University of Groningen Improving pharmacovigilance and the role of the pharmacist Grootheest, Adrianus Cornelis van IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2003 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Grootheest, A. C. V. (2003). Improving pharmacovigilance and the role of the pharmacist Groningen: s.n. Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 06-06-2018
Transcript
University of Groningen
Improving pharmacovigilance and the role of the pharmacistGrootheest, Adrianus Cornelis van
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2003
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Grootheest, A. C. V. (2003). Improving pharmacovigilance and the role of the pharmacist Groningen: s.n.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
The work presented in this thesis was performed at the NetherlandsPharmacovigilance Centre Lareb and the Department of Social Pharmacy andPharmacoepidemiology, GUIDE, Groningen.
The printing of this thesis was financially supported by the NederlandsBijwerkingen Fonds and by WINAp.
Rijksuniversiteit Groningen
Improving pharmacovigilanceand the role of the pharmacist
Proefschrift
ter verkrijging van het doctoraat in de Wiskunde en Natuurwetenschappen aan de Rijksuniversiteit Groningen
op gezag van deRector Magnificus, dr. F. Zwarts,in het openbaar te verdedigen op
maandag 17 november 2003om 14.15 uur
door
Adrianus Cornelis van Grootheestgeboren op 13 april 1948
te Bennekom
Promotor: Prof. dr. L.T.W. de Jong - van den BergCo-promotor: Dr. E.P. van Puijenbroek
Beoordelingscommissie: Prof. dr. A. de BoerProf. dr. J.R.B.J. BrouwersProf. dr. Y.A. Hekster
‘Science does not exist, unless it has been written down’‘Further the judgement is upon the reader’
This book is dedicated to the people of Africa for whom the content has little relevance as yet
Table of contents
Part 1 Introduction 1
1.1 The world of pharmacovigilance 3
1.2 The role of the pharmacist 13
1.3 Outline of the thesis 19
Part 2 Pharmacovigilance 29
2.1 The dawn of pharmacovigilance - Pharmacovigilance in
historical perspective 31
2.2 Leopold Meyler (1903-1973): a pioneer in the study of
adverse effects of drugs 43
2.3 Pharmacovigilance in the Netherlands 51
2.4 Underreporting in the spontaneous reporting of
adverse drug reactions – A pharmacovigilance approach 65
Part 3 The role of the pharmacist 81
3.1 Pharmacists’ role in reporting adverse drug reactions
in an international perspective 83
3.2 Attitudes of community pharmacists in the Netherlands
towards adverse drug reaction reporting 99
3.3 Contribution of pharmacists to the reporting of adverse
drug reactions 113
3.4 Thromboembolism associated with the new contraceptive
Yasmin® 125
Part 4 Improving pharmacovigilance 131
4.1 Intensive monitoring of new drugs based on first delivery
signal from pharmacists: a pilot study 133
4.2 Do pharmacists’ reports of adverse drug reactions reflect
patients’ concerns? 145
4.3 Consumer adverse drug reaction reporting: a new step
in pharmacovigilance? - An overview 157
4.4 Labelling and ‘Dear Doctor letters’
- are they non-committal? 169
Part 5 General discussion and perspectives 177
5.1 Improving pharmacovigilance 179
5.2 Independent pharmacovigilance 187
5.3 The role of the pharmacist 191
5.4 Pharmacovigilance as a scientific discipline 193
Summary 201
Samenvatting 207
List of publications 213
Dankwoord 217
Curriculum vitae 219
Notes on the cover illustrations 221
1Introduction
Chapter 1.1 The world of pharmacovigilance
In 1953, as a result of a storm that happened to coincide with a spring tide, a largenumber of dykes in the south-western coastal area of the Netherlands gave way.Vast areas of the two provinces of Zeeland and Zuid-Holland were inundated andmore than 200 people were drowned. This disaster not only prompted the decisionto raise the dykes but also led to the formulation of the so-called Deltaplan orDeltaworks, a comprehensive project designed to guarantee the safety of the south-western regions of the Netherlands. The scheme comprised closing off estuaries andinlets, raising the dykes and the construction of many other sophisticated civilengineering works. Its completion lasted several decades. This chain of events, acalamity followed by large-scale safety measures to minimise the risk of arecurrence, can also be said to characterise the development of drug safetymonitoring. There are striking parallels between this and the thalidomide tragedyin the 1960s when thousands of babies were born with serious congenitalmalformations as a result of the maternal use of thalidomide (also marketed asSoftenon®). Apart from causing the quality standards for the composition of drugsto be raised and more stringent criteria for the safety and efficacy of drugs to beformulated, the catastrophe also triggered the formation of an extensive system ofpost-marketing surveillance, which ultimately led to the creation of a new scientificdiscipline: pharmacovigilance.
Tragic events like the ‘Softenon drama’ could easily lead to the idea that drugs arehazardous. This would be a misperception. After all, drugs are remarkably safe.(1)As the director-general of the Dutch Ministry of Public Health Muntendamremarked in 1964: ‘The recent events have caused some panic over the new drugs.Quite understandable, but, by and large, unjustified’.(2)A new level of equilibrium needed to be found in which the blessings of the manynew drugs that were released and the potential risks associated with and inherent tothe use of these new medications would be given proportional attention.The rapid advances that have been made in the synthesis of new drugs since the 1930shave drastically changed the nature of health care. The introduction of antibiotics hasmeant that bacterial infections are now relatively easy to treat, even specific infectionslike tuberculosis. Often fatal in the first half of the previous century, today pneumoniaonly rarely leads to mortality, and then usually only in the elderly patient. The natureof psychiatric care has also been notably transformed due to the introduction of
3
psychopharmaca. Psychiatric hospitals, formerly often closed and isolated institutions,turned into open centres situated in parklands, which are now increasingly beingclosed because the improvements due to new drug make ambulant care facilitiespossible. An important, more recent development is the medicinal treatment of gastriccomplaints with H2-receptor antagonists or proton pump inhibitors, virtually makingsurgical interventions for non-malignant gastric disorders a thing of the past. Despite the many benefits we have derived from the development of newmedication we always need to keep in mind that, whereas at the individual leveldrugs are of course a care product, by and large at the societal level they are mainlycommercial products. This implies that for millions, perhaps even billions of peoplemedication is not available: for them the cost of drugs is prohibitive simply becausethey happen to live in a ‘low income country’ or, if they do live in an affluentcountry, belong to the underprivileged classes. By far the largest quantity of drugsis used in the USA, with Europe and Japan at some distance.(3) Africa hardlyfeatures in this story and here, each day thousands of people, mostly children, diefrom illnesses like malaria and the measles or the simplest of infections that are allhighly treatable elsewhere in the world. Clearly, there is no relationship betweenthe burden of illness in a country and its drug consumption, but there is betweenprosperity and the demand for medication. This was unambiguously illustrated bythe recent events in Argentina where in 2002 drug use plummeted with 67% due tothe country’s economic crisis, which is, however, likely to increase the demand formedical care.
1.1.1 Drug safetyAs mentioned earlier, it is essential to recognise that, apart from the blessings of ourmodern medicinal resources, there is a downside too. In his inaugural speech in1969 Meyler already indicated that basically there is no difference between drugsand toxins.(4) Not only are many remedies traditionally derivatives of toxicsubstances, the distinction between the therapeutic effect and the toxic effect of adrug is mainly determined by its dose. Adverse reactions to drugs (ADR) are thusdefined as ‘a response to a drug which is noxious and unintended and which occursat doses normally used in man’.(5)That unforeseen negative effects of drugs can occur even at normal doses is a criticaltheme in pharmacotherapy. When selecting a drug for prescription its safety profileoften is the deciding factor. The awareness that drugs are not by definition safe alsolargely determines the way people in general perceive drugs. The large array of sideeffects mentioned in the Summary of Product Characteristics (SPC) and the PatientPackage Insert (PPI) acts as a deterrent for both the prescriber and the user. Theconcern over drug safety is a concern that is shared by all those involved in theiruse.(6) The main reasons why a drug’s safety profile cannot be all-inclusive prior to
4
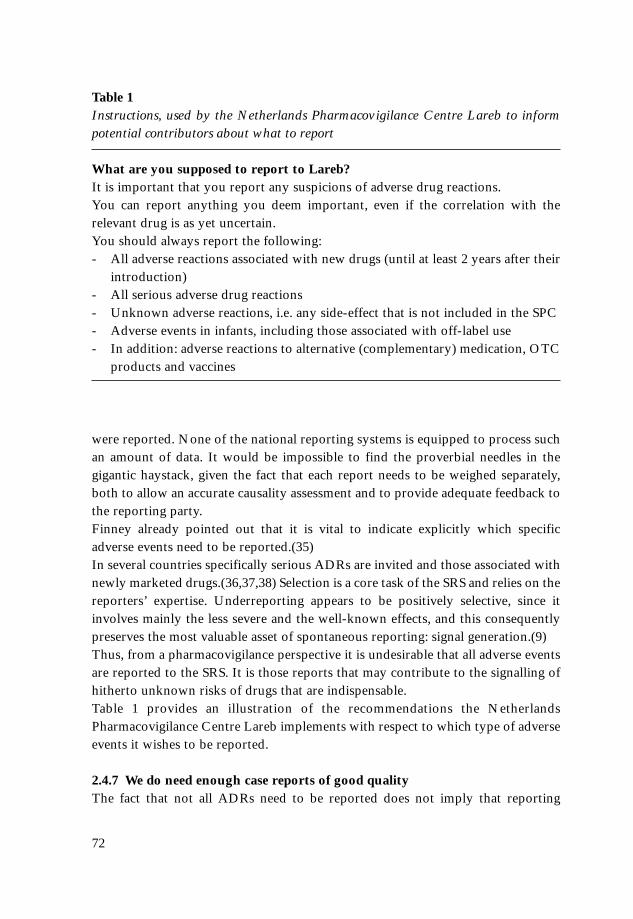
marketing, necessitating post-marketing surveillance, are presented in Table 1.Also the pharmaceutical industry is increasingly focusing more of their attention onthe safety aspect of their products. This is partly brought on by the intensifiednational and international rules and regulations, but also partly induced by the factthat in the past few years a relatively large number of drugs were withdrawn fromthe market because of their adverse effects.(7) Also pharmaceutical companies havecome to realise that it is in their own interest to give more attention to the safetyaspects of drugs.Although they fall outside the scope of this thesis, there are many other aspects thatare all highly relevant for the safety and safe use of drugs. We would like to mentionthorough registration procedures, prescriptions that are consistent with theindication, drugs that are dispensed at the right dose, a proper use of the prescribeddrug (compliance), but also meticulous manufacturing and drug synthesisprocedures based on high-quality components. These matters all seem self-evidentbut, as experience has shown, they not always are.(8)
1.1.2 PharmacovigilanceAccording to the definition in a recent WHO publication pharmacovigilance is thescience and activities relating to the detection, assessment, understanding andprevention of adverse effects or any other possible drug-related problem.(9) This isa more detailed definition than the one Rawlins used in his often-cited lecture for
5
Table 1 Reasons why drug safety issues may not be indentified until the post-marketingperiode1
1. The adverse reaction is rare and therefore undetectable until large number ofpatients have been exposed to the drug
2. There is a long latency between starting the drug and development of theadverse reaction
3. The drug has not been studies in normal clinical practice:- patients treated in clinical practice are likely to have different characteristics to
trial patiens (e.g. demography, other diseases, other medicaton);- in clinical practice a drug is less likely to be used strictly in accordance with
the recommendations by both doctors and patients, and with less monitoring
1. Waller PC, Arlett P. Responding to signals. In: Pharmacovigilance (Mann R, Andrews E, editors). Wiley Chicester 2002.
the Royal College of Physicians in 1994: Pharmacovigilance is the process ofidentifying, and then responding to, safety issues about marketed drugs.(10) Thislatter characterisation came from a report by the Committee on Safety of Medicinesand the Medicines Control Agency in the UK, which explains the emphasis on thepractical implementation of the concept. In the literature pharmacovigilance isfrequently put on a par with Post Marketing Surveillance. This approach highlightspharmacovigilance’s most visible method, viz. the spontaneous reporting system(SRS). In their latest textbook Mann and Andrews define pharmacovigilance as ‘thestudy of the safety of marketed drugs under the practical conditions of clinicalusage in large communities’.(11) But this includes more as only collecting reportsof possible ADRs and looking for signals of new ADRS. In a recent overviewEdwards, looking ahead, mentions five activities that are essential topharmacovigilance.(Table 2).
1.1.3 The circle of knowledge and practicePharmacovigilance is characterised by the fact that it derives its knowledge aboutthe safety of drugs from the clinical usage of drugs in daily practice. Bysystematically recording and analysing the most recent empirical data on clinicaldrug usage new knowledge is obtained. It is especially this latter aspect that hasreceived much attention, both in the literature and in the legislation or other rulesregulating drug surveillance. However, pharmacovigilance is a two-way system,which is represented by the circle of knowledge and practice as depicted in Figure 1. The upper half of the circle represents the aforementioned aspect but the lower half
6
Table 2Activities that are essential to pharmacovigilance according to Edwards1
- suspected ADR signal generation and formation of hypothesis- analysis of all issues around the signal, particularly confirmation (of refutation)
of hypotheses, estimation of the size of the risk and whether susceptible patientsexist
- consideration of possible changed benefit-to-risk issues in therapy- communication of information to health professionals and patients in a useful
way and possible regulatory action- consequence evaluation.
depicts the implementation of the knowledge into the clinical practice. This secondaspect of pharmacovigilance has recently been given more weight. In the pastpharmacovigilance was repeatedly criticised because once its activities had yieldeda signal of an ADR this all too often meant that the licence of the drug concernedwas suspended. Today it has become one of pharmacovigilance’s priorities to tryand find more creative and constructive ways to deal with these signals.(12,13)Ways to improve information and communication facilities are being consideredbut also the quite practical problems associated with the implementation ofmeasures promoting the safe use of drugs are given appropriate attention. Afterall, a drug is never just safe or unsafe: it is only safe when it is applied in theproper dose in patients for whom the individual risk-benefit balance has provenpositive. Mere prevalence rates of ADRs may be irrelevant for specific patientgroups.(14) Pharmacovigilance concerns itself with all the aspects in the circle of knowledge andpractice. Besides tracing and weighing risk factors, it tries to advise doctors andpharmacists on how best to deal with these risks and provide them with tools thatwill enable them to apply their newly acquired knowledge to the treatment of theindividual patient. This approach permits pharmacovigilance to contribute to a safeand rational use of drugs for the benefit and well-being of those patients that aredependent on pharmacotherapy, as is supported in this thesis.
7
Figure 1Circle of Knowledge and Practice
1.1.4 The science of pharmacovigilancePharmacovigilance is the science dedicated to the safety of drugs as used in theclinical practice, based on experiences from the clinical practice, thus generatingknowledge on the harmful effects of drugs, both at the individual and thepopulation level, that will eventually be applied in the clinical practice and thus leadto a safer use of drugs.As in most applied sciences the field of pharmacovigilance is an amalgam ofnumerous other scientific domains, each contributing their own expertise to thefield, which combined knowledge fosters drug safety reasoning. Pharmacovigilanceis essentially a clinical science.(15) To allow a sound judgment of any adverse effectsof drugs we need clinical knowledge at the level of the individual patient. It takesextensive general medical knowledge, preferably supported by direct experiencewith patient care, to be able to make an accurate assessment of the impactpharmacotherapy is likely to have, which becomes even more urgent whenunintended adverse events occur. Clinical pharmacologists have been instrumentalin the development of the field and are still indispensable, as are the pharmaceuticalsciences. By profession, pharmacists are the experts when it comes to drugs. An in-depth knowledge of the mechanisms and behaviour of drugs in the human body areoften crucial to gain insight into the actual effects a drug has, and may also helpexplain a (suspected) adverse drug reaction. Similarly, the field of toxicology is, by its very nature, closely related topharmacovigilance and, from an organisational point of view, has been fullyintegrated in many countries. Many of the insights on adverse effects to drugs wereprovided by toxicologists. Also teratology has played a significant role in this respect. Pharmacoepidemiology, the science concerned with the effects of drugs in largepopulations, has been another key contributor and, among other contributions, hashelped establish the basis for the statistical analysis techniques and risk assessmentsin pharmacovigilance. Finally, with respect to the implementation of the knowledge pharmacovigilancehas helped to acquire, it is now increasingly recognised that the existing means tocommunicate and implement this knowledge need to be improved.(16,17)
Regulatory pharmacovigilanceSome parties have been crucial to the development of pharmacovigilance. It hasbeen the authorities, both at the national and increasingly at the international level,that have initially helped foster the field. Labelled as regulatory pharmacovigilanceby Waller et al., they define pharmacovigilance as ‘the process of evaluating andimproving the safety of marketed medicines’.(18) They underlined theresponsibilities the various governments have in the monitoring of drug safety,which task many national governments took firmly in hand following the
8
thalidomide tragedy.(19,20) It is undeniable that in several countries, most notablyin the USA and UK, legislation has significantly contributed to the advance ofpharmacovigilance as a specialised field of knowledge. The role of the World HealthOrganisation stands out here. The collaborative programme launched under theauspices of the WHO by ten countries in 1968 was the start of an historicinternational cooperative effort, resulting in the WHO International DrugMonitoring Programme.(21) The Technical Report entitled ‘International DrugMonitoring: The Role of National Centres’ published as the proceedings of one ofthe WHO meetings in 1972, laid the theoretical and practical foundation for thefurther development of pharmacovigilance.(5) The programme has also resulted inthe WHO Collaborating Centre for Drug Monitoring (the Uppsala MonitoringCentre) which maintains the international ADR database and fulfils an importantrole particularly by the support it offers to the pharmacovigilance centres in low-income countries.
The role of the pharmaceutical industryThe second great influence on the development of pharmacovigilance is thepharmaceutical industry. This is not surprising since it is their product, a productthey themselves have both developed and manufactured, that is the object of study.From their circles great influence has been exerted to come to internationalagreements, many of which have since been formalised in the various reports theCouncil for International Organisations of Medical Sciences (CIOMS) and theInternational Conference on Harmonisation (ICH) have issued. Initially, thesector’s main interest lay in the epidemiological approach and causality assessment,but nowadays aspects of risk management are also given due attention.
International societiesLastly, it has been the international scientific societies that have been vital infurthering pharmacovigilance as a discipline in its own right. The InternationalSociety of Pharmacoepidemiology, founded in 1984, has helped formulate theepidemiological underpinning of the safety aspects of drugs. The InternationalSociety of Pharmacovigilance (founded as the European Society ofPharmacovigilance in 1992) has promoted the field’s clinical and communicationaspects.
1.1.5 The need for numbersBoth the regulatory authorities and the pharmaceutical industry want hard facts,preferably concrete numbers. This has meant that the epidemiological approach haslong dominated drug safety. Pharmacoepidemiology is the science dedicated to theuse of and the effects of drugs in large numbers of people.(22) It evolved as a sub-
9
discipline of epidemiology in the 1970s and 1980s. The debate on the safety of drugsfollowing the thalidomide affair in the early 1960s played a role here and postmarketing surveillance, the research of the usage and safety of marketed drugs,became one of its key tasks. Methodology, statistics and rates are the foundation ofpharmacoepidemiological reasoning aimed to provide (numerical) conclusions ongroup level.The relationship between pharmacoepidemiology and pharmacovigilance may becharacterised as follows: pharmacoepidemiology, by studying large populations,aims at deriving facts that may also be of relevance to the individual, whereaspharmacovigilance studies the clinical experiences of individuals in order to be ableto draw conclusions that may also be valid for larger sections of the population.Epidemiological and pharmacoepidemiological reasoning have long stood in theway of a full appreciation of pharmacovigilance’s distinctive qualities. Theirapproach based on numerical reasoning, caused attention to be shifted fromthinking in terms of clinical observations (clinical reasoning) to thinking in terms oflarge numbers and averages.(23) Claude Bernard, who did not believe in ‘theaverage patient’, was the first to criticise this approach. He was a strong advocate ofcausal and deterministic reasoning based on clinical observations in the individualpatient. Recently, there has been a broad renewed appreciation of the relevance ofthe individual case as the basis for scientific thinking.(24) Also wherepharmacovigilance relies on data derived from large datasets it is essential to alwaysweigh these findings against the underlying individual case histories before anyconclusions are drawn.(25,26) Apparently it is mostly cases and case series on which the regulatory authoritiesbase their final conclusions and measures; only rarely are their decisions supportedby pharmacoepidemiological research.(27) Moreover, most often the signalsunderlying their decisions are confirmed in the literature eventually.(28)In the light of these facts it is obvious that pharmacovigilance cannot provide aquantitative risk assessment, although its data may in some cases provide anindication. This is a task for the pharmacoepidemiologists since pharmacovigilancehas other objectives. Similar to all clinical disciplines the field of pharmacovigilancehas to deal with countless uncertainties. In this thesis the concept of underreportingis used to illustrate the distinctiveness of pharmacovigilance in relation topharmacoepidemiology.
1.1.6 Spontaneous reporting as the main source of signalsThe signals of adverse drug reactions derived from the experiences with patientsusing the drugs as reported by doctors and pharmacists lie at the heart ofpharmacovigilance. Meyboom defined a signal as a set of data constituting ahypothesis that is relevant to the rational and safe use of a drug in humans.(29) It is
10
pharmacovigilance’s key task to try and underpin this hypothesis, thus confirmingits validity. As stated earlier, the data on which the signal is based originate from thedaily experiences of physicians and pharmacists and have manifested themselves inindividual patients. It is therefore of the utmost importance that appropriatemethods are available to facilitate the collection of these experiences andobservations. In the past few decades several such methods have been developed.The most widely used method is the so-called Spontaneous Reporting System(SRS). A SRS is especially effective for detecting rare and serious adverse drugreactions.(30) All drugs during their whole lifetime are subject to a SRS. It inviteshealth professionals and increasingly also patients to report their observations orinformation to a pharmacovigilance centre. These reports need to contain sufficientinformation to allow an accurate evaluation and a well-founded assessment of therelationship between the suspected ADR and the drug in question (causalityassessment). This implies that a limited number of qualitatively sound reports ispreferred to large quantities of poorly specified reports.The hallmarks of an effective spontaneous reporting system are listed in Table 3. In addition to the SRS pharmacovigilance has several other sources at its disposal.It can make use of the findings generated by the various (pharmaco)epidemiologicalresearch methods; data that may help confirm earlier suspicions. This thesis willalso expand on methods of Intensive Monitoring like Prescription EventMonitoring which has been successfully applied in the UK and New Zealand formany years.(31,32)Publications of case reports are also an important source of information and mayfacilitate the detection of a signal or strengthen earlier signals. And finally, there arethe quantitative methods of signal detection in extensive ADR datasets with whichstudies have been conducted worldwide.(33,34,35) However, this approach shouldbe seen as an additional source of information and not as a panacea for the clinicalassessment of cases.
11
Table 3Hallmarks for an effective spontaneous reporting system (SRS):
- Vigilant users- Creative and competent doctors, pharmacists and other health professionals,
who, when they uncover a likely adverse event, are prepared to report theirsuspicion and do so as fully documented as possible
- Efficient reporting procedures facilitating smooth reporting - A pharmacovigilance centre fully equipped to detect signals
Large sections of this thesis are dedicated to the enhancement of these facets ofpharmacovigilance, hopefully leading to both better and more reports on suspectedadverse drug events.
12
Chapter 1.2The role of the pharmacist
The motivation for this thesis was the observation that the pharmacist’s share in thetotal volume of ADR reports submitted in the Netherlands was considerable,especially when compared to the rest of the world.(36,37) Dutch pharmacists arewell-acquainted with the spontaneous reporting system and they submit roughly40% of the reports the Netherlands Pharmacovigilance Centre Lareb receives. Assuch this is not surprising because from its start it has been Lareb’s aim to promoteADR reporting as a collaborative effort of doctors and pharmacists.(38) Therationale was that a closer cooperation would improve pharmacotherapy since anincreased awareness of adverse effects would not only boost the number andquality of reports but would at the same time encourage these health professionalsto become more actively engaged in the prevention of adverse events, thusencouraging more judicious prescription practices. A recent study shows that in thetwelve months preceding the survey 43% of Dutch community pharmacists hadreported at least one or more ADRs to Lareb.(39)Lareb has always been a testing ground for the cooperation between doctors andpharmacists. In both the General Board and the Scientific Advisory Board as well asat the staff level doctors and pharmacists have always had an equal input. The RoyalNetherlands Society for the Advancement of Pharmacy and the Netherlands Societyof Hospital Pharmacists are both represented in the General Board of Lareb. Withtheir respective clinical and pharmaceutical expertise clinicians and pharmacists eachmake their own specific contribution to the knowledge on adverse drug reactions.
1.2.1 The changing role of the pharmacistThe position of the pharmacist within the health care system has continually beensubject to change. With respect to drug dispensing several tasks can bedistinguished.(40) The pharmacist’s primary mission is to dispense drugs asprescribed by the physician and to ensure these drugs meet the required standards.Nowadays the pharmacist also frequently acts as a consultant on pharmacotherapyand in the UK and USA pharmacists are, to a degree, also authorised to write outprescriptions, which, incidentally, has been a long-standing practice in manycountries where doctors are in short supply.(41,42) The changing role of thepharmacist is most noticeable in The Netherlands. Whereas initially the emphasiswas on the chemical analysis of drugs and its raw materials, the local production ofmedicines and the dispensing role, today the pharmacist’s role has shifted more
13
towards the prevention of adverse drug reactions and interactions, information andinstruction about good use of drugs and is he a consultant on drug therapy, both forphysicians and patients. In the Netherlands a bill is being prepared to award thepharmacist the official status of co-consultant, thus making him jointly responsiblefor pharmacotherapy.(40) Nevertheless, the fundamental role of the pharmacist willalways be to ensure that medicines are used safely.(43)The role the pharmacist plays or is given to play also depends on the circumstancesin which he exercises his profession. In Chapter 3.1 we will elaborate on this issue.The term pharmaceutical care is often used to describe the more comprehensiveinterpretation of the occupation, although the term is given different meanings andoften thought to be too vague.(44,45)In the literature several other ways in which the pharmacist can contribute to thesafe use of drugs are mentioned. In addition to their responsibilities relating to drugdispensing and compliance and their role in ADR reporting, which we will discussin the next section, record keeping, education and their role regarding over-the-counter (OTC) products, both conventional and alternative drugs, are areas wherethey can play a prominent role.(46,47)Since in pharmacy monitoring and consequently also in drug safety more and moreuse is made of automated systems, the pharmacist’s role, both as a user and in hiscapacity of system manager, is also becoming more and more important.
1.2.2 The pharmacist as a reporter of adverse drug reactionsThis thesis specifically focuses on the significance of the pharmacist as a reporter ofadverse drug reactions. As mentioned above, in the Netherlands their contributionis substantial, which cannot be said for the rest of the world. Not only arepharmacists not authorised to report everywhere, even where they are, theircontribution is often still relatively small.(48,49) In an international review, Griffin notes that in 1986 many countries have acceptedpharmacists’ reporting ADRs as standard practice.(50) In 1989 Fincham comments:‘Exclusion of pharmacists simply does not make sense’.(51) In their article in 1993on the differences between European countries Lindquist and Edwards remark:‘Pharmacists who advise patients directly….are the most likely to detect adversereactions’.(52) Roberts et al. conclude in 1994: ‘It is hoped that pharmacists in othercountries will also be encouraged to participate in ADR reporting, a procedure thatcould only lead to better patient care’.(53) The Uppsala Monitoring Centre (UMC)regularly publishes an overview of the ways the national reporting systems in thevarious countries are operated, in which the volume of pharmacist reports are alsolisted.(48) The literature on the actual contribution of pharmacists in ADRreporting often relates to the hospital pharmacist in the USA, Canada and theUK.(54,55,56)
14
The majority of publications concern the ongoing debate in the UK where, for thepast ten years, the desirability of direct reporting by pharmacists has beendiscussed.(43,57)In the various textbooks on pharmacoepidemiology and pharmacovigilance thepharmacist receives little attention, with the exception of Inman who, as early as in1986, devoted a chapter to the role of the pharmacist.(46) The authors examine theircontribution in relation to non-prescription drugs and also point to the medicationhistory pharmacies keep and the edge pharmacists have through the use ofcomputer technology. They conclude by stating: ‘It is to be hoped that protectionof professional territories will not prejudice such a contribution’.
What is important here is that there is mutual respect and acknowledgement ofprofessional expertise. In the literature it has been widely reported that doctorsfully subscribe to a prominent role for pharmacists in drug policies.(58) In Chapter3.1 the role of the pharmacist in relation to ADR reporting is discussed from aninternational perspective. In Chapters 3.2 and 3.3 we focus on the pharmacists’attitude towards and their actual contribution to ADR reporting.
1.2.3 The contribution of the hospital pharmacistHospital pharmacists can also play a significant role in ADR reporting. It is in theirwork environment that the most serious adverse drug events can be seen to occur.Several recent publications have underlined the extent to which adverse drug eventsaccount for hospital admissions. In the US this was 6.7%, for France a percentageof 3.2 has been reported and for Sweden the most recent figure is 12%. (59,60,61)Evidently, there is every reason to make the prevention and recording of adverseevents occurring in hospitals a priority, to control both their harmful effects and thecosts resulting from these events.(62) This process could best be supervised byhospital pharmacists, particularly when they are directly involved in patientcare.(62) Several articles have specifically highlighted this role and have suggestedthat hospital pharmacists could help reduce the ADR incidence ratesubstantially.(54,63) And yet, their potential in this context is not always recognisedas two German studies have shown. Neither of the two studies, one on thedetection of adverse drug reactions in hospitals and the other investigating theincidence of ADRs and the resultant costs, mention the hospital pharmacist.(64,65)Several prerequisites need to be fulfilled to ensure that their contribution willindeed help bring down the number of adverse events and improve ADR reporting:direct involvement in patient care and a functional, widely supported hospitalreporting system in whose management the hospital pharmacist should have a keyrole. Apart from their quantitative relevance, ADR reports from hospitals also raisethe quality of ADR monitoring because of their high-quality
15
documentation.(47,56) If hospitals were to report more, this would also enhancethe surveillance of those drugs that are chiefly used in hospital settings.(47)Moreover, hospital pharmacists also have more and more advanced means at theirdisposal to monitor drug safety, such as sophisticated computer systems anddatabases as well as the possibility to investigate deviant lab test results, whichmethods are not or less available elsewhere.(64,66)The contribution pharmacists make to ADR reporting is by far the largest In theUS. Here the majority of the reports the Food and Drug Administration (FDA)receives direct from health professionals originate from hospitalpharmacists.(67,68,69) The FDA particularly encourages this professional group toreport, also because of the high standard of their reports.(68,70) The fact that theyplay such a key role is the direct result of a stipulation of the Joint Commission onAccreditation of Health Care Organizations (JCAHO) requiring hospitals tosustain an ADR monitoring programme.(69,70,71,72) Evidently, they view suchhospital reporting systems as a crucial element of the national reporting system.The same situation applies to Canada, although that here it was the CanadianSociety of Hospital Pharmacists that took the initiative.(73) The contribution ofhospital pharmacists to their national system was also significantly augmented.(42)The Netherlands Society of Hospital Pharmacists (NVZA) and the NetherlandsPharmacovigilance Centre Lareb took the initiative of drawing up a plan to grantthe hospital pharmacist a structural place in ADR reporting but it will take sometime before such a plan is implemented.(74)In the United Kingdom there has been a long lasting discussion over the positionof the (hospital) pharmacist within the reporting system. As early as in 1982Hardman and Lloyd proposed to grant the hospital pharmacist an active role in themonitoring of adverse drug reactions.(75) A structural collaboration betweenclinicians and hospital pharmacists was proposed by Irvin et al.(76) Winstanley etal. have demonstrated that the initiation of a pharmacy-based reporting scheme ledto a substantial increase of the number of ADR reports, a finding that was laterconfirmed by Lee et al.(67,77) Nevertheless, it was not until 1997 that the hospitalpharmacist was officially allowed to report ADRs to the national SRS.
1.2.4 The contribution of the community pharmacistThis thesis specifically elaborates on the role of the community pharmacist in ADRreporting, which is not surprising since in the Netherlands it is particularly this groupthat contributes most to drug safety monitoring. From an international perspectivethis is quite remarkable because in most other countries this role is predominantlyfulfilled by the hospital pharmacist, whereas in the Dutch system their share isrelatively small. Both the community pharmacist’s attitude (Chapter 3.2) as hisconcrete contribution (Chapters 3.3 and 3.4) are discussed.
16
To date, little is known about their position or contribution in other countries andhas only been described for Cuba.(78) However, in the literature their potential rolein relation to non-prescription medicines (‘over-the-counter drugs’) has receivedsome attention.(79,80) This not only concerns non-prescription drugs but alsoalternative medication; pharmacists are uniquely placed to learn of these ADRs andreport them.(47) As regards the potential role of the pharmacist in relation to ADR reportingFincham stated: ‘Efforts must be expanded to include pharmacists in every ADRsurveillance activity’.(51) Also Kelly’s remark on the subject gets to the heart of thematter: ‘Pharmacovigilance: more a responsibility than a role!’ (49)
17
Chapter 1.3 Outline of the thesis
The present dissertation is about the safety of drugs, more specifically theirsurveillance after the regulatory authorities have judged their efficacy, quality, andsafety sufficiently proven for the drugs to be applied in the clinical practice. Afterthe thalidomide disaster in the early 1960s the awareness that drugs can constitutea serious risk was raised dramatically and, in addition to stringent approvalprocedures, a scheme was developed to monitor the safety of marketed drugs.Pharmacovigilance is responsible for both the scheme’s theoretical underpinningand its practical implementation. For its implementation pharmacovigilance mainlyrelies on a (spontaneous) reporting system where clinicians and pharmacists canreport their suspicions of any adverse drug reactions (ADRs), which aresubsequently analysed. This thesis is about pharmacovigilance, what it entails andhow it can be improved, with particular emphasis on the role pharmacists can playin this process, as is explained in Part 1.
Part 2 of the thesis provides the framework for the subsequent parts of it.Chapters 2.1 and 2.2 expand on various aspects of the history of drug safetymonitoring, where Chapter 2.2 is a tribute to professor dr. L. Meyler, who with hisbook ‘Side effects of drugs’ paved the way for a systematic attention for adverseevents associated with drug use in the clinical practice. Motivated by his personalexperiences, he wrote down his observations at a time when this aspect of drugs wasstill very much underestimated. Chapter 2.3 provides an overview of the various ways in which pharmacovigilanceis implemented in the Netherlands and the organisations that are involved. Thespecial position of the pharmacist in the Dutch situation is also discussed.Chapter 2.4 is dedicated to the unique quality of pharmacovigilance as a scientificdiscipline, which is illustrated by the concept of ‘underreporting’. It is stressed thatthe view that underreporting is its major drawback does not do justice to the realbasis and purpose of pharmacovigilance and that those who take this position donot appreciate what can and cannot be achieved with the data a reporting systemgenerates.
Part 3 expands on the role the pharmacist has or should have in the detection andreporting of adverse drug reactions. Chapter 3.1 compares the situations in the various countries that participate in the
19
WHO Drug Monitoring Programme. In Chapter 3.2 we report the results of asurvey held among Dutch community pharmacists on their attitude to ADRreporting. It is concluded that their knowledge and the conditions are such thattheir commitment to report is high. Several factors that may influence theircommitment and actual reporting behaviour are also discussed.The contribution of Dutch pharmacists to the Netherlands PharmacovigilanceCentre Lareb between the years 1995 and 2000 is analysed in Chapter 3.3, both inquantitative and qualitative terms. During this period their share in the volume ofreported ADRs was indeed substantial, i.e. 40%. The quality of the pharmacistreports is compared to that of the reports Lareb received from physicians.Chapter 3.4 demonstrates how a report Lareb received from a communitypharmacist, containing high-quality information, resulted in a scientific paperpublished in an international journal. The paper warns clinicians and pharmaciststhat, similar to existing oral contraceptives, a newly introduced oral contraceptivealso carries the risk of thrombosis.
Part 4 focuses on what can be done to improve pharmacovigilance, again withspecial reference to the pharmacist.In Chapter 4.1 a pilot study is described in which a method, allowing recentlyapproved drugs to be monitored more intensively, is tested. This method isespecially relevant given that the safety information for new drugs as based on theirclinical usage is still limited.By making use of so-called first delivery signals generated by the automatedsystems of pharmacies, the doctor who has prescribed the drug in question isinvited to anonymously report his or her experiences with its use. Wide-scaleapplication of this method may mean that new insights into the clinical safetyprofile of newly marketed drugs can be obtained sooner.For questions relating to the safety of the drugs they have been prescribed patientswill often turn to the pharmacist. In the Netherlands they have an additional sourceof information at their disposal, namely a national drug helpline (‘GeneesmiddelenInfolijn’), which service is also maintained by pharmacists. By comparing thepatients’ queries the helpline received during one year to the pharmacist reportsthat were submitted to Lareb in the same period, we were able to assess whether thelatter were an accurate representation of the concerns patients expressed. Thefindings of this comparative study are discussed in Chapter 4.2.An alternative way to do justice to the concerns drug users have, is by giving themthe opportunity to report their concern directly to the national pharmacovigilancecentre without mediation of their GP or pharmacist. Chapter 4.3 details the prosand cons of such a system of direct patient reporting.The primary aim of drug safety monitoring or pharmacovigilance is to acquire new
20
insights into the safety of (new) drugs based on the analysis of reports on suspectedadverse events. Ultimately, this new knowledge needs to benefit those that use thedrugs. To achieve this doctors and pharmacists need to be informed about any newrisks or about earlier risks that have been substantiated. The most commonlyapplied method is to adjust the content of the Summary of Product Characteristics(SPC) and consequently the Patient Package Insert (PPI) where, among otheraspects, the drug’s known adverse reactions are outlined, warnings andcontraindications are specified and precautionary measures recommended.In exceptional cases clinicians and pharmacists may be alerted to a suspected risk bymeans of a ‘Dear Doctor Letter’. However, in practice these measures have beenfound to have little impact, which lack of response may sometimes lead to thedrug’s approval being revoked or, alternatively, to the Marketing AuthorisationHolder voluntarily taking the product off the market. If new insights were to beimplemented better, drastic measures like these may be prevented. In Chapter 4.4 this dilemma is discussed in detail and several routes are proposedthat may help to improve the practical implementation of the new knowledge ondrug safety that we have derived from the clinical and practical experiences of bothdoctors and pharmacists, for the benefit of those for whom the medical andpharmaceutical care is intended: the patients.
Part 5 gives a synthesis of this thesis and a perspective into the future.
21
References
1. Jick H. Drugs: remarkably nontoxic. N Engl J Med 1974;291:821-8.
2. Muntendam P. Openingstoespraak. In: Het nieuwe geneesmiddel. Boerhaave CursussenLeiden 1964.
3. Anomymus. World pharma sales growth slows to 7% in 2002. Script 2003;2835:16.
4. Meyler L. Waarom klinische farmacologie? [Why clinical pharmacology?]. Ned TijdschrGeneeskd 1969;113:1275-9.
5. WHO. International Drug Monitoring: The Role of National Centres. Technical ReportSeries. Geneva 1972.
6. Edwards IR. Spontaneous reporting – of what? Clinical concerns about drugs. Br J ClinPharmacol 1999;48:138-41.
7. Waller P. Dealing with uncertainty in drug safety: lessons for the future from sertindole.Pharmacoepidemiol Drug Saf 2003;12:283-88.
8. Figueras A, Laporte J-R. Failures of the therapeutic chain as a cause of drug ineffectiveness.Promotion, misinformation, and economics work better than needs. BMJ 2003;326:895-6.
9. WHO. The Importance of Pharmacovigilance, Safety Monitoring of medical products. WHOGeneva 2002.
10. Rawlins MD. Pharmacovigilance: paradise lost, regained or postponed. The William WitheringLecture 1994. J Royal Coll Phys London 1995;29:41-9.
11. Mann R, Andrews E, editors. Pharmacovigilance. Wiley Chichester 2002.
12. Grootheest AC van, Edwards IR, Labelling and ‘Dear Doctor’ letters: are the noncommittal?Drug Saf 2002;25:1051-55.
13. Seligman PJ. ‘Dear Doctor…’- Evaluating the impact of risk communication efforts.Pharmacoepidemiol Drug Saf 2003;12:291-4.
14. Mills A, Edwards IR. Venous thromboembolism and the pill. Hum Reprod 1999;14:7-10.
15. Moore N. The Role of the Clinical Pharmacologist in the Management of Adverse DrugReactions. Drug Saf 2001;24:1-7.
16. Edwards IR, Hugman B. The challenge of effectively communicating risk-benefit information.Drug saf 1997;17:216-27.
22
17. Edwards IR. Withdrawing drugs: nefazadone, the start of the latest saga. Lancet2003;361:1240.
18. Waller PC, Coulson RA, Wood SM. Regulatory pharmacovigilance in the United Kingdom:current principles and practice. Pharmacoepidemiol Drug Saf 1996;5:363-75.
19. Olsson S. The Role of the WHO Programme on International Drug Monitoring inCoordinating Worldwide Drug Safety Efforts. Drug Saf 1998;19:1-10.
20. Lindquist M, Edwards IR. The WHO Programme for International Drug Monitoring, ItsDatabase, and the Technical Suport of the Uppsala Monitoring Centre. J Rheumatol2001;28:1180-7.
21. Lindquist A.M. Seeing and Observing in International Pharmacovigilance. Academic thesis.Katholieke Universiteit Nijmegen. Nijmegen 2003.
22. Strom BL, editor. Pharmacoepidemiology, 3e edition. Wiley Chichester 2000.
23. Vandenbroucke JP. Het belang van medische casuïstiek te midden van ‘evidence-based’geneeskunde en moleculaire verklaringen. (The importance of case reports as compared toevidence-based medicine and molecular explanations) Ned Tijdschr Geneeskd 2002;36:1699-1703.
24. Vandenbroucke JP. Clinical investigation in the 20th century: the ascendancy of numericalreasoning. Lancet 1998;352 Suppl II:12-6.
25. Meyboom RHB. Detecting adverse drug reactions, Pharmacovigilance in The Netherlands.Thesis. Katholieke Universiteit Nijmegen 1998.
26. Puijenbroek EP van. Quantitative Signal Detection in Pharmacovigilance. Thesis. Universityof Utrecht 2001.
27. Arnaiz JA, Carné X. Riba N, Codina C, Ribas J, Trilla A. The use of evidence inpharmacovigilance. Case reports as the reference source for drug withdrawals. Eur J ClinPharmcacol 2001;57:89-91.
28. Venning GR. Validity of anecdotal reports af suspected adverse drug reactions: the problem offalse alarms. BMJ 1982;284:249-52.
29. Meyboom RHB, Egberts ACG, Edward IR , Hekster YA, Koning FHP de, Gribnau FWJ.Principles of Signal Detection in Pharmacovigilance. Drug Saf 1997;16:355-65.
30. Temple R. Meta-analysis and Epidemiologic Studies in Drug Development and PostmarketingSurveillance. JAMA 199;281:841-4.
31. Coulter DM. The New Zealand Intensive Medicines Monitoring Programme In Pro-activeSafety Surveillance. Pharmacoepidemiol Drug Saf 2000;9:173-80.
23
32. Mann RD. Prescription-event monitoring – recent progress and future horizons. Br J ClinPharmacol 1998;46:195-201.
33. Puijenbroek EP van, Bate A, Leufkens HGM, Lindquist M, Orre R, Egberts ACG. Acomparison of measures of disproportionality for signal detection in spontaneous reportingsystems for adverse adverse drug reactions. Drug Saf 2002;11:3-10.
34. Bate A. The Use of a Bayesian Confidence Propagation Neural Network inPharmacovigilance. Umeå University Medical Dissertations New Series No 846. Umeå 2003.
35. Puijenbroek EP van, Diemont WL, Grootheest AC van. Application of Quantitative SignalDetection in the Dutch Spontaneous Reporting System for Adverse Drug Reactions. Drug Saf2003;26:293-301.
36. Grootheest AC van, Puijenbroek EP van. Apothekers kennen Lareb – is dat zo (Pharmacistsknow Lareb – is that true?). Pharm Weekbl 2002;135:189-91.
37. Puijenbroek EP van, Grootheest AC van. Lareb in maat en getal: kwantiteit versus kwaliteit.[Lareb measured and in numbers: quantity versus quality] Pharm Weekbl 2000;135:501-4.
38. Koning GPH de. A regionalized spontaneous surveillance program for adverse drug reactionsas a tool to improve pharmacotherapy. Academic thesis. Utrecht University, Faculty ofPharmaceutical Sciences, Utrecht 1994.
39. Inspectie voor de Gezondheidszorg. Voorwaarden voor verantwoorde farmaceutischezorgverlening door openbare apothekers onderzocht [Conditions for responsable pharmaceuticcare studied with community pharmacists] (with summary in English). Den Haag 2003.
40. Brouwers JRBJ, Roon EN van, Toering DJ. De ziekenhuisapotheker als farmacotherapeut[The clinical pharmacist as pharmacotherapist]. Pharm Weekbl 2003;138:692-6.
