33
UPPER GI BLEEDING: GUIDELINES AND BEYOND
| Date post: | 30-Apr-2019 |
| Category: |
Documents |
| Upload: | truongduong |
| View: | 216 times |
| Download: | 0 times |

UPPER GI BLEEDING:
GUIDELINES AND BEYOND

DISCLOSURES
• Data safety monitoring boards
– Bayer
• Medications for non-approved indications
– PPIs, erythromycin, octreotide, antibiotics for
UGI bleeding

UGIB: GUIDELINES AND BEYOND Outline
• Initial assessment and treatment of patients
with UGI bleeding
• Management of bleeding ulcers
• Management of bleeding varices

ASSESS RISK OF
PATIENT WITH UGIB
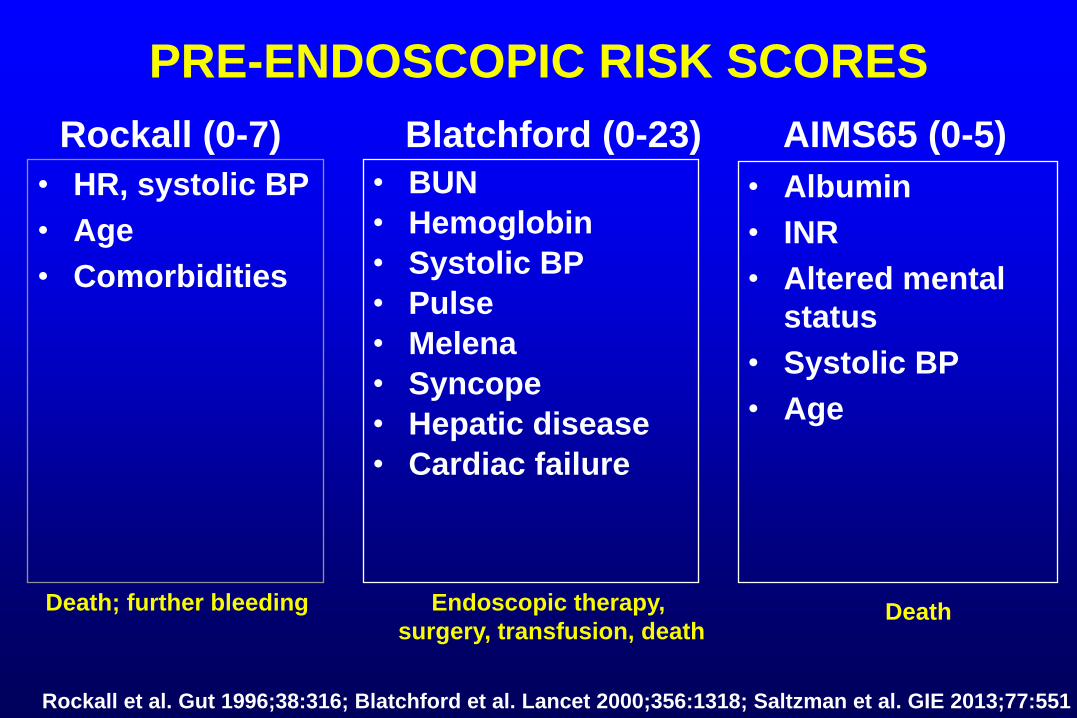
PRE-ENDOSCOPIC RISK SCORES
• HR, systolic BP
• Age
• Comorbidities
• BUN
• Hemoglobin
• Systolic BP
• Pulse
• Melena
• Syncope
• Hepatic disease
• Cardiac failure
Rockall (0-7) Blatchford (0-23) AIMS65 (0-5)
Rockall et al. Gut 1996;38:316; Blatchford et al. Lancet 2000;356:1318; Saltzman et al. GIE 2013;77:551
Endoscopic therapy,
surgery, transfusion, death
Death; further bleeding
• Albumin
• INR
• Altered mental
status
• Systolic BP
• Age
Death

PRE-ENDOSCOPIC UGIB SCORING SYSTEMS Prospective Assessment--6 Centers (US, Europe, Asia, NZ; N=3171)
Area Under Receiver Operating Characteristic (AUROC) Curve
Death Rebleed Intervention
or Death
Hospital
stay >3d
Blatchford 0.70 0.71 0.89 <0.70
Rockall 0.76 0.62 0.69 <0.70
AIMS65 0.79 0.62 0.70 <0.70
Laursen et al. UEGW 2015
0.9-1.0: Excellent
0.8-0.9: Good
0.7-0.8: Fair

