University of Groningen Early onset sepsis in Suriname Zonneveld, Rens IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2017 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Zonneveld, R. (2017). Early onset sepsis in Suriname: Epidemiology, Pathophysiology and Novel Diagnostic Concepts. Rijksuniversiteit Groningen. Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license. More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne- amendment. Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 08-01-2022
Transcript
University of Groningen
Early onset sepsis in SurinameZonneveld, Rens
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2017
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Zonneveld, R. (2017). Early onset sepsis in Suriname: Epidemiology, Pathophysiology and NovelDiagnostic Concepts. Rijksuniversiteit Groningen.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license.More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne-amendment.
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means
without permission of the author.
Financial support for the research in this thesis is greatly acknowledged. The following institutes and organisations provided
funding for completion and printing of this thesis:
Stichting ‘De Drie Lichten’.
Early Onset Sepsis in Suriname
Epidemiology, Pathophysiology, and Novel Diagnostic Concepts
Proefschrift
ter verkrijging van de graad van doctor aan de Rijksuniversiteit Groningen
op gezag van de rector magnificus prof. dr. E. Sterken
en volgens besluit van het College voor Promoties.
De openbare verdediging zal plaatsvinden op
maandag 11 december 2017 om 16.15 uur
door
Rens Zonneveld
geboren op 8 april 1983 te Breda
Early Onset Sepsis in Suriname
Epidemiology, Pathophysiology, and Novel Diagnostic Concepts
Proefschrift
ter verkrijging van de graad van doctor aan de Rijksuniversiteit Groningen
op gezag van de rector magnificus prof. dr. E. Sterken
en volgens besluit van het College voor Promoties.
De openbare verdediging zal plaatsvinden op
maandag 11 december 2017 om 16.15 uur
door
Rens Zonneveld
geboren op 8 april 1983 te Breda
Promotor
Prof. dr. G. Molema
Copromotores
Dr. F.B. Plötz
Dr. M. van Meurs
Beoordelingscommissie
Prof. dr. J.M. Smit
Prof. dr. J.B. van Woensel
Prof. dr. J.G. Zijlstra
TABLE OF CONTENTSChapter 1 General Introduction and Thesis Outline 7
Part I Epidemiology of Early Onset Sepsis in Suriname 23
Chapter 2 Improved Referral and Survival of Newborns after Scaling Up of
Intensive Care in Suriname 27
BMC Pediatrics, Accepted for Publication
Part II Prediction of Early Onset Sepsis 47
Chapter 3 Association between Early Onset Sepsis Calculator and
Infection Parameters for Newborns with Suspected Early Onset Sepsis 51
J Clin Neonatol 2017, 6:159-62
Chapter 4 Immature-to-total-granulocyte Ratio as a Guide for Antibiotic Treatment in
Suspected Early Onset Sepsis in Surinamese Newborns 59
Submitted
Part III The Vascular Pathophysiology of Early Onset Sepsis 71
Chapter 5 Soluble Adhesion Molecules as Markers for Sepsis and the Potential
Pathophysiological Discrepancy in Neonates, Children and Adults 75
Critical Care 2014, 18:204
Chapter 6 Early Onset Sepsis in Surinamese Newborns is Not Associated with
Elevated Serum Levels of Endothelial Cell Adhesion Molecules and
Their Shedding Enzymes 99
Submitted
Chapter 7 Low Serum Angiopoietin-1, high Angiopoietin-2, and high Ang-2/Ang-1
Protein Ratio are Associated with Early Onset Sepsis in Surinamese Newborns 119
Shock 2017, May 22
Chapter 8 Analyzing Neutrophil Morphology, Mechanics, and Motility in Sepsis:
Options and Challenges for Novel Bedside Technologies 133
Critical Care Medicine 2016, 44:218-28
Chapter 9 Summary & Future Perspectives 157
Appendices 169
Appendix I Letter to the editor Critical Care (Critical Care 2016, 20:235-36.) 171
Appendix II Samenvatting (Summary in Dutch) 174
Appendix III Dankwoord 176
Appendix IV List of Publications 180
Appendix V Curriculum Vitae 182
Promotor
Prof. dr. G. Molema
Copromotores
Dr. F.B. Plötz
Dr. M. van Meurs
Beoordelingscommissie
Prof. dr. J.M. Smit
Prof. dr. J.B. van Woensel
Prof. dr. J.G. Zijlstra
1 General Introduction and Thesis Outline
GEN
ERA
L INTRO
DU
CTIO
N
9
1A COMMON CASE OF SUSPECTED EARLY ONSET SEPSIS IN SURINAMEA day prior to giving birth the mother had taken a boat from her village downstream the Suriname
River to the nearest mission post in Debike1. She had been pregnant for eight full moons. Her water
had broken a few days earlier, but the baby had not arrived yet. The friendly datra2 at the mission
post phoned somebody in the city of Paramaribo and spoke Bakratongo3. People in the village had
talked about the new at’oso4 for babies. Many women went there to give birth and they brought
her there too. After six hours she arrived and spent the night in a room with four other women.
She felt like she had korsu5.
Her daughter was born the next day and although she was crying loudly they still took her to
the baby hospital. Doctors and nurses were standing around a glass box that held her daughter.
The doctors seemed confused. One of the nurses spoke her tongo6 and explained that her baby
was doing fine but could have an infection. They had taken her daughter’s blood to see if it was
infected. Depending on her daughter’s condition and the test results they were going to decide
whether to continue the antibiotics they had started. The nurse said her daughter could suffer
from sepsis, wan takru siki fu brudu7.
In the next few days she spent many hours next to the glass box in the spacious baby room.
To her, her daughter seemed healthy and the same as her four earlier children. After three days,
the doctors used a nanai8 to take her brudu9 for the second time. The nurse told her the results
were fine. However, they were still going to finish her treatment with more antibiotics. Finally,
after a total of seven days they started their long journey home.
In this thesis, I focus on newborns admitted to the only neonatal intensive care unit (NICU) in
Suriname, which is located in Paramaribo, with a specific focus on dilemmas of Early Onset Sepsis –
from epidemiology and prediction towards changes in vascular endothelial integrity, principles of
leukocyte-endothelial interaction, and novel diagnostic methodologies for its timely recognition
or exclusion.
Rens Zonneveld, M.D.
July 2017
1 Village located along the Suriname River in the district Sipaliwini in the interior of Suriname.
Translated from the Surinamese language (Sranan Tongo)2 physician;3 Dutch;4 hospital;5 fever;6 language; 7 a serious infection of the blood;8 needle;9 blood.
GEN
ERA
L INTRO
DU
CTIO
N
10
1EARLY ONSET SEPSIS Early onset sepsis (EOS) is defined as onset of sepsis in newborns within 72 hours after birth [1]. When
intra-uterine infection is present, the fetus can become infected due to increased permeability of
the skin and mucosa for bacterial invasion. EOS is also caused by vertical transmission of pathogens
in the vaginal canal from mother to fetus during labor.
EOS is a leading cause of morbidity and mortality amongst newborns [1-6]. In Western (i.e.,
North American and European) countries incidence of blood culture proven EOS ranges from
0.01 to about 1.2 per 1000 live births. Incidence rates of EOS increase with decreasing gestational
age and birth weight, with the highest incidence (i.e., 26 per 1000 live births) and mortality (i.e.,
50-60% of blood culture proven cases) amongst infants with a birth weight below 1000 grams
(2-4). EOS is associated with colonization of the birth canal (about 30% of mothers in Western
countries) with Group B Streptococcus (GBS) [1]. In Western countries over 45% of all cases of
culture proven EOS GBS (45%) is the responsible pathogen, followed by Escherichia coli (E.coli)
(25%) (5,6). Other bacteria that cause EOS include Listeria Monocytogenes, gram-negative enteric
entero and herpes simplex virus) are also identified causes of EOS [1].
After the introduction of intrapartum antibiotics as prophylaxis for GBS, incidence of EOS has
decreased about 10-fold over the last 20 years in many Western countries and South Africa [7].
However, recent data indicates that, while incidence of EOS due to GBS is decreasing, incidence
of EOS with E.coli increases, probably due to altered resistance patterns of E.coli strains [1,5,8].
Additionally, GBS prevention approaches may have contributed to the rise of multi resistant gram-
positive strains, such as Methicillin resistant Staphylococcus aureus, as causes for EOS [1,9-11].
Maternal GBS vaccination to further reduce maternal GBS colonization and incidence of EOS, while
preventing antibiotic exposure, is currently under investigation [12].
EARLY ONSET SEPSIS IN THE NON-WESTERN WORLDStudies of EOS in low resource settings in the non-Western world are severely underrepresented
in the literature [13-16]. The vast majority of data on EOS are from upper-middle to high-income
countries in North America and Europe. Despite the lack of detailed data on EOS in the non-
Western world, there is a strong indication that over 90% of global neonatal deaths due to EOS
occurs in these low-to-middle income countries [17,18]. Large meta-analyses revealed incidence
of EOS in low-income countries at least similar to Western countries [13,15,16]. However, in these
analyses low-income countries represented only 5-10% of the total data leaving the true global
impact of EOS underestimated. Additionally, underdiagnosing (i.e., due to lack of resources and
logistic or financial constraints) and underreporting of EOS are common issues in low-resource
settings further enhancing underestimation of the true global impact of EOS [19,20]. Furthermore,
due to limited local availability of proper laboratory facilities, studies from these countries often
lack blood culture confirmed results. As a result, the spectrum of bacterial pathogens involved
in EOS in the non-Western world remains relatively unclear. More data on incidence, causative
organisms, morbidity and mortality from non-Western countries remain critical before proper
GEN
ERA
L INTRO
DU
CTIO
N
11
1prevention strategies and clinical management of suspected EOS can be achieved. Additionally,
since there is strong indication that incidence rates of culture proven EOS are substantially higher
in the non-Western world versus the Western world, studies from non-Western countries may
contribute immensely to our knowledge on basic and pathophysiological principles of EOS.
EARLY ONSET SEPSIS IN SURINAMESuriname is small developing country on the Northeastern corner of South America with
a multiethnic population of about 550,000 people [21]. About half of the population of Suriname
lives in its capital, the city of Paramaribo. Medical care is provided by four hospitals in Paramaribo,
namely the Academic Hospital Paramaribo, ‘s Lands Hospital, Diakonessen Hospital and St.
Vincentius Hospital, and the Streekziekenhuis in Nickerie. Suriname has an annual birth rate
of approximately 10,000 births. Over 90% of these births take place at the maternity wards of
the hospitals in Paramaribo. In rural parts of Suriname Medical Mission Posts provide primary
health care to the inhabitants, including basic obstetric care.
The earliest data on neonatal mortality in Suriname dates back to the detailed documentations
by Dr. Paul Christiaan Flu (1884 (Paramaribo, Suriname) - 1945 (Leiden, The Netherlands)) from
the early 20th century. In his seminal, yet forgotten, work Flu describes the poor socio-economic
circumstances after over three centuries of slavery and its effect on neonatal and pediatric care
and mortality rates [22]. Between 1900 and 1909, 9,259 live births were recorded of whom 474
died within the first 14 days of life, making a high average death rate of 51.2 per 1000 live births
for that age category. Over half (N=284) of these deaths were the result of pre- and dysmaturity,
yet about one third (N=110) of these deaths were from unknown cause and potentially following
neonatal infection.
Currently, neonatal death rate, defined as death within the first month of life, in Suriname has
decreased, but remains high with 12.9 per 1000 live births [23]. Early neonatal death (i.e., death
within the first 7 days of life) is estimated at 16 per 1000 live births [24]. Preliminary data from
the Suriname Perinatal and Infant Mortality Survey estimates contribution of infection to early
neonatal mortality at 24% (4 per 1000 live births) of all early neonatal deaths [23]. In contrast, in
The Netherlands incidence of EOS alone was 0.19 per 1000 live births in 2014 [25].
These numbers indicate a high burden of neonatal infection in Suriname. About 40 newborns
die each year of infection. Despite the overall idea of the impact of infectious disease in Surinamese
newborns, detailed information regarding incidence, type of infection (i.e., EOS versus LOS),
microbial causes, mortality and morbidity, antibiotic treatment (type and duration), and exact
epidemiological determinants are currently unavailable. In Chapter 2 of this thesis we explore
the epidemiology and outcomes of newborns admitted to Suriname’s neonatal care facility at
the Academic Hospital Paramaribo. This facility was established in 2008 and renewed in 2015 with
expansion of intensive care capacity, training of personnel and new equipment. For this chapter
we hypothesized that tertiary function and morbidity and mortality rates of treated newborns
would improve after the transition to the renewed neonatal care facility. Additionally, the impact
of EOS on mortality of Surinamese newborns is explored.
GEN
ERA
L INTRO
DU
CTIO
N
12
1EARLY ONSET SEPSIS: A DIAGNOSTIC AND THERAPEUTIC DILEMMAEOS can present with relatively mild symptoms resulting in late discovery with high risk for
mortality and morbidity. Furthermore, clinical symptoms of EOS are extremely diverse and difficult
to distinguish from physiologic symptoms of neonatal transition from intra-to-extrauterine life
and other non-infectious neonatal disease [3,9,26]. This complicates clinical decision-making on
start and duration of antibiotic treatment leading to significant overtreatment. For example, in
the European Union almost 8% of newborns are treated with antibiotics for suspected EOS, while
incidence rates of bacterial culture proven EOS range from 0.01 to 0.53 per 1000 live births in those
countries [3].
Blood culturing is considered the golden standard diagnostic test for EOS and takes several
days to become positive. Upon suspicion of EOS, newborns are observed and treated empirically
for EOS with antibiotics for at least 48 hours until results of blood culturing are known [1]. However,
blood cultures are only positive in 0.01 to 1.2 per 1000 live births in countries in the European
Union and North America. Contributing to this low prevalence may be false negativity due to low
yield of bacteria in low sample volumes or low-density bacteremia in general. Nonetheless, over
60% of newborns empirically treated with antibiotics for suspected EOS are treated for longer
than 72 hours even when blood cultures are negative [27]. Antibiotic stewardship is necessary to
reduce this overtreatment [28].
These dilemmas in the management of EOS pose a huge cost and socioeconomic threat,
especially in non-Western countries [1,6,16]. Moreover, it is becoming clear that prolonged
treatment of newborns with antibiotics also can negatively and severely impact early and
long-term neurodevelopment, growth, the developing immune system, and gut microbiome
resistance patterns [29-32].
CURRENT APPROACHES IN PREDICTION OF EARLY ONSET SEPSISSince clinical presentation and blood culturing have poor specificity for EOS, additional approaches
to aid clinical decision-making whether to start and/or continue antibiotic treatment have been
developed in the recent decade. Approaches that are commonly used in the clinic include maternal
risk factor stratification and serial measurement of C-reactive protein (CRP) levels and leukocyte
counts. Each of these has limitations in clinical utility, as will be discussed below.
Maternal Risk Factor Stratification
Maternal risk factors for EOS (i.e., presence and duration of prolonged rupture of the membranes,
intrapartum fever or administration of antibiotics, and presence of maternal GBS colonization,
as the most common cause of EOS in Western countries, have been used to predict presence of
EOS in newborns. In an attempt to overcome the problem of antibiotic overtreatment amongst
near and at term newborns with a gestational age equal or above 34 weeks, a risk stratification
strategy based on these factors and neonatal clinical findings has been developed in 2010 by
Escobar et al., which was revised in 2014 (33). This EOS calculator (available online at https://
GEN
ERA
L INTRO
DU
CTIO
N
13
1neonatalsepsiscalculator.kaiserpermanente.org) provides a quantitative estimation of EOS
risk along with a recommendation whether to start antibiotic treatment. Since its inception,
two retrospective studies revealed that application of the EOS calculator might help to reduce
antibiotic therapy with 50% (34,35). Additionally, the EOS calculator uses local incidence rates of
EOS as a variable, which still have to be established in many non-Western countries.
Correlation of results of the EOS calculator with biomarkers of inflammation in the newborn
may be helpful in further increasing its clinical utility. Therefore, the study in Chapter 3 explores
the relationship of results from the EOS calculator with results of serial measurement of CRP and
leukocyte counts in a cohort of Dutch near and at term newborns. For this study we hypothesized
that higher EOS calculator result, indicating higher risk for EOS, corresponds with an increase in
CRP and low leukocyte counts.
C-reactive Protein
CRP is an endogenous acute phase reactant synthesized by the liver upon infection [36]. Serum
CRP in newborns always represents endogenous synthesis since it passes the placenta in extremely
low quantities [37]. CRP is constitutively present in serum of newborns at very low concentrations
and its levels are dependent on gestational age and birth weight. CRP synthesis starts immediately
after an inflammatory stimulus by chemokines, such as interleukin (IL)-1, and IL-6, with serum
concentrations rising above the usual laboratory threshold of 5 mg/L after 6 hours and peaking
after 48 hours. This delayed synthesis results in poor sensitivity of CRP levels during early EOS.
In most practices, in the newborn suspected and treated with antibiotics for EOS, a repeat CRP
level below the laboratory threshold measured between 24 to 48 hours after start of antibiotics
has negative predictive value of 99% for EOS, yet only in case of a negative blood culture plus
a clinically improved newborn [37]. However, in clinical practice, despite this strong negative
value, the repeat CRP also leads to even more testing, culturing, and longer treatment duration
and hospital stay (38).
Leukocyte Counts
Inflammation and infection causes release of leukocytes from the bone marrow into the circulation.
Leukocyte counts (both total and subset, predominantly neutrophil, counts) have been widely
used to assess EOS [1,3]. However, both leukocyte and neutrophil counts lack specificity for
prediction of EOS [39,40]. Their numbers are dependent on many perinatal factors such as
gestational age, birth weight, type of delivery, and post partum age [41]. Neutropenia has shown
the most specificity for EOS [42]. However, as discussed above, due to low prevalence of positive
blood cultures, clinical decision-making on start and duration of antibiotic treatment is often
based on non-specific clinical symptoms and repeated measurement of CRP. Serial measurement
of low immature-to-total granulocyte (I/T) ratio has been showen to have a negative predictive
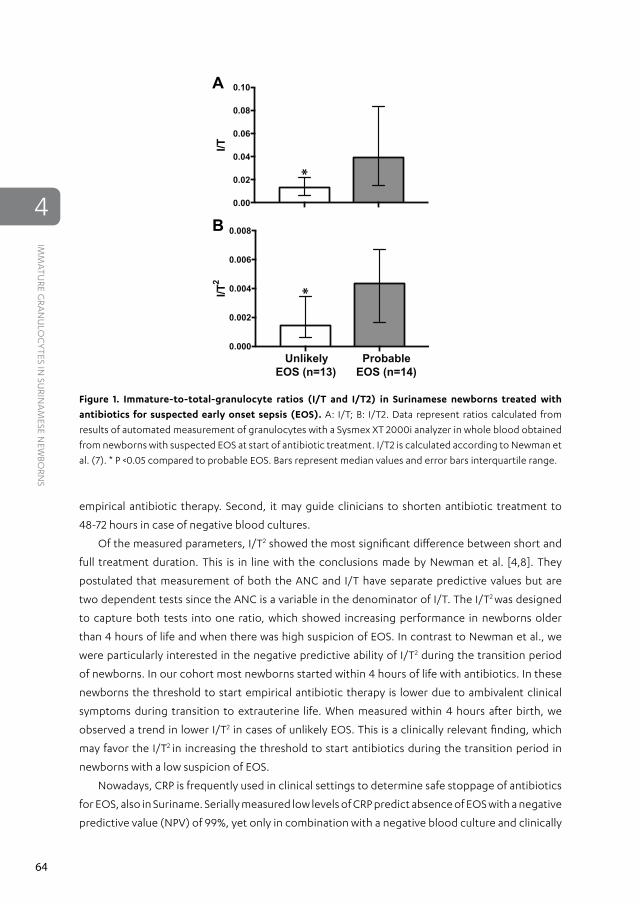
value for blood culture positive EOS of 99% [42]. Chapter 4 explores the relevance of a one-point
automated I/T ratio determination in prediction of duration of antibiotic therapy in a retrospective
cohort of Surinamese newborns with suspected EOS. For this study, we hypothesized that early
GEN
ERA
L INTRO
DU
CTIO
N
14
1establishment of a one-point low I/T ratio is associated with short duration of antibiotic treatment
in suspected EOS. This may prevent start of unnecessary antibiotic treatment, which may help to
reduce the antibiotic burden in developing countries.
EARLY ONSET SEPSIS: A NEED FOR NOVEL DIAGNOSTIC STRATEGIESThe approaches described above have been used for over 20 years and have remained virtually
unchanged. A recent international survey established that in practice only 31% of clinicians use
CRP levels and leukocyte counts as arguments for the decision to start antibiotics [43]. Many other
biomarkers have been investigated, but have not made it into the clinic for various reasons such as
poor specificity, short half lives of biomarkers, lack of reproducibility, or technical issues [44]. At
this point, serial measurement of procalcitonin, an acute phase reactant similar to CRP, is showing
promise in negative prediction of EOS and reduction of antibiotic treatment in Western countries
[45]. However, novel and practical approaches for early and prompt confirmation or exclusion of
EOS remain necessary to reduce antibiotic overtreatment, while improving outcomes. Elements
of the vascular pathophysiology may be relevant for development of these novel approaches,
which will be discussed below.
THE VASCULAR PATHOPHYSIOLOGY OF EARLY ONSET SEPSISThe diagnostic and therapeutic dilemmas of EOS occur, at least in part, because its pathophysiology
remains poorly understood. Endothelial inflammatory activation and leukocyte-endothelial
interactions are key processes in sepsis pathophysiology. Part 3 is aimed to provide more insight
into these processes in newborns to unravel aspects of EOS pathophysiology and provide novel
concepts for its timely diagnosis and management.
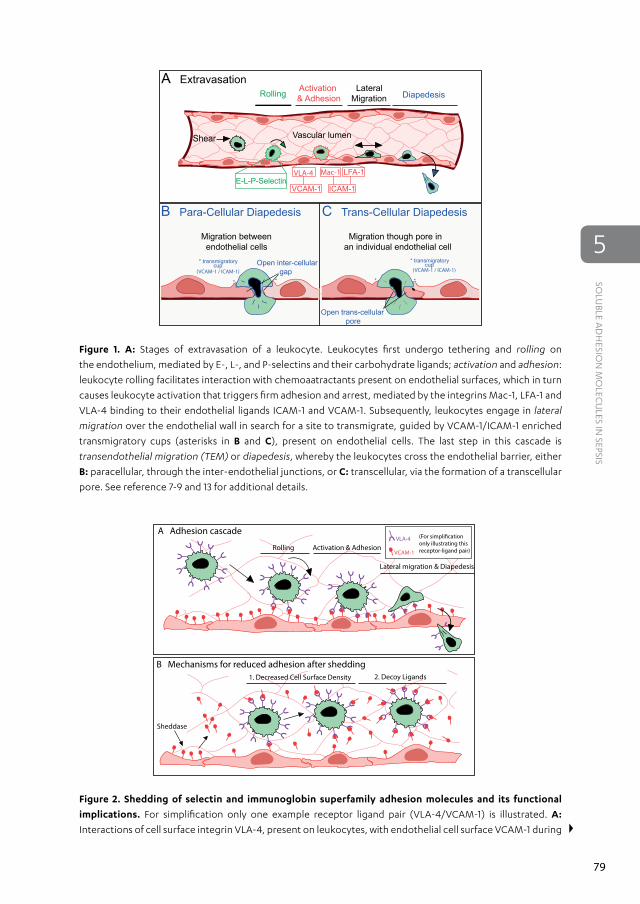
LEUKOCYTE-ENDOTHELIAL INTERACTIONS: SHEDDING OF ADHESION MOLECULES IN EARLY ONSET SEPSISLeukocyte-endothelial interactions are involved in any infectious pathophysiology [46]. A body
of evidence is indicating that aberrant leukocyte, mostly neutrophil, activation and recruitment
towards the endothelium plays a pivotal role in breakdown of the vascular endothelium, which, in
turn, is associated with organ failure and death [47,48]. Bacterial derived lipopolysaccharide (LPS)
drives release of cytokines, such as tumor necrosis-α and interleukins, known as the ‘cytokine storm’.
Additionally, the endothelium becomes activated and increased presence of LPS in the vasculature
is associated with increased expression of endothelial cell adhesion molecules (CAM) P-selectin,
and platelet and endothelial cell adhesion molecule-1 (PECAM-1) [49]. These adhesion molecules
orchestrate tethering, rolling and firm adhesion of leukocytes on and transmigration across
the endothelium [50]. During sepsis, soluble isoforms of adhesion molecules (sCAMs) accumulate
in the bloodstream due to shedding [51]. Shedding represents removal of CAMs from cell surfaces
GEN
ERA
L INTRO
DU
CTIO
N
15
1by enzymes called sheddases, in particular matrix metalloproteinase-9 (MMP-9) and neutrophil
elastase (NE), released from tertiary granules in neutrophils [51]. Both MMP-9 and NE prepare
the extracellular matrix underlying the endothelium to allow transmigration of leukocytes into
inflammatory sites. The activity of MMP-9 is tightly regulated by sheddase antagonist tissue-
inhibitor of metalloproteinases-1 (TIMP-1) to reduce damage to host-tissues and an increased
TIMP-1/MMP-9 ratio was associated with severity and outcome of sepsis in adults [52,53].
Chapter 5 reviews mechanisms for changes in levels of circulating adhesion molecules and their
sheddases during sepsis and age-dependency of their levels in newborns, children and adults.
For Chapter 6 we applied the concept of simultaneous measurement of circulating adhesion
molecules and their sheddases in a cohort of healthy newborns and newborns with suspected
EOS. We hypothesized that higher circulating levels of adhesion molecules sP-selectin, sE-selectin
sVCAM-1, sICAM-1 and sPECAM-1, coincide with higher levels of sheddases MMP-9 and NE, and
sheddase antagonist TIMP-1 in newborns with culture proven EOS versus healthy controls.
ENDOTHELIAL INTEGRITY DURING EARLY ONSET SEPSIS: THE ANGIOPOIETINSEndothelial integrity is maintained by the Angiopoietin/Tie2 Receptor Tyrosine Kinase - system,
which consists of the endothelial restricted receptor Tie-2 and its ligands Angiopoietin (Ang)-1
and Ang-2 [54]. In health, Ang-1 is present in human serum at higher levels than Ang-2 and
promotes endothelial stability through continuous endothelial Tie-2 receptor phosphorylation
[55]. Inflammation leads to higher circulating levels of Ang-2 that is being release from endothelial
cells. Circulating Ang-2 dose-dependently inhibits Tie-2 signaling and acts as an antagonist of Ang/
Tie-2, driving vascular permeability. Emerging clinical evidence indicates a positive correlation of
high Ang-2 levels, and subsequent high Ang-2/Ang-1 ratio with presence, severity, and outcome
of pediatric and adult sepsis [56,57]. It was recently suggested that the Angiopoietins may be
relevant as biomarkers of EOS [58]. Additionally, investigating the dynamics of Ang-1 and Ang-2
in healthy and infected newborns may unravel changes in their levels during EOS. In Chapter 7,
these changes are explored in a large cohort of healthy newborns and newborns with suspected
and culture proven EOS. For this study, we hypothesized that low Ang-1 and high Ang-2 levels are
associated with presence of bacterial culture positive EOS.
