Greg German MD PhD FRCPC DTM&H Medical Microbiologist & Infectious Diseases Consultant Urine Matters on February 10, 2015 CADTH Road Show on Lab Utilization Murchison Centre, Charlottetown PEI www.healthpei.ca/micro
Transcript
Greg German MD PhD FRCPC DTM&H Medical Microbiologist & Infectious Diseases
Consultant
Urine Matters on
February 10, 2015 CADTH Road Show on Lab Utilization Murchison Centre, Charlottetown PEI
www.healthpei.ca/micro
No Disclosures Objectives:
1. Superbugs and Seniors 2. Stewardship: Antibiotics Saving Islanders if Islanders Save Antibiotics 3. Better, Faster, Stronger UTI Data 4. Indwelling Urine Catheters too Dangerous Covered in Mary LeBlanc’s Talk 5. Chronic UTIs Good / Bad / Ugly 6. UTI Care Pathway for LTC Introduction.
Antibiotic Collateral Damage THE PERSON • Drug-drug
interactions • Allergies • Intolerances • Side effects • Need for monitoring • Selection of Other
bugs • ((IV Access))
OUR COMMUNITY • Expense to system • Antibiotic resistance • Creation of superbugs
The SUPERBUGS
Seniors (Age 65+)
• 17.3% of Island population (2013) • Projected to about 1 in 3 by 2040
^October 2011 new testing procedures increased sensitivity of ~20%
*
Cdiff Cases by Age
05
1015202530354045
<20 20-29 30-39 40-49 50-59 60-69 70-79 80-89 90+
20112014
*2014 Data: Lab Generated pending confirmation/validation by Provincial Epidemiologist
*
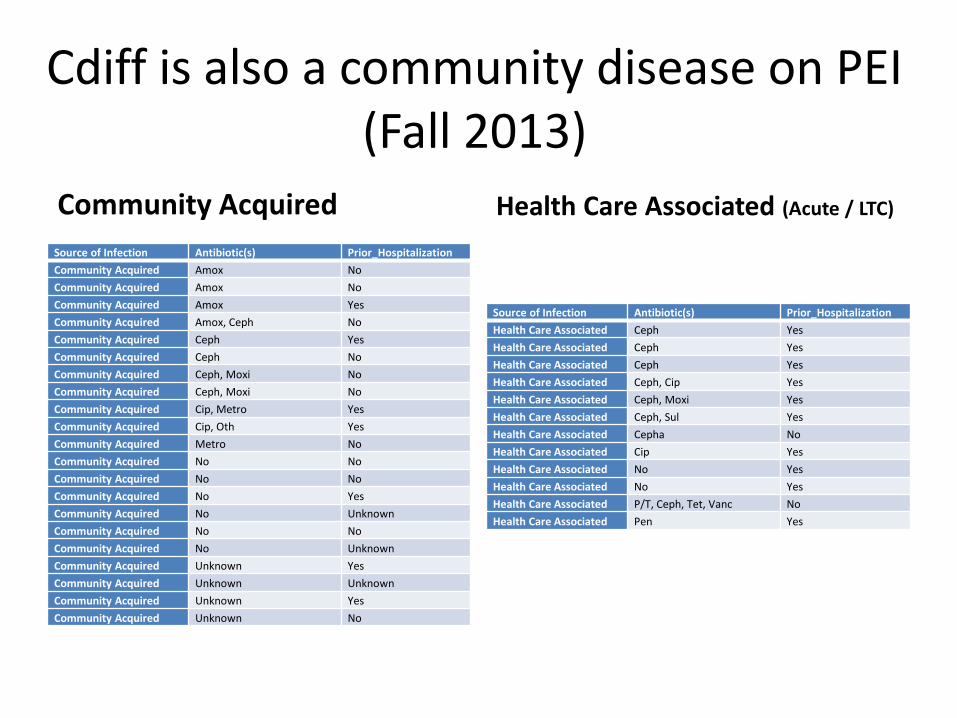
Cdiff is also a community disease on PEI (Fall 2013)
