Urinary Tract Infection in Children: When to Worry Curtis J. Clark, MD a , William A. Kennedy II MD a,b , Linda D. Shortliffe, MD a,b, * Urinary tract infection (UTI) is a significant concern for parents as well as for children who acquire them. While primary care physicians and pediatri- cians are the front line, dealing with the initial management of UTI, they turn to urologists when faced with more complicated infections. This article reviews the diagnosis and management of UTI, and examines scenarios in which the clinician should have a heightened level of concern when dealing with UTI in the pediatric population. The comprehensive epidemiology of UTI has been well described. 1 The overall incidence of UTI in the prepubertal pediatric population is 3% in girls and 1% in boys. The incidence of UTI varies with age and sex. Infant girls have an incidence of 0.4% to 0.1%, which increases to 0.9% to 1.4% between the ages 1 and 5 years, and peaks with an incidence of 0.7% to 2.3% in school-aged girls. In contrast, infant boys have an incidence of UTI of 0.188% (circumcised) and 0.702% (uncircum- cised), which decreases to 0.1% to 0.2% between ages 1 and 5 years, followed by 0.04% to 0.2% in school-aged boys. 2 In febrile children presenting to the emergency department, UTI is more common than in healthy children, with an inci- dence between 3% and 5% in most studies. 3 Racial differences also exist, including a low inci- dence in African American children and higher inci- dence in Caucasian girls relative to other races. 1 Other risk factors associated with UTI include anomalies of the urinary tract (anatomic, func- tional, or neurologic) and systemic abnormalities (diabetes mellitus, compromised immune system, and so forth). The pathogenesis of UTI is based both on the bacteria that cause infection and on patient- specific factors. Bacteria common in UTI are predominantly of enteric origin. Escherichia coli is the most frequent cause of all types of UTI, while group B streptococcal infection is relatively more common in neonates. Bacteria tend to colonize the periurethral area, migrating in a retrograde fashion to reach the urinary tract. Bacteria may also be introduced into the urinary tract via instru- mentation. Systemic infections may also result in UTI through seeding of the urinary system. Once present within the urinary tract, bacteria can be cleared by the emptying of urine or can adhere to the urothelial lining, resulting in infection. After colonization of the urinary tract, virulence factors such as fimbriae may assist bacteria in causing an infection. Diagnosis of UTI is based on clinical symptoms and the results of a urine culture. Classic symp- toms of UTI in adults are dysuria, frequency, hesi- tancy, and flank pain. Unfortunately, young children often lack the ability to identify and describe these symptoms. Symptoms in children Disclosures: L.D.S. is on the Board of directors of Vivus, Inc. a Department of Urology, Lucile Packard Children’s Hospital, Stanford University Medical Center, Stanford University School of Medicine, S-287, 300 Pasteur Drive, Stanford, CA 94305-5118, USA b Department of Pediatric Urology, Lucile Packard Children’s Hospital, Stanford University School of Medicine, S-287, 300 Pasteur Drive, Stanford, CA 94305-5118, USA * Corresponding author. Department of Urology, Lucile Packard Children’s Hospital, Stanford University Medical Center, Stanford University School of Medicine, S-287, 300 Pasteur Drive, Stanford, CA 94305-5118. E-mail address: [email protected]KEYWORDS Urinary tract infection Pediatric Cystitis Pyelonephritis Treatment Urol Clin N Am 37 (2010) 229–241 doi:10.1016/j.ucl.2010.03.009 0094-0143/10/$ – see front matter ª 2010 Elsevier Inc. All rights reserved. urologic.theclinics.com
Transcript
Urinary Tract Infectionin Children: Whento Worry
Curtis J. Clark, MDa, William A. Kennedy II MDa,b,Linda D. Shortliffe, MDa,b,*
Urinary tract infection (UTI) is a significant concernfor parents as well as for children who acquirethem. While primary care physicians and pediatri-cians are the front line, dealing with the initialmanagement of UTI, they turn to urologists whenfaced with more complicated infections. Thisarticle reviews the diagnosis and management ofUTI, and examines scenarios in which the clinicianshould have a heightened level of concern whendealing with UTI in the pediatric population.
The comprehensive epidemiology of UTI hasbeen well described.1 The overall incidence ofUTI in the prepubertal pediatric population is 3%in girls and 1% in boys. The incidence of UTI varieswith age and sex. Infant girls have an incidence of0.4% to 0.1%, which increases to 0.9% to 1.4%between the ages 1 and 5 years, and peaks withan incidence of 0.7% to 2.3% in school-aged girls.In contrast, infant boys have an incidence of UTI of0.188% (circumcised) and 0.702% (uncircum-cised), which decreases to 0.1% to 0.2% betweenages 1 and 5 years, followed by 0.04% to 0.2% inschool-aged boys.2 In febrile children presentingto the emergency department, UTI is morecommon than in healthy children, with an inci-dence between 3% and 5% in most studies.3
Racial differences also exist, including a low inci-dence in African American children and higher inci-dence in Caucasian girls relative to other races.1
Disclosures: L.D.S. is on the Board of directors of Vivus, Ia Department of Urology, Lucile Packard Children’s HoUniversity School of Medicine, S-287, 300 Pasteur Drive,b Department of Pediatric Urology, Lucile Packard ChildrS-287, 300 Pasteur Drive, Stanford, CA 94305-5118, USA* Corresponding author. Department of Urology, LuciMedical Center, Stanford University School of Medicine,E-mail address: [email protected]
Urol Clin N Am 37 (2010) 229–241doi:10.1016/j.ucl.2010.03.0090094-0143/10/$ – see front matter ª 2010 Elsevier Inc. All
Other risk factors associated with UTI includeanomalies of the urinary tract (anatomic, func-tional, or neurologic) and systemic abnormalities(diabetes mellitus, compromised immune system,and so forth).
The pathogenesis of UTI is based both on thebacteria that cause infection and on patient-specific factors. Bacteria common in UTI arepredominantly of enteric origin. Escherichia coliis the most frequent cause of all types of UTI, whilegroup B streptococcal infection is relatively morecommon in neonates. Bacteria tend to colonizethe periurethral area, migrating in a retrogradefashion to reach the urinary tract. Bacteria mayalso be introduced into the urinary tract via instru-mentation. Systemic infections may also result inUTI through seeding of the urinary system. Oncepresent within the urinary tract, bacteria can becleared by the emptying of urine or can adhereto the urothelial lining, resulting in infection. Aftercolonization of the urinary tract, virulence factorssuch as fimbriae may assist bacteria in causingan infection.
Diagnosis of UTI is based on clinical symptomsand the results of a urine culture. Classic symp-toms of UTI in adults are dysuria, frequency, hesi-tancy, and flank pain. Unfortunately, youngchildren often lack the ability to identify anddescribe these symptoms. Symptoms in children
nc.spital, Stanford University Medical Center, StanfordStanford, CA 94305-5118, USAen’s Hospital, Stanford University School of Medicine,
le Packard Children’s Hospital, Stanford UniversityS-287, 300 Pasteur Drive, Stanford, CA 94305-5118.
