56 Journal of Pain and Symptom Management Vol. 18 No. 1 July 1999
Clinical Note
Use of a Metallic Stent for Relief of Symptoms Caused by Superior Vena Caval Obstruction in a Patient with Advanced Cancer: A Case Report
Noel Young, MB BS, FRACR and Paul Glare, MB BS, MA, FRACP
Departments of Radiology (N.Y.) and Medical Oncology and Palliative Care (P.G.), Westmead Hospital, Westmead, New South Wales, Australia
Abstract
This report describes the insertion of a metallic stent in the superior vena cava to relieve the symptoms of malignant superior vena caval obstruction in a 75-year-old woman withfar-advanced lung cancer in whom other methods of symptom control had been ineffective. Her symptoms were quickly relieved by insertion of the stent. She died 1 month following the procedure, without recurrence of the symptoms. The technical aspects of the procedure and the issues affecting the clinical decision-making process in this case are discussed.
Superior vena cava, obstruction, metal stent, cancer, decision-making
Introduction
Aggressive medical treatments with purelypalliative intent are increasingly being offeredto patients with advanced cancer and other dis-eases. There is much disagreement about theappropriateness of such procedures. On theone hand, they challenge the traditional non-technological paradigm of palliative care.
1
Onthe other hand, many of these procedures arenow minimally invasive, and can have an imme-diate and dramatic positive impact on qualityof life in appropriately selected patients, partic-ularly when simpler approaches have been in-effective.
Superior vena cava (SVC) obstruction is acommon problem in cancer patients, and mayoccur in various contexts. The syndrome maybe a presenting problem in newly diagnosedpatients, a thrombotic complication of centralvascular access in patients receiving chemo-therapy, or a manifestation of progressive dis-ease in patients with advanced cancer. Manage-ment of malignancy-induced SVC obstructionpresents a complex clinical challenge. Giventime, adequate collateral circulation can de-velop and the symptoms resolve spontaneously.As a result, no treatment is usually neededwhen the symptoms are mild. In patients withdistressing symptoms, there are various op-tions. Radiotherapy, chemotherapy, and/orcorticosteroids maybe effective. If not, inser-tion of metal stents can be appropriate. We re-port a case of advanced lung cancer in whichclinical judgment indicated that this approachshould be taken.
Address reprint requests to:
Paul Glare MB BS, Depart-ment of Palliative Medicine, Royal Prince Alfred Hos-pital, Missenden Road, Camperdown NSW 2050,Australia.
Accepted for publication: September 21, 1998.
Vol. 18 No. 1 July 1999 Metallic Stents for SVC Obstruction 57
Case Report
A 75-year-old woman who had been a life-long heavy smoker had a history of cancer ofthe right breast in 1974, was treated by mastec-tomy and axillary dissection followed by exten-sive radiotherapy. She remained well until April1996, when she had an episode of hemoptysis.A chest radiograph showed a large mass in theupper lobe of the right lung. Thoracic comput-erized tomography (CT) scan demonstratedtumor infiltration into the adjacent anteriorchest wall and superior mediastinum. Biopsy ofthe mass confirmed adenocarcinoma, but itwas uncertain whether this was a second pri-mary lung cancer or a late metastasis from herprevious breast cancer. No further radiother-apy could be offered because of her prior man-agement. She was treated with tamoxifen andthen medroxyprogesterone in the hope it wasmetastatic breast cancer.
The patient remained asymptomatic untilMay 1997, when she presented with a short his-tory of the symptoms and signs of SVC obstruc-tion, including shortness of breath at rest, stri-dor, and distention of the neck veins. Chestradiography showed the right lung mass to belarger. She was referred to a palliative care phy-sician and treated with dexamethasone, with agood symptom response within 48 hours.