41. Clause S, Fudin J, Mergner A, Lutz JL, Davanaugh MM, Fessler K, Chirumamilla S.Prescibing privileges among pharmacists in Veterans Affairs medical centres. Am J Healt-SystPharm;58:1143-5.
42. Grootheest AC van, Puijenbroek EP van, Jong – van den Berg LTW de. Pharmacists’ role inreporting adverse drug reactions in an international perspective. Pharmacoepidemiol Drug Saf(in press).
43. Beard K. Introduction. In: Adverse Drug Reactions. Pharmaceutical Press. London 2001.
44. Mil F van, McElnay J, Jong-van den Berg LW de, Tromp DFJ. The challenges of definingpharmaceutical care on an international level. Int J Pharm Pract 1999;7:202-8.
45. Strom BL, Hennessy S. Pharmacist Care and Clinical Outcomes for Patients With ReactiveAirways Disease. JAMA 2002;288:1642-3.
46. Poston J, Parish P. The pharmacists. In: Monitoring for drug safety (WHW Inman, editor).MTP Press. Lancaster 1986.
24
47. Major E. The yellow card scheme and the role of pharmacists as reporters. Pharm J2002;269:25-6.
48. Olsson S. National Pharmacovigilance Systems – Country Profiles and Overview (secondedition). Uppsala Monitoring Centre. Uppsala 1999.
49. Kelly B. Pharmacovigilance: more a responsibility than a role. Austr Pharm 2001;20:128.
50. Griffin JP. Survey of the spontaneous adverse drug reactions reporting schemes in fifteencountries. Br J Clin Pharmacol 1986;12:243-7.
51. Fincham JE. Adverse Drug Reaction Reporting and Pharmacists. J Clin Pharm Therapeutics1989;14:79-81.
52. Lindquist M, Edwards IR. Adverse drug reactions reporting in Europe: some problems ofcomparison. Int J Risk Safety Med 1993;4:35-46.
53. Roberts PI, Wolfson DJ, Booth TG. The Role of Pharmacists in Adverse Drug ReactionReporting. Drug Saf 1994:11:7-11.
54. Leape LL, Cullen DJ, Dempsey Clapp M, Burdick E, Demonaco HJ, Erickson JI, Bates DW.Pharmacist Participation on Physician Rounds and Adverse Drug Events in the Intensive CareUnit. JAMA 1999;282:267-70.
55. Wistanley PA, Irvin LE, Smith JC, Orme ML’E, Breckenridge AM. Adverse Drug Reactions:a hospital pharmacy-based reporting scheme. Br J Clin Pharmac 1989;28:113-6.
56. Ahmad SR, Freiman JP, Graham DJ, Nelson RC. Quality of Adverse Drug ExperienceReports Submitted by Pharmacists and Physicians to the FDA. Pharmacoepidem Drug Saf1996;5:1-7.
57. Roberts PI, Wolfson DJ, Booth TG. The Role Of Pharmacists in Adverse Drug ReactionReporting. Drug Saf 1994:11:7-11.
59. Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalizedpatients: a meta-analysis of prospective studies. JAMA 1998;279:1200-5.
60. Pouyanne P, Haramburu F Imbs JL, Bégaud B. Admissions to hospital caused by adverse drugreactions: cross sectional incidence study. BMJ 2000;320:1036.
61. Mjörndal T, Boman MD, Hägg S, Bäckström M, Wiholm B-E, Wahlin A, Dahlqvist R.Adverse drug reactions as a cause for admissions to a department of internal medicine.Pharmacoepidemiol Drug Saf 2002;11:65-72.
62. Anonymus. Top-priority actions for preventing adverse drug events in hospitals.Recommendations of a expert panel. Am J Health-Syst Pharm 1996;53:747-751.
25
63. Bemt PMLA van de. Drug Safety in Hospitalised Patients. Thesis Rijksuniversiteit Groningen.Groningen 2002.
64. Dormann H, Muth-Selbach U, Krebs S, Criegee-Rieck M, Tegeder I, Schneider HT, HahnEG, Levy M, Brune K, Geisslinger G. Incidence and Costs of Adverse Drug Reactions DuringHospitalisation. Drug Saf 2000;22:161-8.
65. Thürmann PA. Methods and Systems to Detect Adverse Drug Reactions in Hospitals. DrugSaf 2001;24:961-8.
66. Emerson AE, Martin RM, Tomlin M, Mann RD. Prospective cohort study of adverse eventsmonitored by hospital pharmacists. Pharmacoepidemiol Drug Saf 2001;10:95-103.
67. Lee A, Bateman DN, Edwards C, Smith JM, Rawlins. Reporting of adverse drug reactions byhospital pharmacists: pilot schema. BMJ 1997;315:520-23.
68. Thürmann PA. Methods and Systems to Detect Adverse Drug Reactions in Hospitals. DrugSaf 2001;24:961-8.
69. Kennedy DL, Goldman SA, Lillie RB. Spontaneous Reporting in the United States. In:Pharmacepidemiology. WHW Strom, editor. John Wiley and Sons. Chichester, UK 2000.
70. Sills JM, Tanner AM, Milstien JB. Food and Drug Administration monitoring of adverse drugreactions. Am J Hosp Pharm 1986;43:2764-70.
71. Accreditation Manual for Hospitals 1993. Joint Commission on Accreditation of HealthcareOrganizations, Oakbrook Terrace, Ill, 1993.
72. Strom BL. Pharmacoepidemiology: Response to the Challenge. Pharmacoepidemiol Drug Saf1995;4:11-4.
73. CSHP. Standards of Practice. Canadian Society of Hospital Pharmacists. 1990.
74. Het melden van bijwerkingen, de rol van de ziekenhuisapotheker. [The reporting of ADRs,the role of the hospital pharmacist]. Lareb 's-Hertogenbosch 2001.
75. Hardman C, Lloyd B. Adverse drug reaction monitoring by ward pharmacists. J Clin HospPharm 1982;7:71-3.
76. Irvin LE, Grimmer SFM, Smith JC. Adverse drug reaction reporting. Br J Pharm Pract1987:316-21.
77. Winstanley PA, Irvin LE, Smith JC, Orme LE, Breckenridge AM. Adverse drug reactions: ahospital pharmacy-based reporting scheme. Br J Clin Pharmac 1989;28:113-6.
78. Debesa F, Giménez G, Firgueras A, Diogène E, Peña JP, Avila J, Laport J-R. Spontaneousreporting of adverse drug reactions in Cuba: integrating continuous education, training andresearch in a network approach. Br J Clin Pharmacol 2002;54:333-6.
26
79. Sinclair HK, Bond CM, Hannaford PC. Pharmacovigilance of Over-the-Counter Productsbased in community pharmacy; a feasible option? Pharmacoepiol Drug Saf 1999;8;479-91.
80. Sinclair HK, Bond CM, Hannaford PC. Long Term Follow-Up Studies of Users ofNonprescription Medicines Purchased from Community Pharmacies. Drug Saf 2001;24:929-39.
27
2Pharmacovigilance
Chapter 2.1 The dawn of pharmacovigilance- Pharmacovigilance in historical perspective
Drug Safety (accepted)
Kees van GrootheestNetherlands Pharmacovigilance Centre Lareb
31
Abstract
In this chapter an anecdotal view from a Dutch perspective is given on somehistorical aspects of both the awareness and the systematic attention regardingadverse drug reactions, in a period before the word pharmacovigilance even existed.What we can learn form history is illustrated by the study of Lely, who discoveredthat 19 people died from digitalis intoxication, due to a production error of thedigitalis tablets. His observations of the symptoms of digitalis intoxication were inthe 18th century already described by Withering in his study on the foxglove. The Professor of Medicines Van Doeveren is another early example of awareness ofadverse drug effects, when he gave the academic lecture called “Remedio Morbi” in 1789 on diseases caused by treatment. This academic lecture was given attentionby Meyler, who wrote his famous book on adverse drug reaction in 1951. His book“Side effects of drugs” is currently in its 14th edition and is still a standard work inthis field. An early example of systemic collection of adverse drug reactions occurred in thebeginning of the 19th century, by the reporting of these during a smallpoxvaccination campaign in the Netherlands. Systematic attention to adverse drug reactions, including the collection of ADRreports, was boosted by the so called thalidomide disaster in the early sixties of thelast century. Since then, governments started to organize national pharmaco-vigilance centres to prevent such a disaster to happen again. The WHO has played an important role in developing this reporting of adverse drugreactions with its WHO International Drug Monitoring Program and the WHOUppsala Monitoring Centre, maintaining the international database of adverse drugreactions.A comprehensive review of the history of pharmacovigilance is still to be written
32
2.1.1 IntroductionSystematic attention to adverse drug reactions started with the thalidomide disaster inthe early sixties of the twentieth century. Of course, also before that period there wasawareness of possible negative aspects of drug therapy. In this chapter we will look,quite anecdotal and mainly from a Dutch perspective, to some historical aspects ofboth the awareness regarding adverse drug events and the systematic attention thathas been given to it in a period when the word pharmacovigilance did not even exist.
2.1.2 Can we learn from the past?In March 1971 A.H. Lely, MD and specialist in internal medicine, received hisdoctorate from Prof. dr. L. Meyler at the University of Groningen for his thesisentitled: ‘Digitalisintoxicatie, waarnemingen betreffende een massale digitoxine-intoxicatie te Veenendaal’ (Digitalis intoxication, observations on a mass digitoxinintoxication in the Dutch town of Veenendaal).(1) Early February 1969 Lely hasdetected symptoms of digitalis intoxication in a number of his patients. Hissubsequent investigations revealed that since December the sixth of the previousyear the local pharmacist had dispensed tablets that were not composed of therecommended 0.25 mg of digoxin but, due to a production error, contained acombination of 0.20 mg of the more potent digitoxin and 0.05 mg of digoxininstead, which magnified the effect of the heart glycoside, making it 2.2-4.2 morestronger than indicated. Lely concluded that this error was implicated in at least 19deaths. Probably this disaster may have caused far more fatalities that were notidentified, despite the fact that nationwide five times as many tablets with thewrong compound and dose had been dispensed than had been the case inVeenendaal and its immediate surroundings.Several aspects of this tragedy merit particular attention. First, there is the fact that untilshort before the pharmacist involved had produced the tablets himself at the pharmacy.The serious production error happened to coincide with his decision to start purchasingand dispensing industrially produced drugs, causing far greater damage than wouldhave been the case if the error was made with a local produced tablet.A second important aspect is that an observant physician had been able to detect theerror based on the symptoms his patients were exhibiting and informed others ofhis suspicions, thus preventing any further harm. It is very likely that many of hiscolleagues were also confronted with the signs of digitalis intoxication. The reasonwhy they failed to recognise the adverse reactions may be that they were not awareof the main concomitant symptoms, namely serious fatigue (93%), disturbed vision(85%), anorexia nervosa (84%), psychological complaints (64%) and abdominalpains (57%).(1) It is also feasible that they may have realised that there were adversereactions but did not inform others of their observations. These elements are stillkey aspects of pharmacovigilance.
33
Within the context of this chapter another aspect of Lely’s study needs to bementioned. Lely points out that the botanist William Withering from Birmingham,England, had already extensively described the symptoms of a digitalis intoxicationas early as in 1785.(2,3) In his book ‘An Account of the Foxglove and Some of ItsMedical Uses: with Practical Remarks on Dropsy and Other Diseases’ he describesthe symptoms as follows: ‘The Foxglove, when given in very large and quicklyrepeated doses, occasions sickness, vomiting, purging, giddiness, confused vision,objects appearing green or yellow; increased secretion of urine, with frequentmotions to part with it, and sometime inability to retain it; slow pulse, even as slowas 35 in a minute, cold sweats, convulsions, syncope and death’.Although the knowledge about the pharmacological properties of digitalis, thediagnostic possibilities and the therapeutic approaches for the treatment of anoverdose have increased significantly in the two centuries following thispublication, the characteristic symptomatology has not changed and has alreadybeen described 200 years before. Knowledge, a keen sense of observation and athorough anamnesis and diagnosis have not only formed, and still form, the basisof medicine, but also of pharmacovigilance, the science that is concerned with thesafe use of drugs in daily practice.Against the background of this case concerning digitalis, some historical aspects ofthe awareness regarding adverse drug reactions and the systematic collection of itwill be discussed.
2.1.3 Adverse drug reactions in historical perspectiveIn 1789, Wouter van Doeveren, Professor of Medicine at Leiden University, gave apublic lecture with the title ‘Remedio morbo, drug diseases or ailments which oftenaffect people as a result of remedies administered to them for therapeuticpurposes’.(4,5,6) This address, which did not appear in print, but the manuscript ofwhich is kept in the University Library of Amsterdam, may be seen as the firstexpression of an emerging scientific interest in adverse drug reactions.(7) Wouter van Doeveren, born in Philippine, a village in the Dutch province of Zeeland,started his study of medicine in Leiden at the age of seventeen. He received a First (anhonours degree cum omnium applausu) for his thesis on worms ‘De vermibusintestinalibus hominum, praecipue de taenia’. This dissertation would long beregarded as a standard work on worms and was translated into German and French.In 1754 he was appointed to the chair of Medicine at Groningen. Here he engaged inmany activities, such as the promotion of the inoculation with cowpox. In 1770 hewas appointed professor of the faculty of medicine at Leiden where he succeededHerman Boerhaave, whose ideas were still the norm at the faculty. Van Doeveren wasa good clinician, an ‘evidence-based’ researcher avant la lettre, and a critic of themedical practices of that time, opposing many of the prevalent irrational therapies.
34
Especially during his time at Groningen University Van Doeveren produced a largebody of research in the fields of anatomy, physiology and obstetrics. Whenstepping down as rector magnificus of Leiden University in 1779 he makes hisfamous Sermo academicus de remedio morbo (‘Academic lecture on diseases as aresult of treatment’).(7) In this address he observes that physicians are seldommoderate in their judgments of treatment methods and are rather inclined to regardthem as either essential or hazardous. He points out the hazards of the artificialinducement of fevers and argued against bloodletting and the administration ofperspiration-inducing drugs for acute fevers. He concludes his speech with theobservation that many illnesses are the result of ‘empirical treatments’ administeredwithout a proper diagnosis, thus causing remedio morbi, illnesses that result froma treatment. He warned his audience: ‘Lest you will not be too easily persuaded tohand out medications, which may carry the risk of your adding a second ailment tothe first, or through which you may perhaps even invite death or accelerate it’!
Earlier in this chapter William Withering (1741-1799) and his 1785 work on thefoxglove is mentioned. His work has become known as the first systematic paperon a medicinal drug and gives attention to the adverse effects of the treatmentwith digitalis. The Royal College of Physicians of London commemorate hisachievements with their annual William Withering lecture. In 1994 Michael D.Rawlins was invited to deliver that year’s lecture.(3) His address that has sincebecome a standard reference in pharmacovigilance, was entitled ‘Pharmaco-vigilance: paradise lost, regained or postponed?’. He stated that in our moderntimes Withering’s work could easily serve as an Expert Report when applying formarketing approval. Withering, for example, explains the synthesis of digitalisfrom the foxglove in a standardised way, describes animal tests conducted onturkeys, details the therapeutic effects and the symptoms associated with anoverdose, emphasising the importance of a proper measurement of the dose.(2)
Without question, ahead of Van Doeveren and Withering others will have pointedto the possible harmful effects of medications although this cannot be corroboratedby specific evidence. The basic principle that therapeutic gain needs to outweighany possible damage was already recorded by Hippocrates: primum nil nocere, firstof all do no harm. There is historical evidence available showing that authorities supervised themanufacture of drugs. These activities ultimately resulted in the Pharmacopee. Oneof the aims of founding the FDA in 1906 also was to impose quality criteria for themanufacture of drugs. More stringent criteria were drawn up in 1938 following 107fatalities caused by the use of ethylene glycol as a solvent.(8)
35
The systematic cataloguing of illnesses that may occur as a concomitant effect ofpharmacotherapy is not taken up until much later. In 1881 a book is published byL. Lewin: ‘Die Nebenwirkungen der Arzneimittel: pharmakologisch – klinischHandbuch’.(9) The key work providing an overview of the existing literature onadverse drug reactions is written by L. Meyler in Dutch under the title ‘Schadelijkenevenwerkingen van geneesmiddelen’ and is published in 1951. It is directlyfollowed by an English translation: ‘Side effects of drugs’, published in 1952. It wassubsequently translated into many other languages.(10,11) New editions appearregularly under the title ‘Meyler’s Side Effects of Drugs’; in 2002 the 14th editionwas released. Meyler’s work, published ten years prior to the thalidomide tragedy,is soon followed by other publications. In 1953 ‘Maladies médicamenteuses’ by C.Albahary is released, followed in 1954 by G. Duchesnay’s ‘Le risque thérapeutique,prévention et traitement des accidents’.(12,13) In 1955 both the English publication‘Reactions with Drug Therapy’ by H.L. Alexander and the German overview‘Erkrankungen durch Arzneimittel, Diagnostik, Klinik, Pathogenese, Therapie’,edited by R. Heintz, appear.(14,15)In 1961 the thalidomide tragedy causes a surge in the publications on adverse drugeffects, famously led by McBride’s article.(16,17)
2.1.4 Pharmacovigilance in historical perspectivePharmacovigilance concerns the science and activities relating to the detection,assessment, understanding and prevention of adverse drug effects or any other possibledrug-related problems, according to a recent WHO publication.(18) Until thethalidomide tragedy in 1961, when the devastating side effects of the drug came tolight, the systematic collection and analysis of adverse drug events had not receivedmuch attention, although there are several examples of a systematic attention for the(negative) effects of drugs that go further back.Already in the beginning of the 19th century the systematic reporting of adverseeffects, in this case regarding vaccines, is noted and will be described here.Above, Van Doeveren’s effort in Groningen to promote the cowpox vaccination ismentioned. He was one of the protagonists in a long-drawn-out debate, initiated byLady Montagu, relating to the religious, medical-scientific and financial implicationsof such an inoculation. During her travels in Turkey in 1718 Lady Montagu had her 6-year-old son vaccinated and, back in England in 1721, also had her 6-year-old daughterimmunised in the presence of three members of the Royal College of Physicians toprove the safety of inoculation. In the Netherlands, the first time the vaccination wasadministered was in Amsterdam in 1748, where Boerhaave’s student TheodoreTronchin, immunised his eldest son after his second son had barely survived a seriousattack of the smallpox.(19) Van Doeveren administers the vaccination for the first timein Groningen in 1759. And although Boerhaave had already claimed that the
36
prophylactic effect of the immunisation was considered to be reliable and safe, also inGroningen a heated debate took place, culminating in a campaign against VanDoeveren. In Leiden the vaccination was prohibited and Van Doeveren undertooklittle to counteract this decision when he became a professor over there. Nevertheless, his efforts to get the cowpox immunisation accepted in Groningenapparently were successful, possibly aided by the hugely positive response toEdward Jenner’s work, who, in 1798, had published his ‘An enquiry into the causesand effects of the variolae vaccinae’, followed a year later by ‘Further observationson variolae vaccinae’. And once again, the Royal College of Physicians played aprominent role and thanks to their involvement and perhaps also partly due to theFrench occupation, a vigorous campaign to boost the use of the cowpox vaccinationis launched in the Netherlands. A directive, dated 25 August 1808, stipulates anumber of measures to promote the vaccination, as is illustrated by a placard the‘Landdrost’ (local administrator) of the province of Groningen has distributed.(20)The three physicians who administered the largest amount of vaccinations, with aminimum of 100, are to be awarded a gold coin to the value of ten ducats. To be eligiblefor the remuneration, they have to submit a record listing the personal data of theirpatients every three months, but also a statement as to ‘whether the injected cowpoxhave taken and have had a regular effect, also stipulating any peculiarities that mayhave occurred’. Thus, in fact, the spin-off of the debate on the cowpox vaccination wasthat its side effects were monitored systematically! What also strikes is the fact that theregulation also mentions that ‘the beneficial effects of the inoculation […] have notonly been proven in this Realm, but have also been conclusively demonstrated in otherNations’. Apparently, evidence was available and exchanged internationally.
In his article on 150 years of pharmacovigilance Philip Routledge refers to a committeethat was set up by The Lancet to collect reports on mortalities resulting fromanaesthesia in Britain and its colonies. The results of which have been published in TheLancet.(21,22) The committee was a reaction to the death of a 15-year-old girl in 1848who had undergone chloroform anaesthesia in connection with an ingrown toenail! In 1950 reports of incidences of aplastic anaemia associated with the use ofchloramphenicol were received in the US.(23) This led the Council on Drugs of theAmerican Medical Association to set up a Blood Dyscrasia Registry.(24)
2.1.5 Drug safety since 1960In 1961 the Australian physician McBride published a letter in The Lancet in which hesuggests a connection between congenital malformations in newly born infants and thehypnotic thalidomide, which was marketed under various names in many countries. Itwas available both as a prescription and as an over-the-counter (OTC) drug and alsoin many compositions of simple analgesics.(16) Thalidomide was first synthesized in
37
1953 and in 1956 an intensive campaign was launched to promote the drug (undervarious names such as Contergan®, Distavel®, Softenon®) first in Germany, then inEngland (1958) and subsequently in other countries. Although McBride had alreadysubmitted his letter in June 1961, the publication appeared in December 1961 afterresubmission. Earlier, on November the 19th 1961, at a conference on paediatrics theGerman physician Dr. Lenz from Hamburg argued that there was a correlationbetween the many births of children with congenital deformities and the use ofthalidomide, which relationship had incidentally already attracted some attentionbefore that time. On 25 November 1961 the manufacturer Chemie Grünenthalwithdrew thalidomide from the market. The number of children born with seriouscongenital malformations as a result of maternal use of thalidomide is estimatedbetween 6,000 and 12,000, the majority of which were born in Germany.(25,26)Noteworthy in this context is that today toxicology and the surveillance of congenitalabnormalities frequently fall outside the scope of the national pharmacovigilancecentres, and have become the designated field of separate specialised organisations.McBride’s appeal ‘Have any of your readers seen similar abnormalities…?’ by whichhe concluded his letter, had much more impact than he ever could have foreseen.(16)
In 1961 the FDA started with the systematic collection of reports on all types ofadverse drug reactions, chiefly through the Hospital Reporting Program. In variouscountries the thalidomide tragedy had prompted the immediate formulation ofcriteria new drugs needed to meet to receive marketing authorisation, whichstandards, apart from quality, also emphasised the safety and efficacy of new drugs.In addition, the governmental marketing authorisation organisations werecommissioned to establish a post-marketing surveillance system to facilitate theearly detection of adverse reactions in order to prevent a similar tragedy fromoccurring in the future. In 1968 ten countries that supported a spontaneousreporting system for adverse drug reactions took the decision to collaborate andjoined the WHO Pilot Research Project for International Drug Monitoring.(27) In1971 a resolution of the Twentieth World Health Assembly laid the foundations forthe WHO international Drug Monitoring Programme.(28) In 1972 a report waspublished which formed the basis of the current international system of nationalcentres collaborating in the WHO Programme.(29,30) The WHO International Drug Monitoring Programme is supported andcoordinated by the WHO Collaborating Centre for International Drug Monitoring(the Uppsala Monitoring Centre), which maintains and implements theinternational database of adverse drug events. Its activities are of major importanceand include providing active support to the pharmacovigilance centres in lowincome countries, and the evaluation and augmentation of pharmacovigilance ingeneral. In 2000 the ‘Guidelines for setting up and running a Pharmacovigilance
38
Centre’ appeared and in 2002 the ‘The Importance of Pharmacovigilance’ ispublished under the auspices of the WHO, which lays the foundation for thefurther theoretical and practical implementation of pharmacovigilance on aninternational scale.(18,31)Both the national authorities and the pharmaceutical industry have played asignificant role in the development of pharmacovigilance, which has resulted in newlegislation and qualitative requirements the industry and their products need tofulfil. The Council for International Organizations of Medical Sciences (CIOMS)and the International Conference on Harmonization (ICH) have been instrumentalis this process.
The literature, both in the form of scientific handbooks and journal articles, bearswitness to the evolution of pharmacovigilance since the 1960s. A relatively smallgroup of scientists have been responsible for providing pharmacovigilance with afirm scientific basis. In his thesis Meyboom mentions the names of Leopold Meyler,Owen Wade, David Finney and William Inman.(32)What strikes one, when studying the literature on the safety of drugs, is that manyof the topics that have recently been presented as novel have been reported onearlier. Apparently, and possibly nowadays more due to the Internet, the scientificmemory is short. As an illustration: the most frequently cited article in the contextof safety of drug is the meta-analysis by Lazarou et al., in which the authorsconclude that 6.7% of all hospitalized patients experience adverse reactions todrugs.(33) However, already in 1955 Barr published an article in the JAMA thatalso reports that 5% of admitted patients are afflicted by ‘major toxic reactions andaccidents’.(34) Similar percentages are given by Seidl et al. in 1966 in relation tohospital admissions and in 1969 by Hurwitz and Wade for drug-relatedcomplaints.(35,36) Time will tell which contributions have genuinely improved thesafety of drugs and its systematic surveillance.
A comprehensive history of pharmacovigilance is still to be written. The introductorychapters of the works by Davies and Wade provide some information.(37,25)Routledge had a concise overview published in The Lancet and Lindquist has recentlywritten an historical overview of the WHO Programme.(21,27) Several of thesepublications offer information about the progress made in the variouscountries.(38,39,40) The development of the pharmacovigilance system in theNetherlands and the role of the Netherlands Pharmacovigilance Centre Lareb hasbeen described by De Koning, Meyboom and Van Grootheest.(32,41,42).Pharmacovigilance is continuously evolving. Waller and Evans have produced ‘Amodel for the future conduct of Pharmacovigilance’. The key concepts for the nearfuture seem to be ‘proactive safety surveillance’ and ‘risk management’.(43-46)
39
References
1. Lely AH. Digitalisintoxicatie, waarnemingen betreffende een massale digitoxine-intoxicatie teVeenendaal. Thesis. State University of Groningen. Stafleu. Leiden 1971.
2. Withering W. An account of the foxglove and some of its medical uses. CGJ and J Robinson.London 1785.
3. Rawlins MD. Pharmacovigilance: paradise lost, regained or postponed. The William WitheringLecture 1994. J Royal Coll Phys London 1995;29:41-9.
4. Doeveren W van. Sermo academicus de remedio morbo, sive de malis, quae hominibus aremedies, sanandi causa adhibitis, saepenumero accidere solent. Academic speech of February8, 1779. Manuscript in University Library Amsterdam.
5. Meyler L. Woord vooraf. In: Meyler L, Schadelijke nevenwerkingen van geneesmiddelen,Supplement II. Van Gorcum. Assen 1958.
6. Meyler L. Introduction drug-induced diseases. In: Drug-induced diseases. L. Meyler, MHPeck, editors. Van Gorcum. Assen 1962.
7. Zwaag P van der. Wouter van Doeveren, leven en werken van een 18-eeuws hoogleraar in degeneeskunde. Van Gorcum’s Historische Bibliotheek nr. 86. Van Gorcum. Assen 1970.
8. Geiling EMK. Cannon PR. pathogenic effects of elixir of sulfanilamide (diethylene glycol)poisoning. JAMA 1938;111:919.
10. Meyler L. Schadelijke nevenwerkingen van geneesmiddelen. Elsevier Publishing Company.Amsterdam 1951.
11. Meyler L. Side Effects of Drugs. Excerpta Medica Foundation. Amsterdam 1952.
12. Albahary C. Maladies médicamenteuses d’ordre thérapeutique et accidental. Masson & Cie.Paris 1953.
13. Duchesnay G. Le risque thérapeutique, prévention et traitement des accidents. G. Doin & Cie.Paris 1954.
14. Alexander HL. Reactions with drug therapy. Saunders Company. Philadelphia 1955.
15. R. Heintz (editor). Erkrankungen durch Arzneimittel, Diagnostiek, Kliniek, Pathogenese,Therapie. Georg Thieme Verlag. Stuttgart 1966.
16. McBride WG. Thalidomide and congenital abnormalities. Lancet 1961;11:1358.
40
17. Sjöstrom Hm, Nilsson R. Thalidomide and the Power of the Drug Companies. PenguinBooks. Harmondsworth, Middx.1972.
18. WHO. The Importance of Pharmacovigilance, Safety Monitoring of medical products. WHOGeneva 2002.
19. Lindeboom GA. Theodore Tronchin (1709-1781). Bijdragen tot de geschiedenis dergeneeskunde XXXVI 1956:49.
20. Placard, Groningen 1808. (collection author).
21. Routledge P. 150 years of pharmacovigilance. Lancet 1998;351:1200-1.
22. Commission on Anaesthetics. Lancet 1893;i:629-38.
23. Rich ML. Fatal case of aplastic anaemia following chloramphencol therapy. Ann Intern Med1950;33:1459.
24. Wallerstein RO, Condit PK, Kasper CK, Brown JW, Morrison FR. Statewide study ofchloramphenicol therapy and fatal aplastic anemia. JAMA 1969;208:2045.
25. Wade OL. The dawn of concern. In: Adverse reactions to drugs: 1-10. Acford Ltd. Chichester1970.
26. Randell T. Thalidomide’s back in the news, but in more favorable circumstances. JAMA1990;263:467-8.
27. Lindquist A.M. Seeing and Observing in International Pharmacovigilance. Academic thesis.Katholieke Universiteit Nijmegen. Nijmegen 2003.
28. WHO. Handbook of resolutions and decisions of the World Health Assembly and ExecutiveBoard, 11th ed., 1971. Geneva, World Health Organization, 1972. WHA 20.51.
29. WHO. International Drug Monitoring: The Role of National Centres. Technical ReportSeries. Geneva 1972.
30. Olsson S. The Role of the WHO Programme on International Drug Monitoring inCoordinating Worldwide Drug Safety Efforts. Drug Saf 1998;19:1-10.
31. UMC. Guidelines for setting up and running a Pharmacovigilance Centre. UMC. Uppsala 2000.
32. Meyboom RHB. Detecting adverse drug reactions, Pharmacovigilance in The Netherlands.Thesis. Katholieke Universiteit Nijmegen 1998.
33. Lazarou J. Pomeranz BH, Cory PN. Incidence of adverse drug reactions in hospitalizedpatients. JAMA 1998;279:1200-5.
34. Barr DP. Hazard of modern diagnosis and therapies – the price we pay. Frank BillingsMemorial Lecture. JAMA 1955;159:1452.
41
35. Seidl LG, Thornton GF, Smith JW, Cluff LE. Studies on the epidemiology of adverse drugreactions. III. Reactions in patients on a general medical service. Bull Johns Hopk Hosp1966;119:299.
36. Hurwitz NA, Wade OL. The incidence of adverse drug reactions in relation to the use of drugsin hospitals. BMJ 1970;1:531.
37. Davis DM, editor. Textbook of Adverse Drug Ractions. 4e ed. Oxford University Press.Oxford 1991.
38. Mann R, Andrews E, editors. Pharmacovigilance. Wiley. Chichester 2002.
39. Strom BL, editor. Pharmacoepidemiology, 3e editon. Wiley. Chichester 2000.
40. Inman B. 30 Years in Postmarketing Surveillance. A Personal Perpective. PharmacoepidemiolDrug Saf 1993;2:239-58.
41. Koning GPH de. A regionalized spontaneous surveillance programme for adverse drugreactions as a tool to improve pharmacotherapy. Thesis. Utrecht University 1994.
42. Grootheest AC van, Puijenbroek EP van. Pharmacovigilance in the Netherlands. In:Pharmacovigilance: 309-15. Mann R, Andrews E, editors. Wiley. Chichester 2002.
43. Waller PC, Evans SJW. A model for the future conduct of pharmacovigilance.Pharmacoepidemiol Drug Saf 2003;12:17-29.
44. Bortnichak EA, Wise RP, Salive ME, Tilson HH. Proactive safety surveillance.Pharmacoepidemiol Drug Saf 2001;10:191-6.
45. Perfetto EM, Ellison R, Ackermann S, Sherr M, Zaugg AM. Evidence-Based RiskManagement: How Can we Succeed?: Deliberations from a Risk Management AdviseryCouncil. Drug Inf J 2003;37:127-34.
46. Head of Agencies. Establishing a European Risk Management Strategy. Report of the Headsof Agencies ad hoc Working Group. 2003. (http://heads.medagencies.org/heads/docs).
42
Chapter 2.2 Leopold Meyler (1903-1973): A pioneer in the study of adverse effects of drugs
Ned Tijdschr Geneeskd (accepted)Int J Risk Saf Med (accepted)
Kees van GrootheestGraham Dukes
43
2.2.1 IntroductionIn 1951, more than a decade before the first rumblings of the thalidomidecatastrophe, a remarkable book appeared in the Netherlands under the authorshipof Leopold Meyler, that a year later appeared in English translation as ‘Side effectof drugs’. At that moment the book was unique in the world - and that is still thecase. The concept underlying it was that physician and pharmacist alike should beprovided with an overview of all that was known regarding the possible adverseeffects of medicines. The need to make existing information widely availableremains, even today, a major challenge in the world of pharmacovigilance.(1) Following Meyler’s book others appeared in various languages, several adoptingdifferent approaches to the topic. One after another most of them have vanished;Davis’ Textbook of Adverse Reactions is a creditable exception, providing anapproach to the topic which complements that of the Meyler series. In themeanwhile, Meyler’s volume, greatly expanded and updated, is still with us and haslong been acknowledged as the standard work on the unwanted effects of medicines.The name of the original author has become incorporated into the title: and‘Meyler’s Side Effects of Drugs’ is commonly known to the user simply as ‘Meyler’.
2.2.2 The thalidomide disasterA little over forty years ago, medical interest in drugs - and particularly new drugs- was limited almost entirely to their proven or possible therapeutic benefits. Inretrospect it is fair to say that it was the paper published by McBride in the Lancetof December 16th 1961 which triggered a broadening of that view.(2) His paper,alongside simultaneous observations from Germany, provided the principal cluesleading to the realization that there was a link between the use of the hypnoticthalidomide and the fact that a great many children were coming into the worldwith congenital defects.(3) It had of course been realized for a long time that medicines could exert adverseeffects. As early as 1779, Prof. Wouter van Doeveren of the University of Leiden,The Netherlands, delivered a public oration entitled ‘Remedio morbi’, with assubtitle: ‘Drug diseases, or diseases persons often obtain as a result of medicinesthey received as a treatment’. His conclusion, recorded more than two centuries agowas: ‘Do not give a drug too readily, with the risk that you may add a seconddisease to the first, or accelerate the patient’s’ decease’.(4)
2.2.3 AwarenessNevertheless, and as late as the mid twentieth century, physicians continued to beprimarily concerned with the positive rather than the negative aspects of medicinaltreatment, a unilateral interest promoted ever more with the arrival of new drugswhich opened therapeutic perspectives hitherto out of reach, such as the effective
45
treatment of tuberculosis. Interest in the side effects which might accompany theuse of these new agents remained sporadic.(5) Only with the thalidomide disaster were the medical profession and the publicthroughout the world alerted acutely to the need both to examine the safety of newmedicines critically prior to their admission to the market, and to studysystematically their emergent adverse effects once they had come into use. The UK‘yellow card’ system for the reporting of suspects adverse effects came into being in1964, and in 1968 W.H.O., set up a pilot project for international collaboration inthe monitoring van adverse drug reactions. The latter was to become what is nowthe W.H.O. Drug Monitoring Programme, which in October 2002 held its 25thAnnual Meeting in Amsterdam.
2.2.4 Leopold MeylerWho was Leopold Meyler, and what inspired him to create this book at thebeginning of the fifties? Meyler was born just a century ago in Rotterdam, wherehis father was an oil merchant of Jewish extraction. The young Meyler studiedmedicine at the University of Leiden and went on to specialize in internal medicine.After his qualification he joined the Medical Clinic of the University of Groningenand set up in practice. The ensuing war and the Nazi occupation of TheNetherlands were a difficult period for the family. Meyler himself had to go intohiding but his wife, whose mother was not Jewish, was periodically able to visithim. At the time of the liberation, however, Meyler was found to be suffering frompulmonary tuberculosis which he had acquired already the occupation but whichmay well have been aggravated by the conditions under which he had been obligedto live. He was admitted to a sanatorium and prescribed a prolonged period of rest.However, enforced rest and inactivity were not in the nature of an active andcommitted physician such as Meyler. Then it was that the specialist treating himsuggested a productive task which he could undertake from his bed: let himundertake a literature study of the side effects of drugs.
2.2.5 His illnessThere was a particular reason for the choice of topic, for Meyler himself had alreadyencountered the problem of adverse effects. To quote the first Dutch edition of hisbook in 1951: ‘The notion of bringing together the disagreeable effects which can beassociated with the use of medicines was inspired by personal experience, in part of avery serious nature’. In his book he describes in detail the experiences of patients suchas himself treated with para-aminosaliocylic acid (PAS), including the occurrence offever in individuals with an allergic constitution. It is known that Meyler himself wasallergic and suffered from asthma (6). In a later Supplement to his book he describedthe serious psychic effects which can be exerted by isonicotinic acid hydrazide (INH).
46
2.2.6 The writing of his bookIn order to examine the literature from his hospital bed, Meyler enlisted the help ofthe library of the University of Groningen. Every week a suitcase full of journalsand books was delivered to him, which he was obliged to return within a few days.The arrangement was continued after his return home. And so it was that the firstversion of his book appeared in 1951 in Dutch, followed by the English version ayear later. Not surprisingly the unusual approach manifested in the book elicited criticism insome quarters, and his motives were questioned. There were those who imaginedthat he was in principle opposed to the use of medicines, and some alternativehealers even viewed him as an ally in questioning the orthodox practice of medicine.Others criticised the manner in which he had classified drugs. Meyler howevercontinued assiduously to gather his evidence and relevant case reports. Supplementswere published to bring the original volume up to date, and his introductoryeditorials provided an answer to his critics, stressing that he sought only to promotethe appropriate and safe use of drugs. Behind the scenes, his books were founded inan encyclopaedic venture into the acquisition of hitherto scattered knowledge,carried through in a period where there were no computers or photocopyingmachines. Instead, he relied on his hand-written notes and a voluminous cardsystem.
2.2.7 Meyler as a personMeyler was a remarkable individual, characterized by firm opinions, a criticalapproach to information and an independence of spirit. He was also a man with abroad interest and an open mind. Above all he remained a highly competentpractising physician with a deep devotion to the interests of his patients. Hisindependence was such that he would not attend meetings sponsored by the drugindustry; if invited as a speaker he would insist on paying his own expenses.His work was formally recognized with his appointment in 1969 as the firstprofessor of Clinical Pharmacology at the University of Groningen. His inauguraloration was entitled ‘Why clinical pharmacology?’ and in it he provides anoverview of the tasks which the clinical pharmacologist is called upon to fulfil.(7)Not surprisingly his paper devotes attention to adverse reactions: ‘The study of sideeffects is of the greatest importance. Increasingly the need is felt to understand moreexactly how side effects come about, and to devise wherever possible means bywhich these unwanted complications can be avoided.’ The definition of a field ofmedical science which was new to The Netherlands was a task to which Meyler waswell suited. He published in many journals and became a sought-after speaker atmeetings both at home and abroad. The Boerhaave courses at the University ofLeyden, for which he was in part responsible, led to the publication of a series of
47
complementary volumes under the title Drug Induced Diseases, each dealing witha particular aspect of drug toxicology. Re-reading his publications today one isstruck by his extraordinary knowledge and erudition but also by the fact that somany of his views remain entirely valid in our time.
2.2.8 The importance of MeylerMeyler died suddenly during a vacation in France in 1973, possibly as aconsequence of an overdose of adrenaline which he had taken because of hispulmonary disorder. As Lammers wrote in an In Memoriam in the NederlandsTijdschrift voor Geneeskunde: ‘One can truly say that he was among the very firstto have realized how frequently drugs can be the cause of otherwise unexplaineddisorders. In our time, that realization has become so commonplace and so self-evident that one can hardly imagine how, in the recent past, the subject was barelythe subject of enquiry’.(8)Leopold Meylers opus magnum, Side Effects of Drugs, evolved from the firstedition onwards, as a multi-author volume with a distinguished team ofcontributors. Up to the seventh edition in 1972, Meyler himself was Editor-in-Chief, latterly supported by Prof. Andrew Herxheimer in London. From 1973 to2000 the volume was edited by Graham Dukes and the series is now to becontinued by Jeff Aronson in Oxford. Many tens of authors from all parts of theworld have made their contributions to ‘Meyler’, which continues to providepractising physicians and pharmacists with a critical review of new data from thescientific literature relating to adverse drug reactions. Yet there are today few whorealize that the name ‘Meyler’ on the cover is that of a doctor lying in a sanatorium,looking for something useful to occupy his mind. Meyler laid the foundations for asystematic approach to the problems of side effects. In his own time his was at firsta voice crying in the wilderness. Had that voice been heeded earlier, the extent ofthe thalidomide disaster might well have been much more limited. Even today, witha worldwide system in place for the detection and study of adverse drug reactions,an Editorial in The Lancet has rightly raised the question as to how that process canbe further refined and extended.(9) As Meyler himself wrote in the forward to hisfirst volume: ‘Let us be entirely clear that it is not our purpose to discourage the useof any of the drugs in our therapeutic arsenal. The reverse is the case. One will bein a position to use a medicine better if one is aware not only of its benefits, but alsoof its risks.’
48
References
1. Grootheest K van, Edwards R. Labelling and ‘Dear Doctor’ Letters: are they noncommittal?Drug Saf 2002;25:1051-5.
2. McBride WG. Thalidomide and congenital abnormalities. Lancet 1961;11:1358.
3. Sjöstrom HM, Nilsson R. Thalidomide and the Power of the Drug Companies. PenguinBooks, Harmondsworth, Middx. 1972.
4. Zwaag P van der. Wouter van Doeveren, leven en werken van een 18e-eeuws hoogleraar in degeneeskunde. Van Gorcum. Assen 1970.
5. Routledge P. 150 years of pharmacovigilance. Lancet 1998;351:1200-1.
6. Meyler L. Schadelijke nevenwerkingen van geneesmiddelen.: Elsevier. Amsterdam 1951.
7. Meyler L. Waarom klinische farmacologie?. Ned Tijdschr Geneeskd 1969;113:1275-9.
8. Lammers W. In Memoriam Prof. Dr. L. Meyler. Ned Tijdschr Geneeskd 1973;117:1522-3.
Kees van GrootheestEugène P. van PuijenbroekNetherlands Pharmacovigilance Centre Lareb’s-Hertogenbosch, the Netherlands.
51
2.3.1 History and organization
HistoryIn the Netherlands, consideration for the surveillance of adverse drug reactionsdeveloped at a relatively early stage. In the early 1950s, at a time when internationalliterature had included only incidental reports of 'side effects', Dr Leo Meyler laidthe basis for more systematic attention to adverse drug reactions. In 1951, hepublished his book (in Dutch) Schadelijke nevenwerkingen van geneesmiddelen(literally, 'Harmful effects of prescription drugs'). The second edition, fully revisedwith a number of supplements, appeared in 1954.In his preface to the first edition, Meyler wrote the following (here in translation):
‘The prescribing of drugs will always entail a greater or lesser degree of risk, and ineach case the physician must ask himself whether the nature of the condition aboutwhich he is being consulted justifies taking such a risk’. Meyler's work wasprompted by his own experiences with tuberculostatic preparations. He warnedalso against the inappropriate use of drugs.Meyler based much of his work on reports in various medical journals, at a timewithout the convenience of the Internet or other conveniences of modern times.The first English edition of Meyler’s seminal work was published as The SideEffects of Drugs: an Encyclopaedia of Reactions and Interactions in 1952. Itsfourteenth edition, edited by Graham Dukes, appeared in 2000. Dukes has been theeditor since the eighth edition, published in 1978, of what has now become thestandard reference work in its field. Dukes' own scientific background was largelygained in the Netherlands.
Organization of pharmacovigilance in the NetherlandsFollowing the thalidomide affair of the late 1950s and early 1960s, the Netherlandsdecided to adopt a more systematic approach to the safety of prescriptionmedicines. The Dutch Medicines Evaluation Board was founded in 1963. Based onthe American model of the Food and Drug Administration, this would assess newpharmaceutical preparations for both effectiveness and safety prior to marketingauthorization. Also in 1963, the Royal Dutch Medical Association (KNMG) joinedthe government in setting up a reporting system for adverse drug reactions. In 1965,the task of processing reports was taken over by the National Drug MonitoringCentre, which was part of the Public Health Supervisory Service and came toacquire an extremely good reputation. With a relatively small staff, the Centreproduced a significant number of publications calling attention to the potentialadverse effects of prescription drugs.(1) Each year, the National Drug MonitoringCentre received approximately thousand reports from interested doctors.
53
In 1986, a number of pharmacists called for greater attention to be devoted to thepotential adverse effects of prescription medicines. These pharmacists wereconvinced that greater awareness of the possibility of adverse effects wouldimprove the quality of pharmacotherapy as a whole. Their initiative led to thecreation of the Lareb Foundation (now: Netherlands Pharmacovigilance CentreLareb), in 1991. Lareb collected reports of adverse effects, mostly made by generalpractitioners and pharmacists. This information was supplementary to the workdone by the National Drug Monitoring Centre and at times created overlap.(2) Anew aspect was that pharmacists felt also their responsibility in the identification ofadverse effects and would consider it their task to call attention to such effects.(3)
In 1995, European legislation having been made more stringent, the Dutchgovernment decided to restructure the system of pharmacovigilance in theNetherlands. Lareb was designated the national centre for all reports of suspectedadverse drug reactions concerning registered drugs. Currently the Health Inspectorate is responsible for monitoring the quality ofpharmacovigilance activities and receives reports relating to preparations that havenot (yet) been given marketing authorization, especially reports of adversereactions that are observed during the statutory clinical trials.