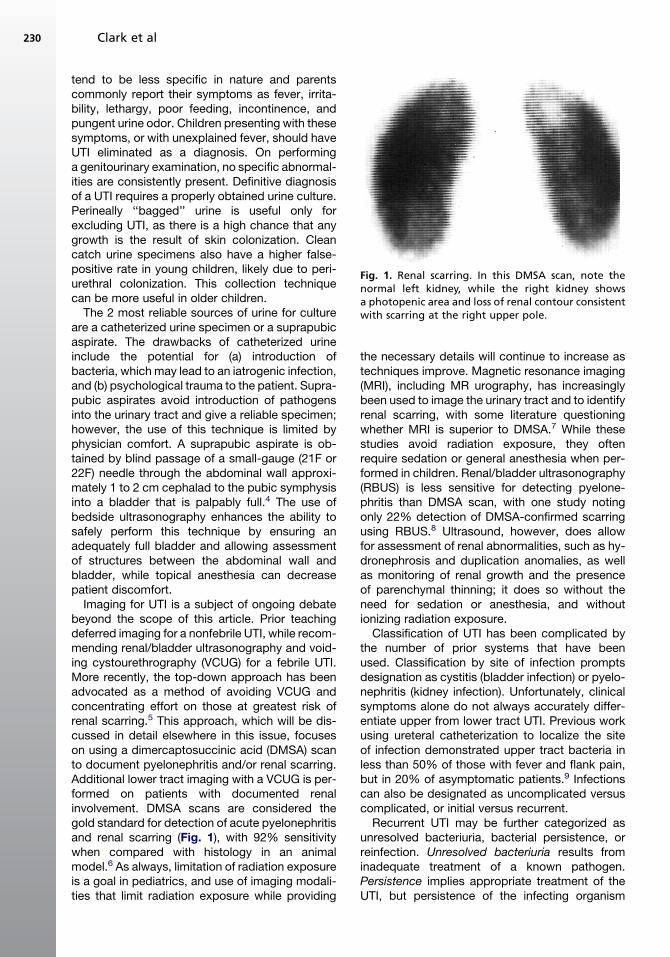
Fig. 1. Renal scarring. In this DMSA scan, note thenormal left kidney, while the right kidney showsa photopenic area and loss of renal contour consistentwith scarring at the right upper pole.
Clark et al230
tend to be less specific in nature and parentscommonly report their symptoms as fever, irrita-bility, lethargy, poor feeding, incontinence, andpungent urine odor. Children presenting with thesesymptoms, or with unexplained fever, should haveUTI eliminated as a diagnosis. On performinga genitourinary examination, no specific abnormal-ities are consistently present. Definitive diagnosisof a UTI requires a properly obtained urine culture.Perineally ‘‘bagged’’ urine is useful only forexcluding UTI, as there is a high chance that anygrowth is the result of skin colonization. Cleancatch urine specimens also have a higher false-positive rate in young children, likely due to peri-urethral colonization. This collection techniquecan be more useful in older children.
The 2 most reliable sources of urine for cultureare a catheterized urine specimen or a suprapubicaspirate. The drawbacks of catheterized urineinclude the potential for (a) introduction ofbacteria, which may lead to an iatrogenic infection,and (b) psychological trauma to the patient. Supra-pubic aspirates avoid introduction of pathogensinto the urinary tract and give a reliable specimen;however, the use of this technique is limited byphysician comfort. A suprapubic aspirate is ob-tained by blind passage of a small-gauge (21F or22F) needle through the abdominal wall approxi-mately 1 to 2 cm cephalad to the pubic symphysisinto a bladder that is palpably full.4 The use ofbedside ultrasonography enhances the ability tosafely perform this technique by ensuring anadequately full bladder and allowing assessmentof structures between the abdominal wall andbladder, while topical anesthesia can decreasepatient discomfort.
Imaging for UTI is a subject of ongoing debatebeyond the scope of this article. Prior teachingdeferred imaging for a nonfebrile UTI, while recom-mending renal/bladder ultrasonography and void-ing cystourethrography (VCUG) for a febrile UTI.More recently, the top-down approach has beenadvocated as a method of avoiding VCUG andconcentrating effort on those at greatest risk ofrenal scarring.5 This approach, which will be dis-cussed in detail elsewhere in this issue, focuseson using a dimercaptosuccinic acid (DMSA) scanto document pyelonephritis and/or renal scarring.Additional lower tract imaging with a VCUG is per-formed on patients with documented renalinvolvement. DMSA scans are considered thegold standard for detection of acute pyelonephritisand renal scarring (Fig. 1), with 92% sensitivitywhen compared with histology in an animalmodel.6 As always, limitation of radiation exposureis a goal in pediatrics, and use of imaging modali-ties that limit radiation exposure while providing
the necessary details will continue to increase astechniques improve. Magnetic resonance imaging(MRI), including MR urography, has increasinglybeen used to image the urinary tract and to identifyrenal scarring, with some literature questioningwhether MRI is superior to DMSA.7 While thesestudies avoid radiation exposure, they oftenrequire sedation or general anesthesia when per-formed in children. Renal/bladder ultrasonography(RBUS) is less sensitive for detecting pyelone-phritis than DMSA scan, with one study notingonly 22% detection of DMSA-confirmed scarringusing RBUS.8 Ultrasound, however, does allowfor assessment of renal abnormalities, such as hy-dronephrosis and duplication anomalies, as wellas monitoring of renal growth and the presenceof parenchymal thinning; it does so without theneed for sedation or anesthesia, and withoutionizing radiation exposure.
Classification of UTI has been complicated bythe number of prior systems that have beenused. Classification by site of infection promptsdesignation as cystitis (bladder infection) or pyelo-nephritis (kidney infection). Unfortunately, clinicalsymptoms alone do not always accurately differ-entiate upper from lower tract UTI. Previous workusing ureteral catheterization to localize the siteof infection demonstrated upper tract bacteria inless than 50% of those with fever and flank pain,but in 20% of asymptomatic patients.9 Infectionscan also be designated as uncomplicated versuscomplicated, or initial versus recurrent.
Recurrent UTI may be further categorized asunresolved bacteriuria, bacterial persistence, orreinfection. Unresolved bacteriuria results frominadequate treatment of a known pathogen.Persistence implies appropriate treatment of theUTI, but persistence of the infecting organism
Urinary Tract Infection in Children 231
within a nidus of infection or within an area that isisolated from treatment. On immediate posttreat-ment urine culture the same bacterial pathogenwill quickly return. Reinfection requires repeatedUTI with different bacteria, which may includedifferent bacterial serotypes and clones. Theimportance of differentiating between persistenceand reinfection is that persistence may be surgi-cally correctable.
TREATMENT OF UTI
Treatment of UTI focuses on the site of infection,presence of fever, and the pathogen causing theinfection. Ampicillin and gentamicin continue tobe the mainstay of empirical treatment of pyelone-phritis. The use of a third-generation cephalo-sporin may be considered with the knowledgethat its coverage will not include Enterococcusand that there is emerging extended-spectrum b-lactam resistance. When a patient has recentlybeen on antibiotics, it is worthwhile to considerusing alternative choices due to the possibility ofresistant bacteria. Once afebrile for 24 to 48 hours,consideration can be given to transitioning to oral(PO) antibiotics. Improvement in serum markerssuch as the white blood cell count or C-reactiveprotein is also encouraging when considering tran-sition to oral antibiotics. The use of longer durationof intravenous (IV) antibiotics has not been shownto be superior to an early transition to PO therapyin preventing scarring based on DMSA scans at 9months.10 In all cases, the combination of IV andoral therapy should include 10 to 14 days of appro-priate antibiotics, with neonates and more severeinfections favoring the longer duration.
