levels were collected in a
specimen tube according to international consensus and were kept on melting
ice during transport to the laboratory where the specimens were centrifuged.
Blood samples for cortisol levels were collected in a specimen coagulation tube.
The analysis of plasmacatecholamines was performed as previously described
[7,8] using a high-performance liquid chromatography with a electrochemical
detection. Serum cortisol levels were determined on an Elecys 2000 analyser
(Roche, Hitachi). Blood samples were also analyzed for arterial blood gasses
and glucose levels.
Data on patients’ characteristics, e.g. age, gender, APACHE II score, hemoglobin
level, Rikers’ Sedation and Agitation score and current medication, was
recorded prior to the interventions.
Chapter 4
63
Statistical analyses
SPSS version 12 was used for all statistical analyses. Descriptive analyses were
performed on patients’ characteristics. Paired T-tests were performed on the
noradrenaline, adrenaline and cortisol values between T0 and T1/T15.
Results
16 Patients were included, resulting in 32 episodes of monitored suctioning.
Patients’ characteristics are shown in table 1. All patients had a hemoglobin level
above 6.0 mMol/l. All patients had a Rikers’ Sedation Agitation Score of 2 to 4
and the score did not change during the RES and MIAS interventions.
Table 1. Patients’ characteristics. n =16
Age, mean (SD) in years 66.9 (6.9)
Gender, male in % 75
Type of patient Medical:
Surgical:
1
7 upper abdominal (4 acute, 3 elective)
4 thoracic-abdominal (4 elective)
3 thoracic (3 elective)
1 neck
APACHE-II score, median (min-max) 22 (11-28)
Total duration of intubation
median (min-max) in days
Duration of intubation on study day
median (min-max) in days
36 (8-154)
15 (8-64)
Type of intubation (endotracheal/tracheostomy) 13 / 3
Non- significant differences were reported between the baseline (T0) values of
RES or MIAS in table 2. All patients returned to baseline levels before the second
intervention (data on individual patients not shown).
Stressreaction
64
Table 2. Baseline and reference values.
Baseline values at T0
Mean (SD)
Reference values
Upper Range Limit
Noradrenaline, in nMol/l 3.27 (1.83) 1.84
Adrenaline, in nMol/l 0.65 (0.99) 0.17
Cortisol, in nMol/l 556 (212) 400
To evaluate the changes in RES and MIAS, differences were calculated between
baseline (T0), one minute post treatment (T1), and 15-minutes post treatment
(T15) in RES or MIAS and plotted in error bars in standard error of the mean
(figures 1 to 3).
Mean arterial Pressure (MaP) increased significantly during suctioning and more
so after the RES treatment (13 mmHg) compared to the MIAS treatment (3
mmHg, P value 0.030).
The immediate rise in noradrenaline and cortisol levels (T1-T0) was significantly
greater in the RES group than in the MIAS group (figures 1 and 3). At 15 minutes
no significant differences were found between both groups as to increase from
baseline (T15-T0). Adrenaline levels did not increase in either group (figure 2).
Glucose levels, PaO2 and PaCO2 did not change during the measurements
(data not shown).
RES T1-T0 MIAS T1-T0 RES T15-T0 MIAS T15-T0
-1,0
-0,8
-0,6
-0,4
-0,2
0,0
0,2
0,4
0,6
0,8
1,0
Mea
n ch
ange
+- 1
SE
Noradrenaline
Figure 1: +/- Standard Error of Mean of change in noradrenaline in nMol/l (* P < 0.005)
*
Chapter 4
65
RES T1-T0 MIAS T1-T0 RES T15-T0 MIAS T15-T0
-1,0
-0,8
-0,6
-0,4
-0,2
0,0
0,2
0,4
0,6
0,8
1,0
Mea
n ch
ange
+- 1
SE
Adrenaline
Figure 2: +/- Standard Error of Mean of change in adrenaline in nMol/l.
RES T1-T0 MIAS T1-T0 RES T15-T0 MIAS T15-T0
-40
-20
0
20
40
Mea
n ch
ange
+- 1
SE
Cortisol
Figure 3: +/- Standard Error of Mean of change in cortisol in nMol/l (* P <0.005).
Discussion
The results of our study show that RES leads to an increase of stress hormones
which is higher than the increase observed in MIAS. This suggests that, by
reducing the RES procedure into a minimally invasive procedure, a reduction in
stress response could be achieved.
*
Stressreaction
66
No significant differences were found in adrenaline responses of the RES
intervention compared to the MIAS intervention. This finding could be explained
by the fact that baseline levels of adrenaline were already elevated to more
than 350% of the Upper Range Limit of the normal level. Perhaps this level of
adrenaline could not increase any further. Adrenaline is produced in the adrenal
medulla and most of the noradrenaline is produced in the sympathetic nerves
and is then released into the bloodstream [12]. Perhaps the production of stress
hormones in the adrenal medulla did not respond to the stimulus anymore,
while the sympathetic nerve endings could still contribute to the response and
produce the required release of noradrenaline.
Baseline catecholamine values during prolonged duration of intubation were
increased as compared to healthy subjects, which indicate that these patients
were in a stressful condition. Our data thus confirm reports in the literature that
patients recall the period of ICU/intubation as a very stressful period [9-11].
The stress of the suctioning procedure is further reflected in a rise of MaP. The
MIAS intervention resulted in a lower increase of MaP, as compared to
traditional RES.
This study looked at stable ICU patients in a limited range of age. It remains to
be investigated whether similar results will be found in less stable patients,
younger patients or the very old population on the ICU. Therefore outcome of
this study is limited to the range of the age investigated.
Conclusions
In summary RES causes a significant increase in noradrenaline and cortisol
response compared to the MIAS intervention. The difference in adrenaline
response is non-significant comparing the two interventions. Baseline
catecholamine levels in ICU patients are elevated compared to healthy subjects.
Extra release of stress hormones during endotracheal suctioning can probably be
avoided by opting for a minimally invasive suctioning strategy.
Chapter 4
67
Reference list 1 Stone KS, Talaganis SA, Preusser B, Gonyon DS: Effect of lung hyperinflation and
endotracheal suctioning on heart rate and rhythm in patients after coronary artery bypass graft surgery. Heart and Lung 1991; 20 (5 Pt 1) 443-50.
2 Adlkofer RM, Powaser M: The effect of endotracheal suctioning on arterial blood gasses in patients after cardiac surgery. Heart and Lung 1978; 7 (6): 1011-1014.
3 Eales CJ: The effects of suctioning and ambubagging on the partial pressure of oxygen and carbon dioxide in arterial blood. South African Journal of Physiotherapy 1989; 45 (2): 53-55.
4 Brown SE, Stansbury DW, Merrill EJ: Prevention of suctioning-related arterial oxygen desaturation. Comparison of off-ventilator and on-ventilator suctioning. Chest 1983; 84 (4): 621-627.
5 Van de Leur JP, Zwaveling JH, Loef BG, Van der Schans CP: Endotracheal suctioning versus minimally invasive airway suctioning in surgical intensive care patients. A prospective randomized clinical trial. Intensive Care Medicine 2003; 29: 426-432.
6 Branson RD, Campbell RS, Chatburn RL, Covington J: Endotracheal suctioning of mechanically ventilated adults and children with artificial airways. American Association Respiratory Care Clinical Practice Guideline. Respiratory Care 1993; 38: 500-504.
7 Smedes F, Kraak JC, Poppe H: Simple and fast solvent extraction system for selective and quantitative isolation of adrenaline, noradrenaline and dopamine from plasma and urine. Journal Chromatograpy 1982; 231 (1): 25-39.
8 Willemsen JJ, Ross HA, Wolthers BG, Sweep CG, Kema IP: Evaluation of specific high-performance liquid-chromatographic determinations of urinary metanephrine and normetanephrine by comparison with isotope dilution mass spectrometry. Annals Clinical Biochemistry 2001; 38 (6): 722-730.
9 Rotondi A, Chelluri L, Sirio C, Mendelsohn A, Schultz R: Patients' recollection of stressful experiences while receiving prolonged mechanical ventilation in an intensive care unit. Critical Care Medicine 2002; 30 (4): 746-752.
10 Pennock BE, Crawshaw L, Maher T, Price T, Kaplan PD: Distressful events in the ICU as perceived by patients recovering from coronary artery bypass surgery. Heart and Lung 1994; 23 (4): 323-327.
11 Johnson MM, Sexton DL: Distress during mechanical ventilation: patients' perception. Critical Care Nurse 1990; 10: 48-57.
12 Eisenhofer G, Kopin IJ, Goldstein DS: Catecholamine Metabolism: A Contemporary View with Implications for Physiology and Medicine. Pharmacolgical Reviews 2004; 56 (3): 331-349.
13 Van de Leur JP, Zwaveling JH, Loef BG, Van der Schans CP: Patient recollection of airway suctioning in the ICU: routine versus a minimally invasive procedure. Intensive Care Medicine 2003; 29: 433-436.
Stressreaction
68
Chapter 5
69
Discomfort and factual recollection in
ICU patients
Johannes P. van de Leur 1,2, Cees P. van der Schans 3,4, Bert G. Loef 5, Betto G.
Deelman 6, Jan H.B. Geertzen 1,2 , Jan H. Zwaveling 7 .
