J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 7 , 2 0 1 8
ª 2 0 1 8 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
P U B L I S H E D B Y E L S E V I E R
Use of Programmed VentricularExtrastimulus During SupraventricularTachycardia to DifferentiateAtrioventricular Nodal Re-EntrantTachycardia From AtrioventricularRe-Entrant Tachycardia
Hiroyuki Ito, MD,a Nitish Badhwar, MD,b Akash R. Patel, MD,c Kurt S. Hoffmayer, MD, PHARMD,d Joshua D. Moss, MD,b
Cara N. Pellegrini, MD,b,e Vasanth Vedantham, MD, PHD,b Zian H. Tseng, MD,b Ronn E. Tanel, MD,c
Henry H. Hsia, MD,b,e Randall J. Lee, MD, PHD,b Gregory M. Marcus, MD, MAS,b Edward P. Gerstenfeld, MD,b
Melvin M. Scheinman, MDb
ABSTRACT
ISS
Fro
olo
De
of
Ca
We
fro
lat
OBJECTIVES This study hypothesized that early coupled ventricular extrastimuli (V2) stimulation might yield a more
robust differentiation between atrioventricular nodal re-entrant tachycardia (AVNRT) and atrioventricular re-entrant
tachycardia (AVRT).
BACKGROUND Programmed V2 during supraventricular tachycardia are useful to differentiate AVNRT from AVRT by
subtracting the ventriculoatrial (VA) interval from the stimulus to atrial depolarization (stimulus atrial [SA]) interval, but
all such maneuvers have limitations.
METHODS Patients with either AVNRT or AVRT were investigated. The entire tachycardia cycle length (TCL) was
scanned with V2 delivered from the right ventricular apex. The SA�VA difference was calculated with V2 clearly resetting
the tachycardia. The prematurity of V2 was calculated by dividing the coupling interval (CI) by the TCL.
RESULTS A total of 210 patients (102 with AVNRT) were included. The SA�VA difference was >70 ms in all AVNRT
patients and was <70 ms in all AVRT patients with right and septal accessory pathways (APs), except for those with
decremental APs, in whom there was an overlap between AVNRT and AVRT with left APs. However, a SA�VA difference
>110 ms with a CI/TCL of <65% distinguished AVNRT from AVRT using the left AP, with sensitivity and specificity of 87%
and 100%, respectively. Ventricular overdrive pacing resulted in tachycardia termination or AV dissociation in 28% of
patients compared with 15% of patients using the V2 technique (p ¼ 0.008).
CONCLUSIONS A SA�VA of >70 ms using the V2 technique differentiated AVNRT from AVRT using septal
and right APs. Use of the V2 technique with a short CI differentiated AVNRT from AVRT using left APs. The V2
technique less frequently resulted in tachycardia termination compared with ventricular entrainment.
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 7 , 2 0 1 8 Ito et al.J U L Y 2 0 1 8 : 8 7 2 – 8 0 Diagnostic Ventricular Extrastimulus in SVT
873
V arious maneuvers have been reported todifferentiate the mechanism of supraven-tricular tachycardias. Ventricular entrain-
ment is one of the most useful maneuvers toidentify atrial tachycardia by confirming the atrial-atrial-ventricular response (1) and to distinguishatrioventricular nodal re-entrant tachycardia(AVNRT) from atrioventricular re-entrant tachycardia(AVRT) by using the difference between the stimulusatrial (SA) interval after ventricular entrainment andthe ventriculoatrial (VA) interval during tachycardiaor using the difference between the post-pacing inter-val (PPI) and tachycardia cycle length (TCL) (2–4).However, this maneuver often results in terminationof the tachycardia or in AV dissociation, which hasbeen found to occur in 5% to 65% of patients (5–9).By contrast, it has been reported that determinationof SA�VA after resetting with ventricular extrastimuli(V2) is also useful in differentiating AVNRT fromAVRT,but there is still overlap in this parameter betweenAVNRT and AVRT using a free wall accessory pathway(AP) (10). Although many maneuvers have beendescribed to differentiate AVNRT from AVRT, all ofthem have limitations.
The purpose of this study was to test these hy-potheses: 1) whether programmed right ventricular(RV) V2 that reset the tachycardia would be equiva-lent to or superior to ventricular entrainment todistinguish AVNRT from AVRT; and 2) whether theuse of early coupling intervals (CIs) might enhancedifferentiation of AVNRT from AVRT.