Although traditional teaching has been thatfebrile UTI should be treated promptly with IV anti-biotics in an inpatient setting to avoid renal scar-ring, recent data have brought this teaching intoquestion. In a study by Hewitt and colleagues11
from Italy, the frequency of renal scarring onDMSA scan at 1 year was similar (approximately30%) in those treated early in a comparison withtreatment by a delayed fashion. Nonetheless,treatment should be started as soon as possibleto relieve symptoms and with the hope of avoidingrenal scarring. Even with upper tract involvement,outpatient treatment of UTI has been shown tobe safe and effective, particularly in older childrenwho are tolerating oral intake and are clinicallystable.12,13 In these cases, outpatient treatmentwith trimethoprim/sulfamethoxazole (TMP/SMX),cephalosporins, or fluoroquinolones are viableoptions. Nitrofurantoin is inadequate when renalinvolvement is suspected as a result of poor tissuelevels. In addition, daily intramuscular (IM) injection
of a once-a-day broad-spectrum antibiotic (suchas ceftriaxone) is an option. This treatment shouldbe continued either until identification/sensitivitiescan direct oral therapy, or for the entire outpatientcourse when more convenient than parenteralantibiotics using a peripherally inserted centralcatheter. A conservative approach of hospitaladmission for IV antibiotics is justified when theclinical picture, social scenario, or patient age(particularly neonates) dictates. In these cases,IV rehydration and broad-spectrum antibioticsare administered.
Cystitis in children can safely be treated usingnitrofurantoin, sulfonamides, TMP/SMX, trimetho-prim alone, and cephalosporins. In addition, cipro-floxacin is also used in children, for whom it isapproved as a second-line therapy in complicatedUTI.14 Use of ciprofloxacin in children is reservedfor more serious cases due to concerns overpotential cartilage damage. Fortunately, in studiesof children who received ciprofloxacin, complica-tions have been reversible after discontinuation.15
Most often, TMP/SMX or nitrofurantoin is a goodinitial therapy for uncomplicated cystitis until finalurine culture and sensitivities have returned.Regional resistance to TMP/SMX is known, andthis should be taken into account in the decisionto use TMP/SMX as initial therapy. Once finalsensitivities are reported, treatment should beadjusted to ensure appropriate antibiotic coverageof the infecting organism. The addition of an IMantibiotic dosage has not been shown to be ofsignificant benefit in febrile UTI16 and its usage incystitis is likely not warranted. Duration of treat-ment is largely age based in this population. A 3-day course is adequate in the clinically stable childwith uncomplicated cystitis,17 while longer treat-ment courses (7–10 days) are likely appropriatefor children younger than 2 years. Althougha recent study from Canada has shown feasibilityof outpatient ambulatory treatment with parenteralantibiotics in 1- to 3-month old children with febrileUTI,18 the very young and those who are dehy-drated, unable to tolerate oral medications, ortoxic appearing warrant a conservative approachwith admission for parenteral antibiotics andhydration.
WHEN TO WORRY LESS
It is important for clinicians to be familiar with situa-tions in which there is a relatively low risk forpatients. These scenarios can be perplexing forparents and primary care physicians who donot encounter such urologic scenarios ona consistent basis. For example, urine culturesgrowing Lactobacillus species, coagulase-negative
Clark et al232
staphylococci, and Corynebacterium species arenot considered pathogens in otherwise healthy chil-dren of 2 months to 2 years old, and treatment isunnecessary.19
During the period of toilet-training, children areat an increased risk of lower UTI because ofchanges in voiding and stooling habits. Less thanoptimal hygiene, in combination with the newlydeveloped ability to hold one’s urine, can lead toUTIs. While still warranting treatment, these infec-tions may be more related to functional changes.In the case of an isolated UTI during toilet-training,establishing good voiding and stooling habits isthe primary goal after initial treatment of the UTI.
The presence of a UTI in the setting of correctedor spontaneously resolved reflux can cause signif-icant anxiety for parents and primary care physi-cians, while not posing as great a risk asperceived. After the initial diagnosis of vesicoure-teral reflux (VUR), parents often become condi-tioned to associate UTI and the risk of damageto the kidneys. The correction of VUR does notdecrease the risk of a child developing a lowerUTI but only eliminates the reflux of infected urineinto the kidney, thereby preventing or delaying thedevelopment of upper UTI. It is important to ensurethat parents understand the purpose of VURcorrection, are informed that VUR correctiondoes not alter host susceptibility to UTI, and arecounseled to seek appropriate treatment for UTI.
Finally, a clinical scenario that is challenging tounderstand is asymptomatic bacteriuria. Clinicalsituations exist in which colonization of the urinarytract is inevitable. In these situations, the presenceof bacteria is normal and does not require treat-ment despite a positive urine culture. Examplesof scenarios in which the urinary tract can be ex-pected to be colonized are patients with long-term indwelling tubes, patients performing cleanintermittent catheterization (CIC), patients withintestinal neobladders or augmented bladders,and patients in whom the urinary tract is openedto the skin (vesicostomy, ureterostomy, and soforth). In these cases, routine bacteria culturedfrom the urinary tract and not causing significantclinical symptoms (dysuria, incontinence, fever,and so forth) should not be treated. One shouldalso favor observation for bacteria noted ona screening urinalysis performed in an asymptom-atic patient without complicating factors. Treat-ment of these asymptomatic bacteria will onlyallow recolonization with different, potentiallymore pathogenic bacteria and increase the riskof antibiotic resistance. Fever in a setting ofasymptomatic bacteriuria should be worked upas a fever of unknown origin, including urineculture and blood cultures, with treatment as
a UTI reserved for cases in which another sourceis not identified. Pyuria on a concurrent urine anal-ysis can aid in confirming the diagnosis of clinicalUTI. While the aforementioned situations areexamples of times when excessive concern isnot warranted, one should always use commonsense when approaching these issues. Whenadditional symptoms, repeated infections, ora confusing clinical scenario presents, furtherinvestigation and an increased clinical index ofsuspicion for the presence of more seriousurologic issues is always reasonable.
WHEN TO WORRY
The authors now focus attention on situations inwhich UTI is more complicated, often requiringa high index of clinical suspicion and a lowthreshold to proceed to admission, broad-spec-trum antibiotics, further investigation, and pedi-atric urology consultation. Attempts have beenmade to sort these infrequent scenarios intomore generalized groups; however, many patho-logic processes could be placed under multipleheadings. The rare nature of very complicatedUTI makes research comparing differentapproaches to treatment difficult. Prospectiveplacebo-controlled studies do not exist. In thesecomplex cases, there are undoubtedly multipleeffective ways to approach treatment. When theliterature does not provide clear evidence support-ing one approach, information is provided on theclinical pathway followed by the authors formanaging these difficult situations.
Some general principles apply in these complexclinical scenarios. The presence of abnormalanatomy, particularly abnormal drainage, shouldalways prompt additional workup in the presenceof UTI. The presence of prior renal scarring shouldalso prompt additional concern, as these patientsare starting with fewer functioning nephrons andhave established they are susceptible to renalinjury. Failure of a patient to respond to conven-tional treatment of a UTI should also promptconcern. Additional workup should be performedto confirm that culture-specific antibiotics arebeing used, that adequate drainage exists, andthat the antibiotics reach all sites of bacterialinfection.