1 Center for Rehabilitation, University Medical Center Groningen, The Netherlands 2 Northern Center for Health Care Research, Groningen The Netherlands
3University for Professional Education, Hanzehogeschool, Groningen, The Netherlands 4 Department of Health Sciences University of Groningen, The Netherlands 5 Departments of Cardio-Thoracic Surgery, University Medical Center Groningen, The Netherlands 6 Departments of Neuro-psychology, University Medical Center Groningen, The Netherlands 7 Departments of General Surgery and Surgical Intensive Care Unit, University Medical Center Groningen, The Netherlands
Published in: Critical Care 2004, 8: 6, R 467-473
Discomfort and factual recollection
70
Abstract
Introduction A stay in the Intensive Care Unit (ICU), though potentially lifesaving, is often considered to cause considerable discomfort to patients. However, retrospective assessment of discomfort is difficult because recollection of stressful events may be impaired by sedation and severe illness during the ICU period. The purpose of this study was to investigate the following questions: a) what was the incidence of discomfort reported by patients recently discharged from the ICU, b) what were the sources of discomfort reported, c) what was the factual recollection of their stay in the ICU and d) was discomfort reported more often in patients with good factual recollection? Patients and methods All ICU patients older than 18 years who had needed prolonged (>24 hours) admission with tracheal intubation and mechanical ventilation were included consecutively into the study. Within three days after discharge from the ICU, a structured face-to-face interview with each individual patient was held. All patients were asked to answer a questionnaire consisting of 14 questions specifically concerning the environment of the ICU they had stayed in. Furthermore, they were asked whether they remembered any discomfort during their stay and if so, which sources of discomfort they could recall. A reference group of surgical ward patients, matched by gender and age to the ICU group was studied to validate the questionnaire. Results In this study, 125 patients discharged from the ICU were included. Data of 123 ICU patients and 48 surgical ward patients were analyzed. The prevalence of recollection of any type of discomfort in the ICU patients was 54% (n=66). These 66 patients were asked to identify the sources of discomfort. The presence of an endotracheal tube, hallucinations and medical activities were identified as sources of discomfort. The median (min-max) score for factual recollection in the ICU patients was 15 (0-28). The median (min-max) score for factual recollection in the reference group was 25 (19-28). Analysis showed that discomfort was positively related to factual recollection (odds ratio 1.1, P<0.001), especially discomfort caused by the presence of an endotracheal tube, medical activities and noise. Hallucinations were reported more often with increasing age. Pain as a source of discomfort was predominantly reported by younger patients. Conclusion In post-discharge ICU patients 54% recalled discomfort. However, memory was often impaired: the median factual recollection score of ICU patients was significantly lower than the median factual recollection score of matched control patients. The presence of an endotracheal tube, hallucinations and medical activities were most frequently reported as sources of discomfort. Patients with a higher factual recollection score presented more risk of remembering the stressful presence of an endotracheal tube, medical activities and noise. Younger patients were more likely to report pain as a source of discomfort.
Chapter 5
71
Introduction
Being admitted to an Intensive Care Unit (ICU) can be considered a stressful life
event, the reason for admission being a critical or even life-threatening
condition. The ICU stay itself may also be stressful. Some patients report vivid
recollections [1-3] whereas others have a poor or even no recollection at all of
their stay on the ICU. In a study among post-surgical patients, ‘no recollection at
all’ ranges from 23% to 38% [4]. Various authors have reported that patients
had unpleasant recollections after a stay on an ICU. Patients recalled discomfort
like anxiety, pain, thirst, sleeplessness, disorientation, shortness of breath, inability
to move, painful medical interventions, and the presence of an endotracheal
tube [5]. Turner [6] specifically mentioned arterial blood gas sampling and
endotracheal suctioning.
However, recollection of discomfort during the ICU stay is inseparably
connected to the quality of recollection itself: events considered stressful at the
time may not be remembered; conversely, recollections of stressful events may
not be based on actual experiences. Jones and co-workers [7] investigated
patients’ estimation of the duration of their ICU stay in order to evaluate the
accuracy of their memories. The patients’ recall of events was generally poor,
and 41% of them felt that they had been confused at some time during their
stay in the ICU. To our knowledge, there is no literature investigating whether
the recollection of discomfort is related to the accuracy of recollection of facts as
such, and for what sources of discomfort this holds true. The purpose of this study
was to describe:
the incidence of discomfort reported by ICU patients,
the sources of their discomfort,
the factual recollection of ICU patients patients and ward patients,
determinants of the recollection of discomfort in ICU patients.
Discomfort and factual recollection
72
Methods
Consecutive ICU patients, who were older than 18 years and who had
undergone intubation for longer than 24 hours, were included in the study.
During mechanical ventilation patients received sedation by continuous infusion
of midazolam (range 1-4 mg/hour) and fentanyl (range 50-150 µg/hour), with
the degree of sedation given depending on their clinical requirements. The
patients participated in a study comparing routine endotracheal suctioning with
minimally invasive airway suctioning. The study was approved by the Medical
Ethics Committee of the University Medical Centre. The Acute Physiology Age
and Chronic Health Evaluation (APACHE) II score was used to quantify the
severity of illness [8] and was recorded on the day of admission to the ICU.
All ICU patients participated in a structured in-person interview, using a
standardized questionnaire, within three days after discharge from the ICU to
the ward. The reference group consisted of post surgical ward patients, matched
for age and sex. Data from the reference group were obtained in a structured
telephone interview conducted within three days after discharge from hospital.
In the questionnaire, all patients were asked to give answers to 14 questions
concerning the ICU environment (lighting, timing of ward rounds, number of
fellow ICU patients), the nursing staff (uniform, male/female) and personal care
(clothing, position of intravenous drip, washing and toilet activities).
Patients from the ICU group were asked whether they remembered any
discomfort during their stay on the ICU, and if they did, they were asked to
specify the sources of discomfort they remembered.
The questions regarding recollection of facts were first asked as open
questions. For each correct answer two points were given to these open
questions. Patients who were unable to answer the open questions were
presented with four multiple choice answers. For each correct answer one point
was given to the multiple choice questions. Summation of the points resulted in
a total score for factual recollection. The range for the total score was 0-28
points.
Chapter 5
73
Statistical analysis
SPSS version 10 (SPSS Inc., Chicago, Il, USA) was used to perform all analyses. To
assess the reliability of the questionnaire, a Cronbach’s alpha was calculated.
Differences between the ICU group and the reference group were analyzed
using the Chi square test for categorical variables and the T-test for normally
distributed intervals or ratio scale variables. Differences between patients who
recalled discomfort and those who recalled no discomfort were analyzed using
the Chi square test in case of categorical variables, the Mann-Whitney test for
ordinal variables and the T-test for normally distributed intervals or ratio scale
variables such as age. To analyze potential determinants of discomfort, logistic
regression was performed. The presence or absence of discomfort was entered as
the dependent variable, and independent variables were as follows: age,
gender, APACHE II score (only in ICU patients), length of stay in the ICU or
ward, factual recollection score and duration of tracheal intubation. Correlation
coefficients between factual recollection score and age were calculated using a
Spearman’s test for categorical variables.
From the logistic regression analysis, odds ratios (OR) were calculated for
all independent variables in the equation. The OR expresses the odds in the
group with the condition relative to the other group without the condition. To
an extent, the OR can be considered a measure of relative risk. An OR greater
than 1 indicates a higher risk and an OR below 1 indicates a lower risk in the
group with the condition relative to the group without the condition.
Results
A total of 125 patients discharged from the ICU were included in this study. Two
patients were unable to respond to the questions. Patient characteristics are
summarized in table 1. In the population studied the prevalence of any
discomfort recalled after discharge from the ICU was 54% (n=66). The sources of
discomfort identified by these 66 patients are summarized in table 2.
Discomfort and factual recollection
74
Table 1. Patients’ characteristics.
Patients’ characteristics ICU-group
n = 123
Reference
n = 48 P-value
Age, mean (sd) 61.5 (16) 60.2 (16) 0.617
Gender, male in % 71 65 0.435
APACHE II score, median (min-max) 11 (2 - 26) na
Type of patient, in % trauma/ medical/ surgical 8 / 7 / 85 13 / 4 / 83 0.537
ICU stay in days, median (min-max) 6.5 (2 - 133) na
Ward stay in days, median (min-max) na 10 (3 - 53)
(na= not applicable)
Table 2. Sources of discomfort.
Sources of discomfort in ICU patients (n = 66) in %*
Endotracheal tube 42
Hallucinations 32
Medical activities 29
Noise and bustle 14
Having pain 12
Thirst 9
Inability to talk 9
Shortness of breath 6
Being afraid 6
* Because patients could list more than one source of discomfort, the summation of percentages
exceeds 100%.
At the time of the interview six patients were disorientated, but were able to
recall discomfort.
The median (min-max) factual recollection score was 15 (0-28) in the ICU
patients and 25 (19-28) in the reference group; the difference between the
groups was highly significant (P<0.001). Analyses of reliability of the
questionnaire for the ICU patients revealed a Cronbach’s alpha of 0.86,
indicating high reliability. Items of factual recollection by ICU patients and the
reference group, in descending order of being identified correctly, are listed in
table 3.
Chapter 5
75
Table 3. Factual recollection.