METHODS
PATIENT CHARACTERISTICS. Consecutive patientswith AVNRT or AVRT who underwent electrophysio-logical studies in participating centers betweenJanuary 2012 and August 2016 were investigated(prospectively after April 2015). Patients wereexcluded if there were $2 tachycardia mechanisms,tachycardia was not sustained, or TCL varied >30 ms.Patients with antidromic AVRT were also excluded.We evaluated clinical characteristics, including age,sex, body mass index, ejection fraction, and presenceof cardiac disease.
ELECTROPHYSIOLOGICAL STUDY. Electrophysiologicalstudies were performed using standard techniques
All authors attest they are in compliance with human studies committe
institutions and Food and Drug Administration guidelines, including patien
visit the JACC: Clinical Electrophysiology author instructions page.
Manuscript received October 30, 2017; revised manuscript received January
after obtaining written informed consent. Allantiarrhythmic drug therapies were dis-continued at least 5 half-lives before theprocedure. Quadripolar electrode catheterswere inserted into the femoral vein andpositioned in the high right atrium, ante-roseptal tricuspid valve (His bundlerecording), and RV apex. A decapolar elec-trode catheter was also inserted into eitherthe femoral vein or the internal jugular veinand positioned in the coronary sinus (CS).Twelve-lead surface electrocardiograms andintracardiac electrograms were recorded andstored on the Prucka CardioLab (GE Health-care, Little Chalfont, United Kingdom)
recording system. Bipolar intracardiac electrogramswere filtered between 30 and 500 Hz and recorded ata speed of 100 mm/s. Bipolar pacing was performed attwice the diastolic threshold from the distal electrodepair.
Tachycardia was induced by programmed stimu-lation from the RV apex and the high right atrium. Ifthe tachycardia was not inducible or not sustained atbaseline, isoproterenol was infused continuously toaccelerate the sinus rate by >20% or to a sinus rate>100/min, and programmed stimulation wasrepeated. Atrial tachycardia was excluded by thepresence of a ventricular-atrial-ventricular responseafter RV entrainment of the tachycardia. The di-agnoses of AVNRT or AVRT were made according toconventional electrophysiological criteria (4,6), andthe results of a successful ablation site. Patients weredefined as having a slowly conducting AP if the VA/TCL was $40%; they were also defined as having anondecremental AP if the VA/TCL was <40% (11). APsites were divided into right-sided, septal, and leftfree wall pathways.
Entrainment of the tachycardia was attemptedwith RV apical pacing at a cycle length of 10 to 30 msshorter than the TCL. Entrainment was confirmedwhen the atrial cycle length was accelerated to thepacing cycle length with the same atrial activationsequence, and the tachycardia resumed after stop-ping the pacing train. The V2 technique was per-formed by delivering a single RV extrastimulusstarting from a CI 10 ms shorter than the TCL. The CIwas decreased in 10-ms steps until resetting occurredor the ventricular effective refractory period was
es and animal welfare regulations of the authors’
t consent where appropriate. For more information,
FIGURE 1 An Example of the V2 Technique in Patients With AVNRT and AVRT
An example of the ventricular extrastimuli (V2) technique in patients with (A) atrioventricular nodal re-entrant tachycardia (AVNRT) and (B)
atrioventricular re-entrant tachycardia (AVRT). The stimulus was delivered from the right ventricular (RV) apex. The stimulated ventricular beat
clearly advanced the next atrial potential on the high right atrium (HRA) catheter. The stimulus atrial (SA) interval, ventriculoatrial (VA) interval,
and the SA�VA difference by using the V2 technique are shown. CS ¼ coronary sinus.
Ito et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 7 , 2 0 1 8
Diagnostic Ventricular Extrastimulus in SVT J U L Y 2 0 1 8 : 8 7 2 – 8 0
874
TABLE 1 Clinical Characteristics
AVNRT (n ¼ 102) AVRT (n ¼ 108) p Value
Age, yrs 50 � 18 23 � 15 <0.001
Male 47 (46) 66 (61) 0.029
BMI, kg/m2 27.1 � 6.3 23.7 � 6.7 <0.001
EF, % 63 � 5 65 � 6 0.079
Medical history
CAD 3 (3) 2 (1) 0.522
AF 3 (3) 1 (1) 0.238
HTN 20 (22) 8 (7) 0.003
HL 17 (18) 4 (3) <0.001
DM 7 (7) 3 (2) 0.116
Values are mean � SD or n (%).
AF ¼ atrial fibrillation; AVNRT ¼ atrioventricular nodal re-entrant tachycardia;AVRT ¼ atrioventricular re-entrant tachycardia; BMI ¼ body mass index; CAD ¼coronary artery disease; DM ¼ diabetes mellitus; EF ¼ ejection fraction; HL ¼hyperlipidemia; HTN ¼ hypertension.
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 7 , 2 0 1 8 Ito et al.J U L Y 2 0 1 8 : 8 7 2 – 8 0 Diagnostic Ventricular Extrastimulus in SVT
875
reached. Resetting was confirmed when the atrialdepolarization following V2 was advanced or delayedby at least 10 ms without termination of the tachy-cardia. V2 with the shortest CI was used as the pri-mary value for measurement.
MEASUREMENTS AND DEFINITIONS. The SA intervalwas measured from the RV stimulus to the rapiddeflection of the earliest reset atrial electrogram onthe high right atrium or CS recording, whichever wasmore clearly seen during the tachycardia (Figures 1Aand 1B). The VA interval was measured from theonset of the surface QRS complex to the rapiddeflection of the atrial electrogram during tachy-cardia on the same electrode that was used for mea-surement of the SA interval. The SA�VA difference
TABLE 2 Electrophysiological Values and Results of DiagnosticManeuvers
VNRT(n ¼ 102)
AVRT(n ¼ 108) p Value
PR during SR, ms 157 � 38 122 � 31 <0.001
QRS during SR, ms 87 � 14 99 � 20 <0.001
TCL, ms 388 � 65 332 � 59 <0.001
VA interval during SVT, ms 68 � 66 157 � 53 <0.001
V2 technique
Coupling interval, ms 240 � 51 237 � 49 0.694
CI/TCL ratio, % 61 � 7.2 71 � 8.3 <0.001
SA � VA (V2), ms 125 � 24 58 � 35 <0.001
PPI � TCL (V2), ms 142 � 34 95 � 41 <0.001
Ventricular entrainment
SA � VA, ms 131 � 25 53 � 28 <0.001
PPI � TCL, ms 166 � 40 88 � 45 <0.001
Values are mean � SD.
CI ¼ coupling interval; PPI ¼ post-pacing interval; SA interval ¼ stimulus atrial;SR ¼ sinus rhythm; SVT ¼ supraventricular tachycardia; TCL ¼ tachycardia cyclelength; VA ¼ ventriculoatrial.
(SA�VA [V2]) was calculated by subtracting the VAinterval during supraventricular tachycardia from theSA interval obtained by using V2 technique. The PPIwas defined as the interval from the stimulation spikeon the RV electrode to the rapid deflection of the nextsensed ventricular electrogram on the sameelectrode.
STATISTICAL ANALYSIS. For statistical analysis, allanalyses were performed using JMP pro 11 for Win-dows (SAS Institute Inc., Cary, North Carolina).Continuous variables were expressed as the mean �SD, and compared using the Student t test or Mann-Whitney test as appropriate. Nominal variables werecompared by Pearson chi-square analysis. Optimalcutoff values of selected continuous variables to di-agnose the tachycardia were determined by receiver-operating characteristic curve analysis. Sensitivity,specificity, and positive and negative predictivevalues and their corresponding 95% confidence in-tervals were calculated. A p value of <0.05 wasconsidered statistically significant.
RESULTS
CLINICAL CHARACTERISTICS. The V2 technique wassuccessfully performed in 210 patients with AVNRT orAVRT (prospectively in 91 patients and retrospec-tively in 119 patients). Of these, there were 113 (53%)men and 99 women, and their mean age was36.5 � 22.0 years. There were 5 (2%) patients withcoronary artery disease and 28 (13%) patients withhypertension.
AVNRT was diagnosed in 102 patients, whereasAVRT was diagnosed in 108 patients. Clinical char-acteristics of each group are shown in Table 1. Thepatients with AVNRT were significantly older and hada higher body mass index than those with AVRT. Thepercentages of hypertension and hyperlipidemiawere significantly greater in patients with AVNRT.
ELECTROPHYSIOLOGICAL DIAGNOSIS AND VALUES
IN THE STUDY GROUP. Electrophysiological studyrevealed typical (slow-fast) AVNRT in 97 patients,atypical (fast-slow) AVNRT in 5 patients, and AVRTwith a slowly conducting AP in 8 patients (3 left, 4septal, and 1 right APs). The other 100 patients withAVRT showed nondecremental VA conduction (46left, 36 septal, and 18 right APs).
Electrophysiological data are shown in Table 2.During tachycardia, TCL was significantly longer andthe VA interval was significantly shorter in those withAVNRT than in those with AVRT (388 � 65 ms vs. 332� 59 ms and 68 � 66 ms vs. 157 � 53 ms, respectively;p < 0.001).
FIGURE 2 SA�VA Difference and PPI�TCL Using the V2 Technique Sorted by Tachycardia Mechanism
(A) SA�VA difference and (B) post-pacing interval (PPI) � tachycardia cycle length (TCL) using the V2 technique sorted by tachycardia mechanism. The numbers of the
patients in each tachycardia mechanism are shown at the bottom. The dashed line drawn at 70 ms (A) represents the discriminant point between the lowest value in
AVNRT (81 ms) and the highest value in AVRT using a septal and right accessory pathway (AP) (69 ms). Abbreviations as in Figure 1.
FIGURE 3 Scatterp
(A) Comparison betw
lowest value in AVNR
of inclination betwee
and 2.
Ito et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 7 , 2 0 1 8
Diagnostic Ventricular Extrastimulus in SVT J U L Y 2 0 1 8 : 8 7 2 – 8 0
876
SALVA DIFFERENCE AND THE PPILTCL USING THE
V2 TECHNIQUE. The results of V2 technique are alsoshown in Table 2. The SA�VA (V2) was significantlylonger in thosewith AVNRT than in patientswith AVRT(125� 24ms vs. 58� 35ms; p<0.001). PPI–TCL (V2)wassignificantly longer in patients with AVNRT than inthosewith AVRT (142� 34ms vs. 95�41ms; p<0.001).
In all patients with AVNRT, including those withatypical forms, SA�VA (V2) was >70 ms, whereas it
lot of SA�VA Difference Using the V2 Technique (SA�VA [V2]) and CI Div
een AVNRT and AVRT using right APs and AVRT using septal APs. The dashe
T and the highest value in AVRT using a septal and right AP. (B) Comparison
n both mechanisms. Patients with AVRT that used slowly conducting APs wer
was <70 ms in all patients with AVRT using right APsand septal APs (Figure 2A). Furthermore, SA�VA(V2) <45 ms was not seen in patients with AVNRT,in patients with AVRT using left APs, and inpatients with AVRT that used the slowly conductingAP, which narrowed the diagnosis to AVRT using aright or septal nondecremental pathway. By contrast,there was wide overlap in PPI�TCL (V2) between thetachycardia mechanisms (Figure 2B).
ided by CI/TCL Ratio
d line drawn at 70 ms represents the discriminant point between the
between AVNRT and AVRT using left APs. Arrows show the difference
e excluded. CI ¼ coupling interval; other abbreviations as in Figures 1
TABLE 3 Differentiation Between AVNRT and AVRT With Left-Sided AP
CI/TCL(%)
Cutoff(ms)
Sensitivity(%)
Specificity(%)
PPV(%)
NPV(%) p Value AUC
<70 110 82 100 100 65 <0.0001 0.963
<65 110 87 100 100 66 <0.0001 0.973
AP ¼ accessory pathway; AUC ¼ area under the curve; NPV ¼ negative predictive value; PPV¼ positive predictivevalue; other abbreviations as in Table 2.
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 7 , 2 0 1 8 Ito et al.J U L Y 2 0 1 8 : 8 7 2 – 8 0 Diagnostic Ventricular Extrastimulus in SVT
877
RELATIONSHIP BETWEEN THE SALVA DIFFERENCE
AND THE CI/TCL RATIO. The relationship betweenthe SA�VA and CI/TCL ratio using the V2 technique isshown in Figures 3A and 3B. Eight patients with AVRTthat used the slowly conducting AP were excludeddue to marked irregularity in their SA�VA differences(127 � 57 ms). There was a significant negative cor-relation between SA�VA and the CI/TCL ratio for bothAVNRT and AVRT regardless of the AP location.SA�VA with a cutoff of 70 ms differentiated AVNRTfrom AVRT using right and septal APs, regardless ofthe CI. There was overlap between AVNRT and AVRTusing the left APs, but the increase in the SA�VA (V2)was steeper for those with AVNRT. The receiver-operating characteristic curve analysis revealed anoptimal SA�VA (V2), with a cutoff of >110 ms with aCI/TCL ratio of <65% that served to best differentiateAVNRT from AVRT using a left AP with sensitivity,specificity, and positive and negative predictivevalues of 87%, 100%, 100%, and 66%, respectively(Table 3).
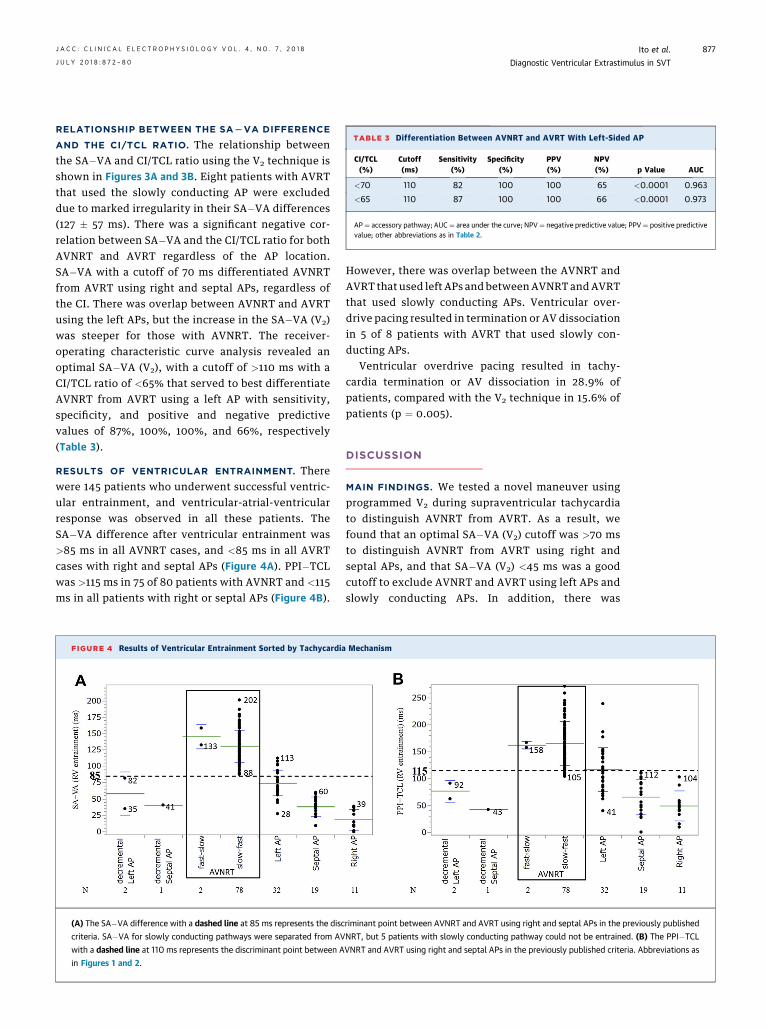
RESULTS OF VENTRICULAR ENTRAINMENT. Therewere 145 patients who underwent successful ventric-ular entrainment, and ventricular-atrial-ventricularresponse was observed in all these patients. TheSA�VA difference after ventricular entrainment was>85 ms in all AVNRT cases, and <85 ms in all AVRTcases with right and septal APs (Figure 4A). PPI�TCLwas >115 ms in 75 of 80 patients with AVNRT and <115ms in all patients with right or septal APs (Figure 4B).
FIGURE 4 Results of Ventricular Entrainment Sorted by Tachycardia
(A) The SA�VA difference with a dashed line at 85 ms represents the disc
criteria. SA�VA for slowly conducting pathways were separated from AV
with a dashed line at 110 ms represents the discriminant point between A
in Figures 1 and 2.
However, there was overlap between the AVNRT andAVRT that used left APs and betweenAVNRT andAVRTthat used slowly conducting APs. Ventricular over-drive pacing resulted in termination or AV dissociationin 5 of 8 patients with AVRT that used slowly con-ducting APs.
Ventricular overdrive pacing resulted in tachy-cardia termination or AV dissociation in 28.9% ofpatients, compared with the V2 technique in 15.6% ofpatients (p ¼ 0.005).
DISCUSSION
MAIN FINDINGS. We tested a novel maneuver usingprogrammed V2 during supraventricular tachycardiato distinguish AVNRT from AVRT. As a result, wefound that an optimal SA�VA (V2) cutoff was >70 msto distinguish AVNRT from AVRT using right andseptal APs, and that SA�VA (V2) <45 ms was a goodcutoff to exclude AVNRT and AVRT using left APs andslowly conducting APs. In addition, there was
Mechanism
riminant point between AVNRT and AVRT using right and septal APs in the previously published
NRT, but 5 patients with slowly conducting pathway could not be entrained. (B) The PPI�TCL
VNRT and AVRT using right and septal APs in the previously published criteria. Abbreviations as
Ito et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 7 , 2 0 1 8
Diagnostic Ventricular Extrastimulus in SVT J U L Y 2 0 1 8 : 8 7 2 – 8 0
878
statistically significant negative correlation betweenSA�VA and the CI/TCL ratio in both AVNRT andAVRT, and SA�VA (V2) >110 ms with a CI/TCLratio <65% was useful to differentiate AVNRT fromAVRT using left APs, with sensitivity and specificityof 87% and 100%, respectively. In addition, V2 wasless likely to cause termination of tachycardia or AVdissociation compared with ventricular entrainment.
PREVIOUS STUDIES. Several reports described thediagnostic value of RV extrastimuli during supra-ventricular tachycardia. Zipes et al. (12) found that aRV extrastimulus during the His refractory periodreset supraventricular tachycardia if an AP was pre-sent. Miles et al. (13) reported the importance of thepre-excitation index in response to a RV extra-stimulus to identify the presence of a left free wallAP. Packer et al. (14) reported the ability and numberof RV extrastimuli to reset supraventricular tachy-cardia to identify the location of the AP using thepre-excitation index. This index was also helpful fordifferentiation of AVNRT from AVRT.
The SA interval is the time period for conductionfrom the stimulation site to the atrium via retrogradeAV node conduction in AVNRT and reflects the con-duction time from the site of ventricular stimulationto the atrium via retrograde AP conduction in ortho-dromic AVRT. Therefore, the results of the SA�VAdifference using the V2 technique should be as usefulas those using ventricular entrainment. Weiss et al.(15) reported that the SA�VA difference after resetwith a RV extrastimulus was longer in those with leftfree wall APs than in those with septal APs, but theydid not show a clear cutoff value and did not distin-guish right free wall APs from AVNRT. García-Fer-nández et al. (10) found that the SA�VA differenceafter reset with single or double RV apex extrastimuliwas useful to differentiate AVNRT from AVRT. How-ever, they combined left and right free wall AP re-sults, and there was overlap between free wall APsand septal APs versus AVNRT. There was also overlapbetween AVNRT and AVRT using left APs in the pre-sent study. It was reasonable that both the SA intervaland the SA�VA difference in AVRT using a left APwould be longer, because the left AP is farther fromthe stimulation site than right or septal APs if thestimulation is delivered from the RV apex.
Generally, it is more challenging to distinguishAVNRT from AVRT using septal or right APs than fromAVRT using left APs, because the latter can be iden-tified by the activation sequence of CS electrodes. Thesimple criterion of the SA�VA difference with a cutoffof <70 ms is reliable in distinguishing AVRT, usingseptal and right APs, from AVNRT. Furthermore, the
SA�VA <45 ms makes this diagnosis more robustcompared with AVRT using a left AP and a slowlyconducting AP.
We did not find a clear cutoff of PPI�TCL (V2) fordistinguishing AVNRT from AVRT, regardless of theAP location. A previous report showed that there wasa significant overlap of PPI�TCL among AVNRT, freewall AVRT, and septal AVRT (7). They suggested theimportance of correcting PPI�TCL by subtracting AVnodal conduction time from the PPI�TCL difference.The results of the present study showed that resettingthe tachycardia with V2 was preferable to using thePPI�TCL to separate AVNRT from AVRT.
COUPLING INTERVAL AND THE SALVA DIFFERENCE.
There are no previous reports that describe the rela-tionship between the CI of the extrastimulus and theSA�VA difference. We found that there was a negativecorrelation between SA�VA and the CI/TCL ratio forAVNRT and AVRT. For those with AVRT using septaland right APs, SA�VA (V2) was always <70 ms,regardless of CI. In the same way, SA�VA (V2) was al-ways >70 ms, regardless of CI in AVNRT. Althoughtherewas overlap betweenAVNRT andAVRT using leftAPs, SA�VA (V2) with a short CI was able to betterdifferentiate between mechanisms by using themagnitude of change in differences at a shorter CI. Wepostulated that this difference was explained by thedecremental nodal conduction in AVNRT comparedwith that of AP-mediated tachycardia. In general, thediagnosis of AVRTwith a left AP was easier than that ofseptal or right APs by considering the atrial activationsequence on the CS catheter, but this simplemaneuvercould be achieved even without use of a CS catheter. Itis noteworthy that some laboratories do not use the CScatheter at the start of the procedure, and in somecountries, cost becomes an important factor in thenumber of catheters that are used.
PROGRAMMED STIMULATION VERSUS VENTRICULAR
ENTRAINMENT. Michaud et al. (4) reported that theSA�VA difference and PPI�TCL after ventricularentrainment were useful in differentiating atypicalAVNRT from AVRT using a septal AP. González-Tor-recilla et al. (2) found that the SA�VA after ventric-ular entrainment was useful in differentiatingatypical AVNRT from AVRT, regardless of the APlocation. Akerström et al. (3) reported that the ma-neuver was useful in all patients with supraventric-ular tachycardia. There is no doubt that ventricularentrainment is useful to diagnose supraventriculartachycardia if it is successfully performed withouttachycardia termination or AV dissociation. A previ-ous report found that entrainment could not beachieved in 15.2% of tachycardias because of
PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE: Several maneu-
vers have been reported for differentiating AVNRT from AVRT,
but all of them have some limitations. In addition, many elec-
trophysiologists want to shorten the time to diagnose supra-
ventricular tachycardia and to reduce the number of catheters
inserted because of concerns about cost. We introduced a simple
maneuver using V2 during supraventricular tachycardia. This
technique differentiated between AVNRT and AVRT regardless of
AP location. Use of the technique may obviate the need for a CS
catheter.
TRANSLATIONAL OUTLOOK: We have shown that this rela-
tively simple technique may be used to quickly diagnose the
mechanism of supraventricular tachycardia. More studies are
required to assess the valve used in the technique to differen-
tiate patients with AVNRT versus decremental APs.
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 7 , 2 0 1 8 Ito et al.J U L Y 2 0 1 8 : 8 7 2 – 8 0 Diagnostic Ventricular Extrastimulus in SVT
879
tachycardia interruption, whereas extrastimuli fromthe RV could be achieved in 99.5% (10). In the presentstudy, the percentage of the cases with evaluabledata was significantly greater with V2 compared withventricular entrainment. Ventricular overdrive pac-ing may cause termination of the tachycardia if animpulse blocks in the orthodromic direction andcollides with the antidromic direction with the pre-vious beat.
There were similar overlaps between AVNRT andAVRT with a left AP in both techniques. It wasreasonable that the SA interval, SA�VA difference,PPI, and PPI�TCL were greater in patients with leftAPs than in those with right or septal APs because thedistance and conduction time from the stimulationsite in the RV to the atrium are greater in those withleft APs compared with other sites. Therefore, theSA�VA in AVRT with the left AP was more likely tooverlap with that in AVNRT compared with AVRTwith right or septal APs. However, use of the V2
technique with the earliest CI effectively separatedleft-sided AP from AVNRT.
AVRT USING SLOWLY CONDUCTING AP. In the studyby Michaud et al. (4), 29 of 44 patients with AVRTusing a septal AP had a long RP (R wave to P wave)interval tachycardia, and all of them had both theSA�VA difference of <85 ms and the PPI�TCLof <115 ms. However, Bennett et al. (11) found thatthe ventricular entrainment criteria for differenti-ating atypical AVNRT from AVRT could not beapplied to AVRT using slowly conducting concealedseptal APs. In the present study, the SA�VA (V2) wasobtained in 8 patients with AVRT using slowly con-ducting APs, but the tachycardia was interrupted byventricular overdrive pacing in 5 patients. In addi-tion, the SA�VA (V2) in these patients was so vari-able that it was difficult to differentiate AVNRT fromAVRT using slowly conducting APs.
STUDY LIMITATIONS. First, this study was a partiallyretrospective analysis with possible unknown con-founders. Second, the number of patients with AVRTthat used slowly conducting APs was small and re-quires further study before any definitive statementcan be made. Another study limitation was that we
could not comment on the incremental value of addi-tional pacing techniques (i.e., para-Hisian pacing ordifferential site pacing) because further diagnosticmaneuvers were left to the discretion of the operators.
CONCLUSIONS
This was a study in which the single V2 was tested fordistinguishing AVNRT from AVRT. A SA�VA (V2) of>70 ms using the V2 technique proved to be excellentfor differentiation of AVNRT from AVRT using septalor right APs. However, there was overlap betweenAVNRT and AVRT with left APs. A SA�VA (V2) of >110ms with a short CI (<65% TCL) effectively differenti-ated AVNRT from AVRT with left APs. The V2 tech-nique less frequently resulted in tachycardiatermination compared with ventricular overdrivepacing. The small number of cases with decrementalAPs did not allow for definitive conclusions.
ADDRESS FOR CORRESPONDENCE: Dr. Hiroyuki Ito,Division of Cardiology, Department ofMedicine, ShowaUniversity, 1-5-8 Hatanodai, Shinagawa-ku, Tokyo142-8666, Japan. E-mail: [email protected].
RE F E RENCE S
1. Knight BP, Zivin A, Souza J, et al. A techniquefor the rapid diagnosis of atrial tachycardia in theelectrophysiology laboratory. J Am Coll Cardiol1999;33:775–81.
2. González-Torrecilla E, Almendral J,García-Fernández FJ, et al. Differences inventriculoatrial intervals during entrainment
and tachycardia: a simpler method for dis-tinguishing paroxysmal supraventriculartachycardia with long ventriculoatrial in-tervals. J Cardiovasc Electrophysiol 2011;22:915–21.
3. Akerström F, Pachón M, García-Fernández FJ,et al. Performance of the SA-VA difference to
differentiate atrioventricular nodal re-entranttachycardia from orthodromic re-entrant tachy-cardia in a large cohort of consecutive patients.Pacing Clin Electrophysiol 2015;38:1066–72.
4. Michaud GF, Tada H, Chough S, et al.Differentiation of atypical atrioventricular nodere-entrant tachycardia from orthodromic
Ito et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 4 , N O . 7 , 2 0 1 8
Diagnostic Ventricular Extrastimulus in SVT J U L Y 2 0 1 8 : 8 7 2 – 8 0
880
reciprocating tachycardia using a septal accessorypathway by the response to ventricular pacing.J Am Coll Cardiol 2001;38:1163–7.
5. HoRT,MarkGE, RhimES, Pavri BB, GreensponAJ.Differentiating atrioventricular nodal re-entranttachycardia from atrioventricular re-entrant tachy-cardia by DeltaHA values during entrainment fromthe ventricle. Heart Rhythm 2008;5:83–8.
6. Segal OR, Gula LJ, Skanes AC, Krahn AD, Yee R,Klein GJ. Differential ventricular entrainment: amaneuver to differentiate AV node re-entranttachycardia from orthodromic reciprocatingtachycardia. Heart Rhythm 2009;6:493–500.
7. González-Torrecilla E, Arenal A, Atienza F, et al.First postpacing interval after tachycardiaentrainment with correction for atrioventricularnode delay: a simple maneuver for differentialdiagnosis of atrioventricular nodal re-entranttachycardias versus orthodromic reciprocatingtachycardias. Heart Rhythm 2006;3:674–9.
8. Knight BP, Ebinger M, Oral H, et al. Diagnosticvalue of tachycardia features and pacing maneu-vers during paroxysmal supraventricular tachy-cardia. J Am Coll Cardiol 2000;36:574–82.
9. Dandamudi G, Mokabberi R, Assal C, et al.A novel approach to differentiating orthodromicreciprocating tachycardia from atrioventricularnodal re-entrant tachycardia. Heart Rhythm 2010;7:1326–9.
10. Javier García-Fernández F, Almendral J,Marta Pachón, González-Torrecilla E, Martín J,Gallardo R. Differentiation of atrioventricularnodal re-entrant tachycardia from orthodromicreciprocating tachycardia by the resettingresponse to ventricular extrastimuli: compari-son to response to continuous ventricularpacing. J Cardiovasc Electrophysiol 2013;24:534–41.
11. Bennett MT, Leong-Sit P, Gula LJ, et al.Entrainment for distinguishing atypical atrio-ventricular node re-entrant tachycardia fromatrioventricular re-entrant tachycardia overseptal accessory pathways with long-RPtachycardia. Circ Arrhythm Electrophysiol 2011;4:506–9.
12. Zipes DP, DeJoseph RL, Rothbaum DA. Unusualproperties of accessory pathways. Circulation1974;49:1200–11.
13. Miles WM, Yee R, Klein GJ, Zipes DP,Prystowsky EN. The preexcitation index: an aid indetermining the mechanism of supraventriculartachycardia and localizing accessory pathways.Circulation 1986;74:493–500.
14. Packer DL, Ellenbogen KA, Colavita PG,O’Callaghan WG, German LD, Prystowsky EN.Utility of introducing ventricular prematurecomplexes during reciprocating tachycardia inspecifying the location of left free wallaccessory pathways. Am J Cardiol 1989;63:49–57.
15. Weiss J, Brugada P, Roy D, Bär FW, Wellens HJ.Localization of the accessory pathway in theWolff-Parkinson-White syndrome from theventriculo-atrial conduction time of right ventric-ular apical extrasystoles. Pacing Clin Electro-physiol 1983;6:260–7.
KEY WORDS coupling interval, prematureventricular extrastimulus, supraventriculartachycardia, ventricular entrainment,ventriculoatrial interval