The Medicines Evaluation Board Agency plays a central coordinating role. It receivesreports from Lareb, as well as those made directly by the pharmaceutical industry,and it advises the Medicines Evaluation Board. The Medicines Evaluation Boardmakes the final decision regarding marketing authorization for the Netherlands.Where deemed necessary, it is empowered to require amendments to a drug's'Summary of Product Characteristics', and in serious cases may revoke a drug'smarketing authorization altogether. The Medicines Evaluation Board includes apharmacovigilance department primarily concerned with adverse drug reactions andwith maintaining international contacts in this field. Many decisions are taken atEuropean level by the European Medicines Evaluation Agency (EMEA).
2.3.2 Spontaneous reporting in the Netherlands: the NetherlandsPharmacovigilance Centre Lareb
Direct responsibility of doctors and pharmacistsThe Netherlands Pharmacovigilance Centre Lareb is an organization which wasfounded by doctors and pharmacists and which is still run by doctors andpharmacists today. All large medical and pharmacists associations are representedon its administrative board. Lareb maintains the national 'spontaneous' reportingsystem for the Netherlands. That this task falls to an independent centre rather than
54
the government sets the Netherlands apart from most other countries. Althoughsome (such as Germany, Switzerland, New Zealand and Great Britain with its DrugSafety Research Unit) have organizations investigating adverse drug reactions thatare allied to universities or professional organizations, the role of professionalpractitioners is particularly prominent in the Netherlands. The governmentrestricts itself to a supervisory and coordinating role, while also providing fundingfor the Lareb's activities.The Dutch model has a significant number of advantages and works very well inpractice. It is doctors and pharmacists who see the occurrence of adverse drugreactions in day-to-day practice. If given co-responsibility for the propermonitoring of drug safety, they will be more inclined to contribute. This enhancesthe premise that doctors and pharmacists are themselves responsible for the safe andresponsible use of prescription drugs. The barriers to reporting suspected adverse reactions would be significantlylowered if those reports were made to a peer group organization. After all, theoccurrence of an adverse reaction may cause the doctor or pharmacist to ask himself(or herself) whether he should assume partial responsibility for this reaction. It ispossible that some would be less eager to report an adverse drug reaction to a'higher authority' such as the government.
Regional organisationFor an organization such as Lareb, in which several professions meet, it is relativelyeasy to maintain an extensive network of doctors and pharmacists. This is indeedfacilitated by Lareb's regional organization under which the Netherlands is dividedinto five regions. Lareb's headquarters in ’s-Hertogenbosch acts as one regionaloffice, with the other four in university hospitals throughout the country. Eachregional office has a regional coordinator, responsible for maintaining contact withthe doctors and pharmacists in that region. Such contact is both individual (throughpersonal visits) and collective, involving presentations in hospitals and to groups ofinvited general practitioners and pharmacists. Wherever possible, education and'refresher' courses are offered. The regional coordinator also personally assesses some of the incoming reports inorder to remain involved in the Lareb's 'core business' and will contribute torelevant publications wherever possible. A meeting of all the Lareb's scientific staffis held monthly at the head office, providing an opportunity for consultation andfurther 'in-service' training. Lareb is a small organization, with a staff of only 18. Some work part-time. Thereare four supportive (administrative) staff members, the remainder are all doctors,pharmacists or medical biologists by profession. Details are to be found on thecentre's website at www.lareb.nl.
55
Marked involvement of pharmacistsIn the context of pharmaceutical patient care, pharmacists in the Netherlands arevery much involved in ensuring safe and responsible use of medicines. Pharmacistsplayed an important part in setting up Lareb. Today, pharmacists provide about40% of the reports the centre receives (see Table 1).
Most reports are made by community pharmacists, which is perhaps to be expectedgiven Lareb's background. Hospital pharmacists lag somewhat behind in thisrespect. Accordingly, Lareb has joined forces with the Netherlands Society ofHospital Pharmacists in attempting to encourage greater involvement on the part ofits members. One objective is to establish a protocol in hospitals whereby housepharmacists are not only expected to provide effective pharmacotherapy, but willalso play a coordinating and facilitating role in terms of the collation andforwarding of adverse drug reaction reports. A survey held in early 2001 indicatedthat 97% of hospital pharmacists are eager to report any adverse reactions; theyknow what must be reported and in what way. The complaint that pharmacists arethemselves able to provide little or no clinical information in a report has beenshown to present no great problem in practice. Often, the good cooperationbetween doctors and pharmacists will ensure that adequate information can begiven, particularly if the relevant report is being made from a hospital situation. Ifnecessary, it is possible to contact the prescribing doctor to obtain furtherinformation. That pharmacists are able to provide a complete picture of a patient'sprescription history is a significant advantage.
The generation of signals The primary objective of any reporting system is to generate a 'signal': an earlyindicator or warning of a potential problem. It may be compared to the task of afire-watcher, who looks for smoke and, if he thinks he spots it, must then determine
whether there is indeed a fire and where that fire is located. In pharmacovigilance,it falls to the Medicines Evaluation Board to determine whether there are sufficientarguments to shout 'fire!', whereupon it will take the necessary measures. The reports received by Lareb are first assessed by one of its staff doctors orpharmacists. They examine the probability of a causal link, and will use the currentliterature, previous reports and the description of the drugs' pharmacologicalmechanism to assist them. The results of their assessment are notified to thereporter as well as to the government. A weekly assessment meeting involves all scientific staff. The reports and theirsubsequent assessments are discussed to determine whether further action isnecessary. Such further action may entail more detailed analysis of the relationshipbetween the reported reaction and the suspect drug. Research within Lareb hasrevealed a number of factors that can play a significant role in the decision toconduct further analysis. These include the seriousness of the reported reaction, thenumber of reports related to similar reports on other drugs received by the centre,and whether existing literature has devoted attention to the suspected reaction. During the weekly assessment meeting, all new reports are discussed and furtheraction is scheduled if there seems to be sufficient justification. As a general rule,such action will entail notifying the Medicines Evaluation Board, and in many casesan article will be published. Computer automation now plays an important role in the internal reportassessment process, with all incoming reports undergoing a set sequence ofevents. The information on the report forms themselves, together with that inany other relevant documentation, is stored in digital form. The weeklyassessment meeting also makes use of information obtained through automatedquantitative signal generation. The 'Reporting Odds Ratio' is calculated for allreports, providing a statistical indication of the reporting frequency of each ofthe suspected reactions compared to other reports in Lareb's database. Theresults of the Bayesian Confidence Propagation Neural Network analysis,submitted quarterly by the WHO Monitoring Centre in Uppsala are alsoautomatically linked to each report. Lareb's database contains over 40,000 reports. Besides providing a valuable aidto case-by-case analysis, quantitative information can also be used to distil usefulinformation from a large collection of data. Such information will not beprovided by a single case analysis. Lareb is particularly interested in thepossibilities for identifying specific syndromes and in detecting interactionsbetween drugs.(4,5) Ongoing research is being conducted into whether certainrisk factors for drug reactions can be identified using the information now filedin the database.
57
CommunicationLareb is a small organization in a big world. Its most important contacts are theprofessional organizations, the government and the pharmaceutical industry.
- Doctors and pharmacistsBecause the Lareb is itself an organization of doctors and pharmacists, it has readyaccess to practitioners in the field. Current European legislation does not permitdirect reporting by patients themselves, although Lareb would not be opposed toits future introduction. Partly in view of the fact that doctors and pharmacistsreport suspected adverse drug reactions on a purely voluntary basis, it is importantto inform them of the importance of reporting. In addition to the feedback itprovides, both direct and in the form of publications, the centre offers targetedinformation to potential reporters in the form of mailings and presentations. Thereport form itself has a carefully designed layout and is distributed in various ways,such as inclusion with the regular Drug Bulletin and the annualParmacotherapeutisch Kompas, the pharmacopoeia which forms a standard deskreference book for 90% of Dutch doctors. It is important that the reporter can relyon respect to privacy and confidentiality. Lareb doesn’t receive any informationabout the identity of the patient and no information about the reporter will be givento third parties. The Dutch law is also strict on privacy.An important mean of communication with the reporting parties is the 'feedbackreport'. Not only is receipt of each report acknowledged, but the assessment madeby the Lareb and the conclusions drawn with regard to the reported adverse drugreaction are notified to the person making the report. Besides wishing to encourage reporting, Lareb believes that it is important to raisethe level of awareness among doctors and pharmacists with regard to adverse drugreactions. This will not only lead to a better standard of reporting but will serve toreduce significantly the harmful effects of prescription medicines as well. Doctorswill prescribe more critically and will be more inclined to consider adverse drugreactions as the cause of complaints at an earlier stage in their differential diagnosis,whereupon they will become able to discontinue use of the drug or to adapt thedosage to avoid both unnecessary costs and unnecessary impact in terms of patienthealth.
- The governmentBecause Lareb is an independent organization working on behalf of thegovernment, good communication with that government is very important.Reports are forwarded to the Medicines Evaluation Board Agency weekly. Every 6weeks, a meeting is held between Lareb, the Agency and the Health Inspectorate.Besides possible 'signals', these meetings also discuss international developments.
58
- Marketing Authorization Holders Needless to say, Lareb maintains close contact with the pharmaceutical industry,which also has a vested interest in effective pharmacovigilance. All serious ('15-days') reports are forwarded to the relevant Marketing Authorization Holder, asrequired by international legislation. These reports are anonymous, neither thepatient nor the reporter can be traced. Similarly, all such reports made directly bythe pharmaceutical industry to the government are entered into Lareb's database.In the short term, the centre aims to achieve a free exchange of less serious reportsas well. All articles concerning a specific preparation are submitted for comment tothe relevant Marketing Authorization Holder prior to publication.
ResultsThe 'output' of Lareb can be assessed by looking at both the quantity and qualityof incoming reports, aspects that owe much to the efforts of the centre. Othercriteria include the number of publications for which the centre has beenresponsible and the number of notifications of possible signals it has made.
- Reports: quantityThe number of incoming reports continues to increase each year. The developmentin the number of reports included in the database is shown in Table 2.Lareb sees under-reporting as an inherent characteristic of a spontaneous reportingsystem and not necessarily as a drawback.
- Reports: quality Although an adequate number of reports are necessary to ensure a reliablereporting system, Lareb attaches greater importance to the quality of those reports. The quality of reports can also be seen to have risen each year. Quality iscontinuously assessed according to a number of criteria, one of which is the extentto which the report is documented. In an increasing number of cases, reports areaccompanied by adequate clinical information, including the specialists' clinicalnotes to the patient’s family practitioner. The fact that more complete informationis now available may be attributed in part to the greater number of reports beingmade by hospital practitioners. The increase in the number of reports adjudged tobe of a serious nature is shown in Table 3.Although preparations which have been on the market for some time mayoccasionally reveal new adverse reactions (as in the case of vigabatrine, which hadbeen available for over 10 years before a link with patients' restricted field of visionwas made), Lareb is particularly interested in new medicines. Table 2 shows thepercentage of reports relating to preparations that have been on the market for lessthan 5 years.
59
- Publications and presentationsHaving adopted a scientific and academic level as the basis for its workingmethods, Lareb is regarded as a serious partner by others, particularly theprofessional organizations. The scientific quality of the Lareb's work ismonitored by a Scientific Advisory Board, comprising experts in variousdisciplines. Each year, Lareb publishes over thirty articles in international or national journals,among which the Dutch Drug Bulletin. It also makes more than 30 presentations togroups of doctors and/or pharmacists and is frequently represented at internationalscientific conferences.
2.3.3 Further initiatives in pharmacovigilance in the NetherlandsBesides the spontaneous reporting system and the activities undertaken by, orunder the auspices of, the government, there are various other pharmacovigilance
60
Table 2Total reports and percentage of serious reports according to the criteria of the WHOor CIOMS
Year Reports WHO criteria CIOMS criteria total % reports serious %reports serious
initiatives in the Netherlands. Of these, the most notable are those undertaken bythe marketing authorization holders and universities.
- Marketing authorization holdersNeedless to say, pharmaceutical companies in the Netherlands must comply withinternational legislation relating to pharmacovigilance. Reports that meet theCIOMS criteria must be made to the Medicines Evaluation Board within 15 daysand will also be included in Lareb's database. In addition, Marketing AuthorizationHolders are required to submit periodic safety update reports, to include allinformation known to them concerning the safety of the preparations for whichthey hold marketing authorization. The Netherlands does not have a tradition ofreports being made directly to the pharmaceutical industry by doctors orpharmacists; the vast majority of reports concerning suspected adverse drugreactions pass through Lareb.
- UniversitiesThree Dutch universities include a department of pharmacoepidemiology. Thesedevote considerable attention to the occurrence of adverse drug reactions at grouplevel. A number of initiatives have been developed whereby these can be studiedmore closely in the context of day-to-day medical and pharmacological practice.The resulting systems are more suitable for the assessment of signals than for theirgeneration. The Department of Pharmacoepidemiology of the University of Utrecht developedthe 'PHARMO' system (which is now operated independently). It is a record-linkage system that uses information provided by a number of pharmacists incombination with hospital clinical records. The department of Epidemiology and Bio-statistics of Rotterdam's ErasmusUniversity is responsible for the IPSI system. It is relying on digital informationrecorded by general practitioners. The Department of Social Pharmacy en Pharmacoepidemiology of the Universityof Groningen, which maintains also the InterActie database, has joined forces withLareb in developing an intensive monitoring system which will use the initialsignals notified by pharmacists as well as responses to surveys conducted amonggeneral practitioners. It is believed that such a system will result in a first impressionof possible adverse reactions in the case of newly authorized preparations.
2.3.4 Summary and future developmentsThe Netherlands can now look back on 50 years of systematic attention for adversedrug reactions. This began with the first edition of the book now popularly knownsimply as Meyler’s, and has developed to a stage in which the emphasis is on
61
effective pharmacovigilance and in which Meyler’s is now the work of severaldifferent authors. On behalf of and in co-operation with the government theNetherlands Pharmacovigilance Centre Lareb maintains the spontaneous reportingsystem for the Netherlands. A notable characteristic of the Dutch situation is thatdoctors and pharmacists are themselves responsible for this system, withpharmacists taking a significant role. Besides continued consideration for both the quantity and quality of reports, thefuture is likely to see further development of automatic signal generation and evengreater concern for good communication with potential reporters, in order toincrease awareness of adverse drug reactions. Developments at the European levelare certain to have a significant influence in this regard.
62
References
1. Koning GPH de. A regionalized spontaneous surveillance programme for adverse drugreactions as a tool to improve pharmacotherapy. Thesis. Utrecht University, Faculty ofPharmaceutical Sciences 1994.
2. Meyboom RHB, Gribnau FWJ, Hekster YA, de Koning GHP, Egberts ACG Characteristicsof Topics in Pharmacovigilance in The Netherlands. Clin. Drug Invest 1996;4:207-219.
3. Koning GPH de, Bakker A, Leufkens HGM. Postmarketing surveillance in pharmacy: anorientation. Pharm Weekbl 1992;127:76-79.
4. Puijenbroek EP van, Egberts ACG, Meyboom RHB, Leufkens HGM. Signalling possibledrug-drug interactions in a spontaneous reporting system: Delay of withdrawal bleedingduring concomitant use of oral contraceptives and itraconazole. Br J Clin Pharmacol1999;47:689-693.
5. Puijenbroek EP van, Egberts ACG, Heerdink ER, Leufkens HGM. Detecting drug-druginteractions using a database for spontaneous adverse drug reactions: An example withdiuretics and non-steroidal anti-inflammatory drugs. Eur J Clin Pharmacol 2000;56:733-738.
63
Chapter 2.4Underreporting in the spontaneous reporting of adverse drug reactions - A pharmacovigilance approach
Submitted
Kees van Grootheest MD1
Ingrid Oosterhuis, student2
Eugène P. van Puijenbroek MD, PhD1
Lolkje T.W. de Jong – van den Berg PharmD, PhD2
1. Netherlands Pharmacovigilance Centre Lareb,’s-Hertogenbosch, the Netherlands.
2. Department of Social Pharmacy and Pharmacoepidemiology, GUIDE, Groningen, the Netherlands
65
Abstract
Spontaneous reporting of adverse drug reactions (ADRs) is the main method fordetecting hitherto unknown adverse effects to drugs. Especially from epidemiologicalcircles spontaneous reporting has been frequently criticised because of the problem ofunderreporting. Underreporting implies that far from all side effects are reported,which makes the spontaneous reporting system (SRS) unsuitable to determine theactual incidence of an ADR. Many attempts have been made to try and establish theextent of underreporting to make the SRS results suitable for epidemiological use.Since its inception, rather than an epidemiological methodology, the SRS hasgradually adopted a pharmacovigilance approach, which development is illustratedon the basis of the phenomenon of underreporting. Pharmacovigilance does notrequire all suspected ADRs to be reported but rather relies on an adequate numberof reports containing a sufficient amount of information to facilitate a causalityassessment that can subsequently help to signal unknown risks of drugs.Underreporting is characteristic of an SRS, which, from a pharmacovigilanceperspective, is a prerequisite and therefore should not a priori be labelled as negative.
66
2.4.1 IntroductionBecause at the time of its introduction the available knowledge about and experiencewith the safety of a new drug is limited, it is essential that the effects of the drug areclosely monitored during its use in clinical practice. This process is commonlyreferred to as Post Marketing Surveillance: the systematic surveillance and scientificevaluation of all intended and unintended effects of medicines on human health, aftertheir release for marketing.(1) The method that is most frequently employed is theso-called spontaneous reporting system (SRS), which system was developed in the1960s and 70s.(2) An SRS operates by requesting health professionals and,increasingly, also the users of medicinal drugs, to report their (negative) experienceswith the drugs to a national reporting centre. Well over 70 countries support such asystem and pass on their reports to the WHO Collaborating Centre for DrugMonitoring (the Uppsala Monitoring Centre).(3,4,5)Spontaneous ADR reporting is the main source of information for the detection ofsignals of drug safety hazards and should remain one of the cornerstones of acomprehensive safety monitoring programme’.(2) The great strength of spon-taneous reporting is that it operates for all drugs throughout their lifetime; it is theonly affordable method of detecting rare ADRs.(6) Nevertheless, since the earlydays of the system’s existence there has been criticism. The issue most frequentlymentioned is that the system of spontaneous reporting is associated withunderreporting: far from all adverse effects are being reported, thus rendering thesystem unsuitable to determine the incidence of a particular ADR.(7,8,9,10)In this paper we will explore underreporting more closely and discuss whether it isindeed justified to consider underreporting as a weakness of the SRS by tracing theoriginal context of the concept of underreporting and by looking at the roleunderreporting plays in today’s practice of pharmacovigilance.
2.4.2 Scientific interest for adverse drug reactionsWhen in the 1960s the world was shocked by the thousands of children that wereborn with serious congenital malformations as a result of the maternal use ofthalidomide, people became awoke of the dangers of possible adverse drugreactions resulting in a raised awareness of ADRs among both the nationalauthorities as well as the scientific community. This paved the way for the newdiscipline of pharmacoepidemiology, which can be regarded as a fusion of clinicalpharmacology and epidemiology.(11) The idea that it should also be possible toderive the incidence of adverse events from the ADR reports that were submittednecessitated the assessment of the extent of underreporting. This idea is alsoreflected in the name most commonly used for the system: spontaneous reportingsystem. In this context the term ‘spontaneous’ denotes basically the at randomgathering of reports, allowing extrapolation to all users. Right from the start of the
67
reporting systems it was clear that far from all adverse events would be reported(and possibly could not be reported) and moreover not all ADRs could beattributed to the suspected drug. In addition, the reporting of ADRs is not random.These facts warranted the conclusion that, although suitable for the detection ofhitherto unknown adverse drug reactions, an SRS was by no means appropriate forthe validation of these adverse effects (signal testing) which requires a differentmethodology, such as clinical trials and case control studies. In the past few yearsthere has been a bipartition in the field of ADR monitoring. The detection of newADRs, which is mainly based on the SRS approach, has now become the domain ofpharmacovigilance (see Figure 1). Pharmacoepidemiology, on the other hand,mainly concerns itself with the validation of ADRs and establishing their incidence,for which it employs its own methods. In other words: pharmacovigilance is chieflyconcerned with the clinical-pharmacological aspects of ADRs andpharmacoepidemiology with their epidemiological context. It needs to be notedthat pharmacoepidemiology has since broadened its scope even further, but this isbeyond the scope of this article. The changes just described are best reflected by thefounding of the International Society of Pharmacoepidemiology (ISPE, 1984) andthe International Society of Pharmacovigilance (originally established as theEuropean Society of Pharmacovigilance in 1992).Against this background it is self-evident that the terms ‘underreporting’ and‘spontaneous’ originally had an epidemiological connotation. However,pharmacovigilance has evolved into a scientific field in its own right, providing thetwo concepts with a different meaning.
68
Figure 1Relation between case reports (spontaneous reporting system) and (pharmaco)epidemiology(modified after Van Puijenbroek (48))
2.4.3 What is underreporting?A review of the literature yielded hundreds of articles on underreporting in relationto the reporting of ADRs. However, we were unable to find an unequivocaldefinition for the concept of underreporting. This lack has led to differentviewpoints and an ambiguous use of the term.The term underreporting is predominantly used to indicate that not all the adverseeffects that occur are reported, although that severe ADRs and adverse effects fornew drugs are more frequently reported than ADRs that are alreadyknown.(9,12,13) It is also used as a reference to the fact that only a minority of thepotential participants contribute to the reporting system; it is known that in generalless than 5% of physicians actually report adverse events.(14,15,16)When we look more closely at the most common interpretation of underreporting,i.e. the fact that only a certain proportion of all possible ADRs is reported, thisraises new questions because in this context underreporting is defined by what isunderstood by the term ADR. The definition that is most frequently used todescribe an ADR is given by the WHO: ‘a response to a medicine which is noxiousand unintended, and which occurs at doses normally used in man’.(17) AnotherWHO publication adds: ‘for the prophylaxis, diagnosis, or therapy of disease, orfor the modification of physiological function’.(18)However, this WHO definition fails to delineate the term ADR adequately, giventhat also adverse events that have not yet been diagnosed are included, for instancea liver dysfunction that has not been identified yet. Although such a disorder fallswithin the category of unintended effects, it cannot be reported. This exampleillustrates that ADR reporting will always be deficient and that for this reason alonethere will always be underreporting. Earlier, Edwards and Aronson already pointedto the unlimited scope of the ADR definition provided by the WHO.(19) The scaleof underreporting is large. In the literature Rawlins is often quoted, who, in hisWilliam Withering Lecture indicated that this was in excess of 90% for seriousreactions and higher for non-serious reactions.(14) Later studies have since shownthat this proportion is in fact considerably higher.(15,16,20) Underreporting is acommon feature of all spontaneous ADR reporting systems.(9)
2.4.4 Underreporting from an epidemiological perspectiveThere have been numerous attempts to try and determine the extent ofunderreporting in order to make the results of the SRS suitable for epidemiologicaluse. If the SRS data are corrected for the ratio of underreporting found, theincidence of an ADR may be determined.(21,22,23) Figure 2 indicates the differencebetween incidence (the proportion of users that have experienced an adverse event)and reporting ratio (the proportion of ADRs that have been reported). The modelof a spontaneous reporting system, however, is not suitable for an incidence
69
assessment. It is evident that the results of an SRS are considerably biased. Apartfrom the fact that not all ADRs are reported, reporting is done on a selective basis.New products are given far greater attention, but also serious ADRs and those thatare widely covered in the media raise the number of incidents that arereported.(24,25)Even though in the 1960s and 70s the contribution and limitations of the SRSreceived a great deal of attention from epidemiological circles, ‘very little that is newhas been written in the past 20 years’.(26) In this context Bortnichak et al. refer toit as the ‘childhood’ of pharmacoepidemiology. Epidemiological methods are notcompatible with a spontaneous reporting system because not all the basicrequirements for proper epidemiological research are being met.(27,28) Alvarez etal. rightly concluded that: ‘It is not possible to estimate incidence rates of adverseeffects using spontaneously reported data’.(9)It is clear that the concept of underreporting should no longer be seen in the lightof its original epidemiological background.
2.4.5 What does pharmacovigilance entail?Pharmacovigilance is the science and the activities relating to the detection,assessment, understanding and prevention of adverse effects or any other possibledrug-related problem.(18) Pharmacovigilance primarily is a clinical science thatemploys various methodologies, of which the spontaneous reporting system is the
70
Figure 2Difference between incidence and reporting ratio (modified after Van Puijenbroek (48))
most important. Other fields of science also contribute, such as various clinicaldisciplines, epidemiology, pharmacy, teratology and toxicology. The essence ofpharmacovigilance is that new information is gathered based on the practicalexperiences with individual patients and that this newly acquired knowledge willbenefit the treatment of the individual patient. The actual dataset of an SRS consistsof a series of case reports. This implies that pharmacovigilance closely resembles thedaily practices of the practitioner’s surgery: although use is made of evidence-baseddata, each new case needs to be assessed separately. This also implies that thereporting of possible ADRs is fraught with uncertainty. It are the cases that arecollected in this way that form the basis for the detection of new signals of adverseevents, just like they constitute the basis for the discovery of new symptomatologyand therapies.(29,30) It is exactly the lack of structure that is characteristic of thiscase-by-case research approach that makes its findings so innovative and makes itso highly sensitive in picking up new phenomena.(31) Serendipity often plays amajor role: a valuable new discovery is made without actually looking for it. It isno coincidence that in response to the increasing interest in evidence-basedmedicine the appreciation of the case report is undergoing a revival.(32)A surveillance system that relies on actual cases is not intended to provide aquantitative account of the risk levels involved. This belongs to the domain ofepidemiologists. But before an idea (for example a signal) can be confirmed orquantified, it first has to be discovered.(29) Although cases and case series rank low in the hierarchy of evidence, thespontaneous reporting system increasingly yields reliable signals, often meetingsufficient criteria for marketing authorities to gear their policy to. Venning et al.demonstrated in their retrospective study that of the 47 evaluated first reports in theliterature the majority (35) had been confirmed 18 years later.(33) In a study intothe 22 drugs that had been withdrawn from the Spanish market in the 1990s Arnaizet al. recently reported that in 18 cases the withdrawal had been based on casereports or case series and in the remaining four cases on randomised clinicaltrials.(34). Both studies were done from an epidemiological viewpoint but underlinethe value of cases. Thanks to the high quality of the reports and accurate causalityassessments the evidence for the signals is constantly gaining in strength and thechance of false positive signals is minimised.
2.4.6 Underreporting is desirableIn pharmacovigilance it is all about collecting those ADR reports that will facilitatethe timely detection of new signals of adverse reactions. Rather than requiring allADRs to be reported, an adequate number of reports containing the right kind ofinformation to allow an accurate causality assessment suffices.From a practical viewpoint alone it would be quite inconvenient if all likely ADRs
71
were reported. None of the national reporting systems is equipped to process suchan amount of data. It would be impossible to find the proverbial needles in thegigantic haystack, given the fact that each report needs to be weighed separately,both to allow an accurate causality assessment and to provide adequate feedback tothe reporting party. Finney already pointed out that it is vital to indicate explicitly which specificadverse events need to be reported.(35)In several countries specifically serious ADRs are invited and those associated withnewly marketed drugs.(36,37,38) Selection is a core task of the SRS and relies on thereporters’ expertise. Underreporting appears to be positively selective, since itinvolves mainly the less severe and the well-known effects, and this consequentlypreserves the most valuable asset of spontaneous reporting: signal generation.(9)Thus, from a pharmacovigilance perspective it is undesirable that all adverse eventsare reported to the SRS. It is those reports that may contribute to the signalling ofhitherto unknown risks of drugs that are indispensable. Table 1 provides an illustration of the recommendations the NetherlandsPharmacovigilance Centre Lareb implements with respect to which type of adverseevents it wishes to be reported.
2.4.7 We do need enough case reports of good qualityThe fact that not all ADRs need to be reported does not imply that reporting
72
Table 1Instructions, used by the Netherlands Pharmacovigilance Centre Lareb to informpotential contributors about what to report
What are you supposed to report to Lareb?It is important that you report any suspicions of adverse drug reactions.You can report anything you deem important, even if the correlation with therelevant drug is as yet uncertain.You should always report the following:- All adverse reactions associated with new drugs (until at least 2 years after their
introduction)- All serious adverse drug reactions- Unknown adverse reactions, i.e. any side-effect that is not included in the SPC- Adverse events in infants, including those associated with off-label use- In addition: adverse reactions to alternative (complementary) medication, OTC
products and vaccines
practices are not subject to specific requirements. Within the framework of GoodPharmacovigilance Practice several authors, most notably Meyboom, haveformulated a number of criteria an SRS needs to fulfil.(39,40,41)Each national SRS needs to receive a sufficient number of ADR reports to allow areliable surveillance of unknown harmful effects of drugs. Evidently, it is paramountthat the quality of the reports meets the highest standards, since it is only the reportsthat are well documented that can contribute to our knowledge about ADRs andwill allow both causality assessments and statistical analyses.(35,41)
We wish to highlight three of the factors that promote high-quality reports.a. The relationship between the national reporting centre and potential reporters
should be characterised by acknowledgement of professionalism andresponsibility.(42)This implies that on the one hand the SRS should operate on a scientifically soundbasis that is appreciated by both the physician and the pharmacist.On the other hand the long-established medical-ethical principle that one does notkeep knowledge that may be relevant for others to oneself should be applied hereas well. The creativity and open-mindedness of the contributors form the basis forqualitatively sound reports. Physicians that fail to report their observations ofadverse events do not comply with the standards of their profession.(7,12)
b. It is essential for the national reporting system to provide the reporting partywith proper feedback.(41,42,43) This way the sender of the report is bothinformed that his or her report has been duly taken account of and receivesinformation about the evaluation the experts at the centre have made. Only whenfeedback is provided on an individual basis will the relationship be fully bilateral.In addition, the various health professions need to be given collective feedbackby means of publications and oral presentations, allowing those involved toappreciate the contributions of the SRS and affording them the opportunity toput the newly acquired knowledge to practice.
c. The literature provides ample information as to which practical requirementsneed to be met, such as proper information to potential reporters, theavailability of a reporting form that is easy to complete, clear instructions aboutwhat needs to be reported, and, for hospitals in particular, facilities that promoteADR reporting. Here, it is recommended to integrate a reporting module intothe computerised systems of general practitioners, pharmacists and hospitals.
In order to increase the number of reports one could also try and raise the numberof those that are allowed to report. The number of studies that have been conductedto gain insight into the attitude of potential reporters and the factors that positivelyor negatively affect the commitment to report is substantial.(12,13,15,42)
73
Pharmacists have long been a valuable source of reports and yet in many countriestheir role in ADR reporting is restricted.(44,45) Nursing staff and patients are alsoincreasingly considered, although the contribution of patient reports is still a pointof debate.(46,47)
2.4.8 Statistical evaluation of the data collectedAs was mentioned above, spontaneous reports are unsuitable for epidemiologicalconclusions as regards incidence assessment. This does not imply that the datasetdoes not allow statistical analyses. From the start, the importance and possibilitiesof storing and analysing the data collected has been recognised, both on a nationaland international basis.(18,35) The fundamental principle of the concept of areporting system was developed by Finney, who also described the criteria foradequate analytical processing of the data.(17)The statistical analysis supplements the case-by-case analysis of the submittedreports.(39,48) The relationships between drugs and ADRs that aredisproportionally present, and that may consequently constitute a signal, are tracedin the dataset, for which several methods are applied.(49,50,51) A recent publicationdescribes the application of such a quantitative signal detection to support the case-by-case analysis in the daily operations of a pharmacovigilance centre.(52)In addition to detecting possible signals of new adverse events these methods canalso be employed to trace drug-drug interactions and drug-related syndromes.(53,54) Repeatedly, it has been shown that underreporting interferes with suchanalyses in certain cases only.(55,56)When applying statistical analyses it is essential to keep in mind that it isspontaneous reports that constitute the basic data. This implies that for eachrelevant report the clinical background needs to be checked.(27,39) As early as in1965 Finney, the architect of statistical analysis of SRS data, wrote: ‘The quality ofresults coming out of a computer cannot be higher than the quality of the recordsput in’.(35) Even when statistical analyses are employed, pharmacovigilance willremain primarily a clinical science.Against this background one needs to be cautious with what is sometimes calledautomated signal selection, where the analysis of the incoming reports is solely leftto software programmes.
2.4.9 Final remarksIt can be concluded that from a pharmacovigilance standpoint it is undesirable thatall adverse reactions are reported to a spontaneous reporting system but only thoseADRs that may contribute to the signal detection of hitherto unknown risksassociated with certain drugs. The adjective spontaneous in this context may be confusing. It should be
74
interpreted as the exploitation of the creativity of health professionals or patients.This can, however, only be done with any success if, as Pasteur taught us, thoseinvolved have a ‘prepared mind’. Providing potential reporters with the properinformation about what constitutes good ADR reporting is paramount. Edwardshas advocated replacing ‘spontaneous reporting’ with ‘concern reporting’.(57)The results of an SRS are unsuitable for epidemiological analyses for severalreasons, despite the valuable contribution epidemiology has made to thedevelopment of the system. This fact has been illustrated by the phenomenon ofunderreporting. If this phenomenon is interpreted from an epidemiologicalperspective, rather than a pharmacovigilance approach, making underreporting aweakness or point of critique, this may easily lead to the wrong conclusions. Bycomparing two WHO publications, one dating from 1972 and the other from theyear 2000, we can neatly illustrate the history of the two different interpretations ofthe concept of underreporting.(17,18) Whereas in 1972 it is stated thatunderreporting makes statistical evaluation more difficult and the reports receivedmay not be representative, in the 2000 publication we read under the headingUnderreporting: ‘…in signal detection not only the quantity but also the relevanceof case reports and the quality of data are important’.Research into underreporting is worthwhile only when it is aimed at thequantitative increase and qualitative enhancement of reports. Specifically, studiesinvestigating what type of reports contribute most to the existing knowledge andwhich methods increase the volume of submission of these types of reports arethought to be most useful. Thus, it may be questioned whether reporting knownadverse reactions, however serious these may be, serve any useful purpose.Underreporting is a characteristic of every SRS and, since this is desirable from apharmacovigilance viewpoint, it should not be aprioristically labelled as a negativeaspect.An SRS is not designed for an exact estimation of incidence rates. Looking forconcrete numbers in the data of a spontaneous reporting system is comparable tolooking for oranges on an apple tree. Not only it is the wrong tree, it also grows inanother country.
75
References
1. Gezondheidsraad (Dutch Health Council): Post Marketing Surveillance in the Netherlands.The Hague 1991.
2. Heads of Agencies. Establishing a European Risk Management Strategy – Report of the Headsof Agencies ad hoc Working Group. Brussels 2003. (http://heads.medagencies.org/heads)
3. Olsson S. The Role of the WHO Programme on International Drug Monitoring inCoordinating Worldwide Drug Safety Effects. Drug Saf 1998;19:1-10.
4. Olsson S. National Pharmacovigilance Systems – Country Profiles and Overview (secondedition). Uppsala Monitoring Centre. Uppsala 1999.
5. Lindquist A.M. Seeing and Observing in International Pharmacovigilance. Thesis. KatholiekeUniversiteit Nijmegen. Nijmegen 2003.
6. Mann RD, Andrews EB. Introduction. In: Pharmacovigilance. Mann R, Andrew E, editors.John Wiley and Sons. Chichester 2002.
7. Finney DJ. The detection of adverse reactions to therapeutic drugs. Stat Med 1982;1:153-61.
8. Rogers AS. The Detection and Identification of Unintented Drug Effects. In:Pharmacoepidemiology. An Introduction (Hartzema AG, Porta M, Tilson HH, editors).Harvey Whitney Books Company. Cincinnati 1998.
9. Alvarez-Requejo A, Carvalja A, Bégaud B, Moride Y, Verga T, Martín Arias LH. Under-reporting of adverse drug reactions – estimate based on a spontaneous reporting schema and asentinel system. Eur J Clin Pharmacol 1998;54:483-8.
10. Moore N, Hall G, Sturkenboom, Mann R, Lagnaoui R, Bégaud B. Biases affecting theproportional reporting ratio (PPR) in spontaneous report pharmacovigilance databases: theexample of sertindole. Pharmacoepidemiol Drug Saf 2003;12:271-81.
11. Strom B L. What is pharmacoepidemiology? In: Pharmacoepidemiology. Strom B L, editor.John Wiley and Sons. Chichester 2000.
12. Eland IA, Belton KJ, Grootheest AC van, Meiners AP, Rawlins MD, Stricker BHCh.Attitudinal survey of voluntary reporting of adverse drug reactions. Br J Clin Pharmacol1999;48:623-7.
13. Moride Y. Haramaburu F, Requejo AA, Bégaud B. Under-reporting of adverse drug reactionsin general practice. Br J Clin Pharamcol 1997;43:177-81.
14. Rawlins MD. Pharmacovigilance: paradise lost, regained or postponed? The WilleamWithering Lecture 1994. J R Coll Physicians Lond 1994;29:41-9.
76
15. Martin RM, Kapoor KV, Wilton LV, Mann RD. Underreporting of suspected adverse drugreactions to newly marketed (‘black triangle’) drugs in general practice: observational study.BMJ 1998;317:119-20.
16. Hasford J, Goettler M, Munter K-H, Müller-Oerlinghausen b. Physicians’ knowledge andattituded regarding the spontaneous reporting system for adverse drug reactions. J ClinEpidemiol 2002;55:945-50.
17. WHO. International Drug Monitoring: The Role of National Centres. Technical Report SeriesNo 498. WHO. Geneva 1972.
18. WHO. The Importance of Pharmacovigilance, Safety Monitoring of medical products. WHO.Geneva 2002.
19. Edwards IR, Aronson JK. Adverse drug reactions: definitions, diagnosis, and management.Lancet 2000;356:1255-9.
20. Bégaud B, Martin K, Haramburu F, Moore N. Rates of Spontaneous Reporting of AdverseDrug Reactions in France. JAMA 2002;288:1588.
21. Tubert-Bitter P, Bégaud B, Moride Y, Chaslerie A, Haramburu F. Comparing the Toxicity ofTwo Drugs in the Framework of Spontaneous Reporting: A Confidence Interval Approach. JClin Epidemiol 1996;49:121-3.
22. Fourrier A, Chaslerie A, Dartigues JF, Bégaud B. Under-Reporting of Adverse Drug Reactionin the Elderly. Pharmacoepidemiol Drug Saf 1995;4:379-80.
23. Stather R. Determining and describing the frequency of ADRs in the SPC. Reactions2002;931:3-4.
24. Wallenstein EJ, Fife D. Temporal Patterns of NSAID Spontaneous Adverse Event Reports.The Weber Effect Revisited. Drug Saf 2001;24:233-7.
25. Griffin JP, Weber JCP. Voluntary systems of adverse drug reaction reporting- Part II. AdvDrug React Pois Rev 1986;1:23-55.
26. Bortnichak EA, Dai WS. Epidemiologists and Adverse Event Data – A Challenge to the Field.Pharmacoepidemiol Drug Saf 1999;8:457-61.
27. Jick H. García Rodriguez LA, Pérez-Gutthann. Principles of epidemiological research onadverse and beneficial drug effects. Lancet 1998;352:1767-70.
28. Skegg DCG. Pitfalls of pharmacoepidemiology. BMJ 2000;321:1171-2.
29. Vandenbroucke JP. Case reports in an evidence-based world. J Roy Soc Med 1999;92:159-63.
30. Goodwin JS. The empirical basis for the discovery of new therapies. Persp Biol Med1991;35:20-36.
77
31. Vandenbroucke JP. Het belang van medische casuïstiek te midden van ‘evidence-based’geneeskunde en moleculaire verklaringen. Ned Tijdschr Geneeskd 2002;36:1699-1703.
32. Charlton BD, Walston F. Individual case studies in clinical research. J Evaluation Clin Pract1998;4:147-55.
33. Venning GR. Validity of anecdotal reports af suspected adverse drug reactions: the problem offalse alarms. BMJ 1982;284:249-52.
34. Arnaiz JA, Carné X. Riba N, Codina C, Ribas J, Trilla A. The use of evidence inpharmacovigilance. Case reports as the reference source for drug withdrawals. Eur J ClinPharmcacol 2001;57:89-91.
35. Finney DJ. The design and logic of a monitor of drug use. J Chron Dis 1965;18:77-98.
36. Grootheest AC van, Puijenbroek EP van. Pharmacovigilance in the Netherlands. In:Pharmacovigilance. Mann R, Andrew E, editors. John Wiley and Sons. Chichester 2002.
37. Kennedy DL, Goldman SA, Lillie RB. Spontaneous Reporting in the United States. In:Pharmacepidemiology. WHW Strom, editor. John Wiley and Sons. Chichester 2000.
38. Davis S, Raine JM. Spontaneous Reporting – UK. In: Pharmacovigilance. Mann R, Andrew E,editors. John Wiley and Sons. Chichester 2002.
39. Meyboom RHB. Detecting adverse drug reactions, Pharmacovigilance in The Netherlands.Thesis. Katholieke Universiteit Nijmegen 1998.
40. Meyboom RHB. The Case for Good Pharmacovigilance Practice. Pharmacoepidemiol DrugSaf 2000;9:335-6.
41. UMC. Guidelines for setting up and running a Pharmacovigilance Centre. Uppsala 2000.
42. Biriell C, Edwards IR. Reasons for Reporting Adverse Drug Reactions – Some ThoughtsBased on an International Review. Pharmacoepidemiol Drug Saf 1997;6:21-6.
43. Grootheest AC van, Puijenbroek EP van. Pharmacovigilance in the Netherlands. In:Pharmacovigilance: 309-15. Mann R, Andrews E, editors. Wiley. Chichester 2002.
44. Grootheest AC van, Puijenbroek EP van, Jong – van den Berg LTW de. Contribution ofpharmacists to the reporting of adverse drug reactions. Pharmacoepeidemiol Drug Saf2002;11:205-10.
45. Grootheest AC van, Olsson S, Couper M, Jong-van den Berg LTW de. The role of pharmacistsin reporting adverse drug reaction in international perspective. Pharmacoepidemiol Drug Saf2003 (in press).
46. Morrison-Griffiths S, Walley TJ, Park BK, Breckenridge AM, Pirmohamed M. Reporting ofadverse drug reactions by nurses. Lancet 2003;361:1347-8.
78
47. Grootheest K van, Graaf L de, Jong – van den Berg LTW de. Consumer Adverse DrugReaction Reporting – A New Step in Pharmacovigilance. Drug Saf 2003;26:211-7.
48. Puijenbroek EP van. Quantitative Signal Detection in Pharmacovigilance. Thesis. Universityof Utrecht 2001.
49. Puijenbroek EP van, Bate A, Leufkens HGM, Lindquist M, Orre R, Egberts ACG. Acomparison of measures of disproportionality for signal detection in spontaneous reportingsystems for adverse adverse drug reactions. Drug Saf 2002;11:3-10.
50. Bate A. The Use of a Bayesian Confidence Propagation Neural Network in Pharmaco-vigilance. Umeå University Medical Dissertations New Series No 846. Umeå 2003.
51. Szarfman A, Machado SG, O’Neill RT. Use of screening algorithms and computer systems toefficiently signal higher-then-expected combinations of drugs and events in the US FDA’sspontaneous reporting data base. Drug Saf 2002;25:381-92.
52. Puijenbroek EP van, Diemont WL, Grootheest AC van. Application of Quantitative SignalDetection in the Dutch Spontaneous Reporting System for Adverse Drug Reactions. Drug Saf2003;26:293-301.
53. Puijenbroek EP van, Egberts AC, Heerding ER, Leufkens HGM. Detecting drug-druginteractions using a database for spontaneous adverse drug reactions: an example withdiuretics and non-steroidal anti-inflammatory drug. Eur J Clin Pharmacol 2000;56:733-8.
54. Puijenbroek EP van, Egberts ACG, Meyboom RHB, Leufkens HGM. Association betweenterbinafine and arthralgia, gever and urticaria: symptoms or syndrome? Drug Saf 2001;10:135-42.
55. Tubert-Bitter P, Bégaud B, Moride Y, Chaslerie A, Haramburu F. Comparing the Toxicity ofTwo Drugs in the Framework of Spontaneous Reporting: A Confidence Interval Approach. JClin Epidemiol 1996;49:121-3.
56. Heijden PGM, Puijenbroek EP van, Buuren S van, Hofstede JW van der. On the assessmentof adverse drug reactions from spontaneous reporting sytems. The influence ofunderreporting on Odds ratios. Stat Med. 2002;21(14):2027-44.
