University of Groningen Different aspects of hyperthermic isolated limb perfusion Ginkel, Robert Johannes van IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2002 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Ginkel, R. J. V. (2002). Different aspects of hyperthermic isolated limb perfusion. s.n. Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license. More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne- amendment. Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 19-12-2021
Transcript
University of Groningen
Different aspects of hyperthermic isolated limb perfusionGinkel, Robert Johannes van
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2002
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Ginkel, R. J. V. (2002). Different aspects of hyperthermic isolated limb perfusion. s.n.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license.More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne-amendment.
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
This research was financially supported by the Dutch Cancer Society (Nederlandse
Kankerbestrijding KWF) grant GUKC 90-06.
ISBN: 90-367-1716-7
Page lay out: P. van der Sijde, Groningen, The Netherlands
Printed by: Ponsen en Looijen BV, Wageningen, The Netherlands
RIJKSUNIVERSITEIT GRONINGEN
DIFFERENT ASPECTS OF HYPERTHERMIC ISOLATED LIMB
PERFUSION
Proefschrift
ter verkrijging van het doctoraat in de
Medische Wetenschappen
aan de Rijksuniversiteit Groningen
op gezag van de
Rector Magnificus, dr. F. Zwarts,
in het openbaar te verdedigen op
woensdag 20 november 2002
om 16.00 uur
door
Robert Johannes van Ginkel
geboren op 12 mei 1964
te Amsterdam
.
Promotores Prof. dr. H.J. Hoekstra
Prof. dr. H. Schraffordt Koops
Prof. dr. W. Vaalburg
Beoordelingscommissie Prof. dr. B.B.R. Kroon
Prof. dr. M.F. von Meyenfeldt
Prof. dr. W.M. Molenaar
Voor opa Hans
Paranimfen Drs. D.J. Klees
Drs. R.P. Winkel
Contents
Chapter 1 General introduction and aim of the thesis 9
Chapter 2 Hyperthermic isolated limb perfusion with cisplatin in the localtreatment of spontaneous canine osteosarcoma:Assessment of short term effectsJournal of Surgical Oncology 1995; 59: 169-176. 29
Chapter 3 Hyperthermic isolated limb perfusion with TNF and cisplatinin the treatment of osteosarcoma of the extremities:A feasibility study in healthy dogsSarcoma 1999; 3: 89-94. 45
Chapter 4 Hyperthermic isolated limb perfusion with cisplatin in fourpatients with sarcomas of soft tissue and boneEuropean Journal of Surgical Oncology 1996; 22: 528-531 57
Chapter 5 Isolated limb perfusion of an irradiated foot with TNF,interferon and melphalanArchives of Surgery 1996; 131: 672-674. 67
Chapter 6 FDG-PET to evaluate response to hyperthermic isolated limbperfusion for locally advanced soft-tissue sarcomaJournal of Nuclear Medicine 1996; 37: 984-990. 77
Chapter 7 [1-11C]-Tyrosine PET to evaluate response to hyperthermicisolated limb perfusion for locally advanced soft-tissuesarcoma & skin cancerJournal of Nuclear Medicine 1999; 40: 262-267. 93
Chapter 8 Value of Continuous Leakage Monitoring with RadioactiveIodine-131 Labeled Human Serum Albumin DuringHyperthermic Isolated Limb Perfusion with TNFand MelphalanAnnals of Surgical Oncology 2002; 9: 355-363. 107
Chapter 9 Summary and conclusionsSamenvatting en conclusies 125
Dankwoord 140
Curriculum vitae 142
Publications 143
9
General introduction and aim of the thesis
10
Chapter 1
Before Tumor Necrosis Factor
The first report of the beneficial effect of intravenously administered nitrogen-mustard
on tumor growth appeared just after the second world war.1 Soon afterwards reports
were published on the advantageous effect of intra-arterially administered nitrogen-
mustard on malignant tumors.2-4 Using technology to support extracorporeal
circulation developed for cardiac surgery in the 1950s, the surgical oncologists Creech,
Krementz, Ryan and Winblad of the Tulane University in New Orleans developed
the technique of isolated limb perfusion (ILP).5 In this procedure the blood circulation
of a tumor bearing limb is isolated from the circulation of the rest of the body by
clamping the major artery and vein and tightening a tourniquet around the root of the
limb. The major artery and vein are subsequently connected to a heart-lung machine
and the cytotoxic drug is administered through this isolated circuit. Key point in ILP
is that the dose of chemotherapeutics used, can be 15-20 fold the maximum systemic
tolerated dose, since vital organs are isolated from the perfusion circuit.6-8
The original patient population treated with ILP was a subgroup of melanoma patients
who had extensive local recurrence in the arm or leg. The initial drug used for ILP to
treat extremity melanoma was melphalan (L-phenylalanine mustard). Melphalan is
an alkylating agent of the bischloroethylamine type comprising nitrogen mustard
and phenylalanine. Phenylanaline is a metabolite of melanin and therefore melphalan
specifically targets melanocytes and melanoma cells. Its cytotoxicity appears to be
related to the extent of its interstrand cross-linking with DNA. Like other bifunctional
alkylating agents, it is effective against both resting and rapidly dividing tumor cells.
In 1959 Creech, Krementz and Ryan described their initial results of patients treated
with regional perfusion. The first patient was a 76 year old male with multiple
melanoma satellites on his upper leg. After regional perfusion with melphalan the
satellites disappeared completely and the patient died at the age of 92 with no local
recurrence. The case history of this patient was frequently illustrated at lectures and
a poster with pictures of this patient decorated the entrance of the surgical ward of
the Tulane University for many years. Cavaliere and co-workers investigated the
addition of hyperthermia in the treatment of cancer and, as this appeared to augment
the anti-tumor effects of melphalan, in doing so they laid the basis for hyperthermic
isolated limp perfusion (HILP).9 At temperatures of 41.5 degrees C and higher a
direct anti-tumor effect was observed however, this was accompanied with
unacceptable local toxicity.10 To avert this increased local toxicity it was established
that mild hyperthermia with temperatures of 39 to 40 degrees C was best used.
Wieberdink introduced the optimal dose calculations of melphalan based on limb
volume instead of patient weight, since the latter may lead to under- or overtreatment
of an individual dependent on body habitus.11 An essential component of HILP is
11
Introduction
monitoring the perfusion leakage to the systemic circulation and being able to make
adjustments during treatment to reduce this leakage. Different methods to measure
leakage are used. Stehlin and associates were the first to describe a method of
continuous external leakage monitoring with radioactive Iodine-131 labeled human
serum albumin (RISA).12 This is still the method most frequently used nowadays. It
places a gamma counter over the precordium with RISA in the perfusion circuit,
which allows continuous readings and estimations of the leak of the perfusion solution
into the systemic circulation.13
From 1969 until recently, ILP with hyperthermia and melphalan was the gold standard
for regional treatment of in-transit melanoma. The response rates to this therapeutic
HILP are considerably higher to any other systemic therapy for this type of tumor.
Objective response rates have been reported as high as 70% to 100%, with complete
response rates between 54% and 65%. The median duration of responses is
approximately 9 months, and some patients experience a long-term disease control
with this regional therapy.14,15
Many publications on HILP for melanoma combine adjuvant perfusions with
therapeutic perfusions, often with different treatment schedules, making the
interpretation of available data very difficult. A publication on the 35-year experience
with HILP of the Tulane Hospital serves as a good example for this problem. Over
1100 cases were reported with a median follow-up longer than 10 years. However,
an evidence based conclusion about the benefit of the procedure could not be made.16
A prospective randomized German study published in the 1980s reported a significant
improvement in survival after adjuvant HILP.17 However, the numbers of patients
treated were small, and the outcome in the control group was much worse than
expected compared to historical controls, which meant that this trial could not be
used in arguing for adjuvant HILP.18 The value of HILP as an adjuvant treatment
modality in patients with high risk stage I disease (more than 1.5 mm Breslow
thickness), was recently evaluated in a prospective randomized trial by the European
Organization for Research on Treatment of Cancer (EORTC).19 This study showed
no overall survival benefit for patients treated with HILP with melphalan followed
by local excision compared to patients that had undergone local excision only.
However, a slight benefit in disease free survival was seen in the perfusion group.
With the publication of this study as a negative trial, no adjuvant HILP should be
performed after resection of primary melanoma. Another patient population that may
benefit from a adjuvant HILP are those who have developed in-transit metastases
that have been excisionally biopsied. These patients are at a much greater risk for
additional recurrences in the limb than patients with high-risk primary cutaneous
melanoma who have not had a regional recurrence. A small prospective study from
12
Chapter 1
Sweden found a significant improvement in tumor free survival in the perfusion
group, however no overall survival benefit was demonstrated.20 In conclusion, adjuvant
HILP with melphalan should not be used for high-risk primary melanoma and should
only be used as an adjuvant in the setting of a clinical trial with patients with in-
transit metastases.
Other chemotherapeutic agents used in HILP for melanoma have shown much lower
subjective response rates often with a higher toxicity. Cisplatin as one of the most
successful alternatives with a 50% to 60% response rate showed a high frequency of
peripheral neuropathy.21-23 The most successful systemic treatment agent for melanoma
is DTIC but used in regional perfusion this agent leads to a complete response rate of
11% and a partial response of only 26%.24
Although HILP was most frequently used in the treatment of extremity melanoma,
the procedure was also applied to soft tissue sarcomas (STS) of the extremity.
Krementz described their initial results in 113 patients. Fifty-four patients treated
with HILP without surgical excision of the tumor showed an early response rate of
83%, however only four patients had a complete regression of the tumor.25 Several
studies were published on the treatment of STS with HILP and melphalan, these
studies also have the problem of being heterogeneous as to the type of STS, disease
stage and therapy performed, making comparison difficult. The local recurrence rates
range from 0% to 25% with a 5-year survival rate of 56% to 69%.26-31 Other perfusion
agents have been investigated in the treatment of STS with HILP. Klaase et al.
described the use of doxorubicin as the sole perfusion agent but this was ineffective.
The complete remissions observed in four patients occurred after perfusion with
doxorubicin combined with melphalan. Local toxicity was high, and tissue necrosis
necessitated amputation in three cases.32 However in a study of Rossi et al, tumor
necrosis was more than 50% in 17 patients (74%) and limb-sparing surgery was
feasible in 20 patients (91%). They concluded that HILP with doxorubicin is an
active and well-tolerated procedure within a multidisciplinary approach of the
treatment of limb sarcomas.33 Pommier and Di Filippo investigated cisplatin as a
perfusion agent in the treatment of STS. 34,35 Seventeen patients whose sarcomas
were measured prior to HILP, none of the patients showed a complete response,
three had a partial response (18%), five had a minimal response (29%), seven had no
change (41%), and two had progression (12%).34 In conclusion, results with HILP
for STS were not impressive and alternative strategies for limb preservation by intra-
venous and intra-arterial adriamycin with preoperative or postoperative radiation
therapy followed by compartmental excisions, were able to provide adequate local
control for most extremity STS.36-39
13
Introduction
Introducing Tumor Necrosis Factor
William Coley, a surgeon who lived and worked in New York City during the second
half of the 19th century, was the first to investigate the phenomenon of tumor necrosis,
occurring in patients suffering from severe infections. By administering preparations
of gram-positive and gram-negative bacteria or their products to patients with
inoperable neoplastic diseases, Coley hoped to bring about an involution of the tumor.
The side effects of Coley’s regimen were unacceptable, however, and his treatment
ultimately fell into disrepute.40,41 Shear and co-workers, seeking to isolate an active
therapeutic fraction from Coley’s toxins, purified what they called the “bacterial
polysaccharide” from Serratia marcescens organisms.42-44 This molecule, now known
as lipopolysaccharide (LPS), was shown to induce hemorrhagic necrosis of
transplantable tumors in mice.45 A major conceptual advance occurred with the work
of O’Malley, et al., who reported that an endogenous factor appeared in the serum of
animals treated with LPS, which could induce hemorrhagic necrosis of tumors grown
in animals that had not been exposed to LPS. This information, though published in
a prominent journal, was largely overlooked for over 20 years.46 The transferability
of tumor-necrotizing activity from one animal to another was then identified by Old
and co-workers, who showed that a factor produced in mice pretreated with Bacillus
Calmette-Guérin (BCG) and subsequently challenged with LPS was capable of
causing hemorrhagic necrosis of the meth A sarcoma, grown in the skin of a recipient
animal.47 The factor was dubbed “tumor necrosis factor” (TNF). A large number of
studies reveal that TNF is produced principally by macrophages.48-51 A long period of
time elapsed between the identification of TNF and its isolation in pure form. TNF
from a human source was first isolated by Aggarwal and colleagues at Genentec.52
The molecular cloning of the TNF DNA was accomplished almost simultaneously
by a number of workers at separate biotechnology firms and the cloning of the human
TNF locus followed soon afterwards.53-56
A lot of articles published both in scientific literature and in popular press claimed,
that this molecule would prove to be a revolutionary tool in the battle against cancer.
However, phase I and II clinical trials of systemic TNF were very disappointing. An
overall response rate of 1-2% was seen in almost 1000 patients treated with systemic
TNF.57-60 The dose-limiting toxicity of TNF was typical hypotension, clearly
delineating the central role of this cytokine as a mediator of the pathophysiology of
septic shock.61-64 This dose-limiting toxicity in patients kept the peak intravascular
level achievable in humans 100-fold lower than the level needed for an anti-tumor
effect in a mouse model.65,66
Because it seemed impossible to achieve effective systemic concentrations of TNF
in patients, and because it appeared to act very rapidly with a short, single treatment
14
Chapter 1
in animal models, TNF was ideally suited for use in HILP. Ferdy Lejeune and Danielle
Lienard, surgical oncologists working in Brussels at the time, were the first to link
high-dose TNF and HILP to treat 19 patients with cutaneous melanoma and 4 patients
with STS in the early 1990s.67 In this setting, the equivalent intravascular levels that
led to responses in mice (1-3 µg/ml) could be achieved in the perfusion circuit.68 In a
pilot study of 3 patients with TNF as the sole perfusion agent, one complete response
of 7 months, one partial response of 21 days, and one minor response lasting for
1 month were observed. Posner described these 3 patients and another 3, treated with
HILP and TNF as the sole perfusion agent. One patient had a complete response,
2 patients had a partial response of less than 1 month’s duration and no response was
seen in 3 patients. HILP with TNF as the sole perfusion agent showed inadequate
activity. Three of these 6 patients had been reperfused with TNF and melphalan
resulting in 2 complete responses and 1 partial response.69 In vitro and vivo studies
had already shown an enhanced cytotoxic activity of TNF when chemotherapeutic
drugs, especially alkylating agents were added.70,71 The treatment regimen conceived
by Lejeune was a combination of preoperative subcutaneous interferon-gamma (IFN)
and perfusion with low-dose IFN, high-dose TNF and melphalan for a 90-minute
treatment period. The IFN was added to the regimen because it synergized with TNF
in pre-clinical studies.72,73 In all 23 cases, an early and spectacular softening of the
tumors was seen within the first 3 days after treatment, consistent with the TNF
effect seen in the murine models. Sixteen of 19 patients with melanoma (84%) and 3
out of 4 patients with a STS (75%) showed a complete response. Three melanoma
(16%) and 1 STS (25%) showed a partial response.67,74
Based on the initial study, two prospective randomized trials were initiated. In Europe,
Lejeune and colleagues started a prospective randomized phase II study of patients
with advanced melanoma of the limbs with in-transit metastasis. They compared 32
patients who received melphalan plus TNF and IFN to 32 patients who received
melphalan plus TNF only. The overall response rate and the complete response rate
were higher for the patients treated with IFN compared to the ones treated with
melphalan TNF only, 100% vs. 91% and 78% vs. 69% respectively, but the differences
were not significant.75 In the United States a trial comparing melphalan alone to the
identical dose of melphalan combined with TNF and IFN was initiated by Fraker in
patients with in-transit melanoma of the extremity with no known disease outside
the extremity. At an interim analysis of this study the complete response rate for
melphalan, TNF and IFN perfusion arm was 80% and 61% for the melphalan alone
perfusion arm. In a subgroup of patients with a high tumor burden of the extremity,
the melphalan, TNF and IFN perfusion arm had a much more dramatic effect (67%
complete responses) than what could be achieved by melphalan alone (17% complete
15
Introduction
responses). Patients with low tumor burden or small tumors showed equivalent results
with both of these two perfusion regimens, 87% complete responses with TNF versus
81% with melphalan only.76 The complete response rate seen with melphalan alone
in this study is somewhat better than that reported by other investigators and in order
to draw conclusions about the value of TNF as an adjunct to HILP in melanoma
patients, more patients need to be included.