Community Acquired Source of Infection Antibiotic(s) Prior_Hospitalization Community Acquired Amox No Community Acquired Amox No Community Acquired Amox Yes Community Acquired Amox, Ceph No Community Acquired Ceph Yes Community Acquired Ceph No Community Acquired Ceph, Moxi No Community Acquired Ceph, Moxi No Community Acquired Cip, Metro Yes Community Acquired Cip, Oth Yes Community Acquired Metro No Community Acquired No No Community Acquired No No Community Acquired No Yes Community Acquired No Unknown Community Acquired No No Community Acquired No Unknown Community Acquired Unknown Yes Community Acquired Unknown Unknown Community Acquired Unknown Yes Community Acquired Unknown No
Health Care Associated (Acute / LTC)
Source of Infection Antibiotic(s) Prior_Hospitalization Health Care Associated Ceph Yes Health Care Associated Ceph Yes Health Care Associated Ceph Yes Health Care Associated Ceph, Cip Yes Health Care Associated Ceph, Moxi Yes Health Care Associated Ceph, Sul Yes Health Care Associated Cepha No Health Care Associated Cip Yes Health Care Associated No Yes Health Care Associated No Yes Health Care Associated P/T, Ceph, Tet, Vanc No Health Care Associated Pen Yes
MRSA
Staph aureus blood stream infections that are MRSA by Antibiogram year
2013: 7.4% 2014: 16%
Mortality (~20%), hospital costs, and relapse rate higher with MRSA
MRSA Blood cultures Cases
• Rare Event on PEI • 2014 N= 8 Average age 80.5 • 2011-2013 N= 11 Average Age 66.4
XDRO eXtensive Drug Resistant Enterobacteriacae
• Public Health Reportable since March 2013 • Used European Definitions:
– (resistant to all but 2 classes of common used antibiotics)
• For urines intermediate or resistant to 3 of 4 following groups of oral antibiotics – Cotrimoxazole – Nitrofurantoin – Amox/clav or cefixime – Ciprofloxacin
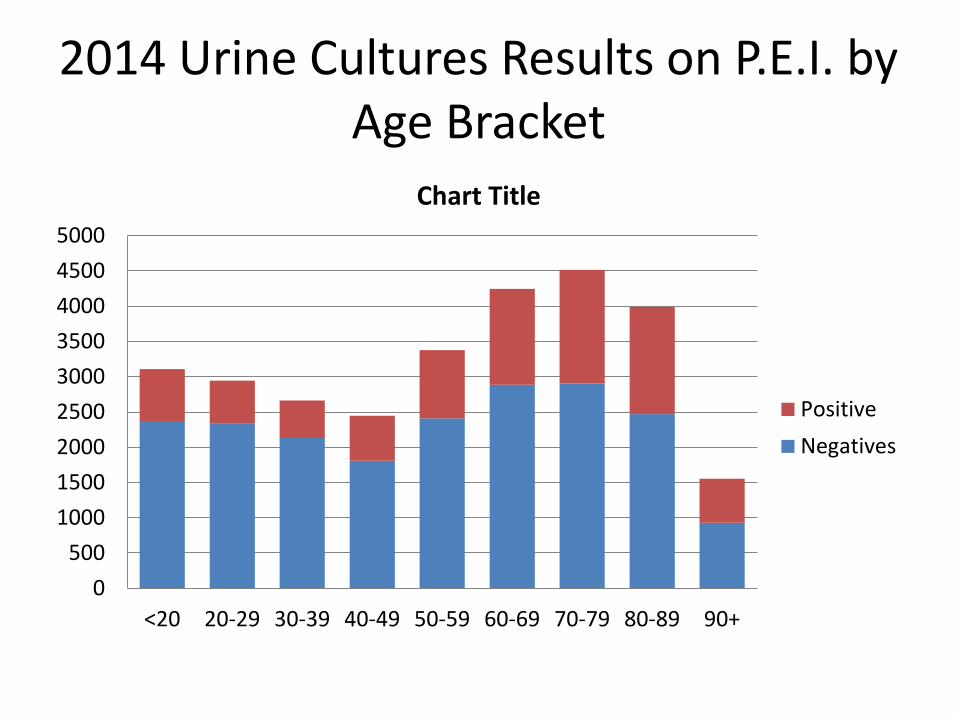
2014 Urine Cultures Results on P.E.I. by Age Bracket
0500
100015002000250030003500400045005000
<20 20-29 30-39 40-49 50-59 60-69 70-79 80-89 90+
Chart Title
PositiveNegatives
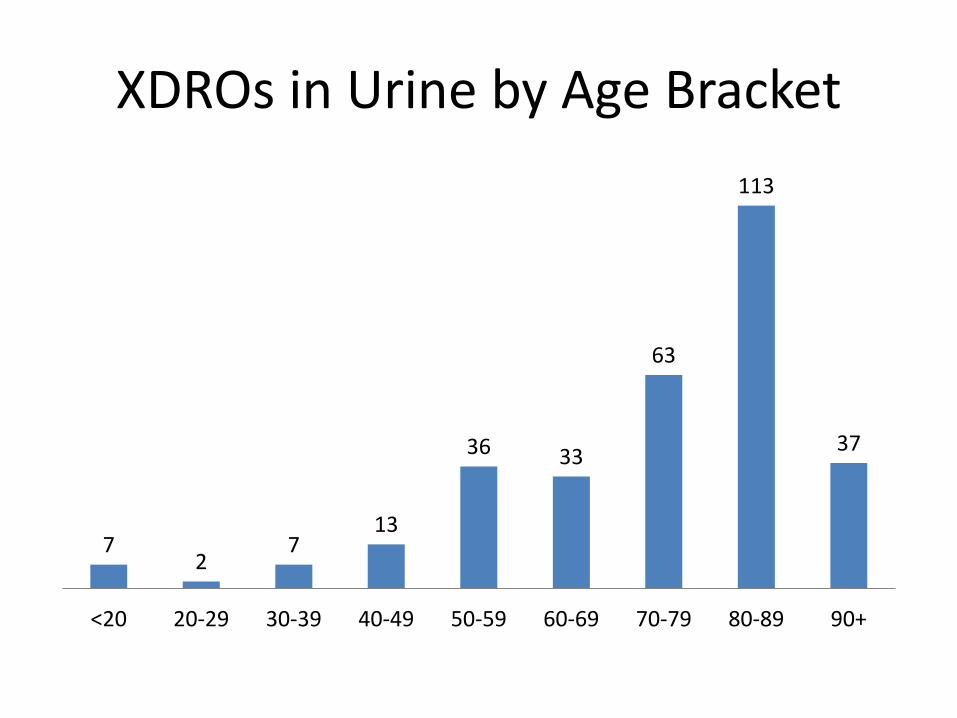
XDROs in Urine by Age Bracket
7 2
7 13
36 33
63
113
37
<20 20-29 30-39 40-49 50-59 60-69 70-79 80-89 90+
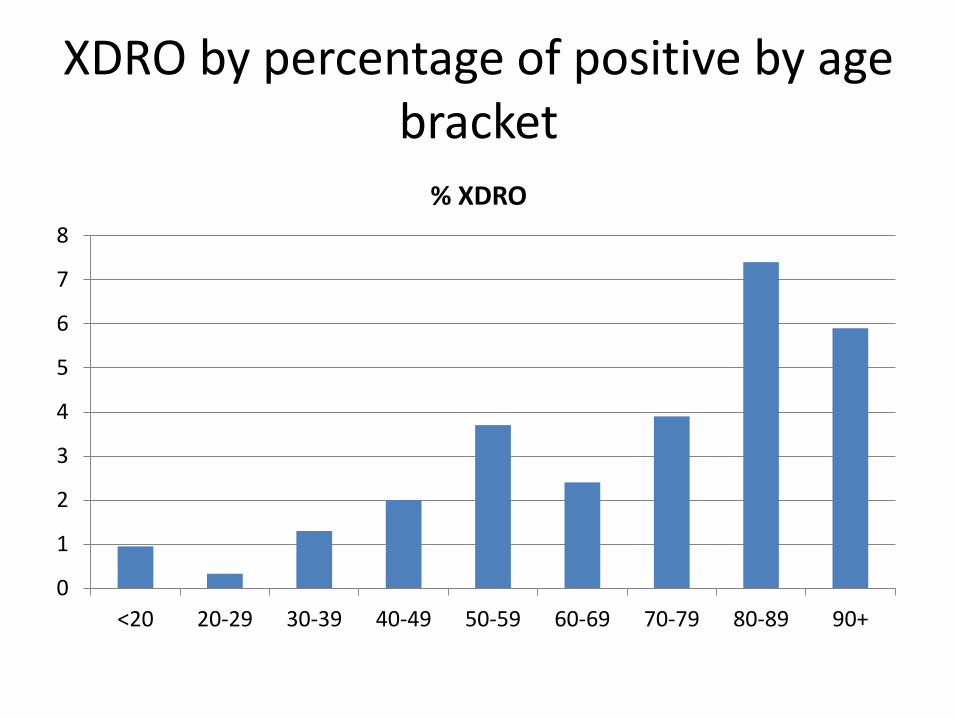
XDRO by percentage of positive by age bracket
0
1
2
3
4
5
6
7
8
<20 20-29 30-39 40-49 50-59 60-69 70-79 80-89 90+
% XDRO
XDRO Bottom Line
• Age 65+ – 1 of every 5 Islanders – 1 of every 2 urine cultures either pos/neg are taken
from this age group – Of the XDROs in the urine 4 of 5 are from patients 65+
• Long Term Care – 135 XDROS from long term care residents in 2014 – 3 of every 5 XDROs in 65+ are from aLTC resident
• NO Carbapenem-resistant Enterobacteriaceae (CRE) at this time
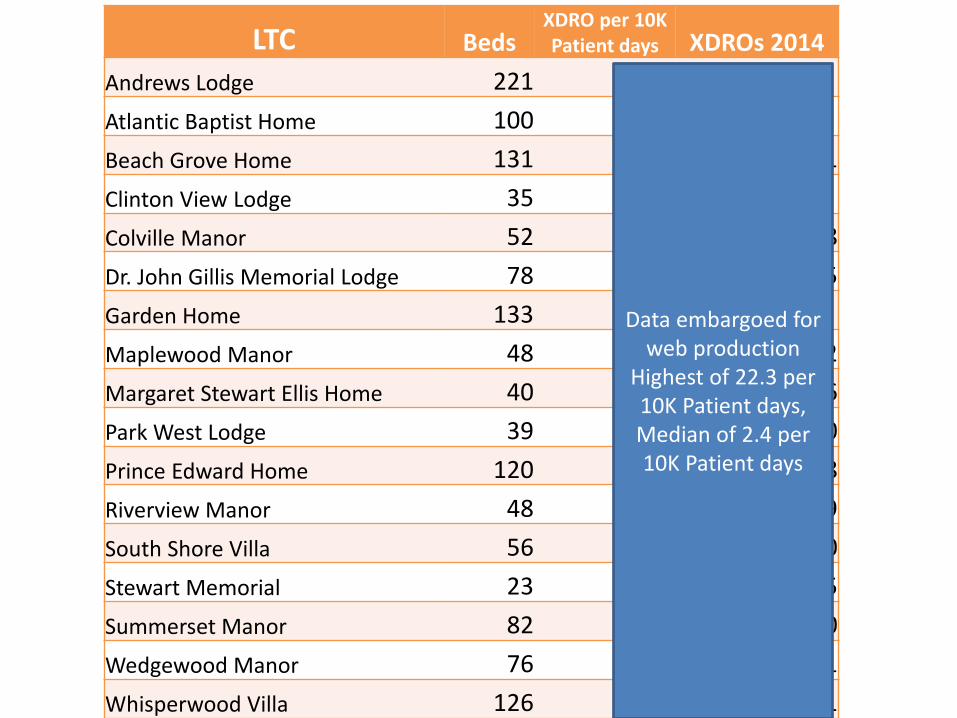
LTC Beds XDRO per 10K Patient days XDROs 2014
Andrews Lodge 221 0.0 Atlantic Baptist Home 100 0.0 Beach Grove Home 131 4.4 21 Clinton View Lodge 35 0.0 Colville Manor 52 4.2 8 Dr. John Gillis Memorial Lodge 78 1.8 5 Garden Home 133 0.0 Maplewood Manor 48 6.8 12 Margaret Stewart Ellis Home 40 4.1 6 Park West Lodge 39 0.0 0 Prince Edward Home 120 1.8 8 Riverview Manor 48 22.3 39 South Shore Villa 56 0.0 0 Stewart Memorial 23 6.0 5 Summerset Manor 82 0.0 0 Wedgewood Manor 76 4.0 11 Whisperwood Villa 126 2.4 11
Data embargoed for web production
Highest of 22.3 per 10K Patient days, Median of 2.4 per 10K Patient days
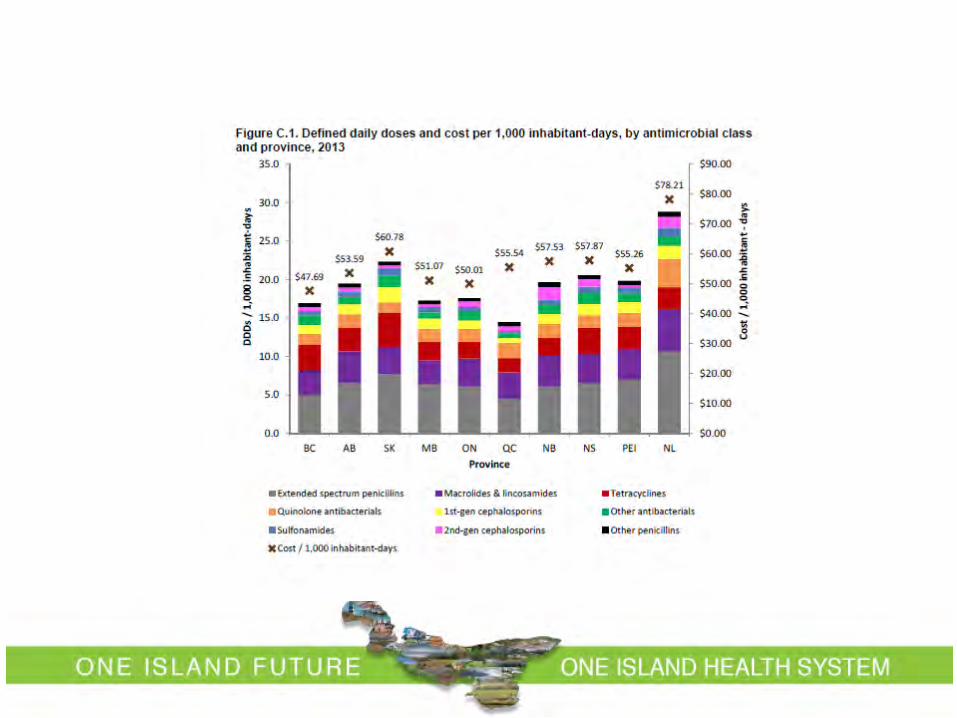
2014 Human Antimicrobial Drug Use Report 2012-2013
Stewardship: Antibiotics Saving Islanders if Islanders Save Antibiotics
What percentage of antibiotic prescriptions are outside of acute care
hospitals?
A. 85%
B. 66%
C. 50%
D. 33%
E. 15%
Stewardship Interventions Prospective audit with
intervention and feedback Education Guidelines and clinical
pathways Antimicrobial order
forms Antibiogram
Formulary restriction and preauthorization Streamlining or de-
escalation of therapy Parenteral to oral
conversions Dose optimization CPOE and decision
support
Modified from: Delit TH et al. Clin Infect Dis. 2007;44(2):159-77.
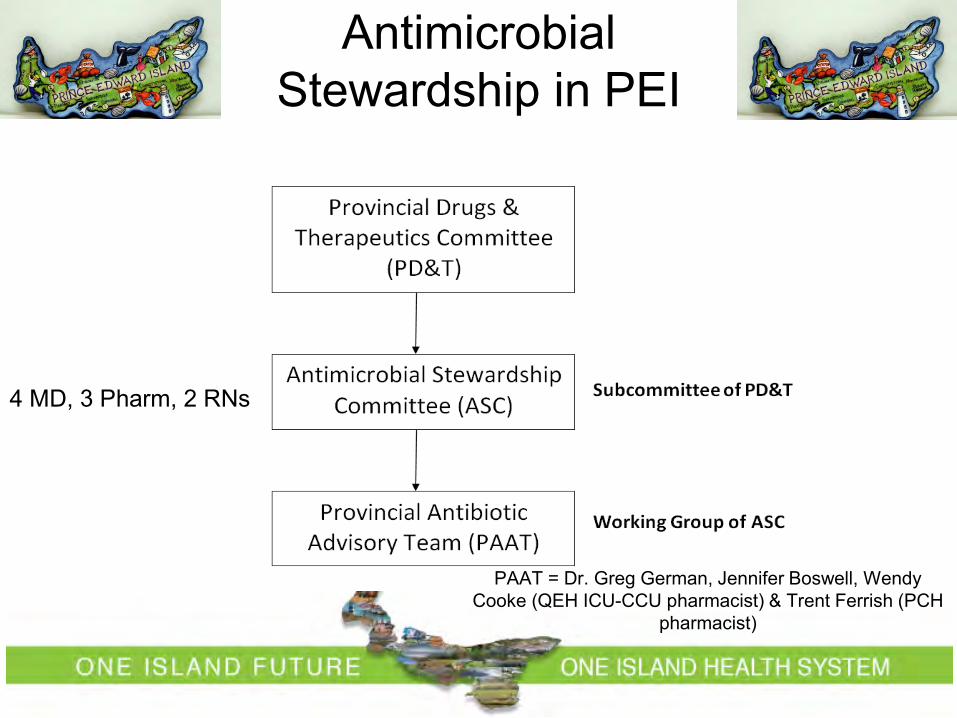
Antimicrobial Stewardship in PEI
PAAT = Dr. Greg German, Jennifer Boswell, Wendy Cooke (QEH ICU-CCU pharmacist) & Trent Ferrish (PCH
pharmacist)
4 MD, 3 Pharm, 2 RNs
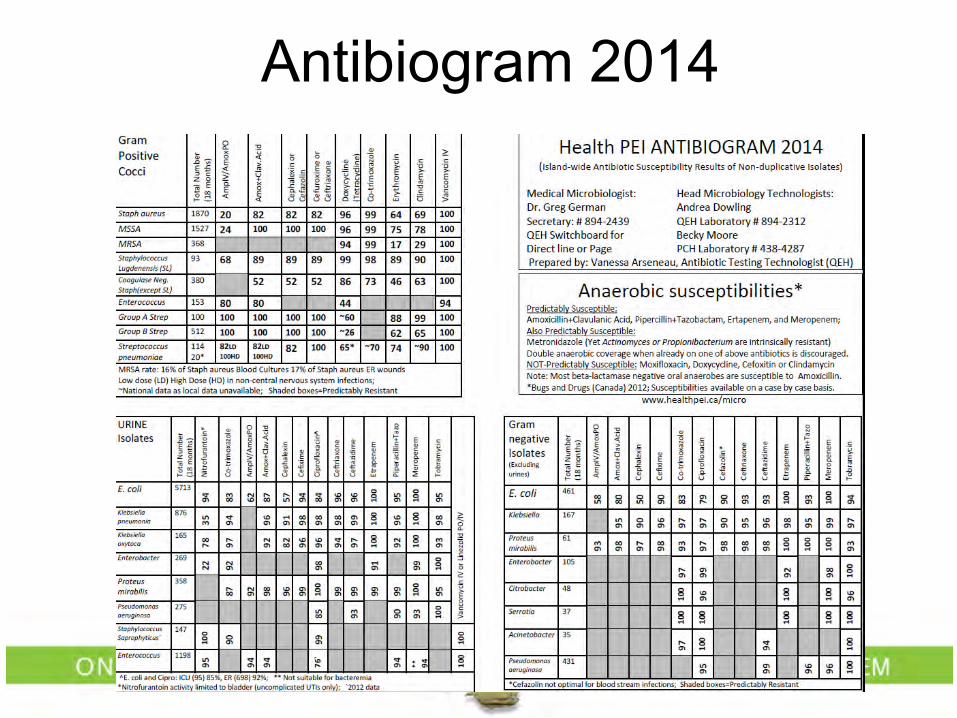
Antibiogram 2014
Local UTI Empiric Treatment Guidelines based on broad consultation
Guideline Development and Review Developed by PAAT (Provincial Antibiotic Advisory Team): Dr. Greg German, Jennifer Boswell, Wendy Cooke (QEH ICU/CCU Pharmacist), Trent Ferrish (PCH Pharmacist)
Individual guidelines reviewed by the following clinicians across the Island:
• Sepsis (9 Syndromes within) Dr. Lenley Adams Dr. Patrick Bergin Dr. Michael Irvine Dr. Paul Seviour Dr. Philip Champion (febrile
neutropenia) Dr. Barry Fleming (intra-abdominal)
• UTI (With and without a Catheter) Dr. Lenley Adams Dr. Scott Campbell Dr. Kate Ellis-Ghiz Dr. Gil Grimes Dr. Michael Irvine Dr. Ian Reid Dr. John Sampson
• Clostridium difficile Dr. Jeremy Beck Dr. Patrick Bergin Dr. Donald Clark Dr. Herb Dickieson Dr. Barry Fleming Dr. Connie Hoare
• Skin/Soft tissue & Diabetic Foot Dr. Katherine Burleigh Dr. Scott Cameron Dr. Ayodeji Harris-Eze Dr. Edmund Harrison Dr. Michael Irvine Kathy Mutch, Enterostomal Therapy Nurse Dr. Ronald Whalen Dr. Scott Wotherspoon
Change in Nitrofurantoin Prescriptions to Females Guidelines on PEI improve prescribing behaviour
• The number of nitrofurantoin prescriptions to females increased 30.7% pre/post-Guidelines, and the change is statistically significant (p < .001).
Before Guidelines Release After Guidelines Release
Mean
Num
ber o
f Nitr
ofur
anto
in P
resc
riptio
ns to
Fem
ale
200
250
300
350
400
450
500
95% Confidence Interval
Antibiotic Resistance develops
75
80
85
90
95
100
PEI2005 PEI2009 PEI2012 PEI2013
Cipro SXT
Percent susceptibility in Urine Isolates for E. coli
50556065707580859095
100
Total (5713) Catheter (205) ER (698) ICU (78)
Cipro SXT Nitro
PEI Antibiotic Susceptibility 2014 E. coli
Jan 2013 – Jun 2014 (18 months)
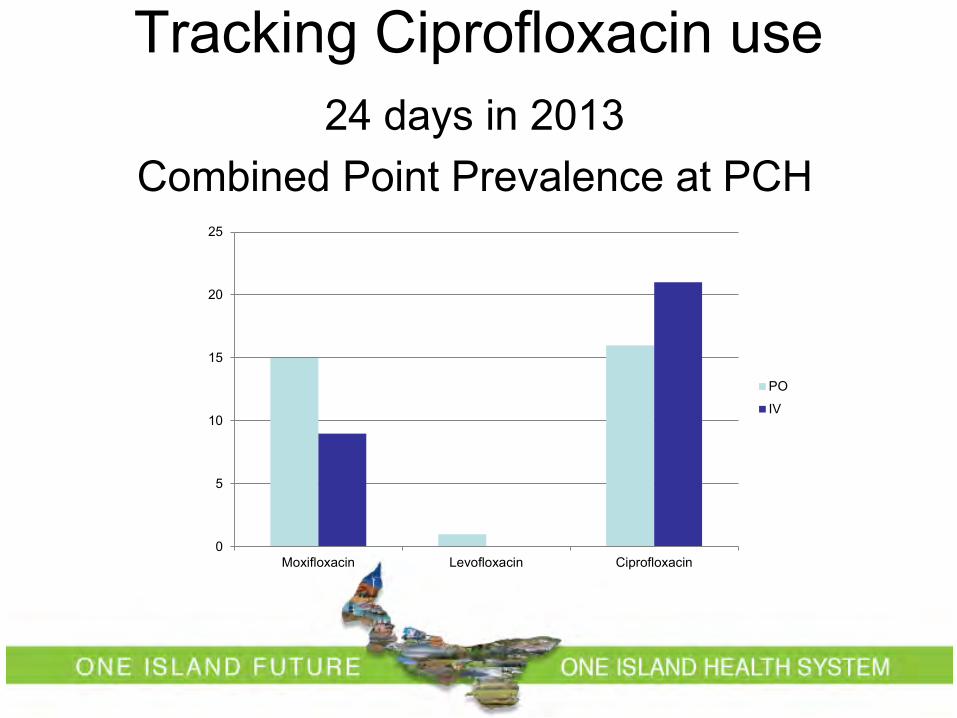
Tracking Ciprofloxacin use 24 days in 2013
Combined Point Prevalence at PCH
0
5
10
15
20
25
Moxifloxacin Levofloxacin Ciprofloxacin
PO
IV
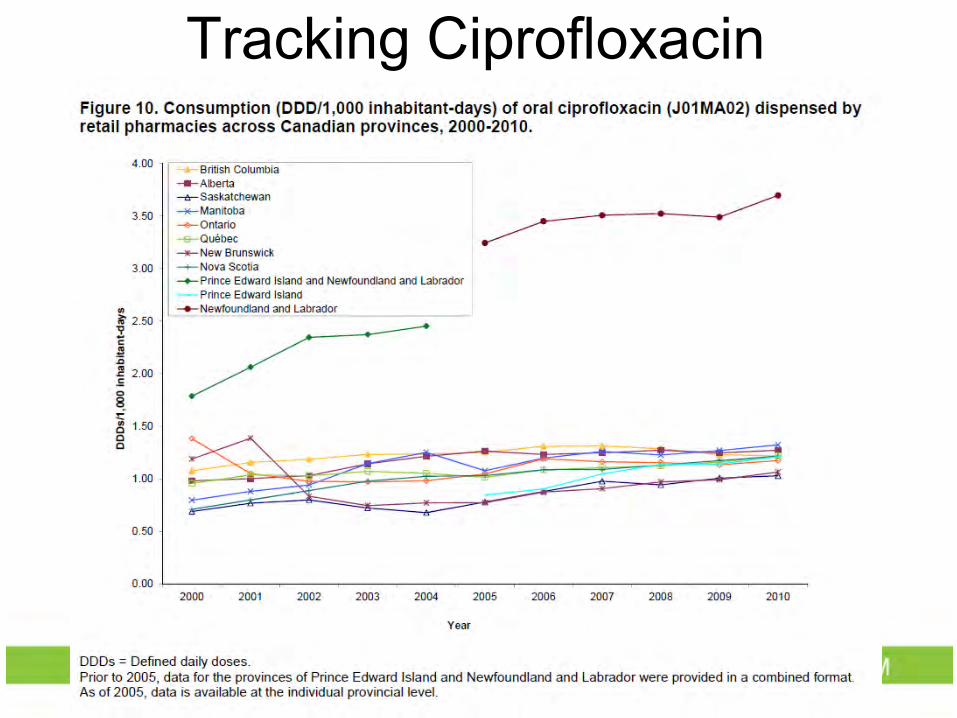
Tracking Ciprofloxacin
Stewardship and Long Term Care
• Not much in the literature • One study suggests use of UTI but not
respiratory guidelines beneficial.
Better faster stronger UTI data
What does GIGO stand for?
Better Faster Strong UTI Data
Sorting of plates into different categories
GOOD
Transporting Urine infections are quantitated and interpreted relative to other organisms. Delay in processing or refrigeration to halt growth leads to false positive (single contaminate grows) or false negative (contaminates overtake pathogen) 1. Outpatient business 2. Cold chain from outside hospital,
clinics or on the ward 3. Lack of Sunday run on the East side
Plan: Test driving a urine stabilizer capsule for specimens transported from the community
Worksheet
⃝Long Term Care
How we Report
• 1-10 x 106 cfu / L • 11-100 x 106 cfu/L (11-50) • 11-100 x 106 cfu/L (51-100) • >100 x 106 cfu/L
• +1 • +2 • +3 • +4
Improving Urine data: avoid GIGO • Prevent UTIs • Better Indications • Better collections • Better transport • Better testing including gram stain • Earlier reporting by fax • Extra susceptibilities testing, rapid screen
or for new oral agents (Fosfomycin)
Chronic UTI Strategies • Estrogen type creams Good evidence, well supported
• Cranberry Juice • Probiotics Oral vs Vaginal? Single Canadian RCT trial show promissing
results for vaginal suppository • Chronic daily / Prophylaxsis antibiotics No supported by infectious diseases
NEJM 1993 0.5mg of Estriol cream vaginally every night for 2-weeks and then 2x/week for 8 months
• (0.5 vs. 5.9 episodes per patient-year)
• N=93 total • 28% stopped
therapy due to minor irritation
NEJM 1974 • Abstract: Twenty-seven adult women and thirteen girls with recurrent urinary
infections were treated to eradicate their infection and then observed for recurrences while sequentially receiving three prophylactic drug regimens and a period with no drug therapy. The prophylactic regimens consisted of sulfamethoxazole, 500 mg daily, methenamine mandelate, 2 g daily, together with ascorbic acid 2 g daily, or trimethoprim, 40 mg, in combination with sulfamethoxazole, 200 mg daily. Children received half the adult doses. Thirty-three infections (3.6 per patient-year) occurred in patients on no drug therapy, 22 (2.5 per patient-year) in those taking sulfamethoxazole, 13 (1.6 per patient-year) in those taking methenamine mandelate and ascorbic acid, and 1 (0.1 per patient-year) in those taking trimethoprim–sulfamethoxazole. Trimethoprim–sulfamethoxazole was also the most effective in preventing colonization of the periurethral area with enterobacteriaceae. These results suggest that a daily low dose of trimethoprim–sulfamethoxazole is effective in preventing reinfections of the urinary tract in females. (N Engl J Med 291:597–601, 1974)
IDSA guidelines
Estrogen Therapy Continued
Cranberry Juice • Vancouver 2002 Can. J. of Urology • ABSTRACT To determine, from a societal perspective, the effectiveness and cost effectiveness
of concentrated cranberry tablets, versus cranberry juice, versus placebo used as prophylaxis against lower urinary tract infection (UTI) in adult women. One hundred fifty sexually active women aged 21 through 72 years were randomized for one year to one of three groups of prophylaxis: placebo juice + placebo tablets versus placebo juice + cranberry tablets, versus cranberry juice + placebo tablets. Tablets were taken twice daily, juice 250 ml three times daily. Outcome measures were: (1) a >50% decrease in symptomatic UTI's per year (symptoms + >or= 100 000 single organisms/ml) and (2) a >50% decrease in annual antibiotic consumption. Cost effectiveness was calculated as dollar cost per urinary tract infection prevented. Stochastic tree decision analytic modeling was used to identify specific clinical scenarios for cost savings. Both cranberry juice and cranberry tablets statistically significantly decreased the number of patients experiencing at least 1 symptomatic UTI/year (to 20% and 18% respectively) compared with placebo (to 32%) (p<0.05). The mean annual cost of prophylaxis was $624 and $1400 for cranberry tablets and juice respectively. Cost savings were greatest when patients experienced >2 symptomatic UTI's per year (assuming 3 days antibiotic coverage) and had >2 days of missed work or required protective undergarments for urgency incontinence. Total antibiotic consumption was less annually in both treatment groups compared with placebo. Cost effectiveness ratios demonstrated cranberry tablets were twice as cost effective as organic juice for prevention. Cranberry tablets provided the most cost-effective prevention for UTI.
Process • 1st Draft Mary LeBlanc, Pam Handrahan, Kelly
Blanchard, with Shelley Woods Based off of UTI pathways from alberta and saskatawan Added RN initiated tests and antibiotics (if medical directive)
• 2nd Draft Greg German and Jennifer Boswell Seperated into with or without a foley, seperated by severity Created almost no side bars / notices Allowed for urine dipstick to triage starting antibiotics Reliance on blood work in several instances
• 3rd Draft, feedback from Dr. Huy Nguyen Removed other classifications of fever Removed blood work, except if temp ≥ 38.5 Add coumadin to work sheet. Made it flow better
• 4th draft feedback from Dr. Grimes, Dr. MacLeod, Dr. Maginnis, and Mary LeBlanc Removed dipstick in almost all instances Limited initiation of antibiotics by nurse to
only one antibiotic (Nitrofurantoin) in only rare circumstance. Added blood work for repeat Cr if none in 3m
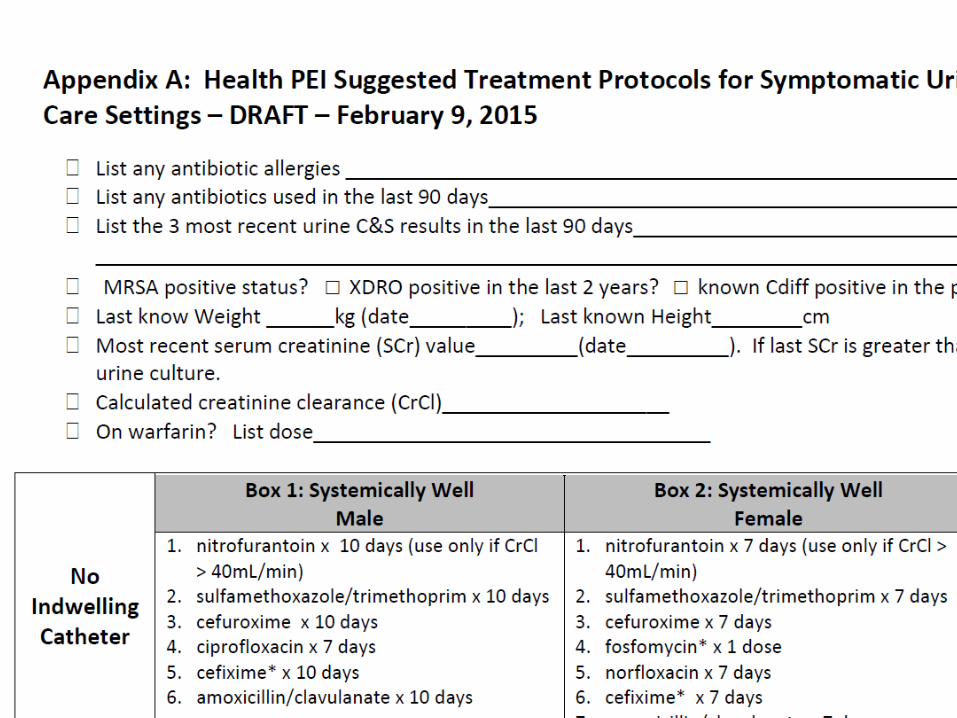
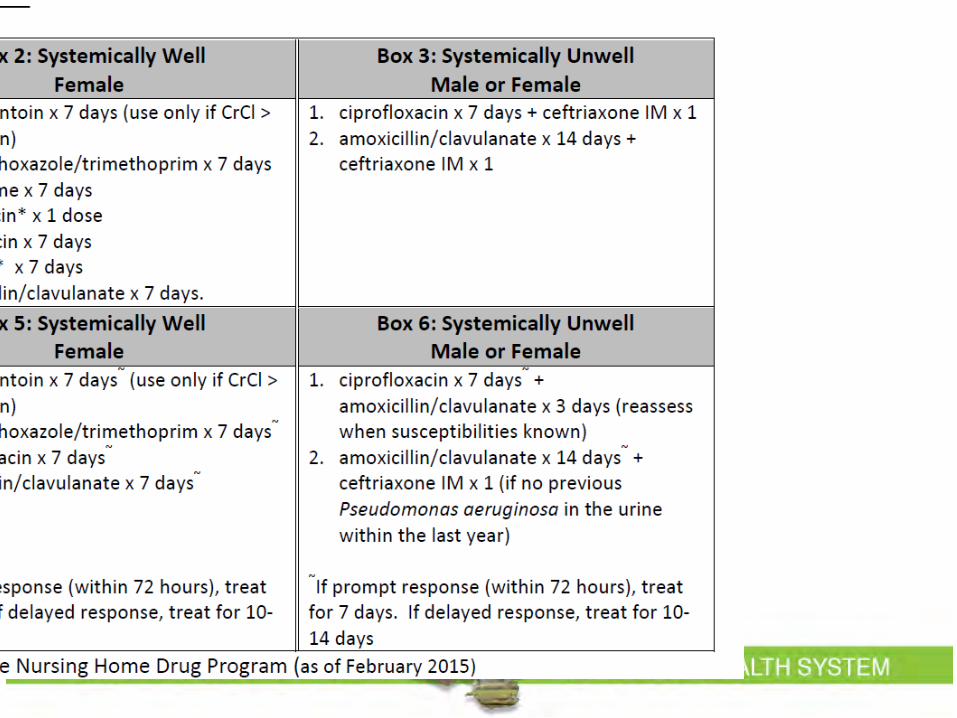
• Worksheet / Appendix A: A data gathering tool to assist in antibiotics Dosing of antibiotics in Seniors by catheter,
severity, and gender. Then by renal function.
Divided by
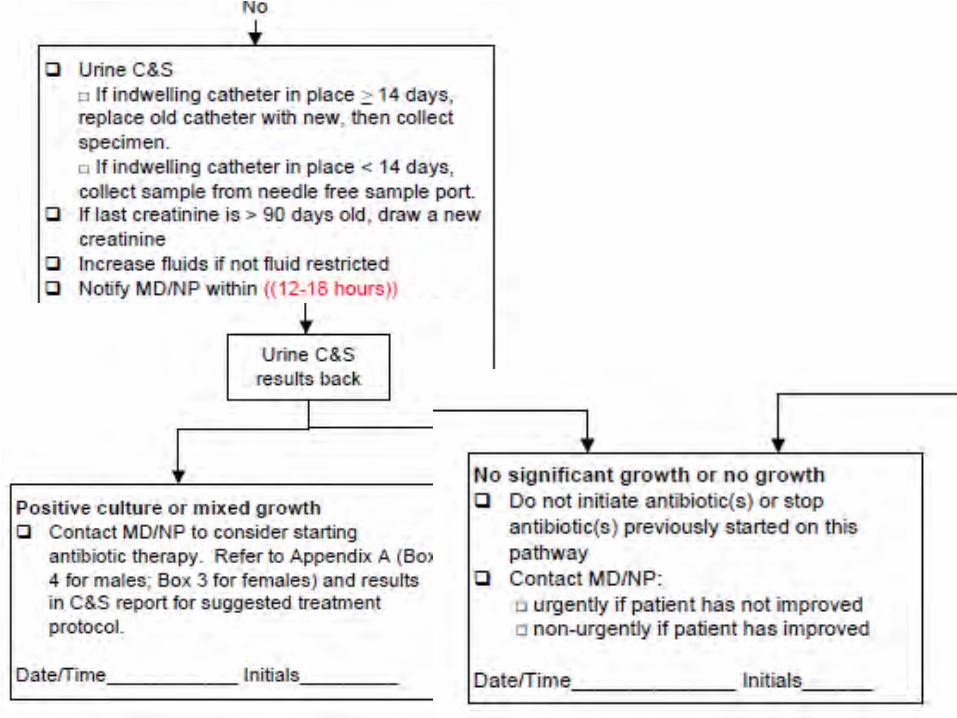
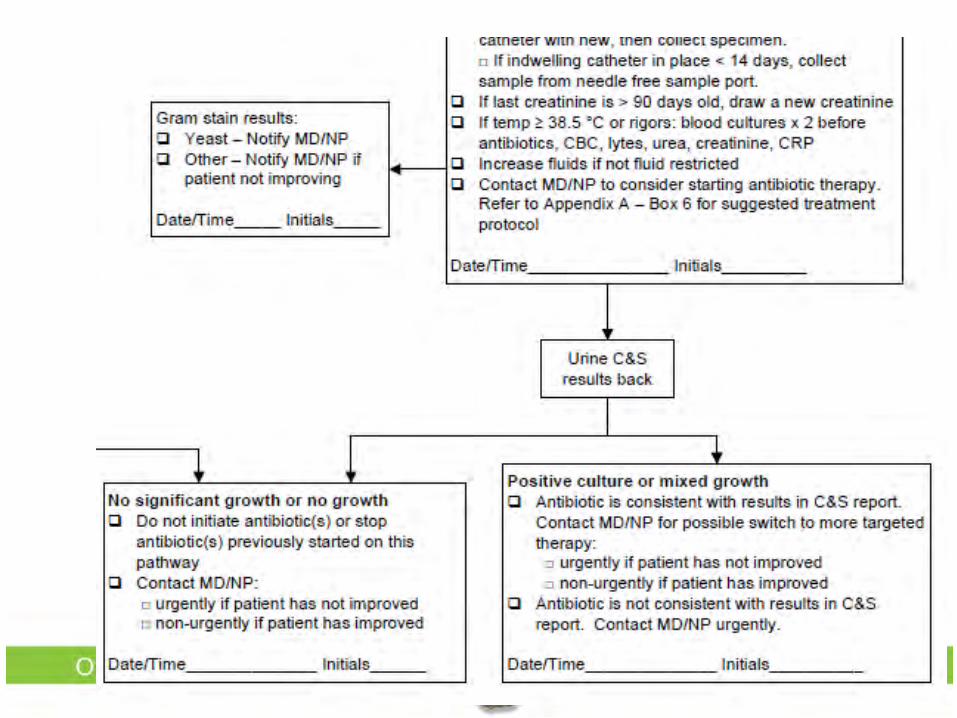
With or without an indwelling catheter
Systemically well or systemically unwell
Indwelling Catheter
Nurse Initiated antibiotics by medical directive
• Thames Valley Family Health Team (London Ontario), 2011 Limited to usually young females as greater
than 2 medication or one blood thinner is a contraindication
• Hamilton Family Health Team, 2014 Nurse able to give treatment course and
modify once susceptibilities are known
Hamilton Family Health Team Nurse initiated antibiotics along list of contraindications
Nitrofurantoin and Benefits
• Less collateral damage: Doesn’t target gut less resistance Doesn’t target gut less C. difficle
• Costs Inexpensive cost effective Opportunity to safe fluroquinolone or
TMP/SMX for future use decrease need for IV antibiotics
Nitrofurantoin and Side effects • Long term use
pulmonary fibrosis • Long term use
peripheral neuropathy • Renal damage
increased toxicity • G6PD Hemolytic
Anemia • Lack of prostate
penetration clinical failure
• Lack of Vaginal penetration in elderly Relapse/Reinfections?
Optimal duration of antibiotic therapy for uncomplicated urinary tract infection in older
women: a double-blind randomized controlled trial
• CMAJ 2004, Laval • 183 women >Age 65 • Bacterial eradication
98% in 3 day group 93% in 7 day group
Use of Nitrofurantoin in Men
• Supported in the UK when pyleonephritis not suspected
• Appreciate may fail therapy due to lack of prostate penetration 20% of all UTI, 50% of recurrent or
associated with catheter have prostate invovlement
Objectives: 1. Superbugs and Seniors 2. Stewardship: Antibiotics Saving Islanders if Islanders Save Antibiotics 3. Better, Faster, Stronger UTI Data 4. Indwelling Urine Catheters too Dangerous Addressed in Mary LeBlanc’s talk. consider order sets in acute care to remove urine caths early
5. Chronic UTIs Good / Bad / Ugly 6. UTI Care Pathway for LTC Introduction.
Acknowledgements
• Jennifer Boswell • Microbiology Laboratory • Shelley Woods, Brenda Worth and Mary
LeBlanc • The House physicians • Lisa Pyke and CADTH • You