Correct % Incorrect % Don’t know %
Group ICU reference ICU reference ICU reference
Type of patients’ clothing** 68 100 12 0 20 0
Gender of nursing staff ** 66 98 7 2 27 0
Place of intravenous access ** 65 98 11 0 24 2
Color of staff uniform ** 62 98 14 2 24 0
Number of fellow patients * 62 71 8 17 30 12
Type of personal hygiene ** 62 98 7 2 31 0
Logo on staff uniform ** 55 88 5 0 40 12
Type of lighting ** 54 96 12 4 34 0
Reason inability to talk ** 50 94 24 6 26 0
Time of personal hygiene ** 48 100 3 0 49 0
Toilet visits ** 42 100 32 0 26 0
Alternative headstand positions of
bed **
42 92 18 6 40 2
Type of food received ** 23 100 54 0 23 0
Time of ward round ** 11 98 34 0 55 2 * P value < 0.05 and **p value < 0.005 from Chi square test between ICU patients and reference group.
ICU patients characteristics are summarized in table 4 separately for the group
that recalled any discomfort and the group that did not recall any discomfort.
Significant differences were found between the two groups in factual
recollection, age and duration of intubation.
Table 4.
Patients’ characteristics of ICU patients with and without a recollecting of discomfort.
Discomfort
(n = 66)
No discomfort
(n = 57)
P value
Age, mean (SD) 59(17) 65(14) 0.004
Gender, male in % 65 77 0.143
Apache II score, median (min-max) 12 (2 - 26) 11 (5 - 24) 0.171
Duration of intubation, median (min-max) 5 (2 - 35) 3 (1 - 57) 0.001
Logistic regression analysis of determinants of recollection of discomfort
confirmed that factual recollection was indeed an independent factor in
predicting recollection of discomfort. The calculated OR was 1.1 (P<0.001), with a
correct percentage in regression analysis of 68%.
Discomfort and factual recollection
76
This implies that the risk for recalling discomfort was 1.1 times higher for each
factual recollection point. Age also was a determinant of recollection of
discomfort. The calculated OR was 0.97 (P=0.006; correct percentage in
regression analysis 66%). This implies that the risk for recalling discomfort was
lower by a factor of 0.97 for each year of advancing age. The duration of
intubation appeared not to be independently related to the recollection of
discomfort. Factual recollection appears to be inversely related to age. Analysis
of the relationship between factual recollection score and age in the ICU group
revealed that the correlation coefficient was -0.352 (P<0.001); in the reference
group it was -0.327 (P=0.023;
figure 1).
�Finally, the recollection of pain
appeared to be related to age
(OR 0.936, P=0.002; correct
percentage in regression analysis
94%). This implies that younger
patients reported more
recollection of discomfort in the
form of pain.
Figure 1. The plot expesses Factual recollection score and Age in the ICU and control group.
Discussion
The results of our study show that a considerable proportion (54%) of patients
discharged from the ICU had a recollection of discomfort during their stay in the
ICU. The presence of an endotracheal tube, medical interventions, noise and
experiences of hallucination were among the sources of discomfort most
frequently reported. To our knowledge, this study is the first to evaluate the
association between recollection of discomfort and intact factual recollection. In
a study conducted by Rose and co-workers [9] in 50 patients, 60% remembered
endotracheal suctioning, and 52% remembered extubation as unpleasant
experiences. In a study by Turner and co-workers [6], arterial blood gas
Age
908070605040302010
Fact
ual R
ecol
lect
ion
scor
e
40
30
20
10
0
-10
Group
Control
ICU
Chapter 5
77
sampling and tracheal suctioning were recalled by 48% and 44% of the patients.
Although those two studies did not investigate the prevalence of discomfort per
se, we conclude that their findings are similar to ours, in that discomfort was
recalled by 54% of ICU patients.
Within the context of ICU patients’ recollections, a memory of an
(stressful) event raises the question of whether this recollection is based on reality
or fantasy/imagination. In the present study we found the degree of factual
recollection to be an important determinant of discomfort, in the sense that
more discomfort was reported by those with better factual recollection. Each
item of factual recollection that was scored correctly increased slightly the risk
for recollection of discomfort. Factual recollection and recollection of discomfort
therefore appeared to be related.
In an ICU many factors contribute to impairment in memory: critical
illness itself, the use of benzodiazepines and opioids, and the common
occurrence of delirious states. When a patient’s health is improving or when
sedative agents are reduced below effective levels, patients tend to remember
more regarding factors, mostly unpleasant, in the ICU. Jones and co-workers [10]
described many causes of amnesia during severe illness, including large dosages
of sedative medication and withdrawal syndromes. Because levels of sedation
strongly influence the function of memory, a weak point in our study is that no
sedation score was recorded to enable us to evaluate the effects of sedatives on
patient recollection. It should also be noted that we did not look for objective
signs of post-discharge psychological distress or examine their relationship to
memories of stressful events, either real or perceived. We merely wished to
improve our understanding of discomfort by taking into account the
confounding role of memory.
The presence of an endotracheal tube, medical activities, and noise and
bustle were the sources of discomfort remembered most frequently (table 2).
This finding is comparable with those of other studies. In a group of 68
ventilated medical patients, Turner and co-workers [6] found a prevalence of
recollection of endotracheal suctioning of 44% and in 26 mainly surgical patients
those investigators found a prevalence of recollection of endotracheal suctioning
of 47% [11]. In a mixed surgical/medical group of cardiac patients (n = 50) Rose
Discomfort and factual recollection
78
and colleagues [9] found a 60% prevalence of recollection of endotracheal
suctioning during the ICU stay.
The reason for discomfort relating to the endotracheal tube may be
endotracheal suctioning. While intubated, patients are regularly suctioned via
the endotracheal tube in order to maintain airway patency. The strong
mechanical stimuli resulting from endotracheal suctioning may explain why the
endotracheal tube is remembered as a prominent source of discomfort. In a
previous study [12], we investigated the recollection of endotracheal suctioning
with two methods of suctioning: Routine Endotracheal Suctioning and Minimally
Invasive Airway Suctioning. In the case of RES, a 49 cm suction catheter was
passed into the lower airways. With MIAS the suction catheter did not enter the
lower airways and suctioning was limited to the endotracheal tube. A
significantly lower prevalence of recollection of airway suctioning was found in
the MIAS group (20%) than in the RES group (41%; P <0.001). Our findings show
that discomfort resulting from the endotracheal tube and its handling can be
reduced by changing the procedure.
Hallucinations were another source of discomfort. In the total ICU
patient group (n=123), 24 (20%; 95% confidence interval 13-23%) patients
experienced hallucinations. This finding is comparable with that of an earlier
and smaller study conducted by Holland and co-workers [2], who found that
10% of patients reported hallucinations. In a more recent study, Ely and
colleagues [13] found that 81.7% of ICU patients developed delirium at some
stage in their ICU stay. Delirium was an important variable, contributing as an
independent predictor to higher 6-month mortality and longer hospital stay.
Delirium was defined as ‘a disturbance in consciousness characterized by an
acute onset and fluctuating course of impaired cognitive functioning so that a
patients’ ability to receive, process, store and recall information is strikingly
impaired’. Clearly, the presence of delirium according to this definition does not
imply the presence of hallucinations. The exact percentage of patients who
recalled hallucinations was not stated in the report by Ely and co-workers.
In studies conducted by Puntillo [14] and Holland and co-workers [2], pain was
reported as a source of discomfort as well. In a post-cardiac surgery population
(n=24), Puntillo [14] described awareness of pain during the ICU period as a
Chapter 5
79
significant problem. Holland and co-workers [2] reported that, in a group of
post surgery patients (n=21), 71% had a recollection of pain. In our study of
mainly surgical ICU patients, only 12% indicated that pain was a source of
discomfort. Differences in type of sedation and pain medication, number of
patients, inclusion criteria and type of questionnaire used are possible
explanations for the low recollection of pain in the present study as compared
with previous ones.
A standardized score to assess recollection in this type of patient was
lacking at the time our study was performed. We developed a factual
recollection questionnaire that may represent a reliable new tool to acquiring
information regarding recollection of facts in post-ICU patients. Analysis of
reliability revealed a high Cronbach’s alpha, and the descriptive data of our
score showed a significant difference between ICU patients and the reference
group. These findings are hardly surprising in view of the considerable
differences between groups in severity of illness and consumption of hypnotics
and sedatives. Further studies are needed to determine the validity and
reliability of this instrument. Jones and co-workers [15] have since proposed a
similar tool (Intensive Care Unit Memory tool), which has been validated in a
number of settings [4,16].
Both good factual recollection and younger age increased the risk for
discomfort. Factual recollection and age were inversely associated with each
other, but this association was weak. The association of increasing age with
reduction in memory function is widely recognized [17,18].
Although factual recollection and recollection of discomfort appear to be
related, increasing the level of sedation is not necessarily the best way to
prevent discomfort. Not only will deep sedation lead to increased length of stay
in the ICU and prolonged ventilator dependency [19] but it may also have an
adverse effect on the rate of post-traumatic stress disorder experienced by
patients after their discharge from the ICU [10]. It has been proposed by various
authors that factual recollection helps to offset the emotional impact of
delusional memories [10,19] and may actually help to avoid adverse
psychological outcomes in this type of patient. The development of drugs that
can eliminate the emotional impact of stressful events in the ICU, while
Discomfort and factual recollection
80
preserving mental clarity and memory, might offer the best way to avoid long-
term psychological distress. Meticulous treatment of delusional states will also
contribute to this end.
Conclusion
In a series of patients discharged from the ICU, 54% recalled discomfort. The
most frequent sources of discomfort cited were presence of an endotracheal
tube, hallucinations and medical interventions. The median factual recollection
score for ICU patients was significantly lower than the median factual
recollection score for ward patients who had not been in an ICU environment.
