Page 1
The UC San Diego AntiViral Research Center sponsors weekly presentations by infectious disease clinicians, physicians and researchers. The goal of these presentations is to provide the most current research, clinical practices and trends in HIV, HBV, HCV, TB and other infectious diseases of global significance. The slides from the AIDS Clinical Rounds presentation that you are about to view are intended for the educational purposes of our audience. They may not be used for other purposes without the presenter’s express permission.
AIDS CLINICAL ROUNDS
Page 2
UPDATE'FROM'AASLD'
Presented'by'Laurel'and'Hardy'
Page 3
• we'talk'about'our'pt'and'both'his'ini@al'treatment'op@ons'for'a'guy'on'TDF/FTC/RAL/DRV/rit'and'how'we'are'trying'to'accommodate'SOF/SMV'now'with'his'HIV'regimen…'
'• Drug'interac@ons'with'ARVs''(Richard):'• Mdrug'interac@on'data'• MHIV'data'with'SOF/NS5a'regimen'(NIH'study'presented'at'AASLD'with'
SOF/LDV)'• Mother'HIV'data'(AbbVie'data'Turquoise'I)'
• Retreatment'of'SOF'and/or'other'HCV'failures/resistance'(David):'• M'retereatment'data'(Gilead'1118'study;'data'from'real'world'cohorts)'• M'resistance'issues'(NS5A'impact'focus)'• Mfuture'regimens'that'might'address'resistance'if'needed.'
Page 4
GJ'• 57'AA'yo'male'• HCV'
– Genotype'1a'– Cirrhosis'F5/6'(bx'3/2014);'no'decompensa@on'– U/S'nega@ve'1/2014;'EGD'w/o'varicies''– Null'responder'to'PEG/'RBV'– Relapse'a`er'12'weeks'SOF/'DVC'
• PMH'– DMII;'HTN'– HBV'and'HAA'immune'
Page 5
HIV'Treatment'Hx'• 5/13M9/14:'DRVr'(BID)/'RAL/'TDF/'FTC'
– 1/09M5/13:'SQV(BID)/'RAL/'TDF/FTC'2004M'09:'TDF/CBV/SQV(1000)'BID/RTV(100)'BID'
– 2000M04:'D4T/3TC/IDV/RTV''– Late'1990s'x'2'weeks:'ZDV'+'2'others?''
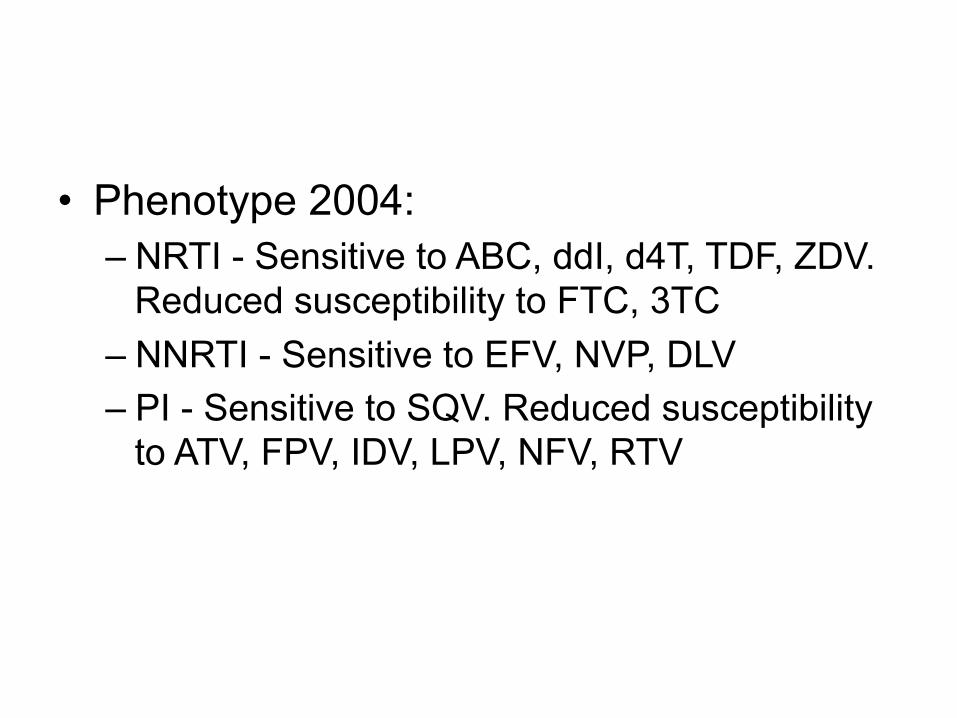
• Phenotype'2004:''– NRTI'M'Sensi@ve'to'ABC,'ddI,'d4T,'TDF,'ZDV.'Reduced'suscep@bility'to'FTC,'3TC''
– NNRTI'M'Sensi@ve'to'EFV,'NVP,'DLV''– PI'M'Sensi@ve'to'SQV.'Reduced'suscep@bility'to'ATV,'FPV,'IDV,'LPV,'NFV,'RTV'
Page 6
What'HCV'regimen'can'be'given'with'his'current'ARV'regimen?'
