US Army Research Institute of Environmental Medicine Medicine and Work Performance at High Altitude Stephen R. Muza, Ph.D. U.S. Army Research Institute of Environmental Medicine Natick, MA, USA 01760 pinions or assertions contained herein are the private views of the author(s) and are not to be const as official or as reflecting the views of the Army or the Department of Defense.
Transcript
US Army Research Institute of Environmental Medicine
Medicine and Work Performance atHigh Altitude
Stephen R. Muza, Ph.D.U.S. Army Research Institute of Environmental Medicine
Natick, MA, USA 01760
The opinions or assertions contained herein are the private views of the author(s) and are not to be construedas official or as reflecting the views of the Army or the Department of Defense.
US Army Research Institute of Environmental Medicine
Overview
1. Biophysics of the Altitude Environment
2. Altitude Acclimatization:
Key Physiological Adaptations
Time-Course
3. High Altitude Stress:
Medical Problems - Altitude Illness
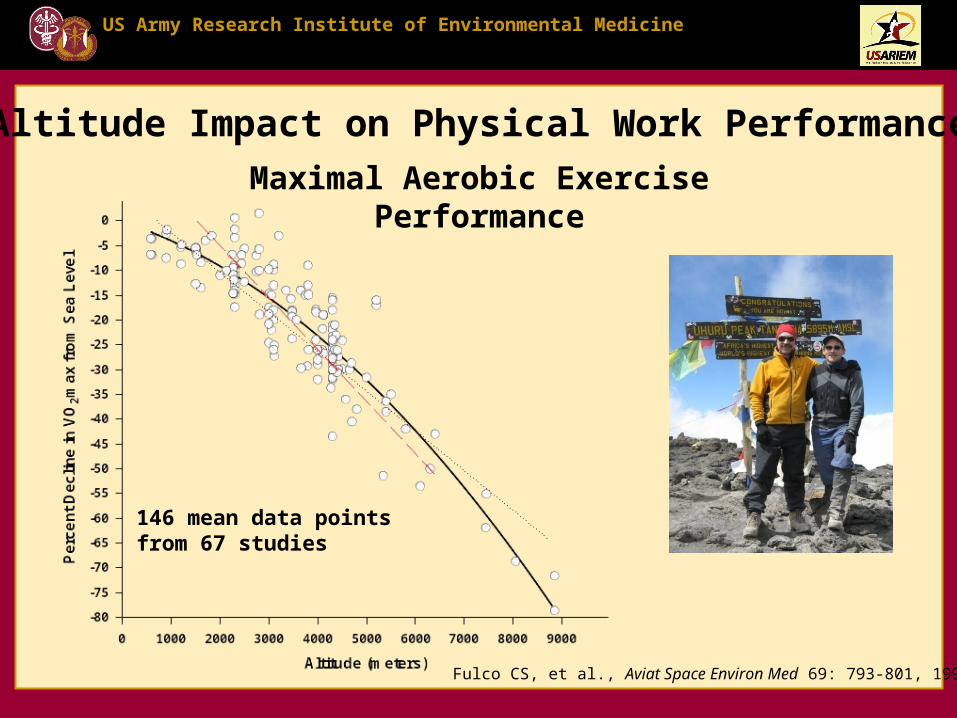
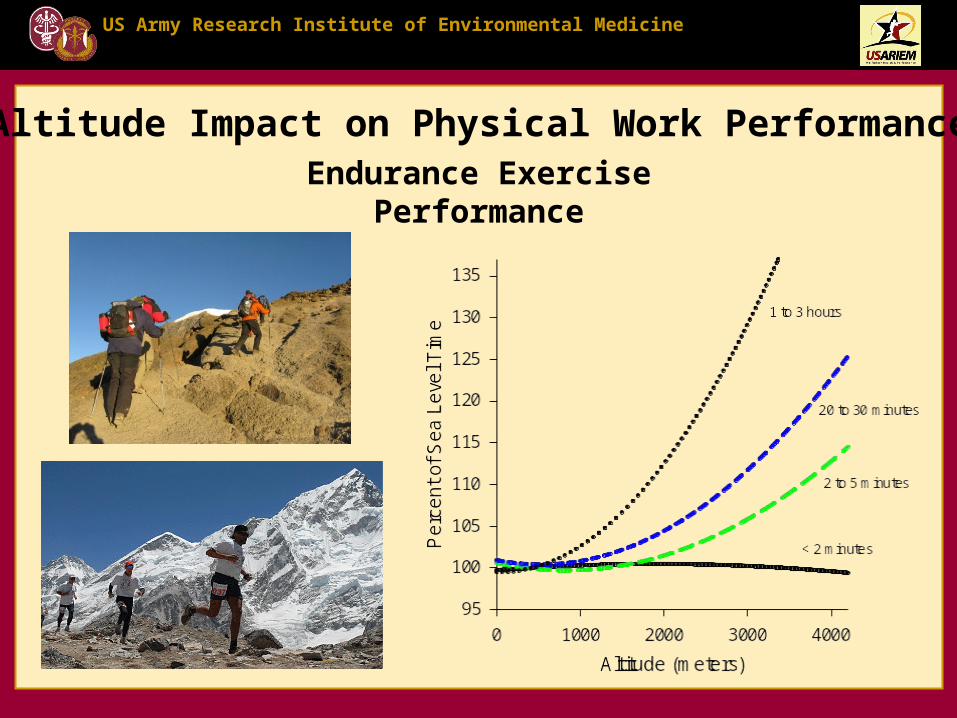
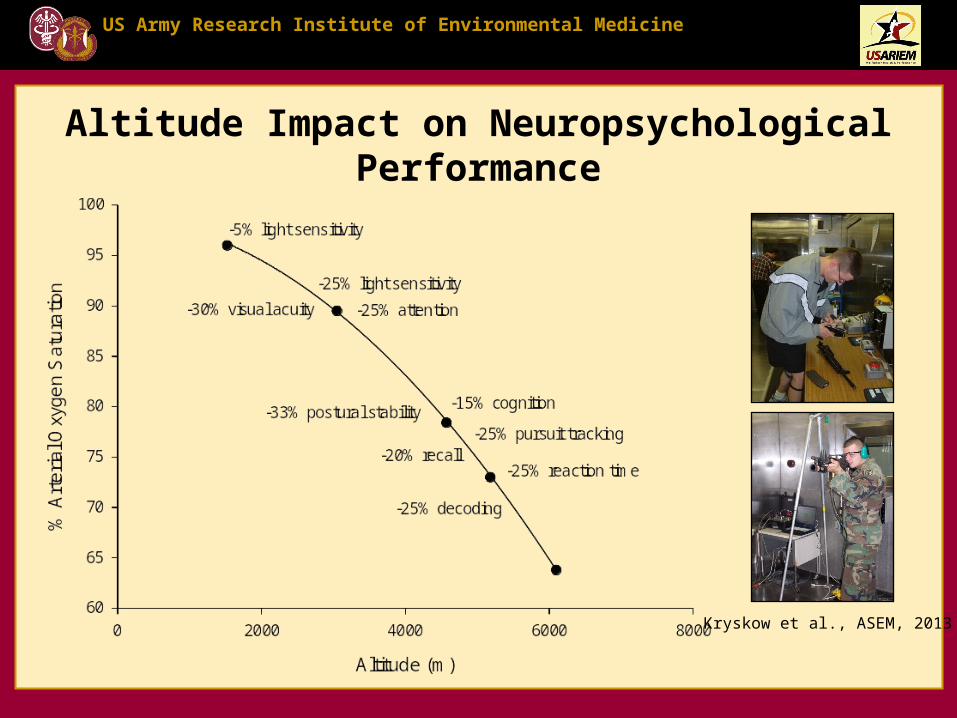
Performance – Physical & Neuropsychological
US Army Research Institute of Environmental Medicine
Easy Access to High Altitude Createsa Health and Performance Problem
Colorado Collegiate Range
ELAPSED TIME (hr)
0 20 40 60 80 100 120
AL
TIT
UD
E (ft)
0
1000
2000
3000
4000
5000
RDU
DEN
Camp 1
Camp 2 Camp 3 Camp 4
US Army Research Institute of Environmental Medicine
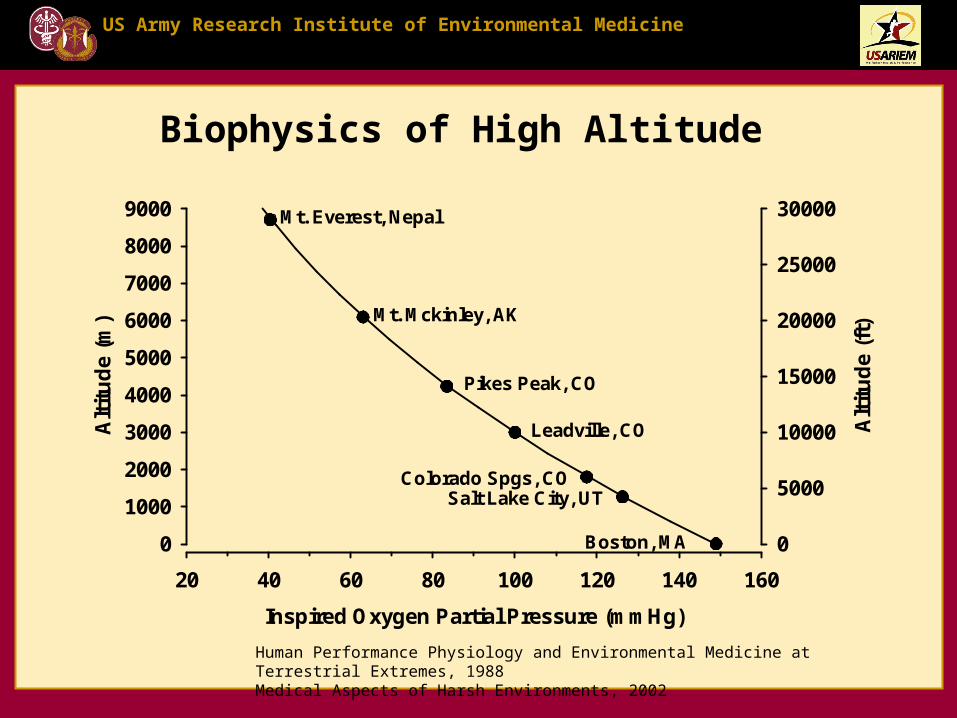
Biophysics of High Altitude