NOVEL ASPECTS OF NEUTROPHILS IN SEPSISManual microscopic analysis of neutrophils and their counts have been part of the clinical
assessment of bacterial infection for over a century [59]. However, manual analysis of counts
and morphology is time consuming, requires experienced laboratory technicians, and lacks
reproducibility. Novel methods allow for measurement of several aspects of neutrophils, in
particular morphology, mechanics and motility. Flow-based automated hematology analysers
(AHAs) are able to determine leukocyte subsets and different granulocyte fractions [42].
Additionally, recent developments in the performance of these AHAs have enabled measurement
of neutrophil size and scatter properties and determination of neutrophil cell surface markers with
GEN
ERA
L INTRO
DU
CTIO
N
16
1immunofluorescence, each with their own sensitivity for presence of sepsis in patients. Chapter 8
and Chapter 9 discuss basic and clinical aspects of neutrophil morphology, mechanics and motility
during sepsis, along with current evidence and future possibilities for the use of these parameters
into the management of sepsis.
GEN
ERA
L INTRO
DU
CTIO
N
17
1REFERENCES1. Simonson KA, Anderson-Berry AL, Delair SF,
Davies HD. Early-onset neonatal sepsis. Clin
Microbiol Rev 2014, 27(1):21-47.
2. Schrag SJ, Farley MM, Petit S, Reingold A, Weston
bedside review: Angiopoietin signalling in critical
illness - a future target? Crit Care 2009, 13(2):207.
55. Parikh SM. Dysregulation of
the angiopoietin-Tie-2 axis in sepsis and ARDS.
Virulence 2013, 4(6):517-24.
56. Fang Y, Li C, Shao R, Yu H, Zhang Q, Zhao L.
Prognostic significance of the angiopoietin-2/
angiopoietin-1 and angiopoietin-1/Tie-2 ratios
for early sepsis in an emergency department.
Crit Care 2015, 14(19):367.
57. Mussap M, Cibecchini F, Noto A, Fanos V. In search
of biomarkers for diagnosing and managing
neonatal sepsis: the role of angiopoietins. J
Matern Fetal Neonatal Med 2013, 26(2):24-6.
58. Giuliano JS Jr, Tran K, Li FY, Shabanova V,
Tala JA, Bhandari V. The temporal kinetics of
circulating angiopoietin levels in children with
sepsis. Pediatr Crit Care Med 2014, 15(1):e1-8.
59. Cornbleet PJ. Clinical utility of the band count.
Clin Lab Med 2002, 22(1):101-36.
I Epidemiology of Early Onset Sepsis in Suriname
2 Improved Referral and Survival of Newborns after Scaling Up of
Intensive Care in Suriname
Rens Zonneveld, Natanael Holband, Anna Bertolini, Francesca Bardi, Neirude Lissone, Peter Dijk,
Frans B. Plötz, Amadu Juliana
BMC Pediatrics, Accepted for Publication
NEO
NA
TAL IN
TENSIV
E CA
RE IN SU
RINA
ME
28
2
ABSTRACTBackground
Scaling up neonatal care facilities in developing countries can improve survival of newborns.
Recently, the only tertiary neonatal care facility in Suriname transitioned to a modern environment
in which interventions to improve intensive care were performed. This study evaluates impact of
this transition on referral pattern and outcomes of newborns.
Methods
A retrospective chart study amongst newborns admitted to the facility was performed and
outcomes of newborns between two 9-month periods before and after the transition in March
2015 were compared.
Results
After the transition more intensive care was delivered (RR 1.23; 95% CI 1.07-1.42) and more outborn
newborns were treated (RR 2.02; 95% CI 1.39-2.95) with similar birth weight in both periods (P=0.16).
Mortality of inborn and outborn newborns was reduced (RR 0.62; 95% CI 0.41-0.94), along with
mortality of sepsis (RR 0.37; 95% CI 0.17-0.81) and asphyxia (RR 0.21; 95% CI 0.51-0.87). Mortality
of newborns with a birth weight <1000 grams (34.8%; RR 0.90; 95% CI 0.43-1.90) and incidence
of sepsis (38.8%, 95% CI 33.3-44.6) and necrotizing enterocolitis (NEC) (12.5%, 95% CI 6.2-23.6)
remained high after the transition.
Conclusions
After scaling up intensive care at our neonatal care facility more outborn newborns were admitted
and survival improved for both in- and outborn newborns. Challenges ahead are sustainability,
further improvement of tertiary function, and prevention of NEC and sepsis.
NEO
NA
TAL IN
TENSIV
E CA
RE IN SU
RINA
ME
29
2
BACKGROUNDNeonatal mortality in developing countries continues to be a chief global health challenge [1,2].
A recent global report indicates that over 40% reduction of neonatal mortality can be achieved
by implementation of institutional care in lower resource countries [3]. In particular, local or
regional neonatal care facilities with integrated availability of perinatal and neonatal intensive
care can reduce mortality [4]. For example, newborns born in a rural hospital featuring a neonatal
intensive care unit (NICU) in Uganda were almost twice as likely to survive than those born outside
[5]. Moreover, introduction of a neonatal care facility in a low-income district in India reduced
neonatal mortality rate (NMR) by 21% after the first two years [6]. Improving interventions within
existing neonatal care facilities (e.g., training of personnel, refurbishment, infection prevention)
can improve mortality and enhance tertiary function for newborns in need of intensive care [6-9].
In Suriname NMR in 2009 was 16.0 per 1000 live births. However, detailed data on demographics
and outcomes of newborns are lacking. In 2008 the neonatal care facility at the Academic Hospital
Paramaribo (AHP), which also incorporated the first and only NICU in Suriname, opened its doors.
The ability to treat premature and critically ill newborns was an important step towards reducing
mortality. At the end of March 2015 the facility moved to a new and modern environment. This
transition solidified availability of neonatal intensive care in Suriname with reinforcement and
training of personnel, new equipment, continuous availability of supplies, and protocol-based
care. Since this facility is the only referral center for newborns requiring intensive care in Suriname,
morbidity and mortality of newborns treated here reflect their outcomes at the national level.
Therefore, as a benchmark for future investigations, we developed a registry to describe
demographics and outcomes of newborns admitted to the neonatal care facility. Additionally, to
evaluate the impact of improvements we compare referral pattern, mortality and morbidity of
newborns treated in periods before and after the transition. Ultimately, this could lead to better
prospective registry and care for critically ill newborns in Suriname.
METHODSStudy Design
We performed a retrospective (pre-and post transition) study in the neonatal care facility of
the AHP during the periods July 1st 2014 to March 29th 2015 (Period 1) and March 31st to December
31st 2015 (Period 2). The impact of the transition was described by analyzing demographics and
outcomes of all inborn and outborn newborns admitted within these two periods. Excluded were
newborns whom were treated in both periods and of whom insufficient information (i.e., no or
incomplete paper charts) was available to confirm outcomes. We received a waiver from our
institutional ethical board.
Setting and Interventions
Suriname is a small middle-income country with a multiethnic society and has an annual birth rate
of about 10,000 births. Over 90% of births take place at delivery rooms of one of four hospitals
situated in Suriname’s capital Paramaribo (inhabited by more than half of Suriname’s population).
NEO
NA
TAL IN
TENSIV
E CA
RE IN SU
RINA
ME
30
2
About 30% of births take place at the delivery room of the AHP. The neonatal care facility at
the AHP serves as the only referral hospital for critically ill newborns. Since the opening in 2008,
between 350-400 newborns are treated each year in one room with 12 beds, with NICU capacity
operating at Level III [9]. Newborns are generally only actively treated with a birth weight (BW) ≥
750 grams and/or gestational age (GA) ≥ 27 weeks.
On March 30th 2015 the facility moved to a completely new, modern and spacious environment
with central climate control and new equipment (i.e., ventilators, incubators, air-humidifiers,
ultrasound machines and multi-parameter monitors). Capacity for mechanical ventilation and
continuous positive airway pressure (CPAP) was doubled. The NICU (6 beds), high care (HC)
(6 beds), and medium care (MC) (4 beds) capacity in the new facility remained the same until
February 2016 (when a separate space for the MC was opened and the NICU capacity increased to
10 beds).
Total expense for the new building and equipment was 2.6 million US dollars. Funds were
collected from kind donations from governmental and private organizations and from Surinamese
companies. Since there were no architects or contractors available within Suriname with experience
in designing a NICU level neonatal care facility, we relied on guidelines from developed countries
and local creativity and practical experience to realize the project within budget, without the need
for expensive consultants. For example, one of the savings came from using venturi mechanism
based suction devices powered by compressed air, avoiding the need for a separate central
vacuum system.
Admission criteria remained the same. Obstetric nurses were trained in neonatal life support
and the number of residents in the obstetric and pediatric department was increased. For both
day and evening shifts a separate resident was assigned to the NICU exclusively. Shortly before
the transition, nurses were trained in intensive neonatal care and their number was expanded
to 1 per 3 or 4 beds. New charts for vital signs, ventilation settings, and fluid management were
implemented. A breast-feeding and nutrition program was started to help reduce cases of
necrotizing enterocolitis (NEC) and mothers were allowed at the bedside twice as long as before.
Systematic infection prevention (i.e., stringent guidelines and more facilities for hand washing,
providing of patient specific (disposable) materials, Extended Spectrum Beta-Lactamase (ESBL)
outbreak control) was enforced.
Data Collection and Analysis
Data were collected from paper medical records on maternal, obstetric and perinatal history,
birth location, reason for admission, hospital course, and outcomes. A single major cause of death
was determined. For each included newborn we determined the highest level of care during
their stay by assigning criteria for NICU, HC or MC retrospectively according to local protocol
(Supplemental Table 1). Primary outcome was mortality: NMR at the AHP and at the neonatal care
facility divided in early (i.e., in-hospital death before 7 days of life) and late (i.e., in-hospital death
of at term newborns after 7 days of life), GA-specific mortality, BW-specific mortality, and cause-
specific mortality. Secondary outcomes were highest level of care, respiratory treatments (CPAP,
mechanical ventilation, surfactant), use of antibiotics, development of respiratory complications,
NEO
NA
TAL IN
TENSIV
E CA
RE IN SU
RINA
ME
31
2
i.e., pneumothorax, bronchopulmonary dysplasia (BPD; i.e., oxygen dependence > 28 days of age),
ventilator-associated pneumonia (VAP; i.e., positive tracheal aspirate culture after ventilation),
development of NEC and sepsis (i.e., early (<72 hours after birth) and late (>72 hours after birth)
onset clinical (i.e., clinical suspicion, treated with antibiotics for 7 days, raised c-reactive protein
levels)) and blood culture positive sepsis, blood and ESBL culture results, and duration of stay.
Statistical Analysis
Incidence rates and epidemiological determinants were calculated for the inclusion period.
Categorical variables are presented as numbers and percentages with 95% confidence intervals
(CI) and continuous variables as means with standard deviations (SD) or, if not normally distributed,
as medians with ranges. Continuous variables were compared with a student t-test and categorical
variables were compared with Chi-Square. Relative risk (RR) and 95% CI were calculated.
P-values < 0.05 were considered statistically significant.
RESULTSDemographics and Referral
A total of 626 newborns were treated at the neonatal care facility of whom 601 (320 before and
281 after the transition) were included (Table 1). Overall demographics were comparable between
both periods, with similar percentages of missing data, showing high prevalence of (antenatal) risk
factors for mortality and morbidity (Table 1). In period 2 significantly more outborn newborns (RR
2.02; 95% CI 1.39-2.95; P<0.001) were treated with similar mean birthweight (2183 ± 845 grams vs.
1915 ± 990 grams; P=0.16). Prematurity was the main reason for admission for all inborn (48.3%; 95%
CI 44.0-52.7) and outborn (66.0%; 95% CI 56.3-74.5) newborns, followed by respiratory distress and
suspected infection (Table 1).
Mortality
NMR of inborn newborns born at the AHP was lower in period 2 (P=0.02) (Table 2). After
the transition, reduction in mortality was greatest in newborns treated at NICU level care (P<0.01),
with a GA above 28 weeks (RR 0.42; 95% CI 0.25-0.72; P=0.002), and outborn newborns (P=0.02).
A trend in decrease in mortality was observed in late mortality (P=0.06), inborn newborns (P=0.07),
and in newborns with a birth weight (BW) above 1500 grams (P=0.07). A significant reduction in
mortality was observed in cases of sepsis (P=0.01) and perinatal asphyxia (P=0.03). Sepsis was
the main cause of death in period 1 (34.5%; 95% CI 23.4-47.7), and second in period 2 (26.7%; 95%
CI 14.2-44.4). For newborns with a BW<1000 grams late-onset sepsis was the main cause of death
in both periods (44.8%; 95% CI 28.4-62.5).
Treatments and Morbidity
Based on our criteria (Supplemental Table 1) significantly more NICU level care was given in
period 2 (P<0.01) (Table 3a). More mechanical ventilation and surfactant were applied after
the transition. No difference in prevalence of VAP or pneumothorax was observed and there was
NEO
NA
TAL IN
TENSIV
E CA
RE IN SU
RINA
ME
32
2
Table 1. Demographics of newborns admitted to the neonatal care facility before and after the transition
Period 1
(July 2014-March 2015)
Period 2
(April 2015-December 2015)
N % (95% CI) N % (95% CI)
Live births Total at AHP 2353 1972
Admissions to
facility
Total
Included
Inborn
Outborn2
331
320
284
36
96.7
88.7 (84.8-91.8)
11.3 (8.2-15.2)
295
281
217
64
95.3
77.2 (72.0-81.7)
22.8 (18.3-28.0)
Maternal age
(Years)
<20
20-34
≥35
Missing
54
168
46
52
16.9 (13.2-21.4)
52.5 (47.0-57.9)
14.4 (11.0-18.6)
16.3
36
140
24
81
12.8 (9.4-17.2)
49.8 (44.0-55.6)
8.5 (5.8-12.4)
28.8
Pregnancy HIV
Diabetes
PIH / Preeclampsia
Antenatal steroids3
Infection risk4
6
18
60
47
47
1.9 (0.9-4.0)
5.6 (3.6-8.7)
18.8 (14.9-23.4)
14.7 (11.2-19.0)
14.7 (11.2-19.0)
2
20
62
55
38
0.7 (0.2-2.6)
7.1 (4.7-10.7)
22.1 (17.6-27.3)
19.6 (15.4-24.6)
13.5 (10.0-18.0)
Mode of delivery Vaginal
Caesarean section
Missing
187
105
28
58.4 (53.0-63.7)
32.8 (27.9-38.1)
8.8
167
94
20
59.4 (53.6-65.0)
33.5 (28.2-39.2)
7.1
Sex Male
Female
162
158
50.6 (45.2-56.1)
49.4 (43.9-54.8)
155
126
55.2 (49.3-60.9)
44.8 (39.1-50.7)
Gestational age
(Weeks)
<28
28-32
33-36
≥37
Missing
16
48
114
132
10
5.0 (3.1-8.0)
15.0 (11.5-19.3)
35.6 (30.6-41.0)
41.3 (36.0-46.7)
3.1
13
47
100
110
11
4.6 (2.7-7.8)
16.7 (12.8-21.5)
35.6 (30.2-41.3)
39.1 (33.6-45.0)
3.9
Birth weight
(Grams)
<1000
≥1000-1499
≥1500
Missing
26
48
242
4
8.1 (5.6-11.6)
15.0 (11.5-19.3)
75.6 (70.6-80.0)
1.3
23
33
221
4
8.2 (5.5-12.0)
11.7 (8.5-16.0)
78.6 (73.5-83.0)
1.4
Apgar Score at 5’ <5
Missing
24
45
7.5 (5.1-10.9)
14.1
7
47
2.5 (1.2-5.1)
16.7 (12.8-21.5)
NEO
NA
TAL IN
TENSIV
E CA
RE IN SU
RINA
ME
33
2
a trend in increases incidence of BPD (P=0.07) (Table 3b). Grade 2 or higher NEC was present at
high incidence in newborns with a BW<1500 grams in both periods (5.4% and 12.5%, respectively).
Sepsis (either early or late-onset) was prevalent in over 30% of patients in both periods, of which
half was LOS. During both periods, outbreaks with ESBL bacteria led to a significant prevalence of
ESBL positive cultures.
Table 1. (continued)
Period 1
(July 2014-March 2015)
Period 2
(April 2015-December 2015)
N % (95% CI) N % (95% CI)
Ethnicity Maroon
Creole
Hindo-Surinamese
Javanese
Amerindian
Chinese
Other5
Missing
87
85
59
15
10
2
31
31
27.2 (22.6-32.3)
26.2 (22.0-31.7)
18.4 (14.6-23.1)
4.7 (2.9-7.6)
3.1 (1.7-5.7)
0.6 (0.2-2.2)
9.7 (6.9-13.4)
9.7
72
72
55
21
7
2
32
20
25.6 (20.9-31.0)
25.6 (20.9-31.0)
19.6 (15.4-24.6)
7.5 (4.9-11.2)
2.5 (1.2-5.1)
0.7 (0.2-2.6)
11.4 (8.2-15.6)
7.1
Initial reason for
admission1
Prematurity
Respiratory distress6
Suspected infection7
Perinatal asphyxia8
Congenital malformations9
Other10
152
119
91
39
42
71
47.5 (42.1-53.0)
37.2 (32.1-42.6)
28.4 (23.8-33.6)
12.2 (9.0-16.2)
13.1 (9.9-17.3)
22.2 (18.0-27.1)
148
122
97
30
35
49
52.7 (46.8-58.4)
43.4 (37.7-49.3)
34.5 (29.2-40.3)
10.7 (7.6-14.8)
12.5 (9.1-16.8)
17.4 (13.4-22.3)
AHP = Academic Hospital Paramaribo; NICU = neonatal intensive care unit; HC = high care; MC = medium care; PIH =
pregnancy-induced hypertension; RDS = respiratory distress syndrome. 1 Newborns could have more than one reason for admission.2 Includes: delivery rooms of four other hospitals in Paramaribo and one other hospital in Nickerie, birth clinics in rural and
interior parts of Suriname, and home births.3Administered in two doses of dexamethasone in the case of suspected premature birth before GA of 34 weeks.4 Includes: premature rupture of membranes (PROM), intrapartum fever and/or antibiotics, positive maternal Group-B
meconium aspiration syndrome, and transient neonatal tachypnea.7 Includes: newborns defined with clinical symptoms of infection by admitting physician.8 Includes: asphyxia defined by admitting physician (e.g., in the case of either need for resuscitation or Apgar <5 beyond
5 minutes; lactate acidosis with base excess <16; coma or seizures after birth; findings with cerebral ultrasound such
as edema).9 Includes: diaphragmatic hernia, congenital heart defects, gastro-intestinal anomalies and neurological malformations.10 Includes: hypoglycemia, dysmaturity, jaundice, and social indications.
NEO
NA
TAL IN
TENSIV
E CA
RE IN SU
RINA
ME
34
2
Tab
le 2
. Mo
rtal
ity
of n
ewb
orn
s tr
eate
d at
the
faci
lity
bef
ore
and
aft
er th
e tr
ansi
tio
n Peri
od
1 (
N=3
20)
(Jul
y 20
14-M
arch
20
15)
Peri
od
2 (
N=2
81)
(Ap
ril 2
015
-Dec
emb
er 2
015
)
Rel
ativ
e R
isk
(95%
CI)
P-va
lue
N%
N%
Ove
rall
mo
rtal
ity
Tota
l at
AH
P (p
er 10
00
live
bir
ths)
1
Tota
l at
faci
lity
To
tal e
arly
neo
nata
l mo
rtal
ity
To
tal l
ate
neo
nata
l mo
rtal
ity
In
bo
rn
O
utb
orn
N
ewb
orn
s w
ith
NIC
U le
vel c
are
23.4
55/3
20
29/3
20
26/3
20
42/2
84
13/3
6
52/1
59
17.2
9.1
8.1
14.8
36.1
32.7
13.2
30/2
81
18/2
81
12/2
81
20/2
17
10/6
4
29/1
72
10.7
6.4
4.3
9.2
15.6
16.9
0.5
6 (0
.36-
0.9
0)
0.6
2 (0
.41-
0.9
4)
0.7
0 (
0.4
0-1
.24)
0.5
3 (0
.27-
1.0
2)
0.6
2 (0
.38-
1.0
3)
0.4
3 (0
.21-
0.8
9)
0.5
2 (0
.35-
0.7
7)
0.0
2
0.0
2
0.2
3
0.0
6
0.0
7
0.0
2
<0.0
1
Ges
tati
ona
l age
-sp
ecifi
c
mo
rtal
ity
<28
wee
ks
28-3
2 w
eeks
33-3
6 w
eeks
≥37
wee
ks
Mis
sing
6/16
12/4
8
14/1
14
20/1
32
3
37.5
25.0
12.3
15.2
8/13
5/47
4/10
0
8/11
0
5
61.5
10.6
4.0
7.3
1.64
(0
.76-
3.53
)
0.4
3 (0
.16-1
.11)
0.3
3 (0
.11-0
.96)
0.4
8 (0
.22-
1.0
5)
0.2
0
0.0
8
0.0
4
0.0
7
Birt
h w
eigh
t-sp
ecifi
c m
ort
alit
y<1
00
0 g
≥10
00
-14
99 g
≥150
0 g
M
issi
ng
10/2
6
13/4
8
30/2
42
2
38.5
27.1
12.4
8/23
6/33
16/2
21
0
34.8
18.2
7.2
0.9
0 (
0.4
3-1.9
0)
0.6
7 (0
.28-
1.59
)
0.5
8 (0
.33-
1.0
4)
0.7
9
0.3
6
0.0
7
NEO
NA
TAL IN
TENSIV
E CA
RE IN SU
RINA
ME
35
2
Tab
le 2
. (co
ntiu
ed)
Peri
od
1 (
N=3
20)
(Jul
y 20
14-M
arch
20
15)
Peri
od
2 (
N=2
81)
(Ap
ril 2
015
-Dec
emb
er 2
015
)
Rel
ativ
e R
isk
(95%
CI)
P-va
lue
Cau
se-s
pec
ific
mo
rtal
ity
Seps
is2
Ea
rly-
ons
et s
epsi
s
La
te-o
nset
sep
sis
Peri
nata
l asp
hyxi
a
Prem
atur
ity
com
plic
atio
n3
Co
ngen
ital
mal
form
atio
ns4
Oth
er5
19/9
6
10/4
4
9/52
12/3
8
7/15
7
12/4
2
5
19.8
22.7
17.3
31.6
4.5
28.6
8/10
9
3/59
5/50
2/30
5/14
8
9/35
6
7.3
5.1
10.0
6.7
3.4
25.7
0.3
7 (0
.17-0
.81)
0.2
2 (0
.07-
0.7
7)
0.5
8 (0
.21-
1.61
)
0.2
1 (0
.51-
0.8
7)
0.7
6 (0
.25-
2.34
)
0.9
0 (
0.4
3-1.
88)
0.0
1
0.0
2
0.2
9
0.0
3
0.6
3
0.7
8
AH
P =
Aca
dem
ic H
osp
ital
Par
amar
ibo
; NIC
U =
neo
nata
l int
ensi
ve c
are
unit
;1 In
clud
ing
dea
ths
at t
he d
eliv
ery
roo
m (
13 b
efo
re a
nd 6
aft
er t
he t
rans
itio
n).
2 In
clud
es: n
ewb
orn
s w
ith
clin
ical
sus
pici
on,
tre
ated
wit
h an
tibi
oti
cs fo
r 7
day
s, r
aise
d c
-rea
ctiv
e pr
ote
in le
vels
, and
po
siti
ve b
loo
d c
ultu
re.
3 In
clud
es: r
espi
rato
ry in
suffi
cien
cy o
r pn
eum
oth
ora
x w
ith
RDS
and
ext
rem
e pr
emat
urit
y, n
ecro
tizi
ng e
nter
oco
litis
; int
rave
ntri
cula
r he
mo
rrha
ge.
4 In
clud
es: d
iaph
ragm
atic
her
nia,
co
ngen
ital
hea
rt d
efec
ts, g
astr
o-i
ntes
tina
l ano
mal
ies
and
neu
rolo
gica
l mal
form
atio
n.5 In
clud
es: p
ersi
sten
t pu
lmo
nary
hyp
erte
nsio
n o
f the
neo
nate
(PP
HN
), p
neum
oth
ora
x, c
ard
iac
tam
po
nad
e, a
nd k
erni
cter
us.
NEO
NA
TAL IN
TENSIV
E CA
RE IN SU
RINA
ME
36
2
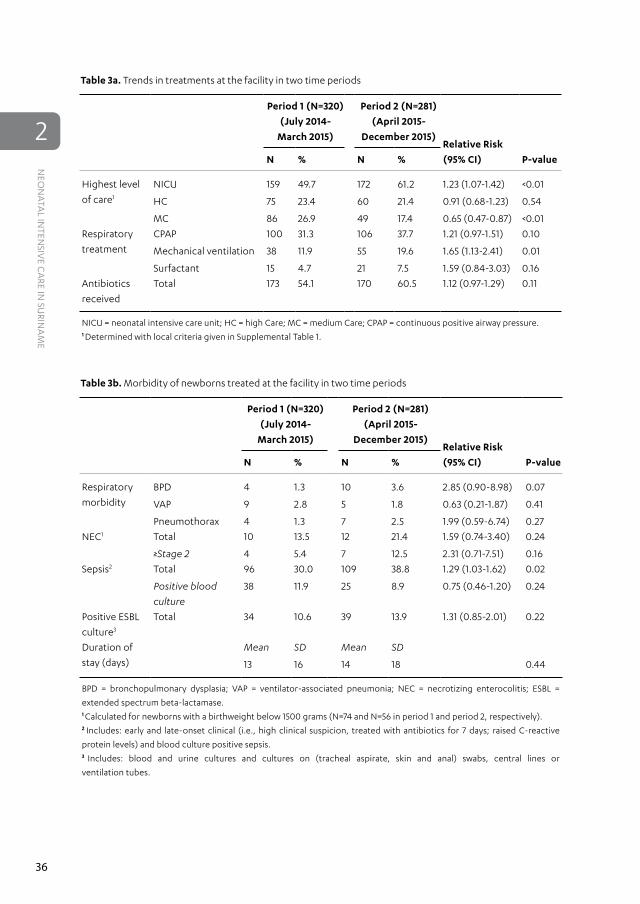
Table 3a. Trends in treatments at the facility in two time periods
Period 1 (N=320)
(July 2014-
March 2015)
Period 2 (N=281)
(April 2015-
December 2015)Relative Risk
(95% CI) P-valueN % N %
Highest level
of care1
NICU
HC
MC
159
75
86
49.7
23.4
26.9
172
60
49
61.2
21.4
17.4
1.23 (1.07-1.42)
0.91 (0.68-1.23)
0.65 (0.47-0.87)
<0.01
0.54
<0.01
Respiratory
treatment
CPAP
Mechanical ventilation
Surfactant
100
38
15
31.3
11.9
4.7
106
55
21
37.7
19.6
7.5
1.21 (0.97-1.51)
1.65 (1.13-2.41)
1.59 (0.84-3.03)
0.10
0.01
0.16
Antibiotics
received
Total 173 54.1 170 60.5 1.12 (0.97-1.29) 0.11
NICU = neonatal intensive care unit; HC = high Care; MC = medium Care; CPAP = continuous positive airway pressure.1 Determined with local criteria given in Supplemental Table 1.