57. Edwards IR. Spontaneous reporting – of what? Clinical concerns about drugs. Br J ClinPharmacol 1999;48:138-41.
79
3The role of thepharmacist
Chapter 3.1
Pharmacists’ role in reporting adverse drug reactions in an international perspective
Pharmacoepidemiol Drug Saf 2003 (in press)
Kees van Grootheest, MD1
Sten Olsson, MSc Pharm2
Mary Couper, MD3
Lolkje T.W. de Jong – van den Berg, PhD, PharmD4
1. Netherlands Pharmacovigilance Centre Lareb, ‘s-Hertogenbosch, The Netherlands
2. WHO Collaborating Centre for International DrugMonitoring, Uppsala, Sweden
3. WHO Programme for International Drug Monitoring, Geneva, Switzerland
4. Department of Social Pharmacy and Pharmacoepidemiology,GUIDE, Groningen, the Netherlands
83
Abstract
IntroductionThe participation of the pharmacist in national spontaneous reporting systems foradverse drug reactions (ADRs) has not always been a matter of course. Even today,there are a number of countries, in particular the Scandinavian countries, wherepharmacists are not authorised to report ADRs. In those countries in which they areallowed to report they do not always use this opportunity.
MethodsWe have conducted a review of the literature to investigate the involvement ofpharmacists in ADR reporting. In addition, we evaluated the pharmacists’ actualcontributions in 2001 by means of an international questionnaire-based surveyamong those countries participating in the WHO Drug Monitoring Programme inSeptember 2002. Apart from the numbers of pharmacists’ reports, respondents wereasked to indicate their assessment of both the quality and the significance of thecontribution. Of the 68 participating countries 41 responded by returning thequestionnaire.
Results and conclusionsThe appreciation of pharmacists’ ADR reports is high in those countries that hadmore experience with greater numbers of pharmacists' reports. The countries thatreceived fewer reports from pharmacists gave lower scores to their contribution. Ifthe specific contribution pharmacists can make to the quantity and quality of ADRreports were to be exploited to a greater extent, this could lead to a substantialimprovement of the international adverse drug reactions reporting system.
84
3.1.1 IntroductionPharmacists play an important role in the field of medicinal drugs including in thescientific field dealing with the safety of drugs - pharmacovigilance. This seems amatter of course. Whereas for doctors pharmacotherapy and the knowledge ofdrugs form only a minor component of their training, the study of pharmacyfocuses almost exclusively on drugs. With respect to pharmacovigilance, bothsound clinical judgement of the adverse drug reaction (ADR) and insight into theeffects of the drug are required to allow a conclusion to be drawn as to therelationship between the adverse event and the drug involved. Currently the role of the pharmacist in the reporting of adverse drug reactions isnot appreciated everywhere. In the Scandinavian countries, for instance,pharmacists are not authorised to report ADRs.(1,2) and in the United Kingdomthey have only recently been allowed to report independently.(3) By contrast, in theNetherlands 40% of the reports on ADRs are submitted by pharmacists and,moreover, their role in the maintenance of pharmacovigilance is substantial.(4)
A retrospective analysis of the pharmacist’s role in ADR reporting The initiative of an international reporting system for adverse drug reactions camein the wake of the thalidomide tragedy in the early 1960s. Although the Food andDrug Administration in the United States had been established some yearspreviously, this disaster was the catalyst for the initiation of systematic collection ofdata on ADRs primarily through the Hospital Reporting Program. In 1968 tencountries operating a national reporting system decided to collaborate under theauspices of the World Health Organization (WHO) and initiated the WHO PilotResearch Project for International Drug Monitoring.(5) In 1971 a resolution of theTwentieth World Health Assembly laid the foundation for the WHO Programmefor International Drug Monitoring.(6) In 1972 a report was published that wouldgive rise to the current international monitoring system of national centrescollaborating in the WHO Programme.(7,8) In 1973 a resolution by the WorldHealth Assembly supporting the report underlined the importance of exchange ofinformation on adverse drug reactions.(9) In the report, whose content is mainlystill relevant today, no mention is made of the pharmacist as a reporter of ADRs,although an Annex does refer to a study from 1965 that made use of dataoriginating from pharmacies.(10,11) In a recent WHO publication entitled TheImportance of Pharmacovigilance there is a passage that reads ‘inviting reports fromall professionals’, but the pharmacist as an independent reporter is notmentioned.(12) The Guidelines for setting up and running a PharmacovigilanceCentre, issued in 2000 by the WHO, does refer to the pharmacist.(13) Here,pharmacists are mentioned on a par with family practitioners and medicalspecialists. Pharmacists, nurses and dentists are also specifically mentioned in the
85
WHO-publication Safety of Medicines. A guide to detecting and reporting adversedrug reactions.(14)
The different roles of the pharmacistThe role of the pharmacist differs between countries but common factors in allcountries are that the knowledge of drugs defines the profession and that qualitycontrol and dispensing are the key tasks since the preparation of drugs nowconstitutes only a minor part of the pharmacist’s responsibility. Increasingly, careaspects and clinical knowledge are becoming essential to the study of pharmacy.However, the contribution pharmacists can make using the model of‘pharmaceutical care’ is not always exploited to its full extent and judgements oftheir contributions in this respect are not always favourable.(15)The various roles of the pharmacist can be categorised as follows:
1. The pharmacist as a dispenser of drugs This is the pharmacist’s traditional role and characteristically defines the imageof the profession. Many practitioners view this as the role befitting thepharmacist. The pharmacist delivers the medication as prescribed by thephysician and monitors its quality. In general and if requested, the pharmacist isexpected to provide information about the drug he or she dispenses althoughthis is often not seen as an integral part of his or her duties.(16) In addition tothe pharmacist’s growing (clinical) expertise, the advanced computerisation ofpharmacies in many countries has led to the awareness that the above is toolimited a role.(17)
2. The pharmacist as a drug consultantThis is the function the hospital pharmacist fulfils in most countries, albeit thathis or her contribution in the pharmacotherapeutic care of patients may varyacross countries. The pharmacist is recognised as an expert on drugs and has aconsultative role in pharmacotherapy. They may help to draft a formulary orassist in the treatment of individual patients undergoing complicated drugtherapies. Much of the literature on pharmacists relates to this function ofhospital pharmacists. In the USA the hospital pharmacist has an explicitcoordinating role when hospitals wish to report adverse events.(18) In theNetherlands legislation is being drafted that will give the pharmacist the statusof co-consultant. Pharmacotherapeutic discussion groups (FTOs), in whichgeneral practitioners and community pharmacists participate, have helpedchange the way general practitioners view the pharmacist.(19) In these FTOs thepharmacotherapy is discussed systematically and, as a rule, decisions concerningthe pharmacotherapeutic policy to be adopted are made by mutual agreement.
86
Few other countries have awarded the status of consultant to the communitypharmacist although in several countries there have been developments in thisdirection.
3. The pharmacist as a ‘substitute doctor’ In many parts of the world there is a shortage of doctors and pharmacists maybe the only providers of medical care available to people. The high costsassociated with health care may be the reason for this deficiency, but also thelarge distances to be travelled may play a role. This implies that patients willconsult the nearest pharmacy and ask for therapy they can afford, without priormedical consultation. It needs to be noted that usually pharmacists or pharmacyassistants who are acting as ‘substitute doctors’ are inadequately trained. Insome African countries, for instance, a registered nurse is qualified to set up andrun a pharmacy. Although this practice mainly occurs in low-income countries,the increasing use of over-the-counter (OTC) medication may also be relevantin this model.
It is clear that the involvement of the pharmacist in the practice of reporting ADRsis closely related to the function in society the profession is given.
What is known? There is relatively little quantitative and qualitative information available about thecontribution of pharmacists in ADR reporting. In an international review, Griffinnotes that in 1986 many countries have accepted pharmacists’ reporting ADRs asstandard practice.(20) In 1989 Fincham comments: ‘Exclusion of pharmacistssimply does not make sense’.(21) In their 1993 article on the differences betweenEuropean countries Lindquist and Edwards remark: ‘Pharmacists who advisepatients directly….are the most likely to detect adverse reactions’.(22) Roberts et al.conclude in 1994: ‘It is hoped that pharmacists in other countries will also beencouraged to participate in ADR reporting, a procedure that could only lead tobetter patient care’. The Uppsala Monitoring Centre (UMC) regularly publishes anoverview of the ways the national reporting systems in the various countries areoperated, in which the volume of pharmacist reports are also listed.(1) Theliterature on the actual contribution of pharmacists in ADR reporting often relatesto the hospital pharmacist in the USA, Canada and the UK.(22-25) The majority of publications concern the ongoing debate in the UK where, for the pastten years, the desirability of direct reporting by pharmacists has been discussed.(26,27)In the various textbooks on pharmacoepidemiology and pharmacovigilance thepharmacist receives little attention, with the exception of Inman who, as early as1986, devoted a chapter to the role of the pharmacist.(28) The authors examine their
87
88
Panel 1Questionnaire send to 68 National Centres participating in de WHO DrugMonitoring Programme
Country :Your name :Organisation :Your email address :
1. Are pharmacists officially permitted to report to the national centre?in your country? yes / no
2. If they are permitted, are they also encourage to report yes / no
3. How many report did you receive in 2001?- total number of reports :- are these reports direct reports from health care professionals
or also reports from pharmaceutical industry?direct from health professionals / industry / both
- origin of the reports to the National Centre: - physicians :- pharmacists :- pharmaceutical industry :- patients/consumers :- other :
4. About pharmacist reports:- how many reports did you receive from hospital pharmacists? :- how many reports did you receive from dispensing or community pharmacists?:
+--------- total number of reports from pharmacist did you receive in 2001? :
5. How do you consider the quality of pharmacists reports compared with those from physicians?- specificity of clinical information: bad/ moderate/ good/ excellent- completeness of case details: bad/ moderate/ good/ excellent- completeness of medication history bad/ moderate/ good/ excellent
6. How do you consider the contribution of pharmacist’s reports to your national centre?non valuable/ moderate valuable / very valuable
7. If you don’t accept pharmacist’s reports: - Are there any plans for the future?- Why are the pharmacists reports not accepted?
8. Do you have any suggestion or comments?
contribution in relation to non-prescription drugs. They also point to the value ofthe medication history that pharmacies keep and the advantage pharmacists havethrough the use of computer technology. They conclude by stating: ‘It is to behoped that protection of professional territories will not prejudice such acontribution’.
3.1.2 An international surveyTo gain insight into the current contribution of pharmacists in ADR reporting, wehave conducted an exploratory survey among countries participating in the WHODrug Monitoring Programme. The aim of our study was to:1. investigate in which countries pharmacists are authorised to report2. determine the proportion of ADR reports submitted by pharmacists3. evaluate per country how the pharmacists’ contributions are valued
MethodsThe survey included countries participating in the WHO Drug MonitoringProgramme. The WHO Programme for International Drug Monitoring iscoordinated from Geneva by the Quality Assurance and Safety of Medicines Team,which is part of the Department of Essential Drugs and Medicines Policy. TheUppsala Monitoring Centre (UMC) has the operational responsibility for theWHO Programme and maintains the international database of the ADRs it receivesfrom the national centres.In September 2002, we sent all invited countries a questionnaire by e-mail (see Panel1) in which they were requested to list their data on the reports that had beensubmitted by pharmacists in the year 2001. After three months, the countries thathad not responded received a reminder. The questionnaire made a distinctionbetween the total number of reports each country had received and the directreports the national centres had received via the spontaneous reporting systemduring that period, which is after subtraction of the reports submitted by thepharmaceutical industry sector (marketing authorisation holders). A furtherdistinction was made between reports originating from hospital pharmacists andthose stemming from community pharmacists.In addition, the respondents were asked to indicate their assessment of the qualityof the reports. If pharmacists did not participate in the national reporting system,the countries were requested to state the reason why they were not included and toprovide any future plans in this respect.
ResultsAt the time of the survey 68 countries participated in the WHO Programme and 41completed forms were returned, two of which (i.e. from Brunei and Suriname)
89
90
Table 1Countries included in our study, year of participation in WHO Drug Monitoring Programme,pharmacists permitted to report, total number of all reports in 2001 and percentage frompharmacists , number of reports direct from health professionals and percentage frompharmacists , total number of reports from hospital pharmacists and community pharmacists.
per- total % % country since mitted number pharm1 direct pharm1 hosp comm
reports in total and more as hundred pharmacist’s reports in a country.2. Total number of pharmacist’s reports; no distinction could be made between hospital
pharmacists and community pharmacists.3. Number for 2000 according to Saarinen.(2)4. Including about 500 reports from nurses5. Including reports direct from patients6. For the USA the percentage of pharmacist report of those who could be identified of the total
number of reports. Kennedy et al. give higher figures for the number of direct reports.(44)
stemmed from countries that did not participate in the programme, but have astatus as observer. Eight countries were associate members meaning that they donot yet meet the criteria for full membership mainly because theirpharmacovigilance systems have only recently become operational, which mayprevent them from being able to submit their reports on a regular basis. Eight of the 41 questionnaires were returned in response to our reminder, makingthe total response of member states of the WHO Programme 57.4% (39/68). Mostof the countries that had participated in the programme for more than ten yearsreturned the questionnaire. Only in three of the 41 responding countries thepharmacist was not authorised to report, i.e. Finland, Norway and Sweden. Of the 68 countries participating in the WHO Programme for International DrugMonitoring in October 2002, a few had only recently joined the programme, as canbe seen in Table 1. Table 1 lists the total number of ADR reports per country for 2001, the number ofreports per profession and the number of reports submitted by pharmacists dividedinto the categories hospital pharmacists and community pharmacists. Fourcountries, Australia, Canada, The Netherlands and Spain, have a considerablecontribution from pharmacists, both in percentage (>20%) and number of reports(>100 reports). This is also the case in Chile and the USA, but a percentage couldnot be calculated. In Table 2 the assessments of the clinical information are presented, as well as theratings of the quality of content and medication history, both per report. Inaddition, the subjective general judgment of the quality of the contributions of thepharmacists to the national reporting systems is provided. The countries that havethe highest score of this subjective general judgment were Australia, Canada,Ireland, Japan, Tanzania and the USA.
3.1.3 DiscussionAlthough in most countries pharmacists are allowed to report ADRs to theirnational reporting systems, only a limited number of countries indicate that thesecontributions are of major significance to the system and quality ratings vary.
Differences per member stateWhat stands out is the fact that in the Nordic countries mentioned (i.e. Finland,Norway and Sweden) pharmacists do not participate in the nationalpharmacovigilance system. This is also the case in countries such as Denmark,Iceland and Estonia. Indonesia, Vietnam, Oman, the Czech Republic, Rumania andSlovakia stated that they do not receive any reports from pharmacists according aWHO survey of 1999.(1) Italy, the United Kingdom and Oman do acceptpharmacist reports. In several countries, such as France, Italy and Spain, the
91
92
Table 2Subjective judgment of specificity of clinical information, completeness of casedetails, completeness of medication history and appreciation of the contribution ofpharmacists’ reports to the National Centre1.
1. Only these countries are included in this figure that accept pharmacist’s ADR reports andanswered the involved questions.
reporting of ADRs is mandatory, including that of pharmacists. It is notable that inSweden nursing staff are authorised to report, whereas pharmacists are not. Ingeneral, only those authorised to prescribe medication are allowed to report ADRs.We did not find a clear relationship between the level of training and theinterpretation of the profession of pharmacist and the fact whether or notpharmacists are allowed to report. In Sweden an extensive study on thecontribution pharmacists can make with respect to the detection of drug-relatedproblems was published recently.(29) In Finland pharmacists are highly trained andthere is an extensive network of pharmacies. Not authorising pharmacists to reporthere is justified as follows: ‘It is thought that limited resources would be used morecost effectively when the reporting is focused on medically confirmed seriousADRs from physicians’.(2) In Norway plans have been developed to involve thepharmacist more closely in the process of ADR reporting, with an emphasis onOTC medication. It must be noted that pharmacist’s reports are accepted whensubmitted in this country, although this occurs only sporadically. Other countries, such as Cuba, Ireland, the Netherlands and Singapore, havelaunched programmes to promote the participation of pharmacists.(30,31)
The quantitative contribution of the pharmacistThe total number of pharmacist reports per country for the year 2001 is presentedin Table 1. In Australia, Canada, France, Japan, the Netherlands, Spain, the UK andthe USA pharmacists submitted more than 1000 ADR reports. All of thesecountries have at least a twenty-year tradition in the systematic collection of ADRs.Chile also received a relatively high volume of pharmacists' reports.The proportional contribution of the pharmacist needs to be taken into accountwhen analysing the number of reports each country has indicated since the reportsare either received directly from health professionals or have been submitted by thepharmaceutical industry. In the latter case, the background of those responsible forthe report is not always known, so the number of pharmacists’ reports could beunderestimated. Some countries could not make this distinction for their direct,spontaneous reports. For these countries the highest percentages of pharmacists'reports received via the spontaneous reporting systems were recorded by Canada(88.3%), Australia (40.3%), the Netherlands (40.2%), Japan (39%), Spain (25.9) andPortugal (23.4%). The actual numbers are represented in Table 1. Percentages ofreports from pharmacists are only calculated if there were more than one thousandreports in total and more than one hundred pharmacists reports in a country.
The qualitative contribution of the pharmacistTable 2 presents the quality assessments of pharmacists' reports as indicated inresponse to the relevant question of the questionnaire. All the countries that had
93
received large quantities of pharmacist reports also awarded high ratings to thecontributions and regarded them as valuable. This also applies to those countries inwhich the proportion of the reports by pharmacists in the total volume received ishigh. It is important to take into consideration that both the quality and significanceratings were subjective. It was also of interest to determine whether, in those countries in which thepharmacists’ contribution was substantial, the reports had predominantly been sentin by hospital pharmacists or mainly by community pharmacists. In Japan, theNetherlands and Portugal community pharmacists submit the bulk of reports; in allother countries most reports stem from hospital pharmacists. In an earlierpublication the contribution of the Dutch pharmacists- community pharmacists inparticular- has been described in more detail.(4) In the Netherlands pharmacistshave played a significant role in the formation of the national reportingsystem.(31,32)The contribution of the hospital pharmacist varies per country. In the USA andCanada this group is instrumental in the ADR reporting by hospitals.(18,33-35)
The pharmacist as an ADR reporterAs has been mentioned above, the pharmacist is appreciated in his or her role ofreporter in countries in which pharmacists have long been closely involved in thenational reporting systems. A review of the literature showed that the quality of thereports of both the hospital pharmacist and the community pharmacist is sufficientto contribute to the systems’ success.(4,25,36) Yet, direct reporting by thepharmacist has not been accepted in all countries. Notable in this respect is that inseveral of the Nordic countries the pharmacist is mainly restricted to the role ofdispensing pharmacist and is not considered sufficiently qualified to report onADRs. Furthermore, in many of the countries in which pharmacists are authorisedto report, their contribution to the system is negligible or non-existent. Although there are differences both with respect to the attitude of the variousnational spontaneous reporting systems towards the pharmacist and to theperception of the function of the profession in society, it is clear that the role of thepharmacist is changing. Fundamental to the pharmacist’s role is to ensure thatmedicines are used safely.(37) The standard practice of preparing and dispensingdrugs is increasingly shifting towards pharmaceutical care. The pharmacist’soriginal field of expertise, primarily in the domains of chemistry and formulae, isevolving into more pharmacotherapy-related clinical knowledge. Several countriesare considering the possibility of authorising the pharmacist to write certainprescriptions such as repeat prescriptions. In the Netherlands steps have been takento award the pharmacist the official status of co-consultant. This will allow thepharmacist access to patient files, which will afford him or her the opportunity to
94
become more actively involved in patient treatment and pharmacovigilance.There is ample evidence that shows that the pharmacist is both willing and capableto adequately fulfil the role of a reporter of ADRs.(25,26,37-41) In addition to thisdirect role, the pharmacist can also play a coordinating role, both in general practiceand in a hospital setting. The fact that in many countries most pharmacies are highlycomputerised is important in this context. The argument against direct reporting by pharmacists is that their clinicalknowledge is limited. On the other hand, one could also argue that the knowledgedoctors have about drugs is often limited since this aspect is not given sufficientattention during their training.(42) The contribution the pharmacist can make willvary per country and will depend on the expertise and the status the profession isgiven within the different health care systems. Cooperation between doctors andpharmacists appears to be of vital importance, with each of the two professionalgroups contributing their respective expertise and experience to promote therational and safe use of medicinal drugs.
3.1.4 ConclusionIn several countries the pharmacist plays a prominent role in ADR reporting.Particularly in those countries that have participated in the WHO Drug MonitoringProgramme longer and accept pharmacists’ reports, the number of pharmacistreports is substantial and the reports are generally highly valued. In a large numberof countries the pharmacist’s contribution is small and in some countries,specifically the Nordic countries, the pharmacist is not authorised to report ADRsindependently to the national reporting system. The aim of a comparison of the various practices and experiences of differentcountries is to learn from the differences.(5,43) With respect to the potentialcontribution pharmacists can make to the national reporting systems, the practicalexperience of countries such as Australia, Canada, the Netherlands and the USAmay significantly improve both the quantity and the quality of the reports onADRs worldwide.
95
References
1. Olsson S. National Pharmacovigilance Systems – Country Profiles and Overview (secondedition). Uppsala Monitoring Centre. Uppsala 1999.
2. Saarinen S. Adverse drug reaction reporting – comparison between Finland and TheNetherlands. Master’s thesis. University of Kuopio. Kuopio 2002.
3. Major E. The yellow card scheme and the role of pharmacists as reporters. Pharm J; 269:25-6.
4. Grootheest AC van, Puijenbroek EP van, Jong – van den Berg LTW de. Contribution ofpharmacists to the reporting of adverse drug reactions. Pharmacoepeidemiol Drug Saf,2002;11:205-10.
5. Lindquist A.M. Seeing and Observing in International Pharmacovigilance. Thesis. KatholiekeUniversiteit Nijmegen. Nijmegen 2003.
6. WHO. Handbook of resolutions and decisions of the World Health Assembly and ExecutiveBoard, 11th ed. World Health Organization. Geneva 1972. (WHA 20.51).
7. WHO. International Drug Monitoring: The Role of National Centres. Technical ReportSeries. WHO. Geneva 1972.
8. Olsson S. The Role of the WHO Programme on International Drug Monitoring inCoordinating Worldwide Drug Safety Efforts. Drug Saf 1998;19:1-10.
9. WHO. Handbook of resolutions and decisions of the World Health Assembly and ExecutiveBoard, Vol 11948-1972. Geneva, World Health Organization, 1973. WHA 16.36 Clinical andpharmacological evaluation of drugs.
10. Esch AF. The planning of a national drug monitoring system. In: International Drug Monitoring:The Role of National Centres. Technical Report Series. WHO Geneva 1972. Annex 3:44-47.
11. Friedman GD, Collen MF, Harris LE, Van Brunt EF, Davis LF. Experience in monitoring drugreactions in outpatiens. JAMA 1971;217:567.
12. WHO. The Importance of pharmacovigilance. Safety Monitoring of medical products. WHO.Geneva 2002.
13. UMC. Guidelines for setting up and running a Pharmacovigilance Centre. UMC. Uppsala 2000.
14. WHO. Safety of Medicines – A guide to detecting and reporting adverse drug reactions.Geneva 2002. (www.WHO/EDM/QSM)
15. Strom BL, Hennessy S. Pharmacists Care and Clinical Outcomes for Patients With ReactiveAirways Disease. JAMA 2002;288:1642-3.
96
16. Moss RL, Garnett WR, Steiner KC. Physician attitudes towards pharmacists counselingpatients on adverse drug reactions. Am J Hosp Pharm 1980;37:243-7.
17. Tilson HH, Hartzema AG, Porta M. Pharmacoepidemiology: The Future. In:Pharmacoepidemiology, an Introduction. Hartzema AG, Tilson HH, Porta M, editors.Harvey Whitney Books Company Cincinnati 1998.
18. FDA. Guideline for Postmarketing Reporting of Adverse Drug Experiences. Department ofHealth and Human Services (85D-0249). FDA 1992.
19. Reebye RN, Avery AJ. Bosch WJHM van den, Aslam M, Nijholt A, Bij A van der. Exploringcommunity pharmacists’ perception of their professional relationship with physicians inCanada and the Netherlands. Int J Pharm Pract 1999;7:149-58.
20. Griffin JP. Survey of the spontaneous adverse drug reactions reporting schemes in fifteencountries. Br J Clin Pharmacol 1986;12:243-7.
21. Fincham JE. Adverse Drug Reaction Reporting and Pharmacists. J Clin Pharm Therapeutics1989;14:79-81.
22. Lindquist M, Edwards IR. Adverse drug reactions reporting in Europe: some problems ofcomparison. Int J Risk Saf Med 1993;4:35-46.
23. Leape LL, Cullen DJ, Dempsey Clapp M, Burdick E, Demonaco HJ, Erickson JI, Bates DW.Pharmacist Participation on Physician Rounds and Adverse Drug Events in the Intensive CareUnit. JAMA 1999;282:267-70.
24. Wistanley PA, Irvin LE, Smith JC, Orme ML’E, Breckenridge AM. Adverse Drug Reactions:a hospital pharmacy-based reporting scheme. Br J Clin Pharmacol 1989;28:113-6.
25. Ahmad SR, Freiman JP, Graham DJ, Nelson RC. Quality of Adverse Drug ExperienceReports Submitted by Pharmacists and Physicians to the FDA. Pharmacoepidem Drug Saf1996;5:1-7.
26. Roberts PI, Wolfson DJ, Booth TG. The Role Of Pharmacists in Adverse Drug ReactionReporting. Drug Saf 1994:11:7-11.
27. Beard K. Introduction. In: Adverse Drug Reactions. A Lee, editor. Pharmaceutical Press,London 2001.
28. Poston J, Parish P. The pharmacist. In: Monitoring for drug safety. WHW Inman, editor. MTPPress. Lancanster 1986.
29. Westerland T. Drug-related problems, indentification, characteristics and pharmacyinterventions. Thesis. Göteborg University 2002.
30. Debesa F, Jiménez G, Figueras A, Diogène E, Peña JP, Avila J, Laporte J-R. Spontaneousreporting of adverse drug reaction in Cuba: integrating continuous education, training andresearch in network approach. Br J Clin Pharmacol 2002;54:334-5.
97
31. Grootheest AC van, Puijenbroek EP van. Pharmacovigilance in the Netherlands. In:Pharmacovigilance. Mann R, Andrew E, editors. John Wiley and Sons. Chichester 2002.
32. Koning GPH. A regionalized spontaneous surveillance programme for adverse drug reactionsas a tool to improve pharmacotherapy. Thesis. Utrecht University 1994.
33. Accreditation Manual for Hospitals 1993. Joint Commission on Accreditation of HealthcareOrganizations, Oakbrook Terrace, Ill, 1993.
34. ASHP guidelines on adverse drug reaction monitoring and reporting. Practice Standards ofASHP 1992-93. American Society of Hospital Pharmacists, Bethesda MD, 1992.
35. Standards of Practice. Canadian Society of Hospital Pharmacists. 1990.
36. Lee A, Bateman DN, Edwards C, Smith JM, Rawlins MD. Reporting of adverse drugreactions by hospital pharmacists: pilot scheme. BMJ;315:519.
37. Grootheest AC van, Mes K, Jong – van den Berg LTW de. Attitudes of communitypharmacists in the Netherlands towards adverse drug reactions reporting. In J Pharm Pract2002;10:167-72.
38. Emerson AE, Martin RM, Tomlin M, Mann RD. Prospective cohort study of adverse eventsmonitored by hospital pharmacists. Pharmacoepidemiol Drug Saf 2001;10:95-103.
39. Green CF, Mottram DR, Raval D, Proudlove C, Randall C. Community pharmacists’ attitudeto adverse drug reaction reporting. Int J Pharm Pract 1999;7:92-9.
40. Sweis D, Wong ICK. A survey on factors that could affect adverse drug reaction reportingaccording to hospital pharmacists in Great Britain. Drug Saf 2000;2:165-72.
41. Green FG, Mottram DR, Rowe PH, Pirmohamed M. Attitudes and knowledge of hospitalpharmacists to adverse drug reaction reporting. Br J Clin Pharmacol 2001;51:81-6.
42. Grootheest AC van, Edwards IR. Labelling and ‘Dear Doctor’ Letters, Are TheyNoncommittal? Drug Saf 2002;25:1051-1055.
43. Hughes ML, Whittlesea CMC, Luscombe DK. Review of National Spontaneous ReportingSchemes, Strengths and Weaknesses. Adv Drug React Toxicol Rev 2002;21:231-41.
44. Kennedy DL, Goldman SA, Lillie RB. Spontaneous Reporting in the United States. In:Pharmacoepidemiology. WHW Strom, editor. John Wiley and Sons. Chichester 2000.
98
Chapter 3.2Attitudes of community pharmacists in the Netherlands towards adverse drug reaction reporting
Int J Pharm Pr 2002;10:267-72.
Kees van Grootheest, MD1
Kyros Mes, PharmD2
Lolkje T.W. de Jong-van den Berg, PharmD, PhD2
1. Netherlands Pharmacovigilance Centre Lareb,’s-Hertogenbosch, the Netherlands.
2. Department of Social Pharmacy and Pharmacoepidemiology, GUIDE, Groningen, the Netherlands
99
Abstract
ObjectiveAim of the study is to gain insight into the attitude and behaviour of communitypharmacists in the Netherlands with respect to the reporting of adverse drugreactions.
MethodsA questionnaire survey conducted among 200 community pharmacists at randomselected from the membership list of the Royal Dutch Society for the Advancementof Pharmacy.
ResultsResponse was 73% (n=147). Community pharmacists in the Netherlands regard thereporting of adverse drug reactions (ADRs) as an integral part of their professionalduties (100%) and they do not experience any major impediments in this respect.This is reflected in the frequency and number of reported ADRs the nationalpharmacovigilance centre receives. The following impediments for reporting werementioned most frequently: the adverse effect is assumed to be already known(32%), the reporting procedure is too time-consuming (25%), and there isuncertainty concerning the causal relationship between ADR and drug (25%). Feedback is mentioned most as the chief impetus for reporting, both with respect tothe actual report submitted and general feedback as provided in publications.Although consultation with the attending clinician is not compulsory in theNetherlands, 55% of the pharmacists deem this an important aspect in the reportingprocess.
ConclusionCommunity pharmacists in the Netherlands are knowledgeable about reportingADRs and highly motivated to do so. This positive attitude towards reportingadverse events is based on the established tradition of pharmacists reporting in theNetherlands.
100
3.2.1 IntroductionPharmacists can play an important role in the detection and reporting of suspectedadverse drug reactions (ADRs). Greater participation by pharmacists in ADRreporting could be an important tool to counter under-reporting of ADRs. Thepharmacist’s role in pharmacovigilance varies from country to country. In themajority of countries participating in the WHO Programme for International DrugMonitoring, pharmacists can report independently, but in the UK for instance theright to report direct has only been achieved in recent years.(1,2) The WHOProgramme is co-ordinated by the Uppsala Monitoring Centre, which maintains aglobal ADR database. The Netherlands has a long history of pharmacists reportingsuspected ADRs. Pharmacists were allowed to submit reports from the beginningof ADR reporting schemes in the Netherlands in 1963, but were boosted with thestart of Lareb’s regional activities in 1986.(3) The contribution of pharmacist ADRreports is substantial in the Netherlands, in terms of both quality and quantity: 40per cent of spontaneous reports to Lareb originate from pharmacists, almost all ofwhom are community pharmacists.(4) Earlier research showed that nearly all Dutch pharmacists were aware of theexistence of the reporting system and familiar with the reporting procedure.Awareness was considerably lower for general practitioners and medical specialists,at 82 per cent and 45 per cent, respectively.(5)However, little was known about pharmacists’ attitude towards their perceived rolein the reporting of ADRs, the factors that encourage or discourage the actualsubmission of reports, and the pharmacists’ behaviour in relation to ADRs. A smallstudy conducted by Green et al. among community pharmacists in the UK is theonly published study of community pharmacists and ADRs.(6) The contribution ofhospital pharmacists has been more extensively investigated.(7,8) However mostpublications on ADR reporting concern the attitude and behaviour of medicalpractitioners.(9,10) Thus, the aim of the present survey was to gain insight into the attitudes and reportingbehaviour of community pharmacists in the Netherlands to ADR reporting.
3.2.2 MethodsA structured, 39-item questionnaire was sent to a stratified random sample of 200community pharmacies in the Netherlands at the end of 2000 with a request for oneof the practising pharmacists to complete it. There were 2,636 practisingcommunity pharmacists working in 1,602 pharmacies in the Netherlands in 2000.A reminder was sent after six weeks. The forms could be returned anonymously.The membership list of the Royal Dutch Society for the Advancement of Pharmacy(KNMP) was consulted to select all registered community pharmacists.Subsequently, from each of the 23 districts into which the KNMP members are
101
102
Table 1Statements given in the questionnaire – pharmacist could give their (dis)agreementin a scale 1 – 4.
1. Reporting ADRs is part of the profession of a pharmacist.2. I feel pharmacovigilance is important.3. I want to be sure the ADR is related to the drug before reporting.4. I do not report ADRs of OTC products delivered by my pharmacy.5. I report an ADR that causes:
a. hospitalisationb. a life threatening situationc. a congenital anomalyd. persistent disability or incapacitye. death of the patient.
6. I report to get more insight about ADR questions at hand.7. I report to show the patient that his concern is taken seriously.8. I always report ADRs because it is part of pharmaceutical care.9. Consulting the physician is important before reporting an ADR.10. I discuss ADRs at the Pharmacotherapy Consultation Group.11. I don’t report because reporting forms are not available.12. I don’t report because I don’t know the address where these reports should be sent.13. The reporting form is to complicated to fill in.14. Reporting ADRs is time consuming.15. All serious ADRs are detected before registration.16. I don’t report ADRs because I want to publish about it myself.17. I don’t report because I am not convinced about the confidential handling of the
report.18. I don’t report ADRs because I fear to harm the confidence of my patients.19. I don’t report because I find it difficult to admit that the patient has got harmed.20. I don’t report because reporting may give the impression that I am ignorant
concerning ADRs.21. I don’t report because I fear legal liability for the reported ADR.22. I am not motivated to report.23. I don’t report because I have insufficient clinical knowledge.24. I don’t report because I don’t know how to report an ADR.25. I don’t report because I am not convinced the ADR is caused by the drug.26. I would report more if:
a. there is an obligation to do sob. there is a feec. I see my colleagues are doing sod. my attention is drawn to it by a publication, for instance the Drug
Bulletine. I received more feedback by mailings.
organised, pharmacists were randomly selected in proportion to the district’s totalnumber of community pharmacists. The questionnaire items were formulated usinga modified version of the Fishbein and Azjen model defining the relationship betweenknowledge, attitude and behaviour, the influence of the social norm and the impedingand facilitating factors involved.(11) The first four questions covered the details andcharacteristics of the participating pharmacist. Pharmacists were asked which school ofpharmacy they had attended and which year they had qualified. The next four itemsconsisted of general questions aimed at establishing the extent of the respondent’sknowledge about the Dutch ADR reporting system. Twenty-six items explored thepharmacist’s attitude to reporting and the factors that either positively or negativelyaffect his or her attitude. These items were worded as a series of statements and thepharmacist was asked to indicate their agreement or disagreement on a Likert scalefrom 1 to 4 (Table 1). One of the statements gave the criteria for serious ADRs set bythe Council for International Organisations of Medical Sciences (CIOMS) and wasintended to assess pharmacists’ knowledge of the criteria.(12) Four questionsinvestigated pharmacists’ behaviour. A final open-ended question invited therespondents to suggest possible ways to increase pharmacists’ motivation to reportADRs. Prior to the survey, the questionnaire was piloted with eight pharmacists,which resulted in adaptation of the phrasing of several of the questions.
3.2.3 ResultsThe first mailing resulted in 120 questionnaires being returned. After the reminder,another 27 responses were received. Thus, a total of 147 of the original 200 formswere returned, a response rate of 73.5%. Of the respondents 56.2% were male and43.8% female; 71.3% indicated being first pharmacist (owner or manager) and28.1% second pharmacist (pharmacist working in a partnership). The distributionof the universities where the pharmacists had trained and the years in which theyqualified were similar to the expected distribution. The data thus indicated that therespondents could be regarded as a representative sample of the total population ofDutch community pharmacists.
- Familiarity with the reporting system All but one respondent indicated being familiar with the way in which ADRreporting is organised in the Netherlands. Almost three-quarters (73%) knew thatthe Netherlands Pharmacovigilance Centre Lareb was an independent foundationof medical practitioners and pharmacists. 27% thought Lareb was an officialgovernment body. This is not surprising since Lareb receives government fundingand reports to the Medicines Evaluation Board. Overall, 68% of respondentsdisagreed with the statement that ‘all serious ADRs are detected beforeregistration.’ Just over three-quarters (76%) said that they used the reporting forms
103
provided in the Farmacotherapeutisch Kompas (the main drug desk reference bookin the Netherlands) and 24% used the forms from the Dutch Drug Bulletin(Geneesmiddelenbulletin). 7% indicated they sometimes also reported electronically.
- Attitude All respondents considered the reporting of ADRs to be integral to theirprofessional duties and, with the exception of one pharmacist, they all acknowledgedthe importance of reporting, although 3.5% said that they were not motivated toreport. 82% saw reporting as an inherent part of pharmaceutical care and the samepercentage said that ADR reporting was an indication of taking patients’ complaintsseriously. More than two-thirds (68%) of the respondents were of the opinion thatreporting adverse effects helped them to gain more insight into the problemsassociated with side effects. A majority (55%) said that, before reporting, theyneeded to be convinced of the causality between the drug and adverse reaction. Inthe Netherlands pharmacists can report independently. However, 55% ofrespondents felt the need to discuss their proposed report with the medicalpractitioner involved before submitting it. Almost half (47%) said that theydiscussed reports with the GPs and pharmacists who participated in their localpharmacotherapy consultation group, a regular forum in which communitypharmacists meet with general practitioners.(13)
- BehaviourOf the pharmacists surveyed, 53% indicated that they had reported more than oneadverse event in the previous year. Although it was not possible to identify individualpharmacists’ reports to Lareb, a comparison could be made with the reports submittedover that period. The results of that comparison suggested that pharmacists’ self-reports overestimated those submitted by a factor of almost three. The majority of pharmacists completed the reporting procedure themselves, with apharmacy assistant doing so in less than 3% of cases. In 96% of cases, the report wassubmitted to the Lareb Centre. Of these reports, 40% were also sent to otherinstitutions: the marketing authorisation holder (MAH) or the pharmacist’s ownprofessional society. Four pharmacists said that they reported solely to the MAH.Adverse reactions to over-the-counter (OTC) products were said to be reported by84% of pharmacists. Over 95% of the respondents indicated that they were aware thatparticularly serious side effects needed to be reported as well as unusual adversereactions and adverse events relating to a newly marketed drug.The survey investigated whether pharmacists recognised adverse events that aredenoted as serious according to the criteria set by the CIOMS as significant eventsto be reported. This proved to be the case for 97% of respondents.
104
- Barriers Pharmacists were asked which factors negatively affected their willingness to report. Aquarter of respondents indicated that reporting ADRs was too time-consuming, and asimilar number mentioned uncertainty concerning the causal relationship betweenADR and drug. The fact that the adverse effect was assumed to be already known wasan obstacle for 32%. An intention to publish their own report on the adverse reactionwas the reason stated for not reporting the ADR for only 3% of the pharmacists. Asingle pharmacist mentioned doubts about the confidentiality of the information as thereason for not reporting and in one other case the pharmacist indicated that they foundit difficult to report that a drug had caused harm to a patient and stated fear of liabilityclaims as the reason for not reporting. Unavailability of the reporting forms and other practical barriers played minorroles: 1.4% and 2%, respectively. Finally, 9% of the respondents thought the formis too complicated. An overview of the scores of the possible barriers to reportingis provided in Table 2.
105
Table 2Impeding factorsLevel of agreement in percentages (n=147)
strongly agree disagree stronglyagree disagree
- no reporting forms available 0 1 33 66- reporting address unknown 0 2 33 65- reporting form too complicated 1 8 40 51- too time-consuming 3 22 40 35- all adverse reactions are known 8 24 46 22- want to publish myself 1.5 1.5 29 68- confidentiality 0 1 38 61- patient confidentiality 0 0 37 63- difficult to admit harm to patient 0 1 38 61- reporting could show ignorance 0 0 41 59- fear of liability 0 1 41 58- no motivation 0 4 44 52- insufficient clinical knowledge 0 2 49 49- do not know how to report 0 2 39 59- causality uncertain 4 21 47 28
- Facilitating factors To investigate which factors might motivate pharmacists to report suspected ADRs,the questionnaire explored their views on a number of factors mentioned in theliterature. In addition, an open-ended question invited them to state their ownsuggestions. Table 3 provides an overview of the suggestions made in response tothe open-ended question.
Of the total sample of pharmacists, 53% mentioned more or improved feedback astheir prime motivator, and 39% indicated that publication on adverse effects injournals like the Geneesmiddelenbulletin was the most important stimulus toreporting. Respondents were asked whether making ADR reporting compulsorywould motivate them to report: 30% answered in the affirmative. Only 18%indicated that receiving financial compensation for reports submitted wouldmotivate them to report more readily. Peer reporting was an important incentive for12% of the respondents.
3.2.4 DiscussionThis is the first published study of Dutch community pharmacists’ familiarity withand attitudes towards ADR reporting, their self-reported behaviour and factorsinfluencing their attitudes. The response rate was good, at over 70%, and analysis
106
Table 3Suggestions to encourage reporting adverse drug reactions, as mentioned by therespondents (open question)
Suggestions are ordered in frequency of occurrence expressed by the number ofrespondents who proposed them.1. feedback 292. publications 263. information about the national centre 174. simplification of reporting procedure 145. promoting reporting as part of professional duty 136. encouraging patients to report adverse drug reactions to the pharmacist 77. financial compensation 78. more attention to ADR reporting in university curriculum 69. database of national centre available on the Internet 610. compulsory reporting 2
of respondents’ demographics indicated that they were representative of the totalpopulation of Dutch community pharmacists. Our findings show that communitypharmacists in the Netherlands have a positive attitude towards reporting ADRs.For pharmacists to report ADRs several practical requirements need to be fulfilled,which are listed in Table 4. In many countries these criteria are not being met. Therehas been little in the published literature about the attitude and behaviour ofcommunity pharmacists in relation to ADR reporting. Green et al described theattitude of community pharmacists in the UK.6 Their study was conducted in 1999,two years after pharmacists in the UK were officially granted the right to reportdirect to the Committee on Safety of Medicines (CSM), following years ofdebate.(14) We compared the results from our survey with the data available in the literature oncommunity pharmacists, hospital pharmacists and medical practitioners.
- Familiarity with the reporting systemAn earlier study of ours had already shown that the familiarity of pharmacists in theNetherlands with the existing ADR reporting system was high.(4) This finding wasconfirmed in the present study: 99% of our respondents indicated being familiarwith the reporting system. Green et al found a comparable percentage forcommunity pharmacists in the UK (93%) and this was even higher for hospitalpharmacists: 97%.(6,8) For medical practitioners in the Netherlands the level ofknowledge about the system was lower, particularly among doctors working inhospitals.(5)
- Attitude Pharmacists are directly involved in pharmacotherapy and consequently might beexpected to regard reporting suspected adverse events as an integral part of theirprofessional duties and this was the case in our study. Our respondents also saw
1. Formal access to the national pharmacovigilance system2. Knowledge about the reporting system3. Availability of the reporting form (paper or electronic)4. Simple and user-friendly reporting form5. Feedback
reporting ADRs as a vital part of pharmaceutical care. The notion that theindividual pharmacist carries professional responsibility within the context ofpharmaceutical care is well developed in the Netherlands.(15) In the UK, Green etal found that 77% of community pharmacists considered ADR reporting aprofessional obligation, and the figure was 86 % for hospital pharmacists.(6,8) Sincethe latter are part of a larger organisation, their contribution could also involvefacilitating, maintaining and supporting a reporting system in their ownhospitals.(16,17)In the Netherlands, pharmacists are not legally bound to consult the patient’sdoctor prior to reporting. Nevertheless, 55% of respondents saw this as animportant element of the reporting process. In Reebye et al’s study, two-thirds ofDutch community pharmacists reported regularly conferring with the GP onmatters of pharmacotherapy, specifically within the framework of thepharmacotherapy consultation group. In these local discussion groups, communitypharmacists and general practitioners meet each other approximately every twomonths.(18) In our survey, 47% of the respondents stated that these were used fordiscussions on ADRs. In the UK, consultation with the GP is part of thepharmacist’s reporting protocol and may be an important barrier, particularly whenthe relationship between pharmacist and doctor is poor or where pharmacists lackconfidence about their knowledge level or skills.(5)
- Behaviour Our study did not investigate the actual behaviour of pharmacists, but did ask fortheir self-reported behaviour. Actual ADR reporting during the years 1995-2000 wasstudied previously.(4) Pharmacists’ own ideas about the number of reports wereoptimistic: they overestimated their actual reporting by a factor of almost three.One explanation for this discrepancy could be that there was confusion betweennumbers of reports and numbers of ADRs: an average pharmacist report containstwo ADRs. Almost all the pharmacists reported to Lareb, but some also sent a duplicate to themarketing authorisation holder. The reason for the high percentage of reports toLareb could be that Lareb is considered by pharmacists to be their organisation.Pharmacists’ high awareness of which ADRs should be considered to be seriousaccording to the CIOMS criteria is in line with the results of the earlier study of thequality of pharmacists’ reports.(4) We found no studies in the literature on thistopic relating to community pharmacists.