• SOF/'LDV'• SIM/'SOF'• SIM/'SOF'RBV'• IFN/'RBV/'SOF'• none'
Page 7
Labs'10/2014'
• Chemistry:''– Cr.'1.3;'AST'39;'ALT'25;'TB'0.5'
• CBC:'– Hg'14.3;'plt'107;'INR'1.0'
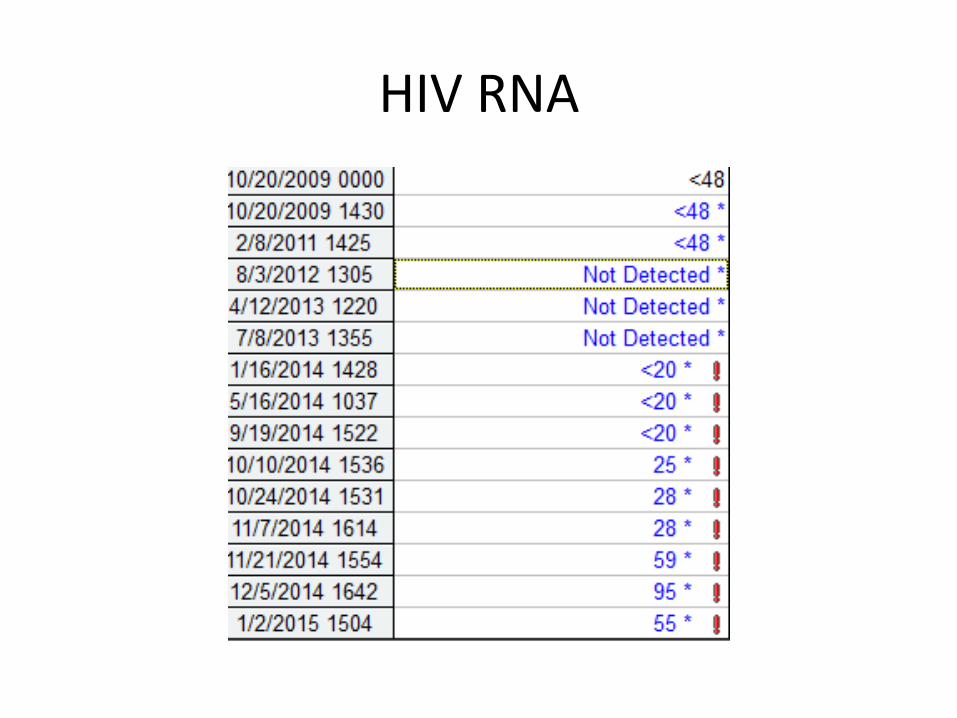
• HCV'RNA:'3,457,502'• APRI'='0.91'(cutoff'1.0);'Fib'4'='4.2'(cutoff'1.45)'• CD4:'509'(33%)'• HIV'RNA:'25'(<20'on'9/19/14)'
Page 8
Significant'drug'interac@ons'of'ARV'and'SOF'include?'
1. TDF'2. All'PIs'3. All'NNRTIs'4. RAL'but'not'other'INSTI'5. none'
Page 9
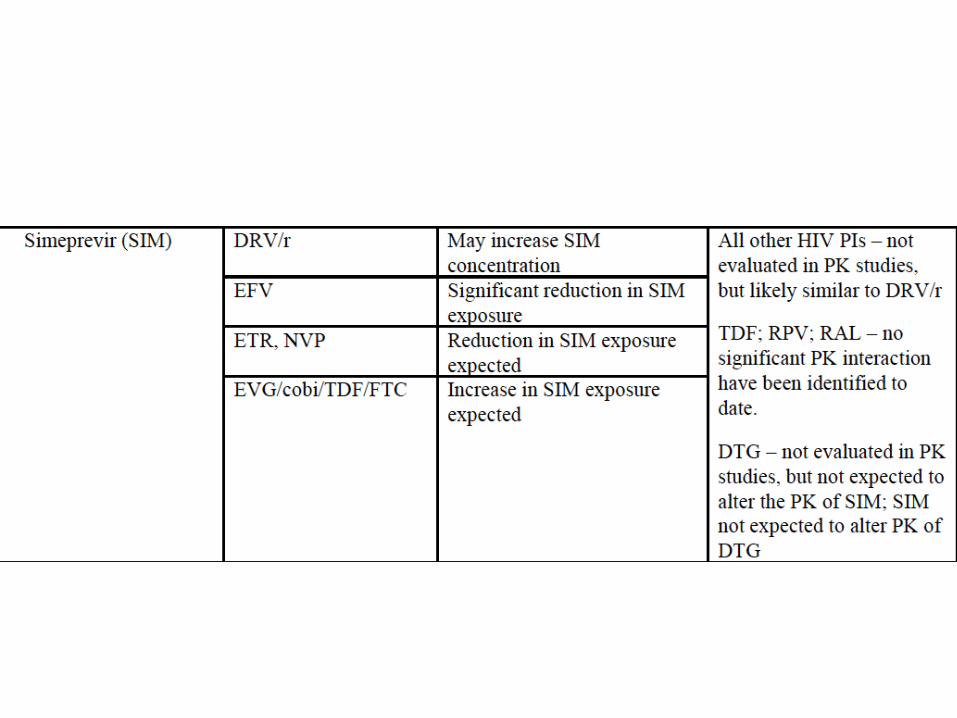
Significant'drug'interac@ons'of'ARV'and'SIM'include?'