When the benefit of TNF with melphalan in HILP for bulky melanoma was observed,
the same regimen was applied to STS.67 The results were much more positive in this
combination compared to melphalan alone, and several series have been published
demonstrating limb preservation in patients deemed to have unresectable tumors
with amputation as the only surgical option.77-79 The overall approach with large
extremity sarcomas that have no local resection options because of their relationship
to neurovascular and bony structures, is to conduct HILP with TNF and melphalan.
This treatment results in significant tumor shrinkage in 6 to 12 weeks. A second
procedure is performed after this period to resect the remaining tumor that is often
reduced in size. Patients with multifocal sarcoma do not undergo the secondary
resection, similar to those patients suffering from in-transit melanoma. The European
trial of 186 patients showed complete responses in 18% and partial responses in 57%
of the cases measuring tumor size.77 HILP with TNF and melphalan was also feasible
in patients with locally advanced extremity STS with disseminated disease as local
control improved the quality of life.80 These studies on bulky extremity sarcomas
demonstrated that TNF acts by attacking the tumor vasculature with rapid elimination
of tumor blood flow within days after treatment.81 Other more unusual tumors of the
extremity such as Merkel cell carcinoma, which often spreads by in-transit metastases
within the limb, as well as eccrine adenocarcinoma and basal and squamous cell skin
carcinoma have been reported to respond to HILP with melphalan plus TNF.82 Again,
because this treatment acts via an apparent antiangiogenic mechanism, it may be
applicable against all solid malignancies, with the tumor endothelium as the target
tissue, which is similar across several histologies.
Toxicity of HILP
Toxicity of HILP can be categorized as a side effect from systemic exposure to the
drugs and as a side effect due to the regional effects of high-dose exposure. The
systemic exposure depends not only on the adequacy of the isolation during HILP,
but is also caused by systemic exposure to the perfused drug during reperfusion.
Although the limb is flushed after perfusion, residual active agents still remain in the
limb either within the intravascular space or in the interstitial fluid, which results in
a systemic peak of drug concentration following the re-establishment of normal
16
Chapter 1
vascular flow to the extremity. Systemic leakage of melphalan has been described
and consisted of nausea and vomiting (22%), bone marrow depression in 4% and
miscellaneous systemic side-effects, including fever and minimal scalp hair loss,
occurring in 19 patients (5%).83 With the introduction of high-dose TNF at levels 10
times the maximum tolerated systemic intravenous bolus, isolation was all the more
important, but it introduced also another path to systemic toxicity namely the induction
of secondary host mediators during HILP that are subsequently released into the
systemic circulation after the perfusion. For standard chemotherapeutics, there is
little or no induction of host mediators.84 The systemic effects of TNF HILP reflect
the reported toxicity present in phase 1 systemic TNF trials. The most serious
complication is hypotension. In the first report by Lienard, 23% (7/31) of the patients
treated experienced hypotension, and 10% (3/31) showed severe hypotension.74 All
patients in this initial trial received dopamine (3 mg/kg/min) at the time of TNF
injection into the perfusate as a prophylaxis against hypotension. The most significant
toxicity of TNF limb perfusions can be summarized as a so called Systemic
Inflammatory Response Syndrome (SIRS). This was observed in all patients and
was accompanied by fever, rise in cardiac output, fall in systemic vascular resistance
and the need for fluid resuscitation and inotropes. Perfusion with melphalan as the
sole perfusion agent did not trigger these effects. Detailed analysis showed positive
correlations between maximum TNF concentrations and systemic vascular resistance
and cardiac index.85 The National Cancer Institute perfusion group demonstrated the
relation between the vascular response and the need for vasopressor support and
systemic TNF levels in patients with TNF leakage as well.86 Lejeune also demonstrated
severe toxicity in patients with leaks of >5%.67,68 Vrouwenraets et al. reported an
absence of severe systemic toxicity of TNF in patients without systemic leakage.87
Stam et al. observed only a mild postoperative toxicity in the event of significant
leakage during perfusion.88 This was easily managed on the ICU with fluid substitution
and, in some cases, with vasopressors. All these systemical side effects of TNF HILP
were minimal, transient, and could easily be managed with appropriate resuscitative
techniques.89,90
The normal tissues in the limb that are perfused such as skin, muscle, peripheral
nerves, blood vessels, bone, cartilage, and synovium comprising the skeletal system,
are also exposed to the same concentrations of anti-neoplastic agents active against
the tumor. Wieberdink developed a grading system to score these regional toxicities.11
The toxicities seen with melphalan are skin erythema, some with areas of blistering
and subcutaneous edema, in virtually all patients.91,92 The skin changes as well as this
edema universally returns to normal after several months. The most important
toxicities are the effects on muscle and peripheral nerves. Myopathy can occur with
17
Introduction
mild muscle discomfort and in the worst case may cause a compartment syndrome
with potential muscle necrosis and subsequent limb loss. This is the main reason
why a prophylactic fasciotomy is performed after HILP at the University Hospital in
Groningen.93 Long term analysis of limb function after fasciotomy showed no impaired
function of the perfused limb compared to the contralateral none perfused limb. 94This
was in contrast with other reports claiming approximately 5% to 10% of the patients
have significant long-term discomfort in their extremity after HILP, a difference that
can be possibly explained by the prophylactic fasciotomy. Initial reports from Lienard
et al. indicate that TNF and IFN add little to the regional toxicity of limb perfusions
compared to melphalan alone. Skin erythema and desquamation, edema, joint stiffness,
and peripheral neuropathy appear to occur in the same number of patients as after
melphalan alone perfusions.
Positron Emission Tomography
Positron Emission Tomography (PET) is a non invasive, diagnostic imaging technique
for measuring the metabolic activity of cells in the human body with the aid of short-
lived positron emitting radiopharmaceuticals. Traditional diagnostic techniques, such
as x-rays, CT scans or MRI, produce images of the body’s anatomy or structure.
The first step in a PET-study is to label a selected compound with a positron emitting
radionuclide. Starting from non-radioactive atoms, a cyclotron is used to produce
radionuclides. In a cyclotron, particles such as protons or deuterons (hydrogen and
deuterium atoms without their orbital electrons) are brought to high energies by
traversing several hundred orbits within the cyclotron. When the protons or deuterons
orbits near the maximum radius of the cyclotron, they are removed through
electrostatic or magnetic deflection and are impinged upon small volume hollow
metallic cylinders filled with a nonradioactive gas or liquid. Nuclear reactions take
place within the cylinder (target) between the high energy particle (proton or deuteron)
and the contents of the target. With different target materials, different radioactive
products can be obtained. These are then separated from the target material and can
be used in the synthesis of more complex radiopharmaceuticals. The most frequently
applied radionuclides in PET are carbon-11 (11C, half-life 20 minutes), nitrogen-13
The production of the radiopharmaceutical is performed with the use of automated
synthesis systems. These are located within lead-walled (5-6 cm thick) cabinets so
called “hot cells”. The precise composition of the radiopharmaceutical is assured by
testing the products with e.g. high pressure liquid chromatography before
administrating them to the patient. Sterility and pyrogen testing are performed on
18
Chapter 1
every dose afterwards.
The radionuclides now incorporated within the radiopharmaceutical, have a surplus
of positive nuclear particles. Because this is an unstable situation, these radionuclides
either capture an electron or emit a positron (which is a particle with the same weight
as an electron, but with a positive charge) to achieve stability, depending on the
energy of the nucleus. After a positron is emitted, it is rapidly slowed down by
interactions within the surrounding tissue until all its kinetic energy (velocity) is
lost. At this point, the positron combines momentarily with an electron. The
combination of particles (positron and electron) then totally annihilates or disintegrates
and results in two diametrically (1800 apart) photons of exactly 511 keV energy. The
pairs of photons are emitted equally from the body in all directions. In general, several
million events (photon pairs) are accumulated for each PET image.
The next step in PET is to detect the emitted photons with the PET camera. The PET
camera used for this study at the University of Groningen contains 8192 crystals
oriented into 16 rings arranged in two rings of 64 detector blocks each 512 detectors
per ring. The 16 rings are used to collect 16 planes (slices) of data and an additional
15 cross-planes (slices) are obtained by collecting photon interactions between
adjacent direct planes for a total of 31 planes. The scanner has a 10.4 cm axial field
of view. Patients are positioned comfortably on a table which moves through the
opening of the scanner. Some patients require only one field of view (10 cm) to
visualize a particular area of the body while others are moved through the scanner
using 9-10 bed positions (90-100 cm) to complete whole body imaging. PET cameras
make use of the fact that the two annihilation quanta have opposite directions. Emitted
photons can be absorbed by the detectors in the camera. Each detector has connections
with many opposite detectors. A signal is said to be caused by annihilation if the
capture of a photon by two opposite detectors coincides within 20 nsec. Simultaneous
detection of two of these photons by detectors on opposite sides of an object places
the site of the annihilation or on about a line connecting the centers of the two detectors.
At this point mapping the distribution of annihilations in the field of view by a
computer is possible and an image can be reconstructed. If the annihilation originates
outside the volume between the two detectors, only one of the photons can be detected,
and since the detection of a single photon does not satisfy the coincidence condition,
the event is rejected. The image achieved is generally presented as a gray scale image
of a cross-section of the patient, with the intensity of each picture element proportional
to the isotope concentration at that point in the patient.
Fluorine-18 labeled 2-fluoro-2-deoxy-D-glucose (FDG) is one of the most widely
used radiopharmaceuticals used in PET and has proven to be of value in the
visualization of various types of tumors.95,96 The use of FDG is based on Warburg´s
19
Introduction
observation of increased glycolysis in cancer cells. The citric acid cycle, which is
more efficient in adenosine triphosphate generation, is suppressed.97 As a result, cancer
cells accumulate the glucose analog FDG which is trapped intracellularly as FDG
phosphate. The FDG consumption, and since FDG acts in the same way as glucose,
the glucose consumption can be determined with the use of a three-compartment
model: plasma-FDG, tissue-FDG and tissue-FDG-6-phosphate, as described by
Sokoloff.98 The tissue components can be measured by the PET camera and the plasma
components can be measured by counting the activity in blood samples. With the
compartment model, the glucose consumption can be calculated in µmol per 100
grams of tissue per minute.
The majority of the PET studies with amino acid tracers have been performed with
L-[methyl-11C]-methionine (MET). 99-101 MET reflects amino acid uptake rather than
protein synthesis and because it is involved in other metabolic pathways such as
transmethylation and polyamine synthesis, this may lead to accumulation of a variety
of nonprotein metabolites in tumor tissue.102-104 This complicated metabolism of
methionine has made it impossible to create a precise metabolic model. Carboxyl-
labeled amino acids, such as L-[1-11C]-tyrosine (TYR), L-[1-11C]-methionine and L-
[1-11C]-leucine, appear to be more appropriate compounds to determine protein
synthesis in tumors.103,105 The main metabolite of these amino acids is 11CO2, which
is rapidly cleared from tissue and exhaled and does not contribute to the PET-measured11C radioactivity in tumor tissue. Using a method developed at the PET Center
Groningen, the protein synthesis rate can be determined using 11C labeled L-amino
acids with a four-compartment model: plasma-amino-acid, tissue-nonprotein-amino-
acid, metabolites and protein-incorporated-amino-acid.106
The aim of this thesis
Hyperthermic isolated limb perfusion is a major surgical procedure and over the
years new developments have been initiated and examined. Traditionally the
University Hospital Groningen plays an important role in the history of regional
perfusion and therefore this thesis describes different aspects of regional perfusion
during the last decade.
1. What are the short term effects of HILP with cisplatin in the local
treatment of spontaneous osteosarcoma in dogs?
2. Is HILP with TNF and cisplatin feasible in the canine model?
3. What are the results of HILP with cisplatin in patients with sarcomas of
soft tissue and bone?
20
Chapter 1
4. What is the relation between the tumor vascularization and the vascular
changes after irradiation therapy?
5. How does HILP influence the glucose metabolism and protein metabolism
as studied by PET, and is it possible to predict the outcome of therapy?
6. Is it worthwhile to monitor continuous leakage with RISA during HILP
with TNF and melphalan?
21
Introduction
References
1 Gilman A, Philips F.S. The biological actions and therapeutic applications of the β-
chlorethyl amines and sulfides. Science 1946; 103: 409-415.
2 Bierman H.R., Kelly K.H., Byron R.L., Dod K.S., Shimkin M.B. Studies on the
blood supply of tumors in men. Intra-arterial Nitrogen Mustard therapy of cutaneous
lesions. J Nat Cancer Inst 1951; 11: 891-897.
3 Klopp CT. Regional intra-arterial nitrogen mustard as an adjunct to radiation therapy.
Department of Surgical Oncology1 and Central Animal Laboratory2, University
Hospital Groningen, The Netherlands.
Sarcoma 1999; 3: 89-94.
Hyperthermic isolated limb perfusion with TNF and
cisplatin in the treatment of osteosarcoma of the
extremities: A feasibility study in healthy dogs
46
Chapter 3
Abstract
The feasibility of hyperthermic isolated limb perfusion (HILP) with tumor necrosis
factor-α (TNF) and cisplatin for the management of osteosarcoma was studied in the
canine model. During seven perfusions in six healthy mongrel dogs (weight 32±2 kg)
the technical aspects of HILP under mild hyperthermia (39-40o) were studied. In five
experiments HILP was performed with TNF alone (0.5 mg/L extremity volume), and
in two experiments TNF was combined with cisplatin (25 mg/L extremity volume).
During the perfusions physiological parameters were monitored and TNF and total
cisplatin concentrations were determined. Perfusion conditions (pH, PCO2, PO
2, flow
and pressure) remained within physiological ranges. Three dogs died within 24 hours
despite a sublethal systemical concentration of TNF that leaked from the perfusion
circuit. Three dogs were terminated; one dog after the second experiment in accor-
dance with Dutch ethical rules; one dog because it showed an invagination of the
small bowel resulting in an ileus; one dog because of necrosis of the perfused limb.
This feasibility study in healthy dogs demonstrated that HILP with TNF and cisplatin
was associated with a high mortality rate and therefore does not allow us to treat
dogs with spontaneous osteosarcoma with TNF and cisplatin HILP. Therefore, an
alternative model should be used in the search for the ideal combination of perfusion
agents for the limb sparing treatment in human osteosarcoma.
Introduction
Osteosarcoma is the most frequent primary malignant bone tumor in humans. Until
the 1970s the most common approach to the management of localized osteosarcoma
was surgical resection, amputation or radiation therapy.1 During the last decades a
definite role for neoadjuvant high dose methotrexate and cisplatin based
polychemotherapy was established.1-4 The potential local tumor effect of systemically
administered cisplatin, however, is limited due to the nephrotoxicity and ototoxicity
of cisplatin. Therefore an attempt was made to increase the local effect of cisplatin
without increasing systemic toxicity by using hyperthermic isolated regional limb
perfusion (HILP) with cisplatin in dogs with spontaneous osteosarcoma.5 These
studies showed an acceptable locoregional toxicity, improved functional outcome at
6 and 12 weeks, and a steadily improving radiological picture. However, the
histological results were modest, with none of the dogs showing a complete response
at 6 weeks after perfusion. The same experience was found in patients with sarcomas
of soft tissue and bone treated with cisplatin HILP.6 Results of recent publications
and of our own experience with a new perfusion modality, which combines tumor
necrosis factor-α (TNF) and melphalan in patients with recurrent melanoma or soft
tissue sarcoma, are very promising.7,8 However, in 6 of 8 evaluable patients with
47
Limb perfusion with TNF and cisplatin in healthy dogs
unresectable osteosarcoma of the lower limb treated with TNF and melphalan HILP,
histological evaluation revealed moderate results with ≥ 80% necrosis in 3 patients,
50%-60% necrosis in 2 patients and < 50% necrosis in one patient. After TNF and
melphalan HILP, limb sparing surgery was possible in 6 patients.9 As cisplatin is one
of the most active chemotherapeutics in the treatment of osteosarcoma, it seems
worthwhile to investigate the results of HILP with TNF and cisplatin. With the high
frequency of occurrence in dogs, canine osteosarcoma is a useful model for evaluation
of new treatment regimens in humans as rapid case accrual and rapid time to reach
measurable end points are possible.10 The canine osteosarcoma therefore appears to
be a valid model for studying the potential treatment of HILP with TNF and cisplatin
in the local treatment of osteosarcoma of the extremity in humans. To establish optimal
HILP conditions using TNF and cisplatin for local tumor control in dogs bearing
osteosarcoma, a feasibility study in healthy dogs was undertaken.