PRE-ENDOSCOPIC RISK ASSESSMENT
• Stratify patients into high/low risk categories
– Level of care (ICU, ward, discharge)
– ?Timing of EGD
• Limitation for individual patient
– Can’t define risk with very high confidence
• Blatchford score 0 of 23: < 1% have intervention
– ? discharge from ED without endoscopy
Rockall et al. Gut 1996;38:316; Blatchford et al. Lancet 2000;356:1318; Stanley et al. Lancet 2009;373:42;
Pang et al. GIE 2010;71:1134; Chen et al. Am J Emerg Med 2007;25:774; Laine, Jensen AJG 2012:107:345

MEDICAL THERAPY
BEFORE ENDOSCOPY?
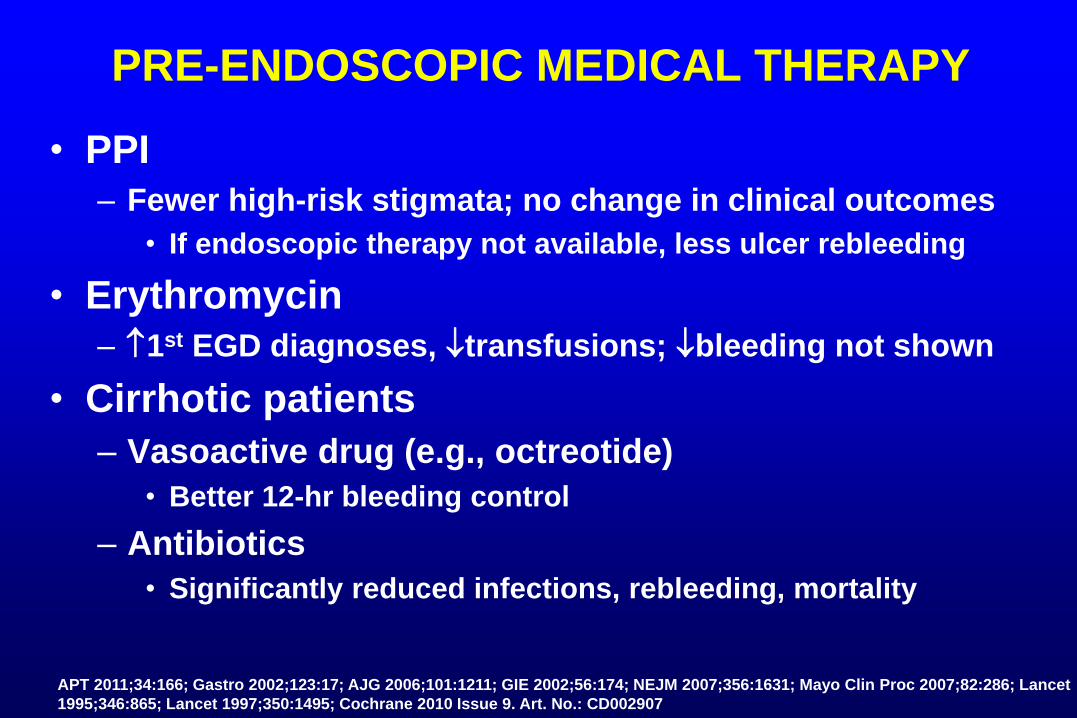
PRE-ENDOSCOPIC MEDICAL THERAPY
• PPI
– Fewer high-risk stigmata; no change in clinical outcomes
• If endoscopic therapy not available, less ulcer rebleeding
• Erythromycin
– 1st EGD diagnoses, transfusions; bleeding not shown
• Cirrhotic patients
– Vasoactive drug (e.g., octreotide)
• Better 12-hr bleeding control
– Antibiotics
• Significantly reduced infections, rebleeding, mortality
APT 2011;34:166; Gastro 2002;123:17; AJG 2006;101:1211; GIE 2002;56:174; NEJM 2007;356:1631; Mayo Clin Proc 2007;82:286; Lancet
1995;346:865; Lancet 1997;350:1495; Cochrane 2010 Issue 9. Art. No.: CD002907