Table 3b. Morbidity of newborns treated at the facility in two time periods
extended spectrum beta-lactamase. 1 Calculated for newborns with a birthweight below 1500 grams (N=74 and N=56 in period 1 and period 2, respectively).2 Includes: early and late-onset clinical (i.e., high clinical suspicion, treated with antibiotics for 7 days; raised C-reactive
protein levels) and blood culture positive sepsis.3 Includes: blood and urine cultures and cultures on (tracheal aspirate, skin and anal) swabs, central lines or
ventilation tubes.
NEO
NA
TAL IN
TENSIV
E CA
RE IN SU
RINA
ME
37
2
DISCUSSIONImprovements at the neonatal care facility led to an increase of newborns that received intensive
care with a significant reduction in their mortality. Furthermore, newborns with a GA above 28
weeks and/or BW≥1500 grams showed a significantly reduced mortality rate. A striking reduction
in mortality was seen in cases of perinatal asphyxia and sepsis. In addition, after the transition
a two-fold increase in admission of outborn newborns, with similar demographics and increased
survival rates, was observed. These findings indicate enhanced tertiary function and centralization
of neonatal intensive care in Suriname, which may play a significant role in reducing neonatal
mortality in Suriname.
Other studies performed in developing countries have shown similar patterns in improvement
of mortality after scaling up of neonatal care facilities. Creation of a level II sick newborn care unit
(SNCU) (i.e., with introduction of bed warmers and central oxygen) in a district hospital in India led
to a significant reduction of regional NMR of mostly newborns with a BW<1500 grams [6]. Another
pre-and-post intervention study in India showed that basic interventions (i.e., promotion of enteral
nutrition, asepsis regulations and training of nurses) led to an immediate and stable reduction of
NMR and birth-weight specific survival of newborns with a BW<1500 grams, but not with a BW<1000
grams, primarily after reduced incidence and mortality of sepsis [7]. Introduction of nasal CPAP at
a NICU in Nicaragua reduced mortality amongst total newborns receiving ventilation assistance
(i.e. either mechanical ventilation or CPAP) [8]. Improvement (i.e., new equipment, refurbishment
and training of personnel) of a newborn unit to a Level III NICU at a teaching hospital in Ghana led
to significant reduction of mortality amongst newborns with a BW<2500 grams, mostly secondary
to significantly reduced incidence of perinatal asphyxia [9].
In these studies, training and expansion of personnel was a universal denominator for
improvement of care, which was also part of our intervention. Systematic training of midwives
in neonatal resuscitation has been a challenge in low resource countries and so far has yielded
positive results only in low risk settings, and takes time with need for strong re-enforcement
and repetition before an effect on neonatal mortality is observed [10-12]. However, increasing
the number of nurses per infant at the NICU may have a beneficial effect on neonatal outcome
[13,14]. Further improvement of survival may then be accomplished with increased capacity for
neonatal intensive care (e.g., increased capacity for (modernized) ventilation). We observed
a significant increase of use of neonatal intensive care commodities in the post-transition period.
Indeed, both higher level and volume of neonatal intensive care have been associated with
better survival of newborns with a BW<1500 grams [15,16]. While this seems an intuitive and logical
effect, it is important to realize that positive effects of higher capacity can only be sustained with
continuous and balanced availability of trained personnel, which can be challenging in the lower
resource setting [17,18]. Illustratively, in our population the reduction of admission rates in the post
transition period coinciding with increased number of nurses per bed may have been beneficial
for survival. However, the amount of nurses per infant at our facility is still less than recommended
for the intended level of care (i.e., one nurse per one or two beds), which may partially explain our
finding that the mortality rate in the most vulnerable small preterm infants (i.e., with a BW<1000
NEO
NA
TAL IN
TENSIV
E CA
RE IN SU
RINA
ME
38
2
grams and <28 weeks of GA) did not decrease [19]. However, restricting the number of beds in
case of understaffing is extremely difficult when there are no other NICU level referral options
in Suriname.
Admission of more outborn neonates indicates an enhanced regional function of our neonatal
care facility, which was shown to be beneficial for their survival depending on the referral system. In
Ghana, survival of outborn newborns at the refurbished NICU was only beneficial to those referred
from private health facilities [9]. In our population, outborn newborns, mostly referred from birth
clinics and private or public Level II SNCUs at other hospitals, died more frequently than inborn
ones in both periods. Delays in transfer or higher prevalence of antenatal (e.g., preeclampsia) and
neonatal (e.g., prematurity) risk factors could have contributed to this [20-22]. However, the fact
that in our study demographics of outborn newborns were similar in both periods indicates
that better survival after the transition was mostly due to enhanced neonatal intensive care,
independent of presence of antenatal and neonatal risk factors. Screening regimens for antenatal
risk factors at surrounding birth clinics and in-utero transfer to our birth clinic, thereby creating
proximity to our neonatal care facility, could further enhance tertiary function and improve
survival in Suriname [23,24].
Mortality due to both perinatal asphyxia and sepsis were reduced in the post transition period.
For inborn newborns, training of obstetric nurses may have contributed to the reduction in
mortality of sepsis and similarly to less cases and better outcome of asphyxia. Additionally, for
both inborn and outborn newborns efficient treatment (e.g., modern equipment for mechanical
ventilation or circulatory support) at our refurbished NICU could have had beneficial effect on
survival of both. In the case of late-onset sepsis, incidence and mortality remained the same
after the transition. This indicates that our asepsis interventions, aimed primarily at prevention of
transmission of pathogens, failed, which is also reflected in similar amounts of ESBL-positive blood
cultures among both study periods. These results stress that in our setting strict enforcement of
asepsis protocol remains challenging, but should be prioritized.
Mortality of newborns with a BW<1000 grams remained high after the intervention. High
mortality of newborns with a BW<1000 grams was also observed in earlier reports in a Level II
SNCU in Jamaica, a Level III neonatal care facility in South Africa and at multiple NICUs in Brazil
and around the world [1,25-27]. In our low-resource setting, the fact that these newborns demand
a disproportionate share of scarcely available human and non-human recourses is a significant
limitation for improvement. However, almost half of them died of late-onset sepsis, indicating that
more effective infection prevention, including antibiotic stewardship, might substantially increase
their survival rates. Additionally, a major cause for morbidity amongst newborns with a BW<1500
grams in our study was NEC (Table 3b). Prevalence of NEC remained high, despite promotion
of feeding with human breast milk. Recent evidence from NICUs in developed countries has
shown that simple interventions (i.e., early human milk feedings, rigorous feeding protocol and
restricted feeding during indomethacin treatment and blood transfusions, and selective antibiotic
usage) can reduce incidence of NEC [28]. These interventions are cost-effective and can also easily
be applied in lower resource settings [29]. A major limitation in our setting is the unavailability
of total parenteral nutrition, but at the same time the low adherence to breast milk offers
NEO
NA
TAL IN
TENSIV
E CA
RE IN SU
RINA
ME
39
2
a major opportunity for improvement. Lastly, the increased number of cases of NEC, along with
the increase in incidence of BPD, may be the unfortunate effect of more intensive care (e.g., more
ventilation, more early antibiotics) and better survival.
Limitations to this study were missing data (e.g., scarce data on additional outcomes
such as intraventricular hemorrhage, retinopathy of the premature, post-discharge survival),
the retrospective nature of this study, and relatively small numbers for complications with a low
incidence. Although we collected data to determine the highest level of care, we were not able to
apply an index to indicate severity of disease of newborns.
CONCLUSIONSThis study shows that scaling up of neonatal intensive care in Suriname substantially reduced
mortality of both in and outborn newborns through its enhanced availability and centralization.
Challenges ahead are sustainability, further improvement of tertiary function, and prevention of
sepsis and NEC with implementation of cost and resource effective interventions.
List of Abbreviations
SNCU = sick newborn care unit
NICU = neonatal intensive care unit
AHP = Academic Hospital Paramaribo
NMR = neonatal mortality rate (i.e., number of neonatal deaths per 1000 live births)
BW = birth weight
GA = gestational age
NEC = necrotizing enterocolitis
BPD = bronchopulmonary dysplasia
VAP = ventilator-associated pneumonia
EOS = early onset sepsis
LOS = late onset sepsis
ESBL = extended spectrum beta-lactamase
Maroon = descendant from Africans that escaped slavery and established independent societies
(e.g., term predominantly used in South America and on Caribbean Islands)
DECLARATIONSEthics
The Suriname Commission for Human Research approved this study (VG-021-14A).
Availability of Data and Materials
The datasets during and/or analyzed during the current study are available from the corresponding
author on reasonable request.
NEO
NA
TAL IN
TENSIV
E CA
RE IN SU
RINA
ME
40
2
Competing Interests
The authors declare that they have no competing interests.
Funding
R. Zonneveld was supported by the Thrasher Research Fund (TRF13064).
Authors’ Contributions
RZ, FBP and AJ conceived of the study. RZ, NH, FB, and AB performed the data search and
analysis. NPAL and PHD contributed in analyzing the data. All authors contributed to drafting
the manuscript, and read and approved the final manuscript.
Acknowledgments
The authors acknowledge the efforts of the employees of the medical archives of the Academic
Hospital Paramaribo for help with the retrieval of all patient charts used for this paper. We also
thank Professor Frans J. Walther at Leiden University and University of California Los Angeles for
careful review of this paper.
NEO
NA
TAL IN
TENSIV
E CA
RE IN SU
RINA
ME
41
2
REFERENCES1. Chow S, Chow R, Popovic M, Lam M, Popovic
M, Merrick J, Stashefsky Margalit RN, Lam H,
Milakovic M, Chow E, Popovic J. A Selected Review
of the Mortality Rates of Neonatal Intensive Care
Units. Front Public Health, 2015;7;3:225.
2. Carlo WA, Travers CP. Maternal and neonatal
mortality: Time to act J Pediatr (Rio J), 2016;426.
3. Black RE, Levin C, Walker N, Chou D, Liu L,
Temmerman M; DCP3 RMNCH Authors Group.
Reproductive, maternal, newborn, and child health:
key messages from Disease Control Priorities 3rd
Edition. Lancet 2016, S0140-6736(16)00738-8.
4. Knippenberg R, Lawn JE, Darmstadt GL,
Begkoyian G, Fogstad H, Walelign N, Paul
VK; Lancet Neonatal Survival Steering Team.
Systematic scaling up of neonatal care in
countries. Lancet 2005, 365(9464):1087-98.
5. Hedstrom A, Ryman T, Otai C, Nyonyintono
J, McAdams RM, Lester D, Batra M.
Demographics, clinical characteristics and
neonatal outcomes in a rural Ugandan NICU.
BMC Pregnancy Childbirth. 2014, 19;14:327.
6. Sen A, Mahalanabis D, Singh AK, Som TK,
Bandyopadhyay S. Impact of a district level sick
newborn care unit on neonatal mortality rate:
2-year follow-up. J Perinatol 2009, 29(2):150-5.
7. Agarwal R, Agarwal K, Acharya U, Christina
P, Sreenivas V, Seetaraman S. Impact of
simple interventions on neonatal mortality
in a low-resource teaching hospital in India. J
Perinatol 2007, 27(1):44-9.
8. Rezzonico R, Caccamo LM, Manfredini V,
Cartabia M, Sanchez N, Paredes Z, Froesch P,
Cavalli F, Bonati M. Impact of the systematic
introduction of low-cost bubble nasal CPAP in
a NICU of a developing country: a prospective
pre- and post-intervention study. BMC
Pediatr 2015, 25;15:26.
9. Enweronu-Laryea CC, Nkyekyer K, Rodrigues
OP. The impact of improved neonatal
intensive care facilities on referral pattern and
outcome at a teaching hospital in Ghana. J
Perinatol 2008, 28(8):561-5.
10. Carlo WA, Goudar SS, Jehan I, Chomba E,
Tshefu A, Garces A, Parida S, Althabe F, McClure
EM, Derman RJ, Goldenberg RL, Bose C, Krebs
NF, Panigrahi P, Buekens P, Chakraborty H,
Hartwell TD, Wright LL; First Breath Study
Group. Newborn-care training and perinatal
mortality in developing countries. N Engl J
Med 2010, 362(7):614-23.
11. Carlo WA, McClure EM, Chomba E,
Chakraborty H, Hartwell T, Harris H, Lincetto
O, Wright LL. Newborn care training of
midwives and neonatal and perinatal
mortality rates in a developing country.
Pediatrics 2010, 126(5):e1064-71.
12. Matendo R, Engmann C, Ditekemena J, Gado
J, Tshefu A, Kinoshita R, McClure EM, Moore
J, Wallace D, Carlo WA, Wright LL, Bose
C. Reduced perinatal mortality following
enhanced training of birth attendants in
the Democratic Republic of Congo: a time-
dependent effect. BMC Med 2011, 9:93.
13. American Academy of Pediatrics Committee
on Fetus and Newborn. Levels of neonatal
care. Pediatrics 2012, 130(3):587-97.
14. Callaghan LA, Cartwright DW, O’Rourke P,
Davies MW. Infant to staff ratios and risk of
mortality in very low birthweight infants. Arch
Dis Child Fetal Neonatal Ed 2003, 88(2):F94-7.
15. Phibbs CS, Baker LC, Caughey AB, Danielsen
B, Schmitt SK, Phibbs RH. Level and volume
of neonatal intensive care and mortality
in very-low-birth-weight infants. N Engl J
Med 2007, 356(21):2165-75.
16. Bartels DB, Wypij D, Wenzlaff P, Dammann
O, Poets CF. Hospital volume and neonatal
mortality among very low birth weight infants.
Pediatrics 2006, 117(6):2206-14.
17. Neogi SB, Malhotra S, Zodpey S, Mohan P.
Does facility based newborn care improve
neonatal outcomes? A review of evidence.
Indian Pediatr 2012, 49(8):651-8.
18. Neogi SB, Malhotra S, Zodpey S, Mohan
P. Challenges in scaling up of special care
newborn units--lessons from India. Indian
Pediatr 2011, 48(12):931-5.
19. British association of perinatal medicine.
Optimal arrangements for neonatal intensive
NEO
NA
TAL IN
TENSIV
E CA
RE IN SU
RINA
ME
42
2
care units in the UK including guidance on their
medical staffing. A framework for practice. 3rd
edition 2014.
20. Sen A, Mahalanabis D, Singh AK, Som
TK, Bandyopadhyay S. Development and
effects of a neonatal care unit in rural India.
Lancet 2005, 366(9479):27-8.
21. Sehgal A, Roy MS, Dubey NK, Jyothi MC. Factors
contributing to outcome in newborns delivered
out of hospital and referred to a teaching
institution. Indian Pediatr 2001, 38(11):1289-94.
22. Arad I, Braunstein R, Bar-Oz B. Neonatal
outcome of inborn and outborn extremely
low birth weight infants: relevance of perinatal
factors. Isr Med Assoc J 2008, 10(6):457-61.
23. Chien LY, Whyte R, Aziz K, Thiessen P, Matthew
D, Lee SK: Canadian Neonatal Network.
Improved outcome of preterm infants when
delivered in tertiary care centers. Obstet
Gynecol 2001, 98(2):247-52.
24. Lorch SA, Baiocchi M, Ahlberg CE, Small DS.
The differential impact of delivery hospital
on the outcomes of premature infants.
Pediatrics 2012, 130(2):270-8.
25. Ballot DE, Chirwa TF, Cooper PA. Determinants
of survival in very low birth weight neonates in
a public sector hospital in Johannesburg. BMC
Pediatr 2010;10:30.
26. Trotman H. Bell Y. Neonatal sepsis in very
low birth weight infants at the University
Hospital of the West Indies. West Indian
Med J. 2006, 55:165-9.
27. Guinsburg R, de Almeida MF, de Castro JS,
Silveira RC, Caldas JP, Fiori HH, do Vale MS,
Abdallah VO, Cardoso LE, Alves Filho N,
Moreira ME, Acquesta AL, Ferrari LS, Bentlin
MR, Venzon PS, Gonçalves Ferri WA, Meneses
Jdo A, Diniz EM, Zanardi DM, Dos Santos
CN, Bandeira Duarte JL, Rego MA. Death
or survival with major morbidity in VLBW
infants born at Brazilian neonatal research
network centers. J Matern Fetal Neonatal
Med 2016, 29(6):1005-9.
28. Talavera MM, Bixler G, Cozzi C, Dail J, Miller RR,
McClead R Jr, Reber K. Quality Improvement
Initiative to Reduce the Necrotizing
Enterocolitis Rate in Premature Infants.
Pediatrics 2016, 137(5).
29. Johnson TJ, Patel AL, Bigger HR, Engstrom
JL, Meier PP. Cost savings of human milk
as a strategy to reduce the incidence of
necrotizing enterocolitis in very low birth
weight infants. Neonatology 2015, 107(4):271-6.
NEO
NA
TAL IN
TENSIV
E CA
RE IN SU
RINA
ME
43
2
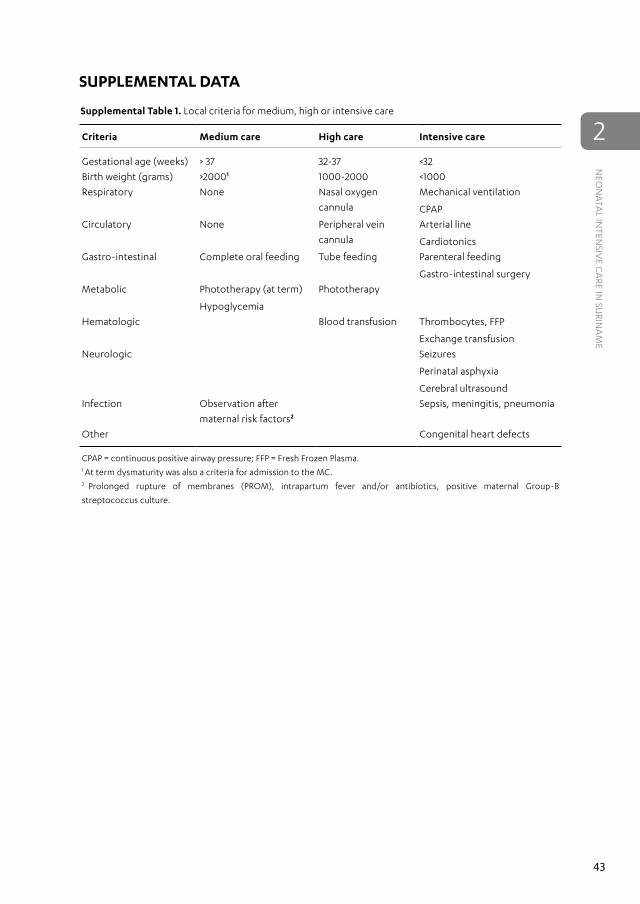
SUPPLEMENTAL DATA
Supplemental Table 1. Local criteria for medium, high or intensive care
CPAP = continuous positive airway pressure; FFP = Fresh Frozen Plasma. 1 At term dysmaturity was also a criteria for admission to the MC.2 Prolonged rupture of membranes (PROM), intrapartum fever and/or antibiotics, positive maternal Group-B
streptococcus culture.
II Prediction of Early Onset Sepsis
3 Association between Early Onset Sepsis Calculator and Infection Parameters for
Newborns with Suspected Early Onset Sepsis
Niek Achten, Rens Zonneveld, Ellen Tromp, Frans B. Plötz
J Clin Neonatol 2017, 6:159-62
EARLY
ON
SET SEPSIS CA
LCU
LATO
R
52
3
ABSTRACTContext
Early onset sepsis (EOS) remains an important clinical problem with significant antibiotic
overtreatment as a result of poor specificity of clinical and infection parameters. Quantitative risk
stratification models such as the EOS calculator are promising, but it is unclear how these models
relate to infection parameters in the first 72 hours of life.
Aim
To evaluate the hypothesis that higher EOS calculator results are associated with (serial) laboratory
infection parameters, in particular an increase in CRP within 24-48 hours, and low leukocyte counts.
Design and Methods
EOS risk estimates were determined for infants born ≥ 34 weeks of gestation who were started
on antibiotic treatment for suspected EOS within 72 hours after birth. EOS risk estimates were
retrospectively compared to (changes in) available laboratory infection parameters including
C-reactive protein (CRP), leukocyte and thrombocyte count.
Statistical Analysis Used
Spearman’s rho rank correlations coefficient was used when testing for correlations between
continuous parameters. Kruskal-Wallis and Mann-Whitney U tests were applied to differences
between stratified risk groups.
Results
EOS risk was not correlated with changes in infection parameters. We found negative correlations
between both EOS risk and CRP level and leukocyte count within 6 hours of the start of antibiotics,
as well as CRP level between 6-24 hours after start of treatment.
Conclusions
In contrast to our hypothesis, high EOS risk at birth was consistently correlated with lower CRP and
leukocyte counts within 24 hours after the start of antibiotics, but not with infection parameters
after 24 hours. Further interpretation of infection parameters during sepsis calculator use needs
to be elucidated.
Key Messages
The sepsis calculator is neither associated with changes in CRP level, nor leukocyte or thrombocyte
count in newborns with suspected early onset sepsis.
EARLY
ON
SET SEPSIS CA
LCU
LATO
R
53
3
INTRODUCTIONEarly onset neonatal sepsis (EOS) remains an important clinical problem in neonatal care. Due to
poor specificity of clinical findings and limited usability of available infection biomarkers, there is
significant over-treatment with antibiotics in the first 72 hours of life of newborns with suspected
EOS [1]. In an attempt to overcome this problem a quantitative risk stratification strategy based on
objective maternal risk factors and neonatal clinical findings has been developed [2]. This model,
hereafter referred to as the EOS calculator, provides a quantitative estimation of EOS risk along
with a recommendation on the use of antibiotics, and is available online. Two retrospective studies
revealed that application of the sepsis calculator may significantly reduce antibiotic therapy and
thus use of the EOS calculator may become more common in clinical practice [3,4].
Despite this promising potential, it is currently unclear how the EOS calculator estimated risk
and recommendations relate to infection parameters in the first 72 hours of life. Serial values in
C-reactive protein (CRP) and leukocyte count are still commonly used as arguments for the start
and duration of antibiotic therapy [1,5]. For this study, our aim was to evaluate the hypothesis that
higher EOS calculator results are associated with (serial) laboratory infection parameters. As EOS
is associated with elevated CRP and a lower leukocyte count [5,6] we particularly hypothesized
high EOS risk estimate to be associated with an increase in CRP within 24-48 hours, and low
leukocyte counts
SUBJECTS AND METHODSStudy Design
Data from a previously established retrospective birth cohort were used for analysis [4]. The study
included all newborns born ≥34 weeks of gestation, who were started on antibiotic treatment for
suspected EOS within 72 hours after birth, in Tergooi Hospital, Blaricum, The Netherlands, during
2014. Exclusion criteria were major congenital anomalies, including chromosomal, and prophylactic
treatment with antibiotics. The study was approved by the Scientific Review Committee of
Tergooi Hospital.
Data Collection
Maternal and neonatal clinical data were derived from hospital records. Local protocol required
routine infection parameter testing in newborns treated for clinically suspected EOS at start
of antibiotic therapy, and follow-up testing at 12-24 hours and/or 24-72 hours after the start of
antibiotic treatment. Infection parameter results were derived from electronic laboratory records.
EOS Calculator Risk Estimates and Stratification
EOS risk estimates were determined using the online calculator as provided by Escobar et al.,
through http://newbornsepsiscalculator.org [2,7]. These estimates represent the estimated
incidence of EOS per 1000 live births, and were calculated individually for each newborn in
the study. The resultant sepsis risk was categorized into three levels; <0.65 (low risk), 0.65-1.54
EARLY
ON
SET SEPSIS CA
LCU
LATO
R
54
3
(intermediate risk), and >1.54 (high risk) per 1000 live births. In addition to using EOS calculator
risk estimate as continuous variables, we used these groups for stratified analysis.
Delta Variables
Since specifically serial values in infection parameters are used to guide clinical decisions [8] we
calculated delta variables when serial values were available. For delta variables, we calculated
absolute differences between values derived from initial blood draw (0-6 hours after start of
treatment) and follow-up values 24 hours after start of treatment. Values derived between 6-24
hours were used as follow-up values if values >24 hours were unavailable.
Statistical Analysis
All data were statistically analyzed using R (version 3.2.1) (http://www.r-project.org). Distributions
of continuous variables were visualized using kernel density plots. Spearman’s rho rank correlations
coefficient was used when testing for correlations between EOS risk estimates and infection
parameters (continuous variables not normally distributed). Kruskal-Wallis and Mann-Whitney U
tests were applied to determine significance of differences between EOS stratified risk groups.
RESULTSAfter exclusion of three newborns with insufficient clinical information to estimate EOS risk, data
from 108 newborns were used for analysis (Table 1).
CRP
We found negative correlations between EOS risk estimations and CRP levels within 6 hours and
between 6 and 24 hours after the start of antibiotics (Spearman’s rho -0.45 and -0.24, respectively).
This was confirmed by EOS stratified group analysis, where the high EOS risk group was associated
with lower CRP levels (<1 versus 11.5 mg/l, p<0.05, Table 1). EOS risk estimate was not correlated with
change in CRP as determined by the delta CRP variable based on serial CRP values.
Leukocytes and Thrombocytes
EOS risk estimate was not correlated with changes in serial leukocytes count. Lower leukocyte
counts within 6 hours after the start of antibiotics were associated with higher EOS risk estimations
(Spearman’s rho -0.30). Leukocyte count within 6 hours after start of antibiotics was lower in
the high-risk group compared to the intermediate/low risk group (p<0.05) (Table 1). There were
no correlations between EOS risk and (serial) thrombocyte counts.
DISCUSSIONIn contrast to our hypothesis, we did not find any correlations between EOS risk and changes in
serial CRP or serial leukocyte or trombocyte counts. We observed negative correlations between
EOS risk estimate and CRP level and leukocyte count within 6 hours of start of antibiotics, as well
EARLY
ON
SET SEPSIS CA
LCU
LATO
R
55
3
as CRP level between 6-24 hours after start of treatment. Analyzing differences between EOS
stratified risk groups, comparable results within 6 hours of start of treatment were found.