Bad Pathology
While a single febrile UTI is a cause for concern,the presence of repeated febrile infections shouldalert all physicians to the need for a more exten-sive evaluation. One must be concerned aboutthe presence of a physiologic or anatomic patientfactor as the origin. While most renal scarring is felt
Urinary Tract Infection in Children 233
to occur with the first episode of pyelonephritis,the ‘‘big bang theory,’’1 recurrent pyelonephritiscan cause increased renal scarring. A comprehen-sive workup, with special focus on voiding andbowel habits, family history of recurrent UTI, andactivities preceding the infections, should beundertaken. Urine culture results should be re-viewed to assess for evidence of bacterial persis-tence. If true persistence exists, further imagingshould be performed to evaluate for a source ofthe bacteria. Renal bladder ultrasonography andvoiding cystourethrography will allow one toquickly assess the upper and lower tract anatomywhile minimizing radiation exposure. Additionalimaging may be required based on the clinical situ-ation. In a toilet-trained child, a urinary flow rateand postvoid residual should be obtained toassess bladder emptying. Consideration shouldbe given to antibiotic prophylaxis.
Pyonephrosis and emphysematous pyelone-phritis are 2 severe infections of the kidney.Pyonephrosis is the presence of purulence andsediment within the renal collecting system. Pre-senting with a picture similar to pyelonephritis,these patients may not have resolution with antibi-otics alone because of the presence of obstruc-tion. In children most pyonephrotic kidneys arenonfunctional or have very poor function.20 Treat-ment always involves broad-spectrum antibioticsand frequently drainage of the collecting system,either via retrograde stent or nephrostomy tubeplacement. Emphysematous pyelonephritis is aninfection with air seen in the collecting system onimaging. This entity is extremely rare in children.Percutaneous drainage and antibiotics should beconsidered first-line therapy. Nephrectomy, whichwas previously considered the treatment ofchoice, should be reserved for those who do notrespond to conservative management.
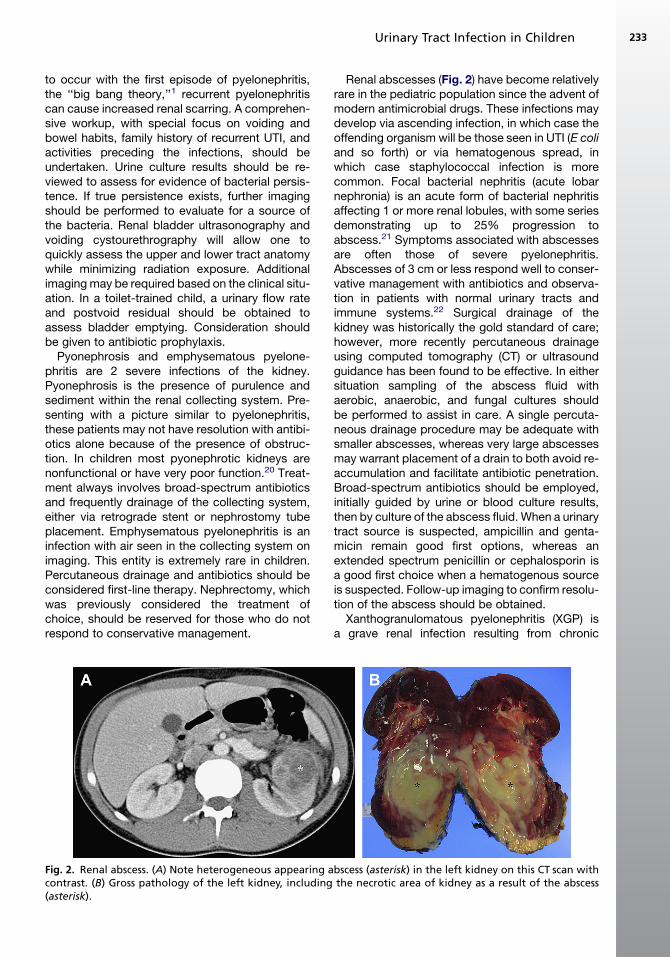
Fig. 2. Renal abscess. (A) Note heterogeneous appearing acontrast. (B) Gross pathology of the left kidney, including(asterisk).
Renal abscesses (Fig. 2) have become relativelyrare in the pediatric population since the advent ofmodern antimicrobial drugs. These infections maydevelop via ascending infection, in which case theoffending organism will be those seen in UTI (E coliand so forth) or via hematogenous spread, inwhich case staphylococcal infection is morecommon. Focal bacterial nephritis (acute lobarnephronia) is an acute form of bacterial nephritisaffecting 1 or more renal lobules, with some seriesdemonstrating up to 25% progression toabscess.21 Symptoms associated with abscessesare often those of severe pyelonephritis.Abscesses of 3 cm or less respond well to conser-vative management with antibiotics and observa-tion in patients with normal urinary tracts andimmune systems.22 Surgical drainage of thekidney was historically the gold standard of care;however, more recently percutaneous drainageusing computed tomography (CT) or ultrasoundguidance has been found to be effective. In eithersituation sampling of the abscess fluid withaerobic, anaerobic, and fungal cultures shouldbe performed to assist in care. A single percuta-neous drainage procedure may be adequate withsmaller abscesses, whereas very large abscessesmay warrant placement of a drain to both avoid re-accumulation and facilitate antibiotic penetration.Broad-spectrum antibiotics should be employed,initially guided by urine or blood culture results,then by culture of the abscess fluid. When a urinarytract source is suspected, ampicillin and genta-micin remain good first options, whereas anextended spectrum penicillin or cephalosporin isa good first choice when a hematogenous sourceis suspected. Follow-up imaging to confirm resolu-tion of the abscess should be obtained.
Xanthogranulomatous pyelonephritis (XGP) isa grave renal infection resulting from chronic
bscess (asterisk) in the left kidney on this CT scan withthe necrotic area of kidney as a result of the abscess
Clark et al234
bacterial pyelonephritis and obstruction. XGP isnamed after the xanthoma cell, a foamy lipid-ladenhistiocyte that is seen on histology in this infection.Although primarily a condition that affects adults,XGP is occasionally seen in children, most oftenmales younger than 8 years. It is most often unilat-eral, causing significant destruction to a kidney.XGP may lead to a total loss of renal function onthe affected side, although it is often focal withinthe kidney in children.23 The most common caus-ative organisms are Proteus mirabilis and E coli.Radiographic imaging is notable for the presenceof obstruction, most often due to a calculus. TheXGP kidney classically has been described ashaving an appearance on CT scan similar toa ‘‘bear paw’’ as a result of dilated calyces andabscesses. Pediatric patients with XGP have clin-ical symptoms ranging from vague complaints tohemodynamic instability and sepsis. In a stablepatient with evidence of XGP, drainage of the col-lecting system, via stent or nephrostomy tube,may allow for true assessment of residual renalfunction. Placement of additional drains may beneeded if nonoperative management is consid-ered safe and desirable. Unfortunately, surgicalintervention is required in the majority of cases,often with the need for total nephrectomy. In rarecircumstances a partial nephrectomy may beeffective.
Bad Anatomy
The presence of anatomically or functionallyabnormal segments of the urinary tract can leadto rapid clinical deterioration when a patientdevelops a UTI. Renal insufficiency is one exampleof a functional issue. Impairment in renal function,as indicated by an elevated serum creatinine,limits the bioavailability of the antibiotics, makingcareful monitoring of serum levels necessary. Forexample, the potentially nephrotoxic antibioticsgentamicin and vancomycin require closemanagement to minimize the risk of renal injury.Imaging options in patients with compromisedrenal function may also be impacted. IV contrastfor CT scans and fluoroscopic examinations canbe nephrotoxic, particularly for those with renalinsufficiency. Gadolinium, which is used ascontrast for MRI, may cause nephrogenicsystemic fibrosis when used in patients with anestimated glomerular filtration rate less than 30mL/min/1.73 m2.24 These limitations may causedifficulties in diagnosing more complicated urinarypathology in this patient population. Another situa-tion in which renal function should prompt height-ened concern is the solitary kidney. When a patientwith a known solitary kidney presents with a febrile
UTI, their clinical condition should be carefullyevaluated to ensure appropriate antibiotics andadequate renal drainage.