1. All'NRTI'2. Some'NNRTI'3. All'PI'boosted'with'RTV'or'cobi'4. 2'and'3'5. none'
Page 10
Significant'drug'interac@ons'of'ARV'and'SOF/LDV'include?'
1. All'NRTI'2. TDF'when'given'with'EFV'or'ETR'3. TDF'when'given'with'a'PIr'4. All'PI'5. 2'M'4''
Page 12
SIM'Metabolism'
• SIM'metabolized'by'CYP'3A'– CYP3A'inhibitors'increase'SIM'– CYP3A'inducers'decrease'SIM'
• SIM'inhibits'intes@nal'CYP3A'but'not'hepa@c'• SIM'inhibits'OATP1B1/3'and'PGP'
Page 13
DDI'between'NRTI'and'HCV'Agents'
ARV$ SOF$ LDS/$SOF$ SIM$
FTC/$3TC$ 00$ 00$ 00$
ABC$ 00$ 00$ 00$
TDF$ 00$ ✖ PIr$$! TDF$
00$
ZDV$ 00$ 00$ 00$
MM'='no'significant'effect'✖''='do'not'use'
AASLD/IDSA/IAS–USA.'hpp://www.hcvguidelines.org.'hpp://aidsinfo.nih.gov/contenqiles/lvguidelines/AdultandAdolescentGL.pdf'
Page 14
DDI'between'TDF'and'LDV/'SOF'
• C24'geometric'mean'ra@o:'2.6'(90%'CI:'2.4M'3.0)'• no'effect'='1.0'• TFV'levels'similar'to'dosing'with'DRVr'+'TDF'
Similar'data'with'RPV'as'EFV'
German'et'al.'15th'Clinical'Pharmacology'Workshop'of'HIV'&'HCV;'2014:'OM06'
Page 15
DDI'between'TDF'and'LDV/'SOF'
• Drug'interac@on'data'with'PIr'+'TDF'+'LDV/SOF'is'not'available'
• DRVr'increases'LDV'(GMR'='1.39)'• TFV'levels'are'expected'to'be'higher'with'PIr'and'LDV/SOF'
AASLD/IDSA/IAS–USA.'hpp://www.hcvguidelines.org.'
Page 16
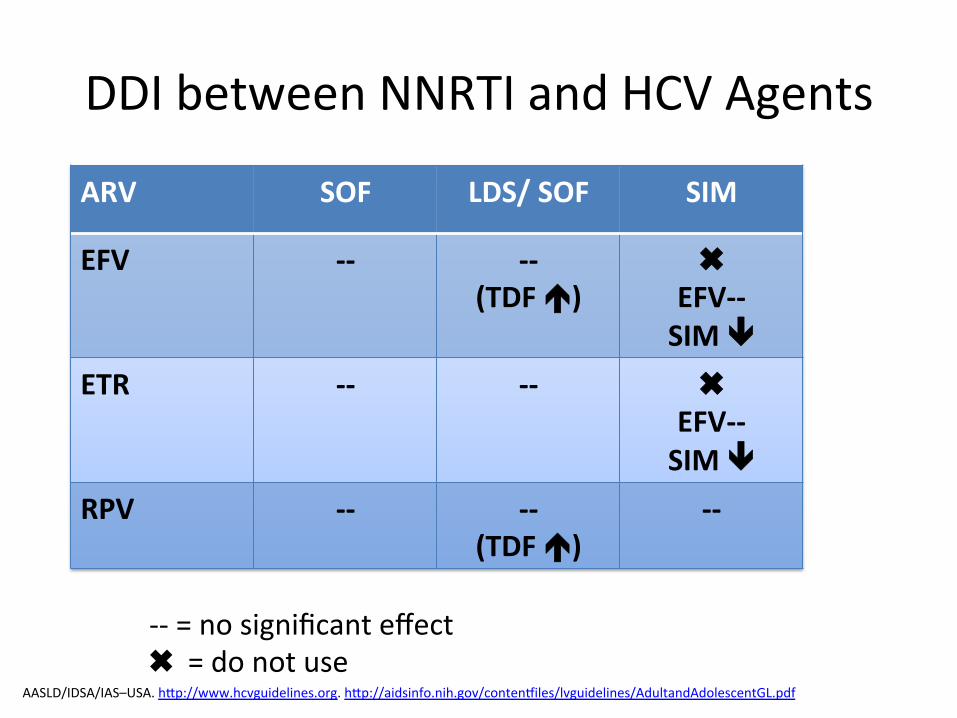
DDI'between'NNRTI'and'HCV'Agents'