Materials and methods
Dogs
During 7 experiments in 6 healthy mongrel dogs with a mean average weight of 32 ±2 kg and a mean age of 6 ± 1 years different aspects of HILP with TNF and cisplatin
were studied. Preoperatively, all dogs were thoroughly clinically evaluated at the
Central Animal Facility of the University of Groningen. The study was approved by
the Animal Welfare Committee of the Faculty of Medicine of the Groningen
University.
Anesthetics
The dogs fastened for 12 hours and were anaesthetized with thiopental (30mg/kg
BW, i.v.)(Pentothal, Abbott, Amstelveen, The Netherlands) and after muscle relaxation
with pancuroniumbromide (0.08 mg/kg BW, i.v.) (Pavulon, Organon, Oss, The
Netherlands), the dogs were ventilated (Ohmeda Modulus 2) with a mixture of O2
and isoflurane. The oxygen concentration in the gas mixture was continuously
measured by means of an oxygen analyzer (Ohmeda Modulus 2) and minute volumes
( 4-6 L/min) were adjusted to maintain an end-expiratory CO2 concentration of 4-5%
(Siemens CO2 - analyzer 930). The dogs were placed in the supine position on a
heated mattress to maintain their normal body temperature of 38 0C.11 During the
operations all dogs were given about 2 L of glucose 5% through a cephalic or internal
jugular vein. Central arterial pressure was recorded as well as an ECG and diuresis.
48
Chapter 3
Operation and Perfusion Techniques
During anaesthesia the volume of the extremity was measured using Archimedes
rule (1.7-2 L). The iliac vessels were exposed under sterile conditions and collateral
vessels were clipped. Cannulas were inserted into the artery (Bardic, 14-18 F) and
vein ( Bardic, 14-18 F). Both cannulas were connected to an extracorporeal circuit
consisting of an occlusive roller pump, a cardiotomy reservoir and a bubble oxygenator
with heat-exchanger. A nylon tourniquet was placed around the base of the extremity
using, a pin in the bone and bandage around the middle to complete the isolation of
the limb from the systemic circulation. The perfusate consisted of 350 ml 5% dextran
40 in glucose 5% (Isodex, Pharmacia AB, Uppsala, Sweden), 250 ml red blood cells
(canine blood donors), 250 ml plasma, 30 ml sodiumbicarbonate 8.4% and 0.5 ml
5000 IU/ml heparin (Thromboliquine, Organon B.V., Oss, The Netherlands). The
mixture of oxygen, air and carbondioxide through the oxygenator was adjusted to
maintain the blood gas values within the physiological range and when necessary,
bicarbonate was added to adjust the pH value.
All perfusions were performed under mild hyperthermic conditions (39-400 C) and
recombinant interferon gamma (IFN) and melphalan in 23 patients with locally
advanced melanomas and soft tissue sarcomas of the extremities.1 The effect on the
tumors was striking: 19 (83%) complete responses and four (17%) partial responses
after a single perfusion with the triple-drug regimen. Local toxicity in the perfused
limb was minimal, 88% grade II and 12% grade III classified according to
Wieberdink.2 These figures are comparable with local tissue toxicity in patients treated
with melphalan as the single perfusion agent. The preliminary results of this study
suggested that high-dose TNF can be administrated safely by regional perfusion.
HILP of the limb with this triple drug regimen was started in 1991 at Groningen
University Hospital in the Netherlands, one of several institutions participating in a
multicenter study. The effect of this new combined modality therapy of isolated limb
perfusion and delayed surgery in a patient with a previous history of irradiation of
the foot is described.
Case report
In 1988 a 57-yr old woman presented with a 5 x 6 cm high grade malignant fibrous
histiocytoma on the lateral side of the right foot without distant metastases. She
refused a curative amputation of the lower leg. Therefore a marginal resection was
performed, followed by 60 Gy external beam radiotherapy, 40 Gy (2 Gy per day) on
the whole foot, and a 20 Gy boost on the tumor (Fig. 1). Two years after initial
treatment the tumor recurred locally without evidence of distant metastases. Again
she refused a lower leg amputation. In an attempted to render the tumor resectable,
69
Radiotherapy prior to HILP with TNF
HILP through the popliteal vessels with 100 mg cisplatin (30mg cisplatin per liter
limb volume) was performed. Histologic biopsy specimens of the tumor obtained 1
and 2 weeks after cisplatin perfusion showed no viable tumor cells, and a complete
remission was observed clinically.
In January 1991 the second local recurrence without distant metastases was observed,
again with persistent refusal by the patient for a curative amputation. During six
months the patient withdrew from follow-up but presented in June 1991 with a local
ulcerating tumor measuring 10 x 12 cm, still without metastatic disease (Fig. 2).
Because of the patients persistent refusal to undergo an amputation, a HILP with
TNF, IFN and melphalan was suggested and informed consent was obtained. One
and 2 days before HILP, a dose of 0,2 mg of IFN (Boehringer Ingelheim, Ingelheim,
Germany) was administered subcutaneously. A 90-minute mild hyperthermic (39°C
to 40°C), popliteal perfusion was performed with 0,2 mg of IFN, 4 mg of TNF
Fig. 1 Clinical appearance of the
patients right foot demonstrating the
radiation field and dosages of the ini-
tial treatment
Fig. 2 Clinical appearance of the
patients right foot demonstrating
the second recurrence
70
Chapter 5
(Boehringer Ingelheim), and 45 mg of melphalan (10 mg/L of limb volume)(Burroughs
Welcome, London, England). Leakage to the systemic circulation measured with131I labeled albumin as a tracer was 2.8 %.3 ECG, urine output, blood pressure,
venous and pulmonary pressures were recorded during and after perfusion until the
second postoperative day. A continuous infusion of dopamine at 2.8 mg/kg/min for
18 hours was given. Postoperatively the patient experienced fever and chills but no
hematological, hepatic or renal toxicity was observed.
A few hours after TNF perfusion, the entire right foot appeared bluish up to a definite
line at the ankle; the rest of the leg had a normal circulation. Two days after perfusion,
the tumor was black and necrotic in concordance with the 60-Gy total dose
Fig. 3 The right foot and ankle re-
gion 2 days after hyperthermic iso-
lated limb perfusion with TNF, IFN
and melphalan. The tumor is black
necrotic and the rest of the foot is
blue, sharply delineated at the edge
of the radiation field.
Fig 4 Left, A necrotic tumor tissue specimen after tumor necrosis factor perfusion (hema-
toxylin-eosin, x64) Right, The border area between nonirradiated normal skin (right) and
irradiated skin (left). The irradiated site demonstrates infiltration of both the dermis and the
epidermis with granulocytes and marked stasis with thrombosis of the microcirculation. In
the nonirradiated area, normal vascular structures are seen (hematoxylin-eosin, x64).
71
Radiotherapy prior to HILP with TNF
radiotherapy field, while the rest of the foot (40-Gy field) was blue and showed
some dry shrinkage of the skin (Fig. 3). Because of the severe necrosis, amputation
of the right foot below the knee had to be performed 9 days after TNF perfusion.
Histological findings were consistent with complete necrosis of the tumor (Fig. 4,
left). The amputation wound healed without complications, and the patient is alive
without evidence of disease 3 years after TNF perfusion and subsequent amputation.
Discussion
In 1975, Carswell et al. showed that tumor-necrotizing activity in the sera of animals
given injections of endotoxin was due to a host factor named tumor necrosis factor
(TNF).4 The mechanisms of the anti tumor activity of TNF however, are still not
elucidated and basis of further research. The results of intralesional or intravenous
administration of recombinant human TNF in mice with solid Meth A sarcoma of the
skin were recently described by van de Wiel and Bloksma.5 Treatment with TNF
caused red discoloration and necrosis of the central portion of the tumor within 24
hours. However, incubation of Meth A cells in the presence of TNF in vitro did not
affect their capacity to incorporate tritiated thymidine, indicating resistance of the
Meth A cells to TNF in vitro and supporting the thought that other mechanisms are
responsible for the observed discoloration and necrosis of the tumor in vivo.
Microscopic investigations of the tumors showed hyperemia, congestion, endothelial
damage and hemorrhage in the central part of the tumor, while just outside the tumor
edema and an infiltrate of polymorphonuclear cells was seen. Locally injected normal
skins with TNF showed moderate vascular effects without necrosis. This and other
investigations demonstrated that the vascular endothelial cells in particular are the
main target cells of this TNF induced antitumor effect.6,7 When incubated with TNF,
cultured endothelial monolayers show two phenomena. Stolpen et al. demonstrated
that TNF causes morphological changes of the endothelial cells, they become
elongated, overlap, rearrange their actin filaments and lose their stainable fibronectin
matrix.8 Suppression of anticoagulant mechanisms and the production of the
procoagulant cofactor tissue factor, is the second phenomenon9. These TNF-induced
changes are more prominent in areas with growing and/or migrating endothelial cells,
a situation that occurs within the tumor bed and explaining why the tumor vasculature
is more susceptible for TNF compared with normal vessels.10 A higher expression of
TNF receptors on the endothelial cell surface of dividing and growing endothelial
cells seem to be the cause of this high sensitivity for TNF.10,11 In summary; TNF
exposure emerges an altered endothelial cell phenotype, anticoagulant mechanisms
are suppressed and tissue factor is produced, leading to fibrin accumulation at the
endothelial cell surface 12 and thrombus formation in the tumor vessel, causing
72
Chapter 5
circulatory stasis and ischemia inside the tumor followed by necrosis of the tumor.
Besides this early vascular phenomenon, a latter in time occurring immune effect
with polymorphonuclear cell binding to the activated endothelium,7,13,14 and a direct
cytotoxic effect of TNF demonstrated in vitro against a variety of cell lines 15,16 are
two other mechanisms that could contribute in the anti-tumor effect of TNF.
In our case, not only the vascularization of the tumor was affected by TNF exposure
but also the microvascularization of the area that had been irradiated 3 years earlier.
Microscopical examination of the border area between irradiated and nonirradiated
areas revealed infiltration of both dermis and the epidermis with granulocytes, and
marked stasis with trombosis of the micro circulation of the irradiated area, causing
necrosis. These phenomena were absent from the perfused nonirradiated area (Fig.
4,right).
Late effects of normal tissues after radiotherapy are well known. Hopewell
demonstrated that arteries of the hamsters cheek pouch showed localized constrictions
after irradiation.17 These constrictions were caused by clones of dividing endothelial
cells and might be the predominant factor influencing the degeneration of the capillary
bed after radiotherapy.18 Evidence of this occlusive effect of vessels by proliferating
endothelial cells after radiation have also been reported by other investigators.19 Since
dividing and migrating endothelial cells are more sensitive to TNF than quiescent
endothelial cells, it is likely that not only the dividing and migrating endothelial cells
of the tumor bed but also the endothelial cells in the irradiated area of the foot in this
patient were activated by TNF, causing stasis and thrombosis of the microcirculation
in both areas. Recently Milas and coworkers also demonstrated a synergistic effect
between radiotherapy and TNF.20,21
One and a half year before TNF perfusion, this patient received HILP with cisplatin.
No literature is available describing the acute or long term effect of cisplatin on the
endothelial cells, however treatment with antineoplastic agents is associated with
vascular toxicity.22 With regard to cisplatin Vogelzang et al. described the relation
between hypomagnesemia and an increased risk of Raynaud´s phenomenon after
cisplatin, vinblastine and bleomycin treatment.23 Jackson et al. described a thrombotic
microangiopathic syndrome characterized by renal insufficiency, microangiopathic
hemolytic anemia and thrombocytopenia in patients treated with an identical
regimen.24 Histological examination of renal biopsy specimens showed marked
luminal narrowing of small arteries as a result of thrombus formation and subintimal
thickening. Whether cisplatin is the sole agent responsible for this vascular effect
remains unclear especially since it is known that bleomycin in this combination
chemotherapy has a prominent effect on endothelial cells.25 Analysis of cisplatin
perfusions data, performed at our clinic showed severe neurotoxicity, yet no signs of
73
Radiotherapy prior to HILP with TNF
vascular disturbances were found (i.e. Raynaud´s phenomenon).26 A synergistic effect
between cisplatin and radiotherapy is known when cisplatin is administered shortly
before or after radiotherapy,27 in this patient the interval between radiotherapy and
cisplatin perfusion lasted to long to make synergism likely.
Other radiation-related or radiation-independent factors may also be contributory,
i.e., the radiation dosage, time interval between radiation and TNF perfusion, and
the irradiated anatomical site. To distinguish the contribution of each of these different
factors experimental investigations should be performed. Awaiting the results of such
experiments, we would like to alert surgeons and radiation oncologists to the possible
complications that may occur after TNF perfusion, when the perfused limb has already
and Raynaud’s phenomenon in patients treated with cisplatin, vinblastine, and
bleomycin. Cancer 1985; 56: 2765-2770.
24 Jackson AM, Rose BD, Graff LG, et al. Thrombotic microangiopathy and renal
failure associated with antineoplastic chemotherapy. Ann Intern Med 1984; 101:
41-44.
25 Nicolson GL, Custead SE. Effects of chemotherapeutic drugs on platelet and
metastatic tumor cell-endothelial cell interactions as a model for assessing vascular
endothelial integrity. Cancer Res 1985; 45: 331-336.
26 Hoekstra HJ, Schraffordt Koops H, De Vries EGE, Van Weerden TW, Oldhoff J.
Toxicity of hyperthermic isolated limb perfusion with cisplatin for recurrent
melanoma of the lower extremity after previous perfusion treatment. Cancer 1993;
72: 1224-1229.
27 Vokes EE. Interactions of chemotherapy and radiation. Semin Oncol 1993; 20: 70-
79.
76
77
Robert J. van Ginkel1
Harald J. Hoekstra1
Jan Pruim2
Omgo E. Nieweg1,3
Willemina M. Molenaar4
Anne M.J. Paans2
Anton T.M. Willemsen2
Wim Vaalburg2
Heimen Schraffordt Koops1
Department of Surgical Oncology1, PET Center2 and Department of Pathology4,
University Hospital Groningen, The Netherlands and Department of Surgery3, The
Netherlands Cancer Institute, Amsterdam, The Netherlands.
Journal of Nuclear Medicine 1996; 37: 984-990.