Younger patients were at greater risk for remembering pain as source of
discomfort. Patients with better factual recollection had greater recollection of
discomfort. Factual recollection and age were inversely related, but this
relationship was weak.
Discomfort thus appears to be a serious problem for patients in an ICU
environment. Its prevalence is probably underestimated because retrospective
assessment of the degree of discomfort when the patient has been discharged
from the ICU is seriously handicapped by global or partial amnesia, caused by
critical illness, delusional states and the use of drugs.
However, the fact that discomfort is not always remembered does not
imply that the patient has not suffered during his or her stay in the ICU.
Reduction in discomfort should remain a focus of attention for both researchers
and clinicians caring for critically ill patients.
Reference list
1. Rundshagen I, Schnabel K, Wegner, Schulte am Esch J: Incidence of recall, nightmare, and hallucination during analgosedation in intensive care. Intensive Care Medicine (2002) 28: 38-43.
2 Holland C, Cason CL, Prater LR: Patients' recollection in critical care. Dimensions of
Critical Care Nursing (1997) 16: 132-141.
3. Rotondi A, Chelluri L, Sirio C, Mendelsohn A, Schultz R: Patients' recollection of stressful experiences while receiving prolonged mechanical ventilation in an intensive care unit. Critical Care Medicine (2002) 30: 746-752.
Chapter 5
81
4. Capuzzo M, Pinamonti A, Cingolini E, Grassi L, Bianconi M, Contu P et al.: Analgesia, sedation and memory of intensive care. Journal of Critical Care (2001) 16: 83-89.
5. Pennock BE, Crawshaw L, Maher T, Price T, Kaplan PD: Distressful events in the ICU as perceived by patients recovering from coronary artery bypass surgery. Heart Lung (1994) 23: 323-327.
6. Turner JS, Briggs SJ, Springhorn HE, Potgieter PD: Patients' recollection of intensive care unit experience. Critical Care Medicine (1990) 18: 966-968.
7. Jones J, Hoggart B, Withey J, Donaghue K, Ellis BW: What the patients say: a study of reaction to an Intensive Care Unit. Intensive Care Medicine (1979) 5: 89-92.
8. Knaus WA, Draper EA, Wagner DP, Zimmerman JE: APACHE II: a severity of disease classification system. Critical Care Medicine (1985) 10: 818-829.
9. Rose D, Roeggla M, Behringer W, Roeggla G, Frass M: Erinnerungreste beatmeter Patienten nach Aufenthalt and der Intensivestation. Wiener klinische Wochenschrift (1999) 111: 148-152.
10. Jones C, Griffiths RD, Humphris G: Disturbed memory and amnesia related to intensive care. Memory (2000) 8: 79-94.
11. Turner JS, Messervy SJ, Davies LA: Recollection of intensive care unit admission in the United Kingdom. Critical Care Medicine (1992) 20: 1363.
12. Van de Leur JP, Zwaveling JH, Loef BG, Van der Schans CP: Patient recollection of airway suctioning in the ICU: routine versus a minimally invasive procedure. Intensive Care Medicine (2003) 29: 433-436.
13. Ely EW, Shintani A, Truman B, Speroff T, Gordon SM, Harrell FE Jr, Inouye SK, Bernard GR, Dittus RS: Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA (2004) 291: 1753-1762.
14. Puntillo KA: Dimensions of procedural pain and its analgesic management in critically ill surgical patients. American Journal of Critical Care (1994) 3: 116-122.
15. Jones C, Griffith RD, Humphries G, Skirrow PM: Memory, delusions, and the developement of acute posttraumatic stress disorder related symptoms after intensive care. Critical Care Medicine (2001) 29: 573-580.
16. Capuzzo M, Valpondi V, Cingolani E, De Luca S, Gianstefani G, Grassi L, Alvisi R: Application of the Italian version of the Intensive Care Unit Memory tool in the clinical setting. Critical Care (2004), 8: R48-R55.
17. Wegesin D, Jacobs DM, Zubin NR, Ventura PR, Stern Y: Source memory and encoding strategy in normal aging. Journal of Clinical Expertise in Neuropsychology (2000) 22: 455-464.
18. Yokota M, Miyanaga G, Yonemura K: Declining of memory functions of normal elderly persons. Psychiatry Clinical Neuroscience (2000) 54: 217-225.
19. Kress JP, Gehlbach B, Lacy M, Pliskin N, Pohlman AS, Hall JB: The long-term psychological
effects of daily sedative interruption on critically ill patients. American Journal of Critical Care Medicine (2003) 168: 1457-1461.
Discomfort and factual recollection
82
Chapter 6
83
Are clinical observations of breathing
and pulmonary function related in
patients after abdominal surgery?
Johannes P. van de Leur 1,2 , Peter Smit 1, Alida A. Broekema 3,
Thomas W. van der Mark 4 , Cees P. van der Schans 1,2.
1 Center for Rehabilitation, University Medical Center Groningen, The Netherlands 2 Northern Center for Health Care Research, Groningen, The Netherlands
3 Department of Anaesthesiology, University Medical Center Groningen, The Netherlands 4 Department of Pulmonology, University Medical Center Groningen, The Netherlands
Published in: Physiotherapy Theory and Practice 2003, 19, 45-52
COB and Pulmonary function
84
Abstract
Introduction Decline in pulmonary function after major abdominal surgery is thought to be identified in daily assessment by observation of breathing and pain intensity. Measurement of pulmonary function is usually not included in the assessment of the patient in the post-operative period. The aim of this study was to investigate the relationship between clinical observation of breathing (COB) and decline in pulmonary function and the relationship between pulmonary function and pain. Patients and methods 89 patients, admitted for elective major mid- and upper-abdominal surgery, participated in our study. COB covered the following parameters: 1) Abdominal expansion, Side expansion, High thoracic expansion, Paradoxical breathing, Symmetry of thorax expansion, Ability to cough, Ability to huff, and Signs of mucus retention. Pain intensity was assessed at rest (VAS) and during breathing exercises and coughing (VAS-F) using a visual analogue scale. FEV1, FVC and PEFR were performed on the pre-operative day and for seven post-operative days. Results The correlation coefficient over seven days between COB and FEV1 was 0.26 (0.002 < P < 0.14), and FVC 0.25 (0.001 < P < 0.2) and PEFR 0.19 (0.001 < P < 0.49). The correlation coefficient between VAS and FEV1 was -0.22 (0.007 < P < 0.642), and FVC -0.22, (0.002 < P < 0.548) and PEFR -0.21 (0.001 < P < 0.725). The correlation coefficient between VAS-F and FEV1 was -0.18 (0.008 < P < 0.581), and FVC -0.20, (0.001 < P < 0.569) and PEFR -0.22 (0.001 < P < 0.794). Conclusion A poor correlation is found between clinical observation of breathing and pulmonary function after abdominal surgery.
Chapter 6
85
Introduction
Pulmonary function is impaired after upper abdominal surgery (Ali, Weisel,
Layug, Kripke and Hechtman 1974; Johnson 1975). Ali (Ali, Weisel, Layug, Kripke,
and Hechtman 1974) found a decrease of forced vital capacity of 63% after
upper abdominal surgery. Ali (Ali, Weisel, Layug, Kripke and Hechtman 1974)
and Johnson (Johnson 1975) found a decline of pulmonary function dependent
upon site of surgical incision. This decline in pulmonary function is due to
changes in diaphragmatic function (Ford, Rosenal, Clergue and Whitelaw 1993;
Bartlett 1980; Simonneau, Vivien, Sartene et al. 1983). Reduction of
diaphragmatic contraction (Morran, Finlay, Mathieson, McKay, Wilson, and
McArdle 1983) and pain intensity (Taura, Planella, Balust et al. 1994) result in
changes in respiratory movements. Daily assessment (Maitre, Similowsky and
Derenne 1995) of the clinical pulmonary status is performed by physiotherapists.
This assessment includes breathing pattern, ability to cough, and evacuation of
mucus. Abnormal breathing pattern and severe pain are considered as
indications for pulmonary function impairment. However, it is not clear whether
this clinical assessment of breathing is a valid method to identify a decrease in
pulmonary function after abdominal surgery. Regular pulmonary function
testing in the post-operative period is uncommon. The purpose of our study was
to investigate the relationship between pulmonary function and clinical
observation of breathing after major abdominal surgery and the relationship
between pulmonary function and pain.
Patients and Methods
After written informed consent 89 adult patients, scheduled for elective major
mid- and upper-abdominal surgery, were included preoperatively. This study
was approved by the hospital ethics committee. Patients included had an
American Society of Anaesthesiologists (ASA) classification 1, 2 or 3. (Owens, Felts
and Spitznagel-EL 1978) and were scheduled for Abdominal Aortic, Pancreatic,
COB and Pulmonary function
86
Hepatobiliary, Upper Abdominal (other), and Colonic surgery. Distribution,
preoperative pulmonary function, and patient characteristics are described in
table 1.