In the high-risk group single point measurement CRP levels were in the normal range at start of
antibiotic therapy, which was started shortly after birth. This can be explained by the fact that CRP
levels represent endogenous neonatal synthesis, rise above 5 mg/l by 6-8 hours and peak around
24-48 hours [9,10]. Negative correlation between high EOS risk and CRP levels at the start of
antibiotic treatment may be explained by the fact that high-risk newborns started with antibiotic
treatment shortly after birth, before endogenous synthesis of CRP occurred. Furthermore, this
may also explain the significant differences of CRP levels of <1 mg/l in high-risk group versus
11.5 mg/l in the low-risk group at the start of antibiotics (P<0.05). In contrast to the high-risk
group, antibiotic therapy was mostly started 12 hours after birth in the low risk group of our
population [4].
Remarkably, CRP levels did not clearly increase in the high-risk group, as CPR level after
24-48h was not significantly raised compared to low and intermediate risk groups. This appears
to contrast with studies confirming that the sensitivity of CRP increases substantially with serial
determinations of CRP 24-48h after the onset of symptoms [9]. However, although EOS-risk is
correlated with infection, still the majority of the newborns in this group had negative blood
cultures, corresponding with persistent low CRP levels. In addition, given the half-life of CRP (19
hours) and clinical studies showing CRP levels decreasing after 16 hours in response to successful
antibiotic therapy, it is well possible that CRP-levels have returned to normal range within 24-48
Table 1. Infection parameters and correlation results among total and stratified risk group analysis.
EOS risk group
Overall
(n=108)
Stratified risk group analysis
Low
(n=41)
Intermediate
(n=10)
High
(n=57)
Infection parameter Median (IQR) n (%) Spearman’s rho Median (IQR)4
CRP
(median, mg/l)
<6 h <1 (13) 100 (93.6) -0.453 11.5(25) <1(8) <1(3)3
6-24 h 7 (23) 82 (75.9) -0.241 11.5(25) 2(8) 5(20)
>24 h 5.5 (17) 58 (53.7) -0.01 7(15) 3(20) 5(26)
Delta 4 (19) 96 (88.9) -0.08 6 (18) 2(21) 4(19)
Leukocytes
(median, x109/L)
<6 h 16.4 (9) 102 (94.4) -0.302 20.6(11) 15.3(20) 15.3(9)2
6-24 h 16.5 (10) 70 (64.8) -0.13 16.6(11) 26.2(15) 14.4(10)
>24 h 13.1 (7) 53 (49.1) -0.19 15.0(5) 14.3(16) 11.4(6)
<6 h 219 (87) 94 (87.0) 0.04 224(112) 217(93) 215(92)
6-24 h 214 (113) 67 (62.0) 0.11 208(159) 233(91) 208(113)
>24 h 245 (106) 49 (45.4) 0.01 241(169) 280(80) 243(105)
Delta 27 (39) 77 (71.3) 0.09 25(57) 32(24) 27(39)
Statistically significant results marked in bold; 1P<0.05, 2P<0.01, 3P<0.001. 4 Mann-Whitney U test, high versus low/intermediate risk group. EOS risk; early onset sepsis risk as calculated with
sepsis calculator.
EARLY
ON
SET SEPSIS CA
LCU
LATO
R
56
3
hours in infected children in the high-risk group, as this group was generally started on antibiotics
within shortly after birth [9,11].
From a clinical point of view these findings underline the puzzling nature of EOS clinical
management, with high EOS risk associated with low CRP levels. In the high-risk group, based
on objective maternal factors and newborn clinical evaluation, antibiotic therapy is started
and continued for 7 days. In this group, (serial) CRP measurement is not of additional value to
discontinue antibiotic therapy in case of negative blood cultures. In the low EOS risk group,
however, serial CRP may serve to discontinue antibiotic treatment after 3 days, given the negative
predictive value of serial low CRP levels [10].
The correlation between higher EOS risk estimates and lower leukocyte counts within 6 hours
after start of antibiotics corresponds with published findings showing lower leukocyte counts
being associated with EOS [6]. It should be noted however, that low leukocyte counts are rare
– reflected in a modest difference in absolute leukocyte count between the high-risk group and
overall median (15.3 vs 16.4 x109/L). Therefore, leukocyte counts are likely to be of limited clinical
value in EOS diagnostics. Finally, (changes) in thrombocyte counts were, in line with published
literature, not related to EOS risk. Thus we do not recommend the use of thrombocyte counts to
guide clinical decisions regarding antibiotics for EOS, regardless of estimated EOS risk.
Limitations of this study include its retrospective nature and selection bias for determination
of infection parameters. However, given the high percentage of available results within 6 hours of
start of antibiotics, we think this bias is limited for the correlations we found. Our sample size is
limited, but given the consistent results among correlation and stratified group level analysis, we
do not expect different results with a larger sample size.
In conclusion, EOS remains an important clinical problem with significant antibiotic
overtreatment as a result of poor clinical and infection parameters. In newborns treated for EOS,
risk estimates are neither associated with changes in CRP level, nor leukocyte or thrombocyte
count. If more widespread use of the sepsis calculator is expected, the interpretation of common
infection parameters in the context of EOS risk needs to be further elucidated.
EARLY
ON
SET SEPSIS CA
LCU
LATO
R
57
3
REFERENCES1. van Herk W, Stocker M, van Rossum AMC.
Recognising early onset neonatal sepsis: An
essential step in appropriate antimicrobial use.
J Infect 2016, 72:S77–82.
2. Escobar GJ, Puopolo KM, Wi S, Turk BJ,
Kuzniewicz MW, Walsh EM, Newman TB,
Zupancic J, Lieberman E, Draper D. Stratification
of risk of early-onset sepsis in newborns ≥ 34
weeks’ gestation. Pediatrics 2014, 133(1):30–6.
3. Shakib J, Buchi K, Smith E, Young PC.
Management of newborns born to mothers with
chorioamnionitis: Is it time for a kinder, gentler
approach? Acad Pediatr 2015, 15(3):340–4.
4. Kerste M, Corver J, Sonnevelt MC, van Brakel
M, van der Linden PD, M. Braams-Lisman BA,
Plötz FB. Application of sepsis calculator in
newborns with suspected infection. J Matern
Neonatal Med 2016, 7058:1–6.
5. Chirico G, Loda C. Laboratory aid to
the diagnosis and therapy of infection in
the neonate. Pediatr Rep 2011, 3(e1):1–5.
6. Newman TB, Puopolo KM, Wi S, Draper D,
Escobar GJ. Interpreting complete blood
counts soon after birth in newborns at risk for
sepsis. Pediatrics 2010, 126(5):903–9.
7. Puopolo KM, Draper D, Wi S, Newman TB,
Zupancic J, Lieberman E, Smith M, Escobar GJ.
Estimating the probability of neonatal early-
onset infection on the basis of maternal risk
factors. Pediatrics 2011, 128(5):e1155-63.
8. van Herk W, el Helou S, Janota J, Hagmann C,
Klingenberg C, Staub E, Giannoni E, Tissieres
P, Schlapbach LJ, van Rossum AM, Pilgrim SB,
Stocker M. Variation in Current Management
of Term and Late-Preterm Neonates at Risk for
Early-Onset Sepsis “An International Survey
and Review of Guidelines”. Pediatr Infect
Dis J 2016, 35(5):494–500.
9. Hofer N, Zacharias E, Müller W, Resch B. An
update on the use of C-reactive protein in
early-Onset neonatal sepsis: Current insights
and new tasks. Neonatology 2012, 102(1):25–36.
10. Simonsen KA, Anderson-Berry AL, Delair SF,
Dele Davies H. Early-onset neonatal sepsis.
Clin Microbiol Rev 2014, 27(1):21–47.
11. Ehl S, Gehring B, Pohlandt F. A detailed analysis
of changes in serum C-reactive protein levels
in neonates treated for bacterial infection. Eur
J Pediatr 1999, 158(3):238–42.
4 Immature-to-total-granulocyte Ratio as a Guide for Antibiotic Treatment in Suspected Early Onset Sepsis in
Surinamese Newborns
Rens Zonneveld, Sheldon Simson, John Codrington, Amadu Juliana, Frans B. Plötz
Submitted
IMM
ATU
RE GR
AN
ULO
CY
TES IN SU
RINA
MESE N
EWBO
RNS
60
4
ABSTRACTObjective
Measurement of immature granulocytes may be helpful in management of early onset sepsis
(EOS) in newborns in developing countries. We evaluate early negative prediction of automated
measurement of a one-point measurement of immature-to-total-granulocyte (I/T) ratio in
newborns with suspected EOS to help decisions on duration of antibiotic treatment.
Methods
A retrospective study was performed amongst newborns with a gestational age ≥34 weeks with
suspected EOS in whom local protocol had been followed for start and duration of antibiotic
treatment, and in whom granulocyte counts had been measured with a Sysmex XT 2000i
automated hematology analyzer.
Results
I/T and I/T2 were significantly lower (P 0.048 and P 0.015, respectively) in newborns with favorable
clinical course and in whom EOS was unlikely. In these newborns antibiotics were stopped 48-72
hours after start after which they all remained healthy.
Conclusion
Low I/T and I/T2 may help to increase the threshold to start empirical antibiotics or to guide safe
stoppage of antibiotics after 48-72 hours. Ultimately, this may help to reduce the antibiotic burden
in developing countries.
IMM
ATU
RE GR
AN
ULO
CY
TES IN SU
RINA
MESE N
EWBO
RNS
61
4
INTRODUCTIONAn estimated tenfold of newborns is empirically, and often unnecessarily, treated with antibiotics
in the first 72 hours of life for suspected early onset sepsis (EOS) [1]. Poor specificity of clinical
symptoms and limited utility of infection biomarkers complicate decisions on start and duration
of antibiotic treatment [1]. Over 60% of antibiotics given empirically before 72 hours of life are
prolonged beyond 48-72 hours despite a negative blood culture and a stable clinical condition
[2]. Furthermore, the threshold to start antibiotics in newborns in developing countries is low [3].
It remains a challenge to safely avoid unnecessary antibiotics in newborns with suspected EOS,
especially in developing countries.
Recent studies indicate that the immature-to-total-granulocyte (I/T) ratio may be promising
tool to identify infection at an early stage and to guide duration of antibiotic therapy (4-8).
Newman et al. proposed combination of the absolute neutrophil count (ANC) and I/T into the I/
T2, to be used in a prediction model for EOS [4]. Higher I/T2 predicted positive blood culture in
suspected EOS. Moreover, low serial immature-to-total-granulocyte ratios (I/T), in combination
with negative blood culture, can be used to discontinue antimicrobial therapy at 36-48 hours [5].
Whether a single point measurement of I/T or I/T2 at start of antibiotics in EOS is already predictive
for negative blood cultures is unknown.
Nowadays, the global availability of high-throughput flow-based automated hematology
analyzers (AHA) facilitates simple and fast measurement of immature granulocytes in developing
countries [6]. The aim of this study is to retrospectively evaluate early negative prediction
of automated measurement of I/T and I/T2 in Surinamese newborns with suspected EOS. We
hypothesized that I/T and I/T2 at start of antibiotic treatment were lower in newborns with unlikely
EOS in whom antibiotics were discontinued after 48-72 hours.
SUBJECTS AND METHODSStudy Design
A retrospective study was performed amongst newborns admitted to the neonatal care facility
at the Academic Hospital Paramaribo (AHP) from September 1st 2015 to May 30th 2016. Included
were newborns with a gestational age (GA) ≥34 weeks, who received antibiotic therapy within
72 hours after birth and with available laboratory results on immature granulocytes. Antibiotics
(intravenous ampicillin and gentamycin) were started for presence of maternal risk factors for EOS
or clinical suspicion. According to local protocol, EOS was considered unlikely if clinical course
had been uneventful (i.e., clinical improvement and no support other than normal volumes of IV
fluids or tube feeding), serial measurement of C-reactive Protein (CRP) was normal (i.e., levels <0.5
mg/dL), and blood culture was negative. Consequently, antibiotic treatment was discontinued
after 48-72 hours. Otherwise treatment was continued for 7 days. Newborns were divided in
two groups, namely: 1) Unlikely EOS: antibiotics discontinued after 48-72 hours; and 2) Probable
EOS: full 7-day treatment. The study protocol was part of a larger study on EOS, which was made
available on clinicaltrials.gov (NCT02486783) and was approved by the Surinamese Medical-Ethical
Board (VG-021-14A).
IMM
ATU
RE GR
AN
ULO
CY
TES IN SU
RINA
MESE N
EWBO
RNS
62
4
Data and Sample Collection
The following data were collected: maternal and prenatal conditions and risk factors, delivery
granulocyte fraction.1 P >0.1 unless stated otherwise.2 Includes: Hindo-Surinamese, Javanese and Amerindian.3 At start of antibiotics.4 At t=48-72 hours after start of antibiotic treatment.
IMM
ATU
RE GR
AN
ULO
CY
TES IN SU
RINA
MESE N
EWBO
RNS
64
4 0.00
0.02
0.04
0.06
0.08
0.10
I/T
A
B
UnlikelyEOS (n=13)
Probable EOS (n=14)
0.000
0.002
0.004
0.006
0.008I/T
2
*
*
Figure 1. Immature-to-total-granulocyte ratios (I/T and I/T2) in Surinamese newborns treated with
antibiotics for suspected early onset sepsis (EOS). A: I/T; B: I/T2. Data represent ratios calculated from
results of automated measurement of granulocytes with a Sysmex XT 2000i analyzer in whole blood obtained
from newborns with suspected EOS at start of antibiotic treatment. I/T2 is calculated according to Newman et
al. (7). * P <0.05 compared to probable EOS. Bars represent median values and error bars interquartile range.
empirical antibiotic therapy. Second, it may guide clinicians to shorten antibiotic treatment to
48-72 hours in case of negative blood cultures.
Of the measured parameters, I/T2 showed the most significant difference between short and
full treatment duration. This is in line with the conclusions made by Newman et al. [4,8]. They
postulated that measurement of both the ANC and I/T have separate predictive values but are
two dependent tests since the ANC is a variable in the denominator of I/T. The I/T2 was designed
to capture both tests into one ratio, which showed increasing performance in newborns older
than 4 hours of life and when there was high suspicion of EOS. In contrast to Newman et al., we
were particularly interested in the negative predictive ability of I/T2 during the transition period
of newborns. In our cohort most newborns started within 4 hours of life with antibiotics. In these
newborns the threshold to start empirical antibiotic therapy is lower due to ambivalent clinical
symptoms during transition to extrauterine life. When measured within 4 hours after birth, we
observed a trend in lower I/T2 in cases of unlikely EOS. This is a clinically relevant finding, which
may favor the I/T2 in increasing the threshold to start antibiotics during the transition period in
newborns with a low suspicion of EOS.
Nowadays, CRP is frequently used in clinical settings to determine safe stoppage of antibiotics
for EOS, also in Suriname. Serially measured low levels of CRP predict absence of EOS with a negative
predictive value (NPV) of 99%, yet only in combination with a negative blood culture and clinically
IMM
ATU
RE GR
AN
ULO
CY
TES IN SU
RINA
MESE N
EWBO
RNS
65
4
improved newborn [2,9]. However, in practice, despite this high NPV, serial measurement of CRP
can also lead to additional testing and longer duration of antibiotic treatment [10]. Based on our
results, the NPV of a one-point measurement of I/T2 may be comparable with serial measurement
of CRP and should now be further evaluated in prospective studies. The I/T2 could then also be
added to an algorithm with serial measurement CRP in order to enhance NPV and clinical utility
of both markers [11]. Last, automated measurement of immature granulocytes performed at
least equal to manual differentiation [12]. The obvious advantages of automated measurement
are the large sample size, the immediate availability of test results for the clinician, and its cost-
effectiveness for the low-resource setting.
Because measurement of immature granulocytes was not part of standard care in Suriname,
the sample size for this study was relatively small. Larger and prospectively included cohorts are
necessary to increase prevalence of positive blood cultures and further controlling for maternal
(e.g., preeclampsia, mode of delivery) and neonatal (e.g., sex, ethnicity, hours of life) factors that
may influence leukocyte differentials [8,13]. However, we studied a homogeneous group of near
term and term newborns so we do not expect our results to differ in larger cohorts. Additionally,
establishing larger cohorts with blood culture confirmed EOS is complicated since prevalence of
positive bacterial blood cultures is low [1].
CONCLUSIONOur results indicate clinical utility of automated measurement of I/T and I/T2 in clinical decision-
making on start and duration of antibiotic treatment in EOS. Ultimately this may contribute to
reduction of the antibiotic burden in Suriname and other developing countries.
Abbreviations and Definitions
ANC = absolute neutrophil count
IG = immature granulocyte
IG% = immature granulocyte fraction of total leukocytes
I/T = immature-to-total-granulocyte ratio
I/T2 = immature-to-total-granulocyte ratio divided by the absolute neutrophil count
Maroon = descendant from Africans that escaped slavery and established independent societies
(e.g., term predominantly used in South America and on Caribbean Islands)
Acknowledgments
RZ was supported by a stipend from the Thrasher Research Fund (TRF13064) and from Tergooi
Hospitals, Blaricum, The Netherlands. The authors acknowled the efforts of all employees of
the Clinical Laboratory of the Academic Hospital Paramaribo for assistance with sample handling.
IMM
ATU
RE GR
AN
ULO
CY
TES IN SU
RINA
MESE N
EWBO
RNS
66
4
Author Contributions
R Zonneveld and FB Plötz designed the study. R Zonneveld, S Simson, A Juliana and J Codrington
collected and analyzed the data. R Zonneveld and FB Plötz drafted the manuscript. S Simson,
A Juliana and J Codrington revised and helped draft the final manuscript. All authors have read
and approved the final manuscript. The authors declare they have no conflict of interest.
IMM
ATU
RE GR
AN
ULO
CY
TES IN SU
RINA
MESE N
EWBO
RNS
67
4
REFERENCES
1. van Herk W, Stocker M, van Rossum AM.
Recognising early onset neonatal sepsis: an
essential step in appropriate antimicrobial use.
J Infect 2016, 72:S77-82.
2. Canty JB, Wozniak PS, Sanches PJ. Prospective
surveillance of antibiotic use in the neonatal
intensive care unit: results from the SCOUT
study. Pediatr Infect Dis J 2015, 34:267-72.
3. Hariharan S, Chen D, Harry C, Ragobar R,
Boodoosingh R, Gangoo C et al. Antimicrobial
prescription and usage in the neonatal
intensive care units of a Caribbean country:
a prospective observational study. J Neonatal
Perinatal Med 2013, 6(4):325-31.
4. Newman TB, Draper D, Puopolo KM, Wi S,
Escobar GJ. Combining immature and total
neutrophil counts to predict early onset sepsis
in term and late preterm newborns: Use of
the I/T2. Pediatr Infect Dis J 2014, 33:798–802.
5. Mikhael M, Brown LS, Rosenfeld CR. Serial
neutrophil values facilitate predicting
the absence of neonatal early-onset sepsis. J
Pediatr 2014, 164(3):522-8.
6. Zonneveld R, Molema G, Plötz FB. Analyzing
Neutrophil Morphology, Mechanics, and Motility in
Sepsis: Options and Challenges for Novel Bedside
Technologies. Crit Care Med 2016, 44(1):218-28.
7. Murphy K, Weiner J. Use of leukocyte counts
in evaluation of early-onset neonatal sepsis.
Pediatr Infect Dis J 2012, 31(1):16-9.
8. Newman TB, Puopolo KM, Wi S, Draper D,
Escobar GJ. Interpreting complete blood
counts soon after birth in newborns at risk for
sepsis. Pediatrics 2010, 126(5):903-909.
9. Hofer N, Zacharias E, Müller W, Resch B. An
update on the use of C-reactive protein in
early-Onset neonatal sepsis: Current insights
and new tasks. Neonatology 2012, 102:25–36.
10. Mukherjee A, Davidson L, Anguvaa L, Duffy
DA, Kennea N. NICE neonatal early onset
sepsis guidance: greater consistency, but more
investigations, and greater length of stay. Arch
Dis Child Fetal Neonatal Ed 2015, 100(3):F248-9.
11. Kerste M, Corver J, Sonnevelt MC, van Brakel
M, van der Linden PD, M Braams-Lisman BA et
al. Application of sepsis calculator in newborns
with suspected infection. J Matern Fetal
Neonatal Med 2016, 7:1-6.
12. MacQueen BC, Christensen RD, Yoder
BA, Henry E, Baer VL, Bennett ST et
al. Comparing automated vs manual
leukocyte differential counts for quantifying
the ‘left shift’ in the blood of neonates. J
Perinatol 2016, 36(10):843-8.
13. Wiland EL, Sandhaus LM, Georgievskaya Z,
Hoyen CM, O’Riordan MA, Nock ML. Adult
and child automated immature granulocyte
norms are inappropriate for evaluating
early-onset sepsis in newborns. Acta
Paediatr 2014, 103(5):494-7.
III The Vascular Pathophysiology of Early Onset Sepsis
5 Soluble Adhesion Molecules as Markers for Sepsis and the Potential
Pathophysiological Discrepancy in Neonates, Children and Adults
Rens Zonneveld, Roberta Martinelli, Nathan Shapiro, Taco W. Kuijpers, Frans B. Plötz, Christopher V. Carman
Critical Care 2014, 18:204
Editorial Comment in: McCulloh RJ, Spertus JA. Separating signal from noise: the challenge of
identifying useful biomarkers in sepsis. Crit Care 2014, 18(2):121
SOLU
BLE AD
HESIO
N M
OLEC
ULES IN
SEPSIS
76
5
ABSTRACTSepsis is a severe and life-threatening systemic inflammatory response to infection that affects
all populations and age groups. The pathophysiology of sepsis is associated with aberrant
interaction between leukocytes and the vascular endothelium. As inflammation progresses,
the adhesion molecules that mediate these interactions become shed from cell surfaces and
accumulate in the blood as soluble isoforms that are being explored as potential prognostic
disease biomarkers. We critically review the studies that have tested the predictive value of soluble
adhesion molecules in sepsis pathophysiology with emphasis on age, as well as the underlying
mechanisms and potential roles for inflammatory shedding. Five soluble adhesion molecules are
associated with sepsis, specifically, E-selectin, L-selectin and P selectin, intercellular adhesion
molecule-1 and vascular cell adhesion molecule-1. While increased levels of these soluble adhesion
molecules generally correlate well with the presence of sepsis, their degree of elevation is still
poorly predictive of sepsis severity scores, outcome and mortality. Separate analyses of neonates,
children and adults demonstrate significant age-dependent discrepancies in both basal and
septic levels of circulating soluble adhesion molecules. Additionally, a range of both clinical
and experimental studies suggests protective roles for adhesion molecule shedding that raise
important questions about whether these should positively or negatively correlate with mortality.
In conclusion, while predictive properties of soluble adhesion molecules have been researched
intensively, their levels are still poorly predictive of sepsis outcome and mortality. We propose
two novel directions for improving clinical utility of soluble adhesion molecules: the combined
simultaneous analysis of levels of adhesion molecules and their sheddases; and taking age-related
discrepancies into account. Further attention to these issues may provide better understanding of
sepsis pathophysiology and increase the usefulness of soluble adhesion molecules as diagnostic
and predictive biomarkers.
SOLU
BLE AD
HESIO
N M
OLEC
ULES IN
SEPSIS
77
5
INTRODUCTIONSepsis [1], due to its detrimental sequelae and limited therapeutic options, continues to be
responsible for many deaths amongst all age groups [2-4]. Growing evidence indicates that
aberrant leukocyte activation and recruitment into host tissues plays a pivotal role in causing
breakdown of the vascular endothelium [5], which in turn leads to organ failure and death [6].
Inflammatory leukocyte recruitment is initiated by soluble mediators (for example, cytokines
or bacterial-derived lipopolysaccharide (endotoxin)), which upregulate adhesion molecule
expression on both leukocytes and the endothelium. This upregulation results in a multistep
adhesion cascade whereby circulating immune cells sequentially roll on, firmly adhere to, and
transmigrate across the endothelium [7-9]. During the progression of inflammatory responses,
soluble isoforms of the leukocyte recruitment adhesion molecules are shed from cell surfaces and
accumulate within the circulating blood plasma [10]. These soluble isoforms have been considered
promising prognostic biomarkers of severity of inflammation but the clinical utility of monitoring
such changes remains poor [11].
One reason for the thus far limited clinical utility of these soluble isoforms is the fact that
shedding in general is neither a passive nor an inevitable consequence of upregulated expression/
cell activation. Most shedding is an active process, which is discretely regulated by diverse
proteolytic enzymes, although cell damage can also variably contribute to soluble adhesion
molecule levels [10]. Although still a matter of controversy, there is increasing evidence
that shedding serves regulatory roles to dampen inflammation (and specifically to reduce
leukocyte– endothelial interactions) and protect the host from excessive collateral damage
[10,12]. Furthermore, age-related differences in both levels of soluble adhesion molecules and
the enzymes that mediate shedding have been observed in both healthy and septic patients (as
discussed in detail below). The relationship between soluble adhesion molecule levels, underlying
inflammatory and shedding activities and clinical outcomes may thus be more complex than
once thought.
The goals of this review are therefore to summarize existing knowledge regarding
the mechanisms and putative functions for shedding of cell surface adhesion molecules/
generation of soluble isoforms, unequivocally identified to exist at elevated levels in the blood of
septic patients, and to investigate how these levels and their shedding differ amongst healthy and
septic neonates, children and adults to improve our understanding and clinical utility of soluble
adhesion molecules.
LITERATURE SEARCHWe performed a comprehensive literature search in MEDLINE using medical subject headings
and text words, supplemented by scanning the bibliographies of the recovered articles. We
combined ‘endothelium’ and ‘leukocytes’ using the term ‘OR’. This search was subsequently
combined with ‘sepsis’ using the Boolean operator ‘AND’. We used a similar search strategy, using
the terms ‘soluble’ and ‘circulating adhesion molecules’. We combined these results with the terms
‘neutrophils’, ‘lymphocytes’ and ‘inflammation’. We then combined these results with the terms
‘children’, ‘neonates’, ‘adults’ and ‘age’.
SOLUBLE ADHESION MOLECULES: FROM CELL SURFACE TO CIRCULATIONFive soluble adhesion molecules were associated with sepsis and their main characteristics are
summarized in Table 1. Three adhesion molecules (E-selectin, L-selectin and P-selectin) belong
to the selectin superfamily and function in leukocyte rolling (Figure 1). Two adhesion molecules
(intercellular adhesion molecule-1 (ICAM-1) and vascular cell adhesion molecule-1 (VCAM-1))
belong to the immunoglobin domain superfamily cell adhesion molecules that are important
for firm adhesion and transendothelial migration [13]. In all cases, inflammatory mediators (for
example, cytokines, thrombin, lipopolysaccharide) first increase cell surface expression of these
molecules followed by the later appearance of shed, soluble isoforms (Table 1 and Figure 2).