ARV$ SOF$ LDS/$SOF$ SIM$
EFV$ 00$ 00$(TDF$!)$
✖EFV00$SIM$"$
ETR$ 00$ 00$ ✖EFV00$SIM$"$
RPV$ 00$ 00$(TDF$!)$
00$
MM'='no'significant'effect'✖''='do'not'use'
AASLD/IDSA/IAS–USA.'hpp://www.hcvguidelines.org.'hpp://aidsinfo.nih.gov/contenqiles/lvguidelines/AdultandAdolescentGL.pdf'
Page 17
No'DDI'between'EFV'and'LDV/'SOF'
• C24'geometric'mean'ra@o:'0.91'(90%'CI:'0.83M'0.91)'
• no'effect'='1.0'• RPV'less'effect'
German'et'al.'15th'Clinical'Pharmacology'Workshop'of'HIV'&'HCV;'2014:'OM06'
Page 18
DDI'between'PIr''and'HCV'Agents'ARV$ SOF$ LDS/$SOF$ SIM$
ATVr$or$ATV/$cobi$
00$ 00$(TDF$!)$
✖SIM$!$
DRVr$or$DRV/$cobi$
00$ 00$(TDF$!)$
✖SIM$!$
MM'='no'significant'effect'✖ ='do'not'use'“Monitor'for'TFVMassociated'adverse'events'in'EFV/FTC/TDF,'or'RTVMboosted'ATV'or'DRV+'TDF/FTC”'
AASLD/IDSA/IAS–USA.'hpp://www.hcvguidelines.org.'hpp://aidsinfo.nih.gov/contenqiles/lvguidelines/AdultandAdolescentGL.pdf;''German'et'al.'AASLD'2014'
Page 19
DDI'between'INSTI'and'MVC'and'HCV'Agents'
ARV$ SOF$ LDS/$SOF$ SIM$
DTG$ 00$ 00$ 00$
RAL$ 00$ 00$ 00$
EVG/cobi/TDF/FTC$
00$ ✖$ ✖$
MVC$ 00$ 00$ 00$
MM'='no'significant'effect'✖''='do'not'use'
AASLD/IDSA/IAS–USA.'hpp://www.hcvguidelines.org.'hpp://aidsinfo.nih.gov/contenqiles/lvguidelines/AdultandAdolescentGL.pdf'
Page 20
No'effect'of'RAL'on'LDV/'SOF'
• C24'geometric'mean'ra@o:'0.89'(90%'CI:'0.81M'0.98)'