Table 1. Patients’ characteristics. n= 89
Age in years, mean (SD) 52 (17)
Gender, male in % 55
ASA physical status in number of patients I/II/III 27/46/16
Type of surgery, in number of patients
Abdominal aortic
Pancreatic
Hepatobiliary
Upper abdominal (other)
Colonic
14
8
16
26
25
Preoperative FEV1 in l/sec, mean (SD) [% pred. (SD)] 3.0 (0.9) [91 (16)]
Preoperative FVC in l, mean (SD) [% pred. (SD)] 3.6 (1.0) [90 (16)]
Preoperative PEFR in l/min, mean (SD) [% pred. (SD)] 430 (120) [91 (20)]
Breathing was assessed during maximum voluntary inspiratory effort while the
patient was in a semi-recumbent position. Every item was scored visually. If
movement was met within the preset criteria than this item was scored as 1, if
not than the item was scored as 0. By entering the scores in the equation a total
score was calculated. The following parameters were scored as present, when
the following criteria were met:
Abdominal expansion (AB): Visible distension movement of the abdominal wall during
inspiration.
Side expansion (ST): Visible outward movement of the lateral chest during
inspiration.
High thoracic expansion (HT): Visible forward and upward movement of the upper
chest during inspiration.
Paradoxical breathing (PARA): Visible inward movement of the abdominal wall when
the chest shows an outward movement or a visible
outward movement of the abdominal wall when the
chest shows an inward movement.
Symmetry of expansion (SYM): Symmetrical movement of the left and right side of the
chest.
Ability to cough (CO): Ability to make a forceful expiration after building up a
positive pressure with a closed glottis at a high volume.
Ability to huff (HU): Forced expiratory volume with an opened glottis at mid
to low volume.
Mucus retention (MU): Presence of rhonchi during palpation of the chest.
Chapter 6
87
Thereafter a total Clinical Observation of Breathing score (COB) was calculated
by the following equation:
COB = HT + ST + AB + SYM - PARA + CO + HU – MU
The highest possible score in this equation is six, reflecting normal breathing with
no apparent mucus retention and the ability to cough and huff.
Forced Expiratory Volume in 1 second (FEV1), Forced Vital Capacity (FVC), and
Peak Expiratory Flow Rate (PEFR) were measured with the patient in the same
semi-recumbent position using an electronic hand-held spirometer "Microplus"
(Sensor Medics, The Netherlands). The accuracy is ± 2% within a flow range of 2
to 12 litres per second. The maximum value for each variable of three attempts
was taken for analysis. All pulmonary function variables were expressed as
absolute values and as percentages of the pre-operative values.
Patients were asked to quantify the pain intensity of operation site on a Visual
Analogue Scale (VAS). The patient was asked to indicate on a 10 cm horizontal
line the level of pain. Pain intensity was measured at rest (VAS). After breathing
exercises and coughing pain intensity was measured (VAS-F) again. The
distance on the line was registered in centimetres with 1 decimal.
Study design
All measurements were performed on the pre-op day and on seven post-
operative days between two and four o’clock in the afternoon. Patients
participated in a prospective randomized clinical trial examining effects of three
groups of post-operative analgesia: continuous epidural morphine combined
with bupivacaine, continuous epidural sufentanil combined with bupivacaine,
and fixed rate intramuscular morfine injections. No difference in pulmonary
function between the three groups of post-operative analgesia was found
(Broekema, Veen, Fidler, Gielen, and Hennis, 1998).
Statistical Analysis
Statistical analysis was performed using SPSS 10. All recorded data were taken
for analysis including those of patients who were discharged or stopped
COB and Pulmonary function
88
cooperating with treatment. In total six patients were discharged early or
stopped their cooperation with the study. Descriptive statistics as mean and
standard deviation (SD) were calculated for the following variables: FEV1, FVC
and PEFR. Median and ranges were calculated on COB, VAS and VAS-F.
For each separate day a Spearman correlation coefficient was calculated
between spirometry variables and COB scores.
Results
Separate clinical items are expressed in percentages in table 2, describing a
change in breathing pattern during the post-operative period. The percentage
of presence of abdominal expansion is reduced in day 1 to 48. The percentage of
presence of abdominal expansion is returned to 94 on day 7. Percentage of
presence of paradoxical breathing is increased in the first three post-operative
days; after the third post-operative day the percentage of this clinical sign is
educed to preoperative levels. Clinical signs of being able to cough reduced to
20 % of pre-operative level. Sign of mucus retention is increased in the first three
post-operative days.
Table 2. Separate clinical observation of breathing (COB) variable expressed as % over 7 days post
COB scores decreased on day 1 as compared to the pre-operative score, and
increased gradually during the seven consecutive following post-operative days
(table 3).
Chapter 6
89
A decline in spirometry values to approximately 50% of the pre-operative
values was observed on day 1. An increase was observed during the following
post-operative days (table 3, figure 1); however, none of the mean values
reached the preoperative values.
Figure 1: Boxplot of the FVC expressed as percentage of the pre-operative values on the post-operative
days, outliers are shown as O.
The median (min-max) pain intensity expressed in VAS was 0 (0 - 2.5) cm on
the pre-operative day. On the first post-operative day the median (min-max)
VAS was 2 (0 - 10) cm. The VAS was reduced to 0.6 (0 - 4.5) cm on day 7 (table
3).
6772777884858089N =
Postoperative day
7654321-1
FVC
as
perc
enta
ge o
f pre
-ope
rativ
e va
lue
140
120
100
80
60
40
20
0
COB and Pulmonary function
90
CO
B, m
edia
n (m
in-m
ax)
5
(3 -
6)
3 (1
- 5
) 4
(1 -
5)
4 (1
- 6
) 5
(2 -
6)
5 (2
- 5
) 5
(0 -
6)
5 (2
- 6
)
R. R
. per
min
ute,
mea
n (s
d)
18 (
5)
21 (
5)
20 (
4)
19 (
4)
19 (
5)
19 (
4)
19 (
4)
20 (
5)
VA
S in
cm
, med
ian
(min
-max
) 0
(0
– 2
.5)
2 (0
- 10
) 1.5
(0
– 6
.9)
0.6
(0
– 8
.5)
0.5
5 (0
- 5
.4)
0.5
(0
– 5
.4)
0.8
(0
– 6
.5)
0.6
(0
- 4
.5)
VA
S-F
in c
m, m
edia
n (m
in-m
ax)
0 (
0 -
3.6
) 3.
6 (0
– 9
.0)
2.7
(0 –
8.6
) 1.7
(0
- 10
) 1.3
(0
- 8
) 0
.9 (
0 –
7.2
) 1.2
(0
– 6
.7)
1.2 (
0 –
6.4
)
FEV
1 in
l/se
c, m
ean
(sd
) %
pre
-op
era
tive
3.0
(0
.9)
1.5
(0
.6)
51 (
15)
1.6 (
0.6
) 53
(15
)
1.8 (
0.7
) 60
(19
)
2.0
(0
.8)
65 (
18)
2.2
(1.0
) 71
(27
)
2.2
(0.8
) 72
(18
)
2.2
(0.8
)
74 (
18)
FVC
in l,
mea
n (s
d)
% p
re-o
per
ativ
e (s
d)
3.6
(1.0
) 10
0
1.8 (
0.7
) 52
(16
)
1.9 (
0.7
) 54
(16
)
2.1
(0.9
) 60
(20
)
2.3
(1.0
) 66
(20
)
2.5
(0.9
) 70
(18
)
2.5
(0.8
) 72
(19
)
2.7
(0.9
)
76 (
20)
PEF
R in
l/m
in, m
ean
(sd
) %
pre
-op
erat
ive
(sd
)
430
(12
0)
100
213
(90
) 51
(21
)
217
(75)
53
(20
)
261 (
95)
63 (
26)
294
(10
7)
70 (
26)
319
(10
9)
77 (
30)
328
(114
)
80 (
29)
331 (
122)
79
(26
)
Th
e A
NO
VA
ove
r th
e p
re-
and
7 p
ost-
oper
ativ
e p
erio
d sh
owed
a si
gnifi
cant
p v
alu
e of
< 0
.00
1 in
all
vari
ab
les.