E-selectin
Soluble isoforms of E-selectin can be found in the supernatant of endothelial cells cultured in vitro
within 24 hours of cytokine activation and are generated through a largely caspase dependent
shedding process [10,14-16]. In healthy individuals low levels of soluble E-selectin (sE-selectin)
are found in serum, but these levels are greatly elevated in septic patients [16,17]. Importantly,
shed sE-selectin from sera of septic patients retained the ability to adhere to granulocytes in vitro
Table 1. Characteristics of adhesion molecules involved in sepsis
1. Decreased Cell Surface Density 2. Decoy Ligands
Lateral migration & Diapedesis
Sheddase
Figure 2. Shedding of selectin and immunoglobin superfamily adhesion molecules and its functional
implications. For simplification only one example receptor ligand pair (VLA-4/VCAM-1) is illustrated. A:
Interactions of cell surface integrin VLA-4, present on leukocytes, with endothelial cell surface VCAM-1 during
SOLU
BLE AD
HESIO
N M
OLEC
ULES IN
SEPSIS
80
5[16]. Shedding of E-selectin has thus been proposed to limit leukocyte–endothelial interactions
both by decreasing the cell surface density on the endothelium and by generating an intravascular
competitive inhibitor or decoy ligand (that is, sE-selectin) for leukocytes, thereby reducing
collateral damage in the host [18]. Indeed, one clinical study found that while sE-selectin was
elevated in septic children, those with the highest levels exhibited the best outcomes and survival
rates [19].
L-selectin
Within approximately 10 to 15 minutes of leukocyte activation by cytokines (for example, tumor
necrosis factor alpha) or lipopolysaccharide, soluble L-selectin (sL-selectin) is measurable in
the blood plasma as a result of cleavage by a disintegrin and metalloproteinase (ADAM)-17
[10,20,21]. Clinical studies show that L-selectin is shed and detected at elevated levels in the plasma
during the systemic inflammatory response [22]. Interestingly, Seidelin and colleagues [22] found
that the greatest survival was among septic adults that presented with the highest levels of sL-
selectin, and similar findings were made in another study focused on children [19]. Additionally,
in an in vitro fluid shear flow model, exogenously added sL-selectin inhibited leukocyte rolling
and firm adhesion to the endothelium in a dose dependent manner, presumably by competing
with cell surface L-selectin for binding of endothelial ligands [23]. Moreover, Ferri and colleagues
have demonstrated that systemic administration of exogenous sL-selectin to mice in vivo reduced
intravascular leukocyte rolling and adhesion, and as a consequence decreased vascular leak in
models of both local inflammation and sepsis [24-26]. Alternatively, addition of a small molecule
inhibitor of shedding increased leukocyte adhesion and vascular leak in the same settings [26].
The authors thus propose a significant protective role for L-selectin shedding in sepsis.
P-selectin
P-selectin is found within both endothelial cells and platelets [27,28]. As with the other selectins,
P-selectin can be measured in its soluble form in cell culture supernatants and in blood plasma,
with greater levels found in septic patient plasma [29]. Mechanisms for P-selectin shedding remain
poorly characterized, although some experimental data show that shedding of P-selectin might
occur through cleavage by matrix metalloproteinase in patients with cardiovascular disease or
hypertension [30,31]. The degree to which plasma soluble P-selectin (sP-selectin) is derived from
endothelial cells versus platelets remains unclear. However, one study found a strong positive
different steps in the leukocyte adhesion cascade; B: Ectodomain shedding of cell surface VCAM-1 (thereby
generating the soluble isoform sVCAM-1) by sheddases might reduce leukocyte adhesion to the endothelium
on two complementary levels: 1) reduction of cell surface density of adhesion molecules (e.g., decreased
endothelial cell surface VCAM-1, in this example); 2) binding of the resulting soluble isoforms to cell surface
ligands (i.e., binding of sVCAM-1 to leukocyte cell surface VLA-4, in this example), thereby serving as
competitive antagonists (or decoy ligands) for the remaining cell-surface adhesion receptors. See reference
11 and the text for more details on functional implications of shedding.
SOLU
BLE AD
HESIO
N M
OLEC
ULES IN
SEPSIS
81
5
correlation between coagulation (disseminated intravascular coagulation, fibrinogen consumption
and thrombin activation markers) and sP-selectin in septic patients, indicating a significant role
for platelet shedding of P-selectin [32]. Independently of its sources, sP-selectin could negatively
modulate direct leukocyte-endothelial interactions and/or indirect platelet mediated secondary
capture of leukocytes on the endothelium (both of which are dependent on P-selectin– platelet
selectin glycoprotein ligand-1 adhesion), although this remains to be tested directly [28].
Intercellular Adhesion Molecule-1
In vitro 1 to 6 hours after activation of endothelial cells by cytokines, soluble ICAM-1 (sICAM-1) can
be measured in culture supernatants, after shedding mediated by neutrophil elastase-dependent,
ADAM-17-dependent and matrix metalloproteinase-9-dependent shedding [10,33-35]. Shedding
of ICAM-1 is thought to promote detachment of leukocytes from the endothelium, thus limiting
local inflammation [10]. Indeed, addition of exogenous neutrophil elastase was shown to be
highly effective at cleaving surface-bound human ICAM-1 in vitro, which in turn abrogated Mac-
1-dependent leukocyte adhesion [36]. Evidence supports a potentially protective role for ICAM-1
shedding during sepsis. Elevated levels of sICAM-1 are well documented in human sepsis [5,6,11],
and studies performed in both humans and mice demonstrate that this is induced within ~
4 hours of endotoxin challenge [37-39]. Significantly, septic children with the highest levels of
sICAM-1 had better outcomes/survival rates [19], suggesting that shedding and loss of cell surface
ICAM-1 from the endothelium may serve a protective function. Interestingly, in a cecal ligation
puncture model of sepsis, ICAM-1-knockout mice – whereby cell-surface ICAM-1 is completely
abolished – exhibited a significant decrease in leukocyte tissue invasion, organ damage and
mortality compared with wild-type mice [37].
Vascular Cell Adhesion Molecule-1
In vitro 1 to 6 hours after cytokine activation, VCAM-1 is measurable in its soluble form (sVCAM-1) in
endothelial cell supernatant through shedding mediated by ADAM-17, cathepsin G and neutrophil
elastase [10]. Singh and colleagues demonstrate that this may be achieved, at least in part,
through the cytokine-mediated (that is, interleukin-1β -mediated and tumor necrosis factor alpha-
mediated) downregulation of tissue inhibitor metalloproteinase-3, which they showed to function
as a tonic suppressor of ADAM-17-mediated VCAM-1 shedding [40]. In response to endotoxin,
sVCAM-1 was observed to be markedly elevated in mice [38] and humans [39]. Furthermore,
increased levels of sVCAM-1 are reported in human sepsis, and higher levels seem to be associated
with increased severity of disease and non-survival [5,6]. Shedding of VCAM-1 is implicated to
counteract the pro-adhesive state of leukocytes to the endothelium both by lowering endothelial
receptor density [10] and by forming sVCAM-1 to act as a competitive inhibitor (or decoy receptor)
of leukocyte very late antigen-4 [40,41] (Figure 2). Interestingly, prednisolone – a synthetic
glucocorticoid shown to be beneficial in the treatment of sepsis – was shown to enhance sVCAM-1
levels, suggesting the intriguing possibility that its mechanism of action may be at least partially
related to potentiation of VCAM-1 shedding [39].
SOLU
BLE AD
HESIO
N M
OLEC
ULES IN
SEPSIS
82
5
LEVELS OF SOLUBLE ADHESION MOLECULES: IMPACT OF AGE Neonates
Basal levels of all soluble adhesion molecules of healthy neonates are comparable with (sICAM-1) or
higher than (sE-selectin, sP-selectin and sVCAM-1) basal levels in children or adults (Tables 2, 3, 4, 5
and 6 and Figure 3). Only the levels of sL-selectin are lower in neonates than in children or adults.
Importantly, in neonatal sepsis, levels of all soluble molecules are increased, but both the relative
and absolute extent of increase is remarkably lower compared with adults or children (Tables 2, 3,
4, 5 and 6 and Figure 3). This raises the important question of whether neonates are less effective
at shedding or less avidly upregulate adhesion molecules in the first place. Indeed, some studies
have been conducted to directly address this issue, which suggests contributions from both of
these mechanisms. Cell surface levels of L-selectin on neutrophils and sL-selectin levels from
cord blood were both lower than the cell surface and the circulating form of L-selectin found in
adult blood [42-44]. Interestingly, when challenged with neutrophil-activating chemoattractants,
neonatal neutrophils exhibited a significantly lower shedding response compared with adult
neutrophils [42,43]. Austgulen and colleagues suggest that these differences may be a reflection of
a developing immune system [45] that shows features of hyporesponsiveness (46). Since neonatal
sepsis/infection is particularly difficult to diagnose and no dependable predictors exist, sE-selectin
[45,47,48], sL-selectin [49,50] and sP-selectin [48,49] as well as sICAM-1 [50-59] and sVCAM-1 [49]
were evaluated as markers for the presence of infection in neonates. However, none of these
soluble isoforms were introduced in a clinical setting because they did not reach predictive ability.
The above discussion (and additional elaborations below) points toward complexities that need to
be resolved before meaningful interpretations can be made.
Children
Generally speaking, the basal levels of soluble adhesion molecules in healthy children are similar to
or lower than those of adults and neonates. However, both the relative amount and the absolute
amount of sE-selectin and sL-selectin during sepsis seem much higher, whereas sP-selectin
levels remain low. On the other hand, sICAM-1 and sVCAM-1 have similar basal levels and sepsis
generates comparable or higher levels versus adults (Tables 2, 3, 4, 5 and 6 and Figure 3). Three
studies assessed age-dependent differences in levels of selectins in healthy children [59,60,64].
Interestingly, infant had significantly lower levels of sL-selectin when compared with toddlers
(average age 2 years) [59]. Additionally, healthy children (age 9 to 15.5 years) were found to have
significantly decreasing sE-selectin levels with increasing age [64]. The authors of all three studies
suggest that potential developmental changes exist in both expression and shedding of selectins,
but that the physiological relevance of these observations remains to be determined.
During sepsis in children, studies show a significant increase in levels of soluble adhesion
molecules [19,61-63]. Interestingly, Briassoulis and colleagues show significant increase of sE-
selectin, as well as sL-selectin and ICAM-1, especially amongst survivors [19]. The authors conclude
that inadequate or suppressed shedding during sepsis might be associated with increased
mortality, and they hypothesize that the shedding process is indeed protective for the host.
SOLU
BLE AD
HESIO
N M
OLEC
ULES IN
SEPSIS
83
5
Tab
le 2
. Lev
els
of s
olu
ble
E-se
lect
in in
neo
nate
s, c
hild
ren
and
adul
ts
sE-s
elec
tin
Stud
y [r
efer
ence
]M
ean
ag
eSe
psi
s cr
iter
ia
Hea
lth
y
(ng
/ml)
1
Num
ber
of
pat
ien
ts (
hea
lth
y)
Sep
sis
(ng
/ml)
1
Num
ber
of
pat
ien
ts (
sep
sis)
Neo
nate
sD
olln
er e
t al
[52]
0-7
day
sC
linic
al91
.4 (
2-21
7.8)
2415
1.7
(37-
362.
2)18
Aus
tgul
en e
t al
[45]
Pre/
at te
rmC
linic
al13
4.1 (
69.5
-280
)16
818
7.7
(118
.4-2
62.2
)24
Edga
r et
al [
57]
0-7
day
sC
linic
al71
(51
-118
)27
135
(94-
192)
192
Gia
nnak
i et
al [4
7]A
t te
rmC
linic
al13
9 ±4
840
Edga
r et
al [
55]
At
term
Clin
ical
71 (
51-1
18)
4615
8 (9
4-20
7)46
Chi
ldre
nA
ndry
s et
al [
60]
6-10
57.6
(36
.7-1
52.2
)68
11-1
542
.1 (2
9.9-
114.
1)90
Paiz
e et
al [
61]
2-16
PRIS
M10
0 (
90-1
10)
4023
0 (
100
-380
)20
Kru
eger
et
al [6
2]3.
5 (0
.2-1
6)A
CC
P/SC
CM
68 (4
9-10
5)22
131 (
112-
146)
22
Wha
len
et a
l [63
]1d
to 17
yD
oug
hty
et a
l.246
±6
1423
077
Nas
h et
al [
64]
970
(35
-121
)81
1559
(25
-119
)
Bria
sso
ulis
et
al [1
9]6.
5 (2
.8)
PRIS
M16
1 ±43
1093
6 ±3
9910
Ad
ults
Pres
terl
et
al [6
5]51
(30
-67)
APA
CH
E II
48.9
(14
.3-8
9.9)
2013
0 (4
0-5
70)
20
Wei
gand
et
al [6
6]58
.7 (4
.4)
AC
CP/
SCC
M29
(14
.3-8
9.9)
785
14
Hyn
nine
n et
al [
67]
49 (
17.2
)A
PAC
HE
II73
(62
-89)
11
Kna
pp e
t al
[68]
51 (
21-9
6)A
PAC
HE
III43
.7 ±
20.3
1594
.5 ±
5428
Osm
ano
vic
et a
l [69
]A
dul
t28
.5 ±
14.3
1811
8 ±8
49
Sod
erq
uist
et
al [
70]
71 (
10-9
1)U
nkno
wn
48 (
20-9
7)15
80 (
22-2
00
)41
Taka
la e
t al
[71
]44
-59
(17-
86)
APA
CH
E II
45 (
10-1
00
)U
nkno
wn
154
(61-
394)
20
Gep
per
t et
al [
72]
59 (
35-8
5)SI
RS
42.8
±19
.47
96.2
±47
.327
De
Pabl
o e
t al
[73
]61
.2 (
3.2)
APA
CH
E II
4836
9852
Kay
al e
t al
[74
]57
.2 (
3.9)
AC
CP/
SCC
M40
.5 ±
4.5
923
1 ±41
.825
Shap
iro
et
al [6
]57
(19
)A
PAC
HE
III49
207
9513
And
rys
et a
l [60
]46
54.3
(8,
3-11
6.9)
68
Gia
nnak
i et
al [4
7]A
dul
t48
±13
40
AC
CP/
SCC
M =
Am
eric
an c
olle
ge o
f ch
est
phys
icia
ns/s
oci
ety
of
crit
ical
car
e m
edic
ine;
APA
CH
E =
acut
e ph
ysio
logy
and
chr
oni
c he
alth
eva
luat
ion;
PRI
SM =
ped
iatr
ic r
isk
of
mo
rtal
ity;
SIR
S =
syst
emic
infla
mm
ato
ry r
esp
ons
e sy
ndro
me.
Age
s ex
pres
sed
in y
ears
unl
ess
oth
erw
ise
stat
ed.
1 Dat
a pr
esen
ted
as
mea
n (r
ange
) o
r m
ean
± st
and
ard
dev
iati
on.
2 C
rite
ria
fro
m (
75).
SOLU
BLE AD
HESIO
N M
OLEC
ULES IN
SEPSIS
84
5
Tab
le 3
. Lev
els
of s
olu
ble
L-se
lect
in in
neo
nate
s, c
hild
ren
and
adul
ts
sL-s
elec
tin
Stud
y [r
efer
ence
]M
ean
ag
eSe
psi
s cr
iter
ia
Hea
lth
y
(ng
/ml)
1
Num
ber
of
pat
ien
ts (
hea
lth
y)
Sep
sis
(ng
/ml)
1
Num
ber
of
pat
ien
ts (
sep
sis)
Neo
nate
sFi
guer
as e
t al
[49]
0-1
4 d
ays
SNA
P-II
580
(52
3-71
7)12
681 (
541-
757)
15
Kour
tis
et a
l [50
]0
-2 d
ays
Clin
ical
1155
7513
31 (
1123
-142
7)14
Gia
nnak
i et
al [4
7]A
t te
rm67
4 ±2
2340
Rebu
ck e
t al
[43]
At
term
463
(338
-557
)22
Koen
ig e
t al
[42]
0-7
day
s32
4 ±2
410
Chi
ldre
nKo
urti
s et
al [
59]
Chi
ldre
n33
56 (
2818
-389
4)10
0
Bria
sso
ulis
et
al [1
9]6.
5 (2
.8)
PRIS
M37
50 ±
321
1062
63 ±
3813
10
Ad
ults
Wei
gand
et
al [6
6]58
.7 (4
.4)
AC
CP/
SCC
M46
07
400
14
Kour
tis
et a
l [50
]A
dul
t95
0 (
700
-122
0)
75
Schl
eiff
enba
um e
t al
[23]
Ad
ult
160
0 ±
800
63
Gia
nnak
i et
al [4
7]A
dul
t93
8 ±1
8140
Rebu
ck e
t al
[43]
Ad
ult
717
(410
-822
)22
Koen
ig e
t al
[42]
Ad
ult
537
±28
9
AC
CP/
SCC
M =
Am
eric
an c
olle
ge o
f che
st p
hysi
cian
s/so
ciet
y o
f cri
tica
l car
e m
edic
ine;
PRI
SM =
ped
iatr
ic r
isk
of m
ort
alit
y; S
NA
P =
sco
re fo
r ne
ona
tal a
cute
phy
sio
logy
. Age
s ex
pres
sed
in y
ears
unle
ss o
ther
wis
e st
ated
.1 D
ata
pres
ente
d a
s m
ean
(ran
ge)
or
mea
n ±
stan
dar
d d
evia
tio
n.
SOLU
BLE AD
HESIO
N M
OLEC
ULES IN
SEPSIS
85
5
Tab
le 4
. Lev
els
of s
olu
ble
P-se
lect
in in
neo
nate
s, c
hild
ren
and
adul
ts
sP-s
elec
tin
Stud
y [r
efer
ence
]M
ean
ag
eSe
psi
s cr
iter
ia
Hea
lth
y
(ng
/ml)
1
Num
ber
of
pat
ien
ts (
hea
lth
y)
Sep
sis
(ng
/ml)
1
Num
ber
of p
atie
nts
(sep
sis)
Neo
nate
sFi
guer
as e
t al
[49]
0-1
4 d
ays
SNA
P-II
272
(152
-288
)12
244
(170
-324
)15
Sita
ru e
t al
[48]
0 d
ays
Clin
ical
104
±71
1022
2 ±1
289
Chi
ldre
nPa
ize
et a
l [61
]2-
16PR
ISM
50 (4
4-60
)40
61 (4
7-11
9)20
Ad
ults
Mo
sad
et
al [3
2]3
SIR
S/SO
FA28
.6 ±
663
±9
176
Fijn
heer
et
al [2
9]A
dul
tSI
RS
122
±38
1039
8 ±2
03
26
Wei
gand
et
al [6
6]58
.7 (4
.4)
AC
CP/
SCC
M32
.1 ±5
.17
296
±56
14
Osm
ano
vic
et a
l [69
]A
dul
tU
nkno
wn
181 ±
4418
305
±158
9
Gep
per
t et
al [
72]
59 (
35-8
5)SI
RS
116.
9 ±3
3.4
729
1 ±22
7.427
Leo
ne e
t al
[76
]45
-47
(16-
21)
SIR
S62
±20
2612
9 ±9
811
AC
CP/
SCC
M =
Am
eric
an c
olle
ge o
f ch
est
phys
icia
ns/s
oci
ety
of
crit
ical
car
e m
edic
ine;
PRI
SM =
ped
iatr
ic r
isk
of
mo
rtal
ity;
SIR
S =
syst
emic
infla
mm
ato
ry r
esp
ons
e sy
ndro
me;
SN
AP
= sc
ore
fo
r
neo
nata
l acu
te p
hysi
olo
gy; S
OFA
= s
eque
ntia
l org
an fa
ilure
ass
essm
ent.
Age
s ex
pres
sed
in y
ears
unl
ess
oth
erw
ise
stat
ed.
1 Dat
a pr
esen
ted
as
mea
n (r
ange
) o
r m
ean
± st
and
ard
dev
iati
on.
SOLU
BLE AD
HESIO
N M
OLEC
ULES IN
SEPSIS
86
5
Tab
le 5
. Lev
els
of s
olu
ble
inte
rcel
lula
r adh
esio
n m
ole
cule
-1 in
neo
nate
s, c
hild
ren
and
adul
ts
sIC
AM
-1St
udy
[ref
eren
ce]
Mea
n a
ge
Sep
sis
crit
eria
Hea
lth
y
(ng
/ml)
1
Num
ber
of
pat
ien
ts (
hea
lth
y)
Sep
sis
(ng
/ml)
1
Num
ber
of p
atie
nts
(sep
sis)
Neo
nate
sFi
guer
as e
t al
[49]
0-1
4 d
ays
SNA
P-II
215
(156
-274
)12
426
(394
-458
)15
Ap
ost
olo
u et
al [
58]
At
term
Clin
ical
358.
4 ±2
8.9
1071
0.7
±56
.610
Do
llner
et
al [5
2]0
-7 d
ays
Clin
ical
244
(95.
2-50
0)
2441
3 (2
55.6
-50
0)
18
Aus
tgul
en e
t al
[45]
Pre/
at te
rmC
linic
al25
8.8
(94-
500
)16
839
4.2
(197
.5-5
00
)24
Bern
er e
t al
[51]
0-3
day
sC
linic
al42
1 (29
1-45
9)35
446
(171
-534
)13
6
Edga
r et
al [
57]
0-7
day
sC
linic
al16
5 (1
30-2
90)
2734
1 (23
6-55
4)19
2
Edga
r et
al [
56]
0-7
day
sC
linic
al20
546
406
46
Chi
ldre
nA
ndry
s et
al [
60]
6-10
346.
8 (2
06.
8-48
6.8)
68
11-1
526
9 (1
84.1-
354)
90
Paiz
e et
al [
61]
2-16
PRIS
M26
0 (
240
-30
0)
4070
5 (4
00
-850
)20
Wha
len
et a
l [63
]1d
to 17
yD
oug
hty
et a
l20
5 ±2
914
595
77
Nas
h et
al [
60]
931
0 (
280
-410
)81
1530
0 (
270
-390
)
Bria
sso
ulis
et
al [1
9]6.
5 (2
.8)
PRIS
M19
9 ±9
810
172
±93
10
Ad
ults
Wei
gand
et
al [6
6]58
.7 (4
.4)
AC
CP/
SCC
M19
07
110
014
Sod
erq
uist
et
al [
70]
71 (
10-9
1)U
nkno
wn
202
(62-
392)
1545
1 (21
6-10
30)
41
Sche
rper
eel e
t al
[77
]58
.9 (
14.9
)SA
PS II
2130
63
Ho
fer
et a
l [78
]65
.9 (
12.4
)A
PAC
HE
II21
9.6
(195
.2-2
85.1)
108
444.
7 (3
30-6
65.5
)18
De
Pabl
o e
t al
[73
]61
.2 (
3.2)
APA
CH
E II
480
3611
00
52
Kay
al e
t al
[74
]57
.2 (
3.9)
AC
CP/
SCC
M20
8 ±2
0.5
986
8 ±1
3125
Shap
iro
et
al [6
]57
(19
)A
PAC
HE
III18
520
724
013
And
rys
et a
l [60
]46
140
(60
.2-2
18.4
)68
Leo
ne e
t al
[76
]45
-47
(16-
21)
SIR
S15
126
824
11
SCC
M =
Am
eric
an c
olle
ge o
f che
st p
hysi
cian
s/ s
oci
ety
of c
riti
cal c
are
med
icin
e; A
PAC
HE
= ac
ute
phys
iolo
gy a
nd c
hro
nic
heal
th e
valu
atio
n; P
RISM
= p
edia
tric
ris
k o
f mo
rtal
ity;
SA
PS =
sim
plifi
ed
acut
e ph
ysio
logy
sco
re; S
IRS
= sy
stem
ic in
flam
mat
ory
res
po
nse
synd
rom
e; S
NA
P =
sco
re fo
r ne
ona
tal a
cute
phy
sio
logy
.1 D
ata
pres
ente
d a
s m
ean
(ran
ge)
or
mea
n ±
stan
dar
d d
evia
tio
n.
2 C
rite
ria
fro
m [
75].
Age
s ex
pres
sed
in y
ears
unl
ess
oth
erw
ise
stat
ed
SOLU
BLE AD
HESIO
N M
OLEC
ULES IN
SEPSIS
87
5
Tab
le 6
. Lev
els
of s
olu
ble
vasc
ular
cel
l adh
esio
n m
ole
cule
-1 in
neo
nate
s, c
hild
ren
and
adul
ts
sVC
AM
-1St
udy
[ref
eren
ce]
Mea
n a
ge
Sep
sis
crit
eria
Hea
lth
y
(ng
/ml)
1
Num
ber
of
pat
ien
ts (
hea
lth
y)
Sep
sis
(ng
/ml)
1
Num
ber
of p
atie
nts
(sep
sis)
Neo
nate
sFi
guer
as e
t al
[49]
0-1
4 d
ays
SNA
P-II
928
(856
-10
05)
1211
12 (
1072
-115
3)15
Aus
tgul
en e
t al
[45]
0-7
day
sC
linic
al19
40 (
110
0-3
500
)16
819
50 (
1190
-349
5)24
Chi
ldre
nA
ndry
s et
al [
60]
6 -1
5 ye
ars
590
.8 (
359.
6-82
2.0
)68
Paiz
e et
al [
61]
2.16
PRIS
M60
0 (
390
-790
)40
1550
(13
60-1
910
)20
Kru
eger
et
al [6
2]3.
5 (0
.2-1
6)A
CC
P/SC
CM
766
(644
-915
)22
1239
(92
8-16
15)
22
Wha
len
et a
l [63
]1d
to 17
yD
oug
hty
et a
l23
1 ±46
1460
077
Nas
h et
al [
64]
9 ye
ars
790
(58
0-1
060
)81
15 y
ears
780
(420
-10
00
)
Ad
ults
Pres
terl
et
al [6
5]51
APA
CH
E II
545
(374
-829
)20
2633
20
Kna
pp e
t al
[68]
51-5
5 (2
1-96
)A
PAC
HE
III56
9 ±9
815
1395
±80
128
Sod
erq
uist
et
al [
70]
71 (
10-9
1)U
nkno
wn
533
(354
-10
18)
1511
73 (
525-
350
0)
41
Ho
fer
et a
l [78
]65
.9 (
12.4
)A
PAC
HE
II15
24.7
(99
1.2-
2038
)10
811
47.9
(88
3.5-
2074
.4)
18
De
Pabl
o e
t al
[73
]61
.2 (
3.2)
APA
CH
E II
890
4816
00
52
Shap
iro
et
al [6
]57
(19
)A
PAC
HE
III10
5049
1550
95
And
rys
et a
l [60
]46
743
(338
-114
8)68
Leo
ne e
t al
[76
]45
-47
(16-
21)
SIR
S45
8 ±1
2326
160
4 ±9
4011
AC
CP/
SCC
M =
Am
eric
an c
olle
ge o
f ch
est
phys
icia
ns/
soci
ety
of
crit
ical
car
e m
edic
ine;
APA
CH
E, a
cute
phy
sio
logy
and
chr
oni
c he
alth
eva
luat
ion;
PRI
SM =
ped
iatr
ic r
isk
of
mo
rtal
ity;
SIR
S =
syst
emic
infla
mm
ato
ry r
esp
ons
e sy
ndro
me;
SN
AP
= sc
ore
for
neo
nata
l acu
te p
hysi
olo
gy.