The presence of poorly functioning andnonfunctional renal segments should prompt addi-tional concern when treating pyelonephritis, asthese areas can pose problems caused by poorantibiotic penetration. Examples of UTI in suchsegments include infection of a dysplastic upperpole moiety in a duplicated system or infection ofa devascularized segment of kidney after renaltrauma. In these cases, antibiotic administrationmay be ineffective and facilitating drainage, viaureteral stenting or percutaneous decompression,should be considered. Surgical excision of suchsegments may also be necessary.
The topic of vesicoureteral reflux (VUR) will bethoroughly addressed elsewhere in this issue.UTI in the setting of VUR can be a cause of signif-icant concern. Previous studies have establishedthat VUR without infection poses little risk for renalscarring or damage.1 When accompanied byinfection, however, VUR can lead to pyelonephritisand subsequent renal scarring, with the potentialfor reflux nephropathy in severe cases. Primarymanagement of VUR is a subject of much debate,particularly the role of antibiotic prophylaxis. Ina patient on antibiotic prophylaxis, developmentof one or more breakthrough infections is concern-ing. Assessment of compliance with antibioticprophylaxis and confirmation of appropriate anti-biotic dosing should be performed. Recent studieshave shown compliance with continual antibioticprophylaxis to be only 40%.25 The patient’s socialsituation should be assessed to ensure thatmedical care is sought in a timely fashion whenUTI symptoms are present. Renal imaging forassessment of renal growth and new scarringshould be undertaken. In these situations it maybe necessary to consider the options for surgicalcorrection of reflux.
Neuropathic bladder is another scenario inwhich anatomic and functional concerns canlead to serious consequences in the case of UTI.Inadequate bladder emptying, high-pressurestoring of urine, and high-pressure voiding cancomplicate the management of UTI. When accom-panying neurologic issues exist (such as myelo-meningocele or spina bifida) or in patients whohave undergone bladder reconstruction, the clin-ical symptoms may be masked. Symptoms maynot be present until an infection is severe or septicshock imminent. A high degree of suspicion isnecessary in these patients, with a low thresholdfor imaging of the upper tracts and evaluation ofthe bladder. High-pressure storage can lead toa trabeculated bladder and secondary VUR with
Urinary Tract Infection in Children 235
resultant risk to the kidneys if UTI occurs. High-pressure voiding or detrusor-sphincter dyssyner-gia might lead to bladder diverticula and chemicalor infectious epididymitis. Inadequate emptyingplaces these patients at risk for bladder stones.Stones may be infectious or noninfectious inorigin. Infectious stones are often a source ofbacterial persistence that will not resolve untilstone extraction is complete.
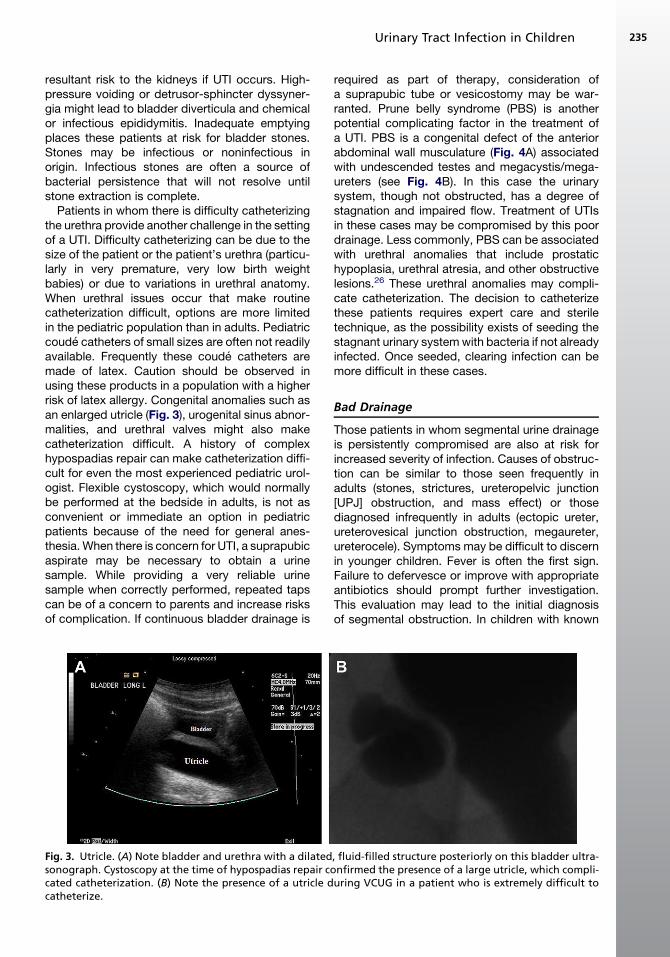
Patients in whom there is difficulty catheterizingthe urethra provide another challenge in the settingof a UTI. Difficulty catheterizing can be due to thesize of the patient or the patient’s urethra (particu-larly in very premature, very low birth weightbabies) or due to variations in urethral anatomy.When urethral issues occur that make routinecatheterization difficult, options are more limitedin the pediatric population than in adults. Pediatriccoude catheters of small sizes are often not readilyavailable. Frequently these coude catheters aremade of latex. Caution should be observed inusing these products in a population with a higherrisk of latex allergy. Congenital anomalies such asan enlarged utricle (Fig. 3), urogenital sinus abnor-malities, and urethral valves might also makecatheterization difficult. A history of complexhypospadias repair can make catheterization diffi-cult for even the most experienced pediatric urol-ogist. Flexible cystoscopy, which would normallybe performed at the bedside in adults, is not asconvenient or immediate an option in pediatricpatients because of the need for general anes-thesia. When there is concern for UTI, a suprapubicaspirate may be necessary to obtain a urinesample. While providing a very reliable urinesample when correctly performed, repeated tapscan be of a concern to parents and increase risksof complication. If continuous bladder drainage is
Fig. 3. Utricle. (A) Note bladder and urethra with a dilatedsonograph. Cystoscopy at the time of hypospadias repair ccated catheterization. (B) Note the presence of a utricle dcatheterize.