Chapter 6
91
CO
B S
CO
RE
0.2
4* [n
= 78
] 0
.35*
[n=
81]
0.3
1* [n
= 80
] 0
.25*
[n=
78]
0.3
6* [n
= 75
] 0
.19
[n=
70]
0.19
[n
= 64
]
R.R
. -0
.13
[n=
80]
-0.3
4* [n
= 85
] -0
.32*
[n=
83]
-0.2
4* [n
= 78
] -0
.33*
[n=
77]
-0.3
9**
[n=
72]
-0.3
1* [n
= 67
]
VA
S -0
.25*
[n=
80]
-0.3
3**
[n=
85]
-0.2
6* [n
= 84
] -0
.14
[n=
78]
-0.19
[n
= 77
] -0
.25*
[n=
72]
-0.18
[n
= 67
]
FEV1
VA
S-F
-0.2
0
[n=
79]
-0.16
[n
= 85
] -0
.16
[n=
84]
-0.2
1 [n
= 75
] -0
.30
* [n
= 77
] -0
.19*
[n=
69]
-0.0
7 [n
= 67
]
CO
B S
CO
RE
0.2
3* [n
= 78
] 0
.35**
[n
= 81
] 0
.27*
[n=
80]
0.2
2* [n
= 78
] 0
.37**
[n
= 75
] 0
.16
[n=
70]
0.17
[n
= 64
]
R.R
. -0
.17
[n=
80]
-0.3
7**
[n=
85]
-0.3
8**
[n=
83]
-0.2
7* [n
= 78
] -0
.29*
[n=
77]
-0.3
6* [n
= 72
] -0
.31*
[n=
67]
VA
S -0
.21
[n=
80]
-0.3
1* [n
= 85
] -0
.20
[n
= 84
] -0
.13
[n=
78]
-0.2
5* [n
= 77
] -0
.33*
[n=
72]
-0.3
1* [n
= 67
]
FVC
VA
S-F
-0.14
[n
= 79
] -0
.13
[n=
85]
-0.0
6 [n
= 84
] -0
.18
[n=
75]
-0.3
7**
[n=
77]
-0.2
6* [n
= 69
] -0
.25*
[n=
67]
CO
B S
CO
RE
0.17
[n
= 78
] 0
.12
[n=
81]
0.19
[n
= 80
] 0
.20
[n
= 78
] 0
.37**
[n
= 75
] 0
.18
[n=
70]
0.0
9 [n
= 64
]
R.R
. -0
.13
[n=
80]
-0.19
[n
= 85
] -0
.15
[n=
83]
-0.2
0
[n=
78]
-0.2
6* [n
= 77
] -0
.33*
[n=
72]
-0.2
8* [n
= 67
]
VA
S -0
.28*
[n=
80]
-0.3
7**
[n=
85]
-0.3
1**
[n=
84]
-0.2
3* [n
= 78
] -0
.09
[n=
77]
-0.16
[n
= 72
] -0
.17
[n=
67]
PEFR
VA
S-F
-0.3
3* [n
= 79
] -0
.42**
[n
= 85
] -0
.20
[n
= 84
] -0
.30
* [n
= 75
] -0
.16
[n=
77]
-0.10
[n
= 69
] -0
.03
[n=
67]
*
p <
0.0
5 **
p,0
.00
1 [
n ]
is th
e ex
act
num
ber
of
pat
ient
s whe
re c
orre
lati
on c
oeff
icie
nt w
as
calc
ula
ted
up
on.
COB and Pulmonary function
92
The median (min–max) pain intensity during breathing exercises and coughing
in VAS-F was 0 (0 - 3.6) on the pre-operative day. On the first post-operative
day the median (min–max) VAS-F was 3.6 (0 - 9) cm. The VAS-F was reduced
to 1.2 (0 – 6.4) cm on day 7 (table 3).
Relationship between clinical observation of breathing and pulmonary function:
COB and FEV1 are significantly correlated on days 1, 2, 3, 4 and 5, COB and FVC
on days 1, 2, 3, 4 and 5, and COB and PEFR on day 5 (table 4).
Relationship between pain intensity and pulmonary function:
VAS and FEV1 are significantly correlated on days 1, 2, 3 and 6 (table 4), VAS
and FVC on days 2 and 3 (table 3), VAS and PEFR on days 1, 2, 3 and 4 (table
4). Differences in exact numbers of patients and the numbers evaluated in the
study are due to missing values and early discharge.
Discussion
In this study we found a significant but poor correlation among COB score, pain
intensity, and pulmonary function variables. Changes in COB score and pain
intensity after upper abdominal surgery underestimate the severe decline in
pulmonary function in these patients. A marked decrease in pulmonary
function and a decline in COB score were found after upper abdominal surgery.
The recovery in pulmonary function was still incomplete seven days after
surgery. Ali (Ali et al. 1974) also described a decline in pulmonary function that
recovers over seven post-operative days to 70% of preoperative values. The
COB score returned to the pre-operative value on day 4.
Changes in breathing pattern, such as the absence of predominant chest or
abdominal movements, could indicate diaphragmatic dysfunction.
Asynchronous thoracic-abdominal movements, i.e., paradoxical breathing, may
indicate respiratory failure.
Chapter 6
93
Non-symmetrical thoracic expansions may indicate atelectasis or pneumonia. In
our study we recorded breathing pattern during voluntary maximal inspiratory
effort. A maximal inspiratory manoeuvre makes movement more visible and
may reflect the patient's vital capacity rather than at rest. In order to compare
clinical observation of breathing with spirometry values we transferred
qualitative data into ordinal quantitative data by using the equation. A
limitation of this study was that the level of voluntary inspiratory effort was not
quantified. Therefore we were unable to determine whether the effort was
indeed the maximum and some clinical signs were not present due to lack of
effort from the patients’ participation. Transfer of physical assessment scores into
an ordinal scoring has earlier been described by Sigg and Fallucca (Sigg &
Fallucca 1983). They classified the following parameters as 0, 1, or 2: respiratory
rate, respiratory pattern, depth of respiration, lung sounds, level of conscious-
ness, colour, blood pressure, pulse, activity, pre-operative physical status (ASA).
These parameters were accumulated into a total score, reflecting the presence
or absence of breathing abnormalities. Our score consists of abdominal
expansion, side expansion, high thoracic expansion, paradoxical breathing,
symmetry of expansion, ability to cough, ability to huff, and signs of retention of
sputum. We classified the scores as 0 or 1. These scores, described by Sigg and us,
include parameters that are clinically used, but were not tested on validity and
reliability. Nominal values as we have used are limited in comparison with ratio
variables. In our equation six nominal variables, when present, are weighed
positive and 2 nominal variables, when present, are weighed negative. In Table
2 we presented these variables separately. Of the positive nominal variables,
high thoracic (HT) and symmetry (SYM) of expansion were seldom not present,
making the equation less susceptible to changes. Nevertheless, in everyday
practice these parameters are taken into consideration as well as emotional and
cognitive behaviour, sweatiness, colour, and respiratory rate.
Spirometry values decreased to about 50% of pre-operative values. After 7
days these values recovered to only approximately 75% of the pre-operative
value. Similar decrease in pulmonary function after abdominal surgery has
been described by several authors. Hansdottir and colleagues (Hansdottir et al.
1996) found a reduction of vital capacity of approximately 50% on the first two
COB and Pulmonary function
94
post-operative days. Tsui (Tsui et al., 1991) described the same reduction in
spirometry values in patients post oesophageal surgery during the first two post-
operative days. Ali (Ali et al. 1974) described a recovery of 70% on the seventh
post-operative day. The decrease in PEFR could be explained by a less forceful
voluntary contraction of the abdominal muscles or reduced motivation. Cotes
(Cotes, 1993) and Nunn (Nunn, 1993) describe PEFR as having an effort depen-
dent factor due to many inhibiting elements including motivation and muscular
force. A less forceful voluntary contraction of the abdominal muscles or reduced
motivation may be due to pain or anxiety of pain.
We found a poor correlation between intensity of pain and decline in
pulmonary function. This is in contrast with the results of the study of Taura et
al. (Taura et al., 1994). Taura showed that FEV1 was decreased in patients with
VAS scores higher than 5. The mean VAS pain score of the patients in Taura's
study was 3.5 cm in the treatment group and 5.3 cm in the placebo group, while
the median VAS score in our study was only 2 cm. The median VAS-F during
breathing exercises and couging was comparable to Taura’s study. Taura did
not differentiate between pain during rest and breathing exercises and
coughing. In our study, patients received post-operatively pain relief for more
than four days, with either continuous epidural (morphine/bupivaciane or
sufentanil/bupivaciane) or fixed-rate intramuscular (morphine) pain relief.
Broekema (Broekema et al. 1998) reported that post-operative analgesia at
rest and during coughing and movement was significantly better in the epidural
groups than in the intramuscular group during the five consecutive days. There
were no significant differences between the epidural groups. If, in our analysis,
pain was a limiting factor in movement and generating muscle force, then a
correlation could be expected among VAS, VAS-F, and spirometry values. Our
study indicates that the decline in pulmonary function after abdominal surgery
is not solely the result of post-operative pain. It has been shown that other
mechanisms may contribute to the decline in pulmonary function after upper
abdominal surgery, such as inhibition of diaphragmatic contraction (Simonneau
et al. 1983; Pansard et al. 1993) through inhibition of the phrenic nerve (Reeve et
al. 1951), different operation techniques and incision sites (Ali et al. 1974; Garcia-
Chapter 6
95
Valdecasas et al. 1988), and abdominal muscles impairment (Sharp et al. 1975;
Duggan et al. 1989).
The validity of the COB score is poor in patients after abdominal surgery.
Because of the poor correlation between intensity of pain and decline in
pulmonary function values, the COB and pulmonary function tests should be
used independently of the intensity of pain to determine the clinical pulmonary
status. This study shows that the COB scoring is a less sensitive instrument. Only
large changes in volumes may be detected during the clinical observation of
breathing. The pulmonary function test can detect smaller decreases in FEV1,
FVC, and PEFR.
Conclusion
Pulmonary function after mid- and upper-abdominal surgery decreases
considerably. The pulmonary function has a poor correlation with clinical
observation of breathing or pain. The COB score relates poorly to pulmonary
function tests because COB score is a less sensitive clinical instrument in our
studied population.
Reference list
Ali J, Weisel RD, Layug AB, Kripke BJ, Hechtman HB. Consequences of post-operative alterations in respiratory mechanics. American Journal of Surgery (1974) 128, 376-382. Bartlett RH. Pulmonary pathophysiology in surgical patients. Surgical Clinics of North America (1980) 60, 1323-1338. Broekema AA, Veen A, Fidler V, Gielen MJ, Hennis PJ. Post-operative analgesia with intramuscular morphine at fixed rate versus epidural morphine or sufentanil and bupivacaine in patients undergoing major abdominal surgery. Anesthesia and Analgesia (1998) 87, 1346-1353. Cotes JE. Maximal flow rates. In: Cotes J.E. (Ed.), Lung function: assessment and application in medicine. (pp. 114-121). London (1993): Blackwell. Duggan J, Drummond GB. Abdominal muscle activity and intra-abdominal pressure after abdominal surgery. Anesthesia and Analgesia (1989) 69, 598-603. Ford GT, Rosenal TW, Clergue F, Whitelaw WA. Respiratory physiology in upper abdominal surgery. Clinics in Chest Medicine (1993) 14, 237-252.