1 Dat
a pr
esen
ted
as
mea
n (r
ange
) o
r m
ean
± st
and
ard
dev
iati
on.
2 C
rite
ria
fro
m [
75].
Age
s ex
pres
sed
in y
ears
unl
ess
oth
erw
ise
stat
ed.
SOLU
BLE AD
HESIO
N M
OLEC
ULES IN
SEPSIS
88
5
Similarly, in a large pediatric ICU study on microcirculatory dysfunction in meningococcal sepsis
in children, levels of sE-selectin, sVCAM-1 and sICAM-1, but not sP-selectin, were significantly
increased in septic patients but negatively correlated with the degree of microcirculatory
dysfunction (a measure of sepsis severity), as assessed by sublingual imaging [61].
Adults
Generally, basal levels of soluble adhesion molecules in adults are similar to or somewhat lower
than those of neonates and children (Tables 2, 3, 4, 5 and 6 and Figure 3). All molecules show
increase during sepsis, with sICAM-1 and sP-selectin exhibiting the greatest increases compared
with neonates and children. Age group stratification in levels of soluble adhesion molecules in
adults is limited. Rudloff and colleagues determined sICAM-1 levels in healthy adults between 18
and 65 years old and reported no age-dependent differences [79].
As discussed above, in a large number of clinical sepsis studies in adults, higher levels of
soluble adhesion molecules were generally related to severity of disease and mortality, although
statistically significant correlations could not be made [5,6,15-17,37,65-74,76-82]. Some studies imply
an alternate interpretation of these levels. For example, clinical studies have demonstrated that
septic adults with modest levels of soluble adhesion molecules (putatively reflecting inadequate/
aberrant shedding) had poorer outcome and higher mortality than those with the highest levels
[22,83]. Donnelly and colleagues found that critically ill patients with lower levels of sL-selectin had
a higher chance of developing adult respiratory distress syndrome [83], and Seidelin and colleagues
found that worse outcomes in septic patients correlated with lesser increases in sL-selectin levels
[22]. Interestingly, one experimental study found significantly decreased leukocyte–endothelial
interaction in a murine cecal ligation model of sepsis upon addition of exogenous sL-selectin into
the circulation at levels comparable with those found in septic adults [27].
ADHESION MOLECULE SHEDDASES IN SEPSIS: A DELICATE BALANCE The levels of adhesion molecules are an indirect result of protein cellular expression levels and
a direct result of the proteolytic activity of sheddases. Thus, as discussed above (for example, see
[42-44], expression and shedding activities can both independently contribute to overall levels
of soluble adhesion molecules in circulation. Several studies have independently assessed levels
of circulating sheddases and sheddase antagonists (that is, tissue inhibitor metalloproteinases) in
clinical and experimental sepsis in efforts to clarify their contribution to pathology. However, so
far these have yielded diverse and inconsistent results showing varied correlation of levels with
protection and pathology [84-88], suggesting a delicate balance is required.
The sensitive relationship between levels/activity of sheddases and outcome/effects in
the host during sepsis is best reflected by studies from Long and colleagues investigating
the role of ADAM-17 in L-selectin shedding in murine sepsis [12,89]. They found that ADAM-17
in mice acts as a homeostatic (rheostat) molecule to control their neutrophil infiltration at sites
of inflammation by regulating surface density of L-selectin. Low ADAM-17 activity results in little
SOLU
BLE AD
HESIO
N M
OLEC
ULES IN
SEPSIS
89
5
L-selectin shedding and too much neutrophil infiltration with subsequent collateral tissue damage.
However, excessive activity of ADAM-17 promotes excessive L-selectin shedding and subsequently
impairs neutrophil infiltration, which is needed to clear inflammation and infection.
Finally, evidence of age-related changes in sheddases and sheddase antagonists (that is,
tissue inhibitor metalloproteinases) has been observed. It is interesting to speculate that these
differences could partially underlie the observed age-related discrepancies in levels of soluble
adhesion molecules [90,91].
CONCLUSIONIncreased levels of soluble adhesion molecules generally correlate well with the presence of sepsis
in neonates, children and adults. However, their levels are still poorly predictive of sepsis severity
scores, outcome and mortality. Our review raises important issues that need further attention,
including age-related discrepancies in soluble adhesion molecule levels and even basic questions
about whether these should correlate positively or negatively with mortality.
First, there is a well-articulated hypothesis (and significant experimental support) that
shedding is indeed principally a homeostatic process that works to reduce inflammation and
promote resolution of inflammation (Figure 4). This is thought to act at two complementary
levels: removal of adhesion molecules from cell surfaces directly reduces the ability for cell–cell
interaction; and the resulting soluble isoforms serve as competitive antagonists (or decoy ligands)
for the remaining cell surface adhesion molecules.
Second, there is substantial evidence that disruption of shedding during sepsis, resulting
in substantially lower levels of soluble adhesion molecules (that is, retention of elevated cell
surface adhesion molecule levels), could lead to exacerbation of inflammation or promotion of
mortality (Figure 4C). Thus, as illustrated in Figure 4, there are many points during the progression
of an inflammatory response whereby the functional significance (with respect to the severity
of the underlying inflammation) of a given level of soluble adhesion molecule varies greatly. In
addition, levels of sheddases are also altered in human and experimental sepsis, suggesting putative
functional contribution for these changes in regulating disease progression. The interaction of
adhesion molecules and sheddases in the dynamic microenvironment of the cellular surfaces
implicates a strong interdependence of these molecules. However, to our knowledge, no studies
exist that combine the assessment of both adhesion molecules and their sheddases to assess
clinical outcome. Thus, a novel and potentially critical opportunity to enhance clinical efficacy of
soluble adhesion molecules exists that remains untapped. Such a combinatorial approach might be
particularly useful for improving both sepsis diagnosis (which is greatly needed for the challenging
situations in the febrile neonate or extreme older person) and our ability to track efficacy of
therapies. Furthermore, serial assessment of the combination of these markers might even be
effective in determining morbidity or mortality risk. Finally, it is interesting to consider whether
regulation of sheddases and adhesion molecules might be regulated in sepsis at the epigenetic
level, potentially offering additional ways to assess disease severity and predict outcomes [92].
SOLU
BLE AD
HESIO
N M
OLEC
ULES IN
SEPSIS
90
5
Additionally, the age-related and comorbidity-related heterogeneity in levels of soluble
adhesion molecules, as well as sheddases, in healthy individuals and septic patients could be an
expression of a different basal state, as well as different responsiveness in sepsis, potentially leading
to discrepancies in pathophysiology and disease progression between neonates, children or
adults. Interestingly, epidemiological research shows a biphasic pattern in age-related difference
in incidence and mortality [2-4]. The incidene of neonatal sepsis is 1 to 8 per 1,000 live births with
mortality rates of 16%. These rates decrease during childhood (0.2/1,000 children, mortality 10%)
and then increase in adults (26.2/1,000 in those over 85 years old, mortality 38.4%) [2-4]. A direct
correlation between these rates and levels of soluble adhesion molecules remains speculative, but
further attention to this could provide new insights.
In conclusion, while predictive properties of soluble adhesion molecules have been researched
intensively, their levels are still poorly predictive of sepsis outcome and mortality. We propose
two novel directions for improving clinical utility of soluble adhesion molecules: the combined
simultaneous analysis of levels of adhesion molecules and their sheddases; and taking age-
related discrepancies into account. Additional investigation of these issues may provide better
understanding of the pathophysiology of sepsis and increased usefulness of soluble adhesion
molecules as diagnostic and predictive biomarkers.
15. Zonneveld R, Jongman R, Juliana A, Zijlmans W,
Plötz FB, Molema G, Van Meurs M. Low Serum
Angiopoietin-1, high Angiopoietin-2, and high
Ang-2/Ang-1 Protein Ratio are Associated with
Early Onset Sepsis in Surinamese Newborns.
Shock 2017, in press.
16. Fattah MA, Omer AF, Asaif S, Manlulu R, Karar T,
Ahmed A, Aljada A, Saleh AM, Qureshi S, Nasr A.
Utility of cytokine, adhesion molecule and acute
phase proteins in early diagnosis of neonatal
sepsis. J Nat Sci Biol Med 2017, 8(1):32-39.
17. Weitkamp JH, Guthrie SO, Wong HR,
Moldawer LL, Baker HV, Wynn JL. Histological
chorioamnionitis shapes the neonatal
transcriptomic immune response. Early Hum
Dev 2016, 98:1-6.
18. Wynn JL, Guthrie SO, Wong HR, Lahni P,
Ungaro R, Lopez MC, Baker HV, Moldawer
LL. Postnatal Age Is a Critical Determinant of
the Neonatal Host Response to Sepsis. Mol
Med. 2015;21:496–504
19. Sugitharini V, Prema A, Berla Thangam
E. Inflammatory mediators of systemic
inflammation in neonatal sepsis. Inflamm
Res 2013, 62(12):1025-34.
20. Edgar JDM, Gabriel V, Gallimore JR,
McMillan SA, Grant J. A prospective study
of the sensitivity, specificity and diagnostic
performance of soluble intercellular adhesion
molecule 1, highly sensitive C-reactive
protein, soluble E-selectin and serum amyloid
A in the diagnosis of neonatal infection. BMC
Pediatr 2010, 16:10–22.
AD
HESIO
N M
OLEC
ULE SH
EDD
ING
IN SU
RINA
MESE N
EWBO
RNS
111
6
21. Fukunaga S, Ichiyama T, Maeba S, Okuda M,
Nakata M, Sugino N, Furukawa S. MMP-9 and
TIMP-1 in the cord blood of premature infants
developing BPD. Ped Pulm 2009, 44: 267-272.
22. Sunagawa S, Ichiyama T, Honda R,
Fukunaga S, Maeba S, Furukawa S. Matrix
metalloproteinase-9 and tissue inhibitor of
metalloproteinase-1 in perinatal asphyxia.
Brain Dev 2009, 31(8):588-93.
23. Figueras-Aloy J, Gómez-López L, Rodríguez-
Miguélez JM, Salvia-Roiges MD, Jordán-
García I, Ferrer-Codina I, Carbonell-Estrany X,
Jiménez-González R. Serum soluble ICAM-1,
VCAM-1, L-selectin and P-selectin levels
as markers of infection and their relation
to clinical severity in neonatal sepsis. Am J
Perinat 2007, 24:331–338.
24. Sitaru AG, Speer CP, Holzhauer S, Obergfell
A, Walter U, Grossmann R. Chorioamnionitis
is associated with increased CD40L
expression on cord blood platelets. Thromb
Haemost 2005, 94(6):1219-23.
25. Schulz CG, Sawicki G, Lemke RP, Roeten BM,
Schulz R, Cheung PY. MMP-2 and MMP-9
and their tissue inhibitors in the plasma
of preterm and term neonates. Pediatr
Res 2004, 55(5):794-801.
26. Edgar JDM, Gabriel V, Craig A, Wheeler D,
Thomas M, Grant J. A low serum sICAM-1
level may assist in the exclusion of neonatal
infection. Biol Neonate 2002, 81:105–108.
27. Apostolou M, Dimitriou H, Kaleyias J,
Perdikogianni C, Stiakaki E, Costalos C,
Kalmanti MC. Levels of soluble ICAM-1 in
premature and full-term neonates with
infection. Mediators Inflamm 2002, 11:95–98.
28. Dollner H, Vatten L, Austgulen R. Early diagnostic
markers for neonatal sepsis: comparing
C-reactive protein, interleukin-6, soluble tumor
necrosis factor receptors and soluble adhesion
molecules. J Clin Epidemiol 2001, 54:1251–1257.
29. Malamitsi-Puchner A, Tziotis J, Mastorakos
G, Protonotariou E, Creatsas G. Adhesion
molecules in early neonatal life. Biol
Neonate 2000, 78(1):65-7.
30. Giannaki G, Rizos D, Xyni K, Sarandakou A,
Protonotariou E, Phocas I, Creatsas G. Serum
soluble E-and L-selectin in the very early neonatal
period. Early Hum Develop 2000, 60:149–155.
31. Giannaki G, Xyni K, Rizos D, Phocas I.
Comparative study of serum soluble VCAM-1
and ICAM-1 levels in the early neonatal period.
Acta Paediatr 1999, 88(12):1413-4.
32. Phocas I, Sarandakou A, Giannaki G, Malamitsi-
Puchner A, Rizos D, Zourlas PA. Soluble
intercellular adhesion molecule-1 in newborn
infants. Eur J Pediatr 1998, 157(2):153-6.
33. Berner R, Niemeyer CM, Leititis JU, Funke A,
Schwab C, Rau U, Richter K, Tawfeek MS, Clad A,
Brandis M. Plasma levels and gene expression
of granulocyte colony-stimulating factor,
tumor necrosis factor-(alpha), interleukin
(IL)-1(beta), IL-6, IL-8, and soluble intercellular
adhesion molecule-1 in neonatal early onset
sepsis. Pediatr Res 1998, 44:469–477.
34. Austgulen R, Arntzen KJ, Haereid PE, Aag S,
Døllner H. Infections in neonates delivered
at term are associated with increased
serum levels of ICAM-1 and E-selectin. Acta
Pediatr 1997, 86:274–280.
35. Lim FT, van Winsen L, Willemze R, Kanhai
HH, Falkenburg JH. Influence of delivery
on numbers of leukocytes, leukocyte
subpopulations, and hematopoietic
progenitor cells in human umbilical cord
blood. Blood Cells 1994,20(2-3):547-58;
discussion 558-9.
36. Lim FT, Scherjon SA, van Beckhoven JM, Brand
A, Kanhai HH, Hermans JM, Falkenburg JH.
Association of stress during delivery with
increased numbers of nucleated cells and
hematopoietic progenitor cells in umbilical cord
blood. Am J Obstet Gynecol 2000, 183(5):1144-52
37. Duijts L, Bakker-Jonges LE, Labout JA, Jaddoe VW,
Hofman A, Steegers EA, Van Dongen JJ, Hooijkaas
H, Moll HA. Perinatal stress influences lymphocyte
subset counts in neonates. The generation R
study. Pediatr Res 2008, 63(3):292-8.
38. Beyrau M, Bodkin JV, Nourshargh S.
Neutrophil heterogeneity in health and
disease: a revitalized avenue in inflammation
and immunity. Open Biol 2012, 2(11):120134.
39. Brown KA, Brain SD, Pearson JD, Edgeworth
JD, Lewis SM, Treacher DF. Neutrophils in
AD
HESIO
N M
OLEC
ULE SH
EDD
ING
IN SU
RINA
MESE N
EWBO
RNS
112
6
development of multiple organ failure in
sepsis. Lancet 2006, 368(9530):157-69.
40. Shapiro NI, Yano K, Sorasaki M, Fischer
C, Shih SC, Aird WC. Skin biopsies
demonstrate site-specific endothelial
activation in mouse models of sepsis. J Vasc
Res 2009, 46(5):495-502.
41. Csonka K, Vadovics M, Marton A, Vágvölgyi C,
Zajta E, Tóth A, Tóth R, Vizler C, Tiszlavicz L,
Mora-Montes HM, Gácser A. Investigation of
OCH1 in the Virulence of Candida parapsilosis
Using a New Neonatal Mouse Model. Front
Microbiol 2017, 8:1197.
42. Molina-Berríos A, Campos-Estrada C, Lapier
M, Duaso J, Kemmerling U, Galanti N, Ferreira
J, Morello A, López-Muñoz R, Maya JD.
Protection of vascular endothelium by aspirin
in a murine model of chronic Chagas’ disease.
Parasitol Res 2013, 112(7):2731-9.
AD
HESIO
N M
OLEC
ULE SH
EDD
ING
IN SU
RINA
MESE N
EWBO
RNS
113
6
SUPPLEMENTAL DATA
Supplemental Table 1. Descriptive statistics of the study group (n=91)
Controls
(n=20)
Early Onset Sepsis
P-value
Blood Culture
Negative (n=65)
Blood Culture
Positive (n=6)
Pregnancy, n (%) Complications1
Chorioamnionitis2
3 (15)
0
16 (25)
18 (28)
1 (17)
0
0.63
Mode of delivery,
n (%)
Vaginal
Caesarean
12 (60)
8 (40)
46 (75)
19 (25)
4 (67)
2 (33)
0.54
Sex, n (%) Male
Female
9 (45)
11 (55)
29 (45)
36 (55)
5 (83)
1 (17)
0.19
Ethnicity, n (%) Maroon and Creole
Hindo-Surinamese
Other3
12 (60)
3 (15)
5 (25)
44 (68)
14 (21)
7 (11)
4 (67)
1 (17)
1 (17)
0.61
Gestational age,
n (%) (weeks)
34-37
37-40
≥40
1 (5)
14 (70)
5 (25)
22 (34)
30 (46)
13 (20)
0
4 (67)
2 (33)
0.06
Apgar score, n (%) <5 0 5 (8) 2 (33) 0.03
Birth weight, Median
(IQR) (grams)
3130 (700) 2840 (835) 3500 (906) 0.02
Age at presentation,
n (%) (hours)
<24
24-48
48-72
4 (20)
7 (35)
9 (45)
43 (66)
13 (20)
9 (14)
2 (33)
1 (17)
3 (50)
<0.01
Clinical course
(at 48-72h), n (%)
CPAP
Mechanical Ventilation
Cardiotonics
Mortality
0
0
0
0
9 (14)
7 (11)
5 (8)
3 (5)
0
2 (33)
1 (17)
2 (33)
<0.001
CPAP = continuous positive airway pressure; N/A = not applicable. 1 Presence of pregnancy-induced hypertension, preeclampsia or diabetes mellitus.2 Defined as intrapartum fever or administration of antibiotics.3 Includes: Javanese, Chinese, Caucasian and Amerindian.
AD
HESIO
N M
OLEC
ULE SH
EDD
ING
IN SU
RINA
MESE N
EWBO
RNS
114
6
Sup
ple
men
tal T
able
2. S
tudi
es r
epo
rtin
g le
vels
of e
ndo
thel
ial c
ell a
dhes
ion
mo
lecu
les
and
shed
ding
enz
ymes
in n
ewb
orn
s
Stud
y [r
ef.]
, yea
r
CA
M o
r
shed
din
g e
nzy
me
Co
ho
rt
Ch
arac
teri
stic
s
Ges
tati
on
al
age
(wee
ks)
Post
nat
al
age
Mai
n R
esul
ts
An
alys
is
Met
ho
d
Hea
lth
y
(ng
/mL)
1
Sep
tic
(ng
/mL)
1
Fata
h et
al.
[16]
,
2017
sE-s
elec
tin
EOS
and
LO
SN
SN
SsE
-sel
ecti
n el
evat
ed in
BC
PSEL
ISA
148.
9 ±
7.917
7.1 ±
3.5
Wei
tkam
p et
al.
[17]
, 20
16
MM
P-9
EOS
and
LO
S25
-36
< an
d ≥
3
day
s
MM
P-9
leve
ls lo
wer
in B
CPS
M
ulti
plex
bea
d
assa
y
NS
NS
Wyn
n et
al.
[18]
,
2015
MM
P-9
Cho
rio
amni
oni
tis
25-3
6N
SM
MP-
9 le
vels
low
er in
cho
rio
amni
oni
tis
Mul
tipl
ex b
ead
assa
y
NS
NS
Sugi
thar
ini e
t al
.
[19]
, 20
13
sIC
AM
-1, N
EEO
S34
-42
0-7
2 ho
urs
sIC
AM
-1 a
nd N
E el
evat
ed
in E
OS
ELIS
A
Ant
ibo
dy
arra
y
sIC
AM
-1/
NE:
NS
sIC
AM
-1: N
S
NE:
499.
2±22
.0
Edga
r et
al.
[20
],
2010
sIC
AM
-1, s
E-se
lect
inEO
S an
d L
OS
24-4
1N
SsI
CA
M-1
and
sE-
sele
ctin
elev
ated
ELIS
AsI
CA
M-1
: 165
(130
-290
)
sE-s
elec
tin:
71
(51-
118)
sIC
AM
-1: 4
05
(252
-666
)
sE-s
elec
tin
158
(94-
207)
Fuka
naga
et
al.
[21]
, 20
09
MM
P, T
IMP-
1U
ninf
ecte
d
new
bo
rns
<30
Co
rd
blo
od
No
diff
eren
ceEL
ISA
MM
P-9:
22
(16-
48)
TIM
P-1:
122
(86-
249)
NS
Suna
gaw
a et
al.
[22]
, 20
09
MM
P-9,
TIM
P-1
Uni
nfec
ted
new
bo
rns
35-4
11-
2 d
ays
NA
ELIS
AN
SN
A
Figu
eras
et
al.
[23]
, 20
07
sIC
AM
-1, s
VC
AM
-1,
sP-s
elec
tin,
EOS
and
LO
S32
-40
1-32
day
ssI
CA
M-1
and
sV
CA
M-1
incr
ease
d o
ver
tim
e.
ELIS
AsI
CA
M-1
: 156
(150
-194
)
sVC
AM
-1: 8
56
(742
-960
)
sP-s
elec
tin:
272
(152
-288
)
sIC
AM
-1: 3
94
(342
-60
0)
sVC
AM
-1: 1
153
(726
-130
7)
sP-s
elec
tin:
244
(170
-324
)
Sita
ru e
t al
. [24
],
200
5
sP-s
elec
tin
Cho
rio
amni
oni
tis
25-4
0C
ord
blo
od
sP-s
elec
tin
elev
ated
in
cho
rio
amni
oni
tis
ELIS
A10
4 ±
7122
2 ±
128
AD
HESIO
N M
OLEC
ULE SH
EDD
ING
IN SU
RINA
MESE N
EWBO
RNS
115
6
Sup
ple
men
tal T
able
2. (
cont
inue
d)
Stud
y [r
ef.]
, yea
r
CA
M o
r
shed
din
g e
nzy
me
Co
ho
rt
Ch
arac
teri
stic
s
Ges
tati
on
al
age
(wee
ks)
Post
nat
al
age
Mai
n R
esul
ts
An
alys
is
Met
ho
d
Hea
lth
y
(ng
/mL)
1
Sep
tic
(ng
/mL)
1
Schu
lz e
t al
. [25
],
200
4
MM
P-9,
TIM
P-1
Uni
nfec
ted
new
bo
rns
25-4
01-
28 d
ays
MM
P-9
high
est
in p
rete
rm
TIM
P-1 h
ighe
st in
at
term
ELIS
AN
SN
A
Edga
r et
al.
[26]
,
200
2
sIC
AM
-1EO
S an
d L
OS
24-4
2N
SsI
CA
M-1
ele
vate
d in
BC
PSEL
ISA
205
(146
-343
)40
6 (3
45-1
180
)
Ap
ost
olo
u et
al.
[27]
, 20
02
sIC
AM
-1EO
S an
d L
OS
25-4
2N
SsI
CA
M-1
ele
vate
d in
BC
PS
ELIS
A35
8.4
± 28
.971
0.7
± 5
6.6
Do
llner
et
al. [
28],
200
1
sIC
AM
-1, s
E-se
lect
inEO
S an
d L
OS
30-4
21-
7 d
ays
sIC
AM
-1 a
nd s
E-se
lect
in
elev
ated
in B
CPS
ELIS
AsI
CA
M-1
: 244
.0
(92.
5-50
0)
sE-s
elec
tin:
91.4
(<2.
0-2
17.8
)
sIC
AM
-1: 3
57.4
(141
.6-5
00
)
sE-s
elec
tin:
151.
7 (3
7.0
-
362.
2)
Mal
amit
si e
t al
.
[29]
, 20
00
sVC
AM
-1, s
PEC
AM
-1U
ninf
ecte
d
new
bo
rns
37-4
01-
5 d
ays
No
cha
nge
bet
wee
n d
ay 1
and
5
ELIS
AsV
CA
M-1
: 134
0
± 58
.3
sPEC
AM
-1: 1
7.5
± 0
.7
NA
Gia
nnak
i et
al.
[30
], 2
00
0
sE-s
elec
tin
Uni
nfec
ted
new
bo
rns
At
term
1-5
day
ssE
-sel
ecti
n d
ecre
ases
bet
wee
n d
ay 1
and
5
ELIS
A13
9 ±
48N
A
Gia
nnak
i et
al.
[31]
, 199
9
sIC
AM
-1, s
VC
AM
-1U
ninf
ecte
d
new
bo
rns
At
term
1-5
day
ssI
CA
M-1
and
sV
CA
M-1
incr
ease
bet
wee
n d
ay 1
and
5
ELIS
AsI
CA
M: 1
79 ±
56.1
sVC
AM
-1: 1
125.
0
± 28
1.0
NA
Pho
cas
et a
l. [3
2],
1998
sIC
AM
-1U
ninf
ecte
d
new
bo
rns
35-4
21-
30 d
ays
sIC
AM
-1 in
crea
ses
bet
wee
n
day
1, 5
and
30
ELIS
A13
7.3
± 62
.0N
A
Bern
er e
t al
. [33
],
1998
sIC
AM
-1EO
S26
-42
0-9
6
hour
s
sIC
AM
-1 lo
wer
in E
OS.
sIC
AM
-1 in
crea
ses
ove
r ti
me
ELIS
A42
1 (29
1-45
9)44
6 (1
71-5
34)
AD
HESIO
N M
OLEC
ULE SH
EDD
ING
IN SU
RINA
MESE N
EWBO
RNS
116
6
Sup
ple
men
tal T
able
2. (
cont
inue
d)
Stud
y [r
ef.]
, yea
r
CA
M o
r
shed
din
g e
nzy
me
Co
ho
rt
Ch
arac
teri
stic
s
Ges
tati
on
al
age
(wee
ks)
Post
nat
al
age
Mai
n R
esul
ts
An
alys
is
Met
ho
d
Hea
lth
y
(ng
/mL)
1
Sep
tic
(ng
/mL)
1
Aus
tgul
en e
t al
.
[34]
, 199
7
sIC
AM
-1, s
VC
AM
-1,
sE-s
elec
tin
EOS
and
LO
S,
pneu
mo
nia
24-4
20
-162
hour
s
sE-s
elec
tin
and
sIC
AM
-1
elev
ated
in in
fect
ed
neo
nate
s
ELIS
AsE
-sel
ecti
n: 8
4.2
(21.
6-23
1.3)
sIC
AM
-1: 2
131.