- Barriers Our survey did not reveal any major barriers preventing pharmacists fromreporting ADRs. The issues mentioned most frequently were considering reporting
108
too time-consuming and assuming that serious ADRs were known beforemarketing. Uncertainty about causality was also mentioned relatively frequently.Practical obstacles, such as the unavailability of forms or unfamiliarity with thereporting procedure, were not found to be significant factors. The same applied toconcerns about liability and possible lack of clinical expertise. Our analysis investigated whether experiencing barriers was related to reportingbehaviour and no such association was found. However, the number of barriersmentioned was small. It is striking that our findings strongly differ from results obtained among hospitalpharmacists in the UK in whom time required to report, insecurity about theirability to recognise possible adverse events, patient confidentiality and the absenceof electronic patient records were mentioned most frequently as barriers.(7,8) Asurvey among GPs revealed that, apart from considerations concerning the natureof the adverse reactions (too well known or too insignificant), the time factor anduncertainty about the causality between ADR and drug were seen as the mainobstacles to reporting.(9,10)Green et al. found that 70% of the community pharmacists in their study said theydid not report side effects of an OTC product they themselves had dispensed. Thiswas not confirmed in our survey: 84% of the respondents said they reported ADRsto OTC products. This is an important finding because pharmacists increasinglyplay a pivotal role in this context.(19)Uncertainty about the causality between a suspected ADR and the drug used ismentioned by both physicians and pharmacists as a barrier to the submission ofreports. This is perhaps unsurprising, and signifies a scientific way of thinking thatrequires certainty for action. However, it is unfortunate that this mind-set preventssome from reporting. After all, pharmacovigilance concerns the gathering of dataon suspected adverse events. It is the task of the national reporting centres to try toestablish the causality between the reported suspected ADRs and the drugs used byelimination of as many uncertainties as possible by means of causality assessmentand statistical methods.(20)
- Facilitating factors Feedback was mentioned most frequently as a factor that would facilitate reporting,both in response to the questionnaire items and as suggestions elicited by the open-ended question. This relates to specific feedback on reports submitted as well asgeneral feedback in terms of publications from the reporting centre. Surprisingly,feedback did not emerge as a facilitating factor in any of the earlier surveys ofcommunity pharmacists, hospital pharmacists or physicians. In the Netherlands,Lareb provides those who submit a report with customised feedback. Pharmacistsin the Netherlands appear to highly appreciate this and see it, together with Lareb’s
109
regular publications, as an important incentive to report. We therefore recommendthat this practice of providing report-related feedback should be more widelyadopted. Pharmacists in the UK predominantly mentioned education and training asimportant motivating factors.(6,7,8) Receiving a fee for reports submitted wasmentioned by just 18% of the Dutch respondents as an incentive, whereas in thestudy by Green et al6 one-third of the pharmacists mentioned financialcompensation. This seems to show that while in the Netherlands ADR reporting ismore generally perceived as inherent to pharmacists’ existing and usual professionalresponsibilities, in the UK it may be seen as a new and additional role. Hospitalpharmacists also indicated the presence of a ‘written hospital policy’ as a motivatingfactor.(7)
3.2.5 ConclusionCommunity pharmacists in the Netherlands were found to have a positive attitudeto ADR reporting. They considered reporting integral to their professionalresponsibilities and reported relatively frequently. Based on the findings available inthe literature, they appear to be ahead of their colleagues in other countries.
110
References
1. Olsson S. National Pharmacovigilance Systems, country profiles and overview. 2nd ed. WHOUppsala Monitoring Centre. Uppsala 1999.
2. Pharmacy ADR reporting now official. Pharm J 1997;258:582.
3. Koning GPH de. A regionalized spontaneous surveillance program for adverse drug reactionsas a tool to improve pharmacotherapy. Thesis. Utrecht University, 1994.
4. Grootheest AC van, Puijenbroek EP van, Jong-van de Berg LTW de. Contribution ofpharmacists to the reporting of adverse drug reactions. Pharmacoepidemiol Drug Saf2002;11:205-10.
5. Grootheest AC van, Puijenbroek EP van. Artsen en apothekers kennen Lareb - is dat zo?[Physicians and Pharmacists know Lareb – is that true?]. Pharm Weekbl 2000;135:489-91.
6. Green CF, Mottram DR, Raval D, Proudlove C, Randall C. Community pharmacists’ attitudeto adverse drug reaction reporting. Int J Pharm Pract 1999;7:92-9.
7. Sweis D, Wong ICK. A survey on factors that could affect adverse drug reaction reportingaccording to hospital pharmacists in Great Britain. Drug Saf 2000;2:165-72.
8. Green FG, Mottram DR, Rowe PH, Pirmohamed M. Attitudes and knowledge of hospitalpharmacists to adverse drug reaction reporting. Br J Clin Pharmacol 2001;51:81-6.
9. Belton KJ, Lewis SC, Payne S, Rawlings MD, Wood SM. Attitudinal survey of adverse drugreaction reporting by medical practitioners in the United Kingdom. Br J Clin Pharmacol1995;39:223-6.
10. Eland EA, Belton KJ, Grootheest AC van, Meiners AP, Rawlins MD, Stricker BHCh.Attitudinal survey of voluntary reporting of drug reactions. Br J Clin Pharmacol 1999;48:623-7.
11. Fishbein M, Azjen I. Belief, attitude, intention and behavior: an introduction to theory andresearch. Reading 1975.
12. CIOMS Working Group IV. Benefit-risk balance for marketing drugs: safety signals. CIOMS.Geneve 1998.
13. Vries CS de. Collaboration in healthcare, the tango to drug safety. Thesis. Groningen 1998.
14. Whittlesea CMC, Walker R. An adverse drug reaction reporting scheme for communitypharmacists. Int J Pharm Pract 1996;4:228-34.
15. Mill JWF van. Pharmaceutical Care, the future in pharmacy. Thesis: Groningen, 1999.
111
16. Emerson AE, Martin RM, Tomlin M, Mann RD. Prospective cohort study of adverse eventsmonitored by hospital pharmacists. Pharmacoepidemiol Drug Saf 2001;10:95-103.
17. Lareb/NVZA. Het melden van bijwerkingen, de rol van de ziekenhuisapotheker. Lareb. ’s-Hertogenbosch 2001.
18. Reebye RN, Avery AJ, Bosch WJHM van den, Aslam M, Nijholt A, Bij A van der. Exploringcommunity pharmacists’ perception of their professional relationship with physicians, inCanada and the Netherlands. Int J Pharm Pract 1999;7:149-58.
19. Sinclair HK, Bond CM, Hannaford PC. Pharmacovigilance of Over-the-Counter Productsbased in community pharmacy; a feasible option? Pharmacoepidemiol Drug Saf 1999;8;479-91.
20. Meyboom RHB. Causal or casual? The role of causality assessment in pharmacovigilance.Drug Saf 1997;16:374-89.
112
Chapter 3.3Contribution of pharmacists to the reporting ofadverse drug reactions
Pharmacoepidemiol Drug Saf 2002;11:205-10.
Kees van Grootheest MD1
Eugène.P. van Puijenbroek MD, PhD1
Lolkje.T.W. de Jong – van den Berg PharmD, PhD2
1. Netherlands Pharmacovigilance Centre Lareb, ’s-Hertogenbosch, the Netherlands.
2. Department of Social Pharmacy and Pharmacoepidemiology,GUIDE, Groningen, the Netherlands.
113
Abstract
AimAim of the study is to get a better view about the possible contribution of pharmacistsreports to the quantity and the quality of reports and in this way to the quality of avoluntary reporting system of adverse drug reactions.
Methods15,293 reports, send to the Netherlands Pharmacovigilance Centre, then namedNetherlands Pharmacovigilance Centre Lareb between 1995 and 2000 wereanalysed for the characteristics of pharmacist’s reports and the differences withreports of physicians, dispersion of adverse drug reaction in relation to the differentSystem and Organ Classes, the seriousness of the reports according to the CIOMS-criteria and the documentation grade of the reports.Two hundred reports were ad random selected and their quality assessed for thequality of the reports.
ResultsPharmacists are responsible for 40% of the reports sent in to Lareb during thisperiod. Their report more frequently concern adverse effects in relation to skin andthe eyes.The seriousness of pharmacist’s report is less as with physician’s reports as is the casewith the documentation grade of reports. Also the quality of the clinical informationof physician’s reports is higher.
ConclusionThe contribution of pharmacists in the voluntary reporting system in theNetherlands is of great importance, both for the number of reports and the qualityof reports.
114
3.3.1 IntroductionReports of suspected adverse drug reactions (ADRs) form the basis of the surveillanceof drugs after marketing. The occurrence of phocomelia in association withthalidomide in the 1960s brought an increasing awareness of the necessity to detectpossible but as yet unknown effects of marketed drugs at an early stage.A voluntary reporting system is an important tool in the detection of signalsindicating a possible relationship between an adverse drug reactions and a particulardrug.(1) A signal can be defined as a set of data constituting a hypothesis relevant tothe rational and safe use of a drug in humans.(2) It is inherent to a spontaneousreporting system that solid conclusions cannot be drawn.(3) To strengthen a signal, asufficient number of reports of suspected ADRs is required and these need to be welldocumented and of good quality. To confirm the suspicion raised by a spontaneousreporting system often analytical studies such as pharmacoepidemiological researchare needed.Regulatory bodies often cannot afford to wait for the results ofpharmacoepidemiological studies to become available.(4) For public health reasonsregulators have to make decisions as soon as the possible relationship between adrug and a serious ADR is sufficiently strong. Due to today’s rapid disseminationof information via the media and the Internet public concern is easily raised,increasing the demand for decisions at an early stage. This has created an urgentneed for reliable information and clear decisions.(5) Since decisions may affect theconditions of registration, the content of the Summary of Product Characteristics(SPC), and may possibly even result in the withdrawal of the product concerned, itis vital that the methodology and results of a reporting system meet the higheststandards. Meyboom has postulated standards reporting systems need tomaintain.(6) These standards not only pertain to the number and quality of reports,but also to the care paid to and the accuracy of the collection process and analysisof the reports received.In a number of countries the pharmacist plays an important role in the reporting ofsuspected ADRs. This is also the case in The Netherlands, where pharmacists havethe possibility to derive crucial information about their clients’ medication historiesfrom the data stored in their computer system. Patients in The Netherlands have ingeneral only one pharmacist where they obtain their medicaments.The Netherlands Pharmacovigilance Centre Lareb maintains a voluntary ADRreporting system for physicians and pharmacists in the Netherlands since 1984 andwas officially appointed as the national reporting centre in 1995.(7) Lareb is fundedby and reports to the Dutch Medicines Evaluation Board. Since its establishment,pharmacists have played an important role in the Lareb pharmacovigilance system,both as reporters and as intermediaries in promoting physicians to participate.Given their substantial role in the reporting and collection of ADRs in the
115
Netherlands, and because in a number of countries pharmacists have also expresseda growing interest in voluntary reporting systems, we have studied the significanceof pharmacists’ reports to Lareb during the period between 1995 and 1999. The aimof the study was to gain a deeper insight into the contribution their reports maketo both the quantity and the quality of the reports and thus into the quality of avoluntary reporting system.
3.3.2 MethodsVarious characteristics of the pharmacists’ reports in the Lareb database betweenJanuary 1, 1995 and January 1, 2000 were analysed and compared with those of thereports originating from physicians. The following characteristics were studied: thedistribution of the ADRs in relation to the different organ systems, the seriousnessof the ADRs reported, and the quality of the reports. In addition to objective
116
Figure 1Grading scheme for the quality of documentation
information about these characteristics, a subjective analysis was conducted inorder to get a more detailed picture of the quality of the information about thesuspected ADR provided in the report.To analyse the distribution of reports in relation to the different organ systems inthe Lareb database, ADRs were first coded according to the WHO AdverseReaction Terminology (WHO-ART).(8) For each report the suspected drug ordrugs were assessed and each ADR was coded with a so-called WHO-preferredterm. Subsequently, each preferred term was attributed to a specific System andOrgan Class (SOC), i.e. a group of preferred terms pertaining to the same organsystem. In order to determine the SOC distribution differences in the reports ofpharmacists and physicians, odds ratios (OR) were calculated for the differentSOCs with corresponding 95% confidence intervals. The odds ratio is defined asthe odds of the number of reports on a specific SOC by pharmacists as comparedto physicians, divided by the odds of the number of all other SOCs reported bypharmacists as compared to physicians. The OR was adjusted for age, gender andyear of reporting. Criteria formulated by the Council for International Organizations of MedicalSciences (CIOMS) were used in order to rate the seriousness of the reports. Thesecriteria were first published in the 1995 Guideline on expedited reporting of ADRsof the International Conference on Harmonization of Technical Requirements forRegistration of Pharmaceuticals for Human Use (ICH) and were subsequentlyadopted by Working Group IV of the CIOMS.(9) The criteria for a serious reportare: death, life threatening, hospitalisation or prolongation of hospitalisation,persistent or significant disability/incapacity and a congenital anomaly/birth defect. In order to assess the quality, we compared reports submitted by pharmacists tothose sent in by doctors using two different methods. Firstly, an automated analysiswas carried out of all reports received during the period under investigation bymeans of the documentation grading scheme as developed by the WHO - seeFigure 1.(10) This so-called documentation grade gives an indication of the qualityof the information provided. However, it does not allow a subjective judgement ofthe information, nor does it take into account any additional information the reportmay contain.Therefore, to evaluate the quality of the reports in a wider perspective, a secondanalysis was carried out. Two hundred reports were additionally judged withrespect to completeness of information and quality of the clinical information. Thereports were blinded for source (physician or pharmacist) and randomly selectedfrom the database. Completeness of information was subjectively scored for sixaspects, each of which was awarded one point (1 means good, 0 means insufficient).The aspects assessed included: basic information about the patient (age and gender),date of onset of the ADR, information about the drug and concomitant medication,
117
118
Table 1Differences in System Organ Classes for pharmacists and physicians
System and Organ Class Odds ratio Number of reported (95% CI) ADRs
skin and appendages disorders 0.8 (0.7-0.9) 3385musculo-skeletal system disorders 0.9 (0.7-1.0) 893collagen disorders 2.4 (0.9-6.0) 25central & peripheral nervous system disorders 1.0 (0.9-1.0) 3227autonomic nervous system disorders 1.0 (0.7-1.5) 93vision disorders 0.6 (0.5-0.7) 735hearing and vestibular disorders 0.8 (0.6-1.0) 171special senses, other disorders 0.5 (0.4-0.7) 404psychiatric disorders 1.8 (1.6-1.9) 2925gastro-intestinal system disorders 0.9 (0.9-1.0) 4069livers and biliary system disorders 5.0 (3.6-7.0) 307metabolic and nutritional disorders 0.9 (0.7-1.2) 261endocrine disorders 1.6 (1.1-2.5) 104cardiovascular disorders, general 1.3 (0.9-1.7) 175myo-, endo-, pericardial & valve disorders 4.1 (1.8-9.1) 46heart rate and rhythm disorders 1.2 (1.0-1.5) 515vascular (extracardiac) disorders 0.9 (0.7-1.2) 229respiratory system disorders 0.8 (0.7-0.9) 871red blood cell disorders 2.2 (1.0-4.6) 36white cell and res disorders 5.7 (3.0-11.1) 87platelet, bleeding & clotting disorders 0.8 (0.6-0.9) 407urinary system disorders 0.8 (0.7-1.0) 322reproductive disorders, male 2.2 (1.6-3.1) 192reproductive disorders, female 1.0 (0.8-1.2) 450foetal disorders 4.3 (1.3-14.4) 23neonatal and infancy disorders 2.5 (0.8-7.7) 17neoplasms 1.2 (0.4-4.3) 11body as a whole-general disorders 1.0 (0.9-1.1) 2645application site disorders 1.2 (0.9-1.7) 186resistance mechanism diorders 0.6 (0.3-1.0) 50secondary terms-events 0.6 (0.2-1.5) 18
95%CI: 95% confidence intervall
information about the period the suspected drug was used and the outcome. Thequality of the clinical information and the quality of the follow-up information wasjudged using a Visual Analogue Scale ranging from 1 to 5. The first 30 reports,selected at random, were rated by four experienced assessors. Differences betweenthese assessors were determined using Cronbach’s alpha. Since no significantdifferences were found, the other 170 reports were assessed by the first author.
3.3.3 ResultsBetween January 1995 and January 2000 Lareb received 15,293 reports covering25,183 ADRs. About 40% of the reports were sent in by pharmacists with themajority of reports submitted by community pharmacists; the contribution ofhospital pharmacists was less than 1%. The differences in system organ classes for which ADRs were reported are depictedin Table 1. Compared to pharmacists, physicians reported statistically significantlymore ADRs related to the cardiovascular system, malfunctions of the liver andpsychiatric disorders, whereas pharmacists reported a significant greater number ofpresumed ADRs of ‘external’ organ systems such as disorders of the skin and eyes. The seriousness ratings of the reports are shown in Figure 2. The percentage ofreports that was coded as serious was twice as high for physicians as it was forpharmacists. The number of serious reports submitted by physicians increasedmore during the period investigated than that of pharmacists. As regards the quality of documentation we found that for both groups the proportionof reports providing more adequate documentation had gradually risen. However, thiseffect was more pronounced for the physicians’ reports, of which about 60% receiveda grade 2 or higher, than for the reports submitted by the pharmacists, of which lessthan 40% were graded as such. The documentation of hospital specialists was of ahigher quality than that of general practitioners (see Table 2)The subjective quality assessment of the 200 investigated reports did not reveal astatistically significant difference regarding the completeness of the informationprovided by pharmacists and physicians (5.39 and 5.35, respectively; p > 0.05).However, for the quality of the clinical information we did find a significantdifference (pharmacists: 3.24, physicians: 3.85; p < 0.001).
3.3.4 DiscussionThe findings of the present study indicate that the contribution pharmacists maketo the voluntary ADR reporting system in the Netherlands is considerable, both interms of quantity and quality of the reports.Our study clearly showed that the pharmacists’ share in the number of reports onADRs submitted to the spontaneous reporting system is substantial. In his thesisDe Koning already reported on their sizeable contribution to Lareb.(11)
119
In the period covered by this study roughly 40% of the reports received annuallyoriginated from pharmacists.In contrast to the Netherlands, in the United Kingdom the number of reportssubmitted by pharmacists is low. Green et al. described the first experiences withreporting by community pharmacists in the UK.(12) Although 93% of the
120
Figure 2Grades of documentation quality of pharmacists, general practitioners and consultants.
Table 2Percentages of serious reports from pharmacists and physicians
Year of Number of serious reports Number of serious reports Odds ratioreporting by physicians by pharmacists (95% CI)
Differences between serious and non-serious reports by physicians and pharmacists:Odds ratio is defined as the odds among the serious cases divided by the odds of thenon-serious cases. 95%CI: 95% confidence interval.
pharmacists indicated to have been aware of the fact that they could report, onlyfew actually did. They were also found to be aware of the importance of reportingADRs and the significant role they could play in their reporting. Green andcolleagues concluded that more research into which factors induce and whichinhibit pharmacists to report is needed.In the United States Syed Rizwanuddin Ahmad et al studied the contribution ofpharmacists to the serious reports received by the FDA.(13) From all seriousreports from health professionals 68% originated from pharmacists. Theyconcluded that the quality of the reports by pharmacists and physicians was equal.The criteria on which the quality assessment was based consisted of, among otheraspects, the presence of a good description of the side effects, medical history,relevant laboratory results and, if possible, a report of a biopsy or autopsy.Physicians reported death resulting from an ADR more frequently. Pharmacistsreported 95% of the hospital admissions due to an adverse drug reaction. It needsto be noted that the majority (85%) of reports submitted to the FDA stem frompharmaceutical companies. This is due to the fact that the sector is obliged by lawto forward all the information it receives from health professionals, which, in theAmerican situation, are predominately physicians. The serious reports the FDAreceives from pharmacists are in general reports from hospital pharmacists. This ismainly accounted for by the fact that also hospitals in the USA are obliged tomaintain a reporting system for ADRs. Sometimes the validity of pharmacists’ reporting is questioned because they cannotprovide clinical information. To compensate for this lack, in the UK a pharmacistcan only report after consultation of the physician treating the patient.(12) In theNetherlands such consultation is not compulsory. Hospital pharmacists, however,are in a good position to include the necessary clinical information in their reports.Since in the Netherlands hospital pharmacists are increasingly actively involved inthe integrated treatment of patients, this will better enable them to submit well-documented reports of suspected ADRs.In the present study we investigated multiple parameters to ensure that we obtainedan accurate picture of the quality of the reports sent in by pharmacists in theNetherlands. The number of ADRs specified per report was not significantlydifferent for pharmacists and doctors. In this context it needs to be noted that a highnumber of adverse reactions per report may indicate that, rather than cleardiagnoses related to ADRs, symptoms are being reported. To assess the seriousness of the reports, we analysed the number of reports rated asserious in concordance with the CIOMS criteria. We found the share of seriousreports from physicians to be twice as high as those from pharmacists. This is notsurprising since the former are more likely to encounter a serious ADR in theircapacity as medical doctors.
121
Regarding the dispersion of reports in relation to the different organ systems, wefound that pharmacists report relatively more on eye and skin diseases and othermore common complaints. This can be explained by the fact that since thesedisorders are more likely to be observed by the patients themselves and they tendto prefer to discuss these effects with a pharmacist. Moreover, such symptoms canbe more easily attributed to the involved organ system. For more seriouscomplaints, however, patients will prefer a medical consultation. Although the quality assessment of 200 randomly selected reports did show a small,though not statistically significant difference in documentation grades (i.e. moredoctors’ reports received a higher grade), overall the completeness of the reportsand the quality of the information was similar for the two professional groups.Pharmacists take up a special position in the reporting of suspected adversereactions of over-the-counter products and especially alternative medicines.Hannaford et al. found that pharmacists are motivated for this role.(14) Theseaspects were not investigated in this study, since the Lareb database contains littleinformation about over-the-counter products and alternative medicines such asherbal products. Research into this aspect of the role of pharmacists in theNetherlands is recommended.
3.3.5 ConclusionOur analysis of the reports the Lareb Centre received between 1995 and 2000revealed that the contribution of pharmacists to the Dutch spontaneous reportingsystem is substantial. Despite the finding that the quality of their reports was, ingeneral, slightly lower than that of those sent in by physicians, as was their share inthe number of serious reports, apart from their considerable quantitativecontribution, pharmacists also provided information that was complementary tothe physicians’ reports. The present findings based on the experiences in the Netherlands show thatpharmacists can indeed play an important role in the reporting of adverse drugreactions.
122
References 1. Edwards IR, Lindquist M, Wiholm BE, Napke E. Quality criteria for early signals of possible
adverse drug reactions. Lancet 1990;336:156-8.
2. Meyboom RH, Egberts AC, Edward IR, Hekster YA, Koning FH de, Gribnau FW. Principlesof signal detection in pharmacovigilance. Drug Saf 1997;16:355-65.
3. Abenhaim L, Moore N, Bégaud B. The role of pharmacoepidemiology in pharmacovigilance.Pharmacoepidemiol Drug Saf 1999;8:S1-7.
4. Rawlin MD. The challenge to pharmacoepidemiology. Pharmacoepidemiol Drug Saf 1995;4:5-9.
5. Effective communications in pharmacovigilance, the Erice report. WHO Uppsala MonitoringCentre. 1998.
6. Meyboom RHB. Good practice in the postmarketing surveillance of medicines. PharmacyWorld Science 1997;19:186-90.
7. Broekmans AW, Lekkerkerker JFF, Koning GHP de, Vree PH. Nieuwe regels voor het meldenvan bijwerkingen na 1995. Ned Tijdschr Geneeskd 1996;140:1166-7.
8. Anonymous. WHO Adverse Drug Reaction Dictionary. WHO Centre for International DrugMonitoring, Uppsala, 1995.
9. CIOMS Working Group IV. Benefit-Risk Balance for Marketing Drugs: Safety Signals.CIOMS, Geneva, 1998.
10. WHO Adverse Reaction Database users’ manual. Uppsala Monitoring Centre. 1996.
11. Koning GPH de. A regionalized spontaneous surveillance program for adverse drug reactionsas a tool to improve pharmacotherapy. Thesis. Utrecht University, 1994.
12. Green CG, Mottram DR, Raval D, Proudlove C, Randall C. Community pharmacists’attitudes to adverse drug reaction reporting. Int J Pharm Pract 1999;7:92-9.
13. Ahmad SR, Freiman JP, Graham DJ, Nelson RC. Quality of adverse drug experience reportssubmitted by pharmacists and physicians to the FDA. Pharmacoepidemiol Drug Saf 1996;5:1-7.
14. Hannaford PC, Bond CM, Sinclair HK. Supporting the safe use of over-the counter medicinesin the UK – a pilot pharmacovigilance study of OTC ibuprofen. Pharmacoepidemiol Drug Saf2000;9:S73.
123
Chapter 3.4Thromboembolism associated with the new contraceptive Yasmin®
BMJ 2003;326:257.
Kees van Grootheest, MDTom Vrieling, PharmD
Netherlands Pharmacovigilance Centre Lareb,’s-Hertogenbosch, the Netherlands.
125
3.4.1 CasesThe Netherlands Pharmacovigilance Centre Lareb, the Dutch spontaneousreporting system for adverse drug reactions, recently received five reports ofthromboembolism as a suspected adverse drug reaction to the new oralcontraceptive ethinylestradiol and drospirenone (Yasmin®)
A 17 year-old woman suddenly collapsed and died after taking the contraceptiveethinylestradiol with drospirenone for a period of six months. Autopsy showed thatshe had a massive pulmonary embolism. No obvious risk factors forthromboembolism, such as smoking, period of long immobilisation, air flights, orconcomitant medication, were evident.(1) Because she died suddenly no bloodsample was taken. Blood taken from her parents did not test positive for any of theknown risk factors: concentrations of proteïne C and antithrombin III were normal.The activated partial thromboplastin time (APTT) and partial thromboplastin time(PTT) were normal, and the existence of factor V Leiden mutation was excluded.
A 28 year old woman changed her oral contraceptive from ethinylestradiol withdesogestrel (Marvelon®) to ethinylestradiol with drospirenone. Four months latershe had thrombosis in one leg and was treated with acenocoumarol. Risk factors orconcomitant drugs were unknown.
Another patient, a 45 year old woman, had deep vein thrombosis in one leg aftertaking ethinylestradiol with drospirenone for two month, as did a 50 year oldwoman who took the contraceptive for three months.
A 35 year old woman had pulmonary thrombosis 17 days after she started takingthe contraceptive. She had given birth four months earlier.
3.4.2 DiscussionEthinylestradiol with drospirenone has been approved as an oral contraceptive inall European Union countries since 2000 and has recently been launched in theUnited Kingdom.(2) The public assessment rapport of the contraceptive gives onlyone suspected case of pulmonary embolism but also says that the number of casesin the preregistration studies are too low for a reliable conclusion on this matter.(3) The risk of thromboembolism for women using the third generation (combined)pill has long been debated. Physicians therefore may prefer a new type of combinedpill, like ethinylestradiol with drospirenone, assuming that these are safer.However, an association of these drugs with a lower risk of thromboembolism hadnot been proved by research.
127
3.4.3 ConclusionOur cases show that also newer contraceptive pills may have a risk ofthromboembolism. At present, insufficient data on the superiority ofethinylestradiol with drospirenone are available.Reporting of adverse drug reactions is important in order to get an insight in thesekind of events.
128
References
1. Winkler UH. Oral contraception in woman at risk of venous disease. Gynaecology Forum2001;6:23-8.
2. Sheldon T. Dutch GPs warned against new contraceptive pill. BMJ 2002;324:869.
3. Official site of the Dutch Medicines Evaluation Board. www.cbg.-meb.nl/nl/docs/gnsmiddl/par-yasmin.pdf (accessed 21 October 2002).
129
4Improvingpharmacovigilance
Chapter 4.1Intensive monitoring of new drugsbased on first delivery signals from pharmacists: a pilot study
Pharmacoepidemiol Drug Saf 2003;12:475-81.
Kees van Grootheest, MD1
Arjen Groote, PharmD2
Lolkje T.W. de Jong-van den Berg, PharmD, PhD2
1. Netherlands Pharmacovigilance Centre Lareb,’s-Hertogenbosch, the Netherlands.
2. Department of Social Pharmacy and Pharmacoepidemiology, GUIDE, Groningen, the Netherlands
133
Abstract
Intensive monitoring can be a valuable tool in the early detection of adverse drugreactions, especially of new drugs. Aim of this pilot study was to investigate thepractical possibilities of a system of intensive monitoring, using the pharmacycomputer system to detect the first dispensing of a new drug.
MethodsEight pharmacists were asked to monitor, using their computer system, when ageneral practitioner prescribed the target drug (rofecoxib). The pharmacists werealso requested to provide the researchers at Lareb with an overview of the patient’smedication history. Subsequently, the pharmacist sent the prescribing physician anenvelope containing information about the project and a reporting form (allprovided by Lareb), which the GP was requested to return to Lareb after the nextvisit of the patient. The items on the questionnaire concerned characteristics of thepatient (anonymous), indication, dose and information about possible adverse drugreactions.
ResultsDuring a four-week period the participating pharmacists signalled 44 firstprescriptions of rofecoxib. For each of these signals the pharmacist provided Larebwith the medication history of the patient involved. Of the prescribing GPs who hadbeen sent the report form 70,5% (n=31) returned the form. Twenty-one of the 31forms were returned within four weeks. The medication histories showed that in 43of the 44 cases the dispensing of the target drug was indeed the first delivery.The participating pharmacists and GPs were also sent an evaluation form. Allpharmacists returned their evaluations, indicating an overall motivation toparticipate in the proposed system. In total seven GPs returned their evaluationforms, three of whom had not reported adverse drug events to the nationalspontaneous reporting centre before.
ConclusionAlthough the number of participants in this trial was small, we conclude thatpharmacists and prescribing physicians are able and willing to contribute to anintensive monitoring system for new drugs.
134
4.1.1 IntroductionOnce a drug has been approved for marketing, the use of the drug attains thecharacter of research in daily practice.(1) The facts about the drug that are knownat that stage are limited in that they are based on research of a restricted population,a sample, moreover, that differs from the general population that will be using thenew drug. This emphasises the importance of close and careful monitoring of thedrug immediately following its introduction and the need for any unwanted adverseevents to be detected at the earliest possible stage. Pharmacovigilance is the sciencededicated to this monitoring process. Drugs monitoring is predominantly based onreports of suspected adverse drug reactions from medical doctors (GPs) andpharmacists, the so-called spontaneous reporting system (SRS), for which purposemost countries have established national reporting centres.(2) The number ofreports submitted during the initial period following the introduction of a new drugis reflected by a distinctive curve, first described by Weber and later adapted byothers(3,4,5). This curve is characterised by a slow rise, reaching its peak near theend of the second year, followed by a slow, gradual drop to a lower, more or lessconstant decreasing value. This implies that in the early stages after a drug has beenreleased little information is available from clinical practice. However, it is essentialthat any negative effects of new drugs are identified as quickly as possible in orderto prevent harm to patients. This has become all the more crucial since increasinglynew drugs are developed that have a powerful impact on the human physiology.Moreover, the registration procedure for drugs targeting illnesses for which noadequate therapy is available has recently been shortened.In this chapter we describe a pilot study in which we tested a detection methodspecifically aimed at this first stage after the introduction of a drug that will allowus to obtain an expedited first impression of possible unknown adverse events. Themethod involves Intensive Monitoring, and makes use of the data pharmacistscollect regarding the first prescription and dispensing of a newly approved drug.Intensive Monitoring is a prospective observation-based cohort study investigatinga specifically selected (new) drug.(6,7) New Zealand has the most comprehensiveset of data on the practical implementation of the method because in this countryan Intensive Medicines Monitoring Programme (IMMP) supplementing thespontaneous reporting system has been operational since 1977. The IMMP is aconstituent component of the Dunedin-based Centre for Adverse ReactionMonitoring (CARM), which independent organisation runs the SRS on behalf ofthe New-Zealand Department of Public Health.(6,8) The IMMS makes use of apermanent cohort of approximately 10,000 drug users. The prescription data arederived from the prescriptions dispensing pharmacists and hospital pharmacistsreceive and report. Within two months the IMMS sends the prescriber aquestionnaire.
135
In the United Kingdom another form of Intensive Monitoring, the so-calledPrescription Event Monitoring (PEM) has been in existence since 1980.(9,10) Thissystem makes use of the prescriptions clinicians submit to the Prescription PricingAuthority. This allows the Drug Safety Research Unit (DSRU) to collect cohorts of20 to 30,000 prescriptions of the drugs under investigation and it sends theprescribing physicians questionnaires, so-called green forms, three to twelvemonths after the date of the first prescription. The Southampton-based DSRU is anindependent organisation founded to complement the SRS.(11)Both in New Zealand and in the United Kingdom there is an interval of severalmonths between the moment the monitoring of a drug is has started until themoment the first data of the Intensive Monitoring become available. We have triedto devise a fast method that would cause the pharmacist, the prescribing clinicianand the national reporting system as little inconvenience as possible. The aim of thepresent pilot study was to explore the possibility to expedite this process by makinguse of the first delivery signals from pharmacies allowing the moment when data onnewly released drugs become available to be brought forward.
4.1.2 MethodFor the duration of one month in the spring of 2001 seven pharmacists, of whomone was associated with two separate pharmacies, were requested to signal when apatient was prescribed rofecoxib, the drug selected for this pilot study, for the firsttime. Two weeks after delivery of the drug the pharmacist sent the prescribing
136
Figure 1Organogram of the flow of information
general practitioner (GP) a questionnaire. In addition, he or she sent theNetherlands Pharmacovigilance Centre Lareb, the Dutch spontaneous reportingcentre, an anonymous overview of the medication history of the patient involved.Together with the questionnaire the GP received written instructions and wasrequested to forward the completed form to Lareb. The information flow betweenthe three parties is depicted in Figure 1. The pharmacists were all participants in a project analysing pharmacy dataconducted by the department of Social Pharmacy and Pharmacoepidemiology ofthe Groningen University in the Netherlands. The pharmacies’ computer systemsautomatically generated the signal indicating a first delivery. This pilot study exclusively monitored prescriptions written out by GPs. Thequestionnaires the GPs received were perforated allowing the details of the patientsto be removed before the form was submitted to Lareb. The form the GPs wereasked to return consisted of a slightly moderated version of the standardised formin use at Lareb in that it did not include the medication history since thisinformation was already provided by the participating pharmacists. Thequestionnaire was marked with the same code as the medication history. Toguarantee that the researchers were blind to the identity of the GPs, the returnenvelopes were opened by secretarial staff that provided the form with a separatecode.The pharmacists and GPs made use of standard return envelopes, which ensuredthat at Lareb the forms submitted were processed according to the usual procedurefor reports on ADRs.Since with this pilot study we intended to test a potential method for intensivemonitoring and not the drug, the choice of drug was of minor importance. Weopted for rofecoxib, which drug had been released on the Dutch market six monthsprior to the trial. It was deemed suitable for this trial because it was a new drug thatwas being prescribed regularly, also by GPs. At the time of the study rofecoxib wassolely indicated for symptomatic treatment of arthrosis. After conclusion of the trial Lareb requested the participating pharmacists and GPsto fill in an evaluation form.
4.1.3 ResultsIn total Lareb received 44 medication histories from the eight pharmacies (sevenpharmacists) participating in the trial. The GPs returned a total of 31 report forms,which implies that 70.5% of the forms the pharmacists forwarded to the GPs weresubmitted to Lareb. All the forms had been completed legibly and in full. Oninquiry it appeared that in three instances in which the GP had prescribed rofecoxibfor the first time, the pharmacist had not included the case in the trial. One case wasnot included because the prescriber and patient were one and the same person and
137
in the two other cases the pharmacist involved had mistakenly omitted inclusion. In 19 of the 31 submitted reports the GP had seen the patient again and in 2 casesan adverse event was reported, both relating to gastric complaints. In one case thepatient involved had been prescribed rofecoxib before. Since we were interested in finding out whether it was possible to speed up the datacollection process of newly marketed drugs, we compared the date the selecteddrug was prescribed with the date the report forms were received by Lareb. Withthe exception of one report all forms had been submitted within six weeks after thedrug had been dispensed. Although outside the scope of this trial, the medication histories and report formsLareb received did provide some insight into the prescription behaviour and use ofrofecoxib (e.g. the patients’ age and gender and dose prescribed) in the clinicalpractice. From the 44 medication histories it was derived that, apart form one case,the recommended initial dose for elderly patients (12,5 mg) was not adhered to anda dose of 25 mg had been prescribed in 43 cases. The 31 forms returned by the GPs,however, showed that 16 of the 31 patients had been above the age of 60. Thisdiscrepancy might be explained by the fact that health insurance companies in theNetherlands only provide full coverage for a 25-mg dose. Moreover, in the case ofa first delivery, compensation is restricted to a maximum of 15 days, which held for37 of the 44 prescriptions. Eleven of the 31 forms stated arthrosis as the indication. All participating pharmacists completed the evaluation form. The most frequentremarks made concerned practical matters such as the return envelopes – the twoseparate envelopes for the prescribing GP and Lareb – which were too much alike. In all cases pharmacists and GPs had been in contact to discuss the trial. Twopharmacists had reservations about cooperating in the proposed method ofIntensive Monitoring on a long-term basis. For one pharmacist this was due topractical reasons (discontinuation of his association with the pharmacy), and thesecond pharmacist indicated not to be able to provide an unequivocal response.Two pharmacists expressed their doubts as to whether GPs would be prepared tomake a long-term commitment to the proposed system. The GPs were requested to return their evaluation forms via their pharmacist toprevent their identity from becoming known to the researchers. In total Larebreceived seven completed forms. A remarkable finding was that three of theseoriginated from GPs who had not reported adverse drug events to the nationalreporting centre Lareb before. Six GPs recognised the potential of the proposeddrug monitoring system. One GP had reservations and mentioned time requiredfor the method and lack of financial compensation as prohibitive.
138
4.1.4 Discussion
Cooperation of pharmacists and physiciansThe main outcome of this pilot study is that a system of Intensive Monitoring isfeasible, allowing information about the effects of newly released drugs in dailypractice to become available at an early stage. Pharmacists and GPs are willing andhave the capability to cooperate in such a system. The pharmacist has a pivotal rolein the proposed system, both with respect to signalling a drug’s first delivery andsubmission of the medication history to the national spontaneous reporting system,as well as forwarding the report questionnaire to the prescribing GP. The eightpharmacies participating in this trial used three different computer systems. Allthree systems proved to have the facility to generate a first delivery signal. In oneinstance only, this function could be linked to an electronic agenda, which couldautomatically generate a reminder indicating the date for the GP forms to be sentout. Although the number of participants in this pilot study was limited, it can beconcluded that the contribution and cooperation of the GPs and pharmacists wasquite satisfactory. It needs to be noted that the pharmacists involved were allexperienced in participating in scientific research. An earlier study found that,overall, pharmacists in the Netherlands are motivated to play an active role inpharmacovigilance.(12)If the number of pharmacists and clinicians were to be extended, apart from earlydetection of adverse drug reactions, the system would also lend itself for moreelaborate research on drug-related aspects. Thus, insight may be gained regardingthe market penetration of a new drug, the indication for which it is prescribed anduser characteristics such as age and gender. In addition, because the system providesdata on both the user population and the use of the drug, Intensive Monitoring is,in principle, also suitable for quantitative analyses.This pilot study investigated the use of the system in primary health care. It is alsofeasible for dispensing pharmacists to generate first deliveries prescribed byspecialists in a similar fashion. Patients that have been admitted to hospital get theirmedication from the hospital’s in-house pharmacy. The response is likely to belower since it is known that, compared to GPs, medical specialists are less willingto cooperate in a reporting system. (13) Examples of Intensive Monitoring in aclinical setting have been described earlier, for instance in the USA.(14)
Comparison with existing Intensive Monitoring systemsThe system proposed in the present study distinguishes itself from the methods ofIntensive Monitoring operative in New Zealand and the United Kingdom withrespect to several aspects. Firstly, the system we tested makes information about a newly introduced drug
139
available more quickly. Figure 2 shows schematic the different curves of number ofreports related to time. All three systems have a period of time between theintroduction of a drug and the decision to start the Intensive Monitoring. When this decision is made, in our system there is only a short time needed toinform pharmacists to provide the first delivery signal and to send the reportingform to the prescribing physician. The existing systems need more time to get thewanted information. Of course there need to be a sufficient number of prescriptionof the drug under investigation in order to get enough reports, however in ouropinion the quality of the reports adds more the outcome of reporting systems asthe number of reports does.(15)Secondly, the method with which the data are collected is considerably lesscomplicated and more cost-effective than its counterparts in New Zealand and the
140
Figure 2 Schematic curves of number of reports in relation to time for different ADRreporting systems
PBIM: Pharmacy-based Intensive MonitoringTIM: Traditional Intensive MonitoringSPR: Spontaneous Reporting Systems
aant
al m
eldi
ngen
tijd
UK since the proposed reporting system closely resembles the reporting methodspharmacists and GPs are already familiar with. There is no need for a separateadministrative system to collect the prescriptions and to receive the wantedinformation from the prescribing physician.The burden on the pharmacist is higher than in the two existing systems and lesstaxing for the GP because a number of details can be derived from the medicationhistory that is provided by the pharmacist. However, this additional task it notlikely to be prohibitive since pharmacists in the Netherlands generally alreadyregard reporting as an integral part of their task in providing pharmaceutical care. In terms of efficiency, the national pharmacovigilance centre has much to gain fromthis system. The spontaneous reporting system receives these reports much likeother reports and can include them in the standard processing procedure by simplylabelling the reports as originating from Intensive Monitoring. There is onedrawback in that all first deliveries need to be recorded, whereas only a smallpercentage will lead to the GP reporting an adverse reaction. This implies that thecapacity of the reporting system will possibly need to be expanded, although anautomated data exchange will keep this to a minimum. A noteworthy detail in this context is that Intensive Monitoring has predominantlyreceived the attention of pharmacovigilance centres that work independently fromthe approval authorities. This applies to both New Zealand and the UnitedKingdom as well as to the Netherlands Pharmacovigilance Centre Lareb.
Possible future developmentsLarge-scale application of the presented system appears possible. The Netherlandshas 1200 pharmacies and with ten first deliveries of a drug under investigation theburden will be limited while at the same time data about well over 10,000 deliveriescan be obtained. Nevertheless, a comprehensive implementation of such a systemwill have its limitations. Whereas pharmacists appear to be motivated to contribute to Intensive Monitoring,whether this will also hold for GPs and other clinicians when the system is appliedon a national scale is uncertain. In general, the existing spontaneous reportingsystems depend on a select, motivated group of physicians; many practisingclinicians do not contribute to the system.(11) Our trial was restricted to GPs andearlier experiences in research involving medical specialists did not look promising.Their reluctance to participate may lie in the fact that a monitoring system requirestheir personal cooperation whereas in the case of pharmacists use can be made ofthe pharmacy’s computer system and infrastructure. Further development of the proposed method and integration of the computersystems of pharmacies and GP surgeries – steps towards which are currently beingundertaken in the Netherlands – will facilitate the electronic exchange and
141
processing of the various data thereby considerably reducing the burden topharmacists and doctors as well as the national reporting system. In this way theGP merely needs to report the suspected adverse event and the subsequentadditional information required will be automatically provided, matched andtransferred.
Additional remarksPost Marketing Surveillance is especially needed to detect type B adverse drugreactions and in a lesser extend type A reactions.(16) Type B reactions have asuggestive time relationship, but will not always be detected in the few weeksbetween the prescription and the moment the prescribing physician fill in thereporting form. In the present trial the prescribing physicians were only asked tofill in a form once, which they returned to Lareb within four weeks. This speed isessential for a system aimed at a prompt detection of signals of as yet unknownadverse drug reactions. The system may be extended by sending out a second formafter for instance three months, thus allowing information about drug reactions tobe gathered in the longer term.In our system the pharmacovigilance centre receives all the information needed,also the concomitant medication. This gives also the possibility to detectinteractions.An important positive side effect of implementation of the proposed systemdeserves special mention. Application of the method will actively involve doctorsand pharmacists in the much-needed process of pharmacovigilance. Of the sevenGPs who submitted their evaluation to Lareb three had not reported an adversereaction before. In other countries findings also indicate that Intensive Monitoringmay induce spontaneous reporting of suspected adverse reactions to drugs.
4.1.5 ConclusionIt is vital that after introduction of a drug information about possible associatedadverse effects can be obtained as soon as possible. The existing monitoringmethods are not designed for this purpose. The method for Intensive Monitoringproposed in this article, which makes use of the first delivery signals frompharmacists, was designed to fill this gap and a first, tentative trial found it to be afast and efficient approach. Both pharmacists and GPs willingly cooperated andproved to be able to contribute actively in this new system facilitating the intensivemonitoring of new drugs.