• no'effect'='1.0'• No'effect'SOF'on'RAL'
German'et'al.'15th'Clinical'Pharmacology'Workshop'of'HIV'&'HCV;'2014:'OM06'
Page 21
To$be$able$to$use$all$HCV$DAA,$what$ARV$regimen?$
1. DRVr/RAL/'ABC/3TC'2. RAL/'ETR/'TDF/FTC'3. 'DTG/ETR/TDF/FTC'4. DTG/RPV/TDF/FTC'5. Other'
Current:'DRVr'(BID)/'RAL/'TDF/'FTC;'Phenotype:''– NRTI'–'Sensi@ve:'ABC,'TDF,'ZDV.'ResistantM'FTC,'3TC''– NNRTI'Sensi@ve:'EFV,'NVP'– PI'–'Sensi@ve:'SQV.'Reduced'suscep@bility'to'ATV,'FPV,'RTV'
Page 22
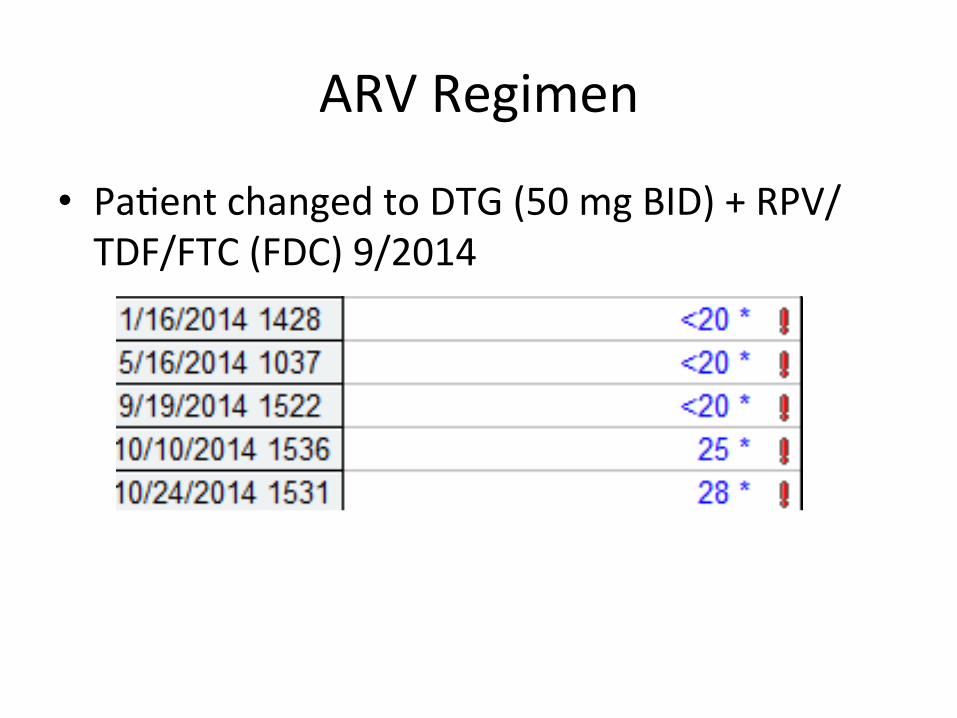
ARV'Regimen'
• Pa@ent'changed'to'DTG'(50'mg'BID)'+'RPV/TDF/FTC'(FDC)'9/2014'
Page 23
What'would'you'do'with'the'ARV'regimen?'
1. Follow'closely,'HIV'RNA's@ll'<200'2. Add'DRVr'3. Order'a'resistance'test'4. pray'
Page 24
Trofile'DNA'(11/7/14)'
Page 25
GENOSURE'ARCHIVE'11/7/14'
Page 26
GENOSURE'ARCHIVE'11/7/14'
Page 27
ARV'Regimen'
• Pa@ent'changed'to'DTG'(50'mg'BID)'+'RPV/TDF/FTC'(FDC)'9/2014'
• 11/21/2014'MVC'added'
Page 28
Other'than'DDI,'does'HIV'coMinfec@on'change'HCV'DAA'selec@on/'outcome?'
1. Yes'2. No'
Page 29
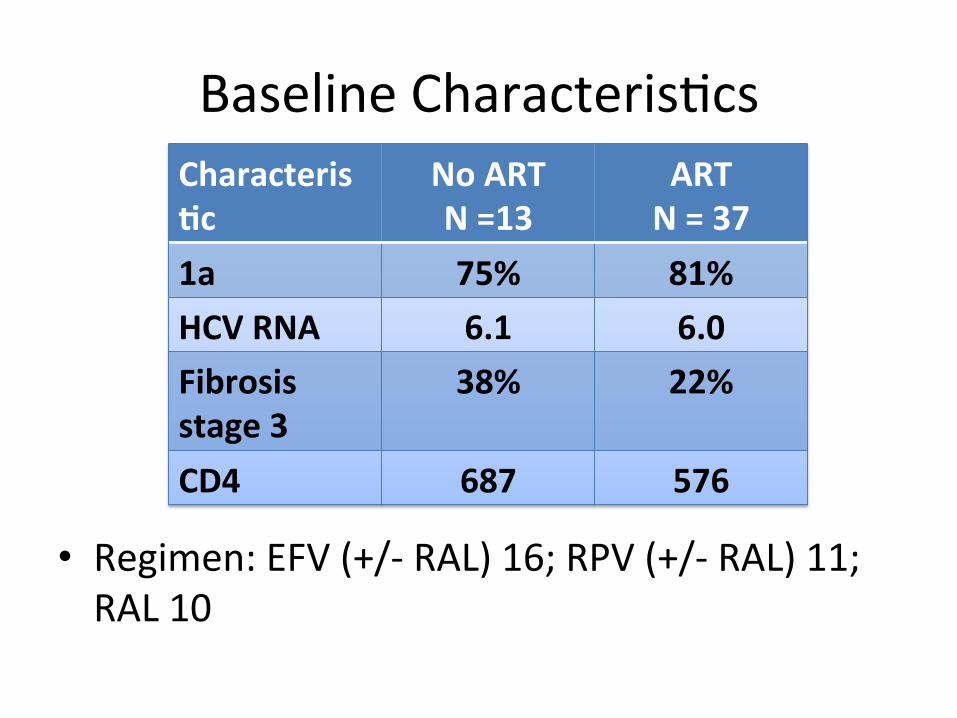
Osinusi A. AASLD 2014; 84
Page 31
CharacterisKc$
No$ART$$N$=13$
ART$N$=$37$
1a$ 75%$ 81%$
HCV$RNA$ 6.1$ 6.0$
Fibrosis$stage$3$
38%$ 22%$
CD4$ 687$ 576$
Baseline'Characteris@cs'
• Regimen:'EFV'(+/M'RAL)'16;'RPV'(+/M'RAL)'11;'RAL'10'
Page 32
Results'• SVR12'='98%'(49/50)'