3
(144
9.5-
350
0.0
)
sVC
AM
-1: 2
37.0
(122
.0-5
00
.0)
NS
CA
M =
end
oth
elia
l ce
ll ad
hesi
on
mo
lecu
le;
sVC
AM
-1 =
so
lubl
e V
ascu
lar
Cel
l A
dhe
sio
n M
ole
cule
-1;
sIC
AM
-1 =
so
lubl
e In
terc
ellu
lar
Ad
hesi
on
Mo
lecu
le-1
; N
E =
neut
roph
il el
asta
se N
A =
No
t
avai
labl
e; N
S =
No
t sp
ecifi
ed; E
OS
= Ea
rly
Ons
et S
epsi
s; L
OS
= La
te O
nset
Sep
sis;
BC
PS =
Blo
od
Cul
ture
Po
siti
ve S
epsi
s.a Le
vels
are
in m
ean
± SD
, mea
n ±
SEM
, med
ian
(int
erq
uart
ile r
ange
), o
r m
edia
n (r
ange
).
7 Low Serum Angiopoietin-1, high Angiopoietin-2, and high Ang-2/Ang-1
Protein Ratio are Associated with Early Onset Sepsis in Surinamese Newborns
Rens Zonneveld, Rianne M. Jongman, Amadu Juliana, Wilco Zijlmans, Frans B. Plötz,
Grietje Molema, Matijs van Meurs
Shock 2017, May 22
AN
GIO
POIETIN
S IN SU
RINA
MESE N
EWBO
RNS
120
7
ABSTRACTPurpose
Vascular inflammation and leakage in sepsis is mediated by Angiopoietin-1 (Ang-1) and -2 (Ang-2)
and their phosphorylation of the endothelial Tie-2 receptor. Levels of Ang-2 change in adults and
children during sepsis, which is associated with severity of sepsis. This study investigates levels of
Ang-1 and Ang-2 in newborns to gain insight in the vascular pathophysiology of early onset sepsis
(EOS) within 72 hours after birth.
Methods
A prospective cohort study was performed amongst 71 Surinamese newborns treated with
antibiotics for suspected EOS and 20 control newborns. Newborns with suspected EOS were
divided in two groups: blood culture negative and positive EOS. Ang-1 and Ang-2 levels were
measured in serum obtained at start of antibiotic treatment and at reevaluation after 48-72 hours.
Results
In this cohort 8.5% of newborns had a positive blood culture. At start of antibiotic treatment
Ang-1 serum levels were lower (P<0.01), and Ang-2 and Ang-2/Ang-1 serum protein ratios higher
(P<0.01 and P<0.01, respectively) in newborns with blood culture positive EOS than in controls.
These levels were not dependent on timing of first blood draw after birth. After 48-72 hours levels
of Ang-1 further decreased in blood culture positive EOS, while in the other groups no change
was observed.
Conclusions
Our findings support the hypothesis that a dysbalance in the Angiopoietins plays a role in
the vascular pathophysiology of EOS.
AN
GIO
POIETIN
S IN SU
RINA
MESE N
EWBO
RNS
121
7
INTRODUCTIONSepsis is a syndrome with physiologic, pathological and biochemical changes induced by an
infection, and occurs in all age groups [1]. Early onset sepsis (EOS) in newborns, defined as onset
of sepsis within 72 hours after birth, remains a clinical diagnostic and therapeutic challenge due
to its non-specific clinical presentation. This is associated with late discovery and undertreatment
of septic newborns or overtreatment with antibiotics of uninfected ones [2-4]. These diagnostic
and therapeutic problems arise because the pathophysiology of EOS is not completely
understood [3-5].
One of the pathological changes in septic patients is microvascular dysfunction leading to
increased vascular inflammation and leakage [6]. Vascular endothelial cells control these changes
through the Angiopoietin/Receptor Tyrosine Kinase (Tie)-2 endothelial receptor system, which
is severely disturbed in sepsis [6,7-9]. The system consists of the ligands Angiopoietin-1 (Ang-1)
and -2 (Ang-2) [9]. In health, Ang-1-Tie2 binding promotes intracellular Tie-2 phosphorylation,
which prevents the occurrence of vascular inflammation and vascular leakage [10]. During sepsis,
Ang-2 dose dependently competes with Ang-1, which inhibits Tie-2 phosphorylation and induces
destabilizing vascular inflammation and leakage [11,12]. In sepsis in children and adults, higher
Ang-2 levels and Ang-2/Ang-1 ratios in blood are associated with presence, severity and outcome of
sepsis, while changes in Ang-1 levels are less uniformly present [13-17]. To date, there is insufficient
knowledge if disturbances in the Angiopoietin/Tie2 system also reflect the activation state of
the endothelium during EOS in newborns [18]. Furthermore, no data exists on the Angiopoietins
during EOS from non-Western countries, such as Suriname.
Therefore, we studied the levels and behavior of Ang-1 and Ang-2 at start of antibiotic
treatment and at reevaluation between 48 to 72 hours in Surinamese newborns with suspected
EOS. We hypothesized that lower Ang-1 and higher Ang-2 and Ang-2/Ang-1 protein ratio were
associated with blood culture positive EOS.
MATERIALS AND METHODSStudy Design and Subjects
A prospective observational cohort study was performed at the neonatal care facility of
the Academic Pediatric Center Suriname at the Academic Hospital Paramaribo. Patients
were included in a 14-month period between April 1st 2015 and May 31st 2016. Newborns with
a gestational age (GA) equal to or above 34 weeks in whom antibiotics were started within the first
72 hours of life for suspected EOS were included. Excluded were neonates of whom no serum was
obtained or not enough information was available after the study period to confirm outcomes.
Written informed consent was obtained from at least one parent for the use of residual serum
and clinical information. The study protocol was approved by the Surinamese Medical-Ethical
Board (VG-021-14A) and was made available on clinicaltrials.gov (Trial registration: NCT02486783
registered 27/6/2015).
AN
GIO
POIETIN
S IN SU
RINA
MESE N
EWBO
RNS
122
7
Clinical Protocol
For all newborns, the standard local protocol for the management of suspected EOS was followed.
This included the start of antibiotics after blood collection for culture and serial laboratory testing
of infectious parameters (t=0). Intravenous ampicillin (50-75 mg/kg/day) and gentamycin (5 mg/
kg/day) were started based on the presence of maternal risk factors for infection (i.e., positive
group B streptococcus culture, (premature) prolonged rupture of membranes, intrapartum
fever or intrapartum antibiotics) and/or clinical signs of infection of the newborn. Controls
were newborns without signs of infection receiving blood draws for hyperbilirubinemia. In these
controls, no antibiotics were started. Newborns in whom antibiotics were started were divided
in two groups based on blood culture result: 1) blood culture negative EOS and 2) blood culture
positive EOS.
Data Collection
For all newborns maternal information (i.e., history, pregnancy complications (i.e., presence of
diabetes mellitus, pregnancy-induced hypertension (PIH) or preeclampsia (PE)) and maternal risk
factors for infection) were recorded, along with gestational age (if unknown according to Ballard),
cloacae (n=2) and Escherichia coli (n=2). Newborns with EOS received respiratory and circulatory
support more often than controls (P<0.001). A total of five newborns with EOS died. White
blood cell, neutrophil and trombocyte counts and CRP levels were not different between groups
(Table 2).
Levels of Angiopoietins
At t=0, median levels of Ang-1 were significantly lower in blood culture positive EOS (28.3 (28.0)
ng/mL) versus controls (77.4 (65.2) ng/mL), P<0.01 (Table 2) (Figure 1A). Median Ang-2 levels
were higher in blood culture EOS (21.1 (13.3) ng/mL) versus controls (10.2 (1.9) ng/mL), P<0.001,
respectively) (Figure 1B). The Ang-2/Ang-1 protein ratio was higher in blood culture positive EOS
(median (IQR) 0.77 (0.77) versus controls (median (IQR) 0.13 (0.13) (P<0.01) (Figure 1C). There was
no difference in median levels of Ang-1, Ang-2 and Ang-2/Ang-1 protein ratio between blood
culture negative EOS and controls.
At t=48-72h, median Ang-1 levels had decreased 21-fold in blood culture positive EOS from
levels at t=0 (P=0.10), while median Ang-2 levels remained high (P=0.99) (Table 2) (Figure 1A-B).
Median levels of Ang-1, Ang-2 and Ang-2/Ang-1 protein ratio were not different when comparing
blood culture positive or blood culture negative EOS with controls.
Levels of Ang-1 and Ang-2 were tested for dependency on timing of first blood draw (t=0) after
birth. For controls and EOS (blood culture negative plus blood culture positive EOS) median levels
at t=0 were not different between newborns if t=0 was before 24 hours or between 24-72 hours
after birth (Figure 2A-B).
Because CRP levels at t=48-72h increased from levels at t=0 in blood culture negative
and positive EOS (Table 2), correlation of Ang-1 and Ang-2 with CRP was assessed amongst 44
newborns with blood culture negative (n=42) and positive (n=2) EOS in whom all data had been
recorded (Figure 3A-B). Lower median Ang-1 (rho -0.46; 95% CI -0.67 to -0.19), but not higher
Ang-2, correlated with higher CRP at t=48-72h.
AN
GIO
POIETIN
S IN SU
RINA
MESE N
EWBO
RNS
124
7
Table 1. Descriptive statistics of the study group (n=91)
Controls
(n=20)
Early Onset Sepsis
P-value
Blood Culture
Negative (n=65)
Blood Culture
Positive (n=6)
Pregnancy, n (%) Complications1
Chorioamnionitis2
3 (15)
0
16 (25)
18 (28)
1 (17)
0
0.63
Mode of delivery,
n (%)
Vaginal
Caesarean
12 (60)
8 (40)
46 (75)
19 (25)
4 (67)
2 (33)
0.54
Sex, n (%) Male
Female
9 (45)
11 (55)
29 (45)
36 (55)
5 (83)
1 (17)
0.19
Ethnicity, n (%) Maroon and Creole
Hindo-Surinamese
Other3
12 (60)
3 (15)
5 (25)
44 (68)
14 (21)
7 (11)
4 (67)
1 (17)
1 (17)
0.61
Gestational age,
n (%) (weeks)
34-37
37-40
≥40
1 (5)
14 (70)
5 (25)
22 (34)
30 (46)
13 (20)
0
4 (67)
2 (33)
0.06
Apgar score, n (%) <5 0 5 (8) 2 (33) 0.03
Birth weight, Median
(IQR) (grams)
3130 (700) 2840 (835) 3500 (906) 0.02
Age at presentation,
n (%) (hours)
<24
24-48
48-72
4 (20)
7 (35)
9 (45)
43 (66)
13 (20)
9 (14)
2 (33)
1 (17)
3 (50)
<0.01
Clinical course
(at 48-72h), n (%)
CPAP
Mechanical Ventilation
Cardiotonics
Mortality
0
0
0
0
9 (14)
7 (11)
5 (8)
3 (5)
0
2 (33)
1 (17)
2 (33)
<0.001
CPAP = continuous positive airway pressure; N/A = not applicable. 1 Presence of pregnancy-induced hypertension, preeclampsia or diabetes mellitus.2 Defined as intrapartum fever or administration of antibiotics.3 Includes: Javanese, Chinese, Caucasian and Amerindian.
DISCUSSIONIn this study, we investigated the serum levels of Ang-1 and Ang-2 to better understand the vascular
pathophysiology in near-term and term Surinamese newborns treated for EOS. Lower levels of
Ang-1, higher Ang-2, and a higher Ang-2/Ang-1 protein ratio in serum of newborns was associated
with blood culture positive EOS at start of antibiotic treatment. Levels of Ang-1 further decreased
over time in newborns with blood culture positive EOS and correlated negatively with higher levels
of CRP. These results indicate a role for the Angiopoietins in vascular inflammation during EOS in
Suriname. An estimated 5-10% of total EOS data is from non-Western countries such as Suriname,
while there is strong indication that over 90% of global deaths due to EOS occurs in these settings
[2,19,20]. Thus, our data add critical basic and clinical knowledge on the true global impact of EOS.
AN
GIO
POIETIN
S IN SU
RINA
MESE N
EWBO
RNS
125
7
Table 2. Infection biomarkers in baseline controls and newborns with suspected and blood culture positive
PREDICTION OF EARLY ONSET SEPSISPrediction of EOS is complicated due to the fact that clinical symptoms and inflammatory
biomarkers are often not specific for presence of EOS [1]. Like in many Western countries, clinical
protocol at the neonatal care facility in Suriname prescribes a combination of perinatal risk factors,
SUM
MA
RY A
ND
FUTU
RE PERSPEC
TIVES
160
9
clinical symptoms of the newborn, and serial assessment of inflammatory biomarkers C-reactive
protein (CRP) and white blood cell count, to predict presence or absence of EOS within 72 hours
after birth. In Part 2 of this thesis we describe tools that may be of additive value in the prediction
of EOS in the clinic.
The online available EOS calculator is a novel tool to predict EOS and help decision making
on start and duration of antibiotic treatment [2]. The EOS calculator is based on five objective
maternal parameters and clinical evaluation of the newborn straight after birth, and provides a risk
estimate on EOS. It is unclear how the EOS calculator relates to levels of CRP and leukocyte and
thrombocyte counts in the first 72 hours of life. Increase of CRP and leukopenia have been shown
to be associated with blood culture positive EOS. In Chapter 3 we investigated the hypothesis
that higher EOS calculator results are associated with increase in CRP within 24-48 hours and low
leukocyte counts. EOS risk estimates were calculated for 108 newborns of 34 weeks of gestational
age, in whom antibiotics were started for suspected EOS. EOS risk estimates were retrospectively
compared to infection parameters CRP, and leukocyte and trombocyte counts. In contrast to our
hypothesis, high EOS risk at birth was consistently correlated with lower CRP and leukocyte counts
within 24 hours after the start of antibiotics, but not with infection parameters after 24 hours.
The study in Chapter 3 does not show correlation with infection parameters CRP and leukocyte
counts that are currently commonly used in the clinic to help decision making on start and duration
of antibiotic treatment in the clinic. However, in a large recent study amongst 204,485 newborns
in the United States determination of EOS risk with the EOS calculator reduced the number of
newborns that received laboratory testing and empirical antibiotic treatment [3]. Retrospective
analysis of the Dutch cohort used in Chapter 3 showed that application of the EOS calculator could
reduce antibiotic treatment with 50% [4]. To further enhance its clinical utility, it may be useful to
investigate association of the EOS calculator with biomarkers, such as immature granulocytes and
markers of endothelial cell activation, discussed in this thesis. Integration of the EOS calculator
with these biomarkers into a novel diagnostic approach is proposed in the last paragraph of
this chapter.
In Chapter 4 we investigated another option to predict EOS and to help decisions on start
and duration of antibiotic treatment. Automated measurement of immature-to-total-granulocyte
(I/T) has been shown to have negative predictive value of EOS [5]. We retrospectively evaluated
a one-point measurement of immature-to-total-granulocyte (I/T) ratio in predicting duration of
antibiotic treatment in EOS in a cohort of Surinamese newborns. I/T ratio was lower in newborns
in whom antibiotics were discontinued at 48-72 hours after start after which they all remained
healthy. We conclude that low I/T ratio may help to increase the threshold to start empirical
antibiotic treatment or to guide safe stoppage of antibiotics after 48-72 hours. Further prospective
investigations in larger cohorts of newborns are necessary to evaluate clinical utility of a one-point
measurement of I/T ratios, and to establish appropriate cut-off values. Nonetheless, it is a quickly
available measurement (i.e., within 10 minutes after blood draw) to help decision-making on start
of antibiotics in suspected EOS. Additionally, the fact that automated hematology analyzers are
becoming universally available in the non-Western world favors their implementation there.
SUM
MA
RY A
ND
FUTU
RE PERSPEC
TIVES
161
9
THE VASCULAR PATHOPHYSIOLOGY OF EARLY ONSET SEPSIS The dilemmas in prediction of EOS in the clinic occur because the pathophysiology of EOS is
poorly understood. In Part 3 of this thesis we focus on the vascular pathophysiology of EOS and
the potential of its molecular aspects for translation into novel diagnostic methodologies.
The vascular pathophysiology of sepsis is associated with interactions between leukocytes
and the vascular endothelium [6]. During sepsis, adhesion molecules are expressed on the cell
membranes of both cell types that orchestrate leukocyte rolling on, adhesion to, and transmigration
across the endothelium [7]. As inflammation progresses, adhesion molecules accumulate in
the blood as soluble forms after shedding by shedding enzymes, or ‘sheddases’, such as matrix
metalloproteinase-9 (MMP-9) and neutrophil elastase [8]. In Chapter 6 we review the studies that
have tested the predictive value of soluble adhesion molecules (sCAMs) in sepsis pathophysiology
in newborns, children and adults. Four endothelial sCAMs, specifically P-selectin, E-selectin,
vascular cell adhesion molecule-1 (VCAM-1), and intercellular adhesion molecule-1 (ICAM-1), along
with one leukocyte adhesion molecule, namely L-selectin, were associated with sepsis. While
increased levels of these sCAMs generally correlated well with the presence of sepsis, their degree
of elevation was poorly predictive of sepsis severity scores, outcome and mortality. Separate
analyses of newborns, children, and adults demonstrated significant age-dependent differences
in both basal and septic levels of sCAMs. Based on the results reported in this review, we proposed
two novel directions for improving clinical utility of sCAMs: 1) the combined simultaneous analysis
of levels of soluble adhesion molecules and their sheddases, and 2) taking age into account in
the interpretation of their levels.
In Chapter 7 we applied this approach in a Surinamese cohort of 20 healthy newborns and 71
newborns with suspected EOS, included within 72 hours after birth. We hypothesized that sCAMs
and sheddases circulate at higher levels in blood culture positive EOS in newborns and that they
are useful as biomarkers for EOS. Soluble CAMs sP-selectin, sE-selectin, sVCAM-1, sICAM-1, and
platelet and endothelial cell adhesion molecule-1 (sPECAM-1), sheddases MMP-9 and neutrophil
elastase, and sheddase antagonist tissue-inhibitor of metalloproteinases-1 (TIMP-1) were measured
simultaneously in serum of 91 newborns. Of the newborns, six (8.5%) had a positive blood culture.
At start of antibiotic treatment and after 48-72 hours no differences were found in levels of sCAMs
and sheddases between blood culture positive EOS, blood culture negative EOS and controls. In
contrast to our hypothesis, these data show that endothelial CAM shedding was not increased in
EOS. Additionally, levels of sCAMs and sheddases were similar in all newborns between straight
and six days after birth, indicating that sCAM shedding remains unchanged in early newborn life.
Levels of sCAMs found in our study corresponded well with levels in other studies in newborns.
However, when compared with earlier reports in adults sCAM levels in newborns are higher. We
concluded that other mechanisms, such as perinatal stress during birth, may drive overall high
levels in all newborns which precludes discrimination between septic and healthy newborns based
on these levels. For these reasons, sCAMs and sheddases may not prove to be useful as biomarkers
for EOS. Thus, our study indicates that simultaneous measurement of sCAMs and sheddases, as
proposed in our review in Chapter 6, does not provide a satisfactory improvement of clinical utility
of sCAM levels in prediction of EOS.
SUM
MA
RY A
ND
FUTU
RE PERSPEC
TIVES
162
9
Vascular inflammation and leakage in sepsis is mediated by Angiopoietin (Ang)-1 and Ang-2
and their binding associated phosphorylation of the endothelial Tie-2 receptor. Levels of Ang-2
change in adults and children during sepsis, which is associated with severity of sepsis. In Chapter 8
we investigated serum levels of Ang-1 and Ang-2 in newborns within 72 hours after birth.
A prospective study was performed in the same cohort of newborns as described in Chapter 7.
At start of antibiotic treatment Ang-1 serum levels were significantly lower and Ang-2 and Ang-2/
Ang-1 serum protein ratios higher in newborns with blood culture positive EOS than in blood
culture negative EOS and controls. These levels were not dependent on timing of first blood
draw after birth. After 48-72 hours, levels of Ang-1 further decreased in blood culture positive
EOS, while in the other groups no change was observed. These findings support the hypothesis
that a dysbalance in the Angiopoietins is associated with the (vascular) pathophysiology of EOS.
Additionally, these findings suggest potential for the Angiopoietins as biomarkers for EOS.
We propose further investigations into the Angiopoietin in EOS at two complementary levels.
First, we propose to measure Ang-1 and Ang-2 levels in peripheral and cord blood in a mouse
model of pregnancy to study both maternal and perinatal factors that may influence Ang-1 and
Ang-2 levels in neonatal mice [9]. In addition, inoculation of neonatal offspring born in this study
with Group B Streptococcus (GBS), to model EOS, within 72 hours could further reveal the vascular
pathophysiology of EOS [10]. Second, from the results of our first study we hypothesize that
serial measurement of high Ang-1, low Ang-2, and low Ang-2/Ang-1 ratio may negatively predict
presence of EOS, and thus be extra arguments for safe stoppage of antibiotics. We propose further
evaluation of Ang-1 and Ang-2 as biomarkers for EOS by repeating the study in Chapter 8 in a larger
Surinamese cohort to establish sensitivity, specificity and appropriate cut-off and predictive values
of the Angiopoietins for EOS. Maternal and perinatal factors may influence levels of Ang-1, Ang-2
and Ang-2/Ang-1 ratios in newborns, for which logistic regression analysis should be performed.
Additionally, the methodological possibilities to enable quick measurement of Ang-1 and Ang-2
levels for clinical purpose should be explored.
While the results from earlier chapters in this thesis provide new avenues for identification and
exclusion of EOS, a continuing need for (development of) novel and clinically useful diagnostic
tools remains. Alterations in neutrophil morphology (size, shape and composition), mechanics
(deformability), and motility (chemotaxis and migration) have been observed during sepsis.
In Chapter 9 we summarized features of neutrophil morphology, mechanics, and motility that
change during sepsis and combined that with an investigation into their clinical utility as markers
for sepsis through measurement with existing and novel technologies. When compared to resting
conditions, sepsis causes an increase in circulating numbers of larger, more rigid neutrophils
that show diminished granularity, migration and chemotaxis. Combined measurement of these
parameters may provide a more complete view on neutrophil phenotype manifestation. For that
purpose, sophisticated automated hematology analysers, microscopy and bedside microfluidic
devices provide clinically feasible, high throughput, and cost limiting means. We propose that
integration of features of neutrophil morphology, mechanics and motility with these new analytical
methods can be useful as markers for diagnosis, prognosis and monitoring of sepsis, and may even
contribute to our basic understanding of its pathophysiology (See also Appendix I).
SUM
MA
RY A
ND
FUTU
RE PERSPEC
TIVES
163
9
OPTIONS AND CHALLENGES FOR A NOVEL DIAGNOSTIC APPROACH FOR EARLY ONSET SEPSIS As discussed above, the major challenge in EOS is its timely identification for prompt initiation of
antibiotic treatment, while preventing unnecessary antibiotic treatment in uninfected newborns.
This is especially true for low resource settings, such as Suriname, where the risk for EOS is relatively
high, and the threshold to start empirical antibiotic treatment is relatively low, when compared to
Western countries. To date, only serial measurement of low levels of CRP, combined with a negative
blood culture and clinically improved newborn, showed negative predictive value for EOS [11]. In
a recent randomized controlled trial amongst 1,710 newborns in eighteen clinics in four European
countries and Canada, a clinical decision-making regimen, in which a four point measurement of
procalcitonin was added to the standard regimen of measurement of CRP and white blood cell
counts alone, was superior in reducing duration of antibiotic treatment [12]. Data in this thesis
show that incidence of blood culture positive EOS in Suriname is higher than reported in this trial
(i.e., estimated between 8-10% versus 1-2%, respectively) indicating that newborns in Suriname
are at higher risk for EOS. Additionally, the safety nets and facilities to properly follow-up clinical
evolution of sent home newborns in whom antibiotics are discontinued, such as home maternity
care, are absent in Suriname. For these reasons, the reported superior new regimen including
procalcitonin cannot be safely applied directly to the Surinamese situation. However, the standard
regimen described in this study was similar to the regimen that is currently used in Suriname.
Thus, it would be interesting to perform a similar randomized controlled ‘non-inferiority’ trial to
compare a novel diagnostic approach with the standard regimen in Suriname.
Starting point of this proposed novel diagnostic approach is the EOS calculator. Since the EOS
calculator is freely available online (also as an app for a smartphone), it is the most affordable
tool to guide clinicians in decision-making on start of antibiotics in cases of suspected EOS in
low resource settings such as Suriname. Especially at medical posts in rural areas of Suriname,
the EOS calculator is an easy-to-use tool to help decision-making on transport of newborns
to the neonatal care facility in the capital Paramaribo for evaluation and treatment. Before
implementation in Suriname, it is important to realize that for optimal performance the EOS
calculator algorithm uses local incidence of EOS is needed. Another variable in the algorithm is
maternal GBS colonization status, which is usually unknown in pregnant women in the Surinamese
setting. Moreover, our prospective studies showed that only gram-negative EOS occurred in our
cohort, indicating that GBS colonization may play an inferior role as causative pathogen of EOS
in Suriname. We are currently performing a prospective observational cohort study in pregnant
women and their newborns in Suriname to evaluate the exact incidence and local risk factors
for EOS and performance of the current EOS calculator. This is intended to ultimately create
a customized EOS calculator with variables that are specific for Suriname. Further improvement
of EOS calculator performance can be achieved when used in combination with novel biomarkers
discussed in this thesis. As discussed above, appropriate cut-off values for both I/T ratio and levels
of Ang-1 and Ang-2 have to be established in larger prospective studies. Once these have been
established, in Suriname the novel diagnostic approach could consists of the following if a newborn
SUM
MA
RY A
ND
FUTU
RE PERSPEC
TIVES
164
9
presents with suspected EOS: 1) immediate determination of EOS risk with a Suriname-specific
EOS calculator, combined with 2) immediate measurement of I/T ratio to help decision-making
on whether to start antibiotic treatment, and then, if antibiotics are started, 3) repeated Ang-2/
Ang-1 ratio determination to help decide whether to continue antibiotic treatment after 48-72
hours after start. This novel diagnostic approach could reduce antibiotic treatment in suspected
EOS in two complementary ways, namely the prevention of start of unnecessary antibiotics, and
safe stoppage of antibiotic treatment after 48-72 hours in the high-risk low resource setting. If
successful, both scenarios would be a major step forward in reducing the burden of antibiotic
treatment in newborns in Suriname and similar low resource settings.
A FUTURE CASE OF SUSPECTED EARLY ONSET SEPSIS IN SURINAME IN 2030After a boat ride from her village down the Suriname River, the mother arrives at the nearest mission
post in Debike1. She is pregnant for eight months and her water has broken a few days earlier. She
has korsu2. The datra3 at the mission post uses an application on his smartphone and puts in her
temperature. He explains that the result of the app tells him to send her to the new hospital in
the city of Paramaribo to give birth because her unborn child may have an infection. She gives
birth to a daughter there the next day. The doctors take her to the baby ward and take her blood.
The results of the blood test come back within 10 minutes, after which they start antibiotics. After
two days the baby is healthy and feeding well. The doctors take her blood again. The nurse tells her
the results are fine and that they will stop the antibiotic treatment. The next day the mother rides
the boat home to her village with a healthy daughter.