AcknowledgementWe want to thank Dr. M.D.B. Stephens for his valuable comments
142
References
1. Porta M, Hartzema AG, Tilson HH. The contribution of epidemiology to the study of druguses and effects. In: Pharmacoepidemiology – an introduction (3e ed). Hartzema AG, Porta M, Tildon HH (editors). Harvey Whitney Books Company, Cincinnati 1998.
2. Olsson S. National Pharmacovigilance Systems, country profiles and overview. 2nd ed. WHOUppsala Monitoring Centre. Uppsala 1999.
3. Weber JCP. Epidemiology of adverse reactions to non-steroidal antiinflammatory drugs.In:Adv in Inflam Res. Rainsford KD, Velo GP (eds), Raven Press, 1984;6:1-7.
4. Haramburu F, Bégaud B, Moride Y. Temporal trends in spontaneous reporting of unlabelledadverse drug reactiorns. br J Clin Pharmacol 1997;44:299-301.
5. Wallenstein EJ, Fife D. Temporal Patterns of NSAID Spontaneous Adverse Event Reports, theWeber Effect Revisited. Drug Saf 2001;24:233-7.
6. Coulter DM. The New Zealand Intensive Medicines Monitoring Programme.Pharmacoepidemiol Drug Saf 1998;7:79-90.
7. Mann RD, Wilton LV, Pearce GL, Mackay FJ, Dunn NR. Prescription-Event Monitoring in1996 – a method of Non-Interventional Observational Cohort Pharmacovigilance.Pharmacoepidemiol Drug Saf 1997;6:S5-11.
8. Coulter DM. The New Zealand Intensive Medicines Monitoring Programme In Pro-activeSafety Surveillance. Pharmacoepidemiol Drug Saf 2000;9:173-80.
9. Mann RD. Prescription-event monitoring – recent progress and future horizons. Br J ClinPharmacol 1998;46:195-201.
10. Mackay FJ. Post-Marketing Studies. The work of the Drug Safety Research Unit. Drug Saf1998;19:143-53.
11. Inman H. Postmarketing Surveillance of Adverse Drug Reactions in General Practice II:Prescription Event Monitoring at the University of Southampton. BMJ 1981;282:1216-7.
12. Grootheest AC van, Puijenbroek EP van, Jong – van den Berg LTW de. Contribution ofpharmacists to the reporting of adverse drug reactions. Pharmacoepidemiol Drug Saf2002;11:205-10.
13. Eland IA, Belton KJ, Grootheest AC van, et al. Attitudinal survey of voluntary reporting ofadverse drug reactions. Br J Clin Pharmacol 1999:48:623-7.
143
14. Grasela TH. Hospital Drug Surveillance Networks: Ad Hoc Pharmacoepidemiologic DataCollection Methods. In: Pharmacoepidemiology – an introduction (3e ed) Hartzema AG,Porta M, Tildon HH (editors). Harvey Whitney Books Company. Cincinnati 1998.
15. Puijenbroek EP. Quantitative Signal Detection in Pharmacovigilance. Thesis. Utrecht 2001.
16. Meyboom RHB, Egberts ACG, Edwards IR, Hekster YA, Koning FHP de, Gribnau FWJ.Principles of Signal Detection in Pharmacovigilance. Drug Saf 1997;16:155-65.
144
Chapter 4.2
Do pharmacists’ reports of adverse drug reactionsreflect patients’ concerns?
Pharmacy World and Science (accepted)
Kees van Grootheest MD1
Eugène P. van Puijenbroek MD, PhD1
Lolkje T.W. de Jong – van den Berg PharmD, PhD2
1. Netherlands Pharmacovigilance Centre Lareb,’s-Hertogenbosch, the Netherlands.
2. Department of Social Pharmacy and Pharmacoepidemiology, GUIDE, Groningen, the Netherlands
145
Abstract
Aim of the studyThe aim of the present study was to investigate whether the concerns patients expressto a Drug Information Line about possible adverse drug reactions (ADRs) they haveexperienced, are sufficiently reflected by the ADR reports submitted by pharmaciststo the Netherlands Pharmacovigilance Centre Lareb with regard to the type ofADRs and the drug groups involved.
MethodsADR-related questions patients addressed to the Dutch Drugs Information Linewere compared with the ADR reports pharmacists sent in to Lareb in the sameperiod. The similarities and differences between the two datasets as thecharacteristics of the suspected ADRs and the kinds of drugs mentioned wereinvestigated, as well as the severity of the reported ADRs. To compare the two datasets and to establish whether significant differences were present, a logistic regressionanalysis was conducted on the reported drugs and ADRs.
ResultsAnalysis of the content of the phone calls yielded 1168 (14.6%) calls concerningpossible experienced ADRs. The suspected ADRs pharmacists reported to theNetherlands Pharmacovigilance Centre Lareb in the same period included 1,734reports. There were only slight differences between the queries patients put to theDrug Information Line regarding possible adverse drug reactions and the reports onsuspected ADRs pharmacists submitted to the pharmacovigilance centre. Withrespect to possible ADRs in the psychiatric spectrum and ADRs associated with theuse of antidepressants, there seems to be a deficiency in the reporting by pharmacists.
ConclusionThe ADRs pharmacists report to the national pharmacovigilance centre reflectpatients’ concerns about ADRs they experience in relation to the medication they aretaking.
146
4.2.1 IntroductionPatients are sometimes concerned about the drugs they take and prove to have agreat number of questions about these drugs.(1) It goes without saying that theycan address these questions to the prescribing doctor or the dispensing pharmacistto have them look into their queries. However, patients in the Netherlands havealso the opportunity to put their questions regarding medication to the nationalDrugs Information Line (DIL), an initiative of the Royal Dutch Association for theAdvancement of Pharmacy (KNMP).(2) This information line is open during officehours; 150 pharmacists provide this service on a voluntary basis. A summary ofeach telephone conversation is stored in a database. The DIL first becameoperational in 1990 and at present approximately 10,000 questions are dealt with. The Netherlands Pharmacovigilance Centre Lareb is the national centre to whichdoctors and pharmacist’s report suspected adverse drug reactions (ADRs).(3) A substantial part (40%) of the number of reports Lareb receives is submitted bypharmacists.(4) This is not surprising since the Dutch pharmacists have made themonitoring of the use of medication and pharmacovigilance one of their prioritiesin the context of the pharmaceutical care they provide.(5-7)In recent years there has been an ongoing debate about the potential contributiondirect consumer reporting of possible ADRs might have for pharmacovigilance.(7,8)One of the arguments in supporting patient’s reporting system is that reporting bypatients could help solve the current underreporting of ADRs. Other considerationsthat have been mentioned concern claims that through consumer reports adverseevents may possibly be detected earlier or that adverse reactions may be broughtforward that might otherwise escape the attention of health professionals.(9,10) Observations and reports made by health professionals generally are a combinationof an interpretation of a description originally provided by the patient and objectiveinformation.(11)In an earlier study regarding the Drug Information Line, Van der Toom andcolleagues studied the question to the DIL during three short periods.(12) Egbertsand colleagues compared information derived from the DIL database with datafrom physicians and pharmacists in the Lareb database and evaluated patientcharacteristics and the drugs involved.(13) In the present study we compared the ADR-related questions patients put to theDrugs Information Line with the ADR reports pharmacists sent in to Lareb in thesame period. More specifically, similarities and differences between thecharacteristics of the suspected ADRs and the kinds of drugs mentioned wereinvestigated. The aim of the study is to establish whether the reports of pharmacistsadequately reflect the questions patients have in relation to possible ADRs theyhave experienced themselves.
147
4.2.2 MethodsIn our study we compare two datasets: one of questions to the Drugs InformationLine and one of pharmacist’s reports to the Netherlands Pharmacovigilance CentreLareb regarding drugs and ADRs. The study covered the period between 1 January1998 and 15 March 1999 and, given that both the Drugs Information Line andLareb work on a national scale, entailed a nationwide comparison. The entire rangeof questions the DIL processed during this period was analysed and coded by anexperienced assessor. The questions related to possible experienced adverse eventswere selected and subsequently categorised for further analysis. Only thosequestions with the following criteria were included in the analyses: the suspecteddrug could be identified, the adverse drug reaction had been experienced by thecaller him/herself and the caller’s sex was known. Enquiries about possible ADRsand calls with too general complaints were excluded.The ADRs mentioned by the various patients were assigned a so-called WHOpreferred term. Subsequently, each preferred term was assigned to one SystemOrgan Class (SOC), i.e. a group of preferred terms pertaining to the same organsystem.(14) The drug concerned was coded according to the first position of theAnatomical Therapeutical Chemical system (ATC-system).(15)Similarly, all the reports of suspected ADRs Lareb received from pharmacistsduring the period under investigation were selected and subsequently coded usingthe procedure described above. To compare the two data sets and to establish whether significant differences werepresent, a logistic regression analysis was conducted on the reported SOCs andATC codes. The odds ratios, (ORs) adjusted for age and gender, of the variousSOCs and ATCs as reported by patients (DIL) and pharmacists (Lareb) were
148
Table 1Number of questions (DIL) and reports (Lareb), ADR-related questions andreports, included cases, suspected drugs and reported adverse drug reactions from theDrug Information Line and from the pharmacist reports submitted to Lareb (1/1/98– 15/3/99)
DIL LarebTotal number of questions DIL and pharmacists reports to Lareb 8340 1734Number of questionsabout experienced ADRs 1168 1734Number of included cases 1041 1734Number of suspected drugs 1041 1814Number of reported adverse drug reactions 1323 2426
calculated as well as the corresponding 95%-confidence intervals. For the statisticalanalysis SPSS 10.0 was used.Next, for both groups the proportion of possible serious reports was estimated. Forthis procedure we applied the criteria for ‘critical term’ as defined by the WHO.(16)Critical terms are a subset of the WHO preferred terms indicative of serious diseasestates that warrant follow up. For this reason critical terms may be of particularinterest for signal generation.
4.2.3 ResultsIn the study period the suspected ADRs pharmacists reported to the NetherlandsPharmacovigilance Centre Lareb that were included in our study totalled 1734 reports,of which 595 concerned men (34.3%) and 1139 women (65.7%). In the same periodthe DIL processed 8012 queries by patients. Analysis of the content of the calls yielded1168 (14.0%) calls concerning possible or suspected ADRs experienced by the callerthemselves. In total, 1041 of the 1168 cases (12.5% of the total number of calls) couldbe included because ADR, suspected drug and sex of the patient were known. Of thesecases, 299 involved men (28.7%) and 742 women (71.3%). The number of included
149
Table 2Distribution of drugs according to ATC main group of reported ADRs of the DrugInformation Line (n=1041) and pharmacists’ reports to the NetherlandsPharmacovigilance Centre Lareb (n=1814).
Code ATC main group DIL Lareb Odds 95% conf. int.
A Alimentary tract and metabolism 50 142 1.68 1.21-2.34B Blood and blood forming organs 33 55 0.94 0.61-1.46C Cardiovascular system 182 453 1.55 1.28-1.88D Dermatologicals 18 47 1.49 0.86-2.59G Genito-urinary system and sex hormones 83 118 0.83 0.62-1.11H Systemic hormonal preparations 42 34 0.46 0.29-0.74J General anti-infectives for systemic use 45 222 3.05 2.19-4.24L Antineoplastics and immunomodulants 15 32 1.22 0.66-2.27M Musculo-skeletal system 49 134 1.65 1.18-2.31N Central nervous system 462 339 0.29 0.24-0.34P Antiparasitic products 6 38 3.64 1.53-8.65R Respiratory system 46 138 1.77 1.26-2.50S Sensory organs 6 28 2.79 1.15-6.77
Only those System Organ Classes that have more than 5 cases are included in this table.The Odds is adjusted for age and gender.
suspected drugs and reported ADRs to Lareb by pharmacists and those reported fromthe Drug Information Line are shown in Table 1. The differentiation in the drugsinvolved, as reported by pharmacists (Lareb) and by patients (DIL) can be found inTable 2. The differences in the reported ADRs as coded per SOC for both groups areshown in Table 3.
drug categoriesLooking at the drug categories, we observed that the number of reports frompharmacists to Lareb was significantly higher for medication directed at treatmentof disorders in the alimentary tract and metabolism, cardiovascular system,antibiotics, musculo-skeletal system and respiratory system (Table 2). By contrast,
150
Table 3Distribution of System Organ Classes for ADRs reported by patients to the DrugInformation Line (n=1223) and for ADRs reported by pharmacists to theNetherlands Pharmacovigilance Centre Lareb (n=2426).
Code System Organ Class DIL Lareb Odds 95% conf.int.
100 skin and appendages disorders 86 369 2.60 2.04-3.32200 musculo-skeletal system disorders 53 119 1.21 0.87-1,68410 central and peripheral nervous system d. 181 337 1.03 0.85-1.25431 vision disorders 44 103 1.28 0.90-1.84432 hearing and vestibular disorders 9 19 1.12 0.50-2.49433 special senses other disorders 18 67 2.20 1.19-3.42500 psychiatric disorders 220 230 0.50 0.42-0.63600 gastro-intestinal system disorders 215 414 1.07 0.90-1.29800 metabolic and nutritional disorders 44 32 0.38 0.24-0.61900 endocrine disorders 8 11 0.69 0.28-1.741010 cardiovascular disorders – general 11 18 0.90 0.43-1.921030 heart rate and rhythm disorders 29 57 1.05 0.67-1.651040 vascular (extracardiac) disorders 11 28 1.39 0.69-2.801100 respiratory system disorders 38 131 1.92 1.33-2.781230 platelet, bleeding & clotting disorders 16 50 1.67 0.95-2.951300 urinary system disorders 9 31 1.88 0.89-3.961410 reproductive disorders, male 18 11 0.27 0.13-0.581420 reproductive disorders, female 40 54 0.80 0.54-1.211810 body as a whole – general disorders 243 288 0.60 0.50-0.73
Only those System Organ Classes that have more than 5 cases are included in this table.The Odds is adjusted for age and gender.
the DIL answered significantly more questions about hormone-based medication(excluding sex hormones) and drugs affecting the nervous system.
adverse drug reactionsThe number of questions that the DIL received about adverse drug reactions washigher for the following SOCs: psychiatric disorders, male reproductive disordersand also for autonomic nervous system disorders (significant, but low numbers) –see Table 3.The ADRs for which Lareb received a higher number of reports from pharmacistsinvolved the following SOCs: ‘Skin’, ‘Special Senses’ and ‘Respiratory System’.
severity of the suspected ADRRegarding the severity of the suspected ADR, as expressed by the number ofreports that met the criteria for ‘critical term‘, we found that of the Lareb reports264 out of 1223 (11.9%) met this standard and this was 91 (7.4%) for the questionsposted to the DIL. Thus, the number of reports on serious ADRs was statisticallysignificantly higher for the pharmacists report to Lareb: OR 1.58 (95% confidenceinterval: 1.23 – 2.02).
4.2.4 DiscussionThe findings of our study show that there are only slight differences between thereports on suspected ADRs pharmacists submitted to our pharmacovigilance centreand the queries patients put to the Drug Information Line regarding possible ADRs.
The majority of the patients reported on by the pharmacists to Lareb and the callersto the DIL, was female. This should be seen in the light of the greater medicalconsumption by women and their concomitant higher use of medication.(17) The need for more information about the drugs being taken and in particular detailsregarding possible ADRs is evident. We included only those questions thatconcerned possible ADRs the patients had experienced themselves that could becoded as a WHO preferred term and of which the suspected drug was known(14.0%). This explains the difference with the study by Van der Toom et al. andEgberts et al. who found that respectively 21.6 and 28% of the callers’ queriesconcerned adverse events.(12,13) Although the difference between the ADRs pharmacists reported to Lareb and thecomplaints the DIL received was significant for the SOCs autonomic nervoussystem disorders and male reproductive disorders, the numbers involved weresmall. This also applies to the SOC metabolic and nutritional disorders mainlyassociated with obesity. For both these categories of questions holds that the callerseems to appreciate the anonymity of the DIL.
151
Many callers mentioned possible ADRs related to psychiatric disorders. This is notexceptional since a considerable proportion of the reports Lareb receives also fallsinto this category. Apparently, questions relating to these subjects are not as easilyput to the pharmacist, which prevents patients from reporting any such adverseeffects. Patients rather turn to their doctor or, again, prefer to call an anonymoushelpdesk. It needs to be noted that an earlier study had revealed that with respectto the SOCs male reproductive disorders and psychiatric disorders Lareb receivedsignificantly more reports from medical practitioners than from pharmacists.(13,17)As regards to the drugs for which adverse reactions were reported, we found that,compared to the pharmacist reports, the number of calls to the DIL about drugsaffecting the CNS were far higher. The calls mainly concerned the largest type ofdrugs of this category, i.e. antidepressants. Van der Toom et al. found also CNSdrugs as the biggest group and Egberts et al. had earlier reported a similar findingregarding antidepressants.(12,13)This is not surprising since the use of antidepressant drugs is still increasing. Theproportion of both adverse events of a psychiatric nature and events associated withthe use of antidepressants is higher for the DIL when compared to the number ofthese ADRs in the pharmacists’ reports to Lareb. Despite the fact that pharmacistsalso operate the DIL, as mentioned earlier the anonymity of the helpline seems toplay a role. The professional background of the person answering the call does notappear to play a role in the patient’s decision to call the DIL. It is possible that forconcerns that relate to the patient’s private life, patients are more inclined to turn tothe DIL and since it is exactly this type of query that worries most users, the needfor a second opinion may be high. This fact may also explain the high incidence ofcalls of this nature.With respect to the severity of the ADRs reported we found that the proportion ofpharmacist’ reports signalling a possibly serious ADR was higher than the numberof questions about possible serious adverse drug reactions addressed to the helpline.This seems to imply that for serious complaints patients tend to go straight to apharmacist.In general, pharmacists’ reports to the Netherlands Pharmacovigilance CentreLareb prove to be a good reflection of the questions patients have regarding ADRs.Pharmacists consider answering questions from patients’ part of the pharmaceuticalcare they give, which function has been fully integrated in the pharmacies’operational procedures. This should be considered in the discussion about the valueof direct ADR reporting by patients, however other and more specific reportingfacilities for patients to report possible ADRs should be taken into account in thisdiscussion.(8)The organisation of a helpline is quite complex: a considerable number of volunteerpharmacists and organisational adaptations are required to operate such a system.
152
These pharmacists have also the possibility to report a possible ADR to the nationalpharmacovigilance centre, which is seldom done for questions answered throughthe Drug Information Line.This study has some weaknesses. It should be taken into account that no causalityassessment has been performed. Such an assessment was not possible due to thelimited information that is obtained from callers to the DIL. This preventsconclusions to be drawn about possible new signals of an ADR. It may be possiblethat some questions to the DIL, if reported to their pharmacist, will be sorted outbecause they were not considered to be a possible ADR in his of her professionalview. Reports from pharmacists to the national pharmacovigilance centre are farmore detailed in comparison with the information given to the information line.This study should not be regarded as a comprehensive study. Of the two groupsinvestigated, only a limited number of factors have been compared. The DrugInformation Line is not designed for the detection of ADRs and only limitedinformation is available. Moreover, possible ADRs are not recorded in astandardised way. It also needs to be noted that it was not possible to determinehow many of the questions patients put to the Drug Information Line had also beenput to their health professionals, who subsequently reported these to Lareb.Both groups which we compared in this study involved pharmacists. The DrugInformation Line is staffed by pharmacists and only the reports pharmacistssubmitted to Lareb were taken into account. Despite the fact that pharmacists arequite willing to answer patient questions about drug use and problems in theirpharmacies, for some users the threshold seems too high. These individuals preferto call the DIL. This finding indicates that the role of the pharmacist, being anexpert in his/her field and thus best equipped to provide independent, professionalinformation in the pharmacy, should be enforced. It is also recommended that thepatient leaflet inform drug users about the fact that possible adverse drug reactionsshould be notified to their health professional, physician or pharmacist.
4.2.5 Conclusion Patients take a keen interest in the drugs they are taking and are frequently in searchof answers to questions concerning these drugs. A substantial part of their worriesconcern possible ADRs. Although the prescribing doctor and dispensingpharmacist are the most obvious and best-equipped persons to address thesequestions to, a telephone service providing information on drugs appears to fulfil aneed. A comparison of the reports pharmacists submit to a spontaneous reportingsystem with questions put to a drug information line shows that, for the aspectsinvestigated, the nature of ADRs as reported by pharmacists match the features ofthe phone queries. However, particularly with respect to possible ADRs in thepsychiatric spectrum and suspected ADRs associated with the use of
153
antidepressants, there proves to be a deficiency in the reporting by pharmacists, butare within Lareb corrected by a higher proportion of reports from physicians.Despite this obvious limitation, it may be concluded that, in general, the ADRspharmacists report to the national pharmacovigilance centre adequately reflect thepatients’ concerns about possible ADRs associated with the medication they aretaking.
AcknowledgementThis study would not have been possible without the help of all those involved in theDrugs Information Line and the Netherlands Pharmacovigilance Centre Lareb.
154
References
1. Bouvy ML, Berkel J van, Roos-Huisman CM de, Meijboom RHB. Patients’ drug-informationneeds: a brief view on questions asked by telephone and on the internet. Pharm World Sci2002;24:43-5.
2. Dumoiseaux V. Evaluatie-onderzoek Geneesmiddel-Infolijn. KNMP. Den Haag 1995.
3. Grootheest AC van, Puijenbroek EP van. Pharmocovigilance in the Netherlands. In:Pharmacovigilance. Mann RD, Andrew EB (editors). John Wiley and Sons. Chichester 2002.
4. Grootheest AC van, Puijenbroek EP van, Jong – van den Berg LTW de. Contribution ofpharmacists to the reporting of adverse drug reactions. Pharmacoepidemiol Drug Saf2002;11:205-10.
5. Grootheest AC van, Mess K, Jong - van den Berg LTW de. Attitude of communitypharmacists toward ADR reporting in the Netherlands. Int J Pharm Pract 2002;10:267-72.
6. Buurma H, de Smet PA, van den Hoff OP, Egberts AC. Nature, frequency and determinantsof prescription modifications in Dutch community pharmacies. Br. J. Clin Pharmacol2001;52:285-91.
8. Grootheest AC van, Graaf L de, Jong - van den Berg LTW de. Consumer reporting: A newstep in pharmacovigilance? An overview. Drug Saf 2003;26:211-17.
9. Wouters J. Patiëntenervaringen, een bron van informatie rijker! Utrecht, 1998.
10. Egberts ACG, Smulders M, Koning GHP de, Meyboom RHB, Leufkens HGM. Can adversedrug reactions be detected earlier? A comparison of reports by patients and professionals. BMJ1996;313:530-1.
11. The Importance of Pharmacovigilance, Safety Monitoring of medicinal products. WorldHealth Organisation, Geneva/Uppsala 2002.
12. Toom E van der, Pasman M, Hielema, AP, Vos R, Jong – van den Berg LTW de. DeGeneesmiddel-Infolijn, een bron van informatie, niet alleen voor patiënten [The DrugInformation Line, a source of information, not only for patients]. Pharm Weekbl1994;129:1131-8.
13. Egberts ACG, Koning FHP, Meyboom RHB, Leufkens HGM. ADR-related questionsreceived by a telephone medicines information service and ADRs received by a spontaneousADR reporting System: a comparison regarding patients and drug. Pharmacoepidemiol DrugSaf 1997;6:269-76.
155
14. WHO Adverse Drug Reaction Dictionary. WHO Uppsala Monitoring Centre. Uppsala 1996.
15. Anatomical Therapeutical Chemical (ATC) Classification Index. WHO Collaborating Centrefor Drug Statistics Methodology. Oslo 1994.
16. Lindquist M. Edwards IR, Fucik H, Nunes HM, Ståhl M. From association to alert – Arevised approach to international signal analyses. Pharmacoepidemiol Drug Saf 1999;8:S15-25.
17. Jong – van den Berg LTW de. Vrouw en geneesmiddel. Pharm Weekbl ;136:1634-8.
18. Rijcken CAW, Dekens-Konter JAM, Knegtering H, Jong – van den Berg LTW de. Reportingsexual function disorders caused by antipsychotic drugs: is there a role for the communitypharmacy? Pharm World Sci 2001;23:169-72.
156
Chapter 4.3Consumer reporting: a new step in pharmacovigilance?- An overview.
Drug Safety 2003;26:211-7.
Kees van Grootheest MD1
Linda de Graaf PharmD1
Lolkje T.W. de Jong – van den Berg PharmD, PhD2
1. Netherlands Pharmacovigilance Centre Lareb,’s-Hertogenbosch, the Netherlands.
2. Department of Social Pharmacy and Pharmacoepidemiology, GUIDE, Groningen, the Netherlands
157
Abstract
The direct reporting of adverse drug reactions by patients is becoming anincreasingly important topic for discussion in the world of pharmacovigilance. At thistime, few countries accept consumer reports.An overview is given of experiences with consumer reporting in various countries ofthe world. The potential contribution of patients reports of adverse drug reactions isdiscussed, both the qualitative and quantitative contribution. The crucial question isone of whether patient reports will increase the number and quality of the reportssubmitted and/or lead to a more timely detection of signals of possible adversereactions, thus contributing to an enhancement of the existing methods of drugsafety monitoring. To date, the data available are insufficient to establish such addedvalue.
158
4.3.1 IntroductionThe direct reporting of adverse drug reactions by patients is becoming aincreasingly important topic for discussion in the world of pharmacovigilance. Inseveral countries there is an ongoing debate about the question or consumer reportswithout physicians or pharmacists as a intermediate are desirable. In this paper weuse the term consumer reporting, however it might be argued that the wordconsumer relate more to a commercial product as to a health care product. Patientreporting could be a better term, relating it more to patients than to the producer’sside of drugs.(1)A key problem in the discussion about the usefulness of consumer reporting is thefact that there is little evidence, especially when we relate consumer reporting tospontaneous reporting. All the information available in the literature regardsresearch using questionnaires or using a drug information service, and is not theresults of experiences with consumer reporting to a centre that collects spontaneousreports.(2-7)In this overview we will make an inventory of experiences with consumer reportingin various countries of the world. The potential contribution of patients reports ofadverse drug reactions will be discussed, both in terms of their qualitative andquantitative contribution.
4.3.2 The necessity of pharmacovigilanceThe advent of pharmacotherapy based on recent scientific advances in the first halfof the twentieth century brought about revolutionary changes in the scope of curesfor numerous diseases. These innovations were of course enthusiasticallywelcomed, and this welcome was almost without question; the negative aspects ofpharmacotherapy received little or no attention. Only when adverse reactions of aparticular drug were evident, were critical questions asked, but otherwise scrutinywas never systematic.(8)It was the Dutchman Meyler who, in 1951, was the first to provide a systematicoverview of ‘side effects of drugs’. His work formed the basis of what is, on aninternational scale, still regarded as the standard work in the field of adverse effectsof drugs.(9)The thalidomide tragedy in the early 1960s induced many countries to set upnational bodies to monitor the safety of drugs, also known as pharmacovigilancecentres. The underlying motive for the establishment of such national centres wasthat, by giving physicians and pharmacists the opportunity to report suspectedadverse events, potential but as yet unknown side effects of drugs would bedetected at an earlier stage. It was thought that serious and extensive damage as hadbeen caused by thalidomide could thus be prevented. European legislation has ledto uniformity in pharmacovigilance within the European Union by stipulating
159
which tasks and responsibilities are to be carried out and assumed by the nationalgovernments, the pharmaceutical industry and the various professional groupsinvolved. Many countries, among which all EU member states, have organised their reportingsystems for potential adverse events in such a way that only physicians andpharmacists are qualified to report.(10) In a number of countries pharmacists arenot necessarily authorised to report.(11) This method of collecting and analysing data from the health care sector is called a‘spontaneous reporting system’ (SRS), the word spontaneous in this contextmeaning that reporting is not compulsory. Consumer reporting was never before anitem in the organisation of SRS; it is only recently that consumer has become a pointof discussion. When we use the term consumer reporting, it is about users of drugsreporting suspected adverse drug reactions to a spontaneous reporting system.
4.3.3 International experiences and developments concerning patient reportsTo date there is little practical experience with patients reporting adverse drugreactions. In a limited number of countries the national reporting system providessome (formal) room for patient reports. Below we will discuss the current situationon consumer reporting in various countries.
United StatesMedWatch, the FDA’s Safety Information and Adverse Event Reporting Program,offers patients some scope to directly report adverse drug reactions. The majorityof reports originating from patients that actually reach the FDA, however, are sentin by the pharmaceutical industry. This sector has the legal obligation to pass on allreports it receives. Thus, questions and complaints from patients concerning drugsaddressed to the marketing authorisation holder are categorised as patient reports.A mere 12% of all reports the FDA receives have been directly submitted byphysicians, pharmacists or health consumers. Approximately a third of thesereports stem from patients.(12) No publications have been done yet about thecontribution of consumer reports to the FDA.
AustraliaSince the early 1990s Australia has been taking its first steps towards creatingfacilities allowing patients to report complaints on drugs. The Australian PatientSafety Foundation runs and maintains the Australian Incident Monitoring System(AIMS). However, only 20% of the reports concern medication and only 4% ofthese are about adverse events. The national reporting system (ADRAC) receivesabout 10,000 reports per year and this includes all appropriately documentedpatient reports. On an annual basis the latter comprise fewer than 100 reports.(13)
160
Scandinavian countriesIn September 2000 Kilen, the Swedish Consumer Institute for Medicines andHealth, organised a conference that was announced as the ‘First InternationalConference on Consumer Reports on Medicines’.(14) The key topic of theconference was: Should patients be given the opportunity to report possible adversedrug reactions direct to a national body? Kilen does collect patient complaints aboutdrugs in Sweden and Norway although these complaints specifically concernaddiction to benzodiazepines and lorazepam in particular. Thus, practical experiencewith comprehensive consumer reporting is still limited and Kilen’s full objectiveshave as yet not been implemented. Remarkable is the fact that in the Scandinaviancountries pharmacists are not allowed to report ADRs to their national centres.
The NetherlandsIn the Netherlands there is no hands-on experience with consumer reportingalthough some research into the topic has been conducted. In 1998 theWetenschapswinkel Geneesmiddelen (Science Shop for Drugs) of the Faculty ofPharmacy of the University of Utrecht published a study in which it wasinvestigated which specific facilities would allow patients to report side effects inthe Netherlands and how these facilities could be adjusted and extended.(15) In around-table conference following the project it was concluded that further researchinto consumer reporting was desirable. Also, two Dutch hospitals have conductedresearch into patients as information source for possible adverse events.(2) Recently the Dutch Consumer Association insisted on the fact the consumershould be able to report suspected adverse drug reactions to the nationalpharmacovigilance centre.
United KingdomIn the UK the Consumers’ Association has also suggested that patients shouldperhaps be offered facilities to report on adverse drug reactions.(16) Again, as inSweden, the late discovery of dependency on benzodiazepines was mentioned as anexample of signals that might be reported earlier by patients than professionals. The Medicines Control Agency (MCA) maintaining the national reporting system inthe UK has responded with caution based on both intrinsic and practical arguments.Nevertheless, in the UK the National Health Service does facilitate the reporting ofcomplaints by patients, and, although the emphasis is not on drugs, adverse effects arealso mentioned in this context.(17) Recently there are new developments regardingdirect consumer reporting because of the intended merger of the Medicines ControlAgency and the Medical Devices Agency. The Medical Devices Agency acceptspatients reports and once the agencies emerge it is would be possible the new agencyalso accept direct reports from consumers of pharmaceuticals.(18)
161
The InternetNovel is the emergence of web sites on the Internet offering patients a forum toexchange their experiences with drugs. Apart from being an expression of thepatients’ need to share and exchange information about medication, thephenomenon also shows that patients are a rich source of information. It is evident,however, that distinguishing valuable from unreliable data on the Internet poses areal problem.(19)
4.3.4 Potential contribution of patient reports on adverse reactionsIn the debate on the advisability of offering patients facilities to report suspectedside effects of drugs, various issues play a part. These will be outlined next.
Qualitative contribution It is to be expected that reports from a patient perspective will cause a shift in thetype of adverse reactions being reported since the reports that now reach thereporting systems may not reflect the adverse events that were originally reportedbecause of the filter applied by physicians and pharmacists.(7) With patient reports,not only side effects that health professionals generally consider less relevant willreceive attention, but also complaints that are usually less easily communicated, forinstance those relating to sexual matters.(20) Similarly, adverse effects caused by theoff-label use of medication (applications deviating from the approved indication)are probably less likely to be reported by doctors than by patients. In addition,doctors may not always be familiar with certain over-the-counter drugs oralternative medication.
Quantitative contributionConsumer reporting will raise the number of reports submitted, which will enhancethe impact of the reporting systems. Despite the fact that research has repeatedlyshown that in the Netherlands the basis of trust between patients and their doctorsand pharmacists is such that this generally does not form a major obstacle, the factthat less than 10% of the professionals involved effectively pass on reports does putthings in an different perspective: many complaints from patients appear to founderon the reluctance of the health care professionals.(21) The huge number of queriesthe Dutch Geneesmiddelen Info Lijn (Drug Information Line) receives suggeststhat the number of reports submitted by patients may be considerable.
Political and strategic considerationsAn important consideration in support of direct reporting by patients is the factthat, given today’s increasing patient awareness and emancipation, it is desirablethat patients are given the opportunity to report suspected side effects themselves.
162
After all, it is the patient that experiences the adverse reactions, which makes himor her the hands-on expert.Reporting through GP or pharmacist implies that complaints are filtered out, whichprevents patient complaints from reaching the reporting system. Since patients andconsumer organisations have acquired a considerable say in determining health carepolicy, perhaps this argument may carry more weight than before.
4.3.5 Possible objections to and limitations of patient reportsConsumer reporting does not seem to get off the ground properly anywhere.Apparently, there are serious obstacles that prevent a timely establishment ofreporting systems for the collection and evaluation of adverse drug reactionsreported by patients.
Establishing the contribution of patient reports in relation to the existing signaldetection systemsThe main obstacle for the development of consumer reporting systems is thefundamental question regarding their intrinsic value. The existing reporting systems, primarily based on spontaneous reporting bydoctors and pharmacists and on obligatory reporting by marketing authorisationholders, have evolved extensively over the past few decades, particularly withrespect to both the quality and the analyses of the reports. As far as we know, no research has been conducted to show that extending thecurrent systems to include reports from patients will add to their value when thesize and speed of signal generation and detection are concerned.
Quality of patient reportsA key issue concerns the quality of the reports submitted by patients. Firstly, thequality as regards the selection of the reports is at stake: Are patients capable ofdistinguishing possible adverse drug reactions from other complaints associatedwith the use of medication? A second aspect relating to the quality of patientreports is their documentation. Is a lay reporter capable of providing a clear andobjective description of the side effects and can he or she supply the relevant clinicalinformation necessary for an adequate evaluation of the report?
4.3.6 DiscussionSince during the clinical trials, carried out in the evaluation and marketingauthorisation stages, the safety of drugs can only be investigated to a limited extent,it is essential to also monitor their safety after marketing. For this purpose, manycountries have set up a national pharmacovigilance system, which, as a rule,functions on the basis of spontaneous reporting by physicians and pharmacists. In
163
this paper the advisability of direct reporting of potential adverse drug reactions bypatients was evaluated. It is evident that patient reports are desirable from a politico-strategic perspective.Edwards has typified the reporting of side effects as concern reporting.(22) Apartfrom the medical professionals, the users of drugs also have such concerns.Physicians, pharmacists and patients all have reason for concern when the safety ofdrugs is concerned and all parties need to be able to express their worries in such away that they can be assured that they are taken seriously and that the necessarysteps will be taken. The fact that patient and consumer organisations haveconsiderable influence on health care policy, lends validity to this argument.Consumer reporting is in line with the striving for quality in the health care system,in the evaluation of which the care taker takes up a key position. Unfortunately, todate few studies into the potential contribution of patient reports on possibleadverse drug reactions are available in the literature. Both Solovitz et al. andMitchell et al. have reported that users of drugs are capable of discriminatingbetween side effects and other complaints or symptoms.(4,5) Mitchell et al. aremore hesitant in this respect, particularly in connection with the patient’s ability toassociate suspected adverse events with a particular drug. However, one may askwhether this should be the reporter’s responsibility. In a retrospective studyEgberts et al. compared the questions posed by the users of drugs with adversereactions reported by physicians and pharmacists in the same period.(6) It appearedthat about a certain number of signals derived from the database of the officialreporting system users had earlier demanded information. Van de Bemt et al. haveshown that when specifically asked for them, hospital patients were able to reporton side effects.(2) In this case the reported effects mainly concerned less seriousreactions that were not known at the time. It needs to be noted, however, that it wasnot investigated whether the reported adverse reactions were effectively related tothe drugs used. Jarernsiripornkul et al. reported that patients are willing to report ifthey are asked to do so.(3)
Both the Netherlands and Australia have been considering whether specific patientgroups could function as reporting parties. Such a reporting system could be efficientlyorganised and could specifically analyse patients’ experiences with particular groups ofdrugs. In this context research into new drugs aimed at particular patient groups, e.g.rheumatics or diabetics, could be thought of, during which study patient organisationscould also be involved. However, if reports are expressly invited, this would be a caseof Intensive Monitoring, which implies research rather than continuous surveillance. Establishing a system to collect patient reports is no easy matter. For instance, arepatients interested in a system specifically aimed at gathering suspected adversedrug reactions or would they prefer a system with a wider scope covering other
164
aspects of pharmacotherapy It is clear that a more comprehensive system will bequite different from a system that focuses solely on possible side effects. Either way,the evaluation and scientific analysis of the reports received will require manpowerand funds. A reporting system raises expectations with those who report, i.e. theyexpect their reports to lead to results, and, in addition, they wish to be informedabout the steps to be taken. With reporting systems for the medical professionssuch feedback has proved essential for their success (22).Setting up a patient reporting system requires a separate organisation. The existingdoctor-pharmacist systems are hesitant in taking on this extra task. This hesitationoriginates from the fear that the system will receive too much ‘noise’ without theadded value of the new system having been established, receiving many but poorlydocumented reports. Again, this relates to the question whether patient reportingsystems should merely concentrate on side effects or whether they should also takeother aspects of drug use relevant to patients, such as queries regarding delivery anduse, into account.Reporting of experienced adverse drug reactions through a health professionalcould mean a kind of filtering. Also could be argued that this filter is a wished one,preventing an overload of national pharmacovigilance centre with invalid reports.There is some parallel with the discussion about direct-to-consumer drugadvertisements.(23) On one hand these advertisement could stimulate consumerreporting. On the other hand in this discussion is also the question for the need ofa ‘learned intermediary’.(24)
Apart from reports that are submitted direct to the national pharmacovigilancecentres, there are also consumer reports that are sent to the pharmaceuticalcompanies that produce the drugs concerned. As mentioned earlier, this latterpractice is quite common in the United States. A recent study has investigated theway the pharmaceutical sector deals with these consumer reports (25). Most drugcompanies include the information derived from such reports in their databases.Moreover, they have the legal obligation to pass on any reliable information abouttheir products to the authorities. In most cases, however, the data received areinsufficient to perform a proper causality assessment.To be able to make a well-founded judgement on the advisability of an independentreporting system for patients the pivotal question in need of an answer is whethersuch a system will add to the value of the existing systems. Such a study should becarried out within the context of a spontaneous reporting system.
Establishing a patient system for political and strategic reasons only, without havingestablished its possible added value first, falls outside the scope of pharmacovigilance. Adverse drug reactions do not only concern patients, both the prescribing doctor and
165
the delivering pharmacist are also involved. Reporting in cooperation with theprescribing doctor and/or pharmacist seems to be preferred method of reporting,supposing these professionals do report. The crucial question is whether patientreports will increase the number and quality of signals of adverse drug reactionsand/or lead to a more timely detection of them, thus contributing to an enhancementof the existing methods of drug safety monitoring. To date, the data available areinsufficient to establish such added value.
166
References
1. International Society of Drug Bulletins (ISDB). Declaration on therapeutic advance in the useof medicines. ISDB. Paris 2001.
2. Bemt PMLA van den, Egberts ACG, Lendering AW, et al. Adverse drug events in hospitalizedpatients. A comparison of doctors, nurses and patients as sources of reports. Eur J ClinPharmacol 1999;55:155-8.
3. Jarernsiripornkul N, Krska J, Capps PAG, Richards RME, Lee A. Patient reporting ofpotential adverse drug reactions: a methodological study. Br J Clin Pharmacol;53:318-25.
4. Mitchell AS, Henry DA, Sanson-Fischer R, et al. Patients as a direct source of information onadverse drug reactions. BMJ 1988;297:891-3.
5. Solovitch BL, Fisher S, Bryand SG, et al. How well can patients discriminate drug-related sideeffects from extraneous new symptoms? Psychopharmoco Bull 1987;23:189-92.
6. Egberts ACG, Smulders M, Koning GHP de, Meyboom RHB, Leufkens HGM. Can adversedrug reactions be detected earlier? A comparison of reports by patients and professionals. BMJ1996;313:530-1.
7. Egberts ACG, Koning FHP de, Meyboom RHB, et al. ADR-related questions received by atelephone medicine information service and ADRs received by a spontaneous ADR reportingsystem: a comparison regarding patients and drug. Pharmacoepidemiol & Drug Saf1997;6:269-76.
8. Routledge P. 150 years of pharmacovigilance. Lancet 1998;351:1200-1200-1.
9. Dukes MNG, Aronson JK, editors. Meyler’s Side Effects of Drugs, 14th edition. Amsterdam:Elsevier, 2001.
10. Procedure for competent authorities on the undertaking of pharmacovigilance activities. In:The rules governing medicinal products in the European Union; Volume 9: 61-77.
11. Grootheest AC van, Puijenbroek EP van, Jong-van den Berg LTW. Contribution of pharmaciststo the reporting of adverse drug reactions. Pharmacoepidemiol & Drug Saf 2002;11:205-10.
12. Anonymous. Direct reporting by consumers – First International Conference. WHOPharmaceutical Newsletters 2000;3:12-3.
13. Knapp DE, Robinson JI, Britt AL. Annual Adverse Drug Experience Report 1995. FDA 1996.
14. Roughead L. Consumer reporting of adverse drug events: a discussion paper for the consumerreporting of adverse drug events working party of the Australian Pharmaceutical AdvisoryCouncil. Paper Kilen Conference, Sigtuna 2000.
167
15. Wouterse JJ. Patiëntenervaringen, een bron van informatie rijker! WetenschapswinkelGeneesmiddelen, Faculteit Farmacie, Universiteit Utrecht. Mei 1998.
16. Anonymous. UK call for patient ADR reporting. Script 2001; 2634:4.
17. Mayor S. NHS introduces new patient safety agency. BMJ 2001;322:1013.
18. Sukker E, UK patients to report ADRs – comment. Script 2002;2784:5.
19. Morel P, Vandel B. Adverse drug reaction monitoring and the Internet: evaluation of the useof the Internet by French Pharmacovigilance Centres and a non-exhaustive survey of websitesof interest for collecting information about adverse drug reactions. Thérapie 1999;54:525-32.
20. Rijcken CAW, Dekens-Konter JAM, Knegtering H, Jong-van den Berg LTW de. Reportingsexual function disorders caused by antipsychotic drugs: is there a role for the pharmacy?.Pharm World Sci 2001;23:169-72.
21. Edwards IR. Spontaneous reporting – of what? Clinical concerns about drugs. Br J ClinPharmacol 1999;48:138-41.
22. Eland IA, Belton KJ, Grootheest AC van, et al. Attitudinal survey of voluntary reporting ofadverse drug reactions. Br J Clin Pharmacol 1999:48:623-7.
23. Watson R. Consumer groups fight plans for ‘direct to patient’ drug advertisements. BMJ2001;323:889.
24. Drazen JM. The consumer and the learned intermediary in health care. N Engl J Med; 346:523-3.
25. Fleuranceau-Morel P. How do pharmaceutical companies handle consumer adverse drugreactions reports? An overview based on a survey of French drug safety managers and officers.Pharmacoepidemiol Drug Saf 2002;11:37-44.
168
Chapter 4.4Labelling and ‘Dear Doctor’ letters - Are they noncommittal?
Drug Safety 2002;25:1051-5.
Kees van Grootheest1
Ralph Edwards2
1 Netherlands Pharmacovigilance Centre Lareb,‘s-Hertogenbosch, The Netherlands
2 The WHO Collaborating Centre for Drug Monitoring,Uppsala, Sweden
169
Abstract
Over the past few years, a number of drugs have been withdrawn for safety reasons,either by drug approval authorities, or by the manufacturer. A recent example is thewithdrawal of cerivastatin in connection with rhabdomyolysis. Several other drugshave also been taken off the market as a security measure, not because the nature ofthe risk involved was unknown but because the risk had proved apparentlyuncontainable. It seems that the inclusion of a warning or contraindication in theSummary of Product Characteristics (SPC) or sending a ‘Dear Doctor’ letter isinsufficient to ensure compliant prescription behaviour. There appears to be adiscrepancy between the careful use of evidence underpinning the SPC content andformal warnings and changes to the SPC and the effect they have on the prescriptionand dispensing of the drugs involved. This results in undue loss or damage for boththe manufacturer and the patient.There are no easy solutions to tackle this problem; the ineffectiveness of labelling and‘Dear Doctor’ letters has ramifications for the whole regulatory/industrial/educational complex.We discuss briefly four possible strategies for improving the current situation,emphasising on the place the prescriber has in this process.The first strategy is education-based. Clinicians need to know about the comparativemerits of the effectiveness and risk of drugs, as well as how they workpharmacologically, toxicologically, and what interactions they have with each other.The second strategy involves improving the information available for clinicians.Frequently, physicians do not consult the SPC for verification, leaving aside whetherthey have taken notice of the contents of the official SPC in the first place. It isrecommended to that the accessibility of SPCs is enhanced for doctors andpharmacists, drawing attention specifically to any changes. There needs to be a singlebody of information that covers every drug.The third strategy involves communication. There is much to be done in this areaboth in terms of follow-up and understanding of health professional’s behaviour andhow to empower best practise.The final strategy involves professional freedom. It goes without saying that doctorswho issue off-label prescriptions may need to justify their actions. Deviating fromthe SPC should always be a considered decision and health professionals need to beaware of the additional responsibilities associated with such a decision. Thedispensing pharmacist can play an important role in the implementation of warningsand contraindications.