Inspired Oxygen Partial Pressure (mmHg)
20 40 60 80 100 120 140 160
Alt
itu
de
(m)
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
Alt
itu
de
(ft)
0
5000
10000
15000
20000
25000
30000
Colorado Spgs, CO
Leadville, CO
Pikes Peak, CO
Mt. Mckinley, AK
Mt. Everest, Nepal
Boston, MA
Salt Lake City, UT
Human Performance Physiology and Environmental Medicine at Terrestrial Extremes, 1988Medical Aspects of Harsh Environments, 2002
US Army Research Institute of Environmental Medicine
PaO2 (mmHg)
0 20 40 60 80 100 120 140
Oxy
gen
Sat
ura
tio
n (
%)
0
20
40
60
80
100
Sea Level
1850 m (Colorado Spgs, CO)
4300 m (Pikes Peak, CO)
Biophysics of High Altitude
SL: CaO2 = 19.6 ml O2%1850 m: CaO2 = 19.2 ml O2%4300 m: CaO2 = 16.5 ml O2%
US Army Research Institute of Environmental Medicine
High Altitude Stress:Impact on Low Altitude Residents
• Decreased Physical Performance (>1,200 m)• Risk of Altitude Sickness (>2,400 m)• Decreased Neuropsychological Performances (>2,400 m)
Medical Aspects of Harsh Environments , 2002
US Army Research Institute of Environmental Medicine
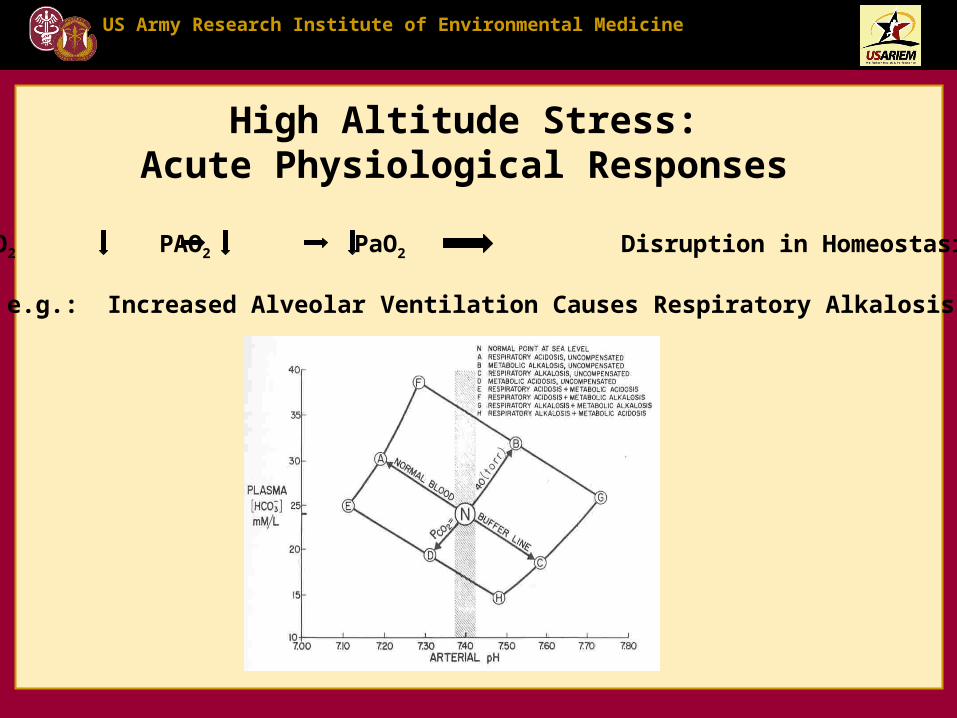
High Altitude Stress:Acute Physiological Responses
US Army Research Institute of Environmental Medicine
High Altitude Stress:Summary of Acute Physiological State
• Systemic hypoxia• Respiratory alkalosis (disrupted acid-base balance)• Orthostatic intolerant (light-headed, syncope)• Pulmonary arterial hypertension (impaired gas exchange)• Altered body fluid regulation: vascular space is leaking, some
tissues develop edema• ???
PIO2 PAO2 PaO2 Disruption in Homeostasis