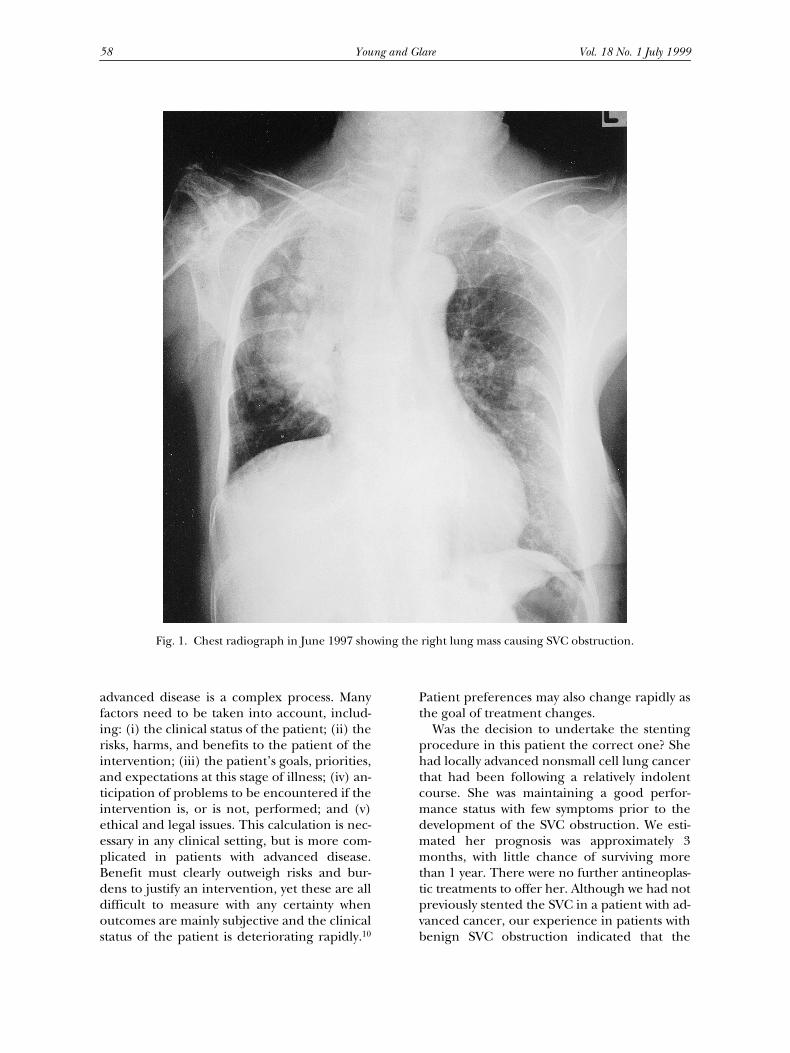
Six weeks later, in mid-June 1997, the pa-tient represented with increasing stridor; swell-ing in the face, neck and arms; and shortnessof breath. The chest radiograph showed themass in the right upper lobe to be much larger,now occupying much of the right lung (Fig. 1).She was very distressed by these symptoms andher scores on a quality-of-life (QOL) question-naire completed on two occasions in the weeksprior to stenting, as part of a separate researchproject, indicated her QOL had fallen from90% of ideal to 70% of ideal as the SVC ob-struction became symptomatic.
Oncologic review was obtained. No furtherradiotherapy was considered possible and che-motherapy was not offered because of the lowprobability that the available agents would ef-fectively palliate her symptoms without causingsubstantial toxicity. Because hormone therapyand corticosteroids were no longer effective,symptom relief by SVC stenting was consideredthe best management option, and the patientwas agreeable to this.
Right arm venography and SVC venographyshowed a high-grade stenosis of the SVC fromtumor encasement and infiltration (Fig. 2). AMemotherm (Angiomed, Karlsruhe, Germany)metal self-expanding stent was placed success-fully across the stricture, with assistance by in-traluminal balloon angioplasty (Fig. 3). Hersymptoms improved dramatically within 24 hours,with resolution of her stridor and improvedshortness of breath. There was also objective re-duction in head, neck, and arm swelling in thefollowing days. The procedure had entailed nocomplications. She returned home 6 days later.
Over the next few weeks, the patient beganto lose weight and became increasingly weak.She had to be admitted to an inpatient hospiceunit where she died a short time later, exactly 1month after stent insertion. There was no re-currence of SVC obstruction clinically.
Discussion
Malignancy is the most common cause of SVCobstruction. Treatment options include radio-therapy, chemotherapy, and surgery.
2–4
Eachhas limitations, and insertion of metallic stentsinto the SVC lumen is an alternative to conven-tional management. The role of this modalityin the palliative care setting is not yet well un-derstood.
Reestablishment of the SVC lumen withmetal stents was first reported in 1986.
5
Severalsmall series have appeared since.
6–9
Rapid reso-lution of the obstruction and the patient’ssymptoms is usually achieved. In one series, themean SVC diameter improved from 3 mm to14 mm with stenting, and the mean pressuregradient across the stenosis fell from 21 mmHg to 3 mm Hg.
7
Complications of this ap-proach are infrequent, with thrombosis, stentmisplacement and migration being the mostcommon. Blockage of the stent by tumor oc-curs rarely.
7
Survival time post-stenting is shortin patients with cancer, usually being less 6months.
8,9
Stent technology and delivery appli-cation is constantly changing. We chose to usea Memotherm metal stent because of its highlyaccurate and simple delivery placement sys-tem. In our patient, balloon angioplasty wasneeded to enable expansion of the stent.
Clinical decision-making regarding the useof modern medical technology in patients with
58 Young and Glare Vol. 18 No. 1 July 1999
advanced disease is a complex process. Manyfactors need to be taken into account, includ-ing: (i) the clinical status of the patient; (ii) therisks, harms, and benefits to the patient of theintervention; (iii) the patient’s goals, priorities,and expectations at this stage of illness; (iv) an-ticipation of problems to be encountered if theintervention is, or is not, performed; and (v)ethical and legal issues. This calculation is nec-essary in any clinical setting, but is more com-plicated in patients with advanced disease.Benefit must clearly outweigh risks and bur-dens to justify an intervention, yet these are alldifficult to measure with any certainty whenoutcomes are mainly subjective and the clinicalstatus of the patient is deteriorating rapidly.
10
Patient preferences may also change rapidly asthe goal of treatment changes.