170
4.4.1 IntroductionWithdrawing a drug from the market is a drastic measure. Over the past few yearsa number of drugs have been withdrawn for safety reasons, either by drug approvalauthorities, or by the manufacturer. A recent example is the withdrawal ofcerivastatin in connection with rhabdomyolysis, occurring especially whencerivastatin is prescribed in combination with gemfibrozil. What was remarkable inthis case was the fact that the Summary of Product Characteristics (SPC) didinclude a warning for this interaction and also that the manufacturer had alerted thehealth professionals in ‘Dear Doctor’ letters about the complication.Several other drugs have also been taken off the market as a security measure, notbecause the nature of the risk involved was unknown but because the risk hadproved apparently uncontainable. It seems that including a warning orcontraindication in the SPC or sending a ‘Dear Doctor’ letter is insufficient toensure compliant prescription behaviour.
4.4.2 PracticeA number of studies have been published on the effects of adjustments of the SPCcontent and ‘Dear Doctor’ letters in connection with the incidence of arrhythmiaassociated with the use of cisapride.(1,2) Notwithstanding the fact that in the USfour label changes and notifications had been issued, in 3.4% of the cases theconcomitant use of at least one contraindicated drug had occurred.(1) It was notuntil the risks of cisapride had received more extensive media attention that the co-dispensing of drugs that should not be taken together with cisapride actuallydecreased.(2)In March 2000, troglitazone was recalled from the market because of life-threatening acute liver failure. The risk was known and was referred to in the SPC.In the US the manufacturer had distributed four ‘Dear Doctor’ letters, whichincluded the recommendation that liver function be tested more frequently.Although subsequently the number of patients tested increased 3-fold, a mere 5%of users were tested in the recommended frequency after 3 months on the drug.(3) Recently, research results on the indications for which rofecoxib is prescribed werepublished in the Netherlands.(4) Rofecoxib was originally approved in theNetherlands for the indication ‘symptomatic treatment of arthrosis’. However,promotional material directed at physicians particularly emphasised ‘pain relief’,even though costs are officially only reimbursed for the indication (osteo)arthrosis.An evaluation of the electronic data collected from the prescribing generalpractitioners showed that over 80% of the prescriptions involved a differentdiagnosis than that of ‘arthrosis’, thus constituting a deviation from the indicationspecified in the SPC. The researchers concluded that rofecoxib is prescribed for awider range of indications than for which it was approved.
171
The content of the SPC is compiled with due consideration of the evidenceavailable, including information from the clinical trials conducted prior tomarketing authorisation. The definitive text is determined by the drug approvalauthorities and the SPC becomes part of the registration file. ‘Dear Doctor’ lettersare drawn up in close co-operation with the manufacturer and the drug approvalauthorities. This also holds for any changes in the content of the SPC, such asalterations resulting from postmarketing research that have led to new insights intothe safety aspects of the drug.
4.4.3 The problemThere appears to be a discrepancy between the careful use of evidence underpinningthe SPC content and formal warnings and changes to the SPC and the effect theyhave on the prescription and dispensing of the drugs involved, as shown by thecases mentioned above. If and when physicians and pharmacists do not adhere tothe SPC and their decisions lead to an increased safety risk, the decision towithdraw a particular drug from the market may be expedited. This results in undueloss or damage for both the manufacturer and the patient.(5) It may be argued,therefore, that physicians and pharmacists should adhere to the indications,warnings and contraindications as described in the SPC. Also, any alterations in thecontent of the SPC should be followed up in daily practice. The same applies forthe information disseminated via ‘Dear Doctor’ letters.Legally, however, physicians can deviate from the indications as described in theSPC. In some cases they have no other option, as occurs for instance in paediatricpractice quite often because of lack of clinical trial information on children. Inaddition, warnings and contraindications can be ignored. There can be soundclinical reason in this. Clinical trial and epidemiological evidence can only providea guide as to the normal group response to a drug or other therapy. It goes withoutsaying that doctors who issue off-label prescriptions may be need to justify theiractions. Deviating from the SPC should always be a considered decision and healthprofessionals need to be aware of the additional responsibilities associated withsuch a decision.
4.4.4 Possible solutionsWe are aware that as we are discussing the ineffectiveness of labelling and ‘DearDoctor’ letters, it has ramifications for the whole regulatory/industrial/educationalcomplex. The complexity of this could easily hinder the necessary debate. We willbriefly discuss four possible strategies. Given that clinicians must interpret evidenceand not try to force patients into convenient algorithms, what can be done toprevent the SPC from being perceived as a prescriptive legal document and to bemore empowering?
172
1. EducationDrug therapy is a complex business. New drugs become available all the time, aswell as new information on old drugs. The clinician, in particular, has the role of the‘learned intermediary’ to evaluate knowledge critically and to use and explain it ina given individual setting. To be a ‘learned intermediary’ health professionals mustunderstand the drugs they use and it is important to acknowledge thatundergraduate curricula are overloaded, and only the rudiments of clinicaltherapeutics can be taught. Clinicians need to know about the comparative meritsin effectiveness and risk of drugs, as well as how they work pharmacologically,toxicologically, and how they interact with each other. Then the clinicians maymake logical inferences for the therapy of the patients they treat.
2. InformationFrequently, physicians do not consult the SPC for verification, leaving asidewhether they have taken notice of the contents of the official SPC in the first place.It is recommended that the accessibility of SPCs for doctors and pharmacists isenhanced, drawing attention specifically to any changes. All evidence-basedfindings, including information obtained in clinical trials performed during the pre-marketing stage (not just didactic statements), need to be made available. Greaterawareness about adverse drug reactions, regarding their significance, recognition,management and prevention, needs to be established. In order to enhance theknowledge of the effects of drugs in the clinical practice it is vital that doctors andpharmacists report suspected adverse effects to their national pharmacovigilancecentres. These centres need to find effective ways to disseminate the data they havecollected to the various professional groups and should be involved in andcontribute to the education of health professionals. In short, there needs to be abody of information for every drug that is available from a single accessible source.There are numerous publications and websites that provide useful information butthey do not have regulatory approval. The Cochrane Foundation provides usefulreviewed information, but does not go far enough in factoring in knowledge otherthan from controlled trials. As argued above, other material is essential to bridge thegap between information from an ideal therapeutic situation and the application ofsuch knowledge in a difficult patient.Publication in national Drug Bulletins and issuing notices on special websitesshould be considered. In this context the US FDA has recently published proposalsregarding improvements of the SPC.(6) Doctors must make decisions on the relative effectiveness and risks of thetreatments they advise for their individual patients. There needs to be much morethought about how to support this essential function. The UK’s National Institutefor Clinical Excellence (NICE) can be seen as a way forward in this respect, for the
173
introduction of new therapies. NICE tackles the difficult issue of reconcilingrelative effectiveness and cost; and issues guidelines, not mandates. A recent reviewof its work so far was positive, although indicating that the magnitude of the tasksfacing NICE is great. The main challenge was seen as providing comprehensivetreatment guidelines into which context any new treatment must be fitted.(7)Similar initiatives have been developed in the US (Centers for Education andResearch on Therapeutics) and The Netherlands (‘Standards’ of The NetherlandsSociety of General Practitioners).
3. CommunicationCommunication is a two-way loop; one must ensure that information is received,understood and acted upon correctly before a communication can be said to havebeen successful.There is much to be done in the area of communication, both in terms of follow-upand understanding of health professionals’ behaviour and how to empower bestpractise. In the Erice Report on drug safety information it is stated that ‘drug safetyinformation must serve the health of the public’.(8) The Erice Declaration alsocommends the idea of actively communicating uncertainty. This is a difficult issue,but in the safety area it has a good deal to recommend it because of the tentativeinformation about many even serious adverse drug reactions.
4. Professional Freedom and Professional ResponsibilityPhysicians and pharmacists have enjoyed great professional freedom. Given theexperiences already described, one needs to ensure that information and systemssupport such freedom. This requires that more attention be given to the feedbackparts of the communication loop mentioned in section 3. More stringentapproaches need to be set in place to find out about deviations from SPCs. Off-labelprescriptions need to be documented and any adverse effects should be reported.The impact of a change in the content of an SPC or a ‘Dear Doctor letter’ will begreater when these conditions are fulfilled, since they will reflect rather than forceclinical practice.
4.4.5 Contribution of pharmacistsThe dispensing pharmacist can play an important role in the implementation ofwarnings and contraindications. Increasingly, pharmacists consider providingpharmaceutical care a part of their professional responsibilities.(9) As withprescription of drugs, dispensing drugs cannot be noncommittal. Pharmacies indeveloped countries have sophisticated computer tools that help them monitordrugs for known interactions, contraindications and other important informationcontained in the SPC. To be able to monitor the indication for which the drug is
174
being prescribed, the pharmacist needs to be informed of the physician’s indicationsfor prescribing the drug. In practice this is as yet rarely the case and many healthprofessionals object to providing this information. Jones et al. conclude in theirstudy that in 89% of the cases in which cisapride had been prescribed inconjunction with a contraindicated drug, both drugs had been dispensed by oneand the same pharmacy.(1) Pharmacists need to be given a pivotal role in thesurveillance of the safe use of drugs.
4.4.6 ConclusionAlthough careful attention is being paid to the contents of SPCs and ‘Dear Doctor’letters it has become clear that this is not enough. There is a gap between thedetermination of an SPC and daily practice. Creative, not a legalistic ways need tobe found that will fill that gap to the benefit of all concerned parties: professionals,registration authorities, pharmaceutical companies and above all: the patientinvolved.
175
References
1. Jones JK, Fife D, Curkendall S, et al. Co-prescribing and co-dispensing of cisapride andcontraindicated drugs. JAMA 2001;286:1607-9.
2. Weatherby LS, Walker AM, Fife D, et al. Contraindicated medications dispensed withcisapride: temporal trends in relation to the sending of ‘Dear Doctor’ letters.Pharmacoepidemiol Drug Saf 2001;10:211-8.
3. Graham DJ, Drinkard CR, Shatin D, et al. Liver enzyme monitoring in patients treated withtroglitazone. JAMA 2001;286:831-3.
4. Jabaay L, Stokx LJ, Bakker DH de. Artrosemiddel in de lift. Med Contact 2001 56:1493-6.
5. Edwards IR, Wiholm BE, Martinez C. Concepts in risk-benefit assessment: a simple meritanalysis of a medicine. Drug Saf 1996;15:1-7.
6. Food and Drug Modernization Act (FDAMA). Public Law 105-17.
7. Raftery J. National Institute for Clinical Excellence (NICE): faster access to moderntreatments?. Analysis of guidance on health technologies. BMJ 2001;323:1300-3.
8. International Conference on Developing Effective Communications in Pharmacovigilance.Effective communications in pharmacovigilance, the Erice report: Report of the Conferenceon Developing Effective Communications in Pharmacovigilance; 1997 Sep 24-27; Erice, Sicily.WHO Uppsala Monitoring Centre, Uppsala 1998.
9. Grootheest AC van, van Puijenbroek EP, de Jong-van den Berg LT. Contribution ofpharmacists to the reporting of adverse drug reactions. Pharmacoepidemiol Drug Saf2002;11:205-10.
176
5General discussion and perspectives
Chapter 5.1Improving pharmacovigilance
In this concluding chapter we shift our attention from the more specific aspects ofpharmacovigilance to the broader, contextual picture with particular emphasis onfuture developments and the role of the pharmacist in all this.In the literature the generation of signals is commonly seen as pharmacovigilance’score task. This indeed has long been the main activity of the professionals working inthis field. Once new signals of adverse drug reactions (ADRs) had been identified,sometimes confirmed by additional (epidemiological) research, they could be weighedagainst the benefits of the treatment and, if necessary, measures could be taken. However, pharmacovigilance is far more than mere signal generation and it is theseother facets of pharmacovigilance that are even more likely to prevent harmfuleffects to patients and the economy. 1. By continuously drawing attention to (the possibility of) adverse reactions to
drugs, physicians are also induce to include suspected ADRs in their differentialdiagnoses at an early stage, thus expediting an appropriate response, whichfrequently implies that the treatment is discontinued. In this way unnecessaryand expensive diagnostic tests can be avoided and the time patients spend in thehospital could be shorter. The physicians’ and pharmacists’ awareness of adverseevents is raised.
2. Raising the awareness of ADRs also is an important instrument to promoterational and safe prescription practices. Again, pharmacovigilance can help toprevent detrimental health effects and control public health expenditure. Giventhat only a limited number of new drugs is released every year and that todaythere is every reason to be conscious and economical when prescribing drugs.Apart from the drug’s effects, the profile of its adverse reactions can be animportant consideration for doctors in their choice of drug therapy.
In other words: awareness of adverse drug reactions may significantly contribute toprudent and sensible prescription practices. This is all the more relevant since it hasbeen shown that about half of all adverse events are avoidable.(1,2) The pointsmentioned above, i.e. enhancement of the status of ADRs in differential diagnosesand promotion of ADRs as the foundation for a rational and careful prescription ofdrugs, illustrate that the impact of pharmacovigilance on a prudent and safe use ofdrugs is much greater and that its scope is far wider than the mere detection ofunknown adverse events.
179
It was also the premise that awareness of and a deeper insight into ADRs,specifically by the enhancement of doctor-pharmacist interactions, wouldpositively affect pharmacotherapy, that lay at the heart of the decision to found theNetherlands Pharmacovigilance Centre Lareb.(3)
Developing pharmacovigilanceThe safety of drugs, and thus pharmacovigilance as the scientific and practicalenvironment for the implementation of drug surveillance, did not receive systematicattention until the disastrous thalidomide episode in the early 1960s. We now havethe third generation of scientists that is dedicated to this field. To prevent any newtragedies from occurring, and within a short space of time, its pioneers were able todevelop a methodology that, based on the daily experiences of the medical practice,made it possible to detect ADRs that had not come to light during the pre-marketingclinical trials, which tests have since been made compulsory. The method wasfounded on a spontaneous reporting system (SRS), which in several countries wassupplemented by a system of Intensive Monitoring. In addition to the practicalimplementation, as formulated in the WHO Technical Report in 1972, which hadfrom an organisational point of view already taken shape in the collaboration of tencountries participating in the WHO International Drug Monitoring Programmelaunched in 1968, the scientific underpinning of the activities has also received dueattention. Finney specifically pointed to the significance of individual cases and theirstatistical relevance.(4) Inman has specified practical solutions for theimplementation of the concept of Intensive Monitoring.(5) In the various reports it has issued, the Council for International Organisations ofMedical Sciences (CIOMS) and the International Conference on Harmonization(ICH) have laid down the regulatory terms the pharmaceutical industry needs tocomply with. The knowledge about ADRs has increased markedly over the years,which is for a large part due to the significant contribution of clinicalpharmacologists and to a lesser degree clinical pharmacists. Pharmacoepidemiologyhas been the main forum for the theoretical underpinning of the importance ofdatabases in which international organisations like the International Society ofPharmacoepidemiology and the International Society of Pharmacovigilance haveplayed a major role. Noteworthy in this context is that in a number of countries,among which the Netherlands, toxicology and teratology, both essential fields foreffective drug safety monitoring, have evolved separately from pharmacovigilanceand have remained independent from the ADR surveillance systems.
Advances in pharmacovigilance are made at a fast pace and concern both thedelineation of its field of knowledge and methodologies as well as their practicalimplementation. Especially with respect to the applications of related disciplines
180
such as clinical pharmacology, (pharmaco)epidemiology, toxicology and teratology,areas like pharmacy and health sciences are increasingly gaining in influence. Issues likely to determine pharmacovigilance in the immediate future are:
- Increasing the volume and enhancing the quality of ADR reports- The role of computerisation - Prospective planning - Applying new knowledge
These issues will be discussed in the next sections.
Increasing the volume and enhancing the quality of ADR reportsIn the light of the arguments made in Chapter 2.4 in reference to Underreporting wewish to stress once again that, especially in countries in which the pharmacovigilancesystem has been firmly rooted, inviting more reports is not the ultimate goal. What isimportant is to gather a sufficient amount of qualitatively sound signals that will allowa reliable surveillance of the safety of drugs. Apart from a continuous monitoring ofall marketed drugs it is essential to obtain information on the possible risks of newlymarketed drugs during normal use as quickly as possible. In our description ofIntensive Monitoring (Chapter 4.1) we outlined a practical method that, by making useof pharmacists’ computerised systems, may provide a fast and accurate first impressionof prescription practices, the indications for which the drug has been prescribed and,if implemented on a larger scale, possible or likely adverse events.
- The role of the National Pharmacovigilance CentreThe thesis by Lindquist shows that, on a global scale, the countries which haveoperated a SRS for some length of time contribute most to pharmacovigilance.(6) Aprerequisite for effective pharmacovigilance is continuity. Potential contributorsneed to be continuously made aware of the importance of reporting suspectedADRs. Moreover, they need to be (made) familiar with the national reportingsystem, which implies that systems should not be subjected to continuous changes. National pharmacovigilance centres sometimes underestimate the importance ofpublic relations and the vital role these play in supporting their other activities.Only if the system’s goals and relevance are advocated systematically and over longperiods of time it will be possible to raise the number and quality of ADR reports.Rather than promoting the centre itself campaigns should be aimed at raising theawareness of ADRs and stress the relevance of systematic attention for ADRs in theday-to-day practice of physicians and pharmacists.(7)
- Promoting and enhancing ADR reportingAs detailed in Chapter 3.2 ample research has been conducted into the motivesunderlying the physician’s and pharmacist’s decision whether or not to report,
181
if indeed reporting is even considered as an option. Here it is essential to exploit theprofessional expertise and to link with the scientific interest potential contributorsmay have.(7) In addition to motivation practical considerations also play animportant role.(8) The format of the reporting form should elicit a response andaccommodate for easy completion. Alternative ways to report ADRs should also betaken into account. One could, for instance, allow the correspondence betweenhealth professionals, detailing the required information, to be submitted. Apartfrom facilities to report via e-mail and websites, the computer systems of generalpractitioners, pharmacists and hospitals can be supplemented with an electronicreport module. Implementation, however, may pose problems. The NetherlandsPharmacovigilance Centre Lareb has had ample experience with such integratedmodules and found that particularly the lack of uniformity in hospital systemsproved a major obstacle. Still, both in terms of volume and quality of ADR reportsas well as in terms of efficiency the system looks promising.
- Reporting by patientsIn Chapter 4.3 on Consumer Reporting we discussed direct reporting by patients.Although at international level the merits of patient reports are being considered, todate the literature does not yet provide any actual results in relation to the detectingof adverse drug reactions. Patient interest in the safety aspects of drugs is great asthe reactions to the side effects of Diethylstilbestrol (DES) and the discussionsabout negative experiences with benzodiazepines and antidepressants have shown. The Netherlands Pharmacovigilance Centre Lareb has recently added a special pageto its website, inviting patients who prefer to do so to report their suspicions ofadverse reactions direct to Lareb (www.meldpuntbijwerkingen.nl). However, thisdoes require them to provide full details to allow Lareb to make a well-foundedevaluation of the relationship between the suspected ADR and the drug mentioned.Patients are also requested to send in (post-paid) a signed print-out of their report,giving Lareb their consent to make further enquiries with their doctor(s) orpharmacist, if necessary. This pilot project is aimed at exploring, by assessing theirquality, whether patient reports may indeed add to the existing knowledge of ADRsor may help to accelerate the detection process. Since also direct patient reportingpharmacovigilance is about enhancing the existing knowledge, other objectivessuch as patient empowerment fall outside the scope of pharmacovigilance.
- FeedbackThe parties that have submitted the report, which, at present, usually concerns adoctor or pharmacist, also need to be informed that the report has been dulyconsidered and should therefore be supplied with a prompt and expert assessment.This feedback also functions as éducation permanente for the sender. By no means
182
all reports lead to new ADR signals, nor is it possible to indicate precisely whattype of reports will actually add to our knowledge. Sometimes it takes years beforean unsubstantiated suspicion is corroborated. This is why all reports need to betaken seriously and why it is essential that the information they contain isdocumented properly. It is recommended to also inform those who havecontributed to the detection of a new signal by submitting their report, for instanceby sending them the publication, in which their information is used for such.New ways to communicate feedback and disseminate new information should beconsidered, e.g. via the Internet. During a debate in the European Parliament on thefuture of pharmacovigilance in Europe it has been stressed to make the collectivedata more accessible to the public. In a recent report the Heads of Agencies of theEMEA (European Medicines Evaluation Agency) have also expressed thedesirability of a ‘dialogue with reporters’.(9) Thus, any findings regarding the safetyof drugs should be made accessible not only for those whose efforts havecontributed to the detection of the signal but for all interested parties, including theusers of drugs. In practice this implies that the data that are made available on the Internet shouldinform the public of the incidence of specific adverse reactions in such a way thattheir correct interpretation does not require any knowledge of the principles ofcausality assessment and statistics. Both at national and European level stepstowards achieving this new information platform are being taken.
The role of computerisation in pharmacovigilanceIt takes more than scientific expertise and ambition to make pharmacovigilanceeffective. Several preconditions, mainly at the managerial level, need to befulfilled.(10) This includes an automation system that is constantly refined and keptup to date.From its start pharmacovigilance has set great store by the use of computers. Asearly as 1972 it was stated that ‘adequate computer facilities are essential if anational monitoring centre is to reach full development’.(11) A number ofapplications that were first recommended 30 years ago, among which ‘rapid fileretrieval for signalling potential new drug hazards’ and storage of first and follow-up reports, are still highly relevant today. Techniques for statistical analyses,specifically in relation to user rates, were proposed and the importance ofinternational compatibility and standardisation of terminology stressed. Possibly,the advances in the field of automation are not as swift as often supposed. Next,some applications of advanced ICT technologies in pharmacovigilance will bediscussed in brief.
183
- Quantitative signal detectionA promising technique to find new signals in large datasets that do not come tolight in a case-by-case analysis is to look for the disproportionality of ADRs inrelation to drugs. The size of today’s datasets and the periods covered now alsoallow us to find drug-drug interactions and associations between ADRs. Variousstatistical methods can be applied for this purpose.(12,13,14) The NetherlandsPharmacovigilance Centre Lareb uses one of these methods in their weeklyassessment meetings.(15)
- EudravigilanceThe EMEA has given priority to drug safety for which setting up its own databaseof ADR reports, known as Eudravigilance, is seen as vital. Expectations are highsince such a Eudravigilance environment will offer many advantages and willprovide structure to the exchange of reports between EU member states.Nevertheless, the database is no more than a collection of reports and as such doesnot provide the much needed answers to the problems surrounding the detection ofADRs and the communication facilities that are required once an ADR has beendiscerned. Human intelligence, creativity and particularly expertise areindispensable to formulate the right questions and to evaluate likely solutionsadequately. It is essential to always return to the individual cases on which thestatistical findings are based. And finally, it should be noted that the Eudravigilance databank is a subset of theWHO databank and consequently the sum total of national databanks and itquestionable how much new information will come out of it. Promoting andcollecting ADR reports and the analysis of the data and subsequent signalgeneration will always remain a task to be conducted at the national level.(9)
- The use of health-care computer systemsIncreasingly, use is made of the information contained in the various databanks ofthe national health care systems. An example is the GPRD (General PractitionersResearch Database) in the UK, now managed by the Medicines Evaluation Agency,which is frequently consulted for information relating to the safety of a particulardrug. In the Netherlands there are several databases available for epidemiologicalresearch, as there are PHARMO (Utrecht), IPCI (Rotterdam) and the InterActieDatabase (Groningen).(16) It is recommended that national pharmacovigilance centres promote the integrationof report modules in the computer systems operated by general practitioners,pharmacists and hospitals. In this way it will be possible to link the data of thesevarious systems to a suspected ADR and to pass the combined data to thepharmacovigilance centre.
184
Prospective surveillance and risk managementThe raison d’être of a Post Marketing Surveillance System is the fact that the clinicalpre-marketing trials of a drug generate a limited amount of information about thedrug’s associated risks.(17) Most of these findings are included in the Summary ofProduct Characterisation (SPC). However, there is safety information that does notmake it to the SPC, even though it may be relevant for pharmacovigilancepurposes.(18) Until recently, access to this type of information was limited and atbest the data are included in the application dossier that is submitted to theregulatory authorities, which file is also not accessible for the general public. Today,the pharmaceutical company (i.e. the Marketing Authorisation Holder) that seeksapproval of a new product is required to also submit a ’pharmacovigilancespecification’ indicating potential risks.(9) This enables the regulators to specifyadditional conditions for the drug’s surveillance, which generally entails targetedepidemiological research. Drug-safety monitoring methods such as thespontaneous reporting system employed in pharmacovigilance may also devoteextra attention to these potential risks. It is recommended to involve (post-marketing) pharmacovigilance experts in the pre-marketing risk assessments. This pro-active surveillance is part of a new approach in pharmacovigilance alsoreferred to as ‘Risk Management Strategy’.(9,19). 'The drug development processmust incorporate early thinking and planning for risk management, integrating riskmanagement into the early stages of the product lifecycle, beginning well beforelaunch’.(20)Both in the USA and in Europe steps have been taken to formulate a concrete riskmanagement policy.(9,20) The International Commission on Harmonisation (ICH)has also announced plans for the development of a guideline on ‘prospectiveplanning of pharmacovigilance’.(21) Europe seems to lead the pack in realising the proposed plans. Here, riskmanagement is defined as ‘the identification and implementation of strategies toreduce risk to individuals and populations’.(9) The basic idea is that for eachproduct, starting with new products for which marketing approval has beenapplied, a product risk management plan is to be drawn up and submitted. Table 1lists the elements such a plan needs to cover. We do need to prevent regulations like these from causing bureaucratic red tape:their aim should be the identification of potential risks and any subsequentmeasures and not meeting regulations, as is now sometime the case, for instancewith the obligation to sent in serious reports within 15 days.
Implementation of new knowledgeIn the Introduction a circle was used to represent what pharmacovigilance is allabout. In the past the emphasis was mainly on deriving knowledge from the
185
experiences made in the clinical practice. However, implementing this newinformation, i.e. applying the acquired knowledge in practical situations allowingthe individual patient to benefit from these new developments, is equally important.In Chapter 4.4 on Labelling it is concluded that we fall short in this respect.Practical measures are mostly restricted to scientific publications whose impact onthe daily practice or regulation is often not immediate, and frequently merely leadsto a moderation of the content of the Summary of Product Characteristics (SPC) orthe distribution of a ‘Dear Doctor letter’. In the more serious cases the marketingauthorisation for the drug involved will be withdrawn. This latter measure wastaken relatively frequently in the past decade, which has prompted a debate onwhether the decisions were always justified.(22) Medication that may constitute arisk for a particular population might be the appropriate treatment for othergroups. There have been cases where drugs were taken off the market becausewarnings were not issued or precautionary measures were not taken.(23,24)Because the regulatory authorities cannot afford to take risks, in a number of suchcases it was decided to withdraw the marketing authorisation. To change these practices will require much effort. The development of newactivities like prospective pharmacovigilance and risk management as mentioned inthe previous section are the first expressions of such a change. However, it isessential to not only assess a drug in terms of its risks but also in terms of its merits.In other words: one should balance the drug’s intrinsic value per case against itslikely harmful effects, preferably also at an individual level. This will lead to a morethorough assessment of the risks involved than when evaluations are merely basedon numbers and averages.(25) The criticism that has been levelled at drug approvalagencies like the FDA in the USA and the MCA in the UK in recent years showsthat this is no easy matter. Chapter 4.4 (‘Labelling’) also provided a number ofpossible solutions to help change the perception of adverse drug reactions. The aimis to enhance the knowledge doctors, pharmacists and consumers, as well as thoserepresenting the consumer at a political level, have of drugs, both with respect tomedical-pharmaceutical aspects and risk perception. The training programmes formedical students and pharmacists should devote more space to pharmacovigilance.And, as indicated above, existing knowledge should be enhanced and made moreeasily accessible for all parties concerned. Only then will we be able to translatewhat we know into practical applications and will drugs be prescribed at a moreindividual basis than is common today. It is the task of pharmacovigilance to supplythe building blocks, making use of both established and new scientific areas,possibly with pharmacogenetics in a prominent role.
186
Chapter 5.2Independent pharmacovigilance
This thesis has been written within the setting of the NetherlandsPharmacovigilance Centre Lareb, which is no coincidence because Lareb offersboth the practical and scientific environment within which applied pharmaco-vigilance research can flourish. The precondition that such an environment should be impartial is fulfilled sinceLareb is an independently operating foundation. Its activities, thoughcommissioned and funded by the national government and does its task on behalfof the Dutch Medicines Evaluation Board, are controlled by a board whosemembers all belong to medical organisations and pharmacists’ and patients’associations. It is therefore not surprising that the theme of the 2001 conferencecelebrating Lareb’s 10th anniversary was ‘independent pharmacovigilance’. In her thesis Lindquist remarks that pharmacovigilance is especially effective incountries where its centres have been in existence longer.(6) The second key factorto success proved to be their independence.(26) It is striking that particularly incountries where the pharmacovigilance systems are essentially autonomous thecentres make the most significant contributions. Besides Lareb, this is illustrated bythe Intensive Medicines Monitoring Programme (IMMP) in New Zealand andother independent institutes like the WHO’s Uppsala Monitoring Centre and theDrug Safety Research Unit (DSRU) in Southampton, England.(27,28) A pharmacovigilance centre has dealings with various bodies and organisations.Next, we will take a closer look at some of the main parties.
- The national governmentIt was the legislation which the various national governments adopted in the secondhalf of the previous century that provided the framework for the development ofpharmacovigilance. Within the context of public health care the authorities areresponsible for the surveillance of the efficacy, safety and quality of drugs. Since the1960s the national and international rules have been further refined and criteria andprocedures have been carefully formulated. For the main part the guidelines forregulatory pharmacovigilance were drawn up by the CIOMS and ICH in which themajor industrialised countries and governments participate.However, there is the risk of over-regulation: compliance with such a multitude ofrules and regulations may require so much time and effort that one may lose sightof the original aims and objectives. For instance, pharmaceutical companies are
187
required to report serious adverse events that have come to their attention within a15-day limit. This is so short that much of their efforts are spent on achieving thesestatutory perimeters, which sometimes goes at the cost of the report’s actualcontent. Also this matter clearly needs to be looked into. With respect to the, ideally, independent position of pharmacovigilance anotheraspect concerning the role of the authorities needs mentioning. The government hasmany tasks, and these include policies on medicinal drugs. Among other issues,drug approval, reimbursement of medication-related costs and economic aspectsfall under their responsibilities. Seen against this background it is crucial forpharmacovigilance to have a fair degree of autonomy to ensure that the collectionand analysis of ADR reports and the dissemination of the knowledge attained doesnot suffer too much from government interference. Of course it is theresponsibility of the national authorities, i.e. the Health Inspectorate, to oversee thequality of the pharmacovigilance activities.
- The pharmaceutical industryMedicinal drugs, pharmacovigilance’s object of study, are the products of the effortsof the pharmaceutical industry. As indicated earlier, basically, for the larger part oftheir ‘life cycle’ drugs are an economic product and pharmaceutical companies arequite influential when it comes to the therapeutic chain.(29) Also in relation to the monitoring of product safety, the companies have their ownresponsibilities, both with regard to the health and ethical aspects of their activitiesas well as the commercial and legal implications. The sector has increased its effortsand expanded their pharmacovigilance activities. This is partly in response to newand more stringent rules and the increased supervision on their implementation,and partly due to the fact that the number of new chemical entities that the sectorreleases has become smaller, offering the industry more scope to monitor theirmarketed products more closely.The methods employed to gather reports on ADRs differ per country. In a numberof countries, among which the USA, Germany and Sweden, the majority of thereports the national pharmacovigilance centres receives stem from thepharmaceutical industry. In most other countries this is less common and here mostreports are sent in by doctors and pharmacists. Generally, this is the favouredsystem, provided that there is an adequate exchange of information between thecentres and the industry. There are no grounds why doctors, pharmacists orpatients should report their observations to the pharmaceutical companies and havethem pass on the reports to the national centres. Direct reporting is faster andaffords the national pharmacovigilance centre the opportunity to contact the senderto obtain any additional information it may need. Moreover, the reports theindustry submits tend to be of inferior quality compared to those of doctors and
188
pharmacists.(30) Having several routes may also be confusing for potentialcontributors.
- UniversitiesThe field of pharmacovigilance is associated with several academic disciplines, morespecifically clinical pharmacology, clinical pharmacy and pharmacoepidemiology aspart of the medical and pharmacy faculties. Pharmacovigilance may be seen as anindependent science with its own paradigm, methodology, rationale and history. Asyet there are no separate chairs for pharmacovigilance where an integrated approachto the questions surrounding drug safety can be developed on the basis of thisparadigm.(31) In some countries, for instance France and Italy, academic centres do,however, fulfil the role of regional reporting systems.
- Professional groups and patientsThe safety of drugs and more specifically their adverse effects are of equal concernto physicians, pharmacists and nurses - in their professional capacity- and patients.The doctor decides on the type of drug to be used, involving the pharmacist andnursing staff each in their own capacity.(32,33) The patient is the one who uses thedrug. Thus, all parties have a direct involvement in the care provided and are notconcerned with the commercial aspects of the medication. Their professional and personal interest in the care aspect of drugs and their directinvolvement in their use make health professionals and patients the most likelypeople to exercise responsibility for the practical implementation of drug safetysurveillance. In between all these parties pharmacovigilance needs its own independent place.
189
Chapter 5.3The role of the pharmacist
It was the role the pharmacist plays or should play in pharmacovigilance that sparkedthe present thesis. In several chapters the various aspects of this role were discussedin detail. As was concluded in Chapter 3.1, pharmacists indeed have a prominent roleto play with respect to knowledge as well as attitude and commitment, and theircontribution is already substantial in many countries. It is recommended to increase their participation especially in those countries wherethey are not authorised to report or where their contribution is limited. In severalcountries, specifically in the Scandinavian countries, this means that pharmacists needto be acknowledged as independent reporters of ADRs. In other countries the formalacknowledgment needs to be followed up by measures to enhance their actualparticipation. Modifications of the pharmacy curriculum are required as well aschanges in the interpretation of the pharmacist’s scope of duties. The attitude doctor’stake towards the profession is also in need of change. As Wade wrote in 1970:‘Doctors should learn to make use of the pharmacist’s knowledge and skills’.(34)The rationale for founding Lareb was the idea that the pharmacist might fulfil acoordinating role in the detection of ADRs and that the collaboration betweendoctors and pharmacists would significantly enhance pharmacotherapy.(9) Generalpractitioners and community pharmacists have already made considerable headwaytowards intensifying their collaboration. In Chapter 3.3 we showed that the pharmacists’ share in the total number of reportsLareb received during a period of five years was substantial, as was their qualitativecontribution. The pharmacist reports, in the Netherlands chiefly originating fromcommunity pharmacists, have their own specific characteristics, which makes thema valuable addition to the reports received from physicians. When we look at theway the pharmacists perceive their role in ADR reporting, as was done in Chapter3.2 we find that they are not only highly motivated but also consider it an integralpart of their professional duties. In Chapter 3.1, an overview covering a largenumber of countries participating in the WHO International Drug MonitoringProgrammes demonstrated that the quantitative contribution pharmacists make tothe national systems is small. Clearly, on a global scale major improvements can bemade and the extent of ADR underreporting can be considerably reduced byactively involving pharmacists in the surveillance of drug safety within the contextof the pharmaceutical care they provide. That their contribution can indeed becrucial was illustrated in Chapter 3.4 by an article on Yasmin®. Here a well-
191
documented report that a community pharmacist had submitted led to animportant message for prescribers and others parties concerned.
- Hospital pharmacists in the Netherlands lagging behindIn the Netherlands, and possibly in many other countries as well, a great dealremains to be done at the hospital level. The volume of reports from Dutchhospitals is relatively low.(35) Hospital pharmacists, who often take a keen interestin the scientific aspects of their profession, could exert their influence when itcomes to raising awareness of ADRs within the context of patient care. Particularlyin complicated circumstances their expertise is insufficiently put to use.Exploitation of their know-how and experience could prevent much harm. Theycould also contribute to ADR reporting in a coordinating capacity, as is the case inthe US and Canada.(36,37) However, the status of the hospital pharmacist as anexpert and co-consultant in pharmacotherapy needs to be acknowledged first. It isrecommended to incorporate this task description in the regulations, e.g. thepolicies regarding quality control, that oblige hospitals to provide good qualityADR reporting procedures. The medical insurance providers in the US and theassociation of hospital pharmacists in Canada have made this a precondition. In theNetherlands the first steps have been taken to draw up such a task description forthe hospital pharmacist but it will still take quite some time before a structured oreven mandatory plan will become effective.(38)
- The contribution of pharmaceutical sciences to pharmacovigilanceThe contribution of the pharmacist, or rather pharmacy, to pharmacovigilanceshould not be limited to the above-mentioned aspects. The various pharmaceuticaldisciplines could also greatly enhance our understanding of the nature of adversedrug reactions. For the detection and assessment of possible ADRspharmacokinetics, pharmacodynamics, and knowledge of chemical relations areoften indispensable. However, within these fields adverse reactions to drugs havenot received systematic attention and their contribution to pharmacovigilance isconsequently still rather limited. Here, again, there is room for improvement bothwith respect to the proactive and passive surveillance of ADRs. If those involved inpharmacy can rise to this challenge, they will significantly help deepen our insightsand widen the scope of pharmacovigilance.
192
Chapter 5.4Pharmacovigilance as a scientific discipline
In the Introduction part of this thesis an attempt was made to definepharmacovigilance as a scientific domain in its own right with its own specificmethodology. As its core tasks we have mentioned deriving knowledge from theclinical practice and the subsequent development of techniques to implement thisnew information. In the last few years much has been achieved as far as the first taskis concerned. Chapters 2.1 and 2.2 were dedicated to the history of pharmaco-vigilance. In Chapter 4.4 we have listed the many items that are still on the agendawith regard how to implement the second task. In this section we will elaborate this latter issue as well as the contributions Larebhas made in further delineating the science of pharmacovigilance. Starting from twoconcepts, i.e. the importance of case studies and a positive view on the risk aspectof drugs, we will catalogue several facets that need to be attended in order toadvance pharmacovigilance as a scientific discipline.
- The contribution of the Netherlands Pharmacovigilance Centre LarebThe Netherlands Pharmacovigilance Centre Lareb, formerly known as theNetherlands Pharmacovigilance Foundation Lareb, has made significantcontributions to the development of pharmacovigilance. To illustrate this we wouldlike to specifically mention four dissertations. In 1994 G.H.P. de Koning receivedhis PhD for his thesis on the development of a regional reporting system foundedon the collaboration of pharmacists and general practitioners and aimed atsupporting pharmacotherapeutic interventions.(3) In 1997 A.C.G. Egbertspublished his combined studies on the sources, detection and interpretations ofsignals, based on his findings on antidepressants.(39) Also R.H.B. Meyboom, whodescribes the Dutch contributions to pharmacovigilance, has had significant impactespecially on the theoretical underpinnings of pharmacovigilance.(40) He writes:‘This thesis aims at increasing our understanding of the scientific basis ofpharmacovigilance’. His work has indeed fostered the development of the modelsfor signal detection, causality assessment and Good Pharmacovigilance Practice. Inhis thesis published in 2001, E.P. van Puijenbroek describes various methods for thedetection of quantitative signals in extensive ADR databanks that can be applied forthe detection of adverse drug reactions as well as drug-drug interactions andsyndromes, i.e. an aggregate of associated symptoms resulting from the use ofdrugs.(41)
193
Pharmacovigilance’s distinguishing features The characteristics that distinguish pharmacovigilance from other fields deservespecial mentioning. In Chapter 2.4 it was demonstrated how a specific pharmaco-vigilance-based approach can prevent ambiguity, as was illustrated by the variousinterpretations given to the term underreporting. Two aspects of drug safety that warrant a special pharmacovigilance-basedapproach in the near future are research on the basis of cases and the risks associatedwith drugs.
- The individual case as the foundation for pharmacovigilanceThe first aspect concerns the significance of the individual case. The fact that atragedy of enormous proportions lay at the root of the advent of pharmacovigilanceand that surveillance of drug safety was primarily seen as a matter of public healthmay have caused the epidemiological side of pharmacovigilance to be given priority.Also the fact that regulatory authorities prefer to base their decisions on numberslike incidence rates, and their decisions always affect large patient groups or eventhe entire population, may have played a role here. And more recently, the potentialimpact of automated data processing and the systematic analysis of large datasets ondrug safety monitoring has raised the expectations for this aspect even further.Nevertheless, ultimately it will always be the individual, the single case that lies atthe heart of pharmacovigilance. It was Claude Bernard who stated that there was nosuch thing as the average patient.(42) Whether the aim is tracing new adverse effectsor finding practical applications for the newly acquired knowledge, it is theindividual patient that should be the subject of attention. In ADR detectionaverages and anonymous data covering larger samples could never be thefoundation on which conclusions are based. Rather, on the basis of individual casesit needs to be assessed whether the data on which conclusions are drawn arecorrect.(43)The same principle applies to the implementation of new insights: althoughdecisions may be right for the average population, they may be less favourable forthe individual patient or smaller categories of patients. When drugs that may be oftherapeutic value for particular patient groups are taken off the market too quicklythis may cause unnecessary harm. Methods need to be developed to prevent this.Paradoxically, the drug that best illustrates this need is thalidomide, the very drugthat shook the foundations of the pharmaceutical world, as was described inChapter 2.1, has nowadays find a new place in pharmaceutical therapy.(44,45,46)Innovations should not only include such areas as education, communication andlegislation, but possibly also the field of pharmacogenetics and pharmacotherapyethics.
194
- The risk aspect of drugs It is an old axiom that says that basically each drug is a poison and that it is the dosethat predominantly determines its therapeutic effect. Despite the many benefits thepharmacotherapeutic innovations have brought in the previous century, thefundamental attitude towards drugs has been one of scepticism, which seems tohave become more pronounced in the last few years. In their ‘future model ofpharmacovigilance’ Waller and Evans have proposed that, rather than trying toidentify risks, pharmacovigilance’s central theme should be about demonstratingsafety.(31) Although it seems as if they were merely toying with two sides of thesame coin, there is more to it than that. The authors stress that, based on aprospective approach we first need to gain insight into the level of safety that hasalready been demonstrated, before we investigate any possible concerns. Thus, theirmodel provides a better idea of a drug’s safety on which its application in the clinicalpractice can be based. This model does imply that doctors need to be cautious whenprescribing new drugs.(47) The benchmark should be the drugs proven safetyrather than it’s proven risks! It is strange that we give a new drug the benefit of thedoubt based on relatively few hard facts and start experimenting with it in the realworld. The reverse approach, i.e. to balance the expected health benefits of a drugwe wish to prescribe against the available data on its safety, seems far more rational.If little is known about the safety of a newly marketed drug, the risk will often beconsidered too high (and will thus become too much of a gamble), which will tipthe balance in favour of a more established treatment for which more evidence isavailable and whose safety records are well-documented. It needs to be noted thatthis model is already applied for the unborn child in the risk assessments of drugsused by the mother.
In the coming years it will be pharmacovigilance’s main challenge to further defineand refine its mission, its paradigm, its methodology and the implementation ofknowledge in both the clinical and pharmaceutical practice.
195
References
1. Lazarou J, Pomeranz BH, Corey PN. Incidence of Adverse Drug Reactions in HospitalizedPatients. JAMA 1998;279:1200-5.
2. Lee A, Bateman DN, Edwards C, Smith JM, Rawlins. Reporting of adverse drug reactions byhospital pharmacists: pilot schema. BMJ 1997;315:520-23.
3. Koning GPH de. A regionalized spontaneous surveillance program for adverse drug reactionsas a tool to improve pharmacotherapy. Thesis. Utrecht University, Faculty of PharmaceuticalSciences, 1994.
4. Finney DJ. The detection of adverse drug reactions to therapeutic drugs. Stat Med 1982;1:153-61.
5. Inman WH. Postmarketing Surveillance of adverse drug reactions in general practice.II:Prescription-event monitoring at the University of Southampton. BMJ (ClinResEd)1981;282:1216-7.
6. Lindquist A.M. Seeing and Observing in International Pharmacovigilance. Thesis. KatholiekeUniversiteit Nijmegen. Nijmegen 2003.