1 Village located along the Suriname River in the district Sipaliwini in the interior of Suriname
Translated from the Surinamese language (Sranan Tongo):2 physician;3 fever.
SUM
MA
RY A
ND
FUTU
RE PERSPEC
TIVES
165
9
REFERENCES1. van Herk W, Stocker M, van Rossum AMC.
Recognising early onset neonatal sepsis: An
essential step in appropriate antimicrobial use.
J Infect 2016, 72:S77–82.
2. Escobar GJ, Puopolo KM, Wi S, Turk BJ,
Kuzniewicz MW, Walsh EM, Newman
TB, Zupancic J, Lieberman E, Draper
D. Stratification of risk of early-onset
sepsis in newborns ≥ 34 weeks’ gestation.
Pediatrics 2014, 133(1):30–6.
3. Kuzniewicz MW, Puopolo KM, Fischer A,
Walsh EM, Li S, Newman TB,, Kipnis P, Escobar
GJ. A Quantitative, Risk-Based Approach to
the Management of Neonatal Early-Onset
Sepsis. JAMA Pediatr 2017, 171(4):365-371.
4. Kerste M, Corver J, Sonnevelt MC, van Brakel
M, van der Linden PD, M Braams-Lisman BA,
Plötz FB. Application of sepsis calculator in
newborns with suspected infection. J Matern
Fetal Neonatal Med 2016, 29(23):3860-5.
5. Mikhael M, Brown LS, Rosenfeld CR. Serial
neutrophil values facilitate predicting
the absence of neonatal early-onset sepsis. J
Pediatr 2014, 164(3):522-8
6. Aird WC. The role of the endothelium in
severe sepsis and multiple organ dysfunction
syndrome. Blood 2003, 101(10):3765-77.
7. Ley K, Laudanna C, Cybulsky MI, Nourshargh
S. Getting to the site of inflammation:
the leukocyte adhesion cascade updated. Nat
Rev Immunol 2007, 7(9):678-89.
8. Garton KJ, Gough PJ, Raines EW. Emerging roles
for ectodomain shedding in the regulation
of inflammatory responses. J Leukoc
Biol 2006, 79(6):1105-16.
9. Reynolds LP, Borowicz PP, Vonnahme KA,
Johnson ML, Grazul-Bilska AT, Wallace JM, Caton
JS, Redmer DA. Animal models of placental
angiogenesis. Placenta 26(10):689-708, 2005.
10. Mancuso G, Midiri A, Beninati C, Biondo
C, Galbo R, Akira S, Henneke P, Golenbock
D, Teti G. Dual role of TLR2 and myeloid
differentiation factor 88 in a mouse model
of invasive Group B streptococcal disease. J
Immunol 2004, 172: 6324-6329.
11. Hofer N, Zacharias E, Müller W, Resch B. An
update on the use of C-reactive protein in
early-Onset neonatal sepsis: Current insights
and new tasks. Neonatology 2012;102:25–36.
12. Stocker M, van Herk W, El Helou S, Dutta
S, Fontana MS, Schuerman FABA, van den
Tooren-de Groot RK, Wieringa JW, Janota J, van
der Meer-Kappelle LH, Moonen R, Sie SD, de
Vries E, Donker AE, Zimmerman U, Schlapbach
LJ, de Mol AC, Hoffman-Haringsma A, Roy M,
Tomaske M, Kornelisse RF, van Gijsel J, Visser
EG, Willemsen SP, van Rossum AMC; NeoPInS
Study Group. Procalcitonin-guided decision
making for duration of antibiotic therapy in
neonates with suspected early-onset sepsis:
a multicentre, randomised controlled trial
(NeoPIns). Lancet 2017, pii. 6736(17)31444-7.
& Appendices
APPEN
DIX
I
171
&
APPENDIX I: MEASUREMENT OF FUNCTIONAL AND MORPHODYNAMIC NEUTROPHIL PHENOTYPES IN SYSTEMIC INFLAMMATION AND SEPSIS
Rens Zonneveld, Grietje Molema, Frans B. Plötz
Letter to the editor of Critical Care
Critical Care 2016, 20:235-36.
We read with great interest the review by Leliefeld et al. [1] published in Critical Care, on the role
of neutrophils in immune paralysis during systemic inflammation (SI). This is of high clinical
importance since immune paralysis potentially increases susceptibility to new infections or may
cause inability to clear existing infections leading to detrimental outcome. One mechanism
proposed for immune paralysis is the release of neutrophil populations with decreased microbicidal
properties [1]. During SI heterogeneous subsets of neutrophils exist with different priming states
and functions [2]. In particular, large numbers of immature neutrophils appear in the circulation
with diminished expression of receptors, important for pathogen killing [3]. We recently reviewed
literature on morphodynamic changes in neutrophils during sepsis [4]. Sepsis increases their
circulating numbers (and percentages of immature neutrophils) and cell size and stiffness, and
decreases migration/chemotaxis, compared to non-diseased conditions or mild infection. Septic
neutrophils are also prone to produce neutrophil extracellular traps (NETs).
Both reviews outline shifting neutrophil identity from an innate responder to a complex immune
cell with different functional and morphodynamic phenotypes depending on the underlying
pathology. The relationship between changes in functional and morphodynamic phenotypes
is not completely understood. For example, inability of circulating neutrophils to migrate to
infectious sites during SI may be the result of diminished expression of chemotactic receptors
(e.g., CXCR2), which is most profound in newly released immature granulocytes [1]. Others have
suggested a hyperadhesive state to the endothelium, due to overexpression of integrins (e.g.,
CD11b/CD18) on their membrane, thereby decreasing their ability to migrate [5]. Whether this
impaired migration interferes with pathogen killing capacity needs to be investigated.
It is important to know that detecting morphodynamic changes in neutrophils is nowadays
clinically feasible with novel technologies [4]. Automated hematology analysers can measure
(immature) neutrophil counts and cell sizes, while microfluidic devices can measure migration
velocities. These methods represent a diagnostic toolbox that enables multi-parameter analysis
of neutrophils during SI and sepsis. When combined with technologies that are still in their infancy
(e.g., flowcytometry to measure degranulation), bedside measurement of functions of neutrophils
and in vitro studies as proposed by Leliefeld (e.g., measurement of intra-or extracellular killing
activity) will become feasible. This approach will combine functional and morphodynamic
neutrophil phenotypes into clinical settings for better understanding of the exact role of
neutrophils in SI and sepsis. Ultimately, this may help to determine whether neutrophils can be
considered rational targets for therapy.
APPEN
DIX
I
172
&
DECLARATIONSEthical approval and consent to participate
Not applicable
Consent for publication
Not applicable
Availability of supporting data
Not applicable
Competing interests
The authors declare that they have no competing interests
Funding
RZ was sponsored by the Thrasher Research Fund
Author’s contributions
RZ, GM and FBP conceived, drafted and finalized the manuscript
Acknowledgments
Not applicable
Authors’ information
Not applicable
APPEN
DIX
I
173
&
REFERENCES1. Leliefeld PH, Wessels CM, Leenen LP,
Koenderman L, Pillay J. The role of neutrophils
in immune dysfunction during severe
inflammation. Crit Care 2016, 20(1):73.
2. Pillay J, Ramakers BP, Kamp VM, Loi ALT,
Lam SW, Hietbrink F, et al. Functional
heterogeneity and differential priming of
circulating neutrophils in human experimental
endotoxemia. J Leukoc Biol 2010, 88:211–20.
3. Navarini AA, Lang KS, Verschoor A, Recher M,
Zinkernagel AS, Nizet V, et al. Innate immune-
induced depletion of bone marrow neutrophils
aggravates systemic bacterial infections. Proc
Natl Acad Sci U S A 2009, 106:7107–12.
4. Zonneveld R, Molema G, Plötz FB. Analyzing
Neutrophil Morphology, Mechanics, and
Motility in Sepsis: Options and Challenges
for Novel Bedside Technologies. Crit Care
Med 2016, 44(1):218-28.
5. Blom C, Deller BL, Fraser DD, Patterson EK,
Martin CM, Young B, Liaw PC, Yazdan-Ashoori
P, Ortiz A, Webb B, Kilmer G, Carter DE,
Cepinskas G. Human severe sepsis cytokine
mixture increases β2-integrin-dependent
polymorphonuclear leukocyte adhesion to
cerebral microvascular endothelial cells in
vitro. Crit Care 2015, 19:149.
APPEN
DIX
II
174
&
APPENDIX II: SAMENVATTING (SUMMARY IN DUTCH)Early Onset Sepsis (EOS) wordt gedefinieerd als een ernstige bacteriële infectie in de bloedbaan
van een pasgeborene die zich manifesteert binnen 72 uur na geboorte. In Westerse landen
krijgt 1 op de 1000 (0.1%) pasgeborenen EOS. Het aantal gevallen van EOS in Suriname is niet
bekend, maar ligt waarschijnlijk veel hoger. Tijdens EOS ontstaat een ontstekingsreactie in
de bloedvaten waarbij met name afweercellen (zogenaamde witte bloedcellen) en het endotheel -
de binnenbekleding van bloedvaten en de barrière tussen bloed en de weefsels - betrokken
zijn. Tijdens EOS kan door verlies van de barrièrefunctie van het endotheel vocht in de weefsels
uittreden wat leidt tot ernstige problemen met de ademhaling en een lage bloeddruk. Het tijdig
starten van antibiotica kan sterfte als gevolg van EOS voorkomen. Echter, EOS kan alleen worden
bevestigd met een kweek van het bloed die pas na enkele dagen groei van aanwezige bacteriën
laat zien. Daarnaast zijn symptomen van EOS slecht te onderscheiden van symptomen die elke
pasgeborene kan vertonen als gevolg van aanpassingsproblemen door de geboorte. Hierdoor is
het tijdig aantonen of uitsluiten van EOS niet goed mogelijk en worden veel pasgeborenen te laat
of juist onnodig behandeld met antibiotica.
Het onderzoek in dit proefschrift richt zich op EOS in Suriname en op aspecten van
de ontstekingsreactie in het bloedvat en daarop gebaseerde methoden van detectie die bij
kunnen dragen aan het stellen van de juiste diagnose. In Suriname wordt gespecialiseerde
zorg aan pasgeborenen geleverd in de Neonatal Care Facility van het Academisch Ziekenhuis
Paramaribo. Het eerste deel van dit proefschrift beschrijft hoe vaak EOS onder de daar
behandelde pasgeborenen voorkomt. In het tweede deel worden twee reeds beschikbare
en toegankelijke methoden getoetst als mogelijk diagnostische test voor EOS in Suriname.
Dit betreft een online verkrijgbaar risicomodel voor EOS, de zogenaamde EOS Calculator, en
de geautomatiseerde kwantitatieve meting van een bepaald type afweercel, de immature
granulocyt. In het derde deel worden drie groepen circulerende eiwitten gemeten in het bloed van
Surinaamse pasgeborenen. Dit zijn de endothelial cell adhesion molecules (CAMs) en sheddases,
die samen de interactie tussen afweercellen en het endotheel verzorgen, en de Angiopoietins, die
betrokken zijn bij het onderhouden van de barrièrefunctie van het endotheel tijdens ontsteking.
Voor deze studies stelden we ons de vraag of deze eiwitten een voorspellende waarde hebben
voor het beloop van de bacteriële infectie.
De resultaten van het onderzoek zijn als volgt. Na vernieuwing van de Neonatal Care Facility
in Paramaribo blijft EOS een groot probleem. Het aantal gevallen van met een bloedkweek
bewezen EOS na de vernieuwing was nog steeds tussen de 50-100 (5-10%) op 1000 pasgeborenen,
hetgeen vele malen hoger is dan in de Westerse landen. 30% van de pasgeborenen kreeg
antibiotica voor een verdenking op EOS. De EOS Calculator helpt om het risico op EOS in te
schatten. Lage bloedwaarden van de immature granulocyt waren voorspellend voor afwezigheid
van EOS en kunnen helpen om onnodige behandeling met antibiotica te voorkomen of de duur
van de behandeling te verkorten. De bloedspiegels van de CAMs en sheddases waren hoog maar
niet geassocieerd met het voorkomen van EOS. Waarschijnlijk hebben deze hoge waarden een
andere oorzaak dan EOS, zoals stress omtrent de geboorte. Meting van de Angiopoietins in
APPEN
DIX
II
175
&
dezelfde groep Surinaamse pasgeborenen liet zien dat er een disbalans ontstaat tijdens EOS tussen
de twee belangrijke vormen Ang-1 en Ang-2. Ang-1 bloedwaarden zijn lager en Ang-2 waarden
hoger in pasgeborenen met EOS waardoor de Ang-2/Ang-1 ratio verandert. Deze bevindingen
geven aan dat het endotheel wordt geactiveerd en betrokken is bij de ontstekingsreactie in
de bloedvaten tijdens EOS. Verder onderzoek moet uitwijzen of het meten van deze eiwitten ook
kan worden gebruikt om EOS aan te tonen of uit te sluiten.
De bevindingen van dit proefschrift laten zien dat EOS een groot probleem is in Suriname.
De combinatie van risico inschatting op EOS met de EOS calculator, mits aangepast voor
de Surinaamse situatie, meting van de immature granulocyt en seriële meting van de Angs kan in
de toekomst mogelijk helpen om onnodig gebruik van antibiotica te reduceren.
APPEN
DIX
III
176
&
APPENDIX III: DANKWOORDHet onderzoek in dit proefschrift werd uitgevoerd op drie verschillende continenten en bracht
mij van de kinderafdeling van Tergooi Ziekenhuizen in Blaricum naar het laboratorium van Harvard
Medical School in Boston, en vervolgens van de kinderafdeling van het Academisch Ziekenhuis
Paramaribo naar het laboratorium van het Universitair Medisch Centrum in Groningen. Ik heb
de eer gehad om samen te werken met een groot aantal zeer inspirerende mensen door wie dit
proefschrift tot stand is gekomen.
Allereerst, copromotor en mentor dr. Frans Plötz. Beste Frans, man van het eerste uur van al het
werk in dit proefschrift. In de afgelopen vijf jaar wil ik graag zeggen dat ik een vriend rijker ben
geworden. Ik kan me onze eerste ontmoeting nog herinneren in de assistentenkamer van Tergooi
Ziekenhuizen in Blaricum in 2011. Je eerste vraag was of ik onderzoek wilde doen. Hierna ben jij
van het eerst geschreven woord van de eerste beursaanvraag tot het laatst geschreven woord van
dit proefschrift zeer betrokken geweest. Onderzoek doen in het buitenland, ver van familie en
vrienden, was niet altijd even makkelijk en je bent me letterlijk overal gevolgd om steun, zowel
inhoudelijk als persoonlijk, te bieden waar nodig. Je was altijd bereikbaar, maar wist ook feilloos
wanneer ik ruimte nodig had. Ik neem jou (levens)lessen mee als het me in de toekomst lukt
om ook anderen te gaan begeleiden in het onderzoek. Ik hoop in ieder geval met je te kunnen
blijven samenwerken.
Mijn promotor, prof. dr. Grietje Molema. Beste Ingrid, dankzij Kate leerde ik je kennen in Boston,
alwaar je mijn poster stond te lezen in de gang van de CVBR. Ik had op dat moment geen promotor
en jij durfde het direct aan om die rol op je te nemen. Door jou zijn de verschillende hoofdstukken
in dit boekje tot een proefschrift geworden. Met jouw steun waagde ik me aan nog een avontuur
in Suriname. Voor jonge onderzoekers heb je de unieke gave om vertrouwen te geven terwijl
je ze blijft uitdagen en grenzen laat opzoeken. Hierin erken je ook altijd de persoon achter de
onderzoeker en geef je ze een eigen plekje. Gelukkig mocht deze onderzoeker bij jou en Nicoline
op de zolder slapen als ik weer eens in Nederland was met een doos met samples en zonder
dak boven mijn hoofd. En het was je dan zelfs niet teveel om in de ochtend boterhammen te
smeren om de dag op het lab mee door te komen. Ik hoop dat ik nog vaak langs mag komen voor
gezelligheid en wetenschap.
Mijn tweede copromotor, Dr. Matijs van Meurs. Beste Matijs, toen ik jou leerde kennen was het
heel fijn om de ervaringen uit Boston met je te kunnen delen en om te merken dat jij vergelijkbare
ervaringen hebt gehad. Vervolgens kon ik op jouw kennis en kunde bouwen om de uitdagende
projecten in Suriname tot een goed einde te brengen. Het was leuk om te merken dat je gaandeweg
steeds enthousiaster werd over de boodschap van mijn proefschrift. Hierdoor kreeg ik daar zelf
ook meer vertrouwen in. Uiteindelijk hebben gesprekken met jou een belangrijke rol gespeeld
in de keuzes die ik heb gemaakt voor de toekomst. Dank hiervoor. Ik hoop dat ik, naast voor
wetenschap, nog vaak langs mag komen voor je advies.
APPEN
DIX
III
177
&
Aan de leden van de beoordelingscommissie prof. dr. J Smit, prof. dr. J.G. Zijlstra en prof. dr. J. van
Woensel: hartelijk dank voor de vlotte en unanieme beoordeling van het proefschrift. I would also
like to express my gratitude to all co-authors who helped perform and improve research for this
thesis: prof. dr. Taco Kuijpers, dr. Nathan Shapiro, Nathanael Holband, Anna Bertoline, Francesca
Bardi, dr. Peter Dijk, Niek Achten, and Ellen Tromp.
Mijn paranimfen Philip Cotterell en Maurice Seleky, makkers van het eerste uur. Zonder onze
gezamenlijke geschiedenis was dit niet mogelijk geweest. Al bijna 30 jaar maken wij alles samen en
van dichtbij mee en deze dag hoort daarbij. Dank dat jullie mij willen bijstaan.
Rianne Jongman, lieve Rianne, dank voor jouw bereidheid om de uitdagende sample analyse met
mij uit te voeren voor dit proefschrift. Een analist is inderdaad de spil in een onderzoeksgroep. Je
hebt me heel veel vaardigheden in het laboratorium geleerd. Toen ik met jou aan de slag kreeg
ik weer plezier en vertrouwen in de pipet. Je was zelf bezig met je promotieonderzoek en toch
maakte je altijd tijd voor me als ik uit Suriname kwam met een doos met samples. Ik hoop dat
laatste nog vaak te kunnen doen en ook onze vriendschap te onderhouden.
In Suriname wil ik beginnen met het bedanken van Amadu Juliana. Lieve Amadu, dank voor het
creëren van een plek om voor het eerst dit soort onderzoek te doen in Suriname, en dank voor
jouw vriendschap. Met alles wat je hebt bereikt en doet blijf je uiterst bescheiden, en dat is zeer
leerzaam. Zoals jij mij begeleidde in de kliniek in Suriname, ben ik bereid om jou in je onderzoek
te begeleiden. Laten we elkaar vooral hier in Suriname tegen blijven komen om nieuwe projecten
te ondernemen, ook samen met Ming-Jan Tang. Lieve Ming, toen we elkaar in Suriname leerden
kennen waren we eigenlijk direct met elkaar bevriend. Ik denk dat het goed voor ons beiden goed
is geweest dat we elkaar hadden om te kunnen sparren over de projecten waar we mee bezig
waren. De uitdagingen waren enorm, maar het is ook jou gelukt om een stempel te drukken op de
zorg voor pasgeborenen in Suriname. Ik hoop in de toekomst veel met je te kunnen samenwerken
om deze lijn door te zetten. Hiervoor is de eerste stap gezet: Stichting P.R.E.S. Neirude Lissone
(boegbeeld van de NICU), Aartie Toekoen (baken van de pediatrie) en Shirley Heath, jullie ook
dank voor jullie deelname aan deze stichting en voor de prettige samenwerking en steun die ik van
jullie heb gehad in mijn tijd in Suriname. Het is altijd weer leuk om jullie te zien. Peter Moons, dank
voor de avonturen die we samen hebben beleefd in Paramaribo en de fietstochten daarbuiten.
Aan mijn collega arts-assistenten van de kinderafdeling Laurindo, Kevin, Safir, Charleen, Majenge,
Rhea, Louella, Natasha, Ritesh, Priya, Marit, Susanne, Femke, Pieter, en alle verpleegkundigen:
grantangi voor de samenwerking en het helpen met de inclusies voor de InSepSur studie. Jullie
hulp is onmisbaar geweest. Ik wil hier ook graag de ouders en pasgeborenen bedanken voor
deelname aan één van de studies.
Van het Scientific Research Center wil ik graag Wilco Zijlmans danken voor de ruimte die daar ik
kreeg om onderzoek te doen. Succes met de verdere opbouw van wetenschap in Suriname. We
APPEN
DIX
III
178
&
hebben samen drie mooie publicaties over Rhesus D van de grond gekregen met een significante
boodschap voor de zorg voor pasgeborenen in Suriname. Shellice, Anisma en Iris, volgens mij
ben ik de eerste die gaat promoveren, maar er zullen er nog vele volgen! Ik zal de ‘keek op
de week’ missen. Sigrid Ottevanger, ook onze banksessies onder de mangoboom zal ik missen,
maar ik hoorde dat we hetzelfde vak gaan uitoefen. Ik voorzie een vruchtbare toekomst!
Van het Academisch Ziekenhuis Paramaribo wil ik dr. John Codrington bedanken. Toen ik je leerde
kennen zette je direct de deur van het klinisch laboratorium wagenwijd open. Zonder jou en de
hulp van alle analisten in het laboratorium was het niet gelukt om deze resultaten te bereiken.
In het bijzonder wil ik ook Sheldon Simson, Judith Liong a Kong en Jimmy Roosblad hartelijk
bedanken voor onze directe samenwerking in het laboratorium. Met elkaar hebben we ook nog
een verfrissend project over het Zika virus tot twee prachtige publicaties gebracht. Dit laatste
was niet mogelijk geweest zonder dr. Stephen Vreden in Paramaribo en prof. dr. Jan Wilschut in
Groningen. Dank voor jullie steun in al mijn projecten en de samenwerking. Volgens mij zitten we
heel erg op één lijn en onze gesprekken hebben er mede toe geleid dat ik heb besloten om het
roer om te gooien en arts-microbioloog te worden. Voor dat laatste dank ik ook Sandra Hermelijn,
want ook jij zette de deur open en ik voelde me altijd zeer welkom op de koffie (met gebak) bij
jou op kantoor. Patricia Wong Lie Song en alle andere analisten van het serologisch laboratorium
van het AZP, dank voor jullie fantastische hulp met sample opslag voor de RheSuN studie. Voor dit
project wil ik ook graag alle verloskundigen en analisten van het AZP, RKZ, Diakonessen en ’s Lands
Hospitaal bedanken. Het was inspirerend om te zien hoe goed er werd samengewerkt en met wat
voor resultaat! Ik wil ook graag Margriet Lamers, Jedda Eppink, en Peter Schmitz bedanken voor
de hulp met dataverzameling. Ik had eigenlijk geen tijd, maar door jullie is het toch gelukt. Henk
Schonewille, Anneke Brand, en Humphrey Kanhai, ik denk dat we iets moois hebben neergezet
en dat we begonnen zijn om de zorg voor pasgeborenen in Suriname, op dit vlak te verbeteren.
Laten we vooral doorgaan. Ik dank het ministerie van Volksgezondheid van Suriname hierbij voor
de unieke kans om dit onderzoek te doen.
In the United States I would like to express my gratitude to the people from the Center for Vascular
Biology Research at Beth Israel Deaconess Medical Center in Boston. Dr. Christopher Carman
and dr. Roberta Martinelli, it all began in your lab. Thank you for letting me work there and learn
about the endothelium, neutrophils, microscopy, and science in general. Also, many thanks to
the members of the Carman lab Grace Teo and Peter Sage. Dr. Nathan Shapiro, thank you for
helping us with samples to analyse. Kate Spokes, thank you for guiding me those two years, our
coffee talks in the hallway of the CVBR, the dinner parties at your place, and for introducing me to
Ingrid. I am sure you and Ann and myself will stay in touch. To the members of the Aird and Dvorak
(in particular prof. dr. W.C. Aird and prof. dr. H. Dvorak), my next-door neighbours, thank you
for the two years of science and fun we had. Stanley, Salvatore and Brian, I had a great time with
you, both in and outside the lab. I still remember how you helped with an online application for
a job in the Netherlands. I did not get the job, but it doesn’t matter. I wish you all well in all your
future endeavours. I am also grateful for all of the friendships I made throughout my stay in Boston.
APPEN
DIX
III
179
&
Vincent, ik mis je, maar volgens mij gaat het heel goed met jou en Pauline en de kids. Ik zie je snel,
waar ook ter wereld.
Van Tergooi Ziekenhuizen Blaricum wil ik graag alle kinderartsen en arts-assistenten uit het
magische jaar 2011-2012 bedanken. Tevens wil ik Karen Verloop van het wetenschapsbureau
de stichting tot Bijstand Tergooi bedanken voor de inhoudelijke en financiële steun voor het
onderzoek en proefschrift. Van de kinderafdeling in het Reinier de Graaf Gasthuis in Delft wil ik
alle kinderartsen, in het bijzonder de opleider Boudewijn Bakker, bedanken voor de gelegenheid
om als arts-assistent te werken en de ruimte om mijn proefschrift af te ronden. Daarnaast
dank ik al mijn collega arts-assistenten voor de ruimte die jullie mij hiervoor hebben gegeven.
In het Universitair Medisch Centrum Groningen wil ik graag alle leden van de EBVDT groep
bedanken voor de vrolijke verwelkomingen en gastvrijheid tijdens de momenten dat ik op het
laboratorium was.
Aan al mijn dierbare vrienden en vriendinnen, ik ben even weg geweest. Iedere keer als ik even
terug was realiseerde ik me hoeveel ik jullie miste, maar merkte ik vooral dat de vriendschap weer
hechter was. Ik ben weer terug in Amsterdam. Laten we vooral doorgaan waar we gebleven waren.
Papa, mama, Erik en Janna. Dank voor de steun in de afgelopen vijf jaar. Jullie hebben me geleerd
om, ondanks tegenslag, toch vooral vooruit te blijven kijken en dat heeft geholpen. Opa, je blijft
mijn inspiratie, en nu op naar de 100 en verder. Lieve T, ik ken je al heel lang, maar sinds kort leer
ik je iedere dag weer beter kennen.
Rens Zonneveld
Paramaribo, oktober 2017
APPEN
DIX
IV
180
&
APPENDIX IV: LIST OF PUBLICATIONSVroon P, Roosblad J, Poeze F, Wilschut J, Codrington J, Vreden S, Zonneveld R. Severity of acute
Zika virus infection: an emergency room surveillance study during the 2015-2016 outbreak in
Suriname. Accepted for Publication.
Zonneveld R, Jongman RM, Juliana A, Molema G, Van Meurs M, Plötz FB. Early onset sepsis in
Surinamese newborns is not associated with elevated serum levels of endothelial cell adhesion