COB and Pulmonary function
96
Garcia-Valdecasas J, Almenara R, Cabrer C, De-Lacy AM, Sust M, Taura P, Fuster J, Grande L, Pera M, Sentis J. Subcostal incision versus midline laparotomy in gallstone surgery: a prospective and randomized trial. British Journal of Surgery (1988) 75, 473-475. Hansdottir V, Bake B, Nordberg G. The analgesic efficacy and adverse effects of continuous epidural sufentanil and bupivacaine infusion on thoracotomy. Anesthesia and Analgesia (1996) 83, 394-400. Johnson WC. Post-operative ventilatory performance: dependence upon surgical incision. American Surgeon (1975) 41, 615-619. Maitre B, Similowsky T, Derenne JP. Physical assessment of the adult with respiratory diseases: inspection and palpation. European Respiratory Journal (1995) 8, 1584-1593. Morran CG, Finlay IG, Mathieson M, McKay AJ, Wilson N, McArdle CS. Randomized controlled trial of physiotherapy for post-operative pulmonary complications. British Journal of Anaesthesia, (1983) 55, 1113-1117. Nunn JF. Measurement of ventilatory capacity. (p 134) In: Nunn JF. Applied Respiratory Physiology. London (1993): Butterworth & Co. Owens WD, Felts JA, Spitznagel-El J. ASA physical status classifications: a study of consistency of ratings. Anesthesiology (1978) 49, 239-243. Pansard JL, Mankikian B, Bertrand M, Kieffer E, Clergue F, Viars P. Effects of thoracic extradural block on diaphragmatic electrical activity and contractility after upper abdominal surgery. Anesthesiology, (1993) 78, 63-71. Reeve EB, Nanson EM, Rundle F.F. Observation on inhibitory reflexes during abdominal surgery. Clinical Science, (1951) 10, 65-87. Sharp JT, Goldberg NB, Druz WS, & Danon J. Relative contributions of rib cage and abdomen to breathing in normal subjects. Journal of Applied Physiology, (1975) 39, 608-618. Sigg LV, Fallucca LL. Recognizing hypoventilation in the recovery room. Association of Respiratory Nurses Journal, (1983) 38, 270-285. Simonneau G, Vivien A, Sartene R, Kunstlinger F, Samii K, Noviant Y, Duroux P. Diaphragm dysfunction induced by upper abdominal surgery. Role of post-operative pain. American Review of Respiratory Disease, (1983) 128, 899-903. Taura P, Planella V, Balust J, Beltran J, Anglada T, Carrero E, Burgues S. Epidural somatostatin as an analgesic in upper abdominal surgery. Pain, (1994) 59, 135-140. Tsui SL, Chan CS, Chan AS, Wong SJ, Lam CS, Jones RD. Post-operative analgesia for oesophageal surgery: a comparison of three analgesic regimens. Anaesthesia and Intensive Care, (1991) 19, 329-337.
97
General discussion and conclusions
General discussion and conclusions
98
After major surgery, artificial ventilation is often necessary to assist decreased
respiratory effort due to anesthetic, sedative medication or surgical procedures.
Artificial ventilation requires a tube, which is inserted through the glottis into the
trachea. The mechanical ventilator pumps air through the tubes into the lungs.
When a pre-set volume or pressure is reached, a valve opens the expiratory
gate and air is released into the atmosphere. The presence of this tube in the
trachea leads to impairment of mucus transport in the lungs and it becomes
impossible for the patient to expectorate accumulated mucus. To relieve the
patient of this accumulated mucus endotracheal suctioning is widely used. This
procedure consists of disconnection from the mechanical ventilator, insertion of a
suction catheter, and application of negative pressure resulting in extraction of
mucus from the main bronchi and trachea. It is assumed that removal of mucus
by endotracheal suctioning improves ventilation and prevents pulmonary
infections. However, until now there is little evidence to support this assumption.
On the other hand, many complications of endotracheal suctioning have been
described: hypoxia, tissue trauma to the tracheal and bronchial mucosa, cardiac
Paradoxale ademhaling, Symmetrie van thorax expansie, Mogelijkheid om te
hoesten, Mogelijkheid om te huffen en Klinische tekenen van mucus retentie.
Pijn intensiteit werd beoordeeld door gebruik van een visueel analoge schaal.
FEV1, FVC en PEFR testen werden uitgevoerd op de preoperatieve dag en op
zeven postoperatieve dagen.
Een slechte correlatie werd gevonden tussen klinische observatie van de
ademhaling en longfunctie of pijn na abdominale chirurgie.
Algemene discussie
De algemene discussie en conclusies combineren de belangrijkste bevindingen
van gedane onderzoeken. Minimaal invasieve luchtweg zuigen is gelijkwaardig
aan routinematig endotracheaal zuigen, maar resulteert in minder suction
related adverse events, minder herinnering van zuigen en minder stress.
Desondanks kan MIAS niet in alle situaties worden toegepast. Minimaal invasief
luchtweg zuigen zou de “default setting” voor mucus clearance bij IC patienten
moeten zijn. Speciale zuigcatheters zouden moeten worden gefabriceerd die
met de beperkte lengte niet langs het einde van de endotracheale tube komen.
Als alternatief, kunnen standaard catheters gemarkeerd worden om aan te
geven dat er te distaal van de endotracheale tube gezogen wordt.
Een IC kan gezien worden als een stressvolle omgeving, hetgeen tot
onplezierige herinneringen kan leiden. Het is onduidelijk, tot op heden, hoe dit
te voorkomen is. Diepere sedatie met standaard medicatie is niet het antwoord
aangezien dit kan leiden tot een verhoogd post-traumatisch dystress syndroom
in de periode na de IC opname. Een multidisciplinaire aanpak voor patienten,
die zijn ontslagen na een langdurig verblijf op de IC, kan wellicht een geschikte
oplossing zijn.
Het huidige klinisch evalueren van longfunctie van patiënten na IC
ontslag is onvoldoende. Accurate metingen van longfunctie met een draagbare
spirometer op de derde dag postoperatief zou geïmplementeerd kunnen
worden, om mogelijke pulmonale complicaties te evalueren.
Samenvatting
120
121
Dankwoord Tijdens het klinisch behandelen van geïntubeerde IC patiënten is het idee ontstaan om onderzoek te doen naar de effectiviteit van het endotracheaal longtoilet. Deze relevante vraag heeft veel subvragen opgeroepen. Helaas is het niet mogelijk om alle vragen en antwoorden te beschrijven in dit proefschrift. Tijdens het opzetten van het onderzoek, data verzamelen, analyseren, en uiteindelijk schrijven van artikelen, heb ik erg veel geleerd. Mijn perceptie van onderzoek doen was als het lezen van een spannend jongensboek. Van idee tot artikel werd het een grote ontdekkingsreis, zoals Jules Verne beschreef in “De reis om de wereld in 80 dagen”. Gelukkig lukte het mij, net als Phileas Fogg, met hulp en door samenwerking het doel te bereiken. Velen hebben bijgedragen aan het tot stand komen van dit proefschrift. Het onderzoek is uitgevoerd onder begeleiding van bureau OKER van de afdeling Revalidatie, op de IC’s van de afdelingen Chirurgie en Thoraxcentrum. Dit proefschrift tot stand gekomen door een unieke samenwerking tussen deze afdelingen. Een aantal van mijn begeleiders wil ik graag persoonlijk bedanken. Dr. C.P. van der Schans, lector Transparante Zorg, Hanzehogeschool te Groningen. Beste Cees, hartelijk dank voor jouw voortdurende inzet en doorzettingsvermogen tijdens dit project. In het bijzonder jouw vertrouwen, in voor en tegenspoed, heeft mij geholpen tot dit product. Jouw kennis en kunde zijn onontbeerlijk geweest in het totstandkomen van dit onderzoek, de opzet, de analyses, de artikelen en het proefschrift. Prof. Dr. J.H. Zwaveling, intensivist, Intensive Care, Academisch Ziekenhuis Maastricht. Beste Jan Harm, hartelijk dank voor de begeleiding, inzet en relativerende opmerkingen. Jouw fundamentele bijdragen met name wat betreft het formuleren van vragen en antwoorden hebben een duidelijke lijn in het proefschrift gebracht. Prof. Dr. J.H.B. Geertzen, revalidatiearts, Revalidatie, Universitair Medisch Centrum Groningen. Beste Jan, je bent een harde werker. Met jouw commentaar op mijn stukken kwamen ze supersnel weer in mijn bezit. Hartelijk dank voor het begeleiden van mijn promotie. Jouw gedrevenheid en inzet hebben veel bijgedragen aan het voltooien van dit proefschrift. Drs. B.G. Loef, intensivist, Thoraxcentrum, Universitair Medisch Centrum Groningen. Beste Bert, de samenwerking met jou is van groot belang geweest om dit project in het Thoraxcentrum te starten, gaande te houden en tot een bevredigend einde te hebben gebracht. Prof. Dr. B.G. Deelman, professor emeritus in Neuropsychologie, Universitair Medisch Centrum Groningen. Beste prof. Deelman, Uw heldere manier van denken heeft mij in de opzet van het onderzoek naar feitelijke herinnering, veel structuur en duidelijkheid gegeven. In het bijzonder voor het ontwikkelen van de vragenlijst, de proces-analyse en de resultaten, zijn de overleg momenten en digitale correspondentie met U belangrijk geweest.