– One'early'HCV'relapse'(wk'2'post'tx)'– One'late'relapse'HCV'at'week'36'post'tx'
• HIV'safety'– No'change'HIV'RNA'in'offMART'group'– One'blip'in'ART'treated,'reMsupressed'– CD4'stable'
• Crea@nine'stable'to'week'12'post'treatment'– Mean'week'12:''crea@nine'change'+0.03;'CrCL'M3.8'– Mean'post'tx'week'12:'crea@nine'change'+0.04;'CrCL'+0.4'
Page 33
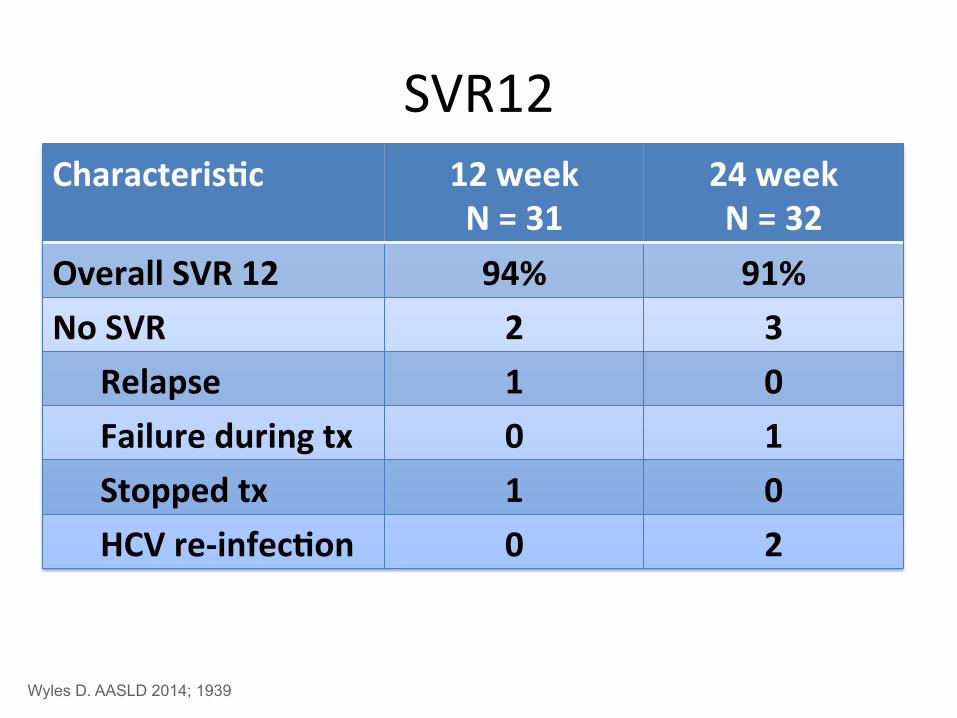
Turquoise'1:'Abbvie'3'DAA'+'RBV'• HIV/'HCV'
– GT'1,'naïve/'experienced,'cirrhosis'(CP'A)'– Stable'ART:'ATVr'or'RAL'
• Paritaprevir/r'(PI)'+ombitasvir'+'dasabuvir'+'RBV'
Wyles D. AASLD 2014; 1939
Page 34
CharacterisKc$ 12$week$N$=$31$
24$week$N$=$32$
HCV$genotype$1a$
97%$ 91%$
HCV$RNA$ 6.5$ 6.6$
Cirrhosis$ 19%$ 19%$
CD4$ 633$ 625$
ARV$=$ATVr$ 52%$ 38%$
Baseline'Characteris@cs'
Wyles D. AASLD 2014; 1939
Page 35
CharacterisKc$ 12$week$N$=$31$
24$week$N$=$32$
Overall$SVR$12$ 94%$ 91%$
No$SVR$ 2$ 3$
Relapse$ 1$ 0$
Failure$during$tx$ 0$ 1$
Stopped$tx$ 1$ 0$
HCV$re0infecKon$ 0$ 2$
SVR12'
Wyles D. AASLD 2014; 1939
Page 36
What'HCV'regimen'would'you'select?'
1. SOF/'LDV'2. SIM/'SOF'3. SIM/'SOF'RBV'4. IFN/'RBV/'SOF'5. Other'6. Need'more'informa@on'
Page 37
Retreatment'of'SOF'failure'with'SOF/LDV'+'RBV:'GSMUSM342M1118'
Wk 0 Wk 12 Wk 36 Wk 24
LDV/SOF + RBV SVR12 SOF failures (n=51)
LDV/SOF SVR12 LDV/SOF failures
LDV/SOF + RBV SVR12 SOF failures (advanced liver disease)
Wyles D. AASLD 2014.