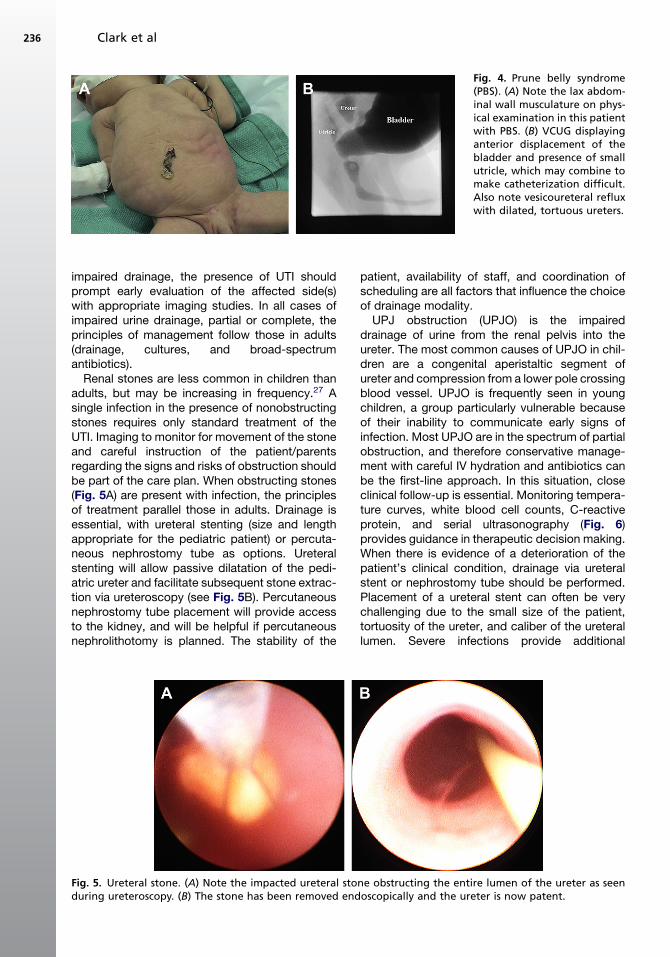
required as part of therapy, consideration ofa suprapubic tube or vesicostomy may be war-ranted. Prune belly syndrome (PBS) is anotherpotential complicating factor in the treatment ofa UTI. PBS is a congenital defect of the anteriorabdominal wall musculature (Fig. 4A) associatedwith undescended testes and megacystis/mega-ureters (see Fig. 4B). In this case the urinarysystem, though not obstructed, has a degree ofstagnation and impaired flow. Treatment of UTIsin these cases may be compromised by this poordrainage. Less commonly, PBS can be associatedwith urethral anomalies that include prostatichypoplasia, urethral atresia, and other obstructivelesions.26 These urethral anomalies may compli-cate catheterization. The decision to catheterizethese patients requires expert care and steriletechnique, as the possibility exists of seeding thestagnant urinary system with bacteria if not alreadyinfected. Once seeded, clearing infection can bemore difficult in these cases.
Bad Drainage
Those patients in whom segmental urine drainageis persistently compromised are also at risk forincreased severity of infection. Causes of obstruc-tion can be similar to those seen frequently inadults (stones, strictures, ureteropelvic junction[UPJ] obstruction, and mass effect) or thosediagnosed infrequently in adults (ectopic ureter,ureterovesical junction obstruction, megaureter,ureterocele). Symptoms may be difficult to discernin younger children. Fever is often the first sign.Failure to defervesce or improve with appropriateantibiotics should prompt further investigation.This evaluation may lead to the initial diagnosisof segmental obstruction. In children with known
, fluid-filled structure posteriorly on this bladder ultra-onfirmed the presence of a large utricle, which compli-uring VCUG in a patient who is extremely difficult to
Fig. 4. Prune belly syndrome(PBS). (A) Note the lax abdom-inal wall musculature on phys-ical examination in this patientwith PBS. (B) VCUG displayinganterior displacement of thebladder and presence of smallutricle, which may combine tomake catheterization difficult.Also note vesicoureteral refluxwith dilated, tortuous ureters.
Clark et al236
impaired drainage, the presence of UTI shouldprompt early evaluation of the affected side(s)with appropriate imaging studies. In all cases ofimpaired urine drainage, partial or complete, theprinciples of management follow those in adults(drainage, cultures, and broad-spectrumantibiotics).
Renal stones are less common in children thanadults, but may be increasing in frequency.27 Asingle infection in the presence of nonobstructingstones requires only standard treatment of theUTI. Imaging to monitor for movement of the stoneand careful instruction of the patient/parentsregarding the signs and risks of obstruction shouldbe part of the care plan. When obstructing stones(Fig. 5A) are present with infection, the principlesof treatment parallel those in adults. Drainage isessential, with ureteral stenting (size and lengthappropriate for the pediatric patient) or percuta-neous nephrostomy tube as options. Ureteralstenting will allow passive dilatation of the pedi-atric ureter and facilitate subsequent stone extrac-tion via ureteroscopy (see Fig. 5B). Percutaneousnephrostomy tube placement will provide accessto the kidney, and will be helpful if percutaneousnephrolithotomy is planned. The stability of the
Fig. 5. Ureteral stone. (A) Note the impacted ureteral stoduring ureteroscopy. (B) The stone has been removed end
patient, availability of staff, and coordination ofscheduling are all factors that influence the choiceof drainage modality.
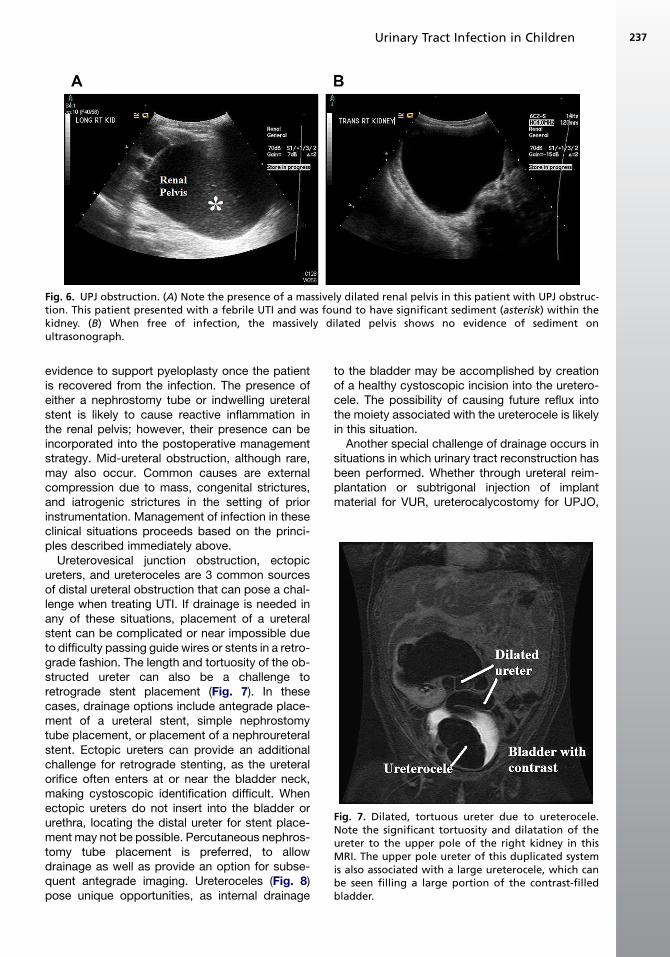
UPJ obstruction (UPJO) is the impaireddrainage of urine from the renal pelvis into theureter. The most common causes of UPJO in chil-dren are a congenital aperistaltic segment ofureter and compression from a lower pole crossingblood vessel. UPJO is frequently seen in youngchildren, a group particularly vulnerable becauseof their inability to communicate early signs ofinfection. Most UPJO are in the spectrum of partialobstruction, and therefore conservative manage-ment with careful IV hydration and antibiotics canbe the first-line approach. In this situation, closeclinical follow-up is essential. Monitoring tempera-ture curves, white blood cell counts, C-reactiveprotein, and serial ultrasonography (Fig. 6)provides guidance in therapeutic decision making.When there is evidence of a deterioration of thepatient’s clinical condition, drainage via ureteralstent or nephrostomy tube should be performed.Placement of a ureteral stent can often be verychallenging due to the small size of the patient,tortuosity of the ureter, and caliber of the ureterallumen. Severe infections provide additional
ne obstructing the entire lumen of the ureter as seenoscopically and the ureter is now patent.
Fig. 6. UPJ obstruction. (A) Note the presence of a massively dilated renal pelvis in this patient with UPJ obstruc-tion. This patient presented with a febrile UTI and was found to have significant sediment (asterisk) within thekidney. (B) When free of infection, the massively dilated pelvis shows no evidence of sediment onultrasonograph.