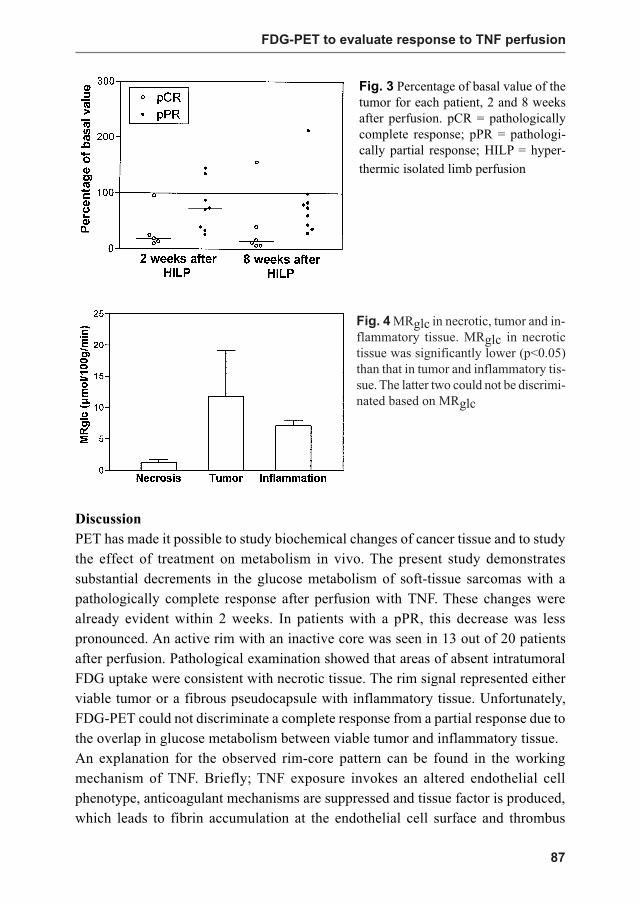
FDG-PET to evaluate response to hyperthermic
isolated limb perfusion for locally advanced soft-
tissue sarcoma
78
Chapter 6
Abstract
We investigated FDG-PET in patients undergoing hyperthermic isolated limb
perfusion (HILP) with TNF, IFN and melphalan for locally advanced soft-tissue
sarcoma of the extremities. Twenty patients (11 women, 9 men; aged 18-80 yrs, mean
age 49 yrs) were studied. FDG-PET studies were performed before, 2 and 8 weeks
after HILP. After the final PET study, the tumor was resected and pathologically
graded. Patients with a pathologically complete response (pCR) showed no viable
tumor after treatment. Those with a pathologically partial response (pPR) showed
various amounts of viable tumor in the resected tumor specimens. Seven patients
showed a pCR (35%) and 12 patients showed a pPR (60%). In one patient,
pathological examination was not performed (5%). The pre-perfusion glucose
consumption in the pCR group was significantly higher than in the pPR group
(p<0.05). Visual analysis of the PET images after perfusion showed a rim of increased
FDG uptake around a core of absent FDG uptake in 12 patients. The rim signal
contained a fibrous pseudocapsule with inflammatory tissue in the pCR group, but
viable tumor tissue was seen in the pPR group. The glucose consumption in the pCR
group at 2 and 8 weeks after perfusion had decreased significantly (p<0.05) compared
with the glucose consumption in the pPR group. Based on the pretreatment glucose
consumption in soft-tissue sarcomas, one could predict the probability of a patient
achieving a complete pathologically response after TNF HILP. FDG-PET indicated
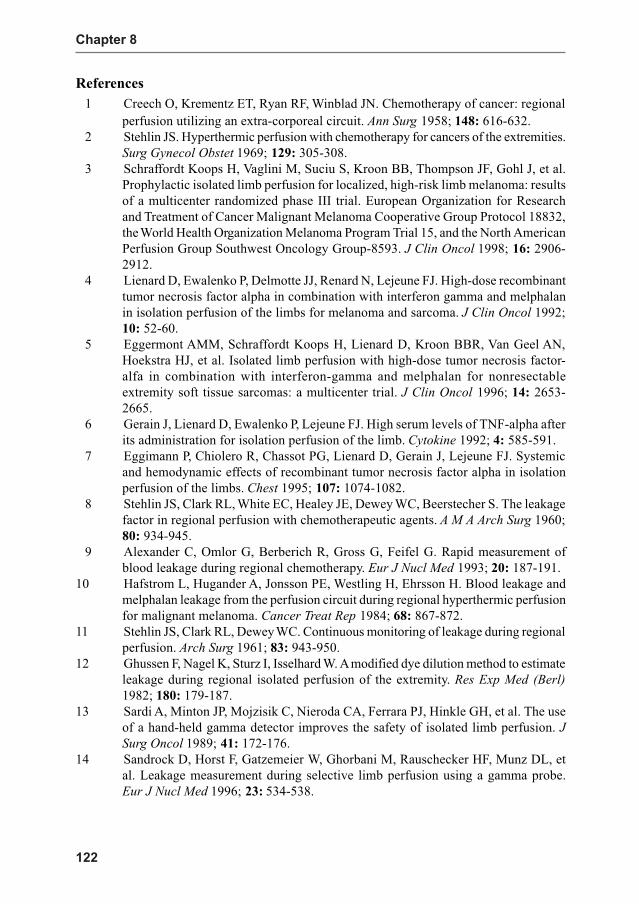
the pathologic tumor response to HILP, although the lack of specificity of FDG, in
terms of differentiation between an inflammatory response and viable tumor tissue,
hampered the discrimination between pCR and pPR.
Introduction
Malignant soft-tissue sarcomas are a heterogeneous group of lesions that all arise
from tissue of mesenchymal origin and are characterized by aggressive local growth
and hematogenic metastases. They account for 1% of all malignant tumors and have
an incidence rate of 2 per 100.000. About 60% of these tumors occur in the extremities
and are often quite large at diagnosis.1 Limb-saving treatment of extremity soft-tissue
sarcomas is a multidisciplinary matter, with surgery and radiotherapy as the usual
treatment protocol.2,3 This combination therapy has avoided ablative surgical
procedures in the majority of patients.
The majority of locally advanced extremity soft-tissue sarcomas are treated by
amputation. Intra-arterial chemotherapy with adriamycin, combined with preoperative
radiotherapy, surgery and postoperative radiotherapy is effective in the treatment of
locally advanced soft-tissue sarcoma, but significant morbidity does occur.4 Recently
Eilber et al. reported a complete response rate of 49% and a limb-saving rate of 98%
79
FDG-PET to evaluate response to TNF perfusion
with neo-adjuvant chemotherapy and radiation for high-grade extremity soft-tissue
sarcoma with low treatment morbidity.5 Hyperthermic isolated limb perfusion (HILP)
also proved to be of value in the treatment for locally advanced extremity soft-tissue
sarcoma.6-8 With HILP, chemotherapeutic tissue concentrations may be up to 20 times
higher than can be attained with systemic administration.9 The introduction of
recombinant tumor necrosis factor-alpha (TNF), interferon-gamma (IFN) and
melphalan in regional perfusion represents a promising new development.10 With
this perfusion regimen, a complete response rate of 55% and a partial response rate
of 40% can be reached in the treatment of locally advanced soft-tissue sarcoma of
the extremities with a limb-saving rate of 90%.11 Since 1991, this perfusion strategy
has been used at our institution for these types of soft-tissue sarcomas.
PET enables visualization and quantification of metabolic processes in vivo. Fluorine-
18-2-fluoro-2-deoxy-D-glucose (FDG) has proven to be of value in the visualization
of various types of tumors.12,13 The use of FDG is based on Warburg´s observation of
increased glycolysis in cancer cells. The citric acid cycle, which is more efficient in
adenosine tri-phosphate generation, is suppressed.14 As a result, cancer cells
accumulate the glucose analog FDG which is trapped intracellularly as FDG
phosphate. FDG-PET can visualize soft-tissue sarcomas, indicate the malignancy
grade and detect locally recurrent disease.15-17 Various clinical reports suggest the
feasibility of FDG-PET to assess tumor response to radiotherapy and chemotherapy.18-20 This particular application of PET as a noninvasive technique to evaluate the
outcome of such often aggravating and expensive therapy may have a significant
effect on patient management. Ineffective treatment could be adjusted or discontinued
in an early stage and effective treatment could be continued with confidence.
The perfusion protocol provides us with histology before and after regional
chemotherapy. The tumor responses to this regional drug treatment are variable. This
clinical setting creates an opportunity to investigate the value of a noninvasive
diagnostic technique in the determination of tumor response to chemotherapy. The
aim of the present study was to investigate FDG-PET in patients undergoing HILP
for locally advanced soft-tissue sarcoma and to correlate PET findings with histology
before and after treatment.
Materials and methods
Patients
Twenty (11 women, 9 men, aged 18-80 yrs, mean age 49 yrs) patients with biopsy-
proven soft-tissue sarcomas were entered in the study. Informed consent was obtained
from each patient. The diagnosis of the tumors was determined in a standard fashion
and graded according to Coindre.21,22 Thirteen patients presented with a newly
80
Chapter 6
diagnosed soft-tissue sarcoma (65%) and seven patients with a local recurrence (35%),
that had been previously treated with surgery alone. Nineteen tumors were located in
the lower limb (95%), and one patient (5%) had a sarcoma located in the right elbow.
All tumors were considered primarily irresectable because of size, their multicentricity
in the limb or fixation to the neurovascular bundle or bone. Median tumor size was
8.5 cm (range 2-30 cm). To render the tumors resectable for limb salvage, patients
were treated with HILP.
Treatment protocol
HILP is based on the technique developed by Creech and Krementz.23 Briefly, after
ligation of all collateral vessels and heparinization of the patient with 3.3 mg heparin/
kg bodyweight (Thromboliquine, Organon BV, Oss, the Netherlands), the axillary,
iliac, femoral or popliteal vessels were cannulated and connected to an extracorporeal
circuit. The perfused limb was wrapped in a thermal blanket to reduce heat loss and
a tourniquet was applied at the root of the extremity to minimize leakage of the
perfusate into the systemic circulation. Perfusion was performed during 90 min under
mild hyperthermia (39-40oC) and physiologically optimal conditions.24 At the start
of perfusion, 3 mg (upper extremity) or 4 mg (lower extremity) TNF (Boehringer,
Ingelheim, Germany) were injected as a bolus into the arterial line. Melphalan
(Burroughs Wellcome, London, England) was administered 30 min later, 10 mg/L
extremity volume (leg) or 13 mg/L extremity volume (arm).25 Since all perfusions
were performed in a Phase II clinical trial, the initial 13 patients in the PET study
also received a dose of 0.2 mg INF (Boehringer, Ingelheim, Germany) subcutaneously
1 and 2 days before perfusion, followed by 0.2 mg INF injected into the arterial line
at the start of perfusion. The final seven patients in the PET study did not receive the
INF. This alteration in treatment schedule was due to the decision of the trial
commission to investigate the additional effect of INF in the perfusion regiment
while the PET study was still in progress.
All perfusions were performed with a bubble oxygenator roller pump and heat
exchanger. The perfusate was oxygenated by a mixture of O2 and CO
2 and consisted
of 350 ml 5% dextran 40 in glucose 5% (Isodex, Pharmacia AB, Uppsala, Sweden),
500 ml blood (250 ml red blood cells, 250 ml plasma), 30 ml 8.4% NaHCO3, 0.5 ml
5000 IU/ml heparin. After 90 min of perfusion, the limb was flushed with 2 liters
dextran 40 in glucose 5% (Isodex, Pharmacia AB, Uppsala, Sweden) and 500 ml
blood (250 ml red blood cells, 250 ml plasma), catheters were removed, the circulation
restored and the heparin antagonized with protamine chloride (Hoffman La Roche,
Mijdrecht, the Netherlands). A lateral fasciotomy of the anterior compartment of the
lower leg or arm was performed to prevent a compartment syndrome.26 Approximately
81
FDG-PET to evaluate response to TNF perfusion
8 weeks after perfusion (median 61 days, range 43-106 days) the residual tumor
masses were excised and pathologically examined.
Pathological examination
The tumor was measured in three dimensions and the percentage of necrosis estimated.
Representative tumor sections were taken, encompassing macroscopically different
tumor areas, including necrosis. Generally, one section per centimeter largest diameter
with a minimum of three was taken. Based on an integration of gross and microscopic
findings, a final estimate of the percentages of viable and necrotic or regressive tumor
was made. If possible, macroscopic examination and tissue sampling were performed
based on the latest PET images. The results were classified as either pathologically
complete response (pCR) or pathologically partial response (pPR), when remaining
viable tumor was observed.
PET imaging
Patients were scheduled for three PET studies: shortly before perfusion (median 14
days, range 1-30 days), two weeks after perfusion (median 13 days, range 7-27 days)
and shortly before resection of residual tumor tissue (median 55 days, range 42-77
days after perfusion). FDG was routinely produced by a robotic system following
the procedure as described by Hamacher27 with a radiochemical purity of more than
98%. PET sessions were performed using a Siemens ECAT 951/31 PET-camera
(Siemens/CTI, Knoxville, USA).
All patients fasted for at least 6 hours before the investigation. Serum glucose levels
were measured before each PET session and were found to be normal. A 20-gauge
needle was inserted into the radial artery under local anesthesia. In the contralateral
arm, an intravenous canula was inserted in the cephalic vein for the injection of the
FDG. The patients were positioned supine in the camera, with the tumor in the field
of view based on physical examination.
After attenuation scanning using 68Ge/68Ga source, 370 MBq (10mCi) FDG were
administered intravenously over 1 min. Dynamic images were acquired from the
time of injection after a dynamic protocol (five 1-min, five 2-min, five 3-min, two 5-
min, two 10-min, for a total duration of 60 min). Simultaneously, 2-ml blood samples
were taken from the arterial canula (time points 0.5, 1, 1.5, 2, 2.5, 3, 3.5, 4, 4.5, 5, 10,
15, 25, 35, 45 and 55 min post-injection). The blood samples were centrifuged and
plasma activity was assessed using a well counter that was cross-calibrated with the
positron camera. Whole-body images were obtained after dynamic scanning. Total
time for the imaging procedure was approximately 2.5 hours.
82
Chapter 6
Data analysis
Images were displayed in coronal, sagittal and transaxial projections on a computer
display applying standard ECAT software (Siemens/CTI, Knoxville, USA) and
interpreted independently by two experienced physicians. Before perfusion, the tumor
location was first defined in all relevant tomographic planes of the study. Each tumor
was outlined automatically with a threshold technique that defines its contours at a
manually chosen percentage of the maximum number of counts per pixel. The level
of the threshold was chosen with the purpose to match the size of the region of
interest with the tumor size as outlined by MRI or CT. For each patient, a fixed
percentage (median 40, range 30-60) was used in all planes. All pixels above the
threshold were used for the calculation. An average time-activity curve as well as the
total volume of the lesion was obtained. Combining the averaged time-activity data
with the plasma input data, the average metabolic rate of glucose consumption
(MRglc) in µmol/100g tumor tissue /min was calculated using Patlak analysis,
assuming a lumped constant of 0.42.28,29 After perfusion, this threshold technique
could not be used since large areas of the tumors became inactive. The MRglc after
perfusion was therefore calculated by placing multiple regions of interest (ROI) over
the original tumor in all relevant planes of the study. Consequently, the necrotic parts
of the tumor that originated after perfusion were incorporated in this calculation.
The MRglc in the active parts of the tumor after perfusion was calculated separately
with the ROI technique. The change in MRglc after perfusion was related to the pre-
perfusional value and expressed as a percentage of basal value.
Visual evaluation of the PET studies was performed by quantifying the degree of
viable (active areas on the PET studies) and necrotic tumor (inactive areas) as a
percentage before and after perfusion.
Statistical analysis
Statistical procedures included a two-factor experiment with repeated measures on
one factor to compare glucose consumption between measures and groups. Analyses
were performed on datasets corrected for missing data according to Winer.30 Posthoc
comparison was made with Student t-tests. A p-value < 0.05 was considered
significant. SPSS/PC+
statistical software was used.
Results
The tumor characteristics, PET results and pathological response for each patient are
summarized in Tables 1 and 2. Pathological examination of the residual tumor mass
showed no viable tumor in seven patients (pCR 35%). In twelve patients, variable
amounts of viable tumor were found (pPR 60%). The pPR group also included one
83
FDG-PET to evaluate response to TNF perfusion
A B C
Ta
ble
1T
um
or ch
aracteristics for each
patien
t.
Pat.
His
tolo
gy
Gra
de
Nu
mb
er L
arg
est
Pe
rfusio
n a
gen
ts
Nr.
of
dia
mete
r
lesio
ns
(MR
I)
1R
ha
bdom
yosarc
om
aP
rimary
31
10 c
mT
NF, IF
N, M
elp
ha
lan
2D
ediffe
rentia
ted m
yxoid
liposarc
om
aP
rimary
31
20 c
mT
NF, IF
N, M
elp
ha
lan
3M
yxo
id lip
osarc
om
aR
ecurre
nt
12
15 c
mT
NF, IF
N, M
elp
hala
n
4P
erip
hera
l neuro
ecto
derm
al tu
mor
Prim
ary
33
8 c
mT
NF, M
elp
hala
n
5M
alig
nant fib
rous h
istio
cyto
ma
Prim
ary
31
5 c
mT
NF, M
elp
hala
n
6M
alig
nant fib
rous h
istio
cyto
ma
Recurre
nt
31
4 c
mT
NF, M
elp
hala
n
7S
yn
ovia
lsa
rco
ma
Prim
ary
31
8 c
mT
NF, M
elp
hala
n
8M
yxo
id c
hondro
sarc
om
aP
rimary
21
8 c
mT
NF, IF
N, M
elp
hala
n
9M
alig
nant fib
rous h
istio
cyto
ma
Prim
ary
21
19 c
mT
NF, IF
N, M
elp
ha
lan
10
Ma
lignant fib
rous h
istio
cyto
ma
Recurre
nt
124 *
2 c
mT
NF, IF
N, M
elp
hala
n
11M
alig
nant s
chw
annom
aR
ecurre
nt
37
5 c
mT
NF, M
elp
hala
n
12
Fib
rosarc
om
aP
rimary
31
23 c
mT
NF, IF
N, M
elp
hala
n
13
Syn
ovio
sa
rco
ma
Prim
ary
31
9 c
mT
NF, IF
N, M
elp
hala
n
14
Myxoid
liposarc
om
aR
ecurre
nt
12
8 c
mT
NF, IF
N, M
elp
hala
n
15
Dediffe
rentia
ted lip
osarc
om
aP
rimary
21
17 c
mT
NF, IF
N, M
elp
ha
lan
16
Le
iom
yo
sa
rco
ma
Recurre
nt
31
12 c
mT
NF, IF
N, M
elp
hala
n
17
An
gio
sarc
om
aP
rimary
31
30 c
mT
NF, M
elp
ha
lan
18
Malig
nant s
chw
annom
aR
ecurre
nt
21
8 c
mT
NF, IF
N, M
elp
hala
n
19
We
ll diffe
rentia
ted lip
osarc
om
aP
rimary
11
29 c
mT
NF, IF
N, M
elp
ha
lan
20
Ma
lignant fib
rous h
istio
cyto
ma
Prim
ary
34
5 c
mT
NF, M
elp
hala
n
* M
ultip
le small lesio
ns o
f the lo
wer leg
(0.5
- 2 cm
); TN
F =
tum
or n
ecrosis facto
r; IFN
= in
terferon
84
Chapter 6
Ta
ble
2P
ET
res
ult
s an
d p
atholo
gic
al r
esponse
for
each
pat
ient
V
isu
al evalu
ati
on
of
the
Meta
bo
lic r
ate
of
glu
co
se (µ m
ol/
10
0g
/min
)
P
ath
olo
gic
al
ev
alu
ati
on
P
ET
stu
die
s
Pat.
B
efo
re H
ILP
A
fter
HIL
P B
efo
re H
ILP
2
weeks a
fter
HIL
P 8
weeks a
fter
HIL
P R
esp
on
se %
via
ble
M
acro
/ m
icro
sco
pic
C
orr
esp
on
den
ce
no
.
% o
f tu
mo
r
%
of
tum
or
Tu
mo
rTu
mo
rR
imC
ore
Tu
mo
rR
imC
ore
tum
or
vie
w o
f P
ET
wit
h h
isto
log
y
acti
ve *
acti
ve *
11
00
< 1
03
6.7
3.7
8.4
0.6
n.q
.n
.q.
n.q
.p
CR
0rim
: p
se
ud
oca
psu
le+
core
: necro
sis
21
00
< 1
04
1.8
n.p
.n
.p.
n.p
.2
.76
.30
.4p
CR
0rim
: p
se
ud
oca
psu
le+
core
: necro
sis
3 8
080
3.6
n.q
.n.q
.n.q
.5.6
Absent
Absent
pC
R0
regre
ssiv
e tum
ort
issue
-
41
00
< 1
03
3.2
6.2
7.9
1.8
5.4
7.2
1.5
pC
R0
rim
: p
se
ud
oca
psu
le+
core
: necro
sis
51
00
< 1
03
6.3
5.0
6.5
1.4
4.3
6.1
0.9
pC
R0
rim
: p
se
ud
oca
psu
le+
core
: necro
sis
61
00
< 1
01
3.3
12
.8A
bse
nt
Ab
se
nt
0.9
Ab
se
nt
Ab
se
nt
pC
R0
reg
ressiv
e t
um
ort
issu
e+
71
00
< 1
01
8.0
4.5
5.9
1.7
7.2
7.4
1.6
pC
R0
rim
: p
se
ud
oca
psu
le+
core
: necro
sis
8 5
05
06
.44
.66
.31
.23
.95
.20
.9p
PR
< 1
0rim
: a
rea
s o
f via
ble
tu
mo
r-
core
: necro
sis
91
00
< 1
01
3.0
4.4
9.1
0.5
4.8
7.4
0.3
pP
R<
10
rim
: a
rea
s o
f via
ble
tu
mo
r
core
: necro
sis
10
100
< 1
04.8
7.0
Absent
Absent
n.p
.n.p
.n.p
.pP
R<
10
are
as o
f via
ble
tum
or
+
11100
< 1
08.0
n.q
.n.q
.n.q
.5.9
Absent
Absent
pP
R<
10
are
as o
f via
ble
tu
mor
+
12
100
< 1
0n.q
.n.p
.n.p
.n.p
.5.8
9.0
1.5
pP
R<
10
rim
: are
as o
f via
ble
tum
or
+
core
: necro
sis
13
100
< 1
012.5
5.0
8.1
1.2
3.6
6.9
1.0
pP
R<
20
rim
: are
as o
f via
ble
tum
or
+
core
: necro
sis
14
50
50
5.0
n.p
.n.p
.n.p
.4.2
Absent
Absent
pP
R50
are
as o
f via
ble
tum
or
+
15
50
50
12.5
9.0
Abse
nt
Absent
10.0
Absent
Absent
pP
R50
are
as o
f via
ble
tu
mor
+
16
50
50
22.5
5.7
10.1
1.0
n.p
.n.p
.n.p
.pP
R50
rim
: are
as o
f via
ble
tum
or
+
core
: necro
sis
17
30
30
3.3
2.9
13.4
1.2
7.1
26.1
1.4
pP
R50
rim
: are
as o
f via
ble
tum
or
+
core
: necro
sis
18
80
40
25.7
n.p
.n.p
.n.p
.11.3
17.3
2.4
pP
R50
rim
: are
as o
f via
ble
tum
or
+
core
: necro
sis
19
100
100
4.3
5.8
Abse
nt
Absent
4.3
Absent
Absent
pP
R100
via
ble
tum
or
+
20
80
< 2
024.2
4.4
8.4
3.0
n.p
.n.p
.n.p
.n.p
.n.p
.n.p
.n.p
.
* =
per
centa
ge
of
tum
or
volu
me
acti
ve
on P
ET
stu
dy;
pC
R =
pat
holo
gic
ally
com
ple
te r
esponse
; pP
R =
pat
holo
gic
ally
par
tial
res
ponse
; n.p
. =
not
per
form
ed;
n.q
. =
no
qu
anti
fica
tio
n
85
FDG-PET to evaluate response to TNF perfusion
Fig 1 Transversal image of a malignant fibrous histiocytoma of the lower leg in Patient 5.
Before perfusion (A) the tumor is clearly depicted as a homogeneous mass with a glucose
uptake of 36.3 µmol/100g tissue/min. Two (B) and 8 weeks after perfusion (C), the glucose
uptake in the tumor decreased to 5.0 and 4.3, respectively. The center of the tumor became
inactive surrounded by an active rim. Pathological examination revealed complete response.
The rim signal corresponded with a fibrotic vascular pseudocapsule with inflammatory tissue
surrounding a core of necrosis.
patient with no change in the percentage of viable tumor after treatment (clinically
this patient showed no response as well). In one patient (5%) the residual tumor was
not excised because of progressive distant disease. This patient died three months
after perfusion and data from this patient are excluded from the remainder of the
analyses.
Forty-nine of the scheduled 60 PET studies were completed (82%). Seven PET studies
were not performed due to patient-related problems. Technical problems prevented
quantification of PET data in four studies. Before perfusion, all tumors were easily
visualized on the baseline FDG-PET images. Twelve patients showed a homogeneous
active tumor on the preperfusion PET study, whereas eight patients also showed
inactive parts in the tumors before perfusion. Visual analysis of the PET images at 2
and 8 weeks after perfusion showed a rim of increased FDG uptake around a core of
absent FDG uptake in 12 patients (5 of 7 pCR, 7 of 12 pPR). The active rim
corresponded in the pCR patients with a fibrotic vascular pseudocapsule with reactive
inflammatory tissue, surrounding a core of absent FDG uptake representing necrosis
(Fig. 1). In patients with pPR, the active rim was found to contain both viable tumor
and an inflammatory response. Thus, the rim signal could correspond with either
viable tumor or a pseudocapsule with an inflammatory reaction. In seven patients
the tumor was visualized after perfusion as a homogeneous mass without the rim-
core configuration (2 of 7 pCR, 5 of 12 pPR). After perfusion, the amount of active
parts in the tumor declined significantly in 11 patients, corresponding with no or less
A B C
86
Chapter 6
than 20 % viable tumor tissue in the pathological specimens in each of these patients.
In two patients (Patients 3, 8) who also showed a good pathological response, the
PET study did not confirm this result. On histological examination, regressive tumor
tissue with an inflammatory reaction was found in Patient 3 and areas of viable tumor
accompanied by inflammatory tissue were found in Patient 8. The PET studies
correctly indicated moderate pathological outcome in six patients. Overall, 17 of 19
responses were correctly indicated by FDG-PET (89%), but the discrimination
between no and small amounts of viable tumor could not be made.
Pre-perfusion glucose consumption in the patients who ultimately had pCR was
significantly higher (p<0.05) than the pPR group (Fig. 2). At 2 and 8 weeks
postperfusion the MRglc in the pCR group had decreased significantly (p<0.05) in
contrast to the MRglc in the pPR group (Fig. 2). The most substantial decrease in
MRglc occurred within 2 weeks after perfusion. Figure 3 shows the percentage of
basal value of the tumor after perfusion. Patients in the pCR group showed a trend
towards a more reduced percentage of basal values than the pPR patients.
Three different histopathological groups could be distinguished after perfusion:
necrotic tissue, represented by the core MRglc of the pCR and pPR group, viable
tumor in combination with an inflammatory response, represented by the rim MRglc
of the pPR group and inflammatory with pseudocapsular tissue, represented by the
rim MRglc of the pCR group. The average MRglc in necrotic tissue was significantly
lower (p<0.05) than the values in tumor and inflammatory tissue, which were in the
same range (Fig. 4).
Fig. 2 MRglc of the tumor with
S.D. before, 2 and 8 weeks after
perfusion. Before perfusion, the
MRglc in the pCR group was sig-
nificantly higher than in the pPR
group (p<0.05). Two and 8 weeks
after perfusion, the MRglc in the
pCR group decreased significantly
(p < 0.05) in contrast to the pPR
group. HILP = hyperthermic iso-
lated limb perfusion.
87
FDG-PET to evaluate response to TNF perfusion
Fig. 3 Percentage of basal value of the
tumor for each patient, 2 and 8 weeks
after perfusion. pCR = pathologically
complete response; pPR = pathologi-
cally partial response; HILP = hyper-
thermic isolated limb perfusion
Fig. 4 MRglc in necrotic, tumor and in-
flammatory tissue. MRglc in necrotic
tissue was significantly lower (p<0.05)
than that in tumor and inflammatory tis-
sue. The latter two could not be discrimi-
nated based on MRglc
Discussion
PET has made it possible to study biochemical changes of cancer tissue and to study
the effect of treatment on metabolism in vivo. The present study demonstrates
substantial decrements in the glucose metabolism of soft-tissue sarcomas with a
pathologically complete response after perfusion with TNF. These changes were
already evident within 2 weeks. In patients with a pPR, this decrease was less
pronounced. An active rim with an inactive core was seen in 13 out of 20 patients
after perfusion. Pathological examination showed that areas of absent intratumoral
FDG uptake were consistent with necrotic tissue. The rim signal represented either
viable tumor or a fibrous pseudocapsule with inflammatory tissue. Unfortunately,
FDG-PET could not discriminate a complete response from a partial response due to
the overlap in glucose metabolism between viable tumor and inflammatory tissue.
An explanation for the observed rim-core pattern can be found in the working
mechanism of TNF. Briefly; TNF exposure invokes an altered endothelial cell
phenotype, anticoagulant mechanisms are suppressed and tissue factor is produced,
which leads to fibrin accumulation at the endothelial cell surface and thrombus
88
Chapter 6
formation in the tumor vessels, causing circulatory stasis and ischemia inside the
tumor followed by necrosis of the tumor cells adjacent to the occluded vessels.31
Necrotic tissue is unable to accumulate FDG and represents the core on the PET
image. The central necrosis elicits an inflammatory response with the formation of a
fibrous pseudocapsule. This is reflected by the rim on the PET image in the pCR
group. On the other hand, peripheral tumor cells may obtain enough nutrients from
the surrounding environment to survive. This is reflected by the rim signal in patients
with pPR. Jones et al. also found an active rim with FDG-PET after neo-adjuvant
chemotherapy of soft-tissue sarcomas. In their patients, the rim signal did not signify
viable tumor but only a fibrous pseudocapsule.32 FDG accumulation in active
inflammatory lesions is in concordance with the observation of Tahara et al. who
found an increased glucose uptake in abdominal abscesses.33 Kubota et al. also found
a high accumulation in macrophages and granulation tissue in a microautoradiographic
study.34 They state that one should consider not only the tumor cells as FDG uptake
source, but also the non-neoplastic cellular elements, that may accompany tumor
growth or necrosis. These phenomena will occur particularly in tumors subjected to
treatment. The fact that both viable tumor and inflammatory tissue accumulate FDG
is one of the major limitations of FDG as the radiopharmaceutical for cancer treatment
evaluation.
One pCR patient showed an elevated MRglc 8 weeks after perfusion, in another pCR
patient, the MRglc did not decrease 2 weeks after perfusion. These observations
could be explained by the inflammatory cell invasion in the tumor. Beside the early
vascular phenomenon, a subsequent immune effect with polymorphonuclear cell
binding to the activated endothelium is another mechanism contributing to the anti-
tumor effect of TNF.35-37 This homing of inflammatory cells in the tumor may be
responsible for a high MRglc after perfusion in these two patients. This is in
concordance with the observation that FDG uptake was diffusely increased in the
remainder of the perfused leg. This phenomenon is thought to be caused by the diffuse
inflammatory reaction that follows perfusion.
Quantitative analysis demonstrated that the pre-perfusion MRglc in the pCR group
was significantly higher than in the pPR group. Thus, high MRglc appears to predict
a good response to TNF perfusion. Since glucose uptake in soft-tissue sarcoma
correlates well with the malignancy grade of the tumor, high grade tumors could be
more susceptible to TNF perfusion.16,17 In 17 of 19 (89%) patients the visual evaluation
of the PET studies corresponded well with the pathological response. In two patients
with a good pathological response, the PET study did not confirm this. In both patients
areas of inflammatory tissue were found on histological examination corresponding
with active areas on the PET scan and therefore resulted in an overestimation of
89
FDG-PET to evaluate response to TNF perfusion
active tumor on the PET scans. Although visual evaluation gave a good indication of
the pathological outcome, the use of FDG-PET in routine clinical monitoring of
response of soft-tissue sarcomas to isolated limb perfusion is hampered by this overlap
between malignant tumor and inflammatory tissue.
Several other investigators have studied whether FDG-PET can be used to monitor
treatment for cancer. FDG uptake was found to decrease as early as 5 days after the
start of systemic therapy for breast cancer. 20,38 A change in FDG uptake was found to
better predict the ultimate outcome than change in tumor size. Decrease in FDG
uptake was more prominent in patients who responded favorably to radiotherapy or
chemotherapy for head and neck cancer compared to non-responding patients.18,39
Similar findings have been reported in other types of tumors and using a variety of
therapeutic schedules.19,40-43 These studies have in common that post-treatment PET
data were correlated with findings of physical examination, radiographic studies or,
at best, fine needle aspiration of the tumor mass, following generally accepted
guidelines.44 In none of these studies have the PET findings been verified by rigorous
microscopic examination of the whole tumor as the gold standard as we have done in
the present study. Our approach appears worthwhile, since change in tumor volume
and viability are not very well correlated. A palpable mass that remains after treatment
may consist of necrosis and fibrosis without viable tumor. On the other hand, viable
tumor may still remain when a palpable tumor that is visible on radiographic images
disappears after treatment. If one wants to investigate whether PET signifies an
improvement over radiographic techniques in the evaluation of treatment, it seems
less appropriate to use those same radiographic techniques as the reference standard.
Our results should be interpreted with caution. Our patient population was limited in
that it was a heterogeneous group of soft-tissue sarcomas and only large tumors were
included (median 8.5 cm). Additional data are needed on FDG-PET in more patients
with other tumor types treated with other drugs. Other PET tracers, such as labeled
aminoacids and 11C-thymidine, may be more suitable to distinguish between tumor
and inflammatory response.
Conclusion
The present study demonstrated that FDG-PET indicates the pathologic tumor
response to chemotherapy in an investigational setting used with isolated limb
perfusion for locally advanced soft-tissue sarcomas. The discrimination between viable
tumor and inflammatory tissue after perfusion treatment, however was hampered by
the limited specificity of FDG. A search for more specific tracers to monitor pathologic
tumor response is needed.
90
Chapter 6
References
1 Mazanet R, Antman KH. Sarcomas of soft tissue and bone. Cancer 1991; 68: 463-
473.
2 Suit HD. Local control and patient survival. Int J Radiat Oncol Biol Phys 1992; 23:
653-660.
3 Sadoski C, Suit HD, Rosenberg A, Mankin H, Efird J. Preoperative radiation, surgical
margins, and local control of extremity sarcomas of soft tissues. J Surg Oncol 1993;
52: 223-230.
4 Hoekstra HJ, Schraffordt Koops H, Molenaar WM, et al. A combination of intraarterial
chemotherapy, preoperative and postoperative radiotherapy, and surgery as limb-
saving treatment of primarily unresectable high-grade soft tissue sarcomas of the
intravascular fibrin formation in meth A fibrosarcomas. J Exp Med 1988; 168: 637-
647.
32 Jones DN, Brizel DM, Charles HC, et al. Monitoring of response to neoadjuvant
therapy of soft tissue and musculoskeletal sarcomas using F18-FDG-PET.
J.Nucl.Med. 1994; 38P (Abstract).
33 Tahara T, Ichiya Y, Kuwabara Y, et al. High [18F]-fluorodeoxyglucose uptake in
abdominal abscesses: a PET study. J Comput Assist Tomogr 1989; 13: 829-831.
34 Kubota R, Yamada S, Kubota K, et al. Intratumoral distribution of fluorine-18-
fluorodeoxyglucose in vivo: high accumulation in macrophages and granulation
tissues studied by microautoradiography. J Nucl Med 1992; 33: 1972-1980.
92
35 Palladino MAJR, Shalaby MR, Kramer SM, et al. Characterization of the antitumor
activities of human tumor necrosis factor-? and the comparison with other cytokines:
induction of tumor-specific immunity. J Immunol 1987; 138 : 4023-4032.
36 Gamble JR, Harlan JM, Klebanoff SJ, Vadas MA. Stimulation of the adherence of
neutrophils to umbilical vein endothelium by human recombinant tumor necrosis
factor. Proc Natl Acad Sci U S A 1985; 82: 8667-8671.
37 Renard N, Lienard D, Lespagnard L, et al. Early endothelium activation and
polymorphonuclear cell invasion precede specific necrosis of human melanoma and
sarcoma treated by intravascular high-dose tumor necrosis factor alpha (TNF). Int J
Cancer 1994; 57: 656-663.
38 Nieweg OE, Wong WH, Singletary SE, Hortobagyi GN, Kim EE. Positron emission
tomography of glucose metabolism in breast cancer. Potential for tumor detection,
staging, and evaluation of chemotherapy. Ann N Y Acad Sci 1993; 698: 423-428.
39 Haberkorn U, Strauss LG, Dimitrakopoulou A, et al. Fluorodeoxyglucose imaging
of advanced head and neck cancer after chemotherapy. J Nucl Med 1993; 34: 12-17.
40 Haberkorn U, Strauss LG, Dimitrakopoulou A, et al. PET studies of
fluorodeoxyglucose metabolism in patients with recurrent colorectal tumors receiving
radiotherapy. J Nucl Med 1991; 32: 1485-1490.
41 Strauss LG, Dimitrakopoulou A, Haberkorn U, Ostertag H, Helus F, Lorenz WJ.
PET studies with FDG in patients with metastatic melanoma prior and after therapy.
Eur.J.Nucl.Med. 1991; 18: 685 (Abstract).
42 Abe Y, Matsuzawa T, Fujiwara T, et al. Clinical assessment of therapeutic effects on
cancer using 18F-2- fluoro-2-deoxy-D-glucose and positron emission tomography:
preliminary study of lung cancer. Int J Radiat Oncol Biol Phys 1990; 19: 1005-
1010.
43 Bares R, Horstmann K, Altehoefer C, et al. FDG-PET to assess local effects of
radiation or chemotherapy in patients with malignant lymphoma. J.Nucl.Med. 1991;
32: 918 (Abstract).
44 Miller AB, Hoogstraten B, Staquet M, Winkler A. Reporting results of cancer
treatment. Cancer 1981; 47: 207-214.
93
Robert J. van Ginkel1
Annemieke C. Kole2
Omgo E. Nieweg1,3
Willemina M. Molenaar4
Jan Pruim2
Heimen Schraffordt Koops1
Wim Vaalburg2
Harald J. Hoekstra1
Department of Surgical Oncology1, PET Center2 and Department of Pathology4,
University Groningen Hospital, The Netherlands and Department of Surgery3, The
Netherlands Cancer Institute, Amsterdam, The Netherlands.
Journal of Nuclear Medicine 1999; 40: 262-267.
L-[1-11C]-Tyrosine PET to evaluate response to
hyperthermic isolated limb perfusion for locally
advanced soft-tissue sarcoma & skin cancer
94
Chapter 7
Abstract
PET with L-[1-11C]-tyrosine (TYR) was investigated in patients undergoing
hyperthermic isolated limb perfusion (HILP) with recombinant tumor necrosis factor
alpha (TNF) and melphalan for locally advanced soft-tissue sarcoma and skin cancer
of the lower limb. Seventeen patients (5 women, 12 men; age range 24-75 y; mean
age 52 y) were studied. TYR-PET studies were performed before HILP, and 2 and 8
weeks afterwards. The protein synthesis rates (PSR) in nanomoles per milliliter per
minute were calculated. After the final PET study, the tumor was resected and
pathologically examined. Patients with a pathologically complete response (pCR)
showed no viable tumor after treatment. Those with a pathologically partial response
(pPR) showed various amounts of viable tumor in the resected tumor specimens. Six
patients showed a pCR (35%) and 11 patients showed a pPR (65%). All tumors were
depicted as a hot spot on the PET study before HILP. The PSR in the pCR group at 2
and 8 weeks after perfusion had decreased significantly (p<0.05) compared to the
PSR before HILP. A significant difference was found in PSR between the pCR and
pPR group at 2 as well as at 8 week (p<0.05). Median PSR in nonviable tumor tissue
was 0.62 and ranged from 0.22 to 0.91. With a threshold PSR of 0.91, sensitivity and
specificity of TYR-PET were 82% and 100%, respectively. The predictive value of a
PSR > 0.91 for having viable tumor tissue after HILP was 100%, whereas the
predictive value of a PSR ≤0.91 for having nonviable tumor tissue after HILP was
75%. On pathological examination the 2 patients in the pPR group with a
PSR < 0.91 showed microscopic islets of tumor cells surrounded by extensive necrosis.
Based on the calculated PSR after HILP, TYR-PET gave a good indication of the
pathological outcome. Inflammatory tissue after treatment did not interfere with viable
tumor tissue on the images, suggesting that it may be worthwhile to pursue TYR-PET
in other therapy evaluation settings.
Introduction
Different metabolic processes such as glycolysis, protein synthesis, uptake of
disaccharides and transamination, are enhanced in tumors when compared to normal
tissues. PET enables visualization and quantification of metabolic processes in vivo.18Fluorine-labeled 2-fluoro-2-deoxy-D-glucose (FDG) is the most commonly used
radiopharmaceutical for PET and has proven to be of value to visualize various types
of solid tumors, to indicate the malignancy grade and to detect locally recurrent
disease.1-4 Various clinical reports suggest the feasibility of FDG-PET to assess tumor
response to radiotherapy and chemotherapy.5-7 A limitation of FDG-PET in therapy
evaluation is the inability to differentiate between viable tumor tissue and
inflammatory tissue.8-10 Therefore, there is a need for alternatives. Ishiwata et al.11
95
TYR-PET to evaluate response to TNF perfusion
have shown that the uptake of amino acids is high in tumor tissue due to an increased
protein synthesis rate (PSR). Amino acids play a minor role in the metabolism of
inflammatory cells, mainly neutrophils, compared to FDG. Most amino acid PET
studies have been performed with L-[methyl-11C]-methionine (MET).12-14 MET reflects
amino acid uptake rather than protein synthesis because it is involved in other
metabolic pathways such as transmethylation and polyamine synthesis.15,16 This
complicated metabolism of methionine has made it impossible to create a precise
metabolic model. Carboxyl-labeled amino acids, such as L-[1-11C]-tyrosine (TYR),
L-[1-11C]-methionine and L-[1-11C]-leucine, appear to be more appropriate compounds
to determine protein synthesis in tumors.16,17 The main metabolite of these amino
acids is 11CO2, which is rapidly cleared from tissue and exhaled and does not contribute
to the PET-measured 11C radioactivity in tumor tissue.
A model was developed to determine the PSR in tumor tissue using TYR.18 Initial
results in patients with brain tumors have been published recently.19 Kole et al. 20
reported a high uptake of TYR and, as a consequence, a high PSR in various types of
malignancies and low uptake in benign lesions. PET with TYR may be of value in
the assessment of the response of a malignant tumor to therapy, because a decrease
in tissue viability may result in a decrease in PSR.
Hyperthermic isolated limb perfusion (HILP) with recombinant tumor necrosis factor
alpha (TNF) and melphalan can usually prevent amputation in patients with locally
advanced soft-tissue sarcoma or extensive local regional melanoma.21,22 The aim of
this study was to investigate PET with TYR in patients undergoing HILP for locally
advanced soft-tissue sarcoma and skin cancer and to correlate PET findings with
histology before and after treatment.
Materials and methods
Patients
Seventeen patients (5 women, 12 men; aged 24-75 yrs; mean age 52 yrs) with biopsy-
proven soft-tissue sarcoma or melanoma participated in the study approved by the
Medical Ethical Committee of the institute. Informed consent was obtained from
each patient. Ten patients presented with a newly diagnosed soft-tissue sarcoma, 2
patients presented with a local recurrence of a soft-tissue sarcoma previously treated
with surgery alone, 4 patients presented with a melanoma and 1 patient presented
with a squamous cell carcinoma. All tumors were located in the lower limb. The
diagnosis of the tumors was determined in a standard fashion and soft-tissue sarcomas
were graded according to Coindre et al.23 All tumors were considered primarily
irresectable because of size, multicentricity in the limb, or fixation to the neurovascular
bundle or bone. Median tumor size was 10 cm (range 3-25 cm). Patients and tumor
96
Chapter 7
characteristics are summarized in Table 1.
Methods
The perfusion technique used at the Groningen University Hospital is based on the
technique developed by Creech et al.24 and has been described in detail previously.22
Briefly, after cannulation of the vessels of the perfused limb, a tourniquet is placed at
the base to prevent systemic leakage. The limb is perfused with 4 mg TNF (Boehringer,
Ingelheim, Germany) administered directly intra-arterially, followed 30 min later by
10 mg/L volume melphalan (Burroughs Wellcome, London, England). Perfusion is
carried out for 90 min under hyperthermic conditions (39-40°C). Preventive measures
to cope with the expected side effects caused by leakage consist of fluid loading and
administration of vasoactive amines. After HILP, patients are mechanically ventilated
until they are hemodynamically stable and receive intensive care management as
described by Zwaveling et al.25 Approximately 8 weeks after perfusion (median 66
Table 1 Tumor characteristics
Pat. Histology Site Grade Number Largest
no. of diameter
lesions ( MRI)
1 Melanoma Recurrent Lower leg n.a. 2 3.5 cm
2 Squamous cell carcinoma Primary Foot n.a. 1 6.0 cm
3 Clear cell carcinoma Primary Lower leg 3 1 10.0 cm
4 Melanoma Recurrent Lower leg n.a. 3 4.0 cm
5 Leiomyosarcoma Primary Lower leg 3 1 12.5 cm
6 Melanoma Primary Lower leg n.a. 1 7.0 cm
7 Synoviosarcoma Primary Popliteal fossa 2 1 4.0 cm
8 Fibrosarcoma Primary Knee 1 1 3.0 cm
9 Synoviosarcoma Recurrent Lower leg 2 1 9.0 cm
10 Haemangiopericytoma Primary Popliteal fossa 2 1 15.0 cm
11 Malignant fibrous histiocytoma Primary Thigh 3 1 23.0 cm
12 Angiosarcoma Primary Lower leg 3 1 12.5 cm
13 Extra-osseous osteosarcoma Primary Thigh 3 1 25.0 cm
14 Myxoid liposarcoma Primary Thigh 1 1 8.0 cm
15 Myxoid liposarcoma Primary Popliteal fossa 2 1 11.0 cm
16 Malignant fibrous histiocytoma Primary Thigh 2 1 10.0 cm
17 Melanoma Primary Toe n.a. 5 3.0 cm
n.a. = not applicable
97
TYR-PET to evaluate response to TNF perfusion
days, range 27-125 days) the residual tumor masses were excised and pathologically
examined. The tumor remnants were measured in three dimensions and the percentage
of necrosis estimated. Representative tumor sections were taken, encompassing
macroscopically different tumor areas including necrosis. As a general rule, one section
per centimeter largest diameter with a minimum of three was taken. Based on an
integration of gross and microscopic findings, a final estimate of the percentages of
viable and necrotic or regressive tumor was made. If possible, macroscopic
examination and tissue sampling was performed based on the latest PET images.
The results were classified as either pathologically complete response (pCR) or
pathologically partial response (pPR), when remaining viable tumor was noted.
PET imaging
Patients were scheduled for three PET studies: shortly before perfusion (n = 17,
median 10 days, range 1 - 23 days), 2 weeks after perfusion (n = 14, median 16 days,
range 12 - 23 days) and shortly before resection of residual tumor tissue (n = 15,
median 55 days, range 47 - 68 days after perfusion). TYR was produced by a modified
microwave-induced Bücherer-Strecker synthesis26 , with a radiochemical purity of
more than 99%. PET sessions were performed using an ECAT 951/31 PET camera
(Siemens/CTI, Knoxville, USA).
All patients fasted for at least 8 hours before the investigation. Serum tyrosine levels
were measured before each PET session and were found to be normal (mean 0.053
mmol/L, range 0.028 - 0.1 mmol/L). A 20-gauge needle was inserted into the radial
artery under local anesthesia. In the contralateral arm, an intravenous canula was
inserted in the cephalic vein for the injection of TYR. The patients were positioned
supine in the camera, with the tumor in the field of view based on physical
examination.
After attenuation scanning using a 68Ge/68Ga source, we administered a mean dose of
322 MBq (range 126 - 381 MBq) TYR intravenously over 1 min. Dynamic images
were acquired from the time of injection following a dynamic protocol (ten 0.5 min,
three 5 min, three 10 min) for a total duration of 50 min. Simultaneously, 2-ml blood
samples were taken from the arterial canula (time points 0.25, 0.5, 0.75, 1.0, 1.25,
1.5, 1.75, 2.25, 2.45, 3.75, 4.75, 7.5, 12.5, 17.5, 25, 35, and 45 min postinjection).
The blood samples were centrifuged and plasma activity of TYR, the 11C-labeled
CO2 and protein levels were measured by high-performance liquid chromatography
(HPLC). The duration of the imaging procedure was approximately 2.5 h.
98
Chapter 7
Data analysis
Images were displayed in coronal, sagittal and transaxial projections on a computer
display using standard ECAT software and were interpreted independently by two
experienced physicians. To determine tumor PSR, one must first define the tumor in
all relevant tomographic planes of the study. Usually this is done by placing regions
of interest (ROIs) in each plane, matching the size of the tumor as outlined by MRI.
The tissue time-activity curves obtained from these ROIs can be averaged and the
average PSR can be calculated. Because this technique is rather laborious, an
alternative method was developed at our institute. By using the same activity threshold
as the one used to define the ROI, we selected all voxels in the study above this
threshold. For each analysis, a fixed percentage of 95% was used. The corresponding
activity was summed and the average time-activity curve and the total volume were
obtained. The advantage of this approach is that the analysis of the whole tumor is
performed quickly and simply and the results are identical to those of the ROI method.
Parts of the tumor that do not accumulate TYR are ignored by this method. By
combining this averaged time-activity data with the plasma input data (corrected for11CO
2 and 11C-proteins), we calculated the average PSR in nanomoles per milliliter
tumor tissue per minute using the modified Patlak analysis as described previously.18
The PSR in contralateral normal tissue was calculated using a ROI technique. A
tumor-to-nontumor ratio (T/N ratio) was calculated from the PSR in tumor tissue
and the PSR in contralateral normal tissue. The change in PSR after perfusion was
related to the preperfusional value and was expressed as a percentage of basal value.
Statistical analysis
The statistical procedures included a two-factor experiment with repeated measures
on one factor to compare PSR between measures and groups. Analyses were performed
on data sets corrected for missing data according to Winer.27 Post hoc comparison
was made with Student´s t-tests. A p value < 0.05 was considered significant. Analysis
was carried out by SPSS.
Results
PET results and pathological response for each patient are summarized in Table 2.
Pathological examination of the residual tumor mass showed no viable tumor in 6
patients (pCR 35%), 3 of whom had a melanoma. In 11 patients, variable amounts of
viable tumor were found at pathological examination (pPR 65%). Forty-six of the
scheduled 51 PET studies were completed (90%). Five PET studies were not
performed due to patient-related problems. All tumors were depicted as a hot spot on
the PET study before HILP with variable degrees of TYR accumulating parts (T/N
99
TYR-PET to evaluate response to TNF perfusion
Ta
ble
2P
ET
results an
d p
atholo
gical resp
onse
Pro
tein
sy
nth
es
is ra
te (n
mo
l/ml/m
in) P
ath
olo
gic
al e
va
lua
tion
Pa
t. Be
fore
HIL
P 2
we
ek
s a
fter H
ILP
8 w
ee
ks
afte
r HIL
P R
es
po
ns
e %
Via
ble
Ma
cro
/mic
ro-s
co
pic
vie
w
no
. Tu
mo
r Co
ntra
lat T
/N ra
tio T
um
or C
on
trala
t T/N
ratio
Tu
mo
r Co
ntra
lat T
/N ra
tio tu
mo
r
12.4
50.1
417.5
0.1
70.1
41
.20.2
20.4
10.5
pC
R0
Rim
with
infla
mm
ato
ry tis
sue
23.5
10.1
523.4
1.0
20.1
66
.40.9
10.2
04.6
pC
R0
Infla
mm
ato
ry tis
sue
32
.53
0.4
35
.9n
.p.
n.p
.n
.p.
0.5
00
.31
1.6
pC
R0
Infla
mm
ato
ry tis
su
e
42.0
60
.40
5.2
0.7
40.2
62
.9n
.p.
n.p
.n
.p.
pC
R0
Infla
mm
ato
ry tis
su
e
52.1
30.4
15.2
0.7
10.2
33
.10.8
50.2
04.3
pC
R0
Rim
with
infla
mm
ato
ry tis
sue
61.3
10.4
03
.30.6
20.2
72.3
0.3
50.2
11
.7pC
R0
Infla
mm
ato
ry tis
sue
72.0
60.2
48
.61.3
90.4
33.2
0.4
80.2
91
.7pP
R<
10
Mic
roscopic
isle
ts o
f via
ble
tum
or
81.7
60.2
57
.00.6
40.2
62.5
0.8
00.2
13
.8pP
R<
10
Mic
roscopic
isle
ts o
f via
ble
tum
or
90.9
20.3
32
.8n.p
.n.p
.n.p
.0.9
90.3
23.1
pP
R<
10
Mic
rosco
pic
isle
ts o
f via
ble
tum
or
10
2.0
00.2
38.7
2.3
00.3
07
.71.4
60.2
26.6
pP
R<
10
Are
as o
f via
ble
tum
or
11
2.3
00.2
68.9
1.2
60.1
87
.02.3
10.1
614.4
pP
R<
10
Are
as o
f via
ble
tum
or
12
5.2
70.2
521.1
2.7
90.1
815.5
n.p
.n
.p.
n.p
.pP
R<
10
Are
as o
f via
ble
tum
or
13
1.6
80
.17
9.9
n.p
.n
.p.
n.p
.3.9
10.4
88
.2pP
R<
20
Rim
with
via
ble
tum
or
14
0.7
30.2
43.4
1.6
10.4
73
.41.8
30.4
83.8
pP
R<
50
Are
as o
f via
ble
tum
or
15
0.6
40.2
42.7
1.3
50.3
34
.12.1
30.6
03.6
pP
R<
50
Are
as o
f via
ble
tum
or
16
2.9
00.4
66.3
1.4
70.4
33
.42.4
80.3
18.0
pP
R<
50
Are
as o
f via
ble
tum
or
17
1.6
10.2
46.7
1.2
40.0
913.8
0.9
40.0
811
.8pP
R<
50
Via
ble
tum
or
Contra
lat =
contra
late
ral n
orm
al tis
sue; p
CR
= p
ath
olo
gic
ally
com
ple
te re
sponse; p
PR
= p
ath
olo
gic
ally
partia
l response; n
.p. =
not p
erfo
rmed
100
Chapter 7
ratio > 1.00 in all patients). Preperfusion PSR in the patients who ultimately went on
to have a pCR was not significantly different from the PSR in the pPR group
(Fig.1). Analysis of the PET images at 2 and 8 weeks after perfusion showed a decrease
of TYR accumulating parts in all pCR patients.
Fig. 1 Protein synthesis rate (PSR) of
tumor with S.D. before, 2 and 8 weeks
after perfusion. Two and 8 weeks after
perfusion, PSR in pathologically com-
plete response (pCR) group decreased
significantly (p<0.05) in contrast with
PSR in pathologically partial response
(pPR) group. Significant difference
was found in PSR between the pCR and
pPR groups at 2 and 8 weeks (p<0.05).
HILP = hyperthermic isolated limb
perfusion
The PSR in the pCR group had decreased significantly at 2 and 8 weeks after perfusion
compared with preperfusional values (p<0.05) in contrast to the PSR in the pPR
group. A significant difference was found in PSR between the pCR and pPR group at
2 as well as at 8 weeks (p<0.05). The most substantial decrease in PSR occurred
within 2 weeks after perfusion. Figure 2 illustrates the succeeding PET studies in
patient 11. After an initial decrease in PSR at 2 wk, a renewed outgrow of the tumor
was observed at 8 weeks after perfusion. Necrosis within the tumor was visualized
as a cold spot. In this patient, TYR-PET indicated the need for an early resection of
the tumor as perfusion did not seem to have the desired result. Pathological
examination revealed areas of viable tumor that encompassed less than 10% of the
total tumor volume.
The median PSR in contralateral muscle tissue was 0.28 and ranged from 0.08 to
0.60. PSR in tumor tissue was higher than in the corresponding contralateral normal
tissue (p<0.05). Median PSR in nonviable tumor tissue was 0.62 and ranged from
0.22 to 0.91. With a threshold PSR of 0.91, the highest value obtained from nonviable
tumor tissue, the sensitivity and specificity of TYR-PET after HILP treatment were
82% and 100%, respectively. The predictive value of a PSR > 0.91 for having viable
tumor after HILP was 100%, whereas the predictive value of a PSR ≤ 0.91 for having
nonviable tumor tissue after HILP was 75% (Fig. 3). The two patients in the pPR
group with a PSR < 0.91, patients 8 and 9, showed microscopic islets of tumor cells
surrounded by extensive necrosis on pathological examination. With a threshold PSR
of 0.48, the lowest value obtained from viable tumor tissue, the sensitivity and
101
TYR-PET to evaluate response to TNF perfusion
specificity of TYR-PET after HILP treatment were 100% and 33%, respectively.
The predictive values for viable and nonviable tumor tissue after HILP were 73%
and 100%, respectively.
Figure 4 shows the percentage of basal value of the tumor after perfusion. All patients
in the pCR group showed a reduction of PSR whereas some pPR patients showed a
reduction and others an increase in PSR after perfusion. The reduction in the pCR
group was significant at 2 and 8 weeks after perfusion. However, based on a certain
percentage of reduction of basal value, no assumption could be made as to whether
or not the individual patient showed a pCR or a pPR.
Two different histopathological groups could be distinguished after perfusion:
nonviable tumor tissue, corresponding with inflammatory tissue, and viable tumor
tissue. Figure 5 shows the PSR in these two different histopathological groups
Fig 2. Transversel PET image of a patient with a malignant fibrous histiocytoma of the thigh
(patient 11). Before perfusion (A) the tumor is clearly depicted as a heterogeneous mass with
a PSR of 2.30 nmol/ml/min. After initial reduction in PSR (1.26) at 2 weeks after perfusion
(B), the malignant fibrous histiocytoma showed renewed growth (PSR 2.31) at 8 weeks after
perfusion (C). The gray scale equates a particular hue to a particular PSR in nmol/ml/min.
PA viable PA Nonviable Total
PET Viable 9 0 9
PET Nonviable 2 6 8
Total 11 6 17
Fig 3. Cross tabulation table with threshold PSR of 0.91. Sensitivity and specificity of TYR-
PET were 82% and 100%, respectively. Predictive value for viable tumor after HILP was
100%, whereas predictive value for nonviable tumor tissue after HILP was 75%. Two patients
in the pPR group with PSR<0.91, showed microscopic islets of tumor cells surrounded by
extensive necrosis on pathological examination. PA = pathology
A B C
102
Chapter 7
compared with the PSR in normal contralateral muscle. The average PSR in
inflammatory tissue was significantly lower than the PSR values in viable tumor
tissue (p<0.05).
Discussion
PET has made it possible to study biochemical changes of cancer tissue and to study
the effect of treatment on metabolism in vivo. This study demonstrates a significant
decline in the protein metabolism of locally advanced soft-tissue sarcomas and skin
cancer with a pathologically complete response after HILP with TNF and melphalan.
These changes were already evident within 2 weeks. In patients with a pPR, this
decrease was not significant. These findings are similar to the results of a previous
study performed in the same manner with FDG.9 With TYR-PET, however, there
was a significant difference at 2 and at 8 weeks in PSR between the pCR and pPR
groups, a finding that was not observed with FDG-PET. That previous finding may
have been caused by the fact that FDG is also accumulated by inflammatory tissue,
resulting in an overlap in glucose metabolism between viable tumor and inflammatory
tissue. In this study, TYR was also accumulated by inflammatory tissue that existed
Fig. 4 Percentage of basal value of tu-
mor for all patients 2 and 8 weeks after
perfusion. pCR = pathologically com-
plete response; pPR = pathologically
partial response; HILP = hyperthermic
isolated limb perfusion
Fig. 5 Protein synthesis rate (PSR) in
viable tumor, inflammatory and con-
tralateral normal tissue. PSR in viable
tumor tissue was significantly higher
than inflammatory tissue (p<0.05)
103
TYR-PET to evaluate response to TNF perfusion
after HILP but was accumulated significantly less than in viable tumor tissue. Because
TYR can better discriminate between viable tumor tissue and inflammatory tissue
than FDG, TYR is a more reliable technique to evaluate treatment response. The
major question for clinicians is the exact timing for the surgical resection after HILP
because the tumoricidal effect of HILP seems to be time related. If the threshold PSR
of 0.91 was exceeded 8 weeks after HILP, we could with certainty predict that viable
tumor was still present and surgical resection of the tumor remnants was indicated.
However, when resection was omitted with a PSR less than 0.91, there was a 25%
chance of leaving microscopic islets of tumor tissue. The resolution of the PET camera
may be the limiting factor in detecting these microscopic islets of viable tumor,
although it remains questionable if these small amounts of tumor tissue surrounded
by avascular necrosis can lead to a local recurrence. Instead of surgical resection,
these patients could possibly also be treated with external beam radiotherapy, and
monitored closely for development of a local recurrence. Leaving residual tumor
mass was safe when PSR was lower than 0.48 after HILP.
Before perfusion, there was no significant difference in PSR between the patients in
the pCR and pPR group. This was in contrast with the results of the FDG study
where we found a significant difference in glucose consumption before perfusion
between both groups.9 So TYR can not be used to predict the likelihood of a response
to HILP. For FDG we also found a correlation between tumor malignancy grade and
the level of glucose metabolism.3 This is not the case for the protein synthesis of the
different grades of soft-tissue sarcomas in this study but the number of patients is
small. This difference between FDG and TYR may be explained by the fact that
FDG is trapped inside the cell as a result of an increased level of glucose transporters
on the cell membrane.28 FDG accumulates as it reaches its end in its metabolic pathway
as FDG-6-phosphate; the more glucose transports there are on the cell membrane,
the more FDG is incorporated in the cell, corresponding with a high malignancy
grade. TYR, not hampered by an anorganic isotope, continues its metabolic pathway
and is not accumulated in the cell.
Combining the results of this study with the results of our previous FDG study, it is
tempting to state that FDG-PET should be performed before HILP to identify patients
who will most likely benefit from this treatment and TYR-PET should be performed
8 weeks after HILP to evaluate the outcome of the therapy. However, our results
should be interpreted with caution since this patient population is a small group of
heterogeneous soft-tissue sarcomas and skin cancers and only large tumors were
included. Additional data are needed on TYR-PET in more patients with other tumor
types treated with other chemotherapeutic agents and pathological examination as
the gold standard.
104
Chapter 7
Conclusion
This study demonstrates that TYR-PET indicates the pathologic tumor response to
chemotherapy in an investigational setting used with HILP with TNF and melphalan
for locally advanced tumors. Based on the calculated PSR after perfusion, a good
indication was found towards the pathological outcome. Inflammatory tissue after
treatment did not interfere with viable tumor on the images, suggesting that it may be
worthwhile to pursue TYR-PET in other therapy evaluation settings.
References
1 Conti PS, Lilien DL, Hawley K, et al. PET and [18F]-FDG in oncology: a clinical
update. Nucl Med Biol 1996; 23: 717-735.
2 Rigo P, Paulus P, Kaschten BJ, et al. Oncological applications of positron emission
tomography with fluorine-18 fluorodeoxyglucose. Eur J Nucl Med 1996; 23: 1641-
1674.
3 Nieweg OE, Pruim J, van Ginkel RJ, et al. Fluorine-18-fluorodeoxyglucose PET
imaging of soft-tissue sarcoma. J Nucl Med 1996; 37: 257-261.
4 Kole AC, Nieweg OE, van Ginkel RJ, et al. Detection of local recurrence of soft-
tissue sarcoma with positron emission tomography using [18F]fluorodeoxyglucose.
Ann Surg Oncol 1997; 4: 57-63.
5 Findlay M, Young H, Cunningham D, et al. Noninvasive monitoring of tumor
metabolism using fluorodeoxyglucose and positron emission tomography in colorectal
cancer liver metastases: correlation with tumor response to fluorouracil [see
comments]. J Clin Oncol 1996; 14: 700-708.
6 Jones DN, McCowage GB, Sostman HD, et al. Monitoring of neoadjuvant therapy
response of soft-tissue and musculoskeletal sarcoma using fluorine-18-FDG-PET.
Blood 1996; 37: 1438-1444.
7 Lindholm P, Leskinen Kallio S, Grenman R, et al. Evaluation of response to
radiotherapy in head and neck cancer by positron emission tomography and
[11C]methionine. Int J Radiat Oncol Biol Phys 1995; 32: 787-794.
8 Kubota R, Yamada S, Kubota K, et al. Intratumoral distribution of fluorine-18-
fluorodeoxyglucose in vivo: high accumulation in macrophages and granulation
tissues studied by microautoradiography. J Nucl Med 1992; 33: 1972-1980.
9 van Ginkel RJ, Hoekstra HJ, Pruim J, et al. FDG-PET to evaluate response to
hyperthermic isolated limb perfusion for locally advanced soft-tissue sarcoma. J
Nucl Med 1996; 37: 984-990.
10 Lewis PJ, Salama A. Uptake of fluorine-18-fluorodeoxyglucose in sarcoidosis. J
dehydrogenase (LDH) with its iso-enzymes, creatine phosphokinase and myoglobin
were taken a day before perfusion, at the day of perfusion, and every day after
perfusion until day 7. A final blood sample was taken one month after perfusion.
Blood samples (3 ml) were collected in EDTA vacutainer tubes, and kept on melting
ice during transport to a centrifuge. Samples were centrifuged for 10 min at 3000
rpm at 0°C and the separated plasma kept at –80°C until analysis.
TNF levels were determined by specific immunoradiometric assay (Medgenix
Diagnostics, Soesterberg, the Netherlands). Samples were processed according to
the guidelines of the manufacturer. IL-6 and CRP levels were measured by in-house
sandwich ELISA’s as described previously19, by using commercial reagents for IL-6
(CLB, Amsterdam, the Netherlands; detection limit 10 ng/L) and for CRP (DAKO,
Glostrup, Denmark; normal level <2.3 mg/L).
Assessment of tumor response
Responses were assessed by standardized World Health Organization criteria.20
Complete response (CR) was defined as the disappearance of all measurable disease
in the limb for longer than 4 weeks, partial response (PR) as regression of the tumor
size by >50% for longer than 4 weeks, and no change (NC) as regression of <50% of
the tumor in the limb or progression of <25% for longer than 4 weeks. To analyze
whether or not a high systemic leakage was of influence in the occurrence of distant
metastasis subanalyses of this parameter in a group of patients with grade II and III
soft tissue sarcomas was performed.
Statistical analysis
Values are expressed as mean ± SEM. Comparison between mean values of different
groups was performed with the unpaired or in case of measuring the same variable in
the same patient at different time points, with the paired Student’s t-test. Areas under
the curve (AUC) were determined by the trapezoid rule. Survival curves were
calculated according to the Kaplan Meier method and log rank test.21 Values of
p ≤ .05 were considered to be statistically significant. Graph Pad Prismâ version 2.0
for Windows (GraphPad, San Diego, CA) statistical software was used.
113
Leakage during isolated limb perfusion with TNF
Results
Systemic leakage
For the 51 perfusions, the mean isotopically measured leakage was 2.9 % (95%
confidence interval, 2.0 – 3.8%, range 0-15.5%). After 60 minutes of perfusion in
the patient with the highest leakage (15.5%), it was noted that the rubber bandage
twisted around the root of the extremity was ruptured. Since this was the cause of the
high leakage and perfusion was not completed, the data from this patient are excluded
from the remainder of the analyses. Systemic leakage was ≤ 2% in 28 perfusions
(55%) and >2% in 23 perfusions (45%). In the latter group, 11 perfusions (22%) led
to systemic leakage of >5%. In addition, analysis of different parameters between
the group of patients with ≤ 2% leakage and the group of patients with >2% leakage,
was made. Figure 1 shows the measured leakage at different perfusion levels. There
was a significant difference between perfusions performed at the iliac and femoral
levels compared with leakage values at the popliteal level, (p < 0.0001 and 0.0159
respectively). There was no leakage encountered in patients with axillary perfusions.
Fig. 1 Scatter diagram of leakage at dif-
ferent perfusion levels, the uninterrupted
line represents mean values. A significant
difference was observed between perfu-
sions performed at the iliac and femoral
levels compared with leakage values at
the popliteal level, (p < 0.0001 and
0.0159 respectively)
Perfusion circuit levels
At 5 minutes, mean TNF levels in the perfusion circuit were 6798 ± 528 ng/ml
(Fig. 2). During perfusion, a significant drop in TNF levels in the perfusion circuit
occurred with a significant lower concentration of TNF in the perfused limb in patients
with >2% leakage at 30 (p = 0.0201), 60 (p = 0.0337) and 89 minutes (p = 0.002).
The calculated mean AUC, indicating the exposure of the perfused limb to TNF, was
18.7% less in the >2% leakage group (p=0.0457). IL-6 levels in the perfusate, as one
of the most important proinflammatory cytokines, progressively increased from 30
minutes until the end of the perfusion, reaching 4.2 ± 1.1 ng/ml in the ≤2% leakage
114
Chapter 8
Fig. 2 Tumor necresis factor (TNF)
levels in the perfusion circuit (mean ±SEM). A significant decrease in TNF
levels occurred with significant lower
concentration of TNF in the perfused
limb in patients with >2% leakage at
30 (p = 0.0201), 60 (p = 0.0337) and
89 minutes (p = 0.002). Mean area un-
der the curve, indicating the exposure
of the perfused limb to TNF, was 18.7%
less in the >2% leakage group
group and 11.7 ± 3.5 ng/ml in the >2% leakage group (p=0.0455). CRP levels in the
perfusion circuit remained at the detection level, and no significant differences were
observed between the leakage groups.
Systemic levels
Systemic TNF levels in patients with >2% leakage were already significantly higher
at 5 min after TNF injection compared with the group of patients with ≤2% leakage.
Peak systemic TNF values of 116.5 ± 28.9 ng/ml were reached in the >2% leakage
group at the end of perfusion, compared with 11.8 ± 3.4 ng/ml in the ≤2% leakage
group (p < 0.0001) (Fig. 3). The calculated mean systemic AUC, indicating the
exposure of the patient to TNF, was 18.1 times higher in the >2% leakage group
(p<0.0001). Ten minutes after release of the tourniquet we observed a significant
systemic peak level of TNF in the ≤2% group possibly caused by the TNF still present
in the perfused limb after the washout procedure (p=0.026). To calculate the correlation
between maximum systemic TNF levels and the maximum monitored leakage using
RISA measured during perfusion, Pearson’s correlation (two-tailed) was used. Figure
4 illustrates the observed correlation with r = 0.7114 and p < 0.0001. A strong
correlation was also found between the maximal observed leakage and maximum
IL-6 concentration measured in the postoperative period (r = 0.7737, P<0.0001).
IL-6 levels appeared in the systemic circulation 30 minutes after the start of the
perfusion and maximal levels were reached 2 hours after HILP (19.5 ± 5.8 ng/ml
≤2% leakage versus 77.7 ± 20.8 ng/ml >2% leakage; p=0.0089). The AUC of IL-6
was 4.7 times higher in the >2%leakage group compared with ≤2% leakage group
(p<0.0243).
115
Leakage during isolated limb perfusion with TNF
CRP started to increase 6 hours after HILP and reached its maximal value 2 days
after perfusion (185.8 ± 25.5 mg/L ≤2% leakage versus 226.7 ± 32.7 mg/L, >2%
leakage; not significant). The AUC of CRP between both groups however was not
significantly different.
Hematological and metabolic parameters
Leukocyte counts increased from 7.7 ± 0.3x109/L to 13.0 ± 0.6x109/L one day after
perfusion. Five, 6, and 7 days after perfusion a significant difference between the
two leakage groups was observed (Fig. 5). Platelet counts decreased from 303.6 ±13.4x109/L before perfusion to 124.3 ± 10.7x109/L 4 days after perfusion.
Fig. 3 Tumor necrosis factor (TNF) lev-
els in the systemic circulation of the pa-
tient (mean ± SEM). A significant dif-
ference was found between the >2%
leakage group and the ≤2% leakage
group is starting 5 min after TNF injec-
tion until the second postoperative day
(p<0.05). The mean systemic area un-
der the curve, indicating the exposure
of the patient to TNF, was 18-times
higher in the >2% leakage group
Fig. 4 Pearson’s correlation (two-
tailed) between maximal systemic TNF
levels measured during perfusion and
maximal monitored leakage using
RISA (r = 0.7114 and P<0.0001)
116
Chapter 8
The low platelet levels persisted longer in the >2% leakage group. Kidney function
was well preserved in all patients, although urea nitrogen and creatinine levels in the
>2% leakage group were significantly higher during the first 5 days after perfusion;
these levels however remained within normal limits. Liver function tests showed an
increase in bilirubin values from 10.5 ± 0.9 µmol/L to 44.8 ± 11.3 µmol/L, 4 days
after perfusion in the >2% leakage group, with significant differences compared with
the ≤2% leakage group (Fig. 6). Figure 6 illustrates the decrease in protein levels and
cholesterol levels after perfusion, with significant differences between both leakage
groups. Alkaline phosphatase increased from 86.1 ± 6.5 U/L to 159.4 ± 32.8 U/L,
aspartate aminotransferase increased from 22.8 ± 1.5 U/L to a maximum of 62.1 ±13.4 U/L on the fifth day after perfusion, alanine aminotransferase increased from
21.9 ± 2.6 U/L to a maximum of 80.3 ± 11.6 U/L on the sixth day after perfusion, and
gammaglutamyltransferase increased from 37.7 ± 8.7 U/L to a maximum of 120.1 ±18.6 U/L on the sixth day after perfusion. LDH increased from 224.8 ± 9.0 U/L to a
maximum of 417.3 ± 19.1 U/L on the second day after perfusion. LDH iso-enzymes
1 and 2 showed a decrease, whereas LDH iso-enzymes 4 and 5 increased one day
after perfusion. LDH iso-enzyme 3 remained at the same level. Creatine phospho-
kinase levels increased from 28.3 ± 2.4 U/L to a maximum of 496.4 ± 197.6 U/L on
Fig. 5 White blood cell count (WBC)
and platelets (PLT) levels from before
perfusion to 30 days after perfusion
(mean ± SEM). * indicates a significant
difference between both leakage groups
(p < 0.05)
117
Leakage during isolated limb perfusion with TNF
the second day after perfusion. Myoglobin levels increased from 30.2 ± 2.4 µg/L to
a maximum of 422.8 ± 99.7 µg/L one day after perfusion. None of these variables
showed a significant difference between both leakage groups.
Tumor Response
In the ≤2% leakage group, 14 patients showed a CR and the same number of patients
a PR. In the >2% leakage group, 11 patients showed a CR, 10 patients a PR and 2
patients had NC. No significant differences in response to TNF HILP were found
between the groups. No significant difference was observed in the occurrence of
distant metastasis or survival in the subanalyses of a group of patients with grade II
or III soft tissue sarcoma and >2% leakage (Fig. 7).
Fig. 6 Bilirubin, protein and cholesterol
levels from before perfusion to 30 days
after perfusion (mean ± SEM). * indicates
a significant difference between both leak-
age groups (p < 0.05)
118
Chapter 8
Discussion
The purpose of continuous leakage monitoring with RISA during HILP is to indicate
the amount of chemotherapeutic agent that is leaking from the perfusion circuit into
the patient’s systemic circulation. When leakage occurs, measures to reduce leakage
should be available. During perfusion there is a dynamic balance between two pressure
compartments: the patients systemic vasculature and the isolated circuit. The pressure
of the former compartment can be influenced by adjusting the systemic blood pressure,
whereas that of the latter can be affected by alterations in the extracorporeal flow
rate. Thus, to decrease leakage, the anesthesiologist can increase the patient’s blood
pressure or the surgeon can reduce the flow rate in the heart-lung machine. Different
methods for measurement of leakage have been used. The previously described method
with RISA is the most frequently used; however, a MEDLINE search to find any
articles calculating the correlation between systemic melphalan levels and leakage
in case of HILP with melphalan only, produced no results. The first report on TNF
levels after HILP with TNF, from Gérain et al. in 1992, demonstrated no significant
correlation between leakage and cytokine levels at any time, raising questions about
the value of the leakage measurement procedure.6
The aim of this study was to investigate whether or not the RISA leakage
measurements during HILP with TNF used in the Groningen University Hospital are
accurate in predicting systemic TNF levels. We observed a good correlation between
maximal systemic TNF levels and the maximum monitored leakage (r = 0.7114;
p < 0.0001). We were surprised to find that the correlation between maximal leakage
and maximal IL-6 concentration measured in the postoperative period was higher
than the correlation between maximal leakage and maximal TNF levels (r = 0.7737
versus r = 0.7114). IL-6 levels occurred in response to TNF, with a high correlation
between maximal levels of both cytokines (r = 8097). Stam et al. also found a strict
correlation between the degree of leakage estimated by isotope monitoring and the
Fig. 7 Absence of distant metastasis in
patients with grade II or III soft tissue sar-
coma. No significant difference was found
between the >2% leakage group and the
≤2% leakage group
119
Leakage during isolated limb perfusion with TNF
measured maximal systemic TNF levels in the same treatment setting (r = 0.7886,
p=0.0067; calculation based on their data).22 They also found a sharper relation
between systemic IL-6 curves and duration of exposure to high TNF levels in patients
with high leakage compared with a group of patients with no leakage. A significant
difference in leakage was found between the iliac/femoral perfusion levels and
popliteal perfusion level. This corresponds with the study of Klaase et al., who assessed
six variables for their influence on systemic leakage. The level of isolation and the
diameter of the venous cannula emerged as significant factors.23 In our study we
could not find a significant role for the diameter of the venous cannula (data not
shown). The importance of the perfusion level could be partly explained by the
different type of isolation technique used, namely, a rubber band tourniquet at the
iliacal level versus a inflatable pressure regulated band at the popliteal level.
In the analysis of our data, we distinguished two leakage groups, with a cutoff point
at 2%. Two percent represents approximately the measurement fault of the RISA
procedure. TNF levels in the perfusion circuit were about 7000 ng/ml, approximately
50-times higher than peak systemic levels. A significantly lower concentration of
TNF in the perfused limb in patients with >2% leakage was demonstrated resulting
in a decreased AUC, indicating an 18.7% lower exposure of the perfused limb to
TNF in the >2% leakage group. This decrease in TNF exposure, however, did not
result in a significant reduction of tumor response between the groups. This result
supports the initiation of TNF dose reduction studies. Thom et al. observed the same
decreased TNF perfusion circuit levels in patients with ≥1% leakage.24 The Rotterdam
perfusion group did not demonstrate a significant difference in perfusion circuit TNF
levels between a high and low-leakage group, possibly because of a limited number
of samples available.22
TNF levels in the systemic circulation of the patients were approximetely 100 ng/ml
in the >2% leakage group at the end of perfusion, compared with 10 ng/ml in the
≤2% leakage group. In patients with ≤2% leakage, systemic TNF exposure was 18.1
times less as calculated by the AUC. On the basis of the hypothesis that micro
metastatic disease is attacked by the leaked TNF and melphalan, a higher systemical
exposure of TNF could have its effect on the occurence of distant metastasis during
follow-up. However, subanalysis of the occurence of distant metastasis or survival
in a group of patients with grade II or III soft tissue sarcomas did not reveal this
phenomenon. IL-6, as one of the most important proinflammatory cytokines, appeared
in the systemic circulation 30 minutes after the start of the perfusion with maximum
levels reached 2 hours after HILP. CRP levels started to increase 6 hours after HILP
and reached its maximum 2 days after perfusion. A three wave pattern was seen; the
first wave caused by the systemically leaked TNF that generated a second wave of
120
Chapter 8
IL-6 some hours after perfusion, followed by a third wave of CRP that lasts for
several days.
TNF leakage was associated with a decrease in leucocyte and platelet count, with
significantly lower values in the >2% leakage group. Representing cytolytic liver
toxicity, a significantly hyperbilirubinemia, hypocholesterolemia and proteinemia
was observed in the >2% leakage group. A increase in the activity of the fraction of
LDH iso-enzymes 4 and 5 after perfusion was partly related to hepatotoxicity and
partly to muscle damage. No significant difference between both leakage groups
was found for creatine phosphokinase levels or myoglobin levels although both
parameters showed a significant rise after HILP. The same results were obtained by
Sorkin et al. who diminished TNF leakage after flow rate reduction during TNF
HILP.25 Analysis of our own flow data in relation to systemic leakage revealed a
weak negative correlation of r = -0.2910 with p = 0.0448 with a mean flow of 455 ±172 ml/min in our perfusions.
Like others, we also found a significant systemic TNF peak in patients with low
leakage after restoration of the circulation of the perfused limb.22,26 Despite a washout
procedure with 2 L of Isodex, TNF in the limb reaches the systemic circulation. A
corresponding rise in RISA was also observed.27 Therefore, today a more extensive
washout with 6 L and massage of the perfused limb is recommended in TNF perfusions
to reduce TNF release.
In a previous study we described the clinical features of HILP with TNF characterized
by a short- lived sepsis-like syndrome.28 This best called SIRS, was seen in all patients
and accompanied by fever, increase in cardiac output, a decrease in systemic vascular
resistance, and the need for fluid resuscitation and inotropes. Perfusion with melphalan
as the sole perfusion agent did not trigger these effects. Detailed analysis showed
positive correlations between maximum TNF concentrations and systemic vascular
resistance and cardiac index. The National Cancer Institute perfusion group
demonstrated the relation between the vascular response with the need for vasopressor
support and systemic TNF levels in patients with TNF leakage as well.24 Lejeune
also demonstrated severe toxicity in patients with leaks of >5%.4,6 Vrouwenraets et
al. reported an absence of severe systemic toxicity of TNF in patients without systemic
leakage.26 Stam et al. observed only a mild postoperative toxicity in the event of
significant leakage during perfusion.22 This was easily managed on the intensive
care unit with fluid substitution and, in some cases, vasopressors. On the basis of
their data, they rightly plead for renewed study of the potential use of TNF
systemically. Currently, SIRS is only seldom seen since the majority of the institutions
performing HILP with TNF and melphalan are experienced and are using a more
extensive washout procedure. One could ask oneself if leakage measurements during
121
Leakage during isolated limb perfusion with TNF
HILP are still worthwhile when side effects of TNF leakage are so easily dealt with.
In this study we demonstrated a good correlation between RISA leakage measurement
and TNF exposure during and after HILP with TNF and melphalan. RISA leakage
measurement serves as a good guide for the effectiveness of isolation during perfusion.
If leakage exceeds the 2% limit during perfusion, less exposure of the tumor bearing
limb to TNF, an increased exposure of the patient’s systemic circulation to TNF, and
more systemic side effects can be expected. Because leakage >2% did not influence
the tumor response, further dose-reduction studies of TNF in the HILP setting are
warranted.
122
Chapter 8
References
1 Creech O, Krementz ET, Ryan RF, Winblad JN. Chemotherapy of cancer: regional
perfusion utilizing an extra-corporeal circuit. Ann Surg 1958; 148: 616-632.
2 Stehlin JS. Hyperthermic perfusion with chemotherapy for cancers of the extremities.
Surg Gynecol Obstet 1969; 129: 305-308.
3 Schraffordt Koops H, Vaglini M, Suciu S, Kroon BB, Thompson JF, Gohl J, et al.
Prophylactic isolated limb perfusion for localized, high-risk limb melanoma: results
of a multicenter randomized phase III trial. European Organization for Research
and Treatment of Cancer Malignant Melanoma Cooperative Group Protocol 18832,
the World Health Organization Melanoma Program Trial 15, and the North American