Page 38
Baseline'Characteris@cs'LDV/SOF$+$RBV$12$weeks$
n=51$
Mean'age,'y'(range)' 54 (27‒68)
Men,'n'(%)' 31 (61)
Black/African'American,'n'(%)' 8 (16)
Hispanic/La@no,'n'(%)' 4 (8)
Mean'BMI,'kg/m2'(range)' 30.4 (21.1‒47.9)
IL28B'nonMCC,'n'(%)' 47 (92)
GT'1a,'n'(%)' 30 (59)
Mean'HCV'RNA,'log10'IU/mL'(range)' 6.2 (4.4‒7.3)
HCV'RNA'≥800,000'IU/mL,'n'(%)' 38 (75)
Prior'HCV'treatment,'n'(%)'
SOF'+'PEG/RBV' 25 (49)
SOF'±'RBV*$ 21 (41)
SOF'placebo†' 5 (10)
Cirrhosis,'n'(%)' 15 (29) Wyles D. AASLD 2014.
Page 39
24
98 100 100 98 98 98
0
20
40
60
80
100
Wk 1 Wk 4 Wk 8 EOT SVR4 SVR12 SVR24
HC
V R
NA
<LLO
Q, %
Error'bars'represent'95%'CIs.'EOT,'end'of'treatment.'
51/51 12/51$ 51/51$
HC
V R
NA
<LLO
Q, %
50/51$50/51$ 50/51$50/51$
OnMTreatment'Viral'Kine@cs'and'SVR'Rates'
Wyles D. AASLD 2014.
14/14'SOF/RBV'failures'achieved'SVR12'with'SOF/LDV'for'12'weeks.'Osinusi&A.&EASL&2014.&
Page 41
But'our'pt'failed'SOF'plus'an'NS5A'(DCV)…'
• What'is'his'resistance'profile'post'failure'likely'to'look'like?'– SOF'resistance?'– DCV'resistance?'
• What'is'the'impact'of'NS5A'resistance'on'treatment'outcomes?'
• Is'there'any'data'on'reMtreatment'of'these'pa@ents?'
'
Page 42
SOF'Resistance'
• AASLD'2013:'No'S282T'in'4'phase'3'studies'– Studies'across'GTs'1M4'(NEUTRINO,'FISSION,'FUSION,'POSITRON)'– 226'nonMSVRs:'221'UDS'(1%'detec@on'level)'
• No'S282T'iden@fied'– 1/294'nonMSVRs'with'S282T'(Svarovskaia&E.&CID&2014)&
• AASLD'2014:'No'S282T'in'phase'3'SOF/LDV'– L159F'+/M'V321A'seen'as'TEVs'– 15%'L159F'with'SOF;'1%'with'SOF/LDV'– impact'on'response?'
• 1.6%'at'baseline'w/'L159F:'100%'SVR'in'SOF/LDV'(23/23)'
Svarovskaia$E.$AASLD$2013.$Gane$E.$#43$AASLD$2014.$
Page 43
Evolution of sofosbuvir resistance in the subject with S282T.
Svarovskaia E S et al. Clin Infect Dis. 2014;59:1666-1674
© The Author 2014. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: [email protected] .
Page 44
NS5A'Inhibitor'Resistance'
• Similar'resistance'papern'for'1st'gen'NS5A'with'respect'to'GT'1a'and'1b'
Kitrinos'KM.'#1949'AASLD'2014.'Wang'C.'AAC'2013'
Page 45
Long'term'DCV'followMup'from'AASLD'
Reddy'KR.'AASLD'2014.'
Page 46
Long'term'DCV'followMup'from'AASLD'
• Median'followMup'ranged'from'41M123'weeks'– Longer'in'pts'treated'with'DCV/P/R'
• Predominant'NS5A'RAVs'– 1a:'Q30E/K/R,'L31M/V,'Y93H/C'''1b:'L31M/V'+'Y93H'
• Persistence'of'NS5A'RAVs'– 86%'(63/73'1a)'and'95%'(56/59'1b)'by'popula@on'at'last'followMup'
– Contrast'to'41%'(1a)'and'29%'(1b)'at'last'followMup'for'NS3'RAVs'
Reddy'KR.'#1965'AASLD'2014.'Wang'C.'AAC'2013.'
Page 47
Impact'of'NS5A'baseline'resistance'is'contextual'
• IFN'vs'IFNMfree'• Strength'of'surrounding'DAAs'
Kitrinos'KM.'#1949'AASLD'2014.'Manns'M.'EASL'2014'
38%'SVR12'in'ASV/DCV'with'baseline'NS5A'RAVs'(compared'to'85%'overall)'
Page 48
Baseline'NS5A'resistance'and'SOF/LDV'
• Deep'sequencing'analysis'of'baseline'samples'(n=1904)'in'phase'2/3'SOF/LDV'studies'– ELECTRON,'LONESTAR'and'ION'studies'
Sarrazin'C.'#1926'AASLD'2014.'