Was the decision to undertake the stentingprocedure in this patient the correct one? Shehad locally advanced nonsmall cell lung cancerthat had been following a relatively indolentcourse. She was maintaining a good perfor-mance status with few symptoms prior to thedevelopment of the SVC obstruction. We esti-mated her prognosis was approximately 3months, with little chance of surviving morethan 1 year. There were no further antineoplas-tic treatments to offer her. Although we had notpreviously stented the SVC in a patient with ad-vanced cancer, our experience in patients withbenign SVC obstruction indicated that the
Fig. 1. Chest radiograph in June 1997 showing the right lung mass causing SVC obstruction.
Vol. 18 No. 1 July 1999 Metallic Stents for SVC Obstruction 59
benefits of the procedure ought to outweighthe burdens in her case. Relief of the SVC ob-struction was the patient’s main priority andshe expected us to be able to do somethingabout it. We could not envisage problems aris-ing later on as a result of stenting (other thanthe known but uncommon complications ofthe procedure), whereas to do nothing andhope for a collateral circulation to developwould cause avoidable prolongation of her cur-rent suffering.
Thus, we could see no ethical problems withthe intervention. The patient understood whatstent insertion involved, our uncertainty aboutits usefulness in her case, and our belief that se-rious side effects were unlikely. She had abso-lutely no hesitation in submitting herself forthe procedure. Although health care resourcesare limited, and there is much concern aboutthe high costs of care in the last year of life, webelieve the cost of the intervention [venogra-phy ($A 700), the device ($A 1800), and the ra-diologist’s fee ($A 1300)] was justified.
As a result of this analysis, we remain con-vinced that the decision to go ahead with stent-ing was the correct one, and the outcomeachieved supports this view. The patient wasvery satisfied, both in terms of the rapidity ofsymptom control and the minimal burden in-volved. The fact that she lived only 1 month af-ter the procedure may have been disappoint-ing from a cost-effectiveness point of view, butin our opinion only served to vindicate the de-cision to intervene when we did. Those who ad-minister health funds might think otherwise.
In conclusion, insertion of metal stents ap-pears to be a safe, effective way of providingsymptomatic relief in malignant SVC obstruc-tion in the palliative care setting. Interven-tional radiology is widely used in other clinicalcontexts
11
and there is no inherent reason whyit should be denied to patients with far ad-vanced cancer, especially if they have symp-toms that can not be relieved more simply.There is now a vast range of readily performed
Fig. 2. A superior vena cavagram performed via aright femoral vein approach shows significant tumorconstriction (open arrow). The right jugular vein isdistended above the SVC stricture (closed arrow). Fig. 3. A superior vena cavagram performed after
the insertion of the metal stent shows significant, al-though subtotal, alleviation of the stenosis.
60 Young and Glare Vol. 18 No. 1 July 1999
procedures that are safe, well-tolerated, andrapidly effective.
12
Correct identification of ap-propriate patients for such aggressive interven-tions is the major challenge facing palliativecare clinicians. An analysis of the relevant clini-cal and ethical factors can inform the decision-making process.
References
1. Tuch H, Woodrow A. Technology in terminalillness (abst). J Pall Care 1995;11:68.
2. Davenport D, Feree C, Blake D, Raben M. Radia-tion therapy in the treatment of superior vena cavalobstruction. Cancer 1978;42:2600–2603.
3. Perez CA, Presant CA, Van Amburg AL. Man-agement of superior vena cava syndrome. Semin On-col 1978;5:123–124.
4. Chen JC, Bongard F, Klein SP. A contemporaryperspective on superior vena cava syndrome. Am JSurg 1990;160:207–211.
5. Charnsangavej C, Carrasco CH, Wallace S,Wright KC, Ogawa K, Richli W, Gianturco C. Steno-sis of the vena cava: preliminary assessment of treat-ment with expandable metal stents. Radiology 1986;161:295–298.
6. Kazushi K, Sonomura T, Mitsuzane K, NishidaN, Yang R, Sato M, Yamada R, Shirai S, Kobayashi H.Self-expandable metallic stent therapy for superiorvena cava syndrome: clinical observations. Radiology1993;189:531–535.
7. Gaines PA, Belli AM, Anderson P, McBride K,Hemingway AP. Superior vena caval obstructionmanaged by the Gianturco 2 Stent. Clin Rad 1994;49:202–208.
8. Matthijs O, Kuijpers TJA, Schmitz PIM, LoosveldO, de Wit R. Self-expanding metal stents for pallia-tive treatment of superior vena caval syndrome. Car-diovasc Intervent Radiol 1996;19:146–151.
9. Shah R, Sabaratnam S, Lowe RA, Mearns AJ.Stenting in malignant obstruction of superior venacava. J Thorac Cardiovasc Surg 1996;112:335–340.
10. Randall F, Downie RS. Palliative care ethics: agood companion. Oxford: Oxford University Press,1996.
11. Thomson KR. Interventional radiology. Lancet1997;350:354–358.
12. Adam A, Hemingway AP. Interventional radiol-ogy. In: Doyle D, Hanks GWC, Mac Donald N, eds.Oxford textbook of palliative medicine, 2nd ed. Ox-ford: Oxford University Press, 1998:239–249.