TIMING OF ENDOSCOPY

TIMING OF ENDOSCOPY FOR UGIB
• Patients hospitalized with UGIB
– ≤ 24 hrs • length of stay, surgery
• Low-risk patients (normal VS, no comorbidity)
– As soon as possible in non-emergent setting
• ≤ 2-6 hrs lowers cost by allowing early discharge (~40-45%)
• High-risk patients (e.g., BP, HR, cirrhosis)
– Consider ≤ 12 hrs • May transfusions, hospital days, mortality
– ?Avoid <2 - <6 hrs
• May adverse events, mortality
Cooper et al. Med Care 1998;36:462; GIE 1999:49:145; Lee et al. GIE 1999;50:755; Bjorkman et al. GIE 2004;60:1; Lin et al. JCG 1996;22:267;
Lim et al. Endoscopy 2011; 43:300; Tsoi et al. Nat Rev Gastr Hep 2009;6:463; Yen et al Am J Em Med 1997;15:644; Laursen et al UEGW 2015

MANAGEMENT OF
BLEEDING ULCERS
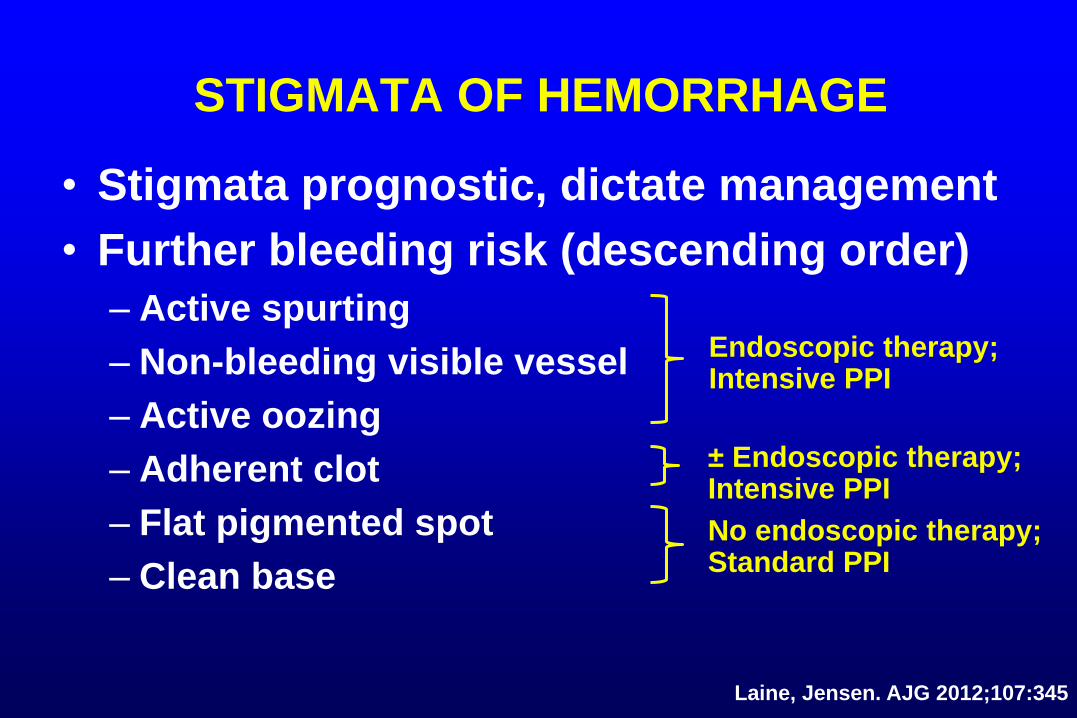
STIGMATA OF HEMORRHAGE
• Stigmata prognostic, dictate management
• Further bleeding risk (descending order)
– Active spurting
– Non-bleeding visible vessel
– Active oozing
– Adherent clot
– Flat pigmented spot
– Clean base
Laine, Jensen. AJG 2012;107:345
Endoscopic therapy; Intensive PPI
± Endoscopic therapy; Intensive PPI
No endoscopic therapy; Standard PPI

ENDOSCOPIC THERAPY Dual Therapy vs. Monotherapy
• Epinephrine should not be used alone
– Less effective than other monotherapies
– Significant benefit by adding 2nd modality
• Thermal, sclerosant, clips can be used alone
• Sclerosant, clips alone may be less effective
for initial hemostasis in active bleeding
Laine, McQuaid. GIE 2009;7:33; Barkun et al. AIM 2010;152:101; Laine, Jensen AJG 2012;107:345

TECHNIQUES FOR ENDOSCOPIC THERAPY Thermal Therapy
• Large 3.2 mm probe with the least angulation and
as close as possible with firm/maximal pressure
• Multiple applications in ulcer base around and on
the bleeding site until bleeding stops, vessel
flattens, and base whitens
• Bipolar electrocoagulation (BPEC): 8-10 second
applications at setting ~15W
• Heater probe: setting of 30 joules
Laine. Gastro 1991;100:107; Laine, Jensen . AJG 2012;107:345