97%'
93%'
GT$1$(n=2137)$
98%'95%'
GT$1b$(n=529)$
96%'92%'
GT$1a$(n=1602)$
NS5A'RAVs'No'NS5A'RAVs'
SVR12'(%)'
Page 49
Baseline'NS5A'resistance'and'SOF/LDV'
Sarrazin'C.'#1926'AASLD'2014.'
<100X'
>100X'
No'RAVs'
Page 50
Impact'of'baseline'NS5A'RAVs'on'outcomes'in'retreatment'
• No'pa@ents'had'SOFMassociated'variant,'S282T,'detected'at'baseline''– 2'pa@ents'had'NS5B'treatmentMemergent'variant'L159F'at'baseline'and'
achieved'SVR'
'
Wyles'D.'AASLD'2014'*1'pa@ent’s'baseline'results'were'not'available.'
n=6/6$
100%$SVR$98%$SVR$
n=43/44$
12%$NS5A$RAVs$
n=6/50'
88%$No$NS5A$RAVs$at$baseline$
n=44/50*'
Page 51
And'of'course'this'is'the'single'LONESTAR'pa@ent…'
Lawitz'E.'#215'AASLD'2013.'
So'we'might'be'able'to'get'away'with'24wks'of'SOF/LDV,'but…'
Page 52
Why'not'just'avoid'the'NS5A'class?'
• This'makes'the'most'sense'intui@vely'• What'is'the'data'with'SOF'+'SIM'+/M'RBV'
– This'is'an'FDA'approved'regimen'• What'does'the'label'say?'• Do'the'Guidelines'help…not'really.'
– RealMworld'data'with'this'regimen?'• Very'liple'in'HIV+'
• Special'considera@ons'in'a'treatment'experienced'cirrho@c?'
Page 53
COSMOS:'Data'in'F3/F4'93' 97'
89'
0'
10'
20'
30'
40'
50'
60'
70'
80'
90'
100'
F3/F4' F3' F4'
Lawitz'E.'Lancet'2014.'
18'23'41'
89' 89'
Naïve' Null'
12'weeks'
24'weeks'
9' 9'
F4'only'
No'conclusion'can'be'drawn'on'the'u@lity'of'RBV.'
Page 54
FDA'label'indica@ons'for'SOF/SIM'
Tes@ng'for'Q80K'“is'not'strongly'recommended'but'may'be'considered.”'No'guidance'on'RBV'is'offered.'
Olysio'package'insert'(11/2014).'
Page 55
Real'world'data:'HCV'Target'
SOF/SIM'groups:'60%'experienced'(27%'PI'failure),'57%'cirrhosis'(47%'decompensa@on).'' ' ' ' ' ' '3%'HIV'CoMinfected'
Jensen'D.'#45'AASLD'2014.'
Page 56
Real'world'data:'HCV'Target'
Jensen'D.'#45'AASLD'2014.'
81'85'
79'
0'
89' 92'87'
75'
0'10'20'30'40'50'60'70'80'90'100'
All' NC' Cirr' DC'
PI'failure' No'PI'
No'data'on'Q80K;'vast'majority'did'not'have'it'tested.'97%'concordance'between'SVR4'and'SVR12.'
SVR4'
Page 57
TRIO'network'realMworld'experience'
65%'of'GT1'received'SOF/SIM'+/M'RBV;'~50%'treatment'experienced.'
Flamm'S.'#983'AASLD'2014.'
Page 58
TRIO'network'realMworld'experience'
No'data'on'Q80K'presented.'
Flamm'S.'#983''AASLD'2014.'
Page 59
SIRIUS'Study'• DoubleMblind'study'• Treatment'experienced'cirrho@c'pa@ents'
– All'failed'both'Peg/RBV'then'P/R/PI'
– Groups'were'well'matched'• Plt'<100k:'18%'vs'17%'• ALB'<3.5:'8%'vs.'17%'
Bourliere'M.'#LBM6'AASLD'2014.'
Page 60
SIRIUS'Study'
Bourliere'M.'#LBM6'AASLD'2014.'Bourliere'M.'#82'AASLD'2014'
Page 61
HCV'regimen'
• SIM/'SOF/'RBV'10/10/14'– Week'2'10/24'– Week'4'11/07'
Page 65
• Phenotype 2004: – NRTI - Sensitive to ABC, ddI, d4T, TDF, ZDV.
Reduced susceptibility to FTC, 3TC – NNRTI - Sensitive to EFV, NVP, DLV – PI - Sensitive to SQV. Reduced susceptibility
to ATV, FPV, IDV, LPV, NFV, RTV
Page 68
GENOSURE'ARCHIVE'11/7/14'