7. Biriell C, Edwards IR. Reasons for Reporting Adverse Drug Reactions – some ThoughtsBased on an International Review. Pharmacoepidemiol Drug Saf 1997;6:21-6.
8. Eland IA, Belton KJ, Grootheest AC van, Meiners AP, Rawlins MD, Stricker BHCh.Attitudinal survey of voluntary reporting of adverse drug reactions. Br J Clin Pharmacol1999;48:623-7.
9. Heads of Agencies. Establishing a European Risk Management Strategy – Report of the Headsof Agencies ad hoc Working Group. 2003.(http://heads.medagencies.org/heads/docs).
10. Uppsala Monitoring Centre. Guidelines for setting up and running a PharmacovigilanceCentre. UMC. Uppsala 2000.
11. WHO. International Drug Monitoring: The Role of National Centres. Technical Report SeriesNo 498. WHO. Geneva 1972.
12. Puijenbroek EP van, Bate A, Leufkens HGM, Lindquist M, Orre R, Egberts ACG. Acomparison of measures of disproportionality for signal detection in spontaneous reportingsystems for adverse adverse drug reactions. Drug Saf 2002;11:3-10.
13. Bate A. The Use of a Bayesian Confidence Propagation Neural Network inPharmacovigilance. Umeå University Medical Dissertations New Series No 846. Umeå 2003.
196
14. Szarfman A, Machado SG, O’Neill RT. Use of screening algorithms and computer systems toefficiently signal higher-then-expected combinations of drugs and events in the US FDA’sspontaneous reporting data base. Drug Saf 2002;25:381-92.
15. Puijenbroek EP van, Diemont WL, Grootheest AC van. Application of Quantitative SignalDetection in the Dutch Spontaneous Reporting System for Adverse Drug Reactions. Drug Saf2003;26:293-301.
16. Leufkens HG, Urquhart J. Automated Pharmacy Record Linkage in The Netherlands. In: In:Pharmacoepidemiology. WHW Strom, editor. John Wiley and Sons. Chichester 2000.
17. Brewer T, Colditz GA. Postmarketing Surveillance and Adverse Drug Reactions – CurrentPerspective and Future Needs. JAMA 1999;281:824-9.
18. Abassi K, Herxheimer. The European Medicines Evaluation Agency: open to criticism. BMJ1998;317:898.
19. Bortnichak EA, Wise RP, Salive ME, Tilson HH. Proactive safety surveillance.Pharmacoepidemiol Drug Saf 2001;10:191-6.
20. Perfetto EM, Ellison R, Ackermann S, Sherr M, Zaugg AM. Evidence-Based RiskManagement: How Can we Succeed?: Deliberations from a Risk Management AdviseryCouncil. Drug Inf J 2003;37:127-34.
21. Barnes J. From E2B to E2E: new ICH topic on pharmacovigilance planning. Reactions2003;950:3-4.
22. Waller P. Dealing with uncertainty in drug safety: lessons for the future from sertindole.Pharmacoepidemiol Drug Saf 2003;12:283-88.
23. Grootheest AC van, Edwards IR, Labelling and ‘Dear Doctor’ letters: are the noncommittal?Drug Saf 2002;25:1051-55.
24. Seligman PJ. ‘Dear Doctor…’- Evaluating the impact of risk communication efforts.Pharmacoepidemiol Drug Saf 2003;12:291-4.
25. Moore N, Hall G, Sturkenboom M, Mann R, Lagnaoui R, Bégaud B. Biases affecting theproportional reporting ratio (PRR) in spontaneous report pharmacovigilance databases: theexample of sertindole. Pharmacoepidemiol Drug Saf 2003;12:271-82.
26. Moore TJ, Psaty BM, Furberg CD. Time to act on Drug Safety. JAMA 1998;279:1571-3.
27. Coulter DM. The New Zealand Intensive Medicines Monitoring Programme.Pharmacoepidemiol Drug Saf 1998;7:79-90.
28. Mann RD, Wilton LV, Pearce GL, Mackay FJ, Dunn NR. Prescription-Event Monitoring in1996 – a method of Non-Interventional Observational Cohort Pharmacovigilance.Pharmacoepidemiol Drug Saf 1997;6:S5-11.
197
29. Figueras A, Laporte J-R. Failures of the therapeutic chain as a cause of drug ineffectiveness.Promotion, misinformation, and economics work better than needs. BMJ 2003;326:895-6.
30. Sills JM, Tanner LA, Milstien JB. Food and Drug Administration monitoring of adverse drugreactions. Am J Hosp Pharm 1986;43:2764-70.
31. Waller PC, Evans SJW. A model for the future conduct of pharmacovigilance.Pharmacoepidemiol Drug Saf 2003;12:17-29.
32. Grootheest AC van, Olsson S, Couper M, Jong-van den Berg LTW de. The role of pharmacistsin reporting adverse drug reaction in international perspective. Pharmacoepidemiol Drug Saf(in press)
33. Morrison-Griffiths S, Walley TJ, Park BK, Breckenridge AM, Pirmohamed M. Reporting ofadverse drug reactions by nurses. Lancet 2003;361:1347-8.
34. Wade OL. Adverse reactions to drugs. Heinemann Medical Books. London 1970.
36. Grasela TH. Hospital Drug Surveillance Networks: Ad Hoc Pharmacoepidemiological DataCollection Methods. In: Pharmacoepidemiology – An Introduction. AG Hartzema, M Porta,HH Tilsson (editors). Harvey Whitney Books Company. Cincinnati 1998.
37. CSHP. Standards of Practice. Canadian Society of Hospital Pharmacists. 1990.
38. Het melden van bijwerkingen, de rol van de ziekenhuisapotheker. [The reporting of ADRs,the role of the hospital pharmacist]. Lareb, 's-Hertogenbosch 2001.
39. Egberts ACG. Pharmacoepidemiological approaches to the evaluation of antidepressantsdrugs. Thesis. University of Utrecht 1997.
40. Meyboom RHB. Detecting adverse drug reactions, Pharmacovigilance in The Netherlands.Thesis. Katholieke Universiteit Nijmegen 1998.
41. Puijenbroek EP van. Quantitative Signal Detection in Pharmacovigilance. Thesis. Universityof Utrecht 2001.
42. Vandenbroucke JP. Clinical investigation in the 20th century: the ascendancy of numericalreasoning. Lancet 1998;352:12-6.
43. Meyboom RHB. Causal or Casual? The role of causality assessment in pharmacovigilance.Drug Saf 1997;16:374-89.
46. Ehrenpreis ED, Kan SV, Cohen LB, Cohen RD, Hanaver SB, et al. Thalidomide therapy forpatients with refractory Crohn’s disease: an open-label trial. Gastroenterology 199;117:1271-7.
47. Lexchin J. Should doctors be prescribing new drugs? Int J Risk Saf Med 2002;15:213-22.
199
201
SSummary
This thesis bears the title: 'Improving pharmacovigilance and the role of thepharmacist'. The main theme is: How can the safety of medicinal drugs bemonitored in a better way? Specific attention is paid to the role the pharmacist canplay in this process.Since the ‘Softenon tragedy’ in the early 1960s there is the awareness that drugs arenot always be a blessing, but can also mean a risk. At that time, over 10,000 childrenwere born with congenital malformations resulting from the maternal use ofthalidomide (Softenon®) during pregnancy. This is why today drugs are examinedbefore they are approved to be applied in the daily, clinical practice. They need tomeet the highest standards with regard to their efficacy, safety and quality. In theNetherlands drugs are granted their marketing authorisation by the ‘College terBeoordeling van Geneesmiddelen’ (Medicines Evaluation Board, MEB), frequentlyin European context. Since the 1960s doctors and pharmacists are also requested to report suspected sideeffects or adverse drug reactions (ADRs) in order to prevent a disaster like theSoftenon tragedy from occurring again. Under the authority of the MEB theNetherlands Pharmacovigilance Centre Lareb collects and analyses the reports onpossible adverse events and reports back to the MEB. Drug safety monitoring, bya close surveillance of the risks associated with the use of drugs, is essential becauseat the time when a drug is granted a marketing authorisation the practicalexperiences with the product are still limited. Only when it is used by many andunder all kinds of different circumstances is it possible to determine whether it issafe or unsafe. Worldwide, drug safety monitoring under the practical conditions ofclinical usage is called pharmacovigilance.
In Part 1 the abovementioned aspects are explained in more detail and it isdescribed that pharmacovigilance is a distinct discipline with its own reasoning,methods and development. The role of the pharmacist in drug safety monitoring isalso discussed and it is noted that, remarkably, in the Netherlands it is thecommunity pharmacist whose contribution is most substantial. In other countriesthe community pharmacist plays a less significant role and here in some countriesit is the hospital pharmacist who contributes most.
Part 2 describes the distinctive position of pharmacovigilance as a scientificdiscipline and thus lays the foundation for the remainder of the thesis. In chapter2.1 an overview is presented in which the attention adverse reactions to drugs havereceived in history. Professor Meyler of the Dutch University of Groningen wasone of the first to pay systematic attention to adverse drug reactions. Chapter 2.2 isdedicated to the remarkable story behind his, still renowned, book entitled ‘Sideeffects of drugs’.
203
Chapter 2.3 describes the way pharmacovigilance is organised in the Netherlands.Special attention is paid to the activities of the Netherlands PharmacovigilanceCentre Lareb, which has a key role in its implementation. This chapter is alsoessential because it describes the background of and the circumstances in which thepharmacist functions in the Netherlands, as will be described in more detail inChapter 3.The discussion of the concept of underreporting in chapter 2.4 underscores theuniqueness of pharmacovigilance as a separate discipline. The term underreportingrefers to the fact that by no means all adverse reactions are reported.Underreporting is often used to challenge pharmacovigilance’s main methodology:the spontaneous reporting system (SRS). We explain that it is the moreepidemiological perspective of the reporting system that accounts for this bias. It isdemonstrated that from a pharmacovigilance standpoint underreporting is in actualfact desirable.
Part 3 discusses the contribution of the pharmacist in the reporting of adverse drugreactions. In chapter 3.1 we look at the contribution of these health professionals inthe various countries participating in the worldwide collaborative programme ofthe World Health Organisation. It is found that the pharmacist is particularlyappreciated in those countries that have been operating an effective reportingsystem for some length of time and where the pharmacist is authorised toparticipate.It is explored why the (community) pharmacist plays such an important role in theNetherlands. To this end, the attitude of the Dutch community pharmacists wasassessed by means of a survey. They proved to regard ADR reporting as an integralpart of their professional duties, inherent to the pharmaceutical care they wish toprovide.To determine the extent of the actual contribution the pharmacists make in theNetherlands, the reports they submitted in the period between 1995 up andincluding 1999 were compared with those sent in by doctors during the sameperiod. This showed that 40% of the reports Lareb had received originated frompharmacists. Overall, their reports were of good quality. Pharmacists tended toreport more eye and skin complaints. Doctors more frequently reported seriousadverse events and the clinical information they provided tended to be moredetailed.To illustrate the importance of well-documented pharmacist reports in chapter 3.4 afemale patient is described who died from thrombosis while on a new oralcontraceptive. Based on, among other indications, this report doctors andpharmacists could be warned that as far as the risk of thrombosis is concerned thisnew pill did not seem to be any different from the more established widely used pills.
204
‘How to improve pharmacovigilance’ is the theme of Part 4. In pharmavovigilanceit is crucial to gain insight into the as yet unknown risks associated with new drugswhen they are used by large numbers of patients in the clinical practice as soon aspossible. In chapter 4.1 a study is reported in which, based on the data generated bythe computer systems of pharmacies, doctors are requested to report to Larebhitherto unknown and serious adverse drug reactions associated with new drugs.Although a small-scale trial, we found that with this method it is possible toencourage the submission of reports soon after a drug has been introduced to themarket. In addition, pharmacists and doctors were found to be motivated toparticipate.It is not only the doctors and pharmacists that have questions and concernsregarding adverse reactions to drugs. Evidently, these are also shared by those usingthe drugs: the patients. For answers, many patients turn to the ‘GeneesmiddelenInfolijn’, a drug helpline operated by pharmacists. In chapter 4.2 these queries arecompared to the reports pharmacists submitted to Lareb. Although the conclusionsare tentative because the information on the questions patients had posed waslimited, the pharmacist reports tended to adequately reflect the complaints aboutside effects the patients had expressed to the helpline.The next logical step would be for patients to report side effects direct to thenational reporting centre. Worldwide, there is little experience with such a system.A common objection raised in this context is that such reports are likely to containinsufficient information to allow conclusions to be drawn about the relationshipbetween the complaint and the drug mentioned. In chapter 4.3 we describe the prosand cons of direct patient reporting based on a review of the available literature.It is the primary objective of pharmacovigilance to uncover new information onadverse drug reactions. It goes without saying that this also means that doctors andpharmacists should apply this new knowledge in their daily practice. In chapter 4.4four examples are given that shows this latter aspect is badly in need ofimprovement. The drastic measure of taking a drug off the market in reaction to itsadverse effects could be avoided in some cases. The main challenge for the future isto ensure that, by exploiting the most recent knowledge; drugs are prescribed anddispensed in such a way that the risk of adverse events is reduced. Severalrecommendations to achieve this goal are given.
Part 5 of the thesis is a synthesis of the issues described in the preceding chapters.By raising their awareness of adverse drug reactions doctors and pharmacists canhelp prevent much harm, both in terms of health and costs. They can contribute byadhering to careful prescription practices and by more readily considering adversereactions as a possible cause of complaints. Awareness of adverse events can thusbecome the foundation for a more effective pharmacotherapy.
205
Suggestions are provided to further improve pharmacovigilance. By encouragingdoctors and pharmacists, and possibly also patients, to submit more and well-documented reports we may add to our knowledge about the incidence of adversedrug reactions. It is essential to take the concern the reporter raises in his or herreport seriously and to provide him or her with proper feedback. Inpharmacovigilance automated systems are becoming increasingly important, also ininternational context. Another significant development is the so-called pro-activesurveillance of drugs, which has been given more weight of late. This method entailsthat when marketing approval of a new product is applied, the manufacturer needsto indicate which risks of adverse reactions he anticipates, which, among othersources, should also be based on the data generated by the pre-marketing trials. Inthis way, extra measures to monitor these likely risks can be taken. In the last part of this thesis the desirability of an autonomous pharmacovigilanceis stressed, that is independent of both the pharmaceutical industry and the nationalauthorities, as well as of other parties involved. Independent scientific analysis is thebest guarantee of an effective drug safety surveillance aimed to protect the interestsof the patient.It is evident that the pharmacist needs to be given an important role in the furtherdevelopment of pharmacovigilance. In those countries where he is not yetauthorised to report or where his contribution is still limited, it is essential to givethe pharmacist, as an expert on medication and as an ADR reporter, the status thathas proven so valuable in the Netherlands. On the other hand, the contribution ofthe Dutch hospital pharmacist needs to be enhanced by awarding him acoordinating role in the promotion of proper drug use, of which ADR reportingforms part.In the final chapter of the thesis the distinctive character of pharmacovigilance isunderpinned once again and it is emphasised that the acquisition of knowledge asderived from the experiences of individual patients is ultimately aimed at improvingthe pharmacotherapy to individual patients. Evidently, drug safety is pivotal in thisprocess. An alternative interpretation of the risk aspects of new drugs is advocated:a drug can only be used safely if its safety has been effectively proven.
206
207
SSamenvatting
Dit proefschrift heeft als titel: ‘Het verbeteren van de geneesmiddelenbewaking ende rol van de apotheker’. Hoofdthema is: hoe is de veiligheid van geneesmiddelenbeter te bewaken? Bij het uitwerken van dit thema wordt bijzondere aandachtgegeven aan de bijdrage die de apotheker daarbij kan leveren.Het is vooral sinds het ‘Softenon drama’ begin jaren zestig van de vorige eeuw dathet besef is gegroeid dat geneesmiddelen behalve een zegen ook een risico kunnenzijn. Toen werden meer dan 10.000 kinderen geboren met aangeboren afwijkingenals gevolg van het gebruik van thalidomide (Softenon®) tijdens de zwangerschap vande moeder. Geneesmiddelen worden nu, voordat zij worden toegelaten tot gebruikin de dagelijkse praktijk, onderzocht. Zij moeten aan hoge eisen voldoen metbetrekking tot hun werkzaamheid, veiligheid en kwaliteit. In Nederland gebeurt detoelating van geneesmiddelen door het College ter Beoordeling vanGeneesmiddelen (CBG), vaak in Europees verband. Het is ook sinds die tijd dat aan artsen en apothekers wordt gevraagd mogelijkebijwerkingen te melden, zodat een ramp als met Softenon zo mogelijk voorkomenwordt. In opdracht van het CBG verzamelt en analyseert het NederlandsBijwerkingen Centrum Lareb deze meldingen van mogelijke bijwerkingen enrapporteert daarover aan dit college. Het bewaken van de veiligheid, door het inkaart brengen van de risico’s van geneesmiddelen, is nodig omdat er vóórgoedkeuring, en daarmee toelating tot de markt, slechts beperkte ervaring met hetmiddel is opgedaan. Pas bij gebruik door velen en onder allerlei verschillendeomstandigheden kan de (on)veiligheid pas echt getoetst worden. Deze bewaking inde dagelijkse praktijk heet internationaal pharmacovigilance.
In Deel 1 wordt bovenstaande uitvoeriger uitgelegd en aangegeven datpharmacovigilance een eigen vakgebied is met eigen denkwijze, methoden enontwikkeling. Ook wordt aangegeven wat de rol van de apotheker bij dezegeneesmiddelenbewaking is, waarbij het opmerkelijk is dat in Nederland deopenbare apotheker een belangrijke bijdrage levert. In het buitenland speelt deopenbare apotheker vaak een minder grote rol en betreft het voornamelijk deziekenhuisapotheker.
Deel 2 wil de eigen plaats van pharmacovigilance als veld van wetenschapbeschrijven en daarmee ook de basis voor de rest van het proefschrift leggen. Inhoofdstuk 2.1 wordt een overzicht gegeven van de aandacht die bijwerkingen vangeneesmiddelen in de loop van de tijd hebben gehad. Eén van de eersten diesystematisch aandacht aan bijwerkingen besteedde was prof. dr. L. Meyler teGroningen. Aan het bijzondere verhaal achter zijn, nog steeds beroemde boek ‘Sideeffects of drugs’, is hoofdstuk 2.2 gewijd.
209
In hoofdstuk 2.3. wordt de organisatie van de geneesmiddelenbewaking inNederland beschreven. Aandacht wordt besteed aan het functioneren van hetNederlands Bijwerkingen Centrum Lareb, dat hierbij een centrale rol speelt. Dithoofdstuk is ook van belang om te begrijpen tegen welke achtergrond de apothekerin Nederland functioneert, zoals beschreven in hoofdstuk 3.De eigen plaats van pharmacovigilance als veld van wetenschap wordt in hoofdstuk2.4 geïllustreerd aan de hand van het begrip onderrapportage. Dit begrip geeft aandat lang niet alle bijwerkingen worden gemeld. Onderrapportage wordt vaakgebruikt als bezwaar tegen de belangrijkste methode van geneesmiddelenbewaking:het vrijwillig meldsysteem. Het misverstand komt voort uit een meer epidemio-logische visie op het meldsysteem. Aangetoond wordt dat onderrapportage vanuithet gezichtspunt van pharmacovigilance juist gewenst is.
Deel 3 gaat over de bijdrage van de apotheker bij het melden van bijwerkingen. Inhoofdstuk 3.1 wordt gekeken naar die bijdrage in de verschillende landen, dieparticiperen in het mondiale samenwerkingsverband van de Wereld GezondheidsOrganisatie. Het blijkt dat de apotheker vooral gewaardeerd wordt in landen die allanger een goed functionerend meldsysteem hebben en waar het de apotheker ooktoegestaan wordt een bijdrage te leveren.Onderzocht is waarom de (openbare) apotheker een grote rol speelt in Nederland.Hiertoe is onderzoek gedaan naar de houding en opvattingen (‘attitude’) vanNederlandse openbare apothekers. Zij blijken het melden van bijwerkingen te zienals onderdeel van hun beroepsverantwoordelijkheid; het maakt deel uit van defarmaceutische zorg die zij willen leveren.Om te kijken welke concrete bijdrage de apothekers in Nederland leveren zijn demeldingen van apothekers over de periode 1995 tot en met 1999 vergeleken met dievan artsen. Hieruit blijkt dat 40% van de meldingen bij Lareb van apothekersafkomstig zijn. Zij zijn als regel van goede kwaliteit. Zij rapporteren relatief meermeldingen van oog- en huidklachten. Artsen melden vaker ernstige bijwerkingen ende klinische informatie van artsenmeldingen is vaak uitvoeriger.In hoofdstuk 3.4 wordt als illustratie van het belang van goede meldingen vanapothekers een patiënte beschreven die overleden is ten gevolge van trombose,terwijl zij een nieuwe anticonceptiepil gebruikte. Mede aan de hand van dezemelding konden artsen en apothekers gewaarschuwd worden dat een nieuwe pilvoor wat betreft het tromboserisico zich wellicht niet onderscheid van oraleanticonceptiva die al langer in gebruik zijn.
‘Hoe de geneesmiddelenbewaking te verbeteren’ is het thema van Deel 4. Het is vanbelang bij geneesmiddelenbewaking om juist van nieuwe geneesmiddelen snelinzicht te krijgen in nog onbekende risico’s bij het gebruik door grotere aantallen
210
patiënten in de dagelijkse praktijk. In hoofdstuk 4.1 wordt een onderzoekbeschreven waarbij, gebruik makend van het computersysteem van de apotheek,aan artsen wordt gevraagd om onbekende en ernstige bijwerkingen van een nieuwgeneesmiddel aan Lareb te melden. Hoewel het hier een proef van beperkte omvangbetreft, blijkt dat het mogelijk is op deze manier snel na introductie van een nieuwgeneesmiddel meldingen te krijgen. Apothekers en artsen blijken ook bereidhieraan mee te werken.Niet alleen artsen en apothekers hebben vragen en zorgen over bijwerkingen vangeneesmiddelen, dat is uiteraard ook het geval bij gebruikers van geneesmiddelen:patiënten. Veel van deze vragen worden gesteld aan de Geneesmiddelen Infolijn,een telefonische service van apothekers. In hoofdstuk 4.2 worden deze vragenvergeleken met de meldingen van apothekers bij Lareb. Hoewel door de beperkteinformatie die beschikbaar is over de gestelde vragen slechts voorzichtige conclusiesmogelijk zijn, blijken meldingen van apothekers goed overeen te komen met deklachten die patiënten hebben over geneesmiddelen, zoals geuit bij deGeneesmiddelen Infolijn.Een volgende stap is uiteraard dat patiënten zelf hun bijwerkingen melden bij hetlandelijk meldcentrum. Hiermee is wereldwijd nog weinig ervaring opgedaan. Eenbezwaar is dat deze meldingen wellicht onvoldoende informatie bevatten om totconclusies te komen over de samenhang tussen de klacht en het gebruiktegeneesmiddel. In hoofdstuk 4.3 worden de pro’s en contra’s van het rechstreeksmelden aan de hand van de beschikbare literatuur op een rijtje gezet.Het doel van pharmacovigilance is het vinden van nieuwe informatie overbijwerkingen. Het is daarbij uiteraard van belang dat deze nieuwe kennis ook doorartsen en apothekers in de praktijk wordt toegepast. Aan de hand van een viertalvoorbeelden wordt in hoofdstuk 4.4 aangegeven dat hier nog veel aan schort. Ditkan soms leiden tot het ‘van de markt halen’ van een geneesmiddel vanwegebijwerkingen, waar dit wellicht te voorkomen was geweest. Het is een belangrijkeuitdaging voor de toekomst om geneesmiddelen zo voor te schrijven en af televeren, dat op grond van de meest actuele kennis, de kans op bijwerkingen zo kleinmogelijk is. Een aantal aanbevelingen wordt gedaan hoe hiertoe te komen.
Deel 5 van het proefschrift is een synthese van hetgeen in de voorgaandehoofstukken is beschreven. Meer aandacht voor bijwerkingen bij artsen enapothekers kan veel schade voorkomen, zowel gezondheidsschade als onnodigekosten. Dit kan door zorgvuldiger voor te schrijven en door bij klachten eerder aande mogelijkheid van een bijwerking te denken. Aandacht voor bijwerkingen kan zode kapstok zijn voor een betere farmacotherapie. Aangegeven wordt hoe de geneesmiddelenbewaking verder verbeterd kan worden.Door meer goede meldingen door artsen en apothekers, en wellicht ook door
211
patiënten, te bevorderen, kan beter inzicht verkregen worden in het optreden vanbijwerkingen. Het is van belang hierbij de zorg van de melder, zoals die blijkt uit demelding, serieus te nemen en de melder goede feedback te geven over de melding.Automatisering speelt in toenemende mate een belangrijke rol bij degeneesmiddelenbewaking, ook in internationaal verband. Een anderebelangwekkende ontwikkeling is de aandacht voor de zogenaamde pro-actievegeneesmiddelenbewaking. Dit betekent dat bij het toelaten van een nieuwgeneesmiddel, door de fabrikant wordt aangegeven welke mogelijke risico’s er zijn,mede op grond van gegevens uit onderzoek vóór registratie. Dit maakt het mogelijkaan deze risico’s bijzondere aandacht te besteden. In de slotbeschouwing is ook aangegeven dat het wenselijk is datgeneesmiddelenbewaking onafhankelijk is, zowel van de farmaceutische industrieals van de overheid, maar ook van andere betrokken partijen. Onafhankelijkewetenschappelijke analyse is de beste garantie van een goede bewaking van deveiligheid met het belang van de patiënt als doel.De rol die de apotheker bij de verdere ontwikkeling van degeneesmiddelenbewaking dient te spelen is evident. In landen waar deze niet kanmelden of dat onvoldoende doet, is het van belang de apotheker alsgeneesmiddelendeskundige en als bron van meldingen die plaats te geven die inNederland zo waardevol blijkt. Daarnaast dient in Nederland deziekenhuisapotheker een grotere rol te spelen als coördinator van een goedgeneesmiddelengebruik, waarvan het melden van bijwerkingen een onderdeel is.In de finale van het proefschrift wordt nogmaals onderbouwing gegeven aan heteigen karakter van pharmacovigilance, zich kenmerkend door het verkrijgen vankennis uit ervaringen van individuele patiënten, ten dienste van een beterefarmacotherapie aan individuele patiënten. De veiligheid van geneesmiddelen staathierbij centraal. Gepleit wordt voor een andere benadering van het risicoaspect vannieuwe geneesmiddelen. Ook voor een geneesmiddel geldt: het kan pas veiliggebruikt worden als veiligheid ervan ook metterdaad is aangetoond.
212
List of publications
related to pharmavovigilance
1. Grootheest AC van. Het Europees registreren van geneesmiddelen: consequenties voorvoorschrijven en patiënt. Ned Tijdschr Geneeskd 1997;141:1305-6.
2. Grootheest AC van. Lareb, Lariam en lariekoek. Med Contact 1997;52:1150-1.
3. Puijenbroek EP van, Grootheest AC van. Bijwerkingen, een verantwoordelijkheid van artsen?Med Contact 1997;52:1156-7.
4. Grootheest AC van. Lareb, het landelijk systeem voor bijwerkingen. Geneesmiddelenbulletin1998:32:23.
5. Feenstra J, Grootheest AC van, Stricker BHCh. De farmacotherapeutische behandeling vanchronisch hartfalen. Hartbulletin 1998.
6. Boxtel CJ van. Hekster YA, Grootheest AC van. Kennis en bewustwording van ongewensteeffecten noodzakelijk. Pharm Weekbl 1998;133:1813.
7. Grootheest AC van. Seedings trials zaaien verwarring. Pharm Weekbl 1999;134:148-9.
8. Grootheest AC van. Vries CS de. Kinderen zijn geen kleine volwassenen. Beter onderzoeknaar geneesmiddelen voor kinderen noodzakelijk. Med Contact 1999;54:1643-5.
9. Grootheest AC van, Puijenbroek EP van, Heeringa M. Bijwerkingen van mefloquine. Onrustondermijnt objectieve beoordeling. Pharm Weekbl 1999;134:114-6.
10. Eland IA, Belton KJ, Grootheest AC van, Meiners AP, Rawlins MD, Stricker BHC. Attitudinalsurvey of voluntary reporting of adverse drug reactions. Br J Clin Pharmacol 1999;48:123-7.
11. Grootheest AC van. Mogelijke bijwerkingen van palivizumab (Synagis®).Geneesmiddelenbulletin 2000;34:86-7.
12. Grootheest AC van, Puijenbroek EP van. Huisartsen kennen Lareb – is dat zo?. Onderzoeknaar de bekendheid meldpunt bijwerkingen. Pharm Weekbl 2002;135:189-91.
13. Heeringa M, Grootheest AC van. Bijwerkingen geen reden tot verandering van indicatie.Profylactisch gebruik van mefloquine. Pharm Weekbl 2000;135:788-92.
14. Heeringa M, Grootheest AC van. Atypische antipsychotica. Ned Tijdsch Geneeskd2000;144:2078-9.
15. Puijenbroek EP van, Grootheest AC van. Kwantiteit versus kwaliteit. Lareb in maat en getal.Pharm Weekbl 2000;135:501-4.
213
16. Diemont WL, Puijenbroek EP van, Grootheest AC van. Klinisch denken en beslissen in depraktijk. Een patiënt met koorts. Ned Tijdsch Geneeskd 2000;144:1853.
17. Voordouw I, Dettingmeyer M, Grootheest AC van. Bijwerkingen van geneesmiddelen. Vasteprik of het fto. Pharm Weekbl 2000;135:41-2.
18. Grootheest AC van, Strauss SMJM, Heeringa M. Bijwerkingen van sildenafil: resultaten vantwee jaar praktijkervaring. Ned Tijdschr Geneeskd 2001;145:526-9.
19. Grootheest AC van. Bupropion (Zyban®): Epileptische aanval als bijwerking.Geneesmiddelenbulletin 2001;35:9.
20. Grootheest AC van, Diemont WL. Nieuwe orale bloedglucoseverlagende middelen. NedTijdschr Geneeskd 2001;145:1911.
21. Puijenbroek EP van, Grootheest AC van, Diemont W, Egberts ACG, Leufkens HGM.Determinants of signal selection in a spontaneous reporting system for adverse drug reactions.Br J Clin Pharmacol 2001;52; 579-86.
22. Vries CS de, Grootheest AC van, Jong-van den Berg LTW de. Spontane meldingen; langs devalkuilen. Pharm Weekbl 2001;136:1104.
23. Diemont WL, Puijenbroek EP van, Grootheest AC van. Renale bijwerkingen vangeneesmiddelen; Het duiden van een associatie. Pharm Weekbl 2001;136:1354-8.
24. Heeringa M, Puijenbroek EP van, Grootheest AC van. Anorexie tijdens gebruik van selectieveserotonine heropname remmers. Huisarts en Wetenschap 2001;44:142-3.
25. Kwan AL, Meiners AP, Grootheest AC van, Lekkerkerker JFF. Risico van convulsies bijgebruik van bupropion als hulpmiddel bij het stoppen met roken. Ned Tijdschr Geneeskd2001;145:277-8.
26. Molen-Eigenraam M van der, Blanken-Meijs JTHM, Heeringa M, Grootheest AC van.Delirium door stijging van clozapinespiegels tijdens ontstekingsreactie. Ned TijdschrGeneeskd 2001;145:427-30.
27. Wagena EJ, Graaf L de, Chavannes NH, Grootheest AC van, Schaijk CP van. Onrust over deveiligheid van bupropion als middel om te stoppen met roken onterecht. Ned TijdschrGeneeskd 2001;145:1489-92.
28. Diemont W, MacKenzie M, Schaap N, Goverde G, Heereveld H, van Grootheest AC,Hekster. Neuropsychiatric symptoms during cefepime treatment. Pharm World Sci2001;23:36.
29. Grootheest AC van, Puijenbroek EP van. Pharmacovigilance in the Netherlands. In:Pharmacovigilance. Mann RD, Andrews EB (editors). Chichester: Wiley (2002) 309-15.
30. Grootheest AC van. Je kunt het niet alleen. Pharm Weekbl 2002;137:338-9.
214
31. Grootheest AC van, Puijenbroek EP van, Jong-van den Berg LTW de. Contribution ofpharmacists to the reporting of adverse drug reactions. Pharmacoepidemiol Drug Saf2002;11:205-10.
32. Grootheest AC van, Mes K, Jong-van den Berg LTW de. Attitudes of community pharmacistsin the Netherlands towards ADR reporting. Int J Pharm Pract 2002;10:267-72.
33. Grootheest AC van, Groote A, Jong-van den Berg LTW de. Pharmacy based intensivemonitoring of adverse drug reactions. Pharmacoepidemiol Drug Saf 2002;11(1):S50.
34. Grootheest AC van, Edwards IR. Labelling and 'Dear Doctor' letters: are they noncommittal?Drug Saf 2002;25:1051-5.
35. Diemont WL, Grootheest AC van. Seksuele bijwerkingen van geneesmiddelen. ModernMedicine 2002;11:650-4.
36. Graaf L de, Grootheest AC van. Meldingen aan Lareb over mogelijke systemische effecten bijgebruik van een hormoon bevattend IUD (Mirena®). Tijdschr v Huisartsgeneesk2002;19:134-7.
37. Grootheest AC van, Graaf L de, Jong-van den Berg LTW de. Consumer adverse drug reactionreporting: a new step in pharmacovigilance? Drug Saf 2003;26:211-7.
38. Grootheest AC van, Puijenbroek EP van, Jong-van den Berg LTW. Een substantiële bijdragevan de apothekers. Het melden van bijwerkingen in Nederland. Pharm Weekbl 2003;138:546-51.
39. Grootheest AC van. Melden nodig voor bewaken veiligheid geneesmiddelen.Geneesmiddelenbulletin 2003;37:9.
40. Grootheest AC van, Vrieling T. Thromboembolism associated with the new contraceptiveYasmin®. BMJ 2003;326:257.
41. Puijenbroek EP van, Grootheest AC van. Bijwerkingen van geneesmiddelen in dehuisartsenpraktijk. Tijdschr v Huisartsgeneesk 2003;20:35-8.
42. Puijenbroek EP van, Diemont WL, Grootheest AC van. Application of quantitative signaldetection in the Dutch spontaneous reporting system for adverse drug reactions. Drug Saf2003;26:193-301.
43. Grootheest AC van, Passier JLM. The Importance of ADR reporting and the role of thepharmacist. Arh Farm Yug 2003:7-11.
44. Grootheest AC van, Groote JK, Jong – van den Berg LTW de. Intensive monitoring of newdrugs based on first prescription signals from pharmacists: a pilot study. PharmacoepidemiolDrug Saf 2003;6:475-481.
215
other publications
1. Grootheest AC van. Kraats en Binnenveld, een historische notitie. Historische Werkgroep deKraats. Veenendaal 1988.
2. Grootheest AC van. Enkele opmerkingen over de geschiedenis van de Hoekelumse brink. In:De Hoekelums Brink, het bewaren waard:2-7. Stichting Milieuwerkgroepen Ede enHistorische Werkgroep de Kraats. Ede 1990.
3. Grootheest AC van. David Philips 1902-1967. Oud Veenendaal 1990:115-27.
4. Grootheest AC van. Kraats en Binnenveld, een overzicht. Eemvallei 1992;1:1-14.
5. Grootheest AC van. Adriaan P. de Kleuver, 1911-1980. Oud Veenendaal 1994:73-85.
6. Grootheest AC van, Smolders LGW. Kadastrale atlas 1832, Stichts en Gelders Veenendaal.Veenendaal. Historische Vereniging Oud Veenendaal 1995.
7. Grootheest AC van. Water in Veenendaal. In: Geschiedenis van Veenendaal. Grootheest ACvan, Bisschop R (editors). Historische Vereniging Oud Veenendaal 2000:35-47. Veenendaal2000.
8. Grootheest AC van. Dolerend in Bennekom. In: Liber Amicorum Angelicus: 12-18.Protestantse Gemeente Engelen 2002. (re-edited also in: De Kostersteen 2003:2-4. UitgaveOud Bennekom).
216
Dankwoord
‘Zij die een proefschrift schrijven zijn, dunkt mij, meer te beklagen dan te benijden,daar zij zich eindeloos aftobben’, zo sprak prof. Meyler eens één van zijnpromovendi toe. Dit keer had Meyler ongelijk, in ieder geval wat mij betreft. Metbuitengewoon veel plezier heb ik dit proefschrift geschreven, op mijnstudeerkamer, begeleid door Bach en voorzien van een sigaartje, dankbaar dat ikdeze mogelijkheid heb gekregen. En voor een dankbaar mens is het makkelijk eendankwoord te schrijven.Velen ben ik erkentelijk voor hun bijdrage, meer dan ik hier kan noemen. Al degenen die hebben bijgedragen aan mijn opleiding en vorming wil ik, in de geestvan de eed van Hippocrates, bedanken met het noemen van de naam van mijn hoofdvan de ‘School met den Bijbel’ te Bennekom, meester H. van Diermen. Hij wistmijn vader aan de hand van een bijbelverhaal te overtuigen dat ik naar demiddelbare school moest gaan.Mijn bijzondere dank gaat uit Lolkje de Jong – van den Berg, mijn promotor. Watin 1998 begon met een aarzelend idee is, mede dank zij jouw vertrouwen in eengoed resultaat en je kritische begeleiding, geworden tot wat nu voorligt.‘Buitenpromovendi’ zijn een lastig soort, maar de afstand bleek geen bezwaar, zelfsniet toen je in Boston verbleef. Groot is ook mijn dank aan mijn co-promotor, Eugène van Puijenbroek. Jouwaltijd maar doorvragen naar de onderbouwing van conclusies, je statistische enanalytische vaardigheden en je bereidheid weer een volgend concept kritisch telezen en van commentaar te voorzien, hebben belangrijk bijgedragen aan ditproefschrift.De leden van de beoordelingscommissie, prof. dr. A. de Boer, prof. dr. J.R.B.J.Brouwers en prof. dr. Y.A. Hekster ben ik erkentelijk voor hun bereidheid hetconcept van dit proefschrift te lezen en van hun oordeel te voorzien. Uit ervaring weet ik dat het welhaast onmogelijk is het traject van een proefschrifttot een goed einde te brengen, als de wetenschappelijke omgeving die daarvoornodig is, ontbreekt. Het Nederlands Bijwerkingen Centrum Lareb heeft me dieomgeving geboden. Bestuur, staf, medewerkers en allen die daar anderzins bijbetrokken zijn, ben ik grote dank verschuldigd. Graag spreek ik mijn dank uit aan alle medeauteurs, in binnen- en buitenland. Mijnbijzondere dank geldt Arjen Groote en Kyros Mes, die als student voor tweehoofdstukken de onderzoeksgegevens hebben verzameld.
217
‘Your manuscript has been reworded to assist our translators’ schreef D.M. Davies,ook een pionier op bijwerkingengebied, eens aan een auteur. Het had over mijkunnen gaan. Ik ben Hanneke Meulenbelt erkentelijk voor haar bijdrage bij devertaling in het Engels.Met veel genoegen bedank ik ook mijn paranimfen. Met Nico van Suchtelen deel ikgrote delen van mijn leven: Bennekom, Sona Bata (Zaïre, nu weer Congo), Rwandaen vooral Veenendaal, waar we tien jaar lang een uiterst plezierigehuisartsenmaatschap hebben gevormd. Jij mocht als steun en toeverlaat vandaagniet ontbreken. Daniël van Grootheest vertegenwoordigt een ander aspect van het leven, waar ikbijzonder aan hecht: de familiebanden. Ik ben er trots op dat mijn zoon nu mijbijstaat. Natuurlijk vertegenwoordig je ook een beetje mijn alma mater; zullen wehet maar als een generale repetitie beschouwen?Met Daniël ben ik aangekomen bij de kleinere kring van ons gezin en die aspectenvan het leven, die de waarde van dit proefschrift verre te boven gaan. Liesbeth enSanne hebben minder gemerkt van het schrijven van dit proefschrift, maar zorgenwel in belangrijke mate voor zoveel zingeving, dat het het schrijvenvergemakkelijkt. Lieve Dirma, wij delen al zo lang zo veel, dat het moeilijk is je bijdrage in woordente vatten. Zullen we maar gewoon zo doorgaan?
218
Curriculum vitae
Kees van Grootheest is 13 april 1948 geboren te Bennekom als zesde kind vanWouter van Grootheest en Jantje van Amersfoort. Na de lagere school volgde hetChristelijk Streeklyceum te Ede, waar hij de opleiding HBS-B volgde (1960-1965).Na de studie Geneeskunde aan de Vrije Universiteit te Amsterdam (1965-1972),deed hij assistentschappen chirurgie (St Joannes de Deo, Haarlem) en verloskundeen gynaecologie (St Lucas Ziekenhuis, Amsterdam). Na de Nationale Tropencursusvoor Artsen (Koninklijk Instituut voor de Tropen) te hebben gevolgd, was hij driejaar werkzaam als arts in het Hôpital Evangélique Sona Bata in Zaïre (1974-1977).Eind november 1978 vestigde hij zich vrij als huisarts in Veenendaal, waar hij ookwerkzaam was als verpleeghuisarts en daarnaast taken deed op het gebied vanverzekeringsgeneeskunde en forensische geneeskunde. In 1986 werd de praktijk inmaatschapsverband voortgezet als Huisartsenpraktijk West in samenwerking metNico van Suchtelen.In deze periode was hij op verschillende terreinen actief: bestuurlijk (o.m. LHV, lidUniversiteitsraad Vrije Universiteit), politiek (diverse functies binnen het CDA),kerkelijk en op het terrein van de lokale geschiedenis. In 1994 en in 1996 was hij drie maanden in het kader van noodhulp werkzaam voorMemisa in Rwanda. Daar besloot hij samen met zijn echtgenote, na bijna 20 jaarhuisarts te zijn geweest, op zoek te gaan naar een nieuwe toekomst.Sinds 1 november 1996 is hij directeur van het Nederlands Bijwerkingen CentrumLareb. De management opleiding volgde hij aan het TIAS, verbonden aan deUniversiteit van Tilburg (opleiders: prof. dr. J. Moen en prof. dr. A. de Roo).Hij was voorzitter van het organisatiecomité dat in 2002 de Annual Meeting ofCollaborating Pharmacovigilance Centres van de WHO in Amsterdam organi-seerde, alsmede de wetenschappelijke conferentie van de International Society ofPharmacovigilance (ISoP). Hij is lid van de Executive Board van ISoP en lid van deEditorial Board van het tijdschrift Pharmacoepidemiology and Drug Safety.Zijn belangstelling is breed, maar betreft buiten zijn gewone werk vooralhistorische kartografie, (lokale) geschiedenis, Afrika en boeken. Hij is gehuwd metDirma Kruithof en vader van drie volwassen kinderen.
219
Notes on the cover illustrations
The illustration depicted on the front cover is a symbolic representation of whatPharmacovigilance entails. It portrays Medicina holding a cockerel in the right hand and holding with in theleft hand Aesculapius’ staff with the snake coiled around it. Medicina hererepresents health care and is depicted as an older, wiser woman as is shown by herwreath of laurels. The cockerel she is holding is the symbol of vigilance.Aesculapius’ staff has been the traditional emblem of health care, where the snakewith its poison is taken to symbolise medicinal drugs. This staff, whose name stemsfrom Asklèpios, the Greek god of medicine, not only represents physicians but isalso used in a much wider context, as is evident from old pharmacopoeias that oftencarry the staff on their title pages.Health care personified, with a drug in the left and vigilance in the right hand, seemsto be an adequate symbol of pharmacovigilance.
The illustration has been taken from Iconologia by Cesare Ripa, from the editionthat appeared in Padua in 1625. The first edition, which was not illustrated, waspublished in Rome in 1593 and the first illustrated volume was issued in 1603.The book was translated and published in Dutch in 1644 by the Amsterdam-basedpublishing firm called Dirck Pietersz. Pers, bearing the title: Iconologia ofuytbeeldinghe des verstants.
Reference: Schouten J. De slangestaf van Asklepios - symbool der geneeskunde. Amsterdam 1963.
The back cover depicts a map of Africa, published by Abraham Ortelius, thatappeared in his Epitome since 1595. Ortelius was the first to publish a systematic‘atlas’ of the whole globe: the Theatrum Orbis Terrarum in 1570. He gavereferences to his sources of knowledge. The Epitome was a pocket edition of thelarge atlas. This map shows one of the theories about the course of the main rivers of Africa:three of them have their common source in a centrally situated lake.
Reference: Broecke M van de, Krogt P van de, Meurer P (editors). Abraham Ortelius and the First
Atlas. H&S 1998.
221
Colofon
Dit proefschrift Improving pharmacovigilance andthe role of the pharmacist is geschreven tussen 1999en 2003. Het is gedrukt door BENDA drukkers teNijmegen, die ook, in samenspraak met de auteur,de vormgeving verzorgde. Het gebruikte lettertypeis Stempel Garamond. Het boek is gedrukt op eenHeidelberg Speedmaster op 115 grs. Hello matpapier van Proost en Brandt. De vormgeving vande omslag is van de hand van Frank Beekhuis teAsten. De oplage bedraagt 1100 exemplaren.