TECHNIQUES FOR ENDOSCOPIC THERAPY Injection Therapy
• Epinephrine (1:10,000 or 1:20,000)
– 0.5 – 2.0 ml aliquots around and in bleeding site
– Active bleeding: treat until bleeding stops, slows
– Non-bleeding: all 4 quadrants around bleeding site
• Absolute alcohol
– 0.1 – 0.2 ml aliquots with limitation of 1 – 2 ml
• Concern about tissue injury with higher volumes
Laine, Jensen . AJG 2012;107:345

TECHNIQUES FOR ENDOSCOPIC THERAPY Clips
• Place clips over the bleeding site and adjacent to
the stigmata of hemorrhage
– Attempting to close the underlying artery
Laine, Jensen . AJG 2012;107:345

ANTISECRETORY THERAPY
• Active bleeding, visible vessel, clot
– IV PPI bolus followed by continuous infusion for
3 days recommended by current guidelines
– Intermittent PPI (oral or IV) comparable to 3-day
course of continuous infusion
– Twice-daily oral PPI from day 4 to 14
• Flat spot, clean base
– Standard oral PPI
Laine, McQuaid CGH 2009;7:33; Barkun et al. AIM 2010;152:101; Laine, Jensen AJG 2012:107:345;
Sachar et al. JAMA Int Med 2014; Cheng et al. Gut 2014;63:1864

MANAGEMENT OF
VARICEAL BLEEDING

COAGULOPATHY AND
THROMBOCYTOPENIA

PT IS NOT A RELIABLE INDICATOR OF COAGULATION STATUS IN CIRRHOSIS
• PT measures procoagulant activity only
• Parallel in pro- and anti-coagulant factors
– Thrombin generation: cirrhotics ≈ healthy subjects
• Elevated PT or INR not predictive of peri-
procedural bleeding in SR of 25 studies
Tripodi et al. NEJM 2011;365:147; Segal et al. Transfusion 2005;45:1413; Tripodi et al. APT 2007;26:14

FRESH FROZEN PLASMA
FOR PROLONGED
PROTHROMBIN TIME

THROMBOCYTOPENIA Platelet Transfusion for Bleeding or High-Risk Procedures?
• Platelets from cirrhotic patients generate
thrombin ~normally
• Decreased platelets → ↓thrombin generation
– 56,000/mm3 generates thrombin at the 10th
percentile of control values
– Rationale for platelet transfusion in patients with
bleeding or undergoing surgery
Tripodi et al. Hepatology 2006;44:440

MANAGEMENT OF ACUTE
BLEEDING EPISODE

MANAGEMENT OF ACUTE
ESOPHAGEAL VARICEAL BLEEDING
• Ligation + vasoactive medication (octreotide)
– Ligation superior to vasoactive medication
– Ligation + octreotide superior to ligation alone
• Consider early TIPS in high-risk patients
– Child C (score ≤ 13), or Child B with active bleeding
• Significant decreases in further bleeding and mortality
– Non-significant decreases in encephalopathy
• Covered SEMS an option if refractory
de Franchis J Hepatol 2015;63:743; Chen et al. J Chinese Med Ass 2006;69:60; Sung et al. Lancet 1995;346:1666;
Monescillo et al. Hepatol 2004;40:793; Garcia-Pagan, et al. NEJM 2010;362:2370

PREVENTION OF RECURRENT
VARICEAL BLEEDING

PREVENTION OF RECURRENT
ESOPHAGEAL VARICEAL BLEEDING
• Ligation + β-blocker
– Combination more effective in reducing variceal
rebleeding than either therapy alone
de Franchis J Hepatol 2015;63:743; Thiele et al. APT 2012;35:1155

PREVENTION OF RECURRENT
ESOPHAGEAL VARICEAL BLEEDING Other Medical Therapies?
• Nitrate (ISMN) + β-blocker decreases HVPG,
variceal rebleeding vs. β-blocker alone
– Increased side effects
• Carvedilol decreases HVPG more frequently
than β-blocker and is clinically effective
– Not different than ISMN + β-blocker or ligation in
RCTs
Gluud et al. APT 2010;32:859; Lo et al. J Gastro Hep 2012;27:1681; Stanley et al. J Hepatol 2014;61:1014

RECURRENT VARICEAL BLEEDING
DESPITE 2° PREVENTIVE THERAPY
• TIPS
de Franchis J Hepatol 2015;63:743
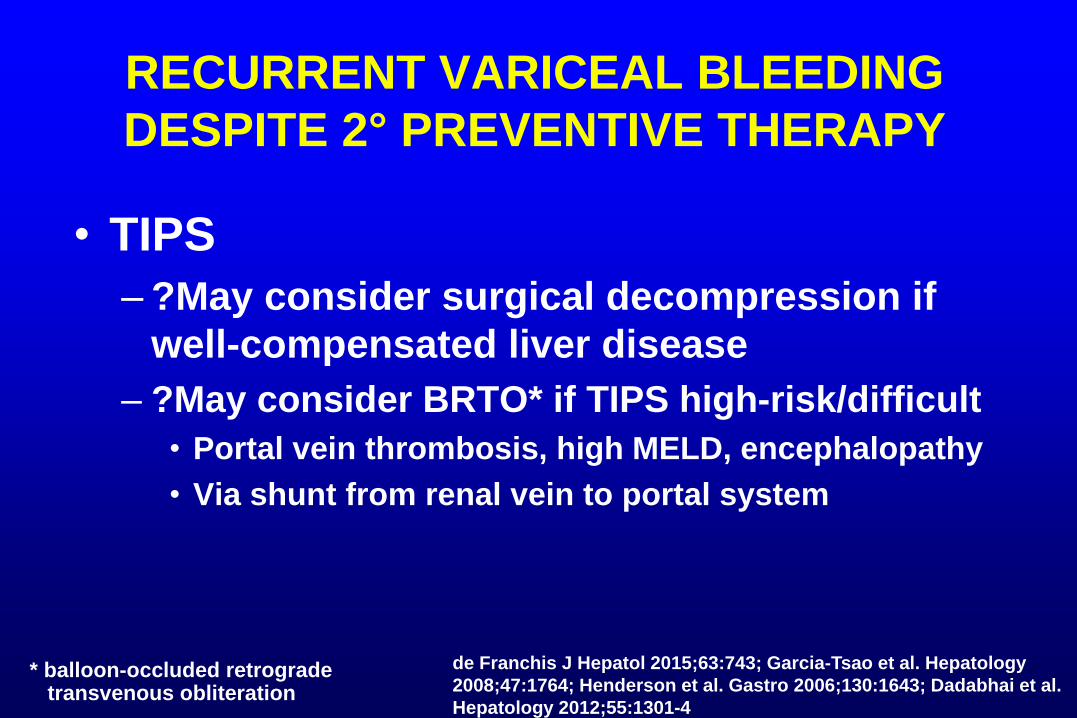
RECURRENT VARICEAL BLEEDING
DESPITE 2° PREVENTIVE THERAPY
• TIPS
– ?May consider surgical decompression if
well-compensated liver disease
– ?May consider BRTO* if TIPS high-risk/difficult
• Portal vein thrombosis, high MELD, encephalopathy
• Via shunt from renal vein to portal system
de Franchis J Hepatol 2015;63:743; Garcia-Tsao et al. Hepatology
2008;47:1764; Henderson et al. Gastro 2006;130:1643; Dadabhai et al.
Hepatology 2012;55:1301-4
* balloon-occluded retrograde transvenous obliteration

INITIAL MANAGEMENT OF UPPER GI BLEEDING
• Assess risk
• Pre-EGD medications
– Consider erythromycin, PPI
• PPIs recommended if EGD delayed or not done
– Cirrhotic: octreotide (w/o PPI), antibiotic
• Early EGD (< 24 hrs)
– Low-risk: as early as 2-6 hrs lowers costs
– High-risk: < 12 hrs may improve outcomes

MANAGEMENT OF MAJOR ULCER BLEEDING
• Endoscopic therapy (repeat for rebleed)
• Constant infusion IV PPI vs. intermittent PPI
• Treat patients with
– Active bleeding
– Non-bleeding visible vessel
– Adherent clot (? PPI alone)

MANAGEMENT OF
ESOPHAGEAL VARICEAL BLEEDING
• Acute Bleeding Episode
– Vasoactive drug (e.g., octreotide x 2-5 days)*
– Antibiotics*
– Endoscopic ligation
– Consider TIPS in high-risk patients
• Prevention of Recurrent Bleeding
– Endoscopic ligation
– β-blocker
• TIPS if failure of medical/endoscopic therapy
* Begin before EGD

