US Army Research Institute of Environmental Medicine
Altitude AcclimatizationA series of physiological adjustments that
compensate for the reduction in ambient oxygen, and restores homeostasis
Table 2–4Summary of major physiological adaptations characteristic of altitude acclimatizationTable 2–4Summary of major physiological adaptations characteristic of altitude acclimatization
• Restored Mental Performance: 1-2 Days
• Decreased Susceptibility to Altitude Illness: 2-5 Days • Improved Sleep Quality: 5-7 Days
• Improved Physical Work Performance: 5-14 Days
• Overall, improved Resilience
Benefits of Acclimatization:
US Army Research Institute of Environmental Medicine
Altitude Acclimatization
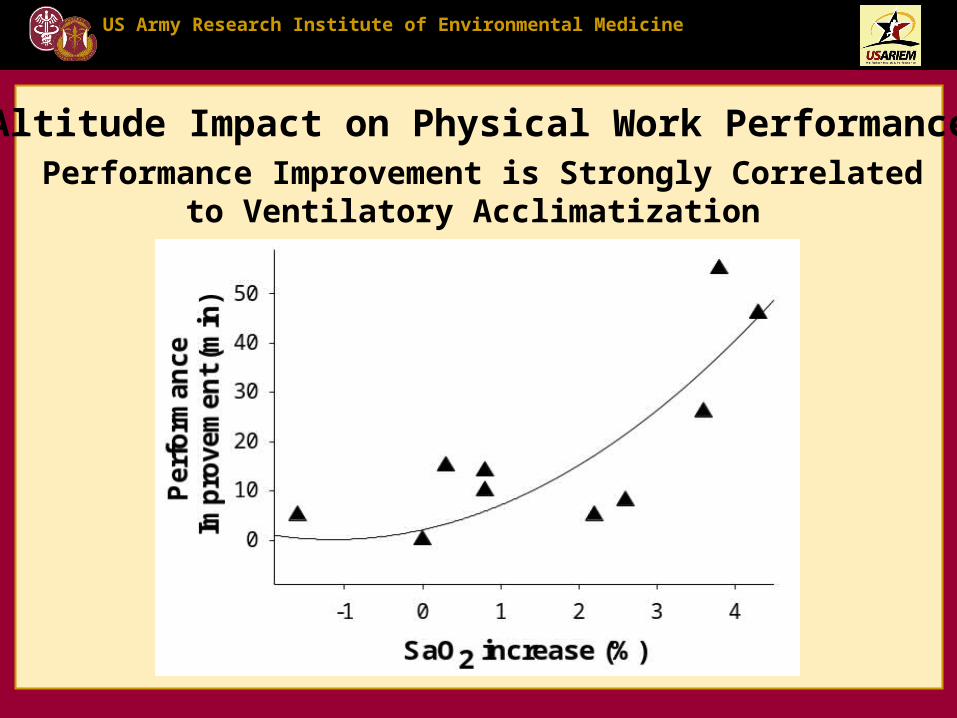
Increase Oxygen Delivery Increase Oxygen UtilizationIncreased Ventilation: Raises partial pressure of arterial O2 (PO2) and arterial oxyhemoglobin saturation (SaO2)
Increased Tissue Extraction of O2 from Capillary Blood
Increased 2,3-diphosphoglycerate and Renal Bicarbonate Excretion: Promotes O2 unloading from hemoglobin
Hypoxia-Inducible Factor (HIF)-Mediated Increased Oxidative Enzyme Function
Increased Sympathetic Activity: Sustains blood flow and blood pressure
Erythropoietin Mediated Increase in Red Blood Cell Mass: Raises arterial O2 content
Table 2–4Summary of major physiological adaptations characteristic of altitude acclimatizationTable 2–4Summary of major physiological adaptations characteristic of altitude acclimatization
Summary of major physiological adaptations characteristic of altitude acclimatization
US Army Research Institute of Environmental Medicine
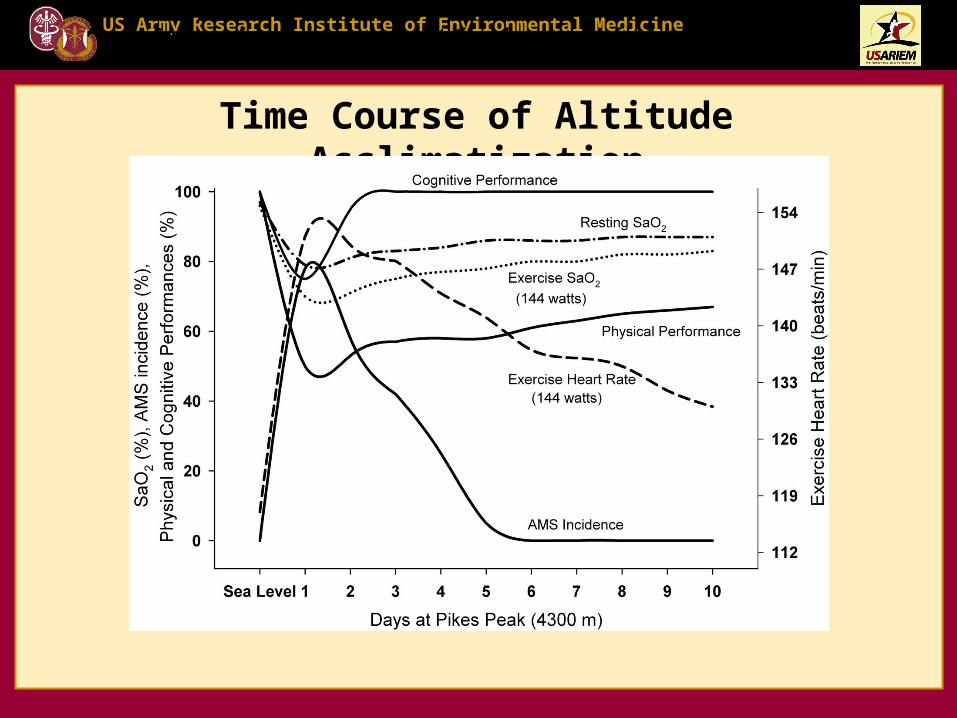
Time Course of Altitude Acclimatization
Table 2–4Summary of major physiological adaptations characteristic of altitude acclimatizationTable 2–4Summary of major physiological adaptations characteristic of altitude acclimatization
US Army Research Institute of Environmental Medicine
Altitude Acclimatization
Increase Oxygen Delivery Increase Oxygen UtilizationIncreased Ventilation: Raises partial pressure of arterial O2 (PO2) and arterial oxyhemoglobin saturation (SaO2)
Increased Tissue Extraction of O2 from Capillary Blood
Increased 2,3-diphosphoglycerate and Renal Bicarbonate Excretion: Promotes O2 unloading from hemoglobin
Hypoxia-Inducible Factor (HIF)-Mediated Increased Oxidative Enzyme Function
Increased Sympathetic Activity: Sustains blood flow and blood pressure
Erythropoietin Mediated Increase in Red Blood Cell Mass: Raises arterial O2 content
Table 2–4Summary of major physiological adaptations characteristic of altitude acclimatizationTable 2–4Summary of major physiological adaptations characteristic of altitude acclimatization
Summary of major physiological adaptations characteristic of altitude acclimatization
US Army Research Institute of Environmental Medicine
Altitude AcclimatizationVentilatory Acclimatization: Increased Hypoxic Ventilatory Response (HVR) Decreased PaCO2 set point Near normalization of pHa Compensated Respiratory Alkalosis Elevated PaO2, SaO2, and CaO2
Altitude Exposure (days)
SL 1 2 3 4 5 7 10
PE
TC
O2
(To
rr)
26
28
30
32
34
36
38
40
42
4422 Women37 Men
4,300 m Altitude Exposure (days)
SL 1 2 3 4 5 7 10 12 19
Res
tin
g S
aO2
(%)
75
80
85
90
95
100
22 Women (Muza et al. 2001)37 Men (Reeves et al. 1993)
US Army Research Institute of Environmental Medicine
Altitude AcclimatizationHematological Acclimatization: Early Response:
High Altitude Cerebral Edema (HACE) – “rare below the death zone” Incidence: ~1% Symptom Complex: Severe Headache, Impaired Mental Status,
Truncal Ataxia, Coma
High Altitude Pulmonary Edema (HAPE) – “leading cause of death” Incidence: 5-15% Symptom Complex: Dyspnea, Severe Fatigue,
Non-productive Cough, becoming productive,Pink & Frothy, Coma
Roach , R.C. et al., Medical Aspects of Harsh Environments , 2002
US Army Research Institute of Environmental Medicine
Beidleman, B.A.. et al., Med. Sci. Sports Exerc.:45, 2013
Acute Mountain Sickness (AMS)
Prediction of AMS:•Time and altitude are key factors•AMS increases 145% every 1000 m•AMS severity peaks 18-24 h•Physical activity increases AMS•Physical activity delays recovery from AMS•Women have lower AMS severity
US Army Research Institute of Environmental Medicine
AMS Criterion
Days at 4,300 m Altitude
SL 1 2 3 4 5 6 7 8 9 10 11 12
AM
S-C
Sev
erit
y S
core
0.0
0.5
1.0
1.5
2.032 men and women lowlandersAMS incidence >80%
Acute Mountain Sickness (AMS)Time Course
US Army Research Institute of Environmental Medicine
Acute Mountain Sickness (AMS)Pathophysiology
Prevailing theory: hypoxia-induced mild edema of both cytotoxic (intracellular) and vasogenic (extracellular) origin
Problem: everyone affected, no correlation with AMS symptoms, no evidence of BBB failure
Recent controversial theory: hypoxia-induced cerebral oxidative-nitrative stress releases noxious biomolecules that activate trigeminovascular nocioceptors to cause headache and AMS (Bailey, D.M. et al, 2009)
US Army Research Institute of Environmental Medicine
High Altitude Cerebral Edema (HACE)Pathophysiology
Prevailing theory: continuum of AMS progressing to vasogenic edema
33 yr male, SL to 5200 m in 6 days,MRI day 2 and 11 months later
MRI of acute and recovered phases of HACE. 7 of 9 patients with HACE showed intense T2 signal in white matter areas, especially the splenium of the corpus callosum.(Hackett, P. et al., JAMA 1998)
US Army Research Institute of Environmental Medicine
Altitude Hypoxia
PaO2
Uneven HPVR
Pulmonary Htn
Pulmonary Pcap
Capillary Stress Failure
Pulmonary Capillary Leak
High Altitude Pulmonary Edema
SNS
Pulmonary Venoconstriction
Vascular PermeabilityAgents?
(exercise, cold)(Endothelin-1, NO)
(HVR, A-a O2, exercise, sleep)
( Alveolar Fluid Absorption)
High Altitude Pulmonary Edema (HAPE)Pathophysiology
HAPE Status
R S (well) S (sick)
PA
Sys
tolic
(m
m H
g)
0
20
40
60
80
100
120
Swenson, E. et.al. JAMA 2002
US Army Research Institute of Environmental Medicine


















































![Presents MUZA CONCERTO —7fi—Jb 2017-2018 tab 1 … · Presents MUZA CONCERTO —7fi—Jb 2017-2018 tab 1 -f)Þy7: (Misirlou) 6/60 2,00011J 1,500PJ] KAWASAKI SYMPHONY HALL](https://static.documents.pub/doc/80x56/5b35fbed7f8b9abc218de5d7/presents-muza-concerto-7fijb-2017-2018-tab-1-presents-muza-concerto-7fijb.jpg)