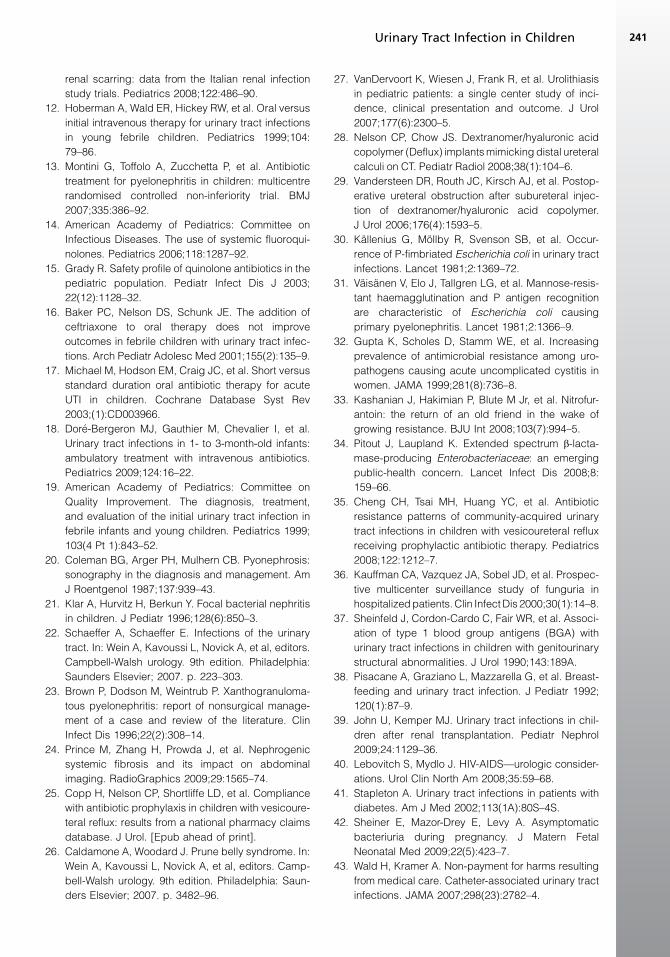
Fig. 7. Dilated, tortuous ureter due to ureterocele.Note the significant tortuosity and dilatation of theureter to the upper pole of the right kidney in thisMRI. The upper pole ureter of this duplicated systemis also associated with a large ureterocele, which canbe seen filling a large portion of the contrast-filledbladder.
Urinary Tract Infection in Children 237
evidence to support pyeloplasty once the patientis recovered from the infection. The presence ofeither a nephrostomy tube or indwelling ureteralstent is likely to cause reactive inflammation inthe renal pelvis; however, their presence can beincorporated into the postoperative managementstrategy. Mid-ureteral obstruction, although rare,may also occur. Common causes are externalcompression due to mass, congenital strictures,and iatrogenic strictures in the setting of priorinstrumentation. Management of infection in theseclinical situations proceeds based on the princi-ples described immediately above.
Ureterovesical junction obstruction, ectopicureters, and ureteroceles are 3 common sourcesof distal ureteral obstruction that can pose a chal-lenge when treating UTI. If drainage is needed inany of these situations, placement of a ureteralstent can be complicated or near impossible dueto difficulty passing guide wires or stents in a retro-grade fashion. The length and tortuosity of the ob-structed ureter can also be a challenge toretrograde stent placement (Fig. 7). In thesecases, drainage options include antegrade place-ment of a ureteral stent, simple nephrostomytube placement, or placement of a nephroureteralstent. Ectopic ureters can provide an additionalchallenge for retrograde stenting, as the ureteralorifice often enters at or near the bladder neck,making cystoscopic identification difficult. Whenectopic ureters do not insert into the bladder orurethra, locating the distal ureter for stent place-ment may not be possible. Percutaneous nephros-tomy tube placement is preferred, to allowdrainage as well as provide an option for subse-quent antegrade imaging. Ureteroceles (Fig. 8)pose unique opportunities, as internal drainage
to the bladder may be accomplished by creationof a healthy cystoscopic incision into the uretero-cele. The possibility of causing future reflux intothe moiety associated with the ureterocele is likelyin this situation.
Another special challenge of drainage occurs insituations in which urinary tract reconstruction hasbeen performed. Whether through ureteral reim-plantation or subtrigonal injection of implantmaterial for VUR, ureterocalycostomy for UPJO,
Fig. 8. (A) Note the appearance of a ureterocele on VCUG (arrow), seen early as the bladder was being filled withcontrast. (B) Note the appearance of another ureterocele as seen on ultrasonograph of the bladder.
Clark et al238
transverse ureteroureterostomy, or ureteropyelos-tomy for strictures, reconfiguration of the ureterscan complicate attempts to drain the affectedkidney(s) if obstruction occurs. Cross-trigonal re-implantation in the correction of VUR may causedifficulty in catheterizing the ureteral orifices. Useof flexible cystoscopes, angle-tipped wires, andpercutaneous bladder access to provide theappropriate angle for intubating the ureteral orificeare techniques that may aid in stent placement.The presence of extensive bladder trabeculationin the setting of reconfigured ureters can furthercomplicate attempts at internal stenting. Thiscondition may be seen in patients with neuropathicbladders or severe dysfunctional eliminationsyndrome in whom ureteral reimplantation hasbeen performed. The addition of intravenousindigo carmine or methylene blue may help inlocating these ureteral orifices. Subtrigonal injec-tion of dextranomer/hyaluronic acid (Deflux,Oceana Therapeutics, Inc, Edison, NJ, USA) maycause anxiety in the face of UTI by mimicking distalureteral stones on CT scan.28 In rare situations,subtrigonal injections have caused obstruction(<0.7%), but ureteral stenting can be accom-plished in these settings.29
Bad/Rare Bugs
The infecting organism in any UTI plays a large rolein how severe an infection becomes, throughpossession of virulence factors, resistance to anti-biotics, and other mechanisms. The classicexample of a mechanism through which bacteriapossess greater virulence is fimbriae, specificallyP-fimbriae. Fimbriae (or pili) are surface structuresinvolved in adherence. P-piliated E coli possessfimbriae that bind the human red cell P-groupantigen, leading to an increased risk of pyelone-phritis. Another factor favoring more virulentbacteria is the presence of mannose-resistant
hemagglutination, which is found in most E colithat cause pyelonephritis.30 Previous work has es-tablished that most bacteria causing pyelone-phritis in children are associated with P-pili ormannose-resistant hemagglutination.31 Additionalmechanisms used by bacteria include hydro-phobic properties and iron-binding capabilities.Additional proteins have been associated withE coli causing pyelonephritis; however, none arecurrently clinically relevant.
Development and usage of new antibiotics hasbrought about antibiotic resistance in bacteria.While resistance to penicillin remains the highest,in recent years resistance to TMP/SMX has beenincreasing.32 In addition, frequent use of fluoroqui-nolones for a variety of infections has led toincreased resistance to these antibiotics, whichhave high utility and good coverage in the urinarytract. Within pediatrics the issue of antibiotic resis-tance takes on greater importance because of thelimited number of antibiotic options approved foruse in children. The most common oral antibioticsused in pediatric urology remain amoxicillin, ceph-alexin, TMP/SMX, and nitrofurantoin. Antibioticresistance to nitrofurantoin remains low, leadingsome to recommend it as first-line treatment forthe uncomplicated afebrile UTI.33 Unfortunately,its lack of tissue levels limits utility in more seriousinfection.
Examples of bacteria affecting the urinary tractwith significant issues related to resistanceinclude: methicillin-resistant Staphylococcusaureus, vancomycin-resistant Enterococcus, andextended-spectrum b-lactamase (ESBL) bacteria,particularly E coli. Increasingly found within hospi-tals and the community, ESBL bacteria posesignificant problems due to the limitations in antibi-otics that may be used to treat them. Extended-spectrum b-lactamase–producing enterobacteriaeare able to inactivate b-lactam antibiotics viahydrolysis.34 One study from Taiwan noted an
Urinary Tract Infection in Children 239
increased risk of ESBL bacteria causing UTI inchildren on cephalexin prophylaxis.35 Surveysfrom multiple countries have demonstrated core-sistance to other antibiotics appearing withinthese bacteria, which has prompted the use ofcarbapenems as the first-line antibiotics in treatingthese infections.34
Atypical infecting organisms in the urinary tractcan also cause infection. A complete discussionof these organisms is beyond the scope of thisarticle. However, these atypical organisms maybe more difficult to diagnose due to their slowgrowth and endemic regions, which may differgreatly from the area of diagnosis. In addition,these atypical organisms may possess antibioticresistance, causing significant difficulty in treat-ment. One of the more common atypical causesof UTI is fungal infection. Fungal UTI is most oftencaused by Candida albicans and presents asa nosocomial infection affecting patients on antibi-otics with indwelling catheters. In these situations,any indwelling catheter should be changed.Consideration should be given to urine alkaliniza-tion and starting antifungal therapy, with theknowledge that resistance to standard antifungalsmay be present.36 Bladder irrigation with ampho-tericin B may be necessary in resistant cases.Upper tract fungal balls may require percutaneousremoval followed by antifungal irrigation. Aspergil-losis is a fungal infection most commonly seen inimmunocompromised individuals, which mayrequire amphotericin B irrigation. Other examplesof atypical pathogens include tuberculosis, whichcan occur in the urinary tract leading to strictures;schistosomiasis, which is a parasite frequentlyleading to bladder fibrosis and an increased riskof bladder cancer; and enterobiasis, which hasbeen implicated in chronic UTI.
Bad Genes/Immune System
Antibiotic use has led to a host of strong patho-gens with variable patterns of resistance. Despiteexposure to potent pathogens, the majority ofpeople do not develop UTI, pointing to the impor-tance of patient factors in the development of UTI.Unfortunately, this remains an area in whichresearch has not seen significant advances withapplicability in the clinical environment. Thediscovery of P-fimbriae as a virulence factor ledto additional research on the P blood group andits role as a receptor. Studies have shown a highprevalence of P1 blood group in both refluxingand nonrefluxing girls with recurrent pyelone-phritis. Other blood groups, such as ABO andLewis, as well as secretor phenotypes may alsoinfluence UTI. Certain Lewis blood types (a�b�,
a1b�) have been found to have a 3-times greaterrisk of recurrent UTI than those with a�b1.37 Whileproviding a basis for recurrent UTI in somepatients, these patient factors are not modifiablenor are they of significant utility in current clinicalpractice.
A variety of disease states and treatments canimpair the immune system and can lead to anincreased risk of infection and increased severityof infections that do occur. Examples include thevery young (neonates), the immunosuppressed(due to transplants or chemotherapy), humanimmunodeficiency virus (HIV) patients, and dia-betics. Neonates have a higher risk of infectionbecause of an incompletely developed immunesystem and deficiency of IgA. This risk of infectioncan be minimized through breastfeeding, which isprotective against infection, likely throughmaternal IgA.38 These patients require a conserva-tive approach, with a low threshold for admissionfor febrile UTI.
The prevalence of febrile UTI in transplantpatients has ranged from 15% to 33% in studies.39
Although E coli remains the most commonbacteria, published series have demonstratedincreased frequencies of other bacteria, includingthose with greater antibiotic resistance. Any infec-tion in these patients causes concern due toimmunosuppression and the risks to the transplantkidney. After treatment of the acute infection,consideration should be given to a complete eval-uation of anatomic, functional, and social factorsthat might be contributing to infection. Patientson chemotherapy also represent an at-risk popula-tion due to their lowered immunity, frequent inpa-tient status, and increased likelihood ofprocedures. UTI in patients on chemotherapyshould be treated aggressively with broad-spec-trum antibiotics, keeping in mind the potentialnephrotoxicity of chemotherapeutic and antibioticagents. Upper tract imaging to rule out anatomicabnormalities or obstruction should be consideredin these patients. Viral UTI is rare in immunocom-petent individuals, but not uncommon in theimmunocompromised patient. While potentiallycausing significant symptoms, such as hemor-rhagic cystitis, these infections are self-limitedand treatment is generally supportive in nature.
Patients with HIV are at increased risk of UTIfrom routine bacterial pathogens, particularlywhen CD4 counts fall below 500/mm3.40 HIV alsoincreases the risk of UTI due to atypical pathogenssuch as fungi, parasites, mycobacteria, andviruses. Diabetes is known to increase the risk ofUTI in adults and children, with more serious infec-tions being more common in diabetics as well.41
Because the prevalence of diabetes in children is
Clark et al240
increasing, the complications of this disease,including UTI, can be expected to increase as well.
Bad Social Situation
How severely a UTI affects a child can be signifi-cantly influenced by the social and family situation.Economic, language, racial, and cultural issuesmay prevent or delay families from seeking care.In these cases, once a patient has presented,careful consideration should be given to thepotential risks and benefits of outpatient versusinpatient treatment. Whether a family can afforda prescribed medication, whether they willremember to administer the medication, andwhether one considers them reliable should thepatient’s condition worsen are just 3 of the manyfactors that must be taken into account. Whenthese questions are posed and uncertaintyremains, it may be the safest course to admit thesick child for observation, in the hope of avoidingprogression of the infection or loss of renal massrelated to medical noncompliance.
Teenage pregnancy is rapidly becoming a socialsituation in which treatment of UTI can be verychallenging. In these patients there can be signifi-cant risks due to UTI for both baby and mother.Although asymptomatic bacteriuria would nor-mally not be treated, in pregnant women itincreases the risk of symptomatic infection,preterm labor, and low birth weight.42 As such, inpregnant women all bacteriuria should be treated.Women who have previously displayed anincreased risk of infection or who have predispos-ing factors should be counseled regarding risks asthey relate to pregnancy.
Nosocomial Infection
A final situation that warrants brief discussion isnosocomial infections. Nosocomial UTI is an infec-tion acquired while in a hospital. A whole articlecould be written about the epidemiology,pathology, treatment, and implications of nosoco-mial UTI. These infections can be significantbecause they occur in a population that is alreadyill and often involve resistant bacteria. Financialchallenges also exist, as Medicare has eliminatedpayment for nosocomial UTI treatment and anyadditional care that occurs as a result of theseinfections.43 Basic principles underlie preventionof nosocomial UTI: appropriate hand washingand cleaning, appropriate care for indwelling tubes(including removal at the earliest medically appro-priate time), and antibiotics when deemednecessary.
SUMMARY
UTI in children is a frequent cause of worry forparents and physicians. While many infectionswill not be severe in nature, one should alwaysconsider potential complicating factors that mayexist in the pediatric population. When a UTIdoes not resolve routinely or when more compli-cated scenarios present, knowledge of thesecomplicating factors can allow accurate diag-nosis. Consideration should be given to the manyapproaches to treatment in developing a treatmentplan for each individual patient.
REFERENCES
1. Shortliffe LD. Infection and inflammation of the pedi-
atric genitourinary tract. In: Wein A, Kavoussi L,