Dankwoord
122
Prof. Drs. W.H. Eisma en Prof. Dr. K. Postema, hoofden Revalidatie Universitair Medisch Centrum Groningen. Beste prof. Eisma en prof. Postema, hartelijk dank voor het geven van de mogelijkheid om als fysiotherapeut binnen de afdeling Revalidatie/Fysiotherapie te promoveren. Klaziena Tiggelaar, Ellen Timmermans, Josje Wiersma-van Donselaar, secretaresses Universitair Medisch Centrum Groningen. Graag wil ik jullie bedanken voor de oneindige keren contact over de wel of niet aangekomen mail, te maken afspraken en ook voor gewoon tijd voor een praatje. Dr. P.U. Dijkstra, epidemioloog-onderzoeker-collega fysiotherapeut Universitair Medisch Centrum Groningen. Beste Pieter, je heb altijd even tijd voor een vriendelijk praatje. Mijn vragen, hoe triviaal ook, zijn door jou altijd serieus beantwoord. Daarna kon ik altijd weer met een goed gevoel aan het werk. Bovendien zijn jouw vrijdagochtend serenades een inspiratie geweest. Paul Nijkrake, hoofd-fysiotherapie. Beste Paul, hartelijk dank voor het creëren van de mogelijkheid om mijzelf te ontplooien. Door jouw manier van processen op een afstand te volgen ontstond er ruimte voor groei en ontwikkeling. Hetgeen wel van beide partijen een duidelijkheid en overeenstemming in communicatie in doel en methode vereist. Margaret Wilson and Denise Britton, colleagues at Lewisham, National Trust University Hospital in London, England. Dear Maggie and Denise, you both have been the basis of my career in respiratory physiotherapy. Thank you for your support, tutoring and friendship. Alle fysiotherapeutische collega’s die bewust of minder bewust aan mijn functioneren hebben bijgedragen in de afgelopen zeven jaar. Graag wil ik jullie bedanken voor de collegialiteit en ruimte die van jullie heb ontvangen om dit project af te ronden. Alle IC verpleegkundige collega’s hartelijk dank voor de kritische noten en bereidheid tot samenwerken binnen dit project. Graag wil ik iedereen bedanken wiens naam ik niet expliciet heb genoemd maar die zijn of haar bijdrage heeft geleverd in het volbrengen van dit zevens jaar durende monsterproject. Dus UMCG-medewerkers van afdeling Inkoop tot Laboratorium: van Raad van Bestuur tot schoonmaakdienst: hartelijk dank. Beoordelingscommisie, Prof. Dr. L.P.H.J. Aarts, anesthesioloog UMCG, Prof. Dr. H.A.M. Kerstjens, longarts UMCG, Prof. Dr. H.A.A.M. Gosselink, fysiotherapeut, Katholieke Universiteit Ziekenhuis, Leuven België. Hartelijk dank voor de bereidwilligheid om zitting te nemen in de beoordelingscommissie en het beoordelen van mijn proefschrift.
123
Rob Douma en René Zorge, paranimfen. Beste Rob, vriend-collega, jouw kracht is een positieve wending te geven in moeilijke tijden d.m.v. knuffels en, op z’n tijd, wat klappen. En René, vriend-zwager, altijd een rustig luisterend oor, jouw aanwezigheid geeft mij ruimte voor een denkproces en de juiste handelingen. Gedrieën zullen wij de promotiedag tot een leuk geheel maken. Last, but not least. Yvonne van de Leur-Hessing, echtgenote en vriendin. Lieve Yvonne, je hebt een belangrijke bijdrage geleverd aan mijn functioneren. Samen hebben we veel lief en leed door gemaakt in de afgelopen negentien jaar. De laatste zeven jaren was ik gewoonlijk langer op het werk en zat vaker achter de computer dan afgesproken. Hiervoor was van jouw kant meestal begrip en medeleven, zeker als het trager ging dan door mij voorgesteld. Zie hier: van uitstel kwam geen afstel. Na de promotie zal de tijdinvestering in het onderzoek nihil zijn, dus veel vrije tijd opleveren. Wees gerust, deze “extra“ tijd zal ik goed benutten.
Dankwoord
124
125
Previous dissertations Rehabilitation Programs Research (from 1998 onwards) This thesis is published within the research program Rehabilitation Programs Research of the Northern Centre for Healthcare Research. More information regarding the institute and its research can be obtained from our internet site: www.med.rug.nl/nch. Rietman JS (2005) Treatment related morbidity in breast cancer patients; a comparative study between sentinel lymph node biopsy and axillary lymph node dissection.
Promotores: prof dr WH Eisma, prof dr HJ Hoekstra, prof dr JHB Geertzen, prof dr JW Groothoff Copromotor: dr PU Dijkstra
Brouwer S (2004) Disability in chronic low back pain.
Promotores: prof dr JHB Geertzen, prof dr JW Groothoff, prof dr LNH Göeken Copromotor: dr PU Dijkstra
Dekker R (2004) Long-term outcome of sports injuries.
Promotores: prof dr HJ ten Duis, prof WH Eisma, prof dr JW Groothoff Copromotor: dr CK van der Sluis
Schegget-Slaterus, MJ ter (2004) The quality of expert advice in relation to the act on facilities for the handicapped. Promotores: prof dr JW Groothoff, prof WH Eisma Schőnherr MC (2003) Functional outcome after spinal cord injury. Promotores: prof WH Eisma, prof dr JW Groothoff Sturms LM (2003) Pediatric traffic injuries; consequences for the child and the parents.
Promotores: prof WH Eisma, prof dr HJ ten Duis, prof dr JW Groothoff Copromotor: dr CK van der Sluis
Meijer JWM (2002) The diabetic foot syndrome; diagnosis and consequences.
Promotores: prof WH Eisma, prof dr JW Groothoff Copromotor: dr TP Links, dr AJ Smit
Schoppen T (2002) Functional outcome after a lower limb amputation.
Promotores: prof WH Eisma, prof dr JW Groothoff, prof dr LNH Göeken Referenten: dr AM Boonstra, dr J de Vries
Noordelijk Centrum voor Gezondheidsvraagstukken
126
Rommers GM (2000) The elderly amputee: rehabilitation and functional outcome.
Promotores: prof WH Eisma Copromotor: dr JW Groothoff
Halbertsma JPK (1999) Short hamstrings & stretching: a study of muscle elasticity.
Promotores: prof WH Eisma, prof dr LNH Göeken Copromotor: dr JW Groothoff Referent: dr ir AL Hof
Geertzen JHB (1998) Reflex sympathetic dystrophy: a study in the perspective of rehabilitation medicine.
Promotores: prof WH Eisma, prof dr HJ ten Duis Copromotor: dr JW Groothoff Referent: dr PU Dijkstra
Sluis CK van der (1998) Outcomes of major trauma.
Promotores: prof dr HJ ten Duis, prof WH Eisma
Stellingen behorende bij het proefschrift
Clearance of bronchial mucus after major surgery Johannes Peter (Hans) van de Leur, 5 oktober 2005
1. Minimal Invasive Airway Suctioning is te verkiezen als eerste behandeling
om bij geïntubeerde IC patiënten geaccumuleerd mucus te verwijderen. (dit proefschrift)
2. Minimal Invasive Airway Suctioning is gelijkwaardig ten opzichte van
Routine Endotracheal Suctioning in beademingsduur in een populatie van langdurig beademde postchirurgische IC patiënten. (dit proefschrift)
3. Ervaringen en meningen over (dis)comfort van patiënten is niet altijd
gebaseerd op feitelijke herinneringen. 4. Preventie van pulmonale complicaties na bovenbuikchirurgie dient voor de
fysiotherapie een hoge prioriteit te zijn. 5. De meeste Suction Related Adverse Events hebben weinig of geen invloed
op de ligduur bij langdurig beademde IC patiënten. (dit proefschrift) 6. De incidentie van pulmonale infecties wordt niet verhoogd door Minimal
Invasive Airway Suctioning ten opzichte van Routine Endotracheal Suctioning, ondanks dat de zuigslang zelf het mucus niet intratracheaal of bronchiaal verwijdert. (dit proefschrift)
7. Routine Endotracheal Suctioning veroorzaakt meer stressrespons dan
Minimal Invasive Airway Suctioning. (dit proefschrift) 8. Routine Endotracheal Suctioning is een veilige optie wanneer Minimal
Invasive Airway Suctioning onvoldoende resultaat geeft bij geaccumuleerd mucus.
9. Resultaat van je onderzoek is een product van uitkomst, public relations
activiteiten en mogelijkheden tot implementatie. 10. Brainstormen kan alleen maar plaatsvinden bij twee of meer partijen met
een hoge en lage ideeëndruk. Bij partijen met gelijkwaardige ideeëndruk kan er geen stroming ontstaan.
11. Motorrijden en promoveren hebben veel overeenkomsten: je kunt het op
latere leeftijd doen en om het te volbrengen heb je veel enthousiasme en doorzettingsvermogen nodig.
12. Mono-disciplinaire behandeling van patiënten met